 Han Su
Han Su Jinlu Yu*†
Jinlu Yu*†- Department of Neurosurgery, First Hospital of Jilin University, Changchun, China
The craniocervical junction (CCJ) is a complex region. Rarely, arteriovenous fistulas (AVFs) can occur in the CCJ region. Currently, it is accepted that CCJ AVFs should only refer to AVFs at the C1-C2 levels. It is reasonable to assume that high cervical CCJ AVFs are being referred to when discussing CCJ AVFs. High cervical CCJ AVFs can be divided into the following four types: dural AVF, radicular AVF, epidural AVF and perimedullary AVF. Until now, it was difficult to understand high cervical CCJ AVFs and provide a proper treatment for them. Therefore, an updated review of high cervical CCJ AVFs is necessary. In this review, the following issues are discussed: the definition of high cervical CCJ AVFs, vessel anatomy of the CCJ region, angioarchitecture of high cervical CCJ AVFs, treatment options, prognoses and complications. Based on the review and our experience, we found that the four types of high cervical CCJ AVFs share similar clinical and imaging characteristics. Patients may present with intracranial hemorrhage or congestive myelopathy. Treatment, including open surgery and endovascular treatment (EVT), can be used for symptomatic AVFs. Most high cervical CCJ AVFs can be effectively treated with open surgery. EVT remains challenging due to a high rate of incomplete obliteration and complications, and it can only be performed in superselective AVFs with simple angioarchitecture. Appropriate treatment can lead to a good prognosis.
1. Introduction
The craniocervical junction (CCJ) is a complex bony region (1). Arteriovenous fistulas (AVFs) are arteriovenous shunting diseases without a nidus that rarely occur in the CCJ region, accounting for 1–2% of all cerebrospinal AVFs (2, 3). CCJ AVFs are uniquely complex due to their inherent angioarchitecture (4–6). CCJ AVFs may present with intracranial hemorrhage due to AVF rupture or edema of the brainstem and upper cervical cord due to venous hypertension (7, 8). For these CCJ AVFs, prompt treatment is needed, mainly including open surgery or endovascular treatment (EVT) (3).
EVT can only be used in certain CCJ AVFs because the feeding arteries of most CCJ AVFs are too small and tortuous, and EVT will result in incomplete obliteration, high recurrence and a risk of complications (9). Currently, open surgery still serves as the first-line treatment for CCJ AVFs. However, open surgery is challenging because of the deep-seated location and complex angioarchitecture of CCJ AVFs (10). Until now, it was difficult to understand the angioarchitecture and provide a proper treatment for CCJ AVFs. Therefore, an updated review of CCJ AVFs is necessary.
2. Definition of high cervical CCJ AVFs
The CCJ region is located between the skull base and the upper cervical spine and is formed by the occipital bone and the first two cervical vertebrae (C1 or atlas and C2 or axis), which span both the lower brainstem and upper cervical cord (Figure 1) (2, 11, 12). The junction of the lower brainstem and upper cervical cord is situated at the level of the most rostral rootlets of the C1 nerve (13, 14). AVFs that occur in the CCJ region are called CCJ AVFs.
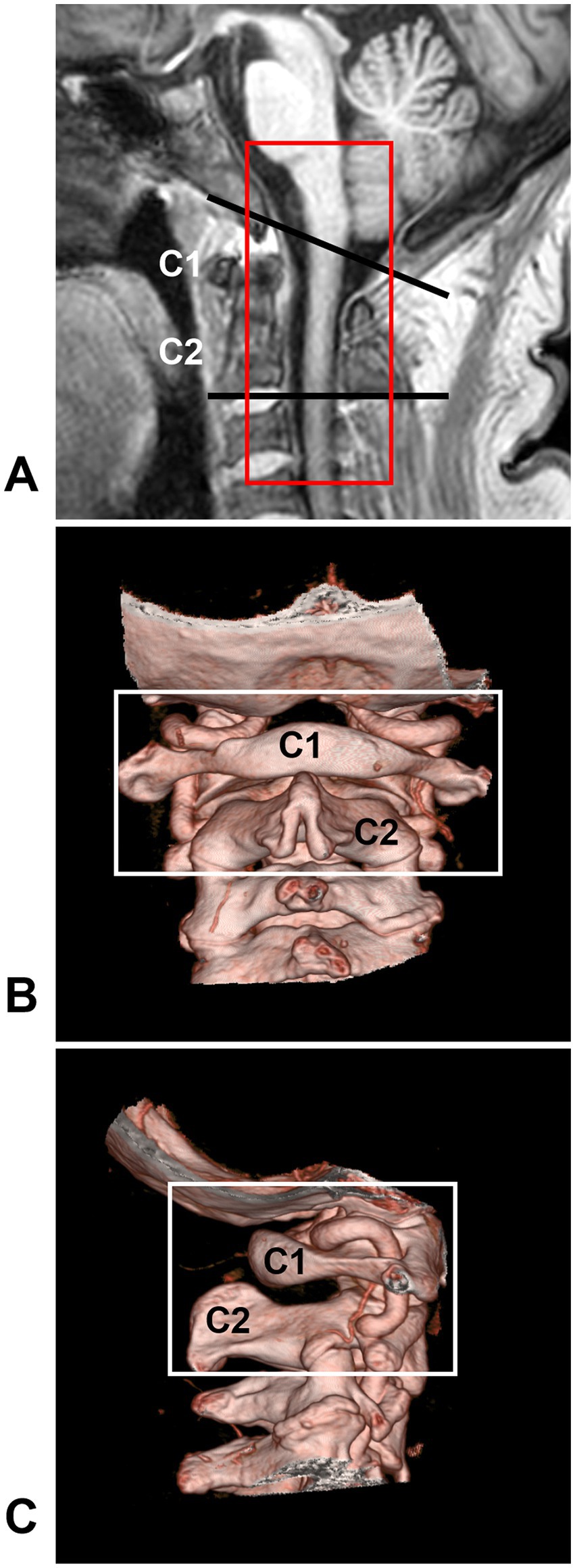
Figure 1. CCJ region definition. (A) MRI showing that the CCJ region was located between two black lines and formed by the occipital bone and C1-2 vertebrae. The red frame indicates the area often involved in CCJ AVF. (B,C) CTA showing the bony CCJ region (frames). AVF, arteriovenous fistula; C1-2, first and second cervical vertebrae; CCJ, craniocervical junction; CTA, computed tomography angiography; MRI, magnetic resonance imaging.
Broadly speaking, CCJ AVFs should contain foramen magnum (FM) DAVFs (15–17). FM DAVFs are located at the anterior condylar confluence, anterior condylar vein (hypoglossal canal), posterior condylar vein (posterior condylar canal), marginal sinus or jugular foramen (18–22). They share similar clinical characteristics and angioarchitectures, and their feeding arteries are derived from the ascending pharyngeal artery (AphA), occipital artery (OA), and posterior meningeal artery of the vertebral artery (VA); their veinous drainage flows into the adjacent sinuses or condylar vein system (17, 20, 23–31).
CCJ AVFs at the C1-C2 levels are different from FM DAVFs, although they include the same elements of FM DAVFs and share a similar drainage pathway (32). Angioarchitectures of CCJ AVFs at the C1-C2 levels are more similar to spinal DAVFs in fistula structure and feeding arteries (4, 30). Therefore, according to some authors’ suggestions, CCJ AVFs should only refer to AVFs at the C1-C2 levels, and FM DAVFs or spinal AVFs at C3 and lower levels should not be included as CCJ AVFs (33–37). In our opinion, we consider the term ‘high cervical CCJ AVFs’ to be more appropriate when discussing CCJ AVFs.
3. Vessel anatomy of the high cervical CCJ region
3.1. Arterial branches
The arteries involved in the high cervical CCJ region mainly originate from the suboccipital V3 segment of the VA, including the radicular (or radiculomeningeal, radiculopial or radiculomedullary) artery, anterior and posterior spinal arteries (ASA and PSA), posterior inferior cerebellar artery (PICA), anterior and posterior meningeal arteries, and some muscular branches (Figures 2A–F) (38–40). Additional contributors include the meningeal branches of AphA and OA (Figures 2G,H) (35, 40–42).
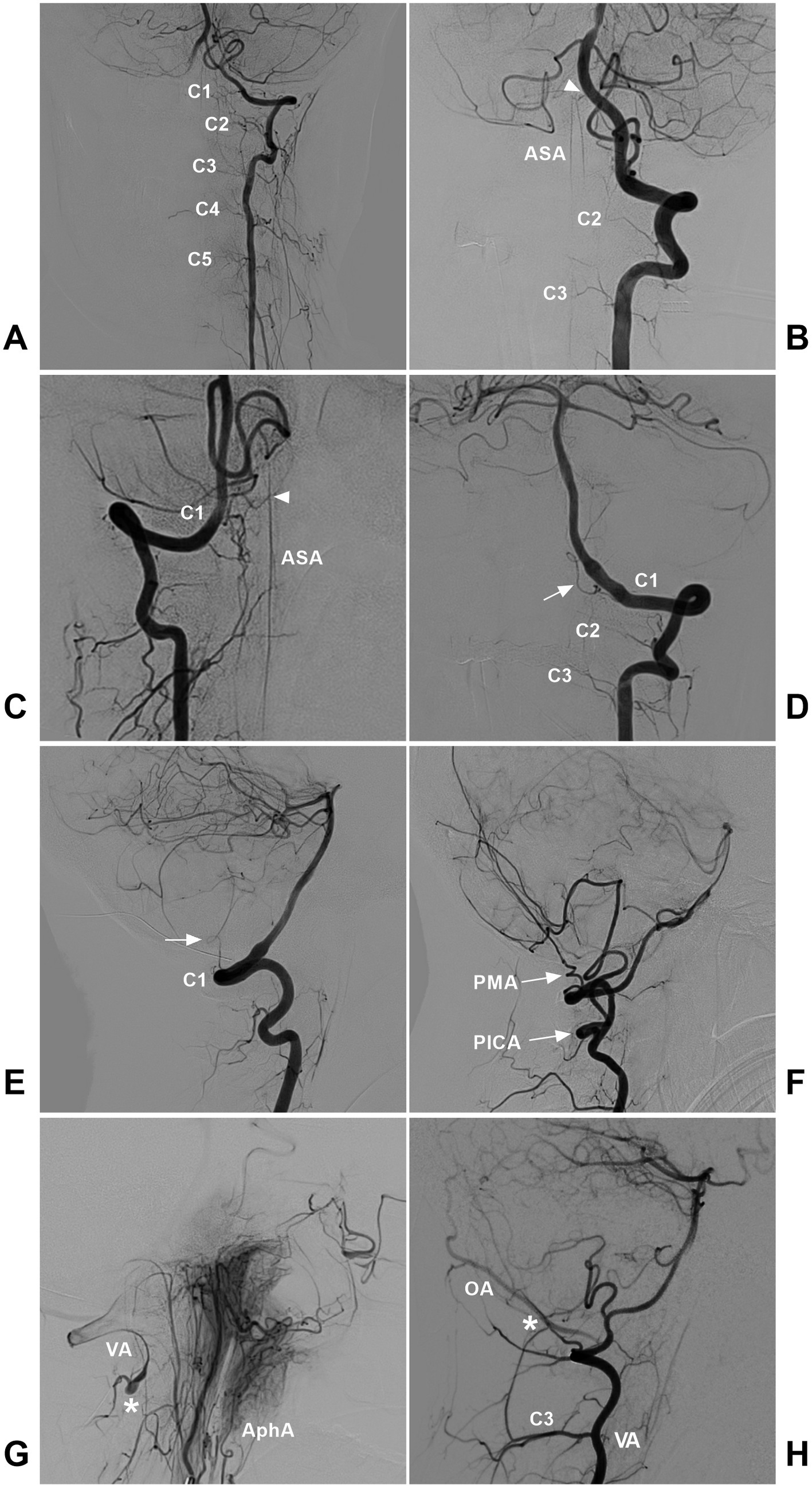
Figure 2. Arteries involved in the high cervical CCJ region. (A) DSA showing the radicular arteries from the VA at the C1-C5 levels. (B) DSA showing the ASA (arrowhead) from VA termination. The ASA had double trunks, and the radicular arteries of the C2-C3 levels could be seen. (C) DSA showing the ASA (arrowhead) originating from the C1 radicular artery. (D,E) DSA of anterior posterior (D) and lateral (E) views showing the C1 radicular artery (arrow). (F) DSA showing the extradural low PICA (PICA with arrow) and the PMA (PMA with arrow) from the VA. (G) DSA showing the anastomosis (asterisk) between the AphA and VA. (H) DSA showing the anastomosis (asterisk) between the OA and muscular branch of the VA. AphA, ascending pharyngeal artery; ASA, anterior spinal artery; C1-C5, first-fifth cervical vertebrae; CCJ, craniocervical junction; DSA, digital subtracted angiography; OA, occipital artery; PICA, posterior inferior cerebellar artery; PMA, posterior meningeal artery; VA, vertebral artery.
The high cervical cord has little radicular inflow, and the radicular arteries are often thin or invisible on digital subtracted angiography (DSA) (Figure 2A) (43, 44). The C1 nerve root is adherent to the VA inferior surface, where the VA gives rise to the C1 radicular artery (Figures 2D,E) (13, 45). The C2 radiculomuscular artery is constant and arises from the VA under the C1 transverse foramen and gives rise to the radicular artery (13, 38, 46). Occasionally, the C3 radicular artery may supply the CCJ region (35). In addition, above the C1 posterior arch, a muscular branch consistently arises from the VA (38). The ASA formed by the union of the paired anterior ventral spinal arteries from intradural VAs or radiculomedullary arteries descends to the CCJ region (Figures 2B,C) (47). The PSAs may arise from the posteromedial surface of the VAs, just outside the dura mater, but they may also be derived from the PICA (48).
3.2. Venous drainage
Venous drainage in the high cervical CCJ region is abundant, complex and varied, including the extradural and intradural drainage systems (13, 14, 49, 50). The extradural drainage system includes the anastomosed paravertebral and epidural venous plexuses (38, 51). The paravertebral venous plexus communicates with the deep jugular vein, sigmoid sinus and suboccipital venous plexus (Figure 3) (13, 40, 52). The intradural drainage system includes the veins of the lower brainstem and upper cervical cord and anterior/posterior median/lateral spinal veins anastomosed with the veins of the medulla oblongata (13, 14, 34). In addition, several bridging veins collect drainage from the lower brainstem and upper cervical cord into adjacent sinuses or the venous plexus via the radicular vein along nerve rootlets (13, 34).

Figure 3. Venous plexuses in the CCJ region. (A) Posterior anterior view (left panel) and oblique view (right panel) CTA showing the anastomosed SVP, PVVP, and DJV. (B) Oblique view (left panel) and lateral view (right panel) CTA showing the anastomosed PVVP and DJV. C1, C2, first and second cervical vertebrae; CCJ, craniocervical junction; CTA, computed tomography angiography; DJV, deep jugular vein; EJV, external jugular vein; IJV, internal jugular vein; PVVP, paravertebral venous plexus; SVP, suboccipital venous plexus.
4. Angioarchitecture of high cervical CCJ AVFs
4.1. Classification and angioarchitecture
High cervical CCJ AVFs can be located on the inner or outer surface of the dura mater, on the spinal nerves, or on the spinal cord surface and can be divided into the following four types: DAVFs, radicular AVFs (RAVFs), epidural AVFs (EAVFs), and perimedullary AVFs (PAVFs) (Figures 4, 5), in which DAVFs and RAVFs tend to occur at the C1 level and EAVFs and PAVFs tend to occur at the C2 level (10, 33, 53, 54).
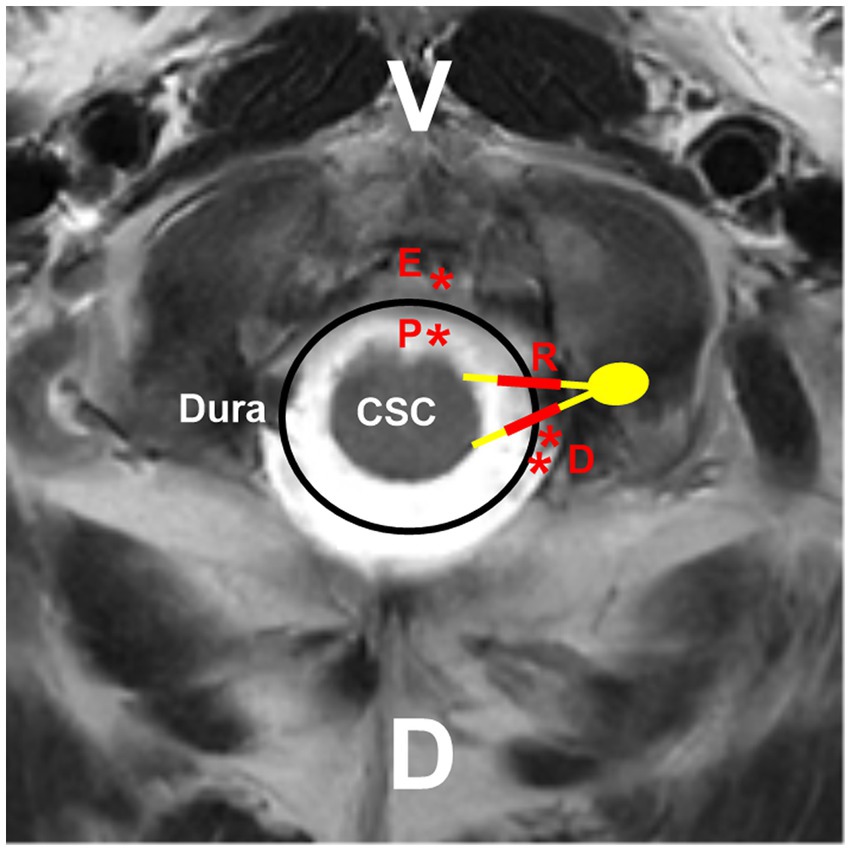
Figure 4. Locations of different high cervical CCJ AVFs. On the hybrid mode pattern of magnetic resonance imaging, the locations of different high cervical CCJ AVFs are shown. PAVF (red P with asterisk) located at the ventral spinal cord surface, RAVF (red R with thick line segments) located at C1-C2 nerves, DAVF (red D with double asterisks) located at the dorsal dura, EAVF (red E with asterisk) in ventral epidural space. AVF, arteriovenous fistula; C1-C2, first and second cervical vertebrae; CCJ, craniocervical junction; CSC, cervical spinal cord; D, dorsal; DAVF, dural AVF; EAVF, epidural AVF; PAVF, perimedullary AVF; RAVF, radicular AVF; V, ventral.
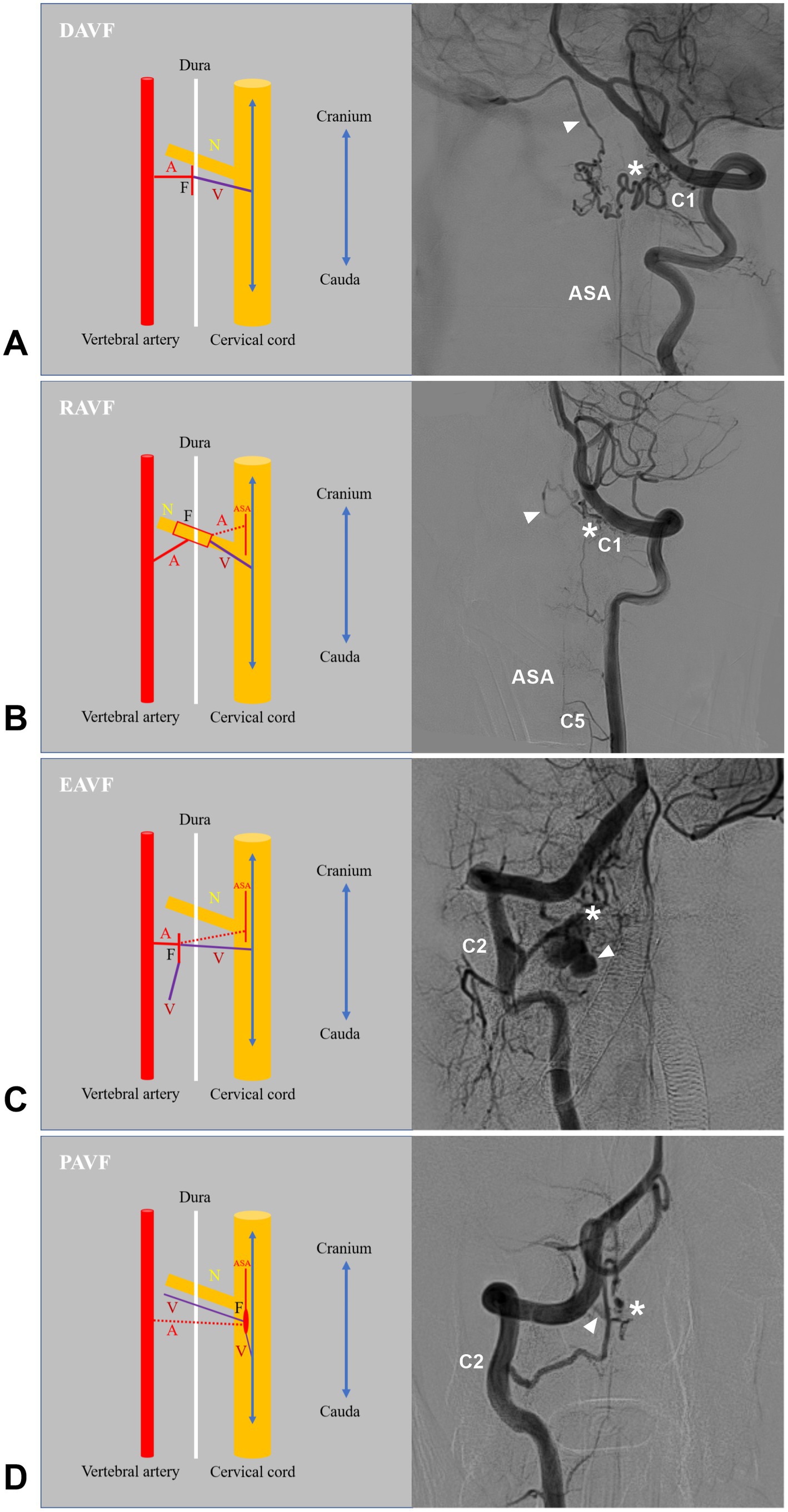
Figure 5. Types of high cervical CCJ AVFs. (A) Left panel showing the structure of DAVF in drawing, a radiculomeningeal artery and a radicular vein connected directly on dural sleeve of nerve root; Right panel showing the angioarchitecture of DAVF, the feeding artery was the C1 radicular artery, the asterisk indicated fistula point, and the arrowhead indicate the drainage into intracranial vein to sigmoid sinus. (B) Left panel showing the structure of the RAVF in drawing, a radicular (radiculomeningeal) artery and a radicular vein connected directly on the spinal nerve root. The ASA branch can be involved as the feeder (dotted line); right panel showing the angioarchitecture of the RAVF. The feeding artery was the C1 radicular artery, the asterisk indicates the fistula point, and the arrowhead indicates drainage into the intracranial vein. (C) Left panel showing the structure of the EAVF in the drawing. There is a direct arteriovenous shunt between the radicular and/or meningeal arteries and the epidural venous plexus. The ASA branch can be involved as the feeder (dotted line); right panel showing the angioarchitecture of the EAVF. The feeding artery is the C2 radicular artery, the asterisk indicates the fistula point, and the arrowhead indicates the drainage. (D) Left panel showing the structure of the PAVF in the drawing. The PAVF is a direct arteriovenous communication without an intervening nidus on the surface of the spinal cord; right panel showing the angioarchitecture of the PAVF. The feeding artery was the C2 radiculomedullary artery, the asterisk indicates the fistula point, and the arrowhead indicates the drainage. A, feeding artery; ASA, anterior spinal artery; AVF, arteriovenous fistula; C1, C2, and C5, first, second and fifth cervical vertebrae; CCJ, craniocervical junction; DAVF, dural AVF; EAVF, epidural AVF; F, fistula point; N, nerve; PAVF, perimedullary AVF; RAVF, radicular AVF; V, draining vein.
High cervical CCJ AVFs may be single or multiple AVFs, and less than 10% of AVFs are multiple AVFs (4, 7, 55). Multiple AVFs may be homogeneous, such as bilateral DAVFs, bilateral RAVFs or bilateral EAVFs (4, 53, 55–57). More often, multiple AVFs are heterogeneous. Different types of AVFs may coexist due to venous hypertension and thrombosis, such as the combinations of DAVF and PAVF, RAVF and PAVF, DAVF and EAVF and PAVF, and DAVF and RAVF and PAVF (2–4, 35, 53, 58–60).
High cervical CCJ AVFs present with multiple feeding arteries connecting to the same draining vein (5). They are mainly fed by the radicular (radiculomeningeal, radiculopial or radiculomedullary) arteries of the VA (Figure 5) and rarely fed by the branch of the low-positioned PICA (Figure 6) (3, 36). Feeding arteries of high cervical CCJ AVFs may be bilateral or multiple segmental (7, 33, 35). Spinal pial arteries from the ASA and PSA (or posterior lateral spinal artery) can be involved in more than half of CCJ AVFs (33). Sometimes, meningeal branches of the AphA and OA can be involved in the feeders for CCJ DAVFs (7, 33, 61). Due to hemodynamic stress, flow-related aneurysms can occur on the feeding artery (34, 53, 59, 62). The rate is not low; in a report by Song et al. (7) aneurysmal structures occurred in 26.2% of CCJ AVFs.
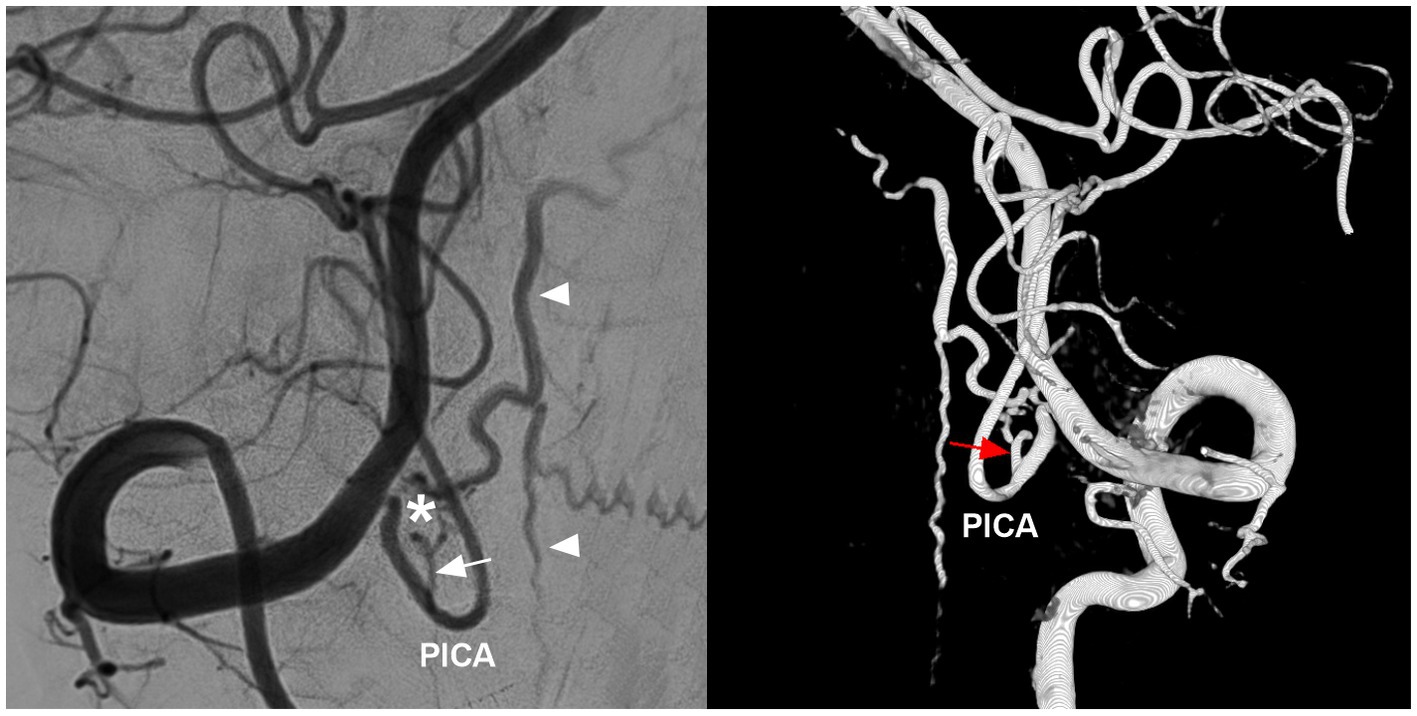
Figure 6. PICA involvement in the feeding artery of high cervical CCJ RAVF. DSA (left panel) and three-dimensional reconstructive DSA (right panel) showing a high cervical CCJ RAVF (asterisk in left panel) fed by the branch of the PICA (arrows); arrowheads in left panel indicate upward and downward draining veins. AVF, arteriovenous fistula; CCJ, craniocervical junction; DSA, digital subtracted angiography; PICA, posterior inferior cerebellar artery; RAVF, radicular AVF.
Most CCJ AVFs had intradural venous drainage, which was ventral to the medulla oblongata or spinal cord (9). Normally, venous drainage of the upper cervical cord flows downward to reach the outlet along the adjacent nerve root by bridging and radicular veins into the lateral epidural venous plexus. When CCJ AVFs occur, due to high hemodynamic pressure, draining veins may extend downward very far, even as far as the thoracic or sacral levels, to reach the outlet (63). High cervical CCJ AVFs also had upward intradural drainage. Even the draining veins can reflux upward into the intracranial venous system due to rich anastomosis (3, 4, 10, 36, 44, 55, 58, 61, 64). Due to the overload of the draining vein, drainage may involve multiple veins or multiple pathways (Figure 7) (33).
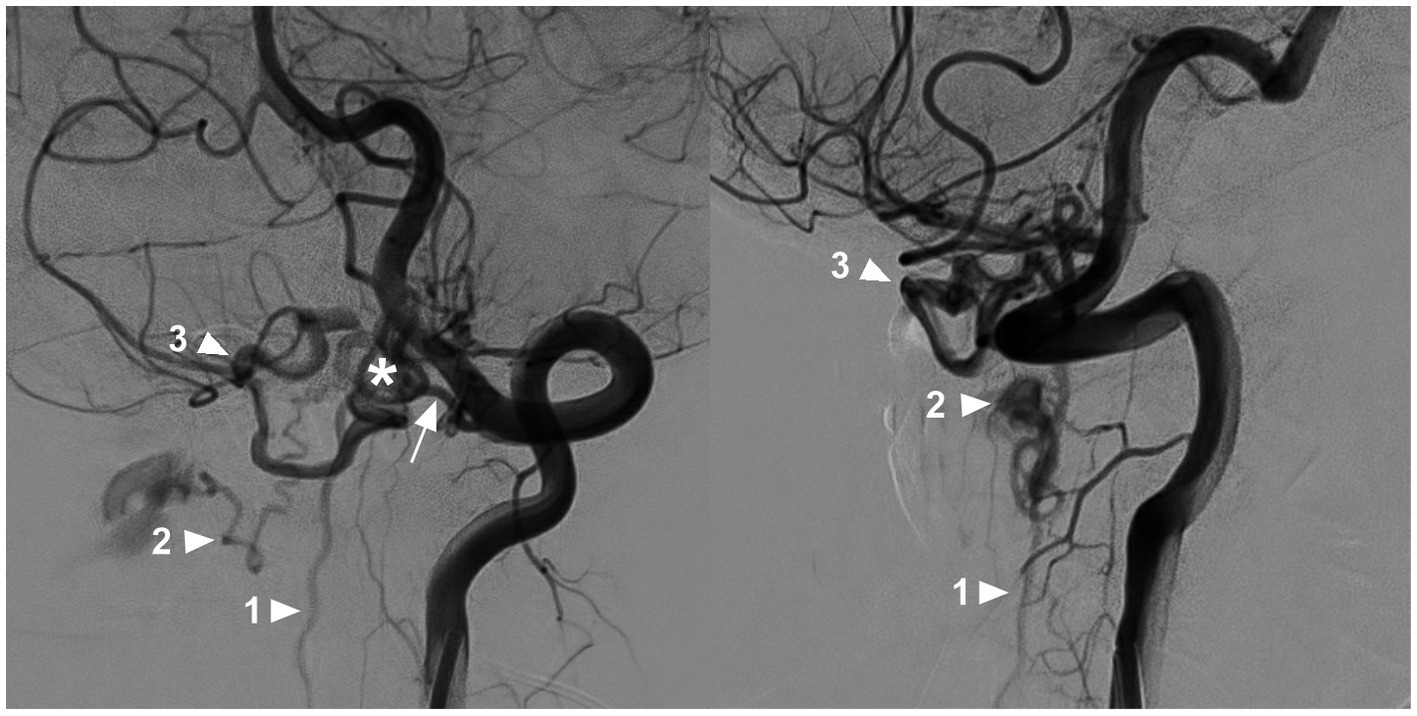
Figure 7. Multiple draining pathways in a high cervical CCJ AVF. Oblique-view DSA of the VA showing a CCJ AVF (asterisk in left panel) supplied by the C1 radicular artery (arrow in left panel); the drainage of the AVF had three pathways: downward into the perimedullary vein (arrowhead with number 1), lateral into the epidural venous plexus (arrowhead with number 2), and upward into the intracranial vein (arrowhead with number 3). AVF, arteriovenous fistula; C1, first cervical vertebrae; CCJ, craniocervical junction; DSA, digital subtracted angiography; VA, vertebral artery.
The drainage pattern of CCJ AVFs determines their clinical manifestation. CCJ AVFs with downward drainage mainly result in congestive myelopathy (Figure 8), whereas those with upward drainage usually result in hemorrhage due to draining vein rupture (Figures 9, 10) (4, 65, 66). In addition, increased hemodynamic stress may lead to varices of the draining veins in nearly 80% of high cervical CCJ AVFs (36, 53, 55).
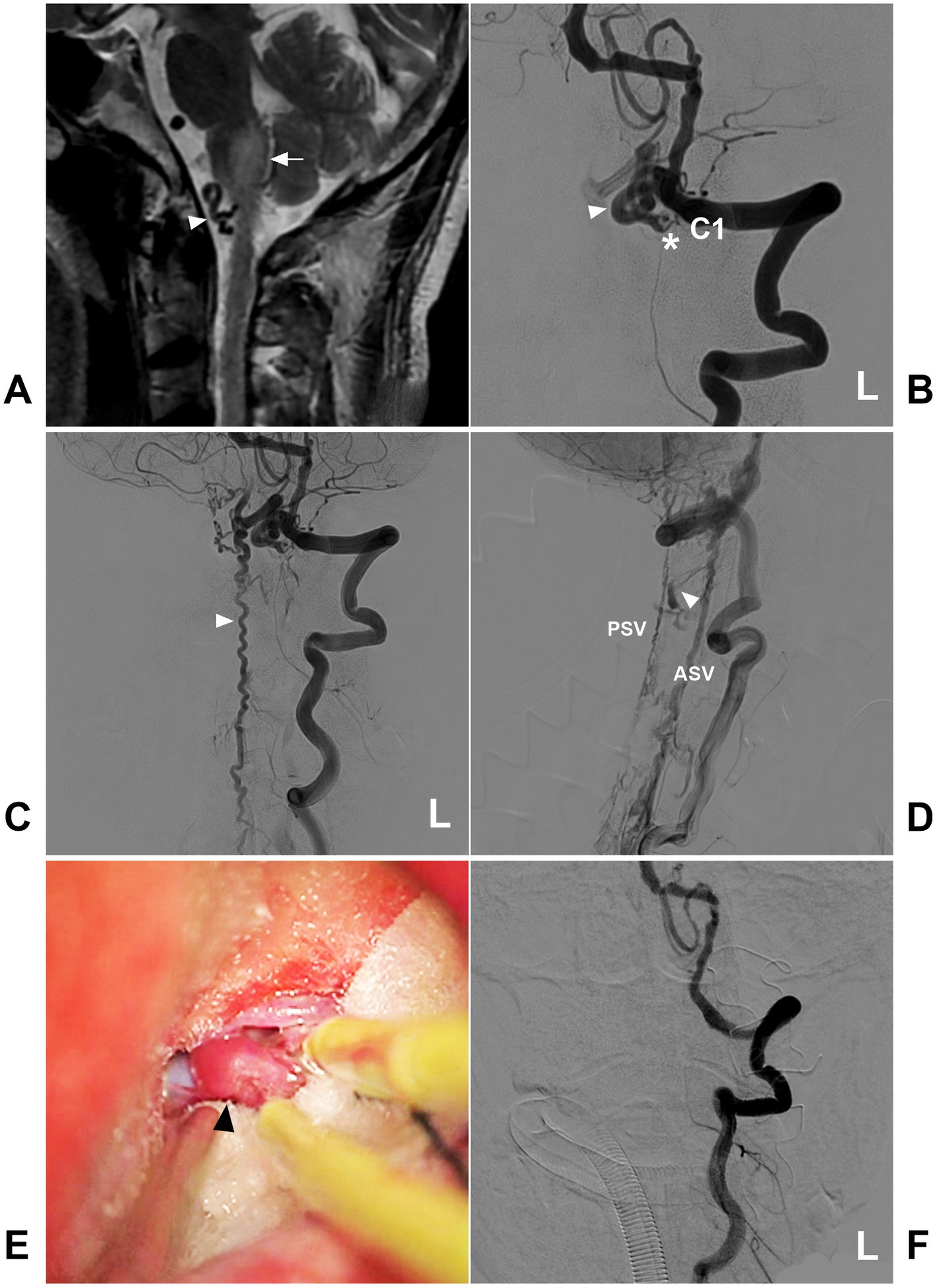
Figure 8. Open surgery in a high cervical CCJ DAVF with downward drainage. (A) MRI showing edema (arrow) of the medulla oblongata and abnormal vessels (arrowhead) in the front of the brainstem. (B) Arterial phase DSA of the left VA showing a CCJ DAVF (asterisk) fed by the C1 radicular artery. The drainage went into the intracranial vein (arrowhead). (C) Late arterial phase DSA of the anterior posterior view showing downward drainage into the perimedullary vein (arrowhead). (D) Late arterial phase DSA of the lateral view showing downward drainage, including downward ASV and PSV, and lateral drainage by the bridging and radicular veins (arrowhead). (E) Intraoperative image showing the thick arterialized draining vein (arrowhead). (F) Postoperative DSA showing that the DAVF was obliterated after the draining vein was coagulated and cut. ASV, anterior spinal vein; C1, first cervical vertebra; CCJ, craniocervical junction; DAVF, dural arteriovenous fistula; DSA, digital subtraction angiography; L, left; MRI, magnetic resonance imaging; PSV, posterior spinal vein; VA, vertebral artery.
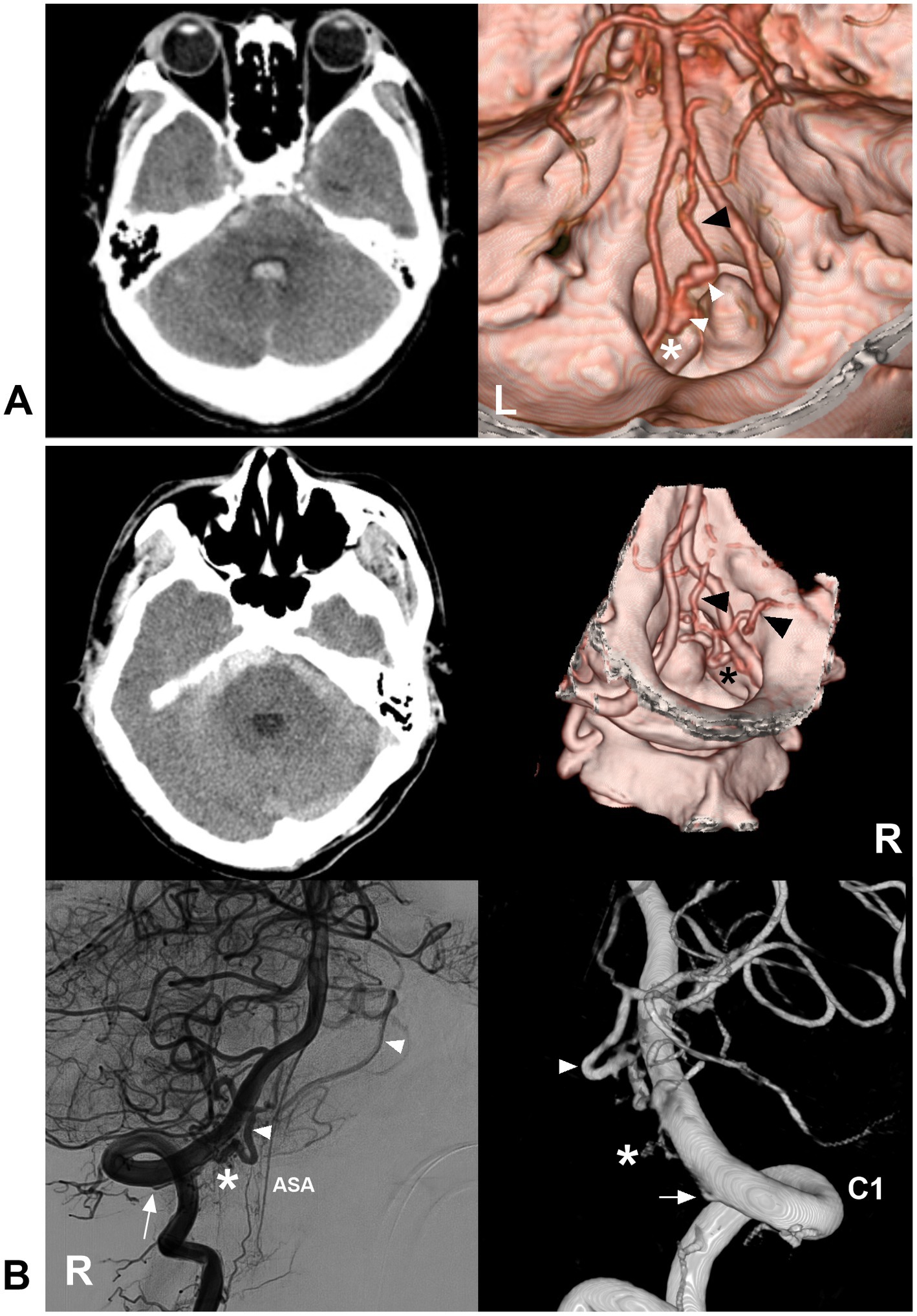
Figure 9. Ruptured CCJ AVF with upward drainage. (A) Left panel: CT showing subarachnoid hemorrhage and fourth ventricle hemorrhage; Right panel: CTA showing that a CCJ AVF (asterisk) had upward venous drainage (black arrowhead) with varices (white arrowheads). (B) Left upper panel: CT showing subarachnoid hemorrhage; right upper panel: CTA showing that a CCJ AVF (asterisk) had upward venous drainage (arrowheads); two-dimensional DSA (left below panel) and three-dimensional DSA (right below panel) showing a RAVF (asterisks) fed by the C1 radicular artery (arrows). The drainage went into the intracranial vein (arrowheads). AVF, arteriovenous fistula; C1, first cervical vertebrae; CCJ, craniocervical junction; CT, computed tomography; CTA, CT angiography; DSA, digital subtracted angiography; RAVF, radicular AVF.
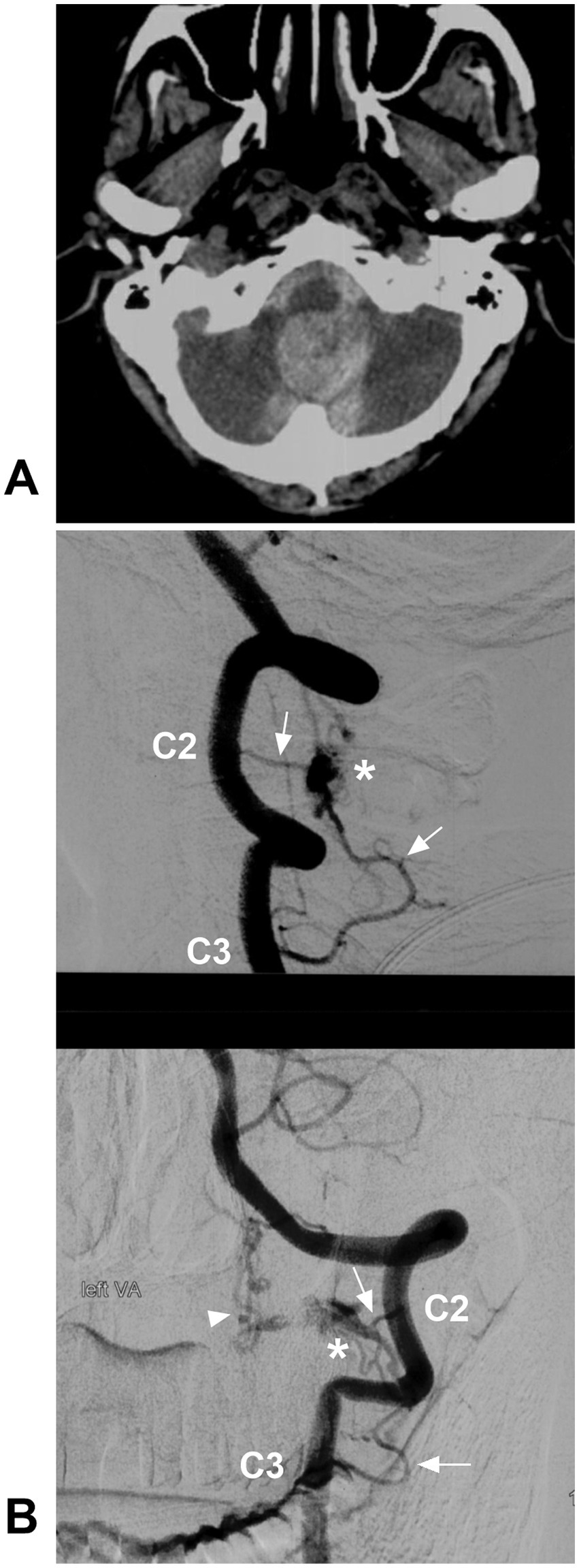
Figure 10. Ruptured CCJ RAVF with upward drainage. (A) CT showing subarachnoid and cisterna magna hemorrhage. (B) Lateral view (upper panel) and anterior posterior view (below panel) DSA of the VA showing an RAVF (asterisks) fed by the C2 and C3 radicular arteries (arrows) and with upward venous drainage (arrowhead in below panel). AVF, arteriovenous fistula; C2 and C3, second and third cervical vertebrae; CCJ, craniocervical junction; CT, computed tomography; DSA, digital subtracted angiography; RAVF, radicular AVF; VA, vertebral artery.
Of these high cervical CCJ AVFs, DAVF tends to present with venous congestion; Intradural RAVF and PAVF tend to accompany aneurysm in fistula and varix on draining vein and may present with hemorrhage (2, 32, 33, 44, 67). In CCJ DAVFs, the unique gadolinium enhancement pattern presenting with a “missing-piece sign” on magnetic resonance imaging (MRI) has been reported as a unique radiologic finding to lead to the early diagnosis of CCJ DAVFs (68). The finding was defined as at least one focal geographic nonenhancing area within a long (>2 vertebral segments) and intensely enhanced segment (69).
4.2. Characteristics of each AVF
4.2.1. DAVF
DAVFs are the most common AVFs in the high cervical CCJ region, accounting for 2.23% of brain and spinal DAVFs (4, 7, 33). They are defined as an abnormal shunt between a radiculomeningeal artery and a radicular vein along the dural sleeve of C1-C2 nerve roots and drain into the intradural veins (Figure 5A) (2, 36). Rarely, the external carotid artery can be involved as a feeder (33–36, 61, 70). High cervical CCJ DAVFs are often fed by dural arteries alone and attached to the dura, and the fistula is wide and irregular. CCJ DAVFs may have upward or downward intradural drainage or lateral epidural drainage (2, 33, 35, 71). For CCJ DAVFs, contrast-enhanced computed tomography angiography and magnetic resonance angiography were useful to detect vascular abnormalities, i.e., dilated draining veins (2).
ASA and PSA can be involved in CCJ DAVFs. According to the feeding arteries and their relationships with the ASA and PSA, Choi et al. (54) classified CCJ DAVFs into three types: type 1 was fed by the radiculomeningeal artery from the VA and was not associated with the ASA or PSA; type 2 was fed by the radiculomeningeal artery, and the radicular artery also supplied the PSA near the fistula point; type 3 had the characteristics of type 1 or type 2 DAVFs, except the ASA also contributed to the fistula; and type 3 was uncommon.
4.2.2. RAVF
RAVFs are defined as the direct communication between a radicular (radiculomeningeal) artery and a radicular vein on spinal C1-C2 nerve roots (Figure 5B) (72, 73). They can be in the extradural or intradural space, and most of them have intradural drainage (3, 32, 33, 72). High cervical CCJ RAVFs have similar appearances to DAVFs, and they are often misdiagnosed as DAVFs (33). However, they are different. RAVFs are often fed by both dural and pial arteries and are located between the dura and spinal cord, usually supplied by the spinal pial artery, but involvement of these arteries is thought to be rare in DAVFs. (Figure 6) (32). RAVFs are often narrow and limited along the spinal nerve root (Figures 9B, 10) (32, 34, 59). Fusion imaging with DSA and MRI might reinforce the differential diagnosis for these two types (32).
4.2.3. EAVF
High cervical CCJ EAVFs are not uncommon (33). They are usually in the ventral epidural space and are an arteriovenous shunt between the radicular and/or meningeal arteries and the epidural venous plexus without a nidus-like structure (Figure 5C) (2, 5, 74). When the epidural venous plexus is opacified directly by any arteries, it is considered an EAVF (32). According to the involvement of the spinal pial artery, they are divided into EAVF with/without pial feeders (5, 33). According to the involvement of the draining vein, EAVFs are divided into types A and B, of which type A fistulas have both epidural and intradural venous drainages, and type B fistulas have only the epidural draining vein (75).
High cervical CCJ EAVFs without the spinal pial artery as the feeder or intradural drainage are generally benign (76). Compared with other CCJ AVFs, EAVFs may have wider drainage, such as the suboccipital venous plexus or posterior cervical vein (32, 56).
4.2.4. PAVF
High cervical CCJ PAVFs are characterized by direct arteriovenous communication without an intervening nidus on the spinal cord surface that consists of single or multiple holes and drains into a single vein (Figure 5D) (33, 77). Most CCJ PAVFs are located ventral or ventrolateral to the cervical cord (62). CCJ PAVFs may often have multiple feeding arteries from the radiculomedullary artery and/or spinal pial arteries and directly drain into the perimedullary veins (3, 33–35, 62). CCJ PAVFs tend to have a high flow nature, so they are often associated with venous varices in the fistulous site or draining vein.
5. Treatment options for high cervical CCJ AVFs
High cervical CCJ AVFs can often present as acute hemorrhage, myelopathy, brainstem dysfunction, radiculopathy, etc. (2, 4, 36, 44, 53, 61, 66, 78–81). For symptomatic or ruptured high cervical CCJ AVFs, treatment should be prompt, including open surgery, EVT or both (53). In general, EVT is useful for EAVFs, rather than other dural and intradural AVFs. Direct surgery may be safe for CCJ AVFs. Therefore, the optimal treatment modality should be examined in the anatomy and type of AVF. In asymptomatic CCJ AVFs without intradural drainage or pial feeder aneurysms, conservative treatment can be considered (32).
5.1. EVT
Although EVT reportedly has the benefit of being a minimally invasive procedure, it is not the best choice for high cervical CCJ AVFs (44, 80, 82). In EVT, the feeding arteries are usually very thin and tortuous and arise from the VA at a straight angle, which makes transarterial catheterization difficult for the fistula (66). Due to substantial feeder vessel tortuosity and diminutive caliber, transarterial EVT may harbor a risk of vessel perforation during microcatheterization. It is difficult to obliterate AVF without spinal cord infarction (Figure 11) (2, 83). EVT is only considered in CCJ AVFs with simple angioarchitecture, such as those with a single feeding artery and no pial feeding artery (Figure 12) (3). For type 1 CCJ DAVFs, EVT may be considered (54). For instance, in the report by Murase et al., a CCJ DAVF with a single feeding artery was successfully embolized by glue under the balloon-assisted technique (66).
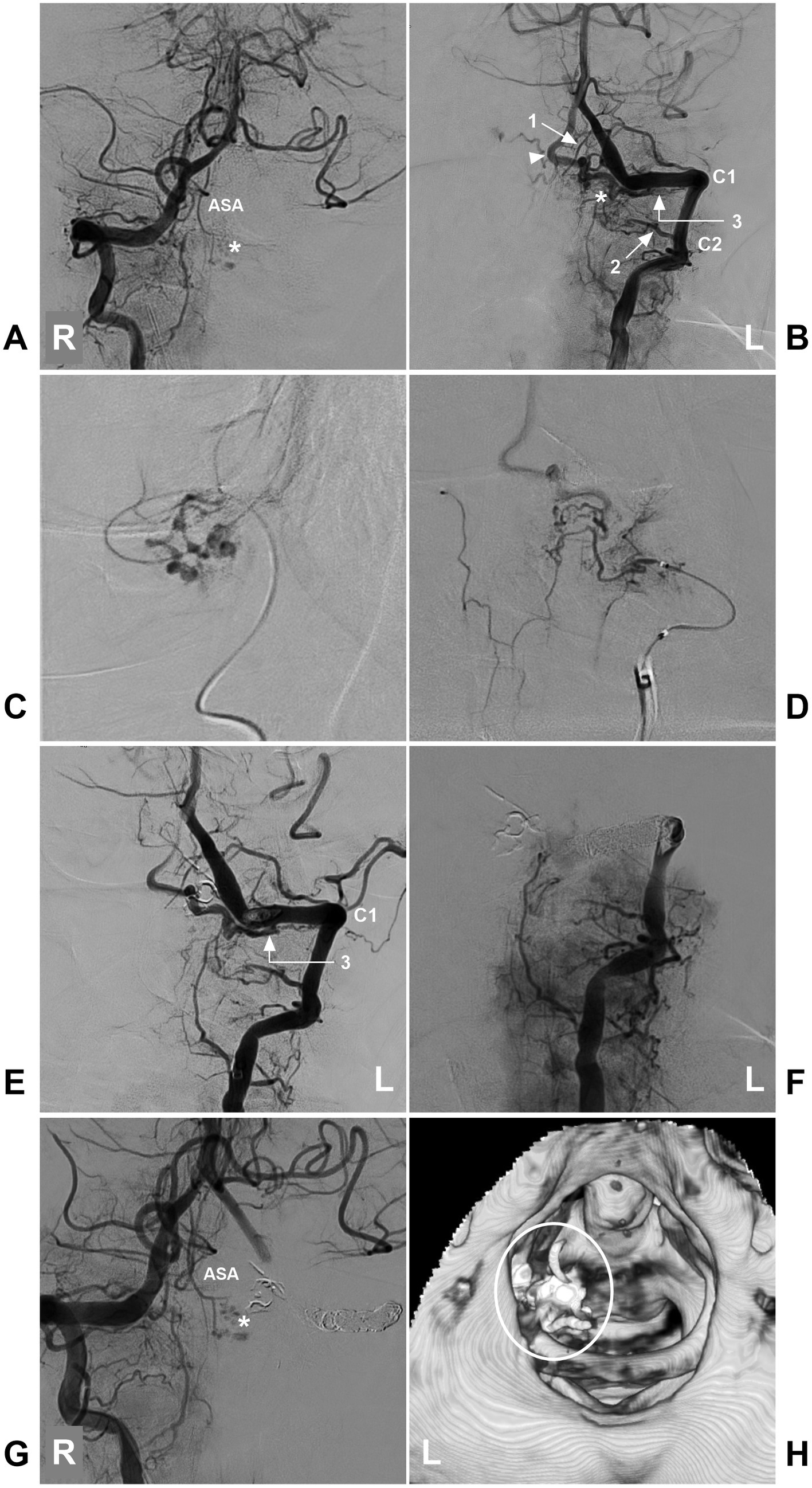
Figure 11. Incomplete EVT in a high cervical CCJ RAVF. (A) DSA of the left VA showing that the ASA supplied the AVF (asterisk). (B) DSA of the right VA showing that the AVF (asterisk) was fed by a brainstem perforating branch of the VA (arrow with number 1), the C2 (arrow with number 2) and C1 (arrow with number 3) radicular arteries, and the arrowhead indicates the draining vein. (C) Selective angiography of the brainstem perforating branch of the VA (arrow with number 1 in B) showing it to supply a part of the AVF. (D) Selective angiography of the C2 radicular artery (arrow with number 2) showing it to supply a part of the AVF. (E) After casting Onyx via two feeding arteries (numbers 1 and 2 in B), DSA of the left VA showing that the AVF was supplied by the C1 radicular artery (number 3 with arrow), confirming RAVF presentation. (F) DSA of the left VA showing that the VA was completely occluded by coiling, and the AVF could not be seen. (G) DSA of the right VA showing a part of the AVF (asterisk) was left. (H) Post-EVT CT reconstruction showing casting Onyx (ellipse), indicating the location of the RAVF. ASA, anterior spinal artery; AVF, arteriovenous fistula; C1-2, first and second cervical vertebrae; CCJ, craniocervical junction; CT, computed tomography; DSA, digital subtracted angiography; EVT, endovascular treatment; L, left; R, right; RAVF, radicular AVF; VA, vertebral artery.
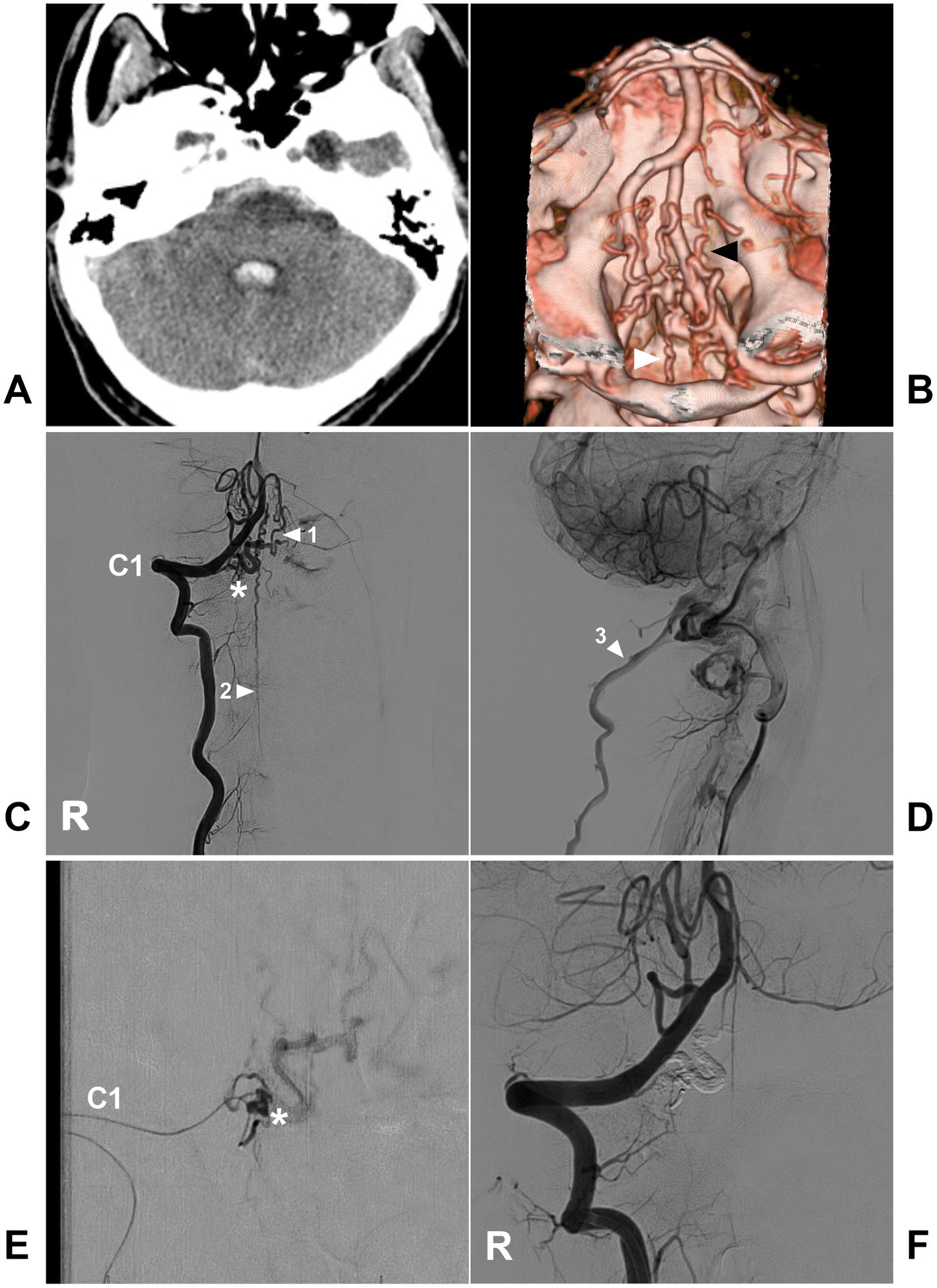
Figure 12. Complete EVT in a CCJ DAVF with a single feeding artery. (A) CT showing subarachnoid hemorrhage and fourth ventricle hemorrhage. (B) CTA showing multiple dilated abnormal veins (arrowheads). (C) Arterial phase DSA of the right VA showing a CCJ DAVF (asterisk) fed by the C1 radicular artery. The drainage went upward into the intracranial vein (arrowhead with number 1) and downward into the perimedullary vein (arrowhead with number 2). (D) Venous phase DSA of the lateral view showing drainage into the deep jugular vein (arrowhead with number 3). (E) Selective angiography of the microcatheter via the C1 radicular artery showing that the fistula was a DAVF (asterisk), and the microcatheter was obtained in the wedge position to perform Onyx casting. (F) Postoperative DSA showing that the DAVF was obliterated completely. C1, first cervical vertebrae; CCJ, craniocervical junction; CT, computed tomography; CTA, CT angiography; DAVF, dural arteriovenous fistula; DSA, digital subtracted angiography; EVT, endovascular treatment; R, right; VA, vertebral artery.
In superselective cases of other CCJ AVFs, EVT can be attempted. For instance, in the report by Alshekhlee et al. (77), a CCJ PAVF was only fed by a thick and straight ASA, and it was successfully coiled via the ASA. Most EAVFs with intradural draining veins can be successfully treated by transarterial embolization with liquid embolic agents; therefore, EVT can be attempted in CCJ EAVFs. In addition, for CCJ EAVFs with accessible vein access, transvenous embolization can be attempted but remains challenging (84).
5.2. Open surgery
Compared to EVT, open surgery has a higher rate of obliteration and is still considered first-line management for high cervical CCJ AVFs (Figures 8, 13) (4, 5, 35, 56, 62, 66, 85, 86). For CCJ DAVFs and RAVFs with an intradural feeder, the surgical goal is to interrupt the intradural feeder and the draining vein by suboccipital craniotomy and C1 laminectomy. For CCJ DAVFs and RAVFs without an intradural feeder, the surgical goal is to interrupt the intradural draining vein (3, 56, 76). For PAVFs, the entire shunt system, including the proper feeders and drainers, was treated with coagulation (35).
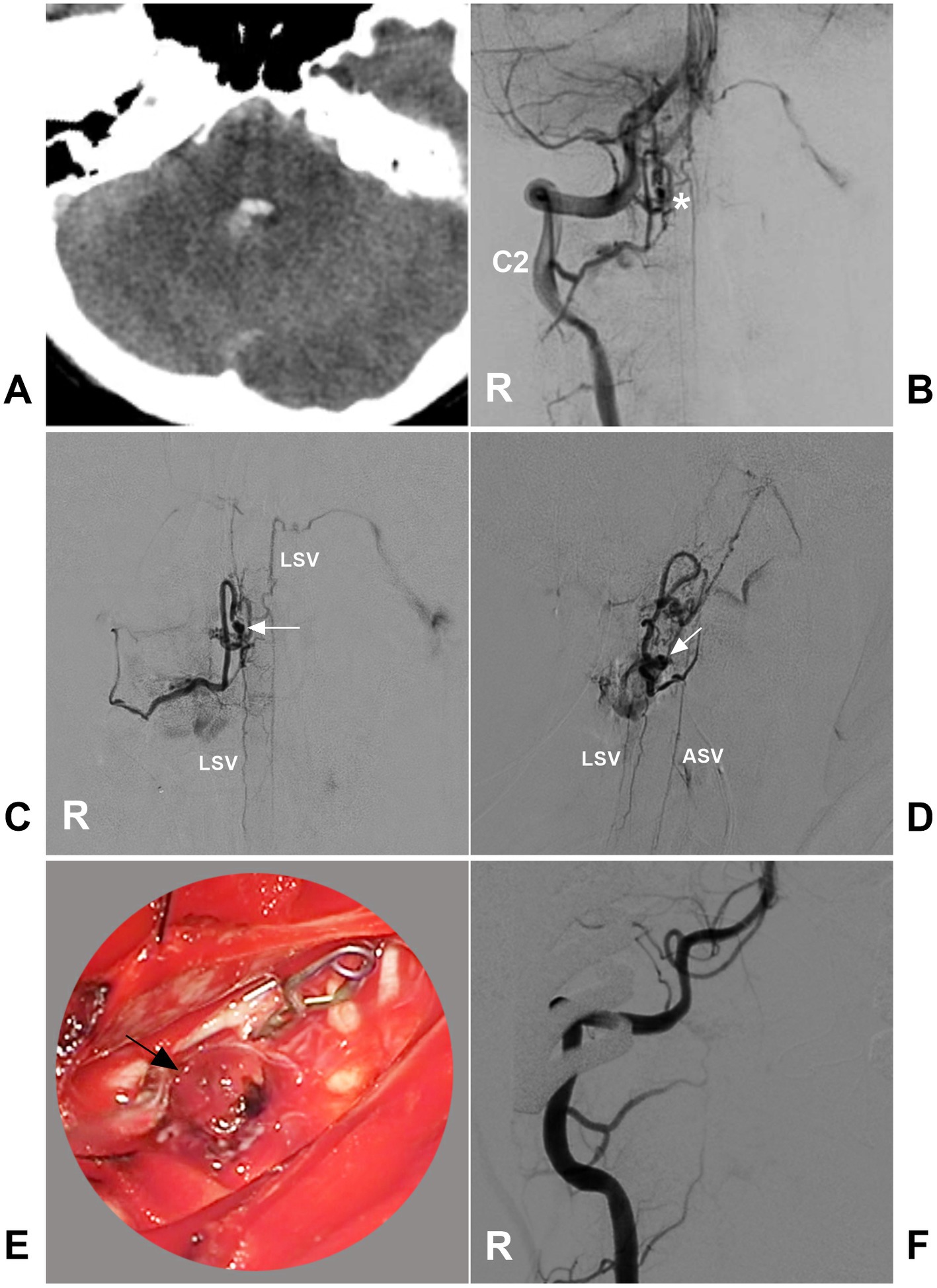
Figure 13. Open surgery in a CCJ PAVF. (A) CT showing subarachnoid hemorrhage and fourth ventricle hemorrhage. (B) Arterial phase DSA of the right VA showing a CCJ PAVF (asterisk) fed by the C2 radicular artery. (C,D) Late arterial phase DSA of the anterior posterior view (C) and lateral view (D) via a microcatheter showing the angioarchitecture of the PAVF. The feeding artery was the C2 radiculomedullary artery, there was aneurysm dilatation (arrows) in the fistula, and the draining veins included the upward and downward ASV and LSV. (E) Intraoperative image showing aneurysm dilatation (arrow) on the dorsal surface of the spinal cord, and the feeding artery was clipped. (F) Postoperative DSA showing that the PAVF was obliterated. ASV, anterior spinal vein; C2, second cervical vertebra; CCJ, craniocervical junction; CT, computed tomography; DSA, digital subtracted angiography; LSV, lateral spinal vein; PAVF, perimedullary arteriovenous fistula; R, right; VA, vertebral artery.
During surgery for CCJ AVFs, it is crucial to distinguish the fistula, feeding arteries, draining vein, normal spinal artery, and normal spinal vein (35). Because it cannot reveal the location of an AVF in the operative field, microsurgery should be performed in a hybrid operating room with the assistance of intraoperative DSA; indocyanine green videoangiography is the minimum necessary requirement (34, 35, 56, 87). Using intraoperative DSA, the minimally invasive technique offers more precise but less destructive access than conventional far lateral suboccipital craniotomy (88). In addition, the fusion of rotation myelography and computed tomography is helpful to find the excised fistula structure (34, 72, 89). The assistance of the endoscope enables observation of the angioarchitecture of the AVF (62).
6. Prognosis and compilation
6.1. Prognosis
Good outcomes are defined by a modified Rankin scale (mRS) score of 0–2. In general, open surgery for high cervical CCJ AVFs can achieve good outcomes in more than 90% of cases (Table 1) (3, 4, 35, 36, 53, 90). In reports with large case series with more EVT attempts, the complete obliteration of CCJ AVF was low, and the prognosis of patients was poor, such as in the reports by Song et al. (7), Takai et al. (9), and Hiramatsu et al. (33) (Table 1). Good outcomes in EVT of CCJ AVFs are usually detailed in case reports, however, which do not accurately represent the universality of the effect of EVT in CCJ AVFs (61, 66, 77). In addition, EVT for CCJ AVFs has been associated with a higher incidence of recurrence (9, 34).
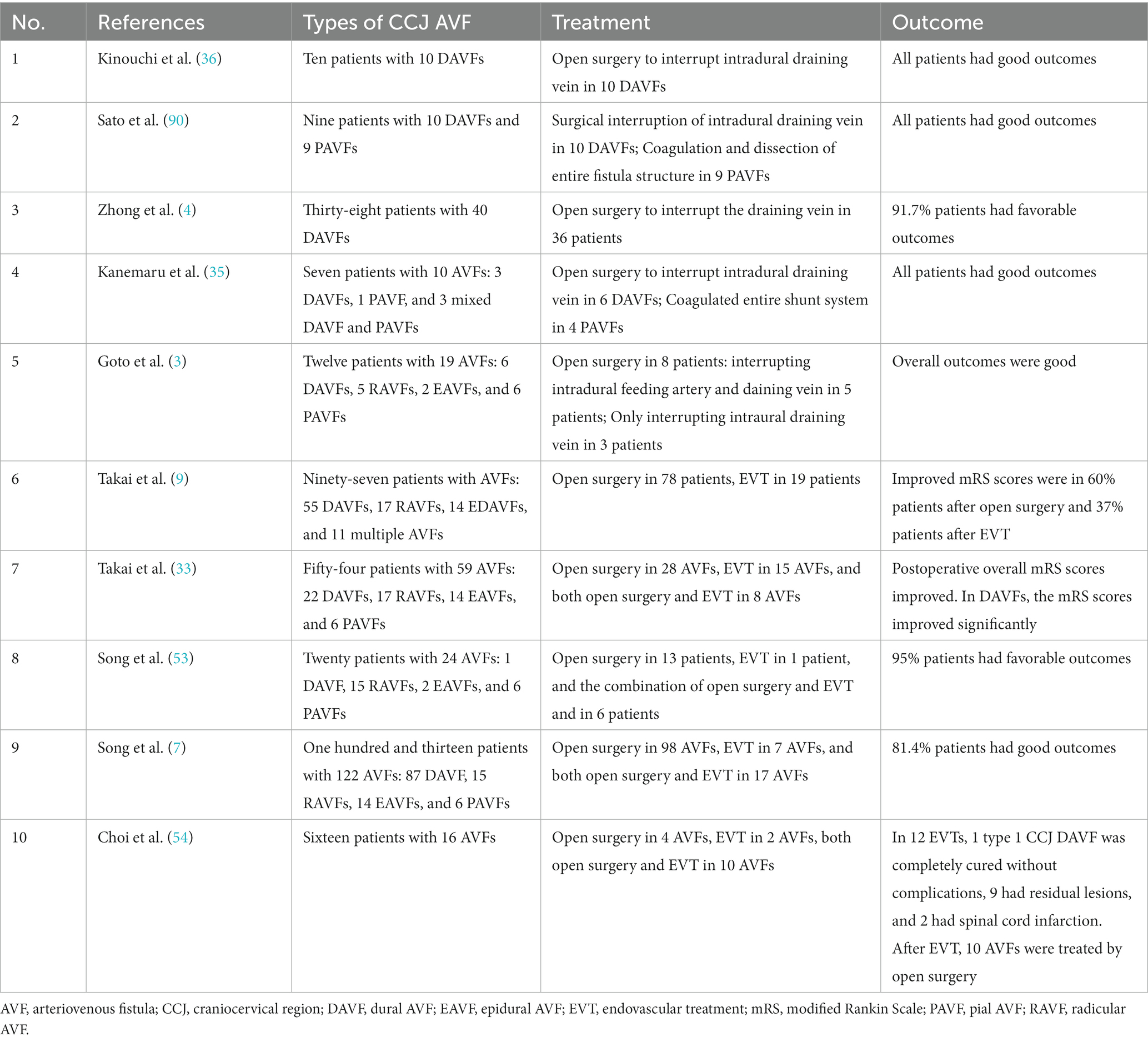
Table 1. Therapeutic outcomes of high cervical CCJ AVFs.
Except for successful obliteration of CCJ AVFs by either open surgery or EVT, many factors can affect the prognosis of high cervical CCJ AVFs. In general, patients who present with hemorrhage may have better outcomes than those who present with venous congestion. Of these high cervical CCJ AVFs, DAVFs tend to present with venous congestion, and intradural RAVFs and PAVFs tend to present with hemorrhage; therefore, CCJ intradural and extradural AVF cases tend to have better outcomes than DAVF cases. In addition, younger age is predictive of a favorable outcome (10, 91). Certainly, prompt diagnosis also offers a greater chance of immediate obliteration and may optimize the outcomes (80).
6.2. Complication
For high cervical CCJ AVFs, complications were always accompanied by open surgery or EVT, including ischemic and hemorrhagic complications, hydrocephalus, and cerebrospinal fluid leakage (4, 7, 37, 92). In open surgery, the rate of complications is approximately 20%, especially in patients with massive hemorrhage or complex CCJ AVFs (4, 7, 8, 13, 93). When performing open surgery, a complete understanding of the angioarchitecture of CCJ AVFs was required to avoid injury to normal nerves and vessels.
Compared with open surgery, EVT has a higher rate of complications (Table 1). In the report by Takai et al. (9), the overall complication rates were 42% in the EVT group, and the ischemic complication rate for the EVT group was 26% for spinal and brainstem infarctions, which was more than threefold higher than that for the open surgery group. Therefore, EVT should be only cautiously performed in certain cases (35).
Given the risk of serious complications associated with the treatment of CCJ AVF, Inoue et al. (94) suggested that prophylactic intervention should be carefully considered in asymptomatic CCJ AVF. In addition, in their report, no case of asymptomatic CCJ AVF became symptomatic during the follow-up observation (94).
7. Summary
Rarely, AVFs occur in the CCJ region. Currently, it is accepted that CCJ AVFs should only be used to refer to AVFs at the C1-C2 levels. It is reasonable that the term ‘high cervical CCJ AVFs’ is more appropriate to use when discussing CCJ AVFs. High cervical CCJ AVFs can be divided into DAVFs, RAVFs, EAVFs and PAVFs. These four types of CCJ AVFs share similar clinical and imaging characteristics. When they become symptomatic, treatment is necessary. Most high cervical CCJ AVFs can be effectively treated with open surgery. EVT should only be used in certain AVFs with simple angioarchitecture. After appropriate treatment, a good prognosis can be obtained.
Author contributions
JY contributed to the conception and design of the review. HS collection of data. JY and HS contributed to drafting the text and preparing the figures. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Offiah, CE. Craniocervical junction and cervical spine anatomy. Neuroimaging Clin N Am. (2022) 32:875–88. doi: 10.1016/j.nic.2022.07.012
2. Iampreechakul, P, Wangtanaphat, K, Wattanasen, Y, Hangsapruek, S, Lertbutsayanukul, P, and Siriwimonmas, S. Dural arteriovenous fistula of the craniocervical junction along the first cervical nerve: a single-center experience and review of the literature. Clin Neurol Neurosurg. (2022) 224:107548. doi: 10.1016/j.clineuro.2022.107548
3. Goto, Y, Hino, A, Shigeomi, Y, and Oka, H. Surgical Management for Craniocervical Junction Arteriovenous Fistula Targeting the Intradural feeder. World Neurosurg. (2020) 144:e685–92. doi: 10.1016/j.wneu.2020.09.041
4. Zhong, W, Zhang, J, Shen, J, Su, W, Wang, D, Zhang, P, et al. Dural arteriovenous fistulas at the Craniocervical junction: a series case report. World Neurosurg. (2019) 122:e700–12. doi: 10.1016/j.wneu.2018.10.124
5. Mansour, A, Endo, T, Inoue, T, Sato, K, Endo, H, Fujimura, M, et al. Clipping of an anterior spinal artery aneurysm using an endoscopic fluorescence imaging system for craniocervical junction epidural arteriovenous fistula: technical note. J Neurosurg Spine. (2019) 31:279–84. doi: 10.3171/2019.1.SPINE18983
6. Padmanaban, V, and Simon, SD. Commentary: microsurgical obliteration of Craniocervical junction Dural arteriovenous fistulas: multicenter experience. Neurosurgery. (2023) 92:e7–8. doi: 10.1227/neu.0000000000002201
7. Song, Z, Ma, Y, Wang, Y, He, C, Li, G, Zhang, P, et al. Arteriovenous fistulas in the craniocervical junction region: with vs. without spinal arterial feeders. Front. Surg. (2022) 9:1076549. doi: 10.3389/fsurg.2022.1076549
8. Wang, Y, Ma, Y, Song, Z, Yang, C, Tu, T, Yang, K, et al. Clinical and prognostic features of venous hypertensive myelopathy from craniocervical arteriovenous fistulas: a retrospective cohort study. J Neurosurg. (2023) 1-11:1–11. doi: 10.3171/2022.11.JNS221958
9. Takai, K, Endo, T, Seki, T, Inoue, T, Koyanagi, I, and Mitsuhara, T. Neurosurgical versus endovascular treatment of craniocervical junction arteriovenous fistulas: a multicenter cohort study of 97 patients. J Neurosurg. (2021) 137:373–80. doi: 10.3171/2021.10.JNS212205
10. Takai, K, Endo, T, Seki, T, and Inoue, T. Congestive myelopathy due to craniocervical junction arteriovenous fistulas mimicking transverse myelitis: a multicenter study on 27 cases. J Neurol. (2022) 270:1745–53. doi: 10.1007/s00415-022-11536-7
11. Offiah, CE, and Day, E. The craniocervical junction: embryology, anatomy, biomechanics and imaging in blunt trauma. Insights Imaging. (2017) 8:29–47. doi: 10.1007/s13244-016-0530-5
12. Vigo, V, Hirpara, A, Yassin, M, Wang, M, Chou, D, De Bonis, P, et al. Immersive surgical anatomy of the Craniocervical junction. Cureus. (2020) 12:e10364. doi: 10.7759/cureus.10364
13. de Oliveira, E, Rhoton, AL Jr, and Peace, D. Microsurgical anatomy of the region of the foramen magnum. Surg Neurol. (1985) 24:293–352. doi: 10.1016/0090-3019(85)90042-4
14. Matsushima, T, Rhoton, AL Jr, de Oliveira, E, and Peace, D. Microsurgical anatomy of the veins of the posterior fossa. J Neurosurg. (1983) 59:63–105. doi: 10.3171/jns.1983.59.1.0063
15. Wang, XC, Du, YY, Tan, Y, Qin, JB, Wang, L, Wu, XF, et al. Brainstem congestion due to Dural arteriovenous fistula at the Craniocervical junction: case report and review of the literature. World Neurosurg. (2018) 118:181–7. doi: 10.1016/j.wneu.2018.06.243
16. Do, AS, Kapurch, J, Kumar, R, Port, J, Miller, JW, and Van Gompel, JJ. The long and winding road: thoracic myelopathy associated with Occipitocervical Dural arteriovenous fistula. World Neurosurg. (2017) 108:998.e7-.e16. doi: 10.1016/j.wneu.2017.09.073
17. Mascalchi, M, Scazzeri, F, Prosetti, D, Ferrito, G, Salvi, F, and Quilici, N. Dural arteriovenous fistula at the craniocervical junction with perimedullary venous drainage. AJNR Am J Neuroradiol. (1996) 17:1137–41.
18. Li, C, Yu, J, Li, K, Hou, K, and Yu, J. Dural arteriovenous fistula of the lateral foramen magnum region: a review. Interv Neuroradiol. (2018) 24:425–34. doi: 10.1177/1591019918770768
19. Kiyosue, H, Okahara, M, Sagara, Y, Tanoue, S, Ueda, S, Mimata, C, et al. Dural arteriovenous fistula involving the posterior condylar canal. AJNR Am J Neuroradiol. (2007) 28:1599–601. doi: 10.3174/ajnr.A0606
20. Hellstern, V, Aguilar-Pérez, M, Schob, S, Bhogal, P, AlMatter, M, Kurucz, P, et al. Endovascular treatment of Dural arteriovenous fistulas of the anterior or posterior condylar vein: a cadaveric and clinical study and literature review. Clin Neuroradiol. (2019) 29:341–9. doi: 10.1007/s00062-018-0669-1
21. Mizutani, K, Akiyama, T, Minami, Y, Toda, M, Fujiwara, H, Jinzaki, M, et al. Intraosseous venous structures adjacent to the jugular tubercle associated with an anterior condylar dural arteriovenous fistula. Neuroradiology. (2018) 60:487–96. doi: 10.1007/s00234-018-1990-8
22. Maus, V, Söderman, M, Rodesch, G, Kabbasch, C, and Mpotsaris, A. Endovascular treatment of posterior condylar canal dural arteriovenous fistula. J Neurointerv Surg. (2017) 9:e7. doi: 10.1136/neurintsurg-2016-012384.rep
23. Padhi, R, Kandasamy, S, Kumaran, B, Kocer, N, and Karmadhari, H. Direct superior ophthalmic vein approach to treat anterior condylar confluence Dural arteriovenous fistula. Neurointervention. (2021) 16:280–4. doi: 10.5469/neuroint.2021.00367
24. Caton, MT, Narsinh, KH, Baker, A, Dowd, CF, Higashida, RT, Cooke, DL, et al. Dural arteriovenous fistulas of the foramen magnum region: clinical features and Angioarchitectural phenotypes. AJNR Am J Neuroradiol. (2021) 42:1486–91. doi: 10.3174/ajnr.A7152
25. Byun, JS, Hwang, SN, Park, SW, and Nam, TK. Dural arteriovenous fistula of jugular foramen with subarachnoid hemorrhage: selective transarterial embolization. J Korean Neurosurg Soc. (2009) 45:199–202. doi: 10.3340/jkns.2009.45.3.199
26. Peto, I, Abou-Al-Shaar, H, and Dehdashti, AR. Right jugular foramen dural arteriovenous fistula Cognard IV. Neurosurg Focus. (2019) 46:V7. doi: 10.3171/2019.2.FocusVid.18667
27. Takahashi, H, Ueshima, T, Goto, D, Kimura, T, Yuki, N, Inoue, Y, et al. Acute Tetraparesis with respiratory failure after steroid Administration in a Patient with a Dural arteriovenous fistula at the Craniocervical junction. Intern Med. (2018) 57:591–4. doi: 10.2169/internalmedicine.9115-17
28. Chen, PY, Juan, YH, and Lin, SK. An isolated unilateral Pontomedullary lesion due to an intracranial Dural arteriovenous fistula mimicking a brain tumor-case and review. J Nippon Med School. (2019) 86:48–54. doi: 10.1272/jnms.JNMS.2019_86-9
29. Sun, HS, Yun, HS, Song, MK, Han, JY, Choi, IS, and Lee, SG. Dural arteriovenous fistula on the brain stem and upper cervical spinal cord - a case report. Ann Rehabil Med. (2011) 35:733–7. doi: 10.5535/arm.2011.35.5.733
30. Yoo, DH, Cho, YD, Boonchai, T, Kim, KM, Kim, JE, Cho, WS, et al. Endovascular treatment of medullary bridging vein-draining dural arteriovenous fistulas: foramen magnum vs. craniocervical junction lesions. Neuroradiology. (2022) 64:333–42. doi: 10.1007/s00234-021-02790-z
31. Kikkawa, Y, Nakamizo, A, Yamashita, K, Amano, T, Kurogi, A, and Sasaki, T. Preoperative evaluation and surgical strategies for craniocervical junction dural arteriovenous fistula with multiple feeders: case report and review of the literature. Fukuoka Igaku Zasshi. (2013) 104:299–308. doi: 10.15017/1397858
32. Matsubara, S, Toi, H, Takai, H, Miyazaki, Y, Kinoshita, K, Sunada, Y, et al. Variations and management for patients with craniocervical junction arteriovenous fistulas: comparison of dural, radicular, and epidural arteriovenous fistulas. Surg Neurol Int. (2021) 12:411. doi: 10.25259/SNI_557_2021
33. Hiramatsu, M, Sugiu, K, Ishiguro, T, Kiyosue, H, Sato, K, Takai, K, et al. Angioarchitecture of arteriovenous fistulas at the craniocervical junction: a multicenter cohort study of 54 patients. J Neurosurg. (2018) 128:1839–49. doi: 10.3171/2017.3.JNS163048
34. Fujimoto, S, Takai, K, Nakatomi, H, Kin, T, and Saito, N. Three-dimensional angioarchitecture and microsurgical treatment of arteriovenous fistulas at the craniocervical junction. J Clin Neurosci. (2018) 53:140–6. doi: 10.1016/j.jocn.2018.04.065
35. Kanemaru, K, Yoshioka, H, Hashimoto, K, Murayama, H, Ogiwara, M, Yagi, T, et al. Efficacy of Intraarterial fluorescence video angiography in surgery for Dural and Perimedullary arteriovenous fistula at Craniocervical junction. World Neurosurg. (2019) 126:e573–9. doi: 10.1016/j.wneu.2019.02.097
36. Kinouchi, H, Mizoi, K, Takahashi, A, Nagamine, Y, Koshu, K, and Yoshimoto, T. Dural arteriovenous shunts at the craniocervical junction. J Neurosurg. (1998) 89:755–61. doi: 10.3171/jns.1998.89.5.0755
37. Takai, K, Endo, T, Seki, T, Inoue, T, Koyanagi, I, and Mitsuhara, T. Ischemic complications in the neurosurgical and endovascular treatments of craniocervical junction arteriovenous fistulas: a multicenter study. J Neurosurg. (2022) 137:1776–85. doi: 10.3171/2022.3.JNS22341
38. Abd el-Bary, TH, Dujovny, M, and Ausman, JI. Microsurgical anatomy of the atlantal part of the vertebral artery. Surg Neurol. (1995) 44:392–400; discussion-1–401. doi: 10.1016/0090-3019(95)00033-X
39. Ulm, AJ, Quiroga, M, Russo, A, Russo, VM, Graziano, F, Velasquez, A, et al. Normal anatomical variations of the V₃ segment of the vertebral artery: surgical implications. J Neurosurg Spine. (2010) 13:451–60. doi: 10.3171/2010.4.SPINE09824
40. Castillo, C, Viñas, FC, Gutikhonda, M, and Diaz, FG. Microsurgical anatomy of the suboccipital segment of the vertebral artery. Neurol Res. (1998) 20:201–8. doi: 10.1080/01616412.1998.11740507
41. Martins, C, Yasuda, A, Campero, A, Ulm, AJ, Tanriover, N, and Rhoton, A Jr. Microsurgical anatomy of the dural arteries. Neurosurgery. (2005) 56:211–251; discussion: 211–251. doi: 10.1227/01.NEU.0000144823.94402.3D
42. Lasjaunias, P, Berenstein, A, and ter Brugge, KG. Craniocervical junction. Clinical vascular anatomy and variations. Berlin, Heidelberg: Springer Berlin Heidelberg (2001). p. 165–260.
43. Rovira, M, Torrent, O, González, F, and Romero, F. Contribution to the study of the arterial nutrition of the cervical spinal cord. Neuroradiology. (1978) 16:375–7. doi: 10.1007/BF00395309
44. Zhao, J, Xu, F, Ren, J, Manjila, S, and Bambakidis, NC. Dural arteriovenous fistulas at the craniocervical junction: a systematic review. J Neurointerv Surg. (2016) 8:648–53. doi: 10.1136/neurintsurg-2015-011775
45. Gutierrez, S, Huynh, T, Iwanaga, J, Dumont, AS, Bui, CJ, and Tubbs, RS. A review of the history, anatomy, and development of the C1 spinal nerve. World Neurosurg. (2020) 135:352–6. doi: 10.1016/j.wneu.2019.12.024
46. Wen, HT, Rhoton, AL Jr, Katsuta, T, and de Oliveira, E. Microsurgical anatomy of the transcondylar, supracondylar, and paracondylar extensions of the far-lateral approach. J Neurosurg. (1997) 87:555–85. doi: 10.3171/jns.1997.87.4.0555
47. Zhang, K, Li, C, Hou, K, and Yu, J. Role of the cervical anterior spinal artery in the endovascular treatment of vascular diseases: bystander, accomplice, victim, or friend? Front Neurol. (2021) 12:761006. doi: 10.3389/fneur.2021.761006
48. Lasjaunias, P, Vallee, B, Person, H, Ter Brugge, K, and Chiu, M. The lateral spinal artery of the upper cervical spinal cord. Anatomy, normal variations, and angiographic aspects. J Neurosurg. (1985) 63:235–41. doi: 10.3171/jns.1985.63.2.0235
49. Matsushima, K, Funaki, T, Komune, N, Kiyosue, H, Kawashima, M, and Rhoton, AL Jr. Microsurgical anatomy of the lateral condylar vein and its clinical significance. Neurosurgery. (2015) 11:135–145. discussion: 45–46. doi: 10.1227/NEU.0000000000000570
50. Yamada, H, Mizutani, K, Akiyama, T, and Toda, M. Extracranial prevertebral venous network of the craniocervical junction: CT-digital subtraction venography analysis. Neuroradiology. (2022) 64:2227–33. doi: 10.1007/s00234-022-02980-3
51. Braun, JP, and Tournade, A. Venous drainage in the craniocervical region. Neuroradiology. (1977) 13:155–8. doi: 10.1007/BF00626278
52. Arnautović, KI. al-Mefty O, Pait TG, Krisht AF, Husain MM. The suboccipital cavernous sinus. J Neurosurg. (1997) 86:252–62. doi: 10.3171/jns.1997.86.2.0252
53. Song, Z, Ma, Y, Hong, T, and Zhang, H. Arteriovenous fistulas fed by spinal arterial feeders at the Craniocervical junction region. Oper Neurosurg (Hagerstown). (2022) 23:472–81. doi: 10.1227/ons.0000000000000390
54. Choi, JH, Park, JC, Ahn, JS, and Park, W. Treatment of dural arteriovenous fistula with intradural draining vein at the craniocervical junction: case series with special reference to the anatomical considerations. World Neurosurg. (2023). doi: 10.1016/j.wneu.2023.04.103
55. Kim, DJ, Willinsky, R, Geibprasert, S, Krings, T, Wallace, C, Gentili, F, et al. Angiographic characteristics and treatment of cervical spinal dural arteriovenous shunts. AJNR Am J Neuroradiol. (2010) 31:1512–5. doi: 10.3174/ajnr.A2109
56. Shimada, K, Yamaguchi, I, Miyamoto, T, Sogabe, S, Miyake, K, Kanematsu, Y, et al. Efficacy of intraarterial indocyanine green videoangiography in surgery for arteriovenous fistula at the craniocervical junction in a hybrid operating room: illustrative cases. J Neurosurg Case Less. (2022) 3:Case 22100. doi: 10.3171/CASE22100
57. Oshita, J, Yamaguchi, S, Ohba, S, and Kurisu, K. Mirror-image spinal dural arteriovenous fistulas at the craniocervical junction: case report and review of the literature. Neurosurgery. (2011) 69:E1166–71. doi: 10.1227/NEU.0b013e318223bab5
58. Sato, H, Wada, H, Noro, S, Saga, T, and Kamada, K. Subarachnoid hemorrhage with concurrent Dural and Perimedullary arteriovenous fistulas at Craniocervical junction: case report and literature review. World Neurosurg. (2019) 127:331–4. doi: 10.1016/j.wneu.2019.02.079
59. Hiramatsu, M, Sugiu, K, Yasuhara, T, Hishikawa, T, Haruma, J, Nishi, K, et al. Angioarchitecture of the Normal lateral spinal artery and Craniocervical junction arteriovenous fistula using contrast-enhanced cone-beam CT. Clin Neuroradiol. (2022) 33:375–82. doi: 10.1007/s00062-022-01218-2
60. Jeon, JP, Cho, YD, Kim, CH, and Han, MH. Complex spinal arteriovenous fistula of the craniocervical junction with pial and dural shunts combined with contralateral dural arteriovenous fistula. Interv Neuroradiol. (2015) 21:733–7. doi: 10.1177/1591019915609128
61. Lang, MJ, Atallah, E, Tjoumakaris, S, Rosenwasser, RH, and Jabbour, P. Remote thoracic myelopathy from a spinal Dural arteriovenous fistula at the Craniocervical junction. Case Report and Rev Literature World Neurosurg. (2017) 108:992.e1–4. doi: 10.1016/j.wneu.2017.08.158
62. Horiuchi, R, Kanemaru, K, Yoshioka, H, Hashimoto, K, Murayama, H, Yagi, T, et al. Endoscope-integrated fluorescence video angiography for the surgery of ventrally located Perimedullary arteriovenous fistula at Craniocervical junction. World Neurosurg. (2020) 137:126–9. doi: 10.1016/j.wneu.2020.01.207
63. Gadot, R, Gopakumar, S, Wagner, K, Xu, DS, Raper, DMS, Burkhardt, JK, et al. Foramen magnum Dural arteriovenous fistula presenting with thoracic myelopathy: technical case report with 2-dimensional operative video. Oper Neurosurg (Hagerstown). (2021) 21:E55–9. doi: 10.1093/ons/opab077
64. Sato, K, Morofuji, Y, Sadakata, E, Horie, N, Izumo, T, Anda, T, et al. A case of Dural arteriovenous fistula at the Craniocervical junction with high signal intensity localized to the thoracic spinal cord on T2-weighted MRI. No Shinkei Geka. (2020) 48:245–51. doi: 10.11477/mf.1436204170
65. Aviv, RI, Shad, A, Tomlinson, G, Niemann, D, Teddy, PJ, Molyneux, AJ, et al. Cervical dural arteriovenous fistulae manifesting as subarachnoid hemorrhage: report of two cases and literature review. AJNR Am J Neuroradiol. (2004) 25:854–8.
66. Murase, S, Fukumura, M, Kuroda, Y, Gon, Y, and Nakazawa, K. Abnormal flow void signs and gadolinium enhancement of vascular lesions for the early diagnosis of angiographically occult dural arteriovenous fistulas at the craniocervical junction: a case report. Interdiscip Neurosurg. (2022) 27:101399. doi: 10.1016/j.inat.2021.101399
67. Song, Z, Ma, Y, Wang, Y, and Zhang, H. Venous hypertensive myelopathy from Craniocervical junction arteriovenous fistulas: rare but not negligible. World Neurosurg. (2023) 173:270–1. doi: 10.1016/j.wneu.2023.02.123
68. Tezuka, T, Nukariya, T, Katsumata, M, Miyauchi, T, Tokuyasu, D, Azami, S, et al. "missing-piece" sign with dural arteriovenous fistula at craniocervical junction: a case report. J Stroke Cerebrovasc Dis. (2023) 32:107152. doi: 10.1016/j.jstrokecerebrovasdis.2023.107152
69. Zalewski, NL, Rabinstein, AA, Brinjikji, W, Kaufmann, TJ, Nasr, D, Ruff, MW, et al. Unique gadolinium enhancement pattern in spinal Dural arteriovenous fistulas. JAMA Neurol. (2018) 75:1542–5. doi: 10.1001/jamaneurol.2018.2605
70. Ishibashi, R, Maki, Y, Ikeda, H, and Chin, M. Intraoperative identification of the lateral spinal artery in a case of craniocervical junction dural arteriovenous fistula surgically obliterated. Neuroradiol J. (2022) 36:351–6. doi: 10.1177/19714009221132950
71. Hashiguchi, A, Mimata, C, Ichimura, H, and Kuratsu, J. Occipital neuralgia as a presenting symptom of cervicomedullary dural arteriovenous fistula. Headache. (2007) 47:1095–7. doi: 10.1111/j.1526-4610.2007.00865.x
72. Takai, K, Komori, T, Kurita, H, Kawai, K, Inoue, T, and Taniguchi, M. Intradural radicular arteriovenous fistula that mimics dural arteriovenous fistula: report of three cases. Neuroradiology. (2019) 61:1203–8. doi: 10.1007/s00234-019-02275-0
73. Wada, K, Tanei, T, Hattori, K, Hatano, H, Fujitani, S, Ito, R, et al. Unique vascular structures of a radicular arteriovenous fistula at the craniocervical junction along the first cervical spinal nerve: a case report. Surg Neurol Int. (2023) 14:85. doi: 10.25259/SNI_122_2023
74. Shetty, GS, Singh, V, Prasad, SN, Phadke, RV, Neyaz, Z, Udiya, A, et al. Spinal epidural fistulas-a separate entity to Dural fistulas with different Angioarchitecture and treatment approach. World Neurosurg. (2021) 149:e600–11. doi: 10.1016/j.wneu.2021.01.126
75. Rangel-Castilla, L, Holman, PJ, Krishna, C, Trask, TW, Klucznik, RP, and Diaz, OM. Spinal extradural arteriovenous fistulas: a clinical and radiological description of different types and their novel treatment with Onyx. J Neurosurg Spine. (2011) 15:541–9. doi: 10.3171/2011.6.SPINE10695
76. Nakagawa, I, Park, HS, Hironaka, Y, Wada, T, Kichikawa, K, and Nakase, H. Cervical spinal epidural arteriovenous fistula with coexisting spinal anterior spinal artery aneurysm presenting as subarachnoid hemorrhage—case report. J Stroke Cerebrovasc Dis. (2014) 23:e461–5. doi: 10.1016/j.jstrokecerebrovasdis.2014.07.012
77. Alshekhlee, A, Edgell, RC, Kale, SP, Kitchener, J, and Vora, N. Endovascular therapy of a craniocervical pial AVF fed by the anterior spinal artery. J Neuroimaging. (2013) 23:102–4. doi: 10.1111/j.1552-6569.2010.00569.x
78. Ogawa, A, Furuya, K, Ueno, T, Naito, Y, and Nakagomi, T. Characteristics and treatment of dural and perimedullary arteriovenous fistula at the craniocervical junction presenting with subarachnoid hemorrhage. No Shinkei Geka. (2012) 40:121–8. doi: 10.11477/mf.1436101644
79. Liu, X, Ogata, A, Masuoka, J, Inoue, K, Nakahara, Y, Shimokawa, S, et al. Dural arteriovenous fistula manifesting as pontine hemorrhage at the craniocervical junction. Acta Neurochir. (2017) 159:831–4. doi: 10.1007/s00701-017-3135-y
80. Wang, JY, Molenda, J, Bydon, A, Colby, GP, Coon, AL, Tamargo, RJ, et al. Natural history and treatment of craniocervical junction dural arteriovenous fistulas. J Clin Neurosci. (2015) 22:1701–7. doi: 10.1016/j.jocn.2015.05.014
81. Salamon, E, Patsalides, A, Gobin, YP, Santillan, A, and Fink, ME. Dural arteriovenous fistula at the craniocervical junction mimicking acute brainstem and spinal cord infarction. JAMA Neurol. (2013) 70:796–7. doi: 10.1001/jamaneurol.2013.1946
82. Sorenson, TJ, De Maria, L, Rangel-Castilla, L, and Lanzino, G. Surgical treatment of previously embolized craniocervical junction dural arteriovenous fistula. Neurosurg Focus. (2019) 46:V2. doi: 10.3171/2019.2.FocusVid.18639
83. Salem, MM, Srinivasan, VM, Tonetti, DA, Ravindran, K, Taussky, P, Yang, K, et al. Microsurgical obliteration of Craniocervical junction Dural arteriovenous fistulas: multicenter experience. Neurosurgery. (2023) 92:205–12. doi: 10.1227/neu.0000000000002196
84. Yoshida, K, Sato, S, Inoue, T, Ryu, B, Shima, S, Mochizuki, T, et al. Transvenous embolization for craniocervical junction epidural arteriovenous fistula with a pial feeder aneurysm. Interv Neuroradiol. (2020) 26:170–7. doi: 10.1177/1591019919874571
85. Oishi, H, Okuda, O, Arai, H, Maehara, T, and Iizuka, Y. Successful surgical treatment of a dural arteriovenous fistula at the craniocervical junction with reference to pre-and postoperative MRI. Neuroradiology. (1999) 41:463–7. doi: 10.1007/s002340050785
86. Sorenson, TJ, La Pira, B, Hughes, J, and Lanzino, G. How I do it: surgical ligation of craniocervical junction dural AV fistulas. Acta Neurochir. (2017) 159:1489–92. doi: 10.1007/s00701-017-3200-6
87. Sun, L, Ren, J, and Zhang, H. Application of the selective indocyanine green videoangiography in microsurgical treatment of a craniocervical junction dural arteriovenous fistula. Neurosurg Focus. (2019) 46:V5. doi: 10.3171/2019.2.FocusVid.18681
88. Li, CR, Shen, CC, Tsuei, YS, Chen, WH, and Lee, CH. Intraoperative DSA-guided minimal approach for craniocervical junction DAVFs obliteration. Acta Neurochir. (2023) 165:1557–64. doi: 10.1007/s00701-023-05585-8
89. Hayashi, N, Tomura, N, Okada, H, Sasaki, T, Tsuji, E, Enomoto, H, et al. Usefulness of preoperative cone beam computed tomography and intraoperative digital subtraction angiography for dural arteriovenous fistula at craniocervical junction: technical case report. Surg Neurol Int. (2019) 10:5. doi: 10.4103/sni.sni_439_17
90. Sato, K, Endo, T, Niizuma, K, Fujimura, M, Inoue, T, Shimizu, H, et al. Concurrent dural and perimedullary arteriovenous fistulas at the craniocervical junction: case series with special reference to angioarchitecture. J Neurosurg. (2013) 118:451–9. doi: 10.3171/2012.10.JNS121028
91. Chen, G, Wang, Q, Tian, Y, Gu, Y, Xu, B, Leng, B, et al. Dural arteriovenous fistulae at the craniocervical junction: the relation between clinical symptom and pattern of venous drainage. Acta Neurochir Suppl. (2011) 110:99–104. doi: 10.1007/978-3-7091-0356-2_18
92. Takai, K, Kin, T, Oyama, H, Shojima, M, and Saito, N. Three-dimensional angioarchitecture of spinal dural arteriovenous fistulas, with special reference to the intradural retrograde venous drainage system. J Neurosurg Spine. (2013) 18:398–408. doi: 10.3171/2013.1.SPINE12305
93. Miyamoto, N, Naito, I, Takatama, S, Iwai, T, and Tomizawa, S. A case of craniocervical junction pial arteriovenous fistula causing postoperative medullary and spinal cord edema. J Stroke Cerebrovasc Dis. (2023) 32:106852. doi: 10.1016/j.jstrokecerebrovasdis.2022.106852
Keywords: craniocervical junction, high cervical cord, arteriovenous fistula, treatment, review
Citation: Su H and Yu J (2023) Treatment of high cervical arteriovenous fistulas in the craniocervical junction region. Front. Neurol. 14:1164548. doi: 10.3389/fneur.2023.1164548
Edited by:
Osama O. Zaidat, Northeast Ohio Medical University, United StatesCopyright © 2023 Su and Yu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jinlu Yu, amx5dUBqbHUuZWR1LmNu; amlubHV5dUBob3RtYWlsLmNvbQ==
†ORCID: Jinlu Yu, https://orcid.org/0000-0003-2329-7946