
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CORRECTION article
Front. Neurol. , 10 May 2023
Sec. Stroke
Volume 14 - 2023 | https://doi.org/10.3389/fneur.2023.1206563
 Napasri Chaisinanunkul1Shaan Khurshid2
Napasri Chaisinanunkul1Shaan Khurshid2 Brian H. Buck3
Brian H. Buck3 Alejandro A. Rabinstein4
Alejandro A. Rabinstein4 Christopher D. Anderson5
Christopher D. Anderson5 Michael D. Hill6
Michael D. Hill6 Jennifer E. Fugate4
Jennifer E. Fugate4 Jeffrey L. Saver7*
Jeffrey L. Saver7*A corrigendum on
How often is occult atrial fibrillation in cryptogenic stroke causal vs. incidental? A meta-analysis.
Chaisinanunkul, N., Khurshid, S., Buck, B. H., Rabinstein, A. A., Anderson, C. D., Hill, M. D., Fugate, J. E., and Saver, J. L. (2023). Front. Neurol. 14:1103664. doi: 10.3389/fneur.2023.1103664
In the published article, there was an error in Figure 3 as published. For the study in the 2nd row and Totals in the 4th row of the figure, the numerator values, denominator values, point estimates, and confidence intervals were not correct. The corrected Figure and its caption appear below.
In the published article, there were errors in those text passages that stated data values based on Figure 3. The following corrections have been made:
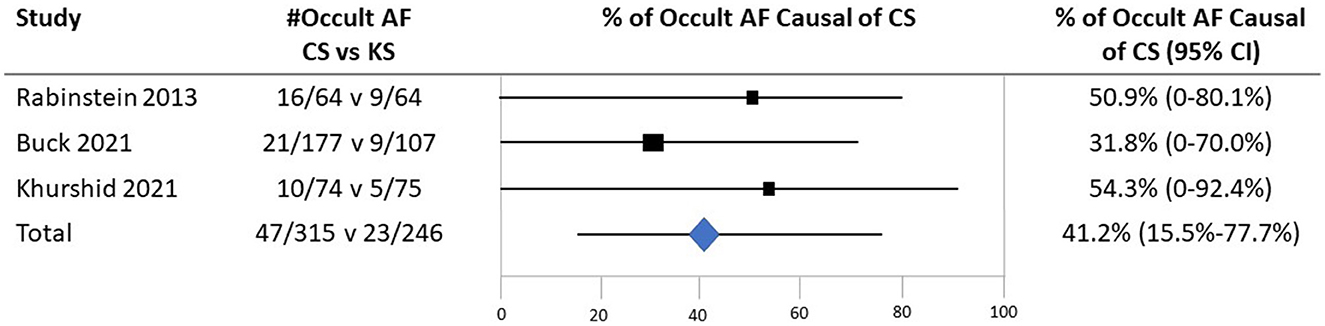
Figure 3. The probability that detected occult atrial fibrillation is causal in patients with CS based on case–control studies examining the prevalence of occult AF in cases with CS vs. controls with the stroke of a determined cause. Individual studies were identified by the first author and year of publication. The second column shows the prevalence of occult AF (# occult AF/total number of patients) in cases vs. controls. Black boxes with sizes corresponding to each study's weight in the analysis represent the point estimate of the probability that the PFO is causal with 95% CIs represented with the gray lines. The diamond in the last row represents the summary estimate of the probability.
A correction has been made to the Abstract Results paragraph.
This sentence previously stated:
“With the application of Bayes' theorem, the corresponding probabilities indicated that, when present, occult AF in patients with CS is causal in 38.2% (95% CI, 0–63.6%) of patients.”
The corrected sentence appears below:
“With the application of Bayes' theorem, the corresponding probabilities indicated that, when present, occult AF in patients with CS is causal in 41.2% (95% CI, 15.5–77.7%) of patients.”
A correction has been made to the Abstract Conclusion paragraph.
This sentence previously stated:
“Current evidence is preliminary, but it indicates that in cryptogenic stroke when occult AF is found, it is causal in about 38.2% of patients.”
The corrected sentence appears below:
“Current evidence is preliminary, but it indicates that in cryptogenic stroke when occult AF is found, it is causal in about 41.2% of patients.”
A correction has been made to Results, 5th paragraph.
This sentence previously stated:
“The summary estimate derived from all three studies indicated that when present among patients with cryptogenic stroke, occult AF is causal in 38.2% (95% CI, 0–63.6%).”
The corrected sentence appears below:
“The summary estimate derived from all three studies indicated that when present among patients with cryptogenic stroke, occult AF is causal in 41.2% (95% CI, 15.5–77.7%).”
A correction has been made to Results, 5th paragraph.
This sentence previously stated:
“Combining the rate of occult AF presence in patients with CS across all series (14.9%) and the frequency with which the detected occult AF is statistically deemed causal (38.2%) projects that occult AF accounts for 5.7% of all cryptogenic strokes (attributable risk).”
The corrected sentence appears below:
“Combining the rate of occult AF presence in patients with CS across all series (14.9%) and the frequency with which the detected occult AF is statistically deemed causal (41.2%) projects that occult AF accounts for 6.1% of all cryptogenic strokes (attributable risk).”
A correction has been made to Discussion, 1st paragraph.
This sentence previously stated:
“Findings indicated that when identified in patients with CS, occult AF is causally related to the index stroke in 38% and incidental in 62%.”
The corrected sentence appears below:
“Findings indicated that when identified in patients with CS, occult AF is causally related to the index stroke in 41% and incidental in 59%.”
A correction has been made to Discussion, 1st paragraph.
This sentence previously stated:
“Given the frequency with which occult AF is detected among patients with CS, the results suggest that occult AF is an important mechanism of CS, accounting for 1 in 17 of all cases of CS, including 1 in 16 cases in patients under the age of 65 years, and 1 in 18 cases in patients who are 65 years and older.”
The corrected sentence appears below:
“Given the frequency with which occult AF is detected among patients with CS, the results suggest that occult AF is an important mechanism of CS, accounting for 1 in 16 of all cases of CS, including 1 in 16 cases in patients under the age of 65 years, and 1 in 18 cases in patients who are 65 years and older.”
A correction has been made to Materials and Methods, subsection Probability of causal vs. incidental, paragraph 1.
This sentence previously stated:
“Probability occult AF is incidental in CS cases = (Prevalence of occult AF in controls) × (1 – Prevalence of occult AF in CS cases) (Prevalence of occult AF in CS cases) × (1 – Prevalence of occult AF in controls)”
The corrected sentence appears below:
“Probability occult AF is incidental in CS cases = [(Prevalence of occult AF in controls) × (1 – Prevalence of occult AF in CS cases)] ÷ [(Prevalence of occult AF in CS cases) × (1 – Prevalence of occult AF in controls)]”
The authors apologize for these errors and state that this does not change the scientific conclusions of the article in any way. The original article has been updated.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Keywords: cryptogenic stroke, atrial fibrillation, cardiac monitoring, attributable risk, diagnosis, epidemiology
Citation: Chaisinanunkul N, Khurshid S, Buck BH, Rabinstein AA, Anderson CD, Hill MD, Fugate JE and Saver JL (2023) Corrigendum: How often is occult atrial fibrillation in cryptogenic stroke causal vs. incidental? A meta-analysis. Front. Neurol. 14:1206563. doi: 10.3389/fneur.2023.1206563
Received: 15 April 2023; Accepted: 27 April 2023;
Published: 10 May 2023.
Approved by:
Robin Lemmens, University Hospitals Leuven, BelgiumCopyright © 2023 Chaisinanunkul, Khurshid, Buck, Rabinstein, Anderson, Hill, Fugate and Saver. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jeffrey L. Saver, anNhdmVyQG1lZG5ldC51Y2xhLmVkdQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.