
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Neurol., 15 June 2023
Sec. Dementia and Neurodegenerative Diseases
Volume 14 - 2023 | https://doi.org/10.3389/fneur.2023.1210974
This article is part of the Research TopicImpacts of Public-Private Collaborative Research on Alzheimer's Disease: The Case of the Innovative Medicines InitiativeView all 12 articles
 Anna-Katharine Brem1,2*
Anna-Katharine Brem1,2* Sajini Kuruppu1
Sajini Kuruppu1 Casper de Boer3,4Marijn Muurling3,4
Casper de Boer3,4Marijn Muurling3,4 Ana Diaz-Ponce5
Ana Diaz-Ponce5 Dianne Gove5
Dianne Gove5 Jelena Curcic6
Jelena Curcic6 Andrea Pilotto7,8,9
Andrea Pilotto7,8,9 Wan-Fai Ng10,11
Wan-Fai Ng10,11 Nicholas Cummins12Kristina Malzbender13Vera J. M. Nies14
Nicholas Cummins12Kristina Malzbender13Vera J. M. Nies14 Gul Erdemli15Johanna Graeber16Vaibhav A. Narayan17Lynn Rochester18,19
Gul Erdemli15Johanna Graeber16Vaibhav A. Narayan17Lynn Rochester18,19 Walter Maetzler20
Walter Maetzler20 Dag Aarsland1,21
Dag Aarsland1,21  on behalf of the RADAR-AD Consortium
on behalf of the RADAR-AD ConsortiumAlzheimer’s disease (AD) and other neurodegenerative diseases such as Parkinson’s disease (PD) and Huntington’s disease (HD) are associated with progressive cognitive, motor, affective and consequently functional decline considerably affecting Activities of Daily Living (ADL) and quality of life. Standard assessments, such as questionnaires and interviews, cognitive testing, and mobility assessments, lack sensitivity, especially in early stages of neurodegenerative diseases and in the disease progression, and have therefore a limited utility as outcome measurements in clinical trials. Major advances in the last decade in digital technologies have opened a window of opportunity to introduce digital endpoints into clinical trials that can reform the assessment and tracking of neurodegenerative symptoms. The Innovative Health Initiative (IMI)-funded projects RADAR-AD (Remote assessment of disease and relapse—Alzheimer’s disease), IDEA-FAST (Identifying digital endpoints to assess fatigue, sleep and ADL in neurodegenerative disorders and immune-mediated inflammatory diseases) and Mobilise-D (Connecting digital mobility assessment to clinical outcomes for regulatory and clinical endorsement) aim to identify digital endpoints relevant for neurodegenerative diseases that provide reliable, objective, and sensitive evaluation of disability and health-related quality of life. In this article, we will draw from the findings and experiences of the different IMI projects in discussing (1) the value of remote technologies to assess neurodegenerative diseases; (2) feasibility, acceptability and usability of digital assessments; (3) challenges related to the use of digital tools; (4) public involvement and the implementation of patient advisory boards; (5) regulatory learnings; and (6) the significance of inter-project exchange and data- and algorithm-sharing.
Digital endpoints in clinical trials are being investigated increasingly in large-scale international projects. The rapid advancement of technological developments allows entirely new approaches to assessing activities of daily living (ADL), sleep and fatigue, motor, cognitive, social, neuropsychiatric, and autonomous body functions with potential for both trials and clinical practice. The appeal lies in the objective, immediate and continuous measurement in both clinical and home settings, the reduction of visits to research or clinic facilities, the accessibility for under-served populations, the potential for better stratification and more personalised therapies, and the possibility to support otherwise time-intense clinical decisions with Artificial Intelligence (AI). This is of specific importance for Alzheimer’s disease (AD), but also other neurodegenerative diseases, such as Parkinson’s disease (PD) and Huntington’s disease (HD), with a predominantly slow progression over years as well as cognitive impairment and fluctuations, which reduce the validity of data from self-rated or one-time assessments.
Functional decline is a significant indicator of progression of neurodegenerative diseases. A range of questionnaires have been developed to assess ADL (1). However, many of these instruments lack sensitivity to change in early stages of a disease and therefore have a limited utility as outcome measures in clinical trials (2, 3). This is of specific importance considering recent developments in disease-modifying drugs for the treatment of AD, such as aducanumab and lecanemab (4) that are targeting early cognitive impairment and emphasise the need for highly sensitive methods. Similar restrictions apply to standard mobility and neuropsychological testing and the query of social skills, sleep, fatigue, neuropsychiatric symptoms, and autonomous body functions with self- and informant-rating questionnaires. Standard assessments are intermittent, costly, and partly rely on subjective information, which is especially problematic in later stages of a neurodegenerative disease. The common goal of the Innovative Health Initiative (IMI)-funded projects RADAR-AD, IDEA-FAST and Mobilise-D is to define digital endpoints relevant for neurodegenerative diseases that provide reliable, objective, and sensitive evaluation of disability, ADL, and health-related quality of life.
RADAR-AD (EC Grant No.806999; www.radar-ad.org) aims to identify and validate remote monitoring technologies (RMTs) to assess functional impairment in all stages of Alzheimer’s disease. The study includes wearables and smartphone apps in the main study (n = 232) and passive at-home sensors in a sub-study (n = 45). The RMTs measure a wide range of cognitive and functional domains, including spatial navigation, activity, sleep, speech, driving behaviour, and gait (5).
IDEA-FAST (EC Grant No. 853981; www.idea-fast.eu) aims to identify digital parameters in patients with PD and HD, and immune-mediated disorders, which are related to fatigue, sleepiness, and sleep quality. A pilot study (6, 7) has informed the design of a larger clinical observational study using different devices concurrently to capture data on ADL-related activities, sleep, physiological and cognitive/psychological variables. In the latter study, up to 2000 participants (PD n = 500; HD n = 200) will be recruited at up to 24 sites across Europe.
Mobilise-D (EC Grant No. 820820; www.mobilise-d.eu) (8) aims to validate a suite of digital mobility outcomes to directly monitor mobility performance continuously over a 7 day duration using a single wearable device in PD (n = 600) and other diseases associated with mobility impairment (chronic obstructive pulmonary disease, multiple sclerosis, proximal femoral fracture) (9, 10).
In this article, we will draw from the findings and experiences of these different IMI projects in discussing (1) the value of remote technologies to assess neurodegenerative diseases; (2) feasibility, acceptability and usability of digital assessments; (3) challenges related to the use of digital tools; (4) public involvement and the implementation of patient advisory boards to guide clinical trials in terms of protocol design, ethical issues, and selection and applicability of digital tools; (5) regulatory learnings; and (6) the significance of inter-project exchange and data- and algorithm-sharing (Figure 1).
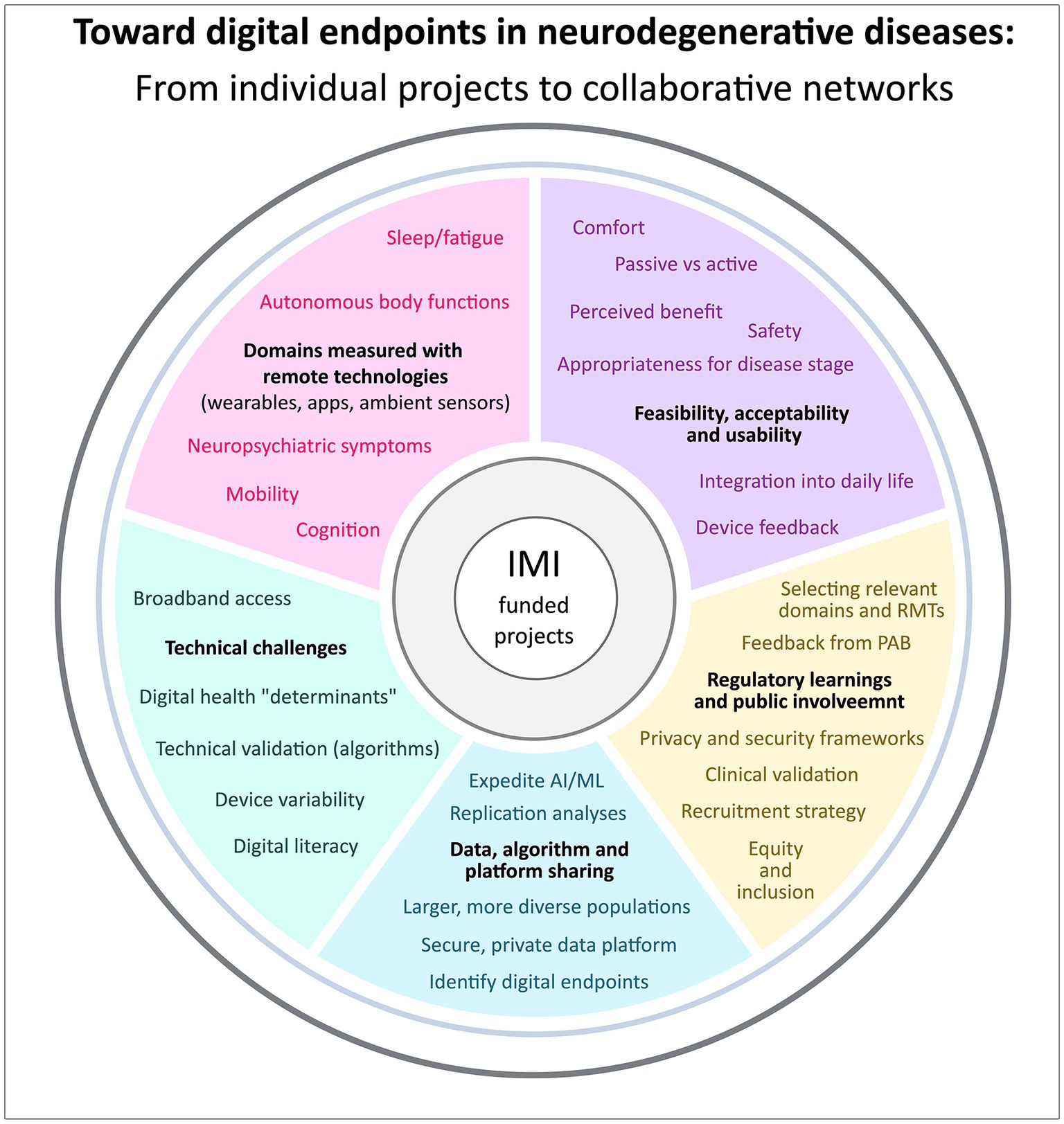
Figure 1. Findings and experiences of RADAR-AD, IDEA-FAST, and Mobilise-D in (1) remote technologies to assess neurodegenerative diseases, (2) feasibility, acceptability and usability of digital assessments, (3) challenges related to the use of digital tools, (4) regulatory learnings and public involvement, and (5) data, algorithm and platform sharing.
Technological advances in the last decade opened a window of opportunity to introduce digital endpoints into clinical trials. RMTs could provide a useful, objective way to measure decline by collecting data that correspond to various functional domains that are clinically relevant. They assess functional ability either passively (i.e., not requiring any interaction with the device, such as is the case with gait measures) or interactively (i.e., requiring an active interaction with the device such as when assessing functional abilities involving cognition). The benefit of RMTs as compared to standard assessments, is that they are objective and can collect data in the real world continuously. They are ideally placed to potentially measure subtle functional changes that are prevalent among individuals in the early, preclinical stages of neurodegenerative diseases, where current methods of cognitive assessments lack the necessary sensitivity (11) and to continuously track changes during the course of a disease. The RMTs used in the different consortia are listed in Table 1.
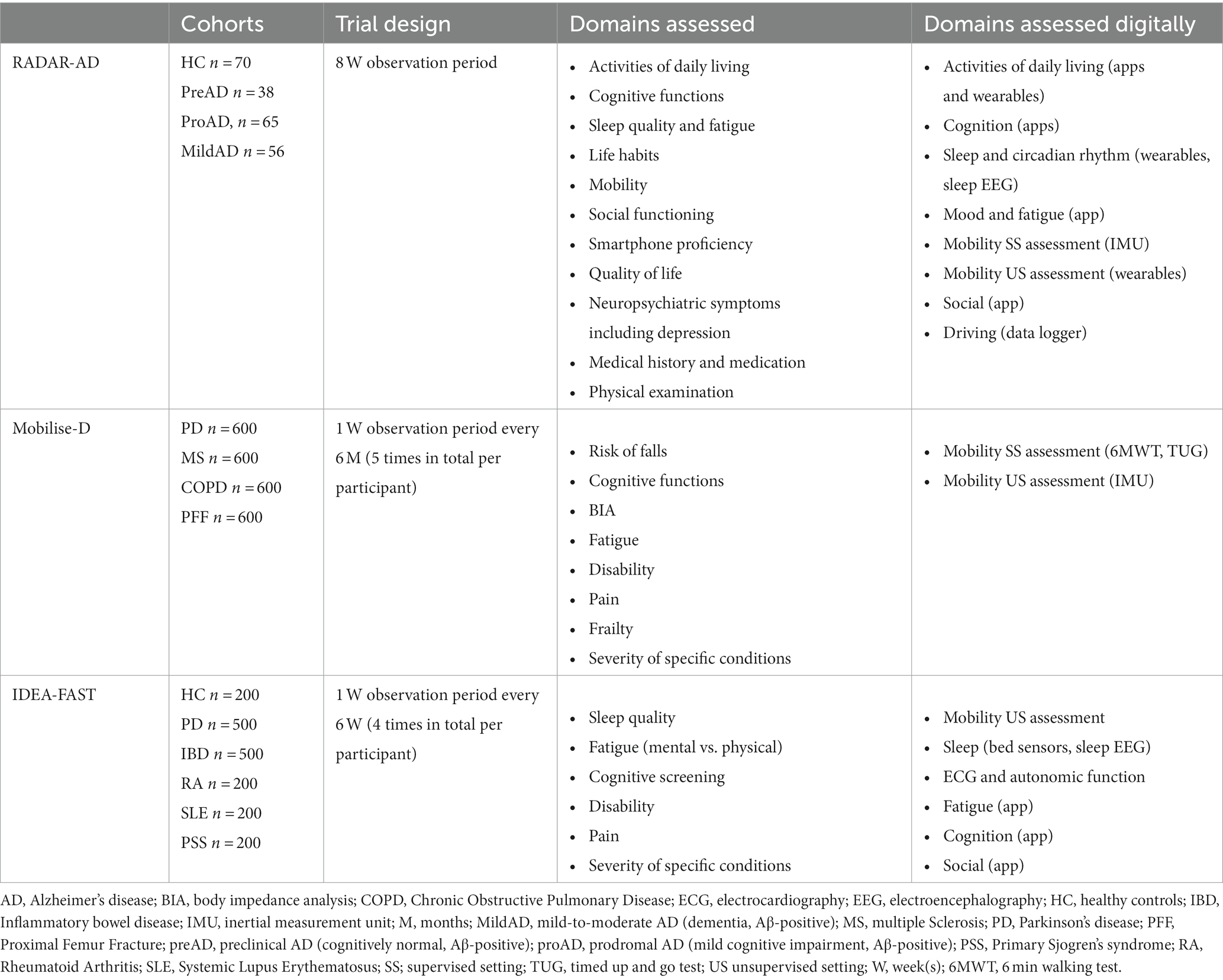
Table 1. Domains assessed in the three IMI-funded consortia RADAR-AD, IDEA-FAST, and Mobilise-D.
In the three consortia, different functional domains were measured. Mobility, for example, was evaluated in various ways within the IMI projects. Mobilise-D applied both supervised (in the presence of study staff) and unsupervised testing using a standardised protocol. In addition to that, home mobility was evaluated using an inertial measurement unit (IMU) for 7 days at different time points. In RADAR-AD, mobility was evaluated using a supervised standardised protocol as well, and home mobility using a wrist-worn IMU for 8 consecutive weeks. In both RADAR-AD and IDEA-FAST, heart rate was measured using a wearable. Another functional domain assessed was sleep. IDEA-FAST and RADAR-AD both made use of an app to actively collect data on sleep, asking the participants daily about their fatigue, sleep pattern and quality. Moreover, sleep was measured passively: RADAR-AD made use of a portable EEG device, which a subset of participants wore every night for a month, while IDEA-FAST used a bed sensor with a force-sensitive piezo-electric film, placed under the mattress. Cognition has been addressed in a supervised standardised way in all consortia. Cognitive data was evaluated remotely using several smartphone apps in RADAR-AD and a web-based application of CANTAB in IDEA-FAST and both consortia collected passive information on smartphone use, including keyboard metrics and GPS location tracking.
Future clinical trials will profit from these recent technological developments, which promise improved sensitivity and specificity of endpoint measures, better external validity, and the need of fewer visits to research or clinical facilities and smaller sample sizes due to more detailed datasets per participant.
The use of RMTs can present challenges with respect to a range of aspects including the validity of measurements, related to sensitivity and specificity (e.g., differentiating sensor information in multi-person households), data quality, e.g., choosing the right time granularity (12), data missingness, which is often due to technical and software issues (13), and subsequent analysis. The use of Artificial Intelligence (AI) to combine and analyse RMT signals brings a multitude of challenges itself (14), including privacy and security concerns (15), gaining informed consent (16), and ethical challenges. These can be addressed by creating regulatory frameworks and promoting public-private partnerships (17). Ensuring equity and inclusion when deploying digital tools is another important challenge. Connectivity and broadband access, device variability/obsolescence and digital literacy are “digital determinants of health” that impact equitable access to digital healthcare and the outcomes from and experience with digital tools (18). To date, 37% of the world’s population has never used the internet. In the European Union, the percentage of older people (aged 65–74) using the internet varies greatly from 25% in Bulgaria to 94% in Denmark and we face a growing age gap in smartphone ownership in emerging economies around the globe (19). Even if a smartphone or PC is available in a household, access might still be restricted due to financial or technical reasons (20). Digital health studies have developed approaches such as “bring-your-own-device studies” (21), providing funding for internet connectivity, or using sensors that are not (continuously) connected to the internet to help address these challenges. Collocation and sharing of best practices across projects will help address these challenges.
It becomes increasingly important to consider the feasibility, acceptance, usability, and ecological validity of digital endpoints in real-world settings. Few studies report on these factors and ageing populations are not well represented in RMT research (22), but are explored in RADAR-AD, IDEA-FAST and Mobilise-D in collaboration with patients and carers. In studies involving wearables and smartphone apps, acceptance to use devices and adherence to protocol are in general positive when they are reported (23, 24). For example, the comfort and acceptability of a wearable sensor to monitor mobility in the Mobilise-D study was very high (23). However, many studies to date lack information on acceptability, adherence and usability (24). Overall, passive devices/apps requiring little or no interaction with a device show higher feasibility, acceptability and usability than interactive devices and are the most researched to date (25). Research in PD reports that the successful implementation of digital technologies is primarily driven by familiarity with the technology and ease of use, costs, motor symptoms hampering the use, experiencing beneficial effects, and feeling safe whilst using the technology (26). In AD, acceptance and adherence can be facilitated by familiarising participants with the devices and providing personal support, lowering technical demands, co-designing solutions and involving relevant stakeholders, introducing participants to the devices at the earliest stages of the disease, and increasing the perception of effectiveness and safety. Barriers mainly include technology anxiety, system failures, and lack of access (27, 28). However, if these factors are addressed, adherence is generally high (85.7%) in older adults (29).
Some of these barriers became apparent in RADAR-AD. For example, engaging with RMTs led to some participants feeling discouraged, as they acted as a reminder for their declining cognition. Cognitive impairment also led to missing data, e.g., participants removed their wearables before going to bed, meaning sleep hygiene could not be tracked. Study partners are essential when it comes to reducing or overcoming (cognitive) barriers—they help with charging/handling RMTs, provide emotional support, and remind participants to keep wearing/using RMTs. Overall, study partners are vital in the adherence and usability of digital tools in neurodegenerative diseases (Muurling et al., submitted)1. In RADAR-AD and IDEA-FAST, participants reported adjustments to daily routines; specifically, acclimating to wearing two wrist-worn wearable devices, using their phone more, and adjusting personal schedules to complete their daily app-based tasks on time. Ergonomic challenges were reported due to the physical design of watches (i.e., watch straps not fitting well or feeling limited in their movements). Similar findings have been collated within multiple systematic reviews on digital tool use in older adults (28, 30, 31). Participants reported individual preferences for the display of the wearable screen (e.g., matching the clock face of their usual watch) and for device feedback (e.g., cognition and activity tracking), which facilitated integration into daily routines. Lack of, or inaccurate device feedback, small screens and small fonts also contributed towards the challenges faced by participants. In the IDEA-FAST pilot study, participants moreover mentioned skin irritations due to adhesive patches, constant worry about the device and insecurities regarding its proper functioning. Also, participants reported being less willing to wear devices that were very visible, complicated to use, or that had to be manipulated at impractical times, e.g., right before sleeping. The roadmap towards translating RMT use from research to clinical practice has to continue to evolve, together with patient and stakeholder involvement, as the benefits and challenges are evaluated (32).
Public Involvement (PI) is about involving people affected by the condition in all aspects of the research process as partners rather than as research participants (33, 34). PI not only provides the patients’ perspective on what research is important and which unmet needs should be addressed, but it is also about understanding and anticipating what aspects of the research may be difficult to manage by the participants, may raise concerns, and how these issues could be addressed. It also involves reflecting about future issues, challenges, and benefits of the project, if and when the results are eventually implemented in the real world. Involving people from minority ethnic groups and other under-served populations is crucial but still remains a challenge (33).
All three consortia involved patients and, in the case of RADAR-AD, also carers in special advisory boards. They provided strategic input to various aspects of consortium activities throughout the projects, including: study protocols and participant-facing documents; digital health technology in general and digital assessments and outcomes in particular; feasibility, usability and acceptability of digital outcome assessment and how it can contribute to improved care; consultation around health technology assessment and regulatory acceptance of digital outcomes; ethical considerations, recruitment and retention strategies; and involvement in promotion activities about the impact and benefits of results. RADAR-AD and IDEA-FAST also collaborated with patient organisations and in IDEA-FAST, two additional groups consisting of patients, consortium members and representatives from patient organisations were formed to develop and review the project activities and to support the design of the two clinical studies.
If digital endpoints are to be used in clinical trials aimed to achieve a market authorisation for medicinal products, it is of paramount importance that the endpoints are accepted by the regulatory authorities. In recent years, the use of RMT-based assessments has increased dramatically (35). However, the number of digital endpoint measures that are qualified is still limited (36) and there are no approved primary or secondary digital endpoints for use in clinical trials in AD or PD yet (35, 37). In RADAR-AD, a regulatory strategy was developed early on, including an extensive evaluation of all qualification opinions and advices and scientific advices of the EMA to gain insight in the types of tools that are intended to be used in clinical trials for supporting/submitting applications for obtaining market authorization (registration trials) (36). The EMA recommendations evolved mainly around the relevance, precision, and accuracy of novel endpoints; validation with current gold standards and clinically meaningful legacy endpoints, including those that matter most to patients (“daily-relevant data”); sensitivity and specificity; good compliance and acceptability; and guarantee of optimal data security and privacy. The RADAR-AD consortium had an initial meeting with the Innovation Task Force in 2020 and is currently in the process of having a Qualification Advice discussion with EMA. The Mobilise-D consortium had two consecutive EMA qualification advices in 2020 (38, 39) and a letter of support was published on the EMA website (40, 41) following each qualification advice. Mobilise-D has furthermore interacted with the Food and Drug Administration (FDA). The IDEA-FAST consortium had two meetings with the EMA between 2020 and 2022. The first meeting with the Innovation Task Force was to discuss the general concepts of developing digital endpoints for fatigue and sleep. The second meeting was to discuss the study design and data analytic plan of a clinical study to identify these digital endpoints which was given general support by the Scientific Advice Working Party.
It is highly recommended for similar consortia to develop a regulatory strategy early on, to ensure that what is being developed will also be accepted in drug trials. It is important to plan for multiple Health Authority meetings utilising Innovation Task Force and EMA Qualification advice meetings as well as meetings with other major Health Authorities, as appropriate. Early advice on study design prior to protocol finalisation/study initiation would be highly desirable. Further development of clear guidance for the use of digital technologies in registration trials could remove some of the regulatory hurdles that currently complicate the development and use of novel improved endpoints (42).
To extend and generalise individual project findings and foster deeper understanding of digital outcomes across neurodegenerative diseases, inter-project exchange and data sharing has gained significance. The full value of data collected in large research programmes can only be realised by enabling a wider set of analytics than is possible through individual consortia. This need is only heightened by the current rapidly expanding popularity in AI and Machine Learning research which relies on large datasets. Sharing resources allows for more rapid research to be undertaken, leading to greater efficacy in terms of advancing state-of-the-art than could be otherwise be achieved working on the data in isolation. For example, the sharing of speech data through DementiaBank (43) has enabled a wide range of different machine learning approaches to be compared and assessed on a common database (44). In such a rapidly growing area of research it is also important to conduct replication analysis and robust generalised testing of proposed digital phenotypes. Sharing and open sourcing algorithms enables these vitally important verification steps.
The sharing of data requires careful considerations to preserve the privacy of participants in a manner that not only meets ethical and statutory requirements, but also meets participants’ expectations regarding distribution of their data. Entire IMI-projects have developed around this topic. For example, the European Platform for Neurodegenerative Diseases (EPND, www.epnd.org) aims to accelerate the discovery of diagnostics and treatments for neurodegenerative diseases by removing barriers to data and sample sharing (45). This includes sharing of digital data, by building a robust and secure data sharing infrastructure and funding a case study of prospective digital (bio)marker data collection. EPND aims to build connections to existing data platforms and facilitate the discoverability of resources; provide secure, private cloud-based workspaces where researchers can perform and save analyses; collaborate with other permissioned users; and develop ethical, legal, and regulatory principles guiding platform design and discovery and sharing of data.
The access to and reuse of research data generated by Horizon 2020 projects is available through the Open Research Data Pilot (ORD Pilot), which is in line with the FAIR (Findable, Accessible, Interoperable, Reusable) principles2 and ensures open access to publications and research data (curated and raw data) including access to, e.g., specialised software or software code, algorithms, and analysis protocols. This allows to build on previous research findings, foster collaboration, promote innovation, and improve transparency in research (46). New projects can be greatly strengthened by reusing infrastructure, such as RADAR-base, and sharing algorithms between consortia that use similar RMTs, such as RADAR-CNS, in the case of RADAR-AD.
We argue that sustainability should be plannable and funded beyond the duration of a project, ideally via IMI-funded platforms, to guarantee a lasting impact and allow following projects to profit from the large data volumes produced by RMTs, previous experiences, including cross-learning about device selection and barriers/facilitators of using digital health technology, especially for studies that are targeting similar demographics and conditions.
Technological advances and collaboration between IMI-funded and other consortia bring new opportunities to develop and introduce digital endpoints into clinical trials that can revolutionise the assessment and tracking of neurodegenerative symptoms. The digitalization of endpoints allows for objective, immediate and continuous measurement in both clinical and home settings, the reduction of visits to research or clinic facilities, greater accessibility for under-served populations, better stratification and more personalised interventions, and AI-supported clinical decisions.
Dag Aarsland, Halil Agin, Vasilis Alepopoulos, Alankar Atreya, Sudipta Bhattacharya, Virginie Biou, Joris Borgdorff, Anna-Katharine Brem, Neva Coello, Pauline Conde, Nick Cummins, Jelena Curcic, Casper de Boer, Yoanna de Geus, Paul de Vries, Ana Diaz, Richard Dobson, Aidan Doherty, Andre Durudas, Gul Erdemli, Amos Folarin, Suzanne Foy, Holger Froehlich, Jean Georges, Dianne Gove, Margarita Grammatikopoulou, Kristin Hannesdottir, Robbert Harms, Mohammad Hattab, Keyvan Hedayati, Chris Hinds, Adam Huffman, Dzmitry Kaliukhovich, Irene Kanter-Schlifke, Ivan Koychev, Rouba Kozak, Julia Kurps, Sajini Kuruppu, Claire Lancaster, Robert Latzman, Ioulietta Lazarou, Manuel Lentzen, Federica Lucivero, Florencia Lulita, Nivethika Mahasivam, Nikolay Manyakov, Emilio Merlo Pich, Peyman Mohtashami, Marijn Muurling, Vaibhav Narayan, Vera Nies, Spiros Nikolopoulos, Andrew Owens, Marjon Pasmooij, Dorota Religa, Gaetano Scebba, Emilia Schwertner, Rohini Sen, Niraj Shanbhag, Laura Smith, Meemansa Sood, Thanos Stavropoulos, Pieter Stolk, Ioannis Tarnanas, Srinivasan Vairavan, Nick van Damme, Natasja van Velthogen, Herman Verheij, Pieter Jelle Visser, Bert Wagner, Gayle Wittenberg, and Yuhao Wu.
Full membership of the Mobilise-D consortium is available on the website http://mobilise-d.eu/wp-content/uploads/2023/06/v9-logos_06.17.2022_Mobilise-D-consortium-members-names.pdf.
Wan-Fai Ng, Christopher Bull, John Isaacs, Chris Lamb, Alison Yarnall, Lynn Rochester, Silvia Del Din, Chloe Hinchliffe, David Halliday, Ashur Rafiev, Bing Zhai, Dan Jackson, Peter Gallagher, Victoria MacRa, Leigh Denley, Ellen Silva, Philip Brown, Helen Gallon, Sean Scott, Phillip McGrouther, Dean Miller, Darren Storey, Lee Briton, Walter Maetzler, Kirsten Emmert, Robert Goeder, Jennifer Kudelka, Corina Maetzler, Hanna Kaduszkiewicz, Tanja Lange, Marie Bornhorst, Hanna Grasshoff, Stefan Schreiber, Sophia Hinz, Friso Muijsers, Kristina Brandt, Tina Hagen-Hurley, Robbin Romijnders, Clint Hansen, Linda Pialek, Kirstin Hansen, Johanna Graeber, Susanna Nikolaus, Florian Schrinner, Pia Görrissen, Paula Cullen, Maren Williams, Andrea Pilotto, Alessandro Padovani, Sabrina Denardi, Giulio Bonzi, Marcello Catania, Valentina Chirico, Fiorenza Cavagnini, Christen Janneke van de Woude, Nynke Borren, Monique Devillers, Nicole Larmonie, Denise Schenk, Hans van Leeuwen, Jorina van der Salm, Iain McInnes, Neil Basu, Joe Galloway, Norelee Kennedy, Alexander Fraser, Hayley Connolly, Sadhbh Ni Mhidigh, Imelda Doolan, Cathal Linnane, Jacques Demotes-Mainard, Linda Stöhr, Neshat Chareh, Hanna Schrinner-Fenske, Martina Esdaile, Alicja Szofer-Araya, Costantino Pitzalis, Michele Bombardieri, Louise Warren, Myles Lewis, Paul Giuliani, Sharon Palmer, Vicky Byers, Yi-Ke Guo, Kai Sun, Danilo Mandic, Mary Morrell, Siyao Wang, Florian Guitton, Yifeng Mao, Ailsa Hart, Shaun Power, Guanyu Tao, Benjamin Vandendriessche, Arno Bossaert, Rebeca Munoz, Hans De Clercq, Pierrick Arnal, Bertrand Fatus, Evgeniia Kurash, Maya Dorsey, Miles Parkes, Sree Subramanian, Louise Stockley, Rona Smith, Renata Schaeffer, Jérôme Kalifa, Jonathan Chauvin, Clémence Pinaud, Adrien Bennetot, Alexandra Belfiore, Laura Carrasco Marin, Mayca Marín, Jennifer Jimenez, Miriam Grande, Susana Donate, Evert-Ben van Veen, Daniel Groos, Martin Boeckhout, Beatrice van der Velden, Olenka van Ardenne, Denis Groot, Nebo Savic, Irene Schluende, Franziska Klepka, Simon Beniston, Veli Stroetmann, Rainer Thiel, Daniel Schmidtmann, Karin Breuer, Jessica Paul, Shahan Tariq, Alexandra Prodan, Griselda Marku, Tiago Guerreiro, André Rodrigues, Diogo Branco, Livia Moreira, Carla Marques, Hélia Rodrigues, Fabio Roli, Davide Ariu, Stefania Casula, Battista Biggio, Luca Piras, Luca Didaci, Matteo Mauri, Joaquim Ferreira, Leonor Correia Guedes, Inês Dias, Ana Teresa, Joana Costa, Mariana Matos, Teemu Ahmaniemi, Luc Cluitmans, Jani Mäntyjärvi, Juha Kortelainen, Rajdeep Nath, Emmi Antikainen, Kinga Koski, Francesca Cormack, Michele Veldsman, Laura Keylock, James Dobson, Janet Griffiths, Nick Taptiklis, Julian Fierrez, Aythami Morales, Ruben Tolosana, Alejandro Pena, Luis Gomez, Rafael Oliveros, Ruben Vera-Rodriguez, DaQing Zhang, Xujun Ma, Mossaab Hariz, Pei Wang, Djamal Zeghlache, Jordi Evers, Laura Siepman, Martijn Niessen, Ralf Reilmann, Robin Schubert, Atbin Djamshidian-Tehrani, Grzegorz Witkowski, Halina Sienkiewicz-Jarosz, Malgorzata Dusza-Rowinska, Klaus Seppi, Katarina Schwarzova, Corinne Horlings, Samuel Labrecque, Anita Malik, Wolfram Rieneck, Maria B. Lauvsnes, Roald Omdal, Katrine Norheim, Svein Skeie, Anne Hjelle, Hilde Norvik, Dave Wenn, Mike Jackson, Luisa Avedano, Bella Haaf, Tatiana Negurita, Susanne de Bot, Carola Buitelaar, Kasper van der Zwaan, Laura Kuijper, Adrie van Weeghel, Ian Bruce, John McBeth, Liz Fay, Joanna Jozefiak, James Prior, Denise Faulkner, Ioannis Pandis, Nikolay Manyakov, Stefan Avey, Meenakshi Chatterjee, Kenneth Mosca, Cesar Calderon, Rana Rehman, Melissa Mendez-Nguyen, Lori Warring, Marc Walton, Bethany Paxson, Diana Koletzki, Shyla Jagannatha, Zhi (Carrie) Li, Drew Elias, Kai Langel, Dario Masullo, Matthew Roche, Victoria Zolfaghari, Sarah Weingast, Maurizio Facheris, Tony Bannon, Matt Czech, Jie Shen, Shiv Patel, Michelle Crouthamel, Josh Cosman, Sean Turner, Magnus Jörntén-Karlsson, Tim Ruckh, Folke Folkvaljon, Jörgen Jensen, Neil Newman, Susan Forda, Birgit Steckel-Hamann, David Dexter, Nikul Bakshi, Joe Mather, Seleen Ong, Carla Cox, Yiorgos Christakis, Hao Zhang, Carrie Nothcott, Elaine Borthwick, David Nobbs, Jens Schjodt-Eriksen, Sebastian Holst, Florian Lipsmeier, Jason Hannon, Nadir Ammour, Haneen Njoum, Hillol Sarker, Imane Brigui, Raolat Abdulai, Xavier Benain, Jimena Diaz DeLeon, Manon Cariou, Fabrice Bonche, Vincent Mittoux, Sheila Thomas, Caroline Zutterling, Juliette Muszka, Frederique Guilbert, Xavier Brusson, Gwenaelle Corre, Babak Boroojerdi, Coralie Domange, Phil Scordis, Kasper Claes, Valentina Ticcinelli, Chengliang Dai, Giovanni Campana, Sarah Bilali, Oliver Stumpp, Mireille Delval, David Marquet, Gwenaelle de Keyser, Claudia Mazza, Alexandra Auffret, Jeremy Edgerton, Juha Rouru,Minna Korolainen, Sammeli Liikkanen, Mikko Kuoppamäki, Marina Lindford, Anssi Mäkiniemi, Toni Sarapohja, Olavi Kilkku, Antonella Chiucchiuini, Brian Tracey, Dimitri Volfson, Tairmae Kangarloo, Francesco Onorati, Wojtek Piwko, Geert van Gassen, Todd Swick, Armella Escher, Pietro Artoni, Robert Latzman, Mike Chambers, Elizabeth Amstutz, Nick Bott, Laura Rosen, Ieuan Clay, Aiden Doherty, Sara Riggare, Dina de Sousa, Cate Titterton, Heather Hunter, Ulli Funken, Jill Shutt, Werner Rammele, Jean Heather, Paul Howard.
A-KB and DA conceived the idea. A-KB wrote the initial draft. All authors contributed to the article and revised it critically for important intellectual content and approved the submitted version.
The RADAR-AD project has received funding from the Innovative Medicines Initiative 2 Joint Undertaking under grant agreement No 806999. This Joint Undertaking receives support from the European Union’s Horizon 2020 research and innovation programme and EFPIA and Software AG. See www.imi.europa.eu for more details. This communication reflects the views of the RADAR-AD consortium and neither IMI nor the European Union and EFPIA are liable for any use that may be made of the information contained herein. Research of Alzheimer Center Amsterdam is part of the neurodegeneration research program of Amsterdam Neuroscience. Alzheimer Center Amsterdam is supported by Stichting Alzheimer Nederland and Stichting Steun Alzheimercentrum Amsterdam. The MOBILISE-D project has received funding from the Innovative Medicines Initiative 2 Joint Undertaking under grant agreement No. 820820. This Joint Undertaking receives support from the European Union’s Horizon 2020 research and innovation programme and the European Federation of Pharmaceutical Industries and Associations (EFPIA). The IDEA-FAST project has received funding from the Innovative Medicines Initiative 2 Joint Undertaking under grant agreement No. 853981. This Joint Undertaking receives support from the European Union’s Horizon 2020 research and innovation programme and EFPIA and associated partners.
This paper represents independent research partly funded by the National Institute for Health Research (NIHR) Maudsley Biomedical Research Centre at South London and Maudsley NHS Foundation Trust and King’s College London. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care. We thank all consortium members of RADAR-AD, Mobilise-D, and IDEA-FAST.
AP received grant support from Ministry of Health (MINSAL) and Ministry of Education, Research and University (MIUR), from Airalzh Foundation, LIMPE-DSIMOV society and MI H2020 initiative (MI2-2018-15-06); he received speaker honoraria from Abbvie, Bial, Biomarin, Roche and Zambon Pharmaceuticals. W-FN has consulted for Novartis, GlaxoSmithKline, Abbvie, BMS, Sanofi, MedImmune, Janssen, Resolve Therapeutics and UCB. LR receives consultancy from MJ Fox Foundation and grant support from the EU, NIHR, MRC, PDUK, Dunhill Medical Trust, Cure Parkinson’s Trust, EPSRC, MJ Fox Foundation. DA has received research support and/or honoraria from Astra-Zeneca, H. Lundbeck, Novartis Pharmaceuticals, Evonik, Roche Diagnostics, and GE Health, and served as paid consultant for H. Lundbeck, Eisai, Heptares, Mentis Cura, Eli Lilly, Cognetivity, Enterin, Acadia, EIP Pharma, and Biogen. JC was employed by Novartis Institutes for Biomedical Research (NIBR), Basel, Switzerland and GE was employed by Novartis Pharmaceuticals Corporations, Cambridge, MA, United States.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. ^Muurling M, de Boer C, Hinds C, Atreya A, Doherty A, Alepopoulos V, et al. and the RADAR-AD Consortium. Feasibility and user experience of remote monitoring in Alzheimer’s disease. (submitted)
1. Kaur, N , Belchior, P , Gelinas, I , and Bier, N . Critical appraisal of questionnaires to assess functional impairment in individuals with mild cognitive impairment. Int Psychogeriatr. (2016) 28:1425–39. doi: 10.1017/S104161021600017X
2. Sikkes, S , de Lange-de Klerk, ESM , Pijnenburg, YAL , Scheltens, P , and Uitdehaag, BMJ . A systematic review of instrumental activities of daily living scales in dementia: room for improvement. J Neurol Neurosurg Psychiatry. (2009) 80:7–12. doi: 10.1136/jnnp.2008.155838
3. Sikkes, SAM , Lange-de Klerk, ESM , Pijnenburg, YAL , Gillissen, F , Romkes, R , Knol, DL, et al. A new informant-based questionnaire for instrumental activities of daily living in dementia. Alzheimers Dement (2012) 8:536–543. doi: 10.1016/j.jalz.2011.08.006
4. van Dyck, CH , Swanson, CJ , Aisen, P , Bateman, RJ , Chen, C , Gee, M, et al. Lecanemab in early Alzheimer’s disease. N Engl J Med. (2023) 388:9–21. doi: 10.1056/NEJMoa2212948
5. Owens, AP , Hinds, C , Manyakov, NV , Stavropoulos, TG , Lavelle, G , Gove, D, et al. Selecting remote measurement technologies to optimize assessment of function in early Alzheimer’s disease: a case study. Front Psych. (2020) 11:582207. doi: 10.3389/fpsyt.2020.582207
6. Antikainen, E , Njoum, H , Kudelka, J , Branco, D , Rehman, RZU , Macrae, V, et al. Assessing fatigue and sleep in chronic diseases using physiological signals from wearables: a pilot study. Front Physiol. (2022) 13:968185. doi: 10.3389/fphys.2022.968185
7. Chen, L , Ma, X , Chatterjee, M , Kortelainen, JM , Ahmaniemi, T , Maetzler, W, et al. Fatigue and sleep assessment using digital sleep trackers: insights from a multi-device pilot study. Annu Int Conf IEEE Eng Med Biol Soc. (2022) 2022:1133–6. doi: 10.1109/EMBC48229.2022.9870923
8. Rochester, L , Mazzà, C , Mueller, A , Caulfield, B , McCarthy, M , Becker, C, et al. A roadmap to inform development, validation and approval of digital mobility outcomes: the mobilise-D approach. DIB. (2020) 4:13–27. doi: 10.1159/000512513
9. Mazzà, C , Alcock, L , Aminian, K , Becker, C , Bertuletti, S , Bonci, T, et al. Technical validation of real-world monitoring of gait: a multicentric observational study. BMJ Open. (2021) 11:e050785. doi: 10.1136/bmjopen-2021-050785
10. Mikolaizak, AS , Rochester, L , Maetzler, W , Sharrack, B , Demeyer, H , Mazzà, C, et al. Connecting real-world digital mobility assessment to clinical outcomes for regulatory and clinical endorsement-the mobilise-D study protocol. PLoS One. (2022) 17:e0269615. doi: 10.1371/journal.pone.0269615
11. Amariglio, RE , Donohue, MC , Marshall, GA , Rentz, DM , Salmon, DP , Ferris, SH, et al. Alzheimer’s disease cooperative study. Tracking early decline in cognitive function in older individuals at risk for Alzheimer disease dementia: the Alzheimer’s disease cooperative study cognitive function instrument. JAMA Neurol. (2015) 72:446–54. doi: 10.1001/jamaneurol.2014.3375
12. Wakim, NI , Braun, TM , Kaye, JA , and Dodge, HH . Choosing the right time granularity for analysis of digital biomarker trajectories. Alzheimers Dement (N Y). (2020) 6:e12094. doi: 10.1002/trc2.12094
13. Day, JO , Smith, S , Noyce, AJ , Alty, J , Jeffery, A , Chapman, R, et al. Challenges of incorporating digital health technology outcomes in a clinical trial: experiences from PD STAT. J Parkinsons Dis. (2022) 12:1605–9. doi: 10.3233/JPD-223162
14. Kelly, CJ , Karthikesalingam, A , Suleyman, M , Corrado, G , and King, D . Key challenges for delivering clinical impact with artificial intelligence. BMC Med. (2019) 17:195. doi: 10.1186/s12916-019-1426-2
15. Gochoo, M , Alnajjar, F , Tan, T-H , and Khalid, S . Towards privacy-preserved aging in place: a systematic review. Sensors (Basel). (2021) 21:3082. doi: 10.3390/s21093082
16. Mazzochi, AT , Dennis, M , and Chun, H-YY . Electronic informed consent: effects on enrolment, practical and economic benefits, challenges, and drawbacks-a systematic review of studies within randomized controlled trials. Trials. (2023) 24:127. doi: 10.1186/s13063-022-06959-6
17. Sheikh, A , Anderson, M , Albala, S , Casadei, B , Franklin, BD , Richards, M, et al. Health information technology and digital innovation for national learning health and care systems. Lancet Digit Health. (2021) 3:e383–96. doi: 10.1016/S2589-7500(21)00005-4
18. Richardson, S , Lawrence, K , Schoenthaler, AM , and Mann, D . A framework for digital health equity. NPJ Digit Med. (2022) 5:–6. doi: 10.1038/s41746-022-00663-0
19. Rosenberg, S. Smartphone ownership is growing rapidly around the world, but not always equally. Pew Research Center’s Global Attitudes Project (2019). Available at: https://www.pewresearch.org/global/2019/02/05/smartphone-ownership-is-growing-rapidly-around-the-world-but-not-always-equally/ (Accessed April 19, 2023).
20. Goedhart, NS , Broerse, JE , Kattouw, R , and Dedding, C . ‘Just having a computer doesn’t make sense’: the digital divide from the perspective of mothers with a low socio-economic position. New Media Soc. (2019) 21:2347–65. doi: 10.1177/1461444819846059
21. Cho, PJ , Yi, J , Ho, E , Shandhi, MMH , Dinh, Y , Patil, A, et al. Demographic imbalances resulting from the bring-your-own-device study design. JMIR Mhealth Uhealth. (2022) 10:e29510. doi: 10.2196/29510
22. Guu, T-W , Muurling, M , Khan, Z , Kalafatis, C , Aarsland, D , Ffytche, D, et al. Wearable devices: underrepresentation in the ageing society. The Lancet Digital Health. (2023) 5: e336–e337. doi: 10.1016/S2589-7500(23)00069-9
23. Keogh, A , Alcock, L , Brown, P , Buckley, E , Brozgol, M , Gazit, E, et al. Acceptability of wearable devices for measuring mobility remotely: observations from the Mobilise-D technical validation study. Digit Health. (2023) 9:205520762211507. doi: 10.1177/20552076221150745
24. Holthe, T , Halvorsrud, L , and Lund, A . Digital assistive technology to support everyday living in community-dwelling older adults with mild cognitive impairment and dementia. Clin Interv Aging. (2022) 17:519–44. doi: 10.2147/CIA.S357860
25. Piau, A , Wild, K , Mattek, N , and Kaye, J . Current state of digital biomarker technologies for real-life, home-based monitoring of cognitive function for mild cognitive impairment to mild Alzheimer disease and implications for clinical care: systematic review. J Med Internet Res. (2019) 21:e12785. doi: 10.2196/12785
26. Laar, A , Silva de Lima, AL , Maas, BR , Bloem, BR , and de Vries, NM . Successful implementation of technology in the management of Parkinson’s disease: barriers and facilitators. Clin Park Relat Disord. (2023) 8:100188. doi: 10.1016/j.prdoa.2023.100188
27. Boyle, LD , Husebo, BS , and Vislapuu, M . Promotors and barriers to the implementation and adoption of assistive technology and telecare for people with dementia and their caregivers: a systematic review of the literature. BMC Health Serv Res. (2022) 22:1573. doi: 10.1186/s12913-022-08968-2
28. Thordardottir, B , Malmgren Fänge, A , Lethin, C , Rodriguez Gatta, D , and Chiatti, C . Acceptance and use of innovative assistive technologies among people with cognitive impairment and their caregivers: a systematic review. Biomed Res Int. (2019) 2019:9196729–18. doi: 10.1155/2019/9196729
29. Nicosia, J , Aschenbrenner, AJ , Adams, SL , Tahan, M , Stout, SH , Wilks, H, et al. Bridging the technological divide: stigmas and challenges with technology in digital brain health studies of older adults. Front Digit Health. (2022) 4:880055. doi: 10.3389/fdgth.2022.880055
30. Moore, K , O’Shea, E , Kenny, L , Barton, J , Tedesco, S , Sica, M, et al. Older adults’ experiences with using wearable devices: qualitative systematic review and Meta-synthesis. JMIR Mhealth Uhealth. (2021) 9:e23832. doi: 10.2196/23832
31. Bastoni, S , Wrede, C , da Silva, MC , Sanderman, R , Gaggioli, A , Braakman-Jansen, A, et al. Factors influencing implementation of eHealth technologies to support informal dementia care: umbrella review. JMIR Aging. (2021) 4:e30841. doi: 10.2196/30841
32. van Eijk, RPA , Beelen, A , Kruitwagen, ET , Murray, D , Radakovic, R , Hobson, E, et al. A road map for remote digital health technology for motor neuron disease. J Med Internet Res. (2021) 23:e28766. doi: 10.2196/28766
33. Gove, D , Diaz-Ponce, A , Georges, J , Moniz-Cook, E , Mountain, G , Chattat, R, et al. European working group of people with dementia. Alzheimer Europe’s position on involving people with dementia in research through PPI (patient and public involvement). Aging Ment Health. (2018) 22:723–9. doi: 10.1080/13607863.2017.1317334
34. Roberts, C , Rochford-Brennan, H , Goodrick, J , Gove, D , Diaz-Ponce, A , and Georges, J . Our reflections of patient and public involvement in research as members of the European working group of people with dementia. Dementia (London). (2020) 19:10–7. doi: 10.1177/1471301219876402
35. Masanneck, L , Gieseler, P , Gordon, WJ , Meuth, SG , and Stern, AD . Evidence from ClinicalTrials.gov on the growth of digital health technologies in neurology trials. npj Digit Med. (2023) 6:23. doi: 10.1038/s41746-023-00767-1
36. Dekker, MJHJ , Stolk, P , and Pasmooij, AMG . The use of remote monitoring technologies: a review of recent regulatory scientific advices, qualification opinions, and qualification advices issued by the European medicines agency. Front Med (Lausanne). (2021) 8:619513. doi: 10.3389/fmed.2021.619513
37. Bloem, BR , Post, E , and Hall, DA . An apple a day to keep the Parkinson’s disease doctor away? Ann Neurol. (2023) 93:681–5. doi: 10.1002/ana.26612
38. Viceconti, M , Hernandez Penna, S , Dartee, W , Mazzà, C , Caulfield, B , Becker, C, et al. Toward a regulatory qualification of real-world mobility performance biomarkers in Parkinson’s patients using digital mobility outcomes. Sensors (Basel). (2020) 20:5920. doi: 10.3390/s20205920
39. Viceconti, M , Tome, M , Dartee, W , Knezevic, I , Hernandez Penna, S , Mazzà, C, et al. On the use of wearable sensors as mobility biomarkers in the marketing authorization of new drugs: a regulatory perspective. Front Med (Lausanne). (2022) 9:996903. doi: 10.3389/fmed.2022.996903
40. European Medicines Agency . Letter of support for mobilise-D digital mobility outcomes as monitoring biomarkers. (2021) Available at: https://www.ema.europa.eu/en/documents/other/letter-support-mobilise-d-digital-mobility-outcomes-monitoring-biomarkers-follow_en.pdf
41. European Medicines Agency . Letter of support for mobilise-D digital mobility outcomes as monitoring biomarkers. (2020). Available at: https://www.ema.europa.eu/en/documents/other/letter-support-mobilise-d-digital-mobility-outcomes-monitoring-biomarkers_en.pdf
42. Landers, M , Dorsey, R , and Saria, S . Digital endpoints: definition, benefits, and current barriers in accelerating development and adoption. DIB. (2021) 5:216–23. doi: 10.1159/000517885
43. Lanzi, AM , Saylor, AK , Fromm, D , Liu, H , MacWhinney, B , and Cohen, ML . DementiaBank: theoretical rationale, protocol, and illustrative analyses. Am J Speech Lang Pathol. (2023) 32:426–38. doi: 10.1044/2022_AJSLP-22-00281
44. Luz, S , Haider, F , de la Fuente, GS , Fromm, D , and MacWhinney, B . Editorial: Alzheimer’s dementia recognition through spontaneous speech. Front Comput Sci. (2021) 3:780169. doi: 10.3389/fcomp.2021.780169
45. Bose, N , Brookes, AJ , Scordis, P , and Visser, PJ . Data and sample sharing as an enabler for large-scale biomarker research and development: the EPND perspective. Front Neurol. (2022) 13:1031091. doi: 10.3389/fneur.2022.1031091
46. Open access —H2020 online manual. Available at: https://ec.europa.eu/research/participants/docs/h2020-funding-guide/cross-cutting-issues/open-access-data-management/open-access_en.htm (Accessed April 20, 2023).
Keywords: Alzheimer’s disease, Parkinson’s disease, Huntington’s disease, neurodegenerative diseases, dementia, digital biomarker, remote measurement technologies, digital health technologies
Citation: Brem A-K, Kuruppu S, de Boer C, Muurling M, Diaz-Ponce A, Gove D, Curcic J, Pilotto A, Ng W-F, Cummins N, Malzbender K, Nies VJM, Erdemli G, Graeber J, Narayan VA, Rochester L, Maetzler W and Aarsland D (2023) Digital endpoints in clinical trials of Alzheimer’s disease and other neurodegenerative diseases: challenges and opportunities. Front. Neurol. 14:1210974. doi: 10.3389/fneur.2023.1210974
Edited by:
Donald C. Lo, National Center for Advancing Translational Sciences (NIH), United StatesReviewed by:
Linus Jönsson, Karolinska Institutet (KI), SwedenCopyright © 2023 Brem, Kuruppu, de Boer, Muurling, Diaz-Ponce, Gove, Curcic, Pilotto, Ng, Cummins, Malzbender, Nies, Erdemli, Graeber, Narayan, Rochester, Maetzler, Aarsland and on behalf of the RADAR-AD Consortium. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anna-Katharine Brem, a2F0eS5icmVtQGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.