 Fasihah Irfani Fitri1,2†
Fasihah Irfani Fitri1,2† Carmen Lage3,4†
Carmen Lage3,4† Tatyana Mollayeva2,5,6,7,8,9†
Tatyana Mollayeva2,5,6,7,8,9† Hernando Santamaria-Garcia4,10,11†Melissa Chan2,12Marcia R. Cominetti2,13Tselmen Daria4,14Gillian Fallon4Dominic Gately2Muthoni Gichu2,15Sandra Giménez4,16Raquel Gutierrez Zuniga2,17
Hernando Santamaria-Garcia4,10,11†Melissa Chan2,12Marcia R. Cominetti2,13Tselmen Daria4,14Gillian Fallon4Dominic Gately2Muthoni Gichu2,15Sandra Giménez4,16Raquel Gutierrez Zuniga2,17 Rafi Hadad4,18
Rafi Hadad4,18 Tanisha Hill-Jarrett4,19Mick O’Kelly4,20Luis Martinez4,19Paul Modjaji2Ntkozo Ngcobo2,21
Tanisha Hill-Jarrett4,19Mick O’Kelly4,20Luis Martinez4,19Paul Modjaji2Ntkozo Ngcobo2,21 Rafal Nowak4,22Chukwuanugo Ogbuagu4,23Moïse Roche2,24
Rafal Nowak4,22Chukwuanugo Ogbuagu4,23Moïse Roche2,24 Cristiano Schaffer Aguzzoli4,25
Cristiano Schaffer Aguzzoli4,25 So Young Shin4,26Erin Smith4,27Selam Aberra Yoseph4,28Yared Zewde4,28
So Young Shin4,26Erin Smith4,27Selam Aberra Yoseph4,28Yared Zewde4,28 Yavuz Ayhan4,29*
Yavuz Ayhan4,29*- 1Department of Neurology, Faculty of Medicine, Universitas Sumatera Utara, Medan, Indonesia
- 2Senior Atlantic Fellow at the Global Brain Health Institute/Trinity College, UCSF, Dublin, Ireland
- 3Department of Neurology, Marques de Valdecilla University Hospital - Valdecilla Research Institute (IDIVAL), Santander, Spain
- 4Senior Atlantic Fellow at the Global Brain Health Institute/Trinity College, UCSF, San Francisco, CA, United States
- 5Canada Research Chairs, Ottawa, ON, Canada
- 6The KITE Research Institute, Toronto Rehabilitation Institute, University Health Network, Toronto, ON, Canada
- 7Dalla Lana School of Public Health, University of Toronto, Toronto, ON, Canada
- 8Temerty Faculty of Medicine, University of Toronto, Toronto, ON, Canada
- 9Acquired Brain Injury Research Lab, Department of Occupational Science and Occupational Therapy, Faculty of Medicine, University of Toronto, Toronto, ON, Canada
- 10Center of Memory and Cognition Intellectus, Hospital Universitario San Ignacio Bogotá, Bogotá, Colombia
- 11Pontificia Universidad Javeriana (PhD Program in Neuroscience) Bogotá, Bogotá, Colombia
- 12Department of Social Sciences, University of Luxembourg, Luxembourg, Luxembourg
- 13Department of Gerontology, Federal University of São Carlos, São Carlos, Brazil
- 14Gladstone Institutes, San Francisco, CA, United States
- 15Division of Geriatric Medicine at the Ministry of Health, Nairobi, Kenya
- 16Multidisciplinary Sleep Unit, Memory Unit, Hospital de la Santa Creu i Sant Pau, Universitat Autònoma de Barcelona, Barcelona, Spain
- 17Hospital Quirónsalud Valle del Henares, Madrid, Spain
- 18Rambam Health Care Campus, Haifa, Israel
- 19Memory and Aging Center, Medical Center, University of California, San Francisco, CA, United States
- 20National College of Art and Design, Dublin, Ireland
- 21Department of Psychiatry, University of KwaZulu-Natal, Durban, South Africa
- 22Neuroelectrics (Spain), Barcelona, Spain
- 23Faculty of Basic Clinical Sciences, Nnamdi Azikiwe University Teaching Hospital, Nnewi, Nigeria
- 24Division of Psychiatry, UCL, London, United Kingdom
- 25Department of Psychiatry, School of Medicine, University of Pittsburgh, Pittsburgh, PA, United States
- 26College of Nursing, Inje University, Busan, Republic of Korea
- 27Stanford University, Stanford, CA, United States
- 28College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia
- 29Department of Psychiatry, Faculty of Medicine, Hacettepe University, Ankara, Türkiye
Brain health refers to the state of a person’s brain function across various domains, including cognitive, behavioral and motor functions. Healthy brains are associated with better individual health, increased creativity, and enhanced productivity. A person’s brain health is intricately connected to personal, social and environmental factors. Racial, ethnic, and social disparities affect brain health and on the global scale these disparities within and between regions present a hurdle to brain health. To overcome global disparities, greater collaboration between practitioners and healthcare providers and the people they serve is essential. This requires cultural humility driven by empathy. Empathy is a core prosocial value, a cognitive-emotional skill that helps us understand ourselves and others. This position paper aims to provide an overview of the vital roles of empathy, cooperation, and interdisciplinary partnerships. By consciously integrating this understanding in practice, leaders can better position themselves to address the diverse challenges faced by communities, promote inclusivity in policies and practices, and further more equitable solutions to the problem of global brain health.
Introduction
In today’s interdependent world, prioritizing and improving brain health becomes a vital goal in advancing the collective health of populations across the globe (1, 2). The term “brain health” is not a standardized one. According to the World Health Organization (WHO), brain health is “the state of brain functioning across cognitive, sensory, social–emotional, behavioral and motor domains, allowing a person to realize their full potential over the life course, irrespective of the presence or absence of disorders” (3). There is heterogeneity among institutions and researchers on how brain health is defined, a recent literature review on definitions of brain health revealed that, despite these differences, the common thread is the conceptualization of brain health as dynamic and multidimensional, encompassing both objectively measured and perceived components (4).
Progressively realizing the global right to brain health and global interdependence (i.e., worldwide mutual dependence between countries) allows systematically identifying and eliminating inequities stemming from social processes. Global leaders need to appreciate the effects of culture on dynamics between people and communities and to consciously commit to developing cultural humility. Cultural humility involves recognizing the values and perspectives of different cultures, advocating for inclusive and culturally sensitive approaches, and identifying the unique barriers that contribute to health and other social disparities. Empathy, a fundamental aspect of social interaction, a construct that accounts for a sense of similarity in feelings experienced by oneself and others, is essential to truly acknowledging the needs of others, for open conversation around challenging topics and for creative problem solving (Figure 1).
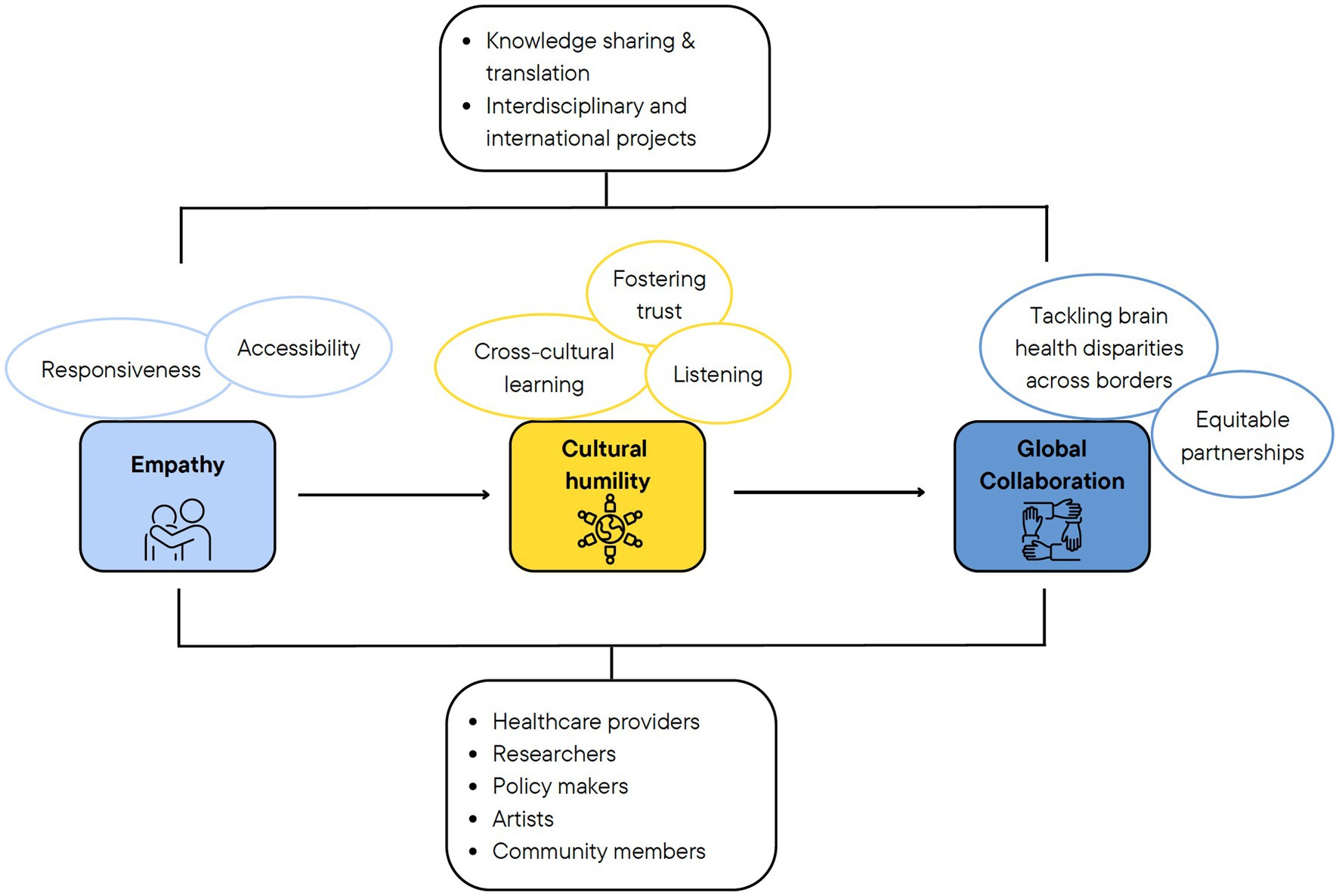
Figure 1. Framework outlining the position advanced in the paper. The value of empathy in tackling disparities in brain health by encouraging more responsive and accessible services, fostering trust among and between diverse populations through cultural humility, and pursuing collaborative interdisciplinary efforts to create responsive, accessible, and effective systems of care.
In this position paper, we argue that empathy, cultural humility and cooperation as fundamental for eliminating disparities and achieving global equity in brain health. We start by explaining inequalities and demonstrating disparities in global brain health. Then we identify cultural humility and emphasize its role in dealing with the global health problems. We focus on empathy and discuss how empathy and cooperation can challenge the biases and assumptions that underpin brain health disparities. Finally, we envision how art and science collaborations can remove barriers between individuals, institutions, and nations, and improve the prospects for equity in brain health across the world.
Global inequalities affect the most vulnerable social groups
Health inequalities and health inequity have been defined in various ways with overlapping use (5). According to the World Health Organization (WHO), health inequalities are measurable differences in health across population subgroups, and health equity is defined as the absence of unfair, avoidable or remediable differences in health among population groups, defined by social, economic, demographic or geographic characteristics (6, 7). Different theories were developed to explain health inequalities. The inequalities might be associated with the differences based on culture, health behaviors, social mobility or genetics; however the main causal factor for the differences in health outcomes is suggested to be the differences in socioeconomic status of social groups, as proposed by the structural theory (8). This understanding calls for a more systematic way of approaching the concern of brain health inequalities for individuals and communities, as they perpetuate cycles of disadvantage and contribute to broader health inequities. The 2021 Global Health Security Index, an indicator of health security and related capabilities across 195 countries, analyzing experience from the COVID-19 pandemic, concluded that most countries came unprepared maintaining a capable accessible health system, where preparedness needs of vulnerable populations were most often neglected (9). Examples of vulnerable populations include people with cognitive and physical disabilities, chronic health conditions (e.g., diabetes, heart disease), and mental health issues (10). These vulnerabilities are also known risks for brain health across the world, including high, middle- and low-income countries.
Understanding brain health disparities
Disparities in brain health are evident in different facets. Take the resource aspect as an example. The number of specialists and healthcare workers, the number of facilities per individual, and their resources respecting brain health widely vary across the globe. There is a clear lack of brain health workforce particularly in Africa and South East Asia (11, 12). This discrepancy remains when the workforce is classified by income level; low and lower-middle-income countries are in a very disadvantageous position. Disparities are overwhelming for brain health risk factors, which include but are not limited to education (13), smoking (14), diabetes (15), and hypertension (16). A brief survey on disparities in dementia among the authors of this paper from 17 countries and 5 continents displayed the existence of apparent inequalities in access to assessment and treatment [unpublished data, presented at the Global Brain Health Institute (GBHI) Annual Meeting 2022]. The surveyors found such disparities also existed within the countries and varied with social and economic factors.
Wealth, education, occupational status, race/ ethnicity or gender predict variations in health status on an individual level, these factors converge with a dynamic interdependent process influencing the health outcomes (17). Wealth disparities, measured according to the distribution of wealth from economic activity through jobs and demands, income, and pollution levels, exist both between and within countries (18). Disparities in the distribution of wealth across the globe are reflected in global peace (19). The 2021 Global Peace Index highlighted the connection between peace and health, emphasizing the role of disparities within and between nations associated with domestic and international conflicts, respectively (19). A responsible, ethical, and inclusive global health approach constitutes a genuine foundation to take action to promote brain health across the globe (20). The aim remains to disrupt disparities in brain health within and between countries. It is hard to imagine a more significant challenge for the leaders than to combat disparities.
Disparities display the existence of global inequities in health
Disparities among different social groups remain a problem for brain health across the globe as exemplified in dementia. In the US, even though there is an overall decline in the disparities trend in dementia prevalence (21), racial and ethnic disparities remain significant (22–25). The annual incidence of dementia among African American and Hispanic American populations was significantly higher as compared to Caucasian population (26), and the burden of known risk factors for dementia differed among ethnic groups (27). The Global Council on Brain Health, a collaboration of experts convened by the AARP emphasizes the role of social determinants of health and identifies health disparities as a policy imperative (10, 28). The US National Plan to Address Alzheimer’s Disease (29) includes efforts to address inequities in dementia risk factors among vulnerable populations, based on needs assessment and developing targeted plans addressing any system gaps that stand in the way of such efforts. In Canada, the rates of dementia and its modifiable risk factors started to decrease, and protective factors increase, according to the 2021 annual report to Parliament on Canada’s national dementia strategy, A Dementia Strategy for Canada: Together We Aspire (30). The progress is attributed to collective aspirations embedded in the strategy’s national objectives including advancing knowledge of Canadians about modifiable risks of dementia, access to quality care, and raising awareness of, and elimination of stigmatizing behaviors. Despite these collective efforts, some populations within Canada have been identified as more likely to face barriers to equitable care and/or are at higher risk of developing dementia, including transgender and non-binary adults living with dementia, Indigenous people, and people from ethnic populations and those living in rural and remote communities (31, 32).
In the low – and middle income countries, socioeconomic factors including indices of poverty were associated with increased dementia rates in South Africa (33), Colombia (34), Chile (35), and Brazil (36). While dementia rates are exponentially growing in all countries of the world, and projections display that almost 150 million individuals will be affected by dementia by 2050 (37, 38), the estimations rates are disproportionately high for low to middle-income countries as compared to high income countries (39).
Unjustified and avoidable differences in race/ethnicity, gender, and class-based socioeconomic differences exist in many other neurological and mental health disorders across the globe (40–43), with disparities started to emerge during early stages of brain development (44). The effects of these individual factors on brain health may be distinct and particularly robust on individuals with intersectional identities. This is alarming and calls for action of global leaders for equity in brain health. It also recognizes the importance of investing in efforts to identify and discuss challenges related to disparities, identify opportunities for global collaboration and action, and share ideas for a global strategy.
Overcoming disparities requires respectful dialog, and its essence is cultural humility
Effectively addressing global disparities in brain health requires collaboration among diverse groups of people from different cultural backgrounds. To ensure successful interactions, it is crucial to appreciate the cultural constructs and history of partners (45, 46).
Cultural humility refers to a more thoughtful and substantive understanding of other cultures and people which are unlike our own, and application of such understanding in practice. Tervalon and Murray-Garcia first coined the term “cultural humility” as a corrective to cultural competence, a skill that can be taught, acquired, and achieved, and it is frequently referred to as a necessary and sufficient condition for working effectively with diverse groups of people possessing ethnic, racial, and class differences (47). Cultural humility involves actively engaging in the process of learning about other cultures, their worldview, and any oppression or discrimination that they may have historically experienced, while also being mindful of our thoughts and feelings regarding those cultures. This includes overcoming any preconceived assumptions, prejudices, and biases people carry (45, 46).
Cultural humility calls for application in various aspects of life, including clinical work, education, and research. The need for cultural humility is particularly important in clinical practice, where clinicians are working with people from widely diverse cultural backgrounds. Putting aside their own belief systems and considering patients’ and caregivers’ perspectives is an essential skill for clinicians when developing a patient-centered treatment or care plan (48, 49). Inquiring about patients’ backgrounds, practices, religion, and culture, is essential to avoid stereotyping and in determining individual patient’s needs, goals, and preferable treatment options, to be in line with the paradigm of person-centered care. Cultural humility helps to create deeper connections and understanding between patients and care providers, which may increase patient satisfaction and care outcomes for vulnerable groups/minorities.
It is important to emphasize the role of cultural humility in identifying, addressing, preventing, and eliminating racism and discrimination in healthcare institutions (50–53). Racism in healthcare politics was suggested as a root cause of racial health inequities in the US (51). Discrimination may also be evident based on religion or other social factors. Historical attitudes toward the health care institutions, especially among marginalized communities, can shape their perceptions and health-related decisions (54, 55). Understanding and resolving underlying factors affecting trust in medical institutions play a crucial role in moderating the likelihood of individuals pursuing medical care (56, 57).
In research, especially in health research, the application of cultural humility allows the researchers to generate culture-sensitive hypotheses, apply culturally-neutral methods, and analyze the results with an appreciation of the influence of their own culture (58). Multicultural projects having a common goal but different resources in executing the same mutual interests have challenges. Each party has inherent differences, differing values, methods and rewards. Understanding the basic motivations, values, and sensitivities of each party in multicultural projects is crucial, as it lays the foundation for proper recognition and acknowledgment of their independence. This is essential because it fosters an environment of respect and inclusivity, allowing diverse groups to collaborate effectively toward a common goal. Acknowledging and respecting cultural differences becomes pivotal in international collaboration, as such recognition paves the way for meaningful communication and conflict resolution, promoting successful outcomes for all parties involved.
A troubling aspect in research is funding disparity for ethnic and racial minorities and women, and non-English speaking countries. Cultural humility allows us to reflect on the ways global funding and publishing agencies impact scientific research, and how scholars with cultures and languages other than English are frequently excluded due to biases or language barriers, and limited access to funding (58, 59).
Cultural humility is also essential in education, especially in disciplines emphasizing professional training and tied to a patient or client (e.g., nursing, medicine, and counseling). Humanities-based disciplines (e.g., art, music, literature, film, and theater) are well-positioned to incorporate cultural humility by addressing the perspectives of people in ways that encourage critical reflection, empathy, and appreciation for diversity in human artistic creativity (60).
Art as a manifestation and media of cultural humility
Artistic manifestations are the fingerprints of a culture. Whether it is a painting, a dance, or a novel, artistic works are shaped by the character and the history of the culture in which they are created (61). Therefore, being exposed to artistic expressions can help us to understand a different culture and its particular perspective of the world (62). While this can help us recognize and embrace our own culture’s uniqueness, it can also help us appreciate others and embrace diversity. In the global health scenario, this means that art can be a tool to promote respectful intercultural dialog.
But, also importantly, art reflects our cultural past. In traditional artistic expressions, we can recognize the diverse influences that have carved a culture across time. We can also identify some of the same features in other - separated- cultures, realizing that they are not watertight compartments throughout history. This way, barriers between cultures begin to blur, our cultural arrogance smooths because we are aware of how much we share, and we start to recognize ourselves as habitants of one unique world, and not so different from our pairs.
Embracing cultural humility offers a valuable approach to navigating diversity and counter impediments to disparities that emerged from marginalization and stigmatization of disadvantaged communities. In light of disparities in brain health, cultural humility can foster empowerment, inclusivity, and respectful global collaborations.
The role of empathy in brain health leadership
Leadership skills are required to promote public health changes to protect and promote brain health (63). Leaders must profoundly understand their own and global community (64–66), including cultural beliefs, practices, and political views, to create and implement reproducible, sustainable, and scalable interventions to protect brain health. Leaders need to create cross-culture connections to navigate global landscape, and to be in a position to influence people from diverse backgrounds. No problem will be solved without being connected with those who struggle, and a meaningful connection is impossible without empathy and cooperation (67).
Empathy is essential for lasting social change and sustainable collaborative actions to disrupt disparities. Empathetic traits are predictors of conflict-free decision-making and interpersonal cohesion that help to accept and integrate social changes (68). In this section, we will briefly introduce the concept of empathy including its biological underpinnings as it relates to the topic of the current issue.
The fundamentals of empathy
Empathy is considered the capacity to understand, feel and assess what other individuals experience in its context (69). Empathy encompasses many motor, affective-emotional, social, cognitive, and behavioral processes which are mediated by the activity in a set of neural areas, including the temporal pole, the precuneus, the ventromedial prefrontal cortex, the bilateral angular gyrus, the amygdala, the insula, and the sensorimotor cortices (69).
A primer on empathy in the context of social interactions
Success in social interactions is critical for promoting leadership in improving health (70). Social interactions in humans are rooted in different implicit and intrapsychic social cognitive skills (69). Social cognition studies have explored the processes that underlie social and emotional perception and their integration (71): the processes that allow humans to have empathy for others, including the capacity to mimic others’ motor behaviors (motor resonance processes) (72), sharing the emotional and painful experiences of others (affective sharing) (73, 74) and understanding others’ intentions, mental and emotional states (perspective taking) (75); as well as the processes that lead to increased drive and motivation for helping others and behaving in a cooperative manner (cooperative behavior or compassion) (76).
Empathy is so essential for human communication that the lack or loss of empathy are not variants in the human behavioral repertoire; they are symptoms. Two conditions that prominently affect the ability to empathize are psychopathy and behavioral variant frontotemporal dementia (bvFTD). The harmful actions and violation of the rights of others in psychopathy is associated with a lack of empathy (77). In bvFTD, the loss of empathy results in severe problems in close relationships (78). These display that the empathic ability is crucial for our most basic human connections.
In relation to empathy, humans can also behave in cooperative and altruistic forms in certain situations (68, 79–81). Cooperation is an organizing principle in human societies (82, 83). Evolutionary explanations of cooperation were proposed including kin selection, reciprocity and group selection; the extent of the use of these mechanisms and the ability to learn from the others are suggested to be different in humans than other organisms (83). Cooperation is dependent on empathy where individuals’ cooperative capacity are affected by whether they recognize the moral view of the others (84, 85), but empathy is not the sole decisive factor (86). These behaviors are represented in a set of brain areas, including the orbitofrontal cortices and ventral striatum. Moreover, cooperation is determined by other psychological traits including motivation, drive and positive affect all of which promote well-being (87, 88).
Empathy and cooperative behaviors (sometimes referred as compassion behaviors) (76) are crucial skills for promoting leadership in brain health. Public health leaders must understand health disparities, recognize the suffering, and share an urgency to intervene. The impact of actions on improving brain health are highly determined by the level of understanding of individuals to be served. That understanding requires empathy and cooperation (87, 88).
The role of empathy and cooperation in brain health leadership
Measuring an individual’s ability to read the emotional state of others, to be empathetic with their affective states, to infer their mental states and cooperation are vital steps in the development of adaptive forms of leadership. Individuals with high social cognitive skills can use these skills to nurture positive relationships with others. If brain health leaders can reflect on the level of empathy in their leadership decisions, they can succeed in improving the performance of their teams.
One principal form of leadership that relies on empathy and cooperative skills is the servant leadership approach (64). Understanding the emotions, actions and decisions of the people being served is crucial in the operational process of this leadership and this information is used to deploy the team in the most effective way as well as to develop strategies that best fit the target population. This approach helps the leaders elevate non-privileged staff members’ efforts (65).
In brain health, as the suffering of the patients may involve a dehumanizing process in which the patients lose their autonomy; empathy and cooperation become essential features of the medical management. Most of the time, families and close relatives are responsible for the care of the patients, which also puts family members in a vulnerable situation. In those scenarios, empathy is crucial for fitting more humanistic interventions, focused on promoting autonomy and participation, so as the cooperation skills, the ability of behaving to cover for and favor others’ needs.
Empathy and cooperation are both critical to promote brain health changes. However, those processes do not always interact in a parsimonious manner, rather paradoxical interactions may occur. Although some aspects of empathy such as the empathic concern are positively associated with motivation and orientation to help others, different domains of empathy could attenuate prosocial behaviors (89). Notably, personal distress experienced by individuals with high empathy when seeing others’ suffering could sometimes reduce their cooperative skills (90). The emotional responses (i.e., heightened sensitivity and compassion, affective empathy), may reduce the capacity to trigger behavioral motivation to cooperate and to mobilize appropriate actions for helping others (89, 91). The mentioned effect has been previously reported in health settings in which physicians and nurses could be affected by their capacity to help when they experience a high degree of distress toward other’s needs (92–94). High personal distress could affect leaders’ capacity to cope with emotional demands and organize and implement concrete actions for promoting positive changes. Considering that empathy and cooperation are critical processes to initiate actions and promote changes, leaders working in community should be prepared to deal with emotional load.
Empathy and cooperation align with radical collaboration
For successful leadership in global brain health, we find radical collaboration essential. Radical collaboration is a term coined by Tamm and Luyet over 20 years ago, which refers to “an animated network of actors working toward a shared frame of collective action” (95). Its importance is emphasized particularly for global problems where the efforts of single entities do not suffice to overcome the depth of the problem. Radical collaboration settings leverage individuals’ interests and intrinsic motivations while grounding collaboration in freely made commitments between peers (95). By grounding themselves in partnership, peers anchor with empathetic, cooperative, and equitable scenarios, featuring a fluid approach to leadership granted by the trust. These facets of radical collaboration paint a striking alternative to the traditional corporate model by providing more opportunities for the less-privileged actors (96). Radical collaboration has been applied on a global scale by the United Nations General Assembly during the COVID-19 pandemic when responding to global crises and reaching sustainable development goals (97).
Radical collaboration could also be beneficial to tackle brain health challenges particularly in low-income countries in which specific social disparities might play a significant role in brain health (98). Leaders in brain health should establish dialog with local leaders based on empathy and cultural humility to understand the social, medical and cultural conditions that regionally determine brain health. Leaders can then draw, coordinate, and build structured plans. It is essential to recognize the unique challenges faced by each community and to address systemic issues, to effectively promote equity in access to resources and opportunities, and responsive care (99, 100).
Radical collaboration principles have also been applied to resolve issues related to global disparities in brain health. The Atlantic Fellowship for Equity in Brain Health at the GBHI is located in UCSF Memory and Aging Center and Trinity College, Dublin, and offers a year-long fellowship program to professionals including clinicians, scientists, artists, art producers, and economists from around the world (101). The program is sponsored by the Atlantic Institute and run in collaboration with other programs that promote fairer, healthier, and inclusive societies. By embracing diverse perspectives of fellows coming from high-, middle-, and low-income countries within the processes of problem-solving including idea generation, solution finding, and innovation, and practicing empathy and cultural humility, future leaders for equity in brain health facilitate equitable and non-hierarchical interactions, which are critical to overcome misunderstanding, low trusts, interpersonal and political conflicts, facilitate active and lasting collaborations, and stimulate positive societal change.
Conclusion
Disparities exist on different levels between and within countries, affecting brain health from birth to death. Cultural humility is essential in addressing disparities across populations, given their diverse needs and access and the impact that bias and lack of understanding can have on systems and the consequent perpetuation of inequalities. Empathy and its conscious utilization in daily interactions and collaborative models are required for cultural humility, cooperation, and collaboration. It may appear straightforward in the era of globalization but the recorded persistent and growing health and social disparities tell a different story and call for a more active approach.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
This manuscript was prepared as a statement paper following the authors joint presentation at the GBHI Annual Meeting at 2022. All authors contributed to the design and the content of the above mentioned presentation and the manuscript. FF, CL, TM, HS, and YA wrote the first draft. YA wrote the first draft and edited the final manuscript. YA supervised the authorships and the writing of the manuscript. All authors revised the working drafts. All authors contributed to the article and approved the submitted version.
Acknowledgments
This manuscript was prepared based on the session presented by the authors at the 2022 Annual Meeting of the Atlantic Fellows for Equity in Brain Health at the GBHI.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Avan, A, and Hachinski, V, Brain Health Learn and Act Group. Brain health: key to health, productivity, and well-being. Alzheimers Dement. (2022) 18:1396–407. doi: 10.1002/alz.12478
2. Dawson, WD, Smith, E, Booi, L, Mosse, M, Lavretsky, H, Reynolds, CF, et al. Investing in late-life brain capital. Innov Aging. (2022) 6:igac016. doi: 10.1093/geroni/igac016
3. WHO. Brain health. Available at: https://www.who.int/health-topics/brain-health#tab=tab_1 [Accessed May 30, 2023]
4. Chen, Y, Demnitz, N, Yamamoto, S, Yaffe, K, Lawlor, B, and Leroi, I. Defining brain health: a concept analysis. Int J Geriatr Psychiatry. (2021) 37. doi: 10.1002/gps.5564
5. Braveman, P. What are health disparities and health equity? We need to be clear. Public Health Rep. (2014) 129:5–8. doi: 10.1177/00333549141291S203
6. WHO. Health inequities and their causes. (2018). Available at: https://www.who.int/news-room/facts-in-pictures/detail/health-inequities-and-their-causes [Accessed September 12, 2023]
7. Hosseinpoor, AR, and Bergen, N. Health inequality monitoring: a practical application of population health monitoring. In M. Verschuuren, H. van Oers, editors. Population health monitoring: climbing the information pyramid. (Cham: Springer International Publishing) (2018), pp. 151–173.
8. McCartney, G, Collins, C, and Mackenzie, M. What (or who) causes health inequalities: theories, evidence and implications? Health Policy. (2013) 113:221–7. doi: 10.1016/j.healthpol.2013.05.021
9. Homepage - GHS index. (2021). Available at: https://www.ghsindex.org/ [Accessed February 7, 2023]
10. Lock, SL, Chura, LR, Dilworth-Anderson, P, and Peterson, J. Equity across the life course matters for brain health. Nat Aging. (2023) 3:466–8. doi: 10.1038/s43587-023-00413-1
11. WHO. Atlas: country resources for neurologicaldisorders In: WHO and the World Federation of Neurology, editors.World Health Organization. 2nd ed. Geneva: World Health Organization (2017)
13. Barro, R, and Lee, J-W. A new data set of educational attainment in the world, 1950–2010. Cambridge, MA: National Bureau of Economic Research (2010).
14. GBD 2015 Tobacco Collaborators. Smoking prevalence and attributable disease burden in 195 countries and territories, 1990-2015: a systematic analysis from the global burden of disease study 2015. Lancet. (2017) 389:1885–906. doi: 10.1016/S0140-6736(17)30819-X
15. NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in diabetes since 1980: a pooled analysis of 751 population-based studies with 4.4 million participants. Lancet. (2016) 387:1513–30. doi: 10.1016/S0140-6736(16)00618-8
16. NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: a pooled analysis of 1201 population-representative studies with 104 million participants. Lancet. (2021) 398:957–80. doi: 10.1016/S0140-6736(21)01330-1
17. Cole, ER. Intersectionality and research in psychology. Am Psychol. (2009) 64:170–80. doi: 10.1037/a0014564
18. Wu, Y-T, Daskalopoulou, C, Muniz Terrera, G, Sanchez Niubo, A, Rodríguez-Artalejo, F, Ayuso-Mateos, JL, et al. Education and wealth inequalities in healthy ageing in eight harmonised cohorts in the ATHLOS consortium: a population-based study. Lancet Public Health. (2020) 5:e386–94. doi: 10.1016/S2468-2667(20)30077-3
19. Global Peace Index Map. The Most & least peaceful countries. (2023). Available at: https://www.visionofhumanity.org/maps/#/ [Accessed February 7, 2023]
20. Alkire, S, and Chen, L. Global health and moral values. Lancet. (2004) 364:1069–74. doi: 10.1016/S0140-6736(04)17063-3
21. Hudomiet, P, Hurd, MD, and Rohwedder, S. Trends in inequalities in the prevalence of dementia in the United States. Proc Natl Acad Sci U S A. (2022) 119:e2212205119. doi: 10.1073/pnas.2212205119
22. Power, MC, Bennett, EE, Turner, RW, Dowling, NM, Ciarleglio, A, Glymour, MM, et al. Trends in relative incidence and prevalence of dementia across non-Hispanic black and white individuals in the United States, 2000-2016. JAMA Neurol. (2021) 78:275–84. doi: 10.1001/jamaneurol.2020.4471
23. Steenland, K, Goldstein, FC, Levey, A, and Wharton, W. A Meta-analysis of Alzheimer’s disease incidence and prevalence comparing African-Americans and Caucasians. J Alzheimers Dis. (2016) 50:71–6. doi: 10.3233/JAD-150778
24. Lin, P-J, Zhu, Y, Olchanski, N, Cohen, JT, Neumann, PJ, Faul, JD, et al. Racial and ethnic differences in hospice use and hospitalizations at end-of-life among Medicare beneficiaries with dementia. JAMA Netw Open. (2022) 5:e2216260. doi: 10.1001/jamanetworkopen.2022.16260
25. Kornblith, E, Bahorik, A, Boscardin, WJ, Xia, F, Barnes, DE, and Yaffe, K. Association of race and ethnicity with incidence of dementia among older adults. JAMA. (2022) 327:1488–95. doi: 10.1001/jama.2022.3550
26. Mehta, KM, and Yeo, GW. Systematic review of dementia prevalence and incidence in United States race/ethnic populations. Alzheimers Dement. (2017) 13:72–83. doi: 10.1016/j.jalz.2016.06.2360
27. Levine, DA, Gross, AL, Briceño, EM, Tilton, N, Kabeto, MU, Hingtgen, SM, et al. Association between blood pressure and later-life cognition among black and white individuals. JAMA Neurol. (2020) 77:810–9. doi: 10.1001/jamaneurol.2020.0568
28. GCBH. How to sustain brain healthy behaviors: Applying lessons of public health and science to drive change. (2022). Available at: https://www.aarp.org/health/brain-health/global-council-on-brain-health/behavior-change/ [Accessed June 2, 2023]
29. ASPE. National Plan to address Alzheimer’s disease: 2022 update. (2022). Available at: https://aspe.hhs.gov/reports/national-plan-2022-update [Accessed June 2, 2023]
30. Public Health Agency of Canada. A Dementia Strategy for Canada: Together We Aspire. Canada: Ministry of Health (2019).
31. Alzheimer Society of Canada. Understanding how dementia is affecting culturally diverse communities across Canada. (2022). Available at: https://alzheimer.ca/en/whats-happening/news/understanding-how-dementia-affecting-culturally-diverse-communities-across-Canada [Accessed November 13, 2023]
32. Canadian Centre for Economic Analysis. Dementia in Canada: Prevalence and Incidence 2020 to 2050. (2022). Available at: https://www.cancea.ca/index.php/2022/07/16/dementia-in-canada-prevalence-and-incidence-2020-to-2050/ [Accessed November 24, 2023]
33. Trani, J-F, Moodley, J, Maw, MTT, and Babulal, GM. Association of multidimensional poverty with dementia in adults aged 50 years or older in South Africa. JAMA Netw Open. (2022) 5:e224160. doi: 10.1001/jamanetworkopen.2022.4160
34. Mejia-Arango, S, Garcia-Cifuentes, E, Samper-Ternent, R, Borda, MG, and Cano-Gutierrez, CA. Socioeconomic disparities and gender inequalities in dementia: a community-dwelling population study from a middle-income country. J Cross Cult Gerontol. (2021) 36:105–18. doi: 10.1007/s10823-020-09418-4
35. Hojman, DA, Duarte, F, Ruiz-Tagle, J, Budnich, M, Delgado, C, and Slachevsky, A. The cost of dementia in an unequal country: the case of Chile. PloS One. (2017) 12:e0172204. doi: 10.1371/journal.pone.0172204
36. Feter, N, Leite, JS, Alt, R, and Rombaldi, AJ. Ethnoracial disparity among patients with dementia during COVID-19 pandemic. Cad Saude Publica. (2021) 37:e00028321. doi: 10.1590/0102-311x00028321
37. Livingston, G, Huntley, J, Sommerlad, A, Ames, D, Ballard, C, Banerjee, S, et al. Dementia prevention, intervention, and care: 2020 report of the lancet commission. Lancet. (2020) 396:413–46. doi: 10.1016/S0140-6736(20)30367-6
38. GBD 2019 Dementia Forecasting Collaborators. Estimation of the global prevalence of dementia in 2019 and forecasted prevalence in 2050: an analysis for the global burden of disease study 2019. Lancet Public Health. (2022) 7:e105–25. doi: 10.1016/S2468-2667(21)00249-8
39. Prince, MJ, Wimo, A, Guerchet, MM, Ali, GC, Wu, Y-T, and Prina, M. World Alzheimer Report 2015 - The Global Impact of Dementia: An analysis of prevalence, incidence, cost and trends. Alzheimer’s Disease International. (2015). Available at: http://www.alz.co.uk/research/world-report-2015
40. The Lancet Neurology. Disparities in neurological care: time to act on inequalities. Lancet Neurol. (2020) 19:635. doi: 10.1016/S1474-4422(20)30211-8
41. Saadi, A, Himmelstein, DU, Woolhandler, S, and Mejia, NI. Racial disparities in neurologic health care access and utilization in the United States. Neurology. (2017) 88:2268–75. doi: 10.1212/WNL.0000000000004025
42. Kirwan, PD, Hibbert, M, Kall, M, Nambiar, K, Ross, M, Croxford, S, et al. HIV prevalence and HIV clinical outcomes of transgender and gender-diverse people in England. HIV Med. (2021) 22:131–9. doi: 10.1111/hiv.12987
43. McCarron, MO, Clarke, M, Burns, P, McCormick, M, McCarron, P, Forbes, RB, et al. A neurodisparity index of nationwide access to neurological health care in Northern Ireland. Front Neurol. (2021) 12:608070. doi: 10.3389/fneur.2021.608070
44. Dumornay, NM, Lebois, LAM, Ressler, KJ, and Harnett, NG. Racial disparities in adversity during childhood and the false appearance of race-related differences in brain structure. Am J Psychiatry. (2023) 180:127–38. doi: 10.1176/appi.ajp.21090961
45. Yeager, KA, and Bauer-Wu, S. Cultural humility: essential foundation for clinical researchers. Appl Nurs Res. (2013) 26:251–6. doi: 10.1016/j.apnr.2013.06.008
46. Foronda, C. A theory of cultural humility. J Transcult Nurs. (2020) 31:7–12. doi: 10.1177/1043659619875184
47. Tervalon, M, and Murray-García, J. Cultural humility versus cultural competence: a critical distinction in defining physician training outcomes in multicultural education. J Health Care Poor Underserved. (1998) 9:117–25. doi: 10.1353/hpu.2010.0233
48. Schouler-Ocak, M, Bhugra, D, Kastrup, MC, Dom, G, Heinz, A, Küey, L, et al. Racism and mental health and the role of mental health professionals. Eur Psychiatry. (2021) 64:e42. doi: 10.1192/j.eurpsy.2021.2216
49. Stubbe, DE. Practicing cultural competence and cultural humility in the care of diverse patients. Focus (Am Psychiatr Publ). (2020) 18:49–51. doi: 10.1176/appi.focus.20190041
50. Churchwell, K, Elkind, MSV, Benjamin, RM, Carson, AP, Chang, EK, Lawrence, W, et al. Call to action: structural racism as a fundamental driver of health disparities: A presidential advisory from the american heart association. Circulation. (2020) 142:e454–68. doi: 10.1161/CIR.0000000000000936
51. Bailey, ZD, Feldman, JM, and Bassett, MT. How structural racism works - racist policies as a root cause of U.S. racial health inequities. N Engl J Med. (2021) 384:768–73. doi: 10.1056/NEJMms2025396
52. Braveman, PA, Arkin, E, Proctor, D, Kauh, T, and Holm, N. Systemic and structural racism: definitions, examples, health damages, and approaches to dismantling. Health Aff (Millwood). (2022) 41:171–8. doi: 10.1377/hlthaff.2021.01394
53. WHO. Strengthening primary health care to tackle racial discrimination, promote intercultural services and reduce health inequities. Geneva: WHO (2022).
54. Thompson, HS, Manning, M, Mitchell, J, Kim, S, Harper, FWK, Cresswell, S, et al. Factors associated with racial/ethnic group-based medical mistrust and perspectives on COVID-19 vaccine trial participation and vaccine uptake in the US. JAMA Netw Open. (2021) 4:e2111629. doi: 10.1001/jamanetworkopen.2021.11629
55. Bazargan, M, Cobb, S, and Assari, S. Discrimination and medical mistrust in a racially and ethnically diverse sample of California adults. Ann Fam Med. (2021) 19:4–15. doi: 10.1370/afm.2632
56. Musa, D, Schulz, R, Harris, R, Silverman, M, and Thomas, SB. Trust in the health care system and the use of preventive health services by older black and white adults. Am J Public Health. (2009) 99:1293–9. doi: 10.2105/AJPH.2007.123927
57. Kadambari, S, and Vanderslott, S. Lessons about COVID-19 vaccine hesitancy among minority ethnic people in the UK. Lancet Infect Dis. (2021) 21:1204–6. doi: 10.1016/S1473-3099(21)00404-7
58. Aronson, J, Burgess, D, Phelan, SM, and Juarez, L. Unhealthy interactions: the role of stereotype threat in health disparities. Am J Public Health. (2013) 103:50–6. doi: 10.2105/AJPH.2012.300828
59. Amano, T, Ramírez-Castañeda, V, Berdejo-Espinola, V, Borokini, I, Chowdhury, S, Golivets, M, et al. The manifold costs of being a non-native English speaker in science. PLoS Biol. (2023) 21:e3002184. doi: 10.1371/journal.pbio.3002184
60. Haynes-Mendez, K, and Engelsmeier, J. Cultivating cultural humility in education. Child Educ. (2020) 96:22–9. doi: 10.1080/00094056.2020.1766656
61. Morriss-Kay, GM. The evolution of human artistic creativity. J Anat. (2010) 216:158–76. doi: 10.1111/j.1469-7580.2009.01160.x
62. Zaidel, DW. Art and brain: insights from neuropsychology, biology and evolution. J Anat. (2010) 216:177–83. doi: 10.1111/j.1469-7580.2009.01099.x
63. Wang, Y, Pan, Y, and Li, H. What is brain health and why is it important? BMJ. (2020) 371:m3683. doi: 10.1136/bmj.m3683
64. Bruce-Golding, J. Leading change: a reflection on leadership approaches for equity and teacher career progression. Impact. (2021) 11:49–58.
65. Mahsud, R, Yukl, G, and Prussia, G. Leader empathy, ethical leadership, and relations-oriented behaviors as antecedents of leader-member exchange quality. J Manag Psychol. (2010) 25:561–77. doi: 10.1108/02683941011056932
66. McTeer, M. Leadership and public policy. Policy Polit Nurs Pract. (2005) 6:17–9. doi: 10.1177/1527154404272147
67. Holt, S, and Marques, J. Empathy in leadership: appropriate or misplaced? An empirical study on a topic that is asking for attention. J Bus Ethics. (2012) 105:95–105. doi: 10.1007/s10551-011-0951-5
68. Decety, J, Bartal, IB-A, Uzefovsky, F, and Knafo-Noam, A. Empathy as a driver of prosocial behavior: highly conserved neurobehavioral mechanisms across species. Philos Trans R Soc Lond B Biol Sci. (2016) 371:20150077. doi: 10.1098/rstb.2015.0077
69. Frith, CD, and Frith, U. Mechanisms of social cognition. Annu Rev Psychol. (2012) 63:287–313. doi: 10.1146/annurev-psych-120710-100449
70. Skinner, C, and Spurgeon, P. Valuing empathy and emotional intelligence in health leadership: a study of empathy, leadership behavior and outcome effectiveness. Health Serv Manage Res. (2005) 18:1–12. doi: 10.1258/0951484053051924
71. Frith, C. Role of facial expressions in social interactions. Philos Trans R Soc Lond B Biol Sci. (2009) 364:3453–8. doi: 10.1098/rstb.2009.0142
72. Bastiaansen, JACJ, Thioux, M, and Keysers, C. Evidence for mirror systems in emotions. Philos Trans R Soc Lond B Biol Sci. (2009) 364:2391–404. doi: 10.1098/rstb.2009.0058
73. Singer, T, Seymour, B, O’Doherty, J, Kaube, H, Dolan, RJ, and Frith, CD. Empathy for pain involves the affective but not sensory components of pain. Science. (2004) 303:1157–62. doi: 10.1126/science.1093535
74. Singer, T, Seymour, B, O’Doherty, JP, Stephan, KE, Dolan, RJ, and Frith, CD. Empathic neural responses are modulated by the perceived fairness of others. Nature. (2006) 439:466–9. doi: 10.1038/nature04271
75. Melloni, M, Lopez, V, and Ibanez, A. Empathy and contextual social cognition. Cogn Affect Behav Neurosci. (2014) 14:407–25. doi: 10.3758/s13415-013-0205-3
76. Singer, T, and Klimecki, OM. Empathy and compassion. Curr Biol. (2014) 24:R875–8. doi: 10.1016/j.cub.2014.06.054
77. Lockwood, PL. The anatomy of empathy: vicarious experience and disorders of social cognition. Behav Brain Res. (2016) 311:255–66. doi: 10.1016/j.bbr.2016.05.048
78. Takeda, A, Sturm, VE, Rankin, KP, Ketelle, R, Miller, BL, and Perry, DC. Relationship turmoil and emotional empathy in frontotemporal dementia. Alzheimer Dis Assoc Disord. (2019) 33:260–5. doi: 10.1097/WAD.0000000000000317
79. Caprara, GV, Alessandri, G, and Eisenberg, N. Prosociality: the contribution of traits, values, and self-efficacy beliefs. J Pers Soc Psychol. (2012) 102:1289–303. doi: 10.1037/a0025626
80. de Vignemont, F, and Singer, T. The empathic brain: how, when and why? Trends Cogn Sci (Regul Ed). (2006) 10:435–41. doi: 10.1016/j.tics.2006.08.008
81. Drayton, LA, and Santos, LR. Is human prosocial behavior unique? In: JD Greene, I Morrison, and MEP Seligman, editors. Positive Neuroscience. Oxford: Oxford University Press. (2016) 73–88.
82. Nowak, MA. Five rules for the evolution of cooperation. Science. (2006) 314:1560–3. doi: 10.1126/science.1133755
83. West, SA, Cooper, GA, Ghoul, MB, and Griffin, AS. Ten recent insights for our understanding of cooperation. Nat Ecol Evol. (2021) 5:419–30. doi: 10.1038/s41559-020-01384-x
84. Rumble, AC, Van Lange, PAM, and Parks, CD. The benefits of empathy: when empathy may sustain cooperation in social dilemmas. Eur J Soc Psychol. (2009) 40:856–66. doi: 10.1002/ejsp.659
85. Radzvilavicius, AL, Stewart, AJ, and Plotkin, JB. Evolution of empathetic moral evaluation. Elife. (2019) 8. doi: 10.7554/eLife.44269
86. Osman, M, Lv, J-Y, and Proulx, MJ. Can empathy promote cooperation when status and money matter? Basic Appl Soc Psychol. (2018) 40:201–18. doi: 10.1080/01973533.2018.1463225
88. Luengo Kanacri, BP, Eisenberg, N, Tramontano, C, Zuffiano, A, Caprara, MG, Regner, E, et al. Measuring prosocial behaviors: psychometric properties and cross-National Validation of the Prosociality scale in five countries. Front Psychol. (2021) 12:693174. doi: 10.3389/fpsyg.2021.693174
89. Decety, J, and Yoder, KJ. Empathy and motivation for justice: cognitive empathy and concern, but not emotional empathy, predict sensitivity to injustice for others. Soc Neurosci. (2016) 11:1–14. doi: 10.1080/17470919.2015.1029593
90. Chen, J. Empathy for distress in humans and rodents. Neurosci Bull. (2018) 34:216–36. doi: 10.1007/s12264-017-0135-0
91. Lockwood, PL, Ang, Y-S, Husain, M, and Crockett, MJ. Individual differences in empathy are associated with apathy-motivation. Sci Rep. (2017) 7:17293. doi: 10.1038/s41598-017-17415-w
92. Jordan, MR, Amir, D, and Bloom, P. Are empathy and concern psychologically distinct? Emotion. (2016) 16:1107–16. doi: 10.1037/emo0000228
93. Jeffrey, D. Empathy, sympathy and compassion in healthcare: Is there a problem? Is there a difference? Does it matter? J R Soc Med. (2016) 109:446–52. doi: 10.1177/0141076816680120
94. Hunt, P, Denieffe, S, and Gooney, M. Running on empathy: Relationship of empathy to compassion satisfaction and compassion fatigue in cancer healthcare professionals. Eur J Cancer Care (Engl). (2019) 28:e13124. doi: 10.1111/ecc.13124
95. Tamm, J, and Luyet, R. Radical Collaboration. Five Essential Skills to Overcome Defensiveness and Build Successful Relationships. Harper Collins: (2010).
96. Howell, K, and Wilson, BB. Preserving community through radical collaboration: affordable housing preservation networks in Chicago, Washington, DC, and Denver. Hous Theory Soc. (2019) 36:319–37. doi: 10.1080/14036096.2018.1490812
97. Pickering, B, Biro, T, Austin, CC, Bernier, A, Bezuidenhout, L, Casorrán, C, et al. Radical collaboration during a global health emergency: development of the RDA COVID-19 data sharing recommendations and guidelines. Open Res Europe. (2021) 1:69. doi: 10.12688/openreseurope.13369.1
98. Santamaria-Garcia, H, Sainz-Ballesteros, A, Hernandez, H, Moguilner, S, Maito, M, Ochoa-Rosales, C, et al. Factors associated with healthy aging in Latin American populations. Nat Med. (2023) 29:2248–58. doi: 10.1038/s41591-023-02495-1
99. CDC. Social determinants of health: Frequently asked questions. (2019). Available at: https://www.cdc.gov/nchhstp/socialdeterminants/faq.html [Accessed June 2, 2023]
100. U.S. Department of Health and Human Services, Office of Disease Prevention and Health Promotion. Healthy people 2030. Available at: https://health.gov/healthypeople/priority-areas/social-determinants-health [Accessed June 2, 2023]
101. Global Brain Health Institute. Who we are | global brain health institute. Available at: https://www.gbhi.org/about [Accessed September 3, 2023]
Keywords: empathy, brain health, cultural humility, disparity, equity, leadership, value
Citation: Fitri FI, Lage C, Mollayeva T, Santamaria-Garcia H, Chan M, Cominetti MR, Daria T, Fallon G, Gately D, Gichu M, Giménez S, Zuniga RG, Hadad R, Hill-Jarrett T, O’Kelly M, Martinez L, Modjaji P, Ngcobo N, Nowak R, Ogbuagu C, Roche M, Aguzzoli CS, Shin SY, Smith E, Yoseph SA, Zewde Y and Ayhan Y (2023) Empathy as a crucial skill in disrupting disparities in global brain health. Front. Neurol. 14:1189143. doi: 10.3389/fneur.2023.1189143
Edited by:
Stephen D. Ginsberg, Nathan Kline Institute for Psychiatric Research, United StatesReviewed by:
Leonardo Christov-Moore, University of Southern California, United StatesCopyright © 2023 Fitri, Lage, Mollayeva, Santamaria-Garcia, Chan, Cominetti, Daria, Fallon, Gately, Gichu, Giménez, Zuniga, Hadad, Hill-Jarrett, O’Kelly, Martinez, Modjaji, Ngcobo, Nowak, Ogbuagu, Roche, Aguzzoli, Shin, Smith, Yoseph, Zewde and Ayhan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yavuz Ayhan, eWF2dXouYXloYW5AZ2JoaS5vcmc=
†These authors have contributed equally to this work and share first authorship