
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Neurol. , 02 June 2023
Sec. Neurological Biomarkers
Volume 14 - 2023 | https://doi.org/10.3389/fneur.2023.1153690
This article is part of the Research Topic Biomarkers in Neurology, Volume II View all 16 articles
 Miguel Cabanillas-Lazo1,2,3
Miguel Cabanillas-Lazo1,2,3 Carlos Quispe-Vicuña1,2,3
Carlos Quispe-Vicuña1,2,3 Claudia Cruzalegui-Bazán1,2,3
Claudia Cruzalegui-Bazán1,2,3 Milagros Pascual-Guevara1,2,3
Milagros Pascual-Guevara1,2,3 Nicanor Mori-Quispe4Carlos Alva-Diaz1,4,5*
Nicanor Mori-Quispe4Carlos Alva-Diaz1,4,5*Background and objectives: Guillain-Barre syndrome (GBS) is an immune-mediated neuropathy. This has raised the possibility that the neutrophil-lymphocyte ratio (NLR) may be a biomarker of its activity. We conducted a systematic review and meta-analysis to summarize the evidence of NLR as a potential biomarker for GBS.
Methods: We systematically searched databases (PubMed, Ovid-Medline, Embase, Scopus, Web of Science, SciELO Citation Index, LILACS, and Google Scholar) until October 2021 for studies evaluating pre-treatment NLR values in GBS patients. A meta-analysis using a random-effects model to estimate pooled effects was realized for each outcome and a narrative synthesis when this was not possible. Subgroup and sensitivity analysis were realized. GRADE criteria were used to identify the certainty of evidence for each result.
Results: Ten studies from 745 originally included were selected. Regarding GBS patients versus healthy controls, a meta-analysis of six studies (968 patients) demonstrated a significant increase in NLR values in GBS patients (MD: 1.76; 95% CI: 1.29, 2.24; I2 = 86%) with moderate certainty due to heterogeneity of GBS diagnosis criteria used. Regarding GBS prognosis, assessed by Hughes Score ≥ 3, NLR had a sensitivity between 67.3 and 81.5 and a specificity between 67.3 and 87.5 with low certainty due to imprecision, and heterogeneity. In relation to respiratory failure, NLR had a sensitivity of 86.5 and specificity of 68.2 with high and moderate certainty, respectively.
Discussion: With moderate certainty, mean NLR is higher in GBS patients compared to healthy controls. Furthermore, we found that NLR could be a prognostic factor for disability and respiratory failure with low and moderate certainty, respectively. These results may prove useful for NLR in GBS patients; however, further research is needed.
Systematic review registration: https://www.crd.york.ac.uk/PROSPERO/, identifier: CRD42021285212.
Guillain-Barre syndrome (GBS), an immune-mediated peripheral neuropathy, is the most common cause of acute flaccid paralysis and is characterized by rapidly progressive weakness or sensory loss usually followed by slow clinical recovery (1). The annual global incidence rate is 1–2 cases per 100,000 people per year (2). The global prevalence of GBS has shown an increase of 6.4% from 1990 to 2019, reporting in the latter year, more than 150,000 cases and more than 44 000 years lived with disability (YLD) (3). Also, Asia and Central and South America are the regions with the highest frequency (30–65%) of the axonal subtype of GBS which is the most severe subtype of the disease (4). In addition, death or severe disability results in almost 20% of patients despite adequate treatment (5).
The most frequent risk factor of GBS is gastrointestinal and respiratory infection (6), which generates a cellular and humoral response by T and B cells. The latter induces an antiganglioside antibody response that crosses the blood-nerve barrier and activate the complement. Likewise, T-cell activation leads to cytokine release, Schwann cell damage and myelin destruction (7). This mechanism results in axonal degeneration of motor and sensory fibers of cranial and peripheral nerves (1). This is known as “molecular mimicry autoimmunity.”
Despite that the role of the neutrophil in GBS pathophysiology is not well understood, several investigations suggest the neutrophil-to-lymphocyte ratio (NLR) as a possible index of immune function, since the systemic inflammation generated by the disease usually results in neutrophilia and lymphocytopenia (1, 6–8).
Although the diagnosis of GBS is mainly based on a combination of clinical criteria, cerebrospinal fluid (CSF) analysis and nerve conduction studies (Brighton criteria); some criteria are not present in early stages of the disease, such as cytological albumin dissolution (after the first week) or alterations in neuroconduction studies (after the second week) (9). This has led to the search for biomarkers to establish a rapid and accurate diagnosis, using serum, peripheral nervous tissue and CSF as the main sources.
Despite all this, there is a lack of accessible and reliable biomarkers of systemic inflammation in neurology, which could provide information to differentiate or predict GBS activity (10–12). The neutrophil-to-lymphocyte ratio (NLR) is calculated from the white blood cell count and is a new biomarker used in neurological diseases such as autoimmume encephalitis and multiple sclerosis (8, 13). Even now, it's part of routine blood tests and is therefore available for research as possible alternatives. So, the importance of NLR lies of its performance, its low cost, its availability in routine examinations and its easy acceptance by physicians and patients.
NLR is more reflective of systemic inflammation compared to other leukocyte subtypes, is easier to obtain by blood test, and is stable and reliable (14). Given that the prognosis of GBS is not fully elucidated, NLR could be an accessible prognostic factor of GBS activity and severity. For those reasons, this systematic review summarizes current knowledge about the potential of NLR as a biomarker in GBS.
This systematic review was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (15). The study protocol was registered in PROSPERO with the code CRD42021285212.
We searched in PubMed, Ovid-Medline, Embase, Scopus, Web of Science, SciELO Citation Index, LILACS and Google Scholar until October 2021. The search strategy is detailed in Supplementary Table 1. There were no restrictions on language or publication date. We completed the search by reviewing the bibliographic references of the included studies and selecting the articles that met the requirements.
Studies were included if they met the following criteria: (1) Analytical observational studies (cross-sectional, case-control and cohort studies); (2) Studies included adult participants (aged > 18 years old) and (3) NLR values assessed at pre-treatment period in GBS patients. We excluded narrative and systematic reviews, studies in non-humans, case reports, conference abstracts and letters.
Results from electronic searches were exported to Endnote X9 and duplicate documents were removed. After, two reviewers (CCB and MPG) performed a peer review process using Rayyan QCRI (https://rayyan.qcri.org/) for the selection of articles according to the inclusion criteria and then reading the full text. Any discrepancies were resolved by consensus or a third author (CAD). The complete list of excluded articles is provided in Supplementary Table 2.
Our outcomes were (1) Assessment of NLR comparing GBS patients with healthy control subjects (NLR is the biochemical parameter calculated by dividing the absolute neutrophil count by the absolute lymphocyte count); and (2) Assessment of NLR comparing GBS mild and severe, which was assessed with at least one of the following from discharge: (a) Hughes's score (16) using a scale from 0 to 6 ranging from no symptoms to death, (b) Medical Research Council (MRC) scale (17) using a scale from 0 to 5 ranging from no visible contraction to active movement against full resistance, or (c) respiratory failure.
Two authors (CCB and MPG) independently carried out information using a data extraction form and any disagreements were resolved by consensus and ultimately a third author (CAD). We extracted the following information: title of the study, first author, year of publication, study design, country where the study was performed, number of participants, sex, age, sample time, criteria for diagnosis of GBS, mean or median NLR according to sample stratification, follow-up crude and adjusted association measures, type of outcome and its definition. We contacted the corresponding author through email if additional data was needed.
The quality of the studies was assessed with the Newcastle Ottawa Scale (18) by two authors (MCL and CQV) and any discrepancies were resolved by consensus. This tool evaluates the quality of published observational studies and is based on three items: selection, comparability, and outcome/exposure. Each item has sub-items, on which a star-based score was assigned. Studies with scores ≥ 6 were considered as having a low risk of bias (high quality), scores of 4–5 as having a moderate risk of bias, and scores < 4 as having a high risk of bias (19). If the studies had a double design (cases and controls, cohorts), the design was considered according to the main objective of the study.
A meta-analysis was planned for each outcome; however, when this was not possible due to unavailable data, narrative synthesis was performed. Meta-analyses were performed using the inverse variance method and the randomized effects model. The variance between studies (τ2) was estimated using the DerSimonian-Laird method. Mean differences (MD) with their 95% confidence intervals (CI 95%) were pooled if the studies had a confounder control. Heterogeneity between studies was assessed using the I2 statistic. Heterogeneity was defined as low if I2 < 30%, moderate if I2 = 30–60%, and high if I2 > 60%. The metacont function of the meta-package in R 4.1.0 was used (www.r-project.org).
We performed subgroup analyses by reported diagnostic criteria. Finally, we performed a leave-one-out sensitivity analysis, and other only including studies with case-control matches.
Two authors (CQV and CCB) assessed the certainty of our pooled results and narrative synthesis applying the Grading of Recommendation, Assessment, Development, and Evaluation (GRADE) on continuous outcomes (29) and narrative synthesis (30), respectively. This assessment is based on five domains: study limitations (risk of bias of the studies included), imprecision (sample size and confidence interval), indirectness (generalizability), inconsistency (heterogeneity), and publication bias as stated in the GRADE handbook (31) and prognostic factor (32). We adapted the assessment to our results. The certainty of the evidence was characterized as high, moderate, low, or very low.
This systematic review included published and open information in which no human subjects participated. Thus, no ethics committee approval was required.
We identified 745 studies through our systematic search. We removed duplicated and screened 610. Finally, 10 articles (6, 20–28) were included (Figure 1).
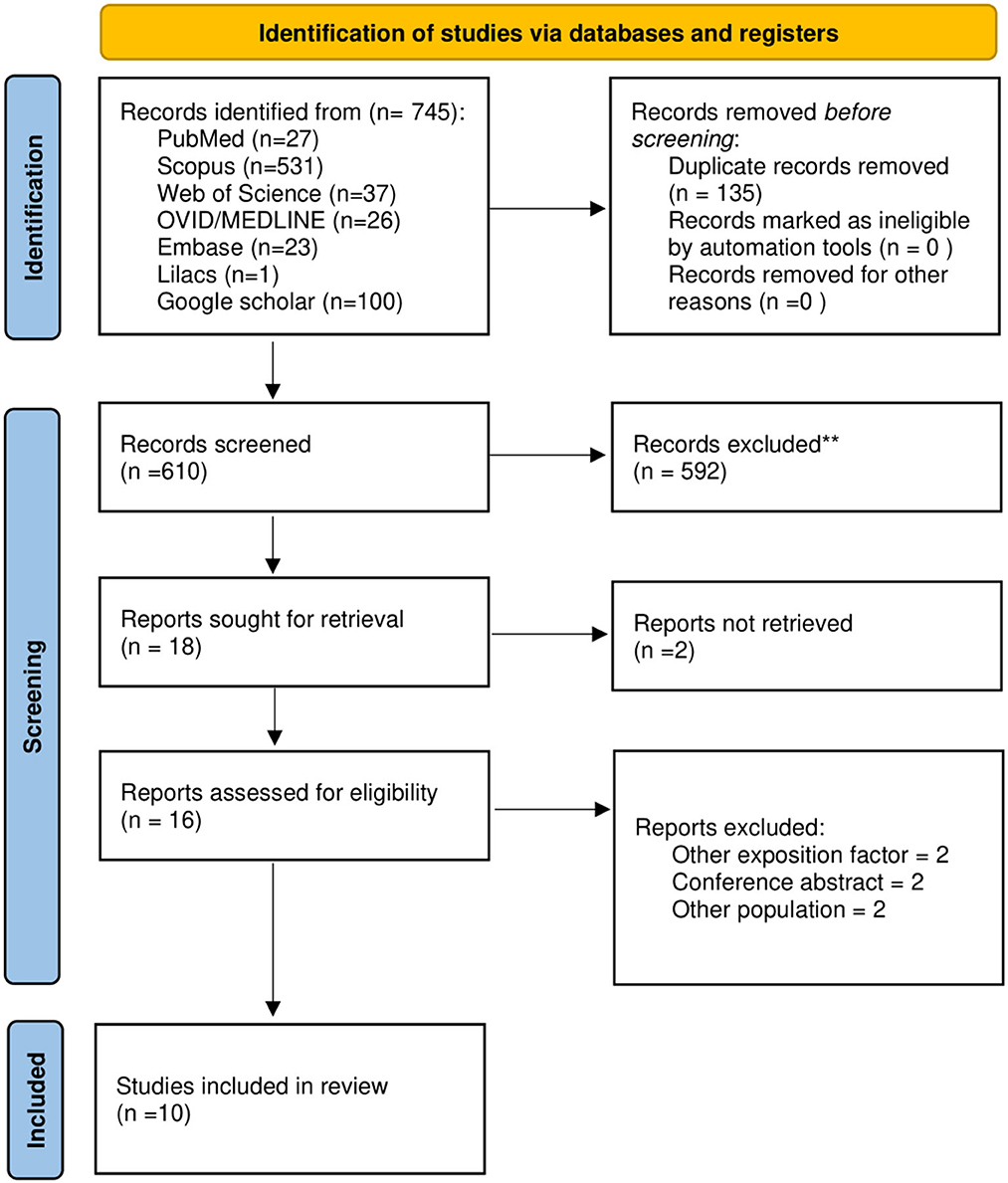
Figure 1. PRISMA flowchart of included studies.
Five studies (21–25) included both cohort and case-control designs, four (6, 26–28) included only retrospective cohorts and one (20) was a case-control study. The total number of participants was 1,626 (1,055 GBS patients and 571 healthy controls). The average age range of GBS patients was between 32.3 and 55.0. The studies characteristics are summarized in Table 1.
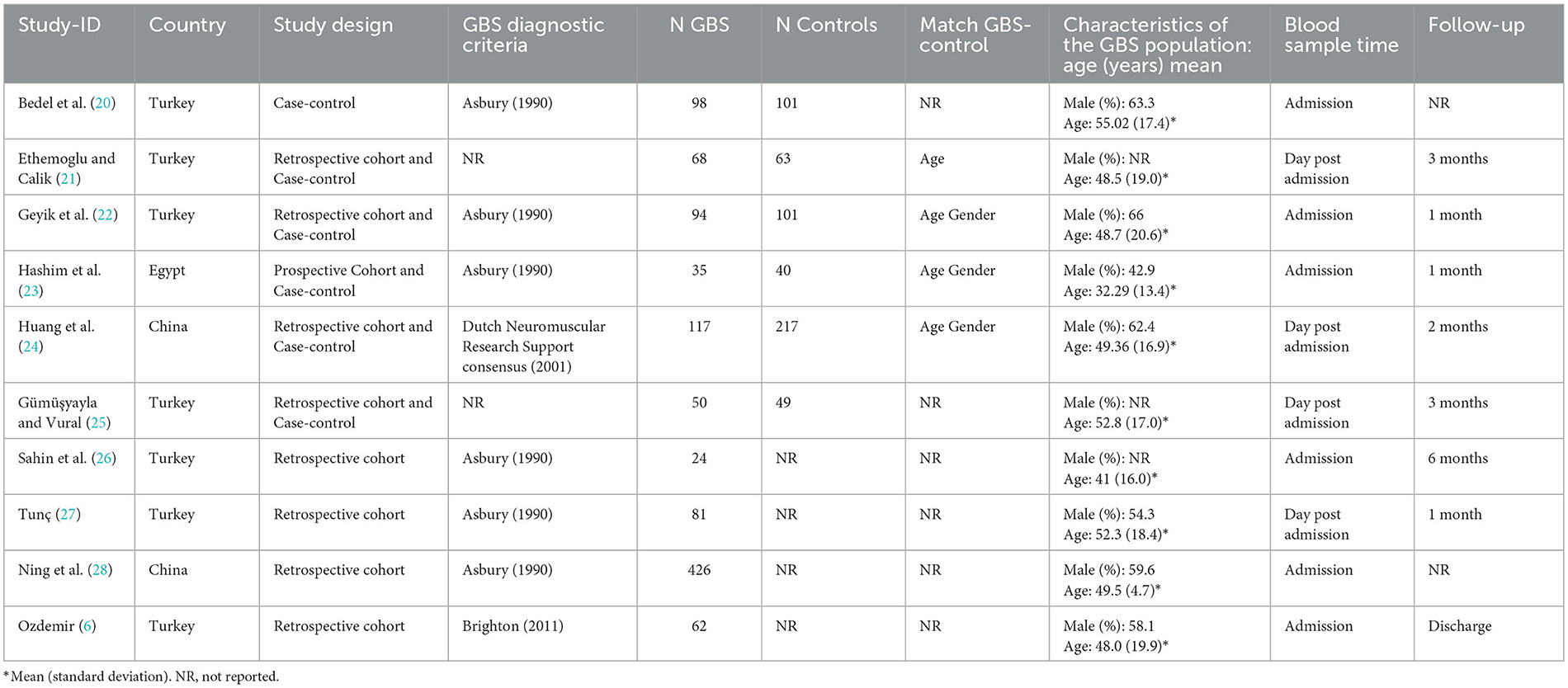
Table 1. Characteristics of included studies evaluating the clinical significance of neutrophil-to-lymphocyte ratio (NLR) in Guillain-Barré syndrome (GBS) (n = 10).
Among the ten studies that met our inclusion criteria, six (20–25) were pooled. A total of 968 participants were selected, of which 430 were assigned to the GBS group and 538 to the control group. In the pooled analysis, a significant increase in NLR was observed in GBS vs. control groups but with high heterogeneity (MD: 1.76; 95% CI: 1.29; 2.24; I2 = 86%) (Figure 2).
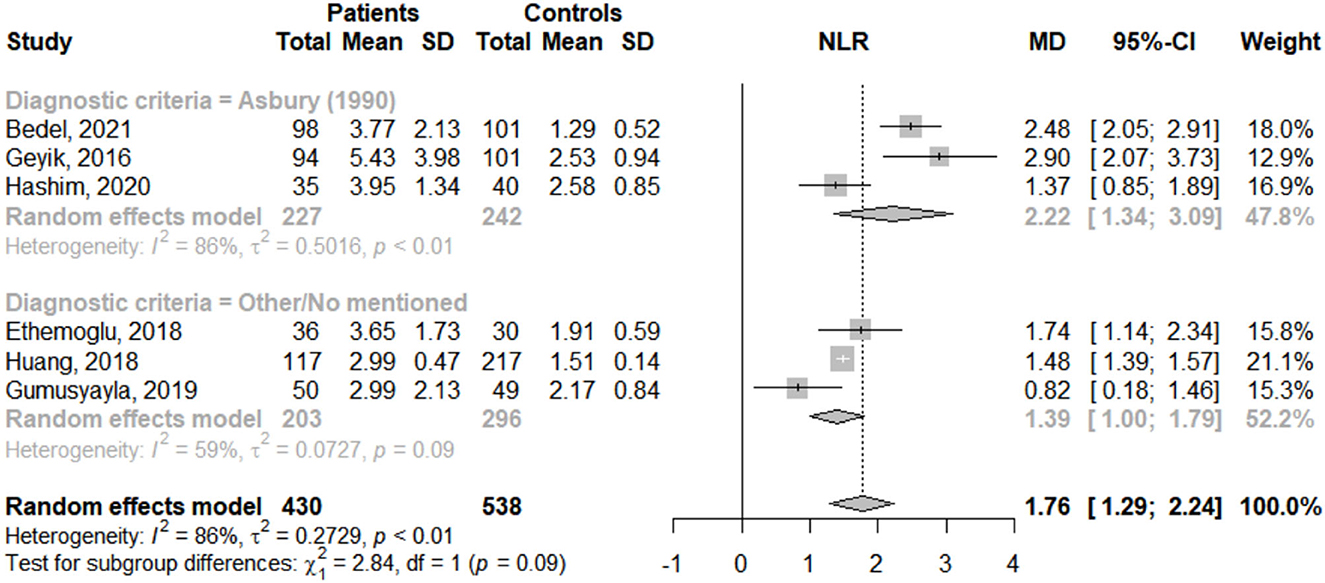
Figure 2. Mean difference of neutrophil-to-lymphocyte ratio (NLR) between GBS patients and healthy controls according to reported diagnostic criteria.
To identify potential sources of heterogeneity, subgroup analysis was performed according to reported diagnostic criteria. NLR was significantly higher in GBS patients compared to healthy controls regardless of whether GBS was diagnosed with Asbury criteria (MD: 2.22; 95% CI: 1.34; 3.09; I2 = 86%) or other/no mentioned (MD: 1.39; 95% CI: 1.00; 1.79; I2 = 59%) (Figure 2). In addition, heterogeneity was high among studies that used the Asbury criteria and moderate in those that used other/no mentioned.
Regarding sensitive analysis, when single studies were sequentially removed, no significant effect on the pooled MD was observed, with an effect size ranging from 1.59 to 1.94 and I2 ranged from 76 to 89 (Supplementary Table 3). Additionally, when studies without case-control match were excluded, no significant effect was described (MD: 1.75; 95% CI: 1.29; 2.21; I2 = 75%). These suggest that the results estimated by meta-analysis were stable (Supplementary Table 4).
Nine studies (6, 21–28) (925 GBS patients) assessed NLR as a poor prognostic factor. Only three reported sensitivity and specificity. Regarding prognosis of disability (Hughes ≥ 3), Hashim et al. (23) included 35 patients whose cut-off point was 4.4 with a sensitivity of 81.5% and specificity of 87.5%, Huang et al. (24) included 117 participants whose cut-off point was 3.05 with a sensitivity of 67.3% and specificity of 67.3% (Table 2).
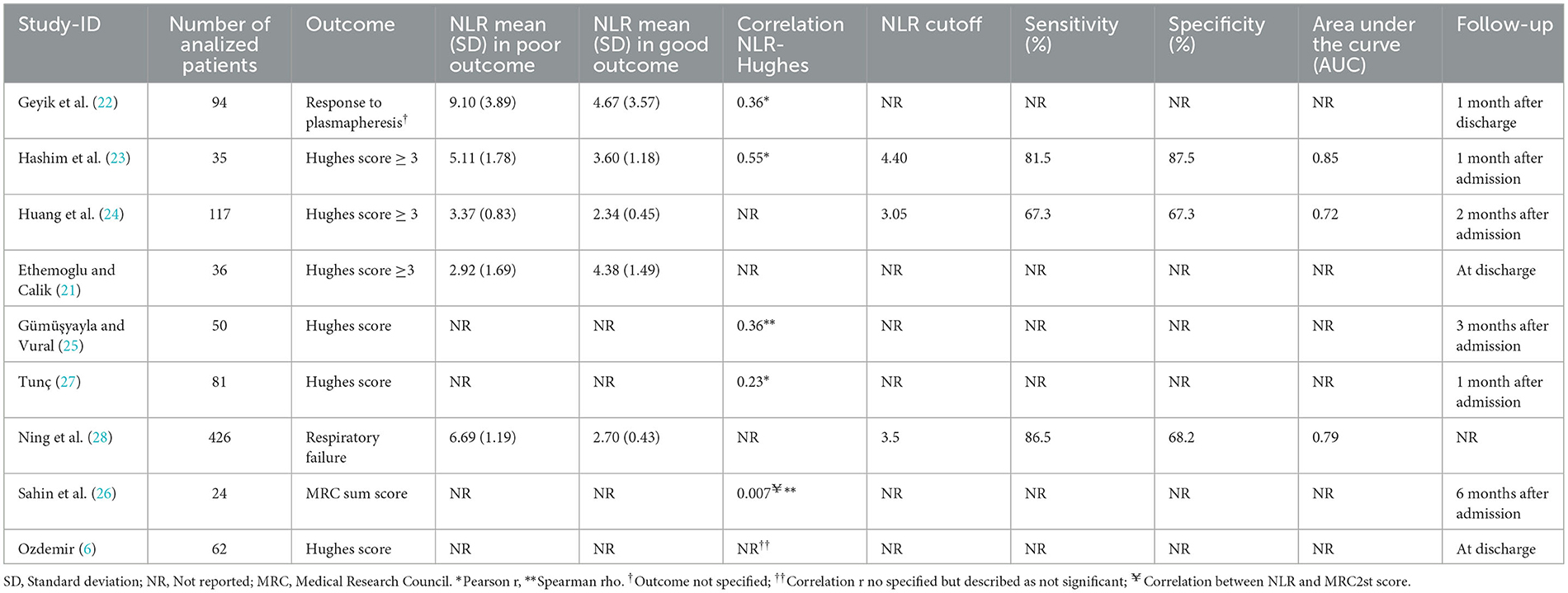
Table 2. Characteristics of included studies evaluating the use of neutrophil-to-lymphocyte ratio (NLR) as a prognosis factor of Guillain-Barré syndrome (GBS) patients (n = 9).
For the respiratory failure outcome, only one large-size study reported this. Ning et al. (28) included 426 patients whose cut-off point was 3.5 with a sensitivity of 86.5% and a specificity of 68.2% (Table 2).
We performed the risk of bias of the ten included studies. Eight articles had “low risk of bias.” Among the cohort studies, Gümüşyayla et al. (25) scored the lowest for deficiencies in the comparability domain, while Ning et al. (28), Huang et al. (24), and Ethemoglu et al. (21) scored the highest. The only case-control design considered for risk of bias assessment (20) scored 6/9 for deficiencies in information response rate and the selection of controls (Supplementary Table 5).
Regarding GBS patients and healthy controls, we judged the certainty of the included evidence as moderate. We started the evaluation from high certainty because we included observational studies (comparative observational design). We downgraded according to the high heterogeneity between the studies (I2 = 86%) (Table 3). About the severity and respiratory failure outcome, we started the assessment from high certainty because all included studies were observational studies (cohort design). For severity, Hughes's score ≥ 3 had a low certainty for sensitivity and specificity, downgraded according to inconsistency due to high heterogeneity (studies showed a sensitivity of 67.3 to 81.5 and specificity of 67.3 to 87.5) and imprecision (sensitivity and specificity crossed through the imprecision point of 70%). For respiratory failure, was assessed as moderate and high certainty to specificity and sensitivity, respectively, downgraded according to imprecision (specificity crossed through the imprecision point of 70%).
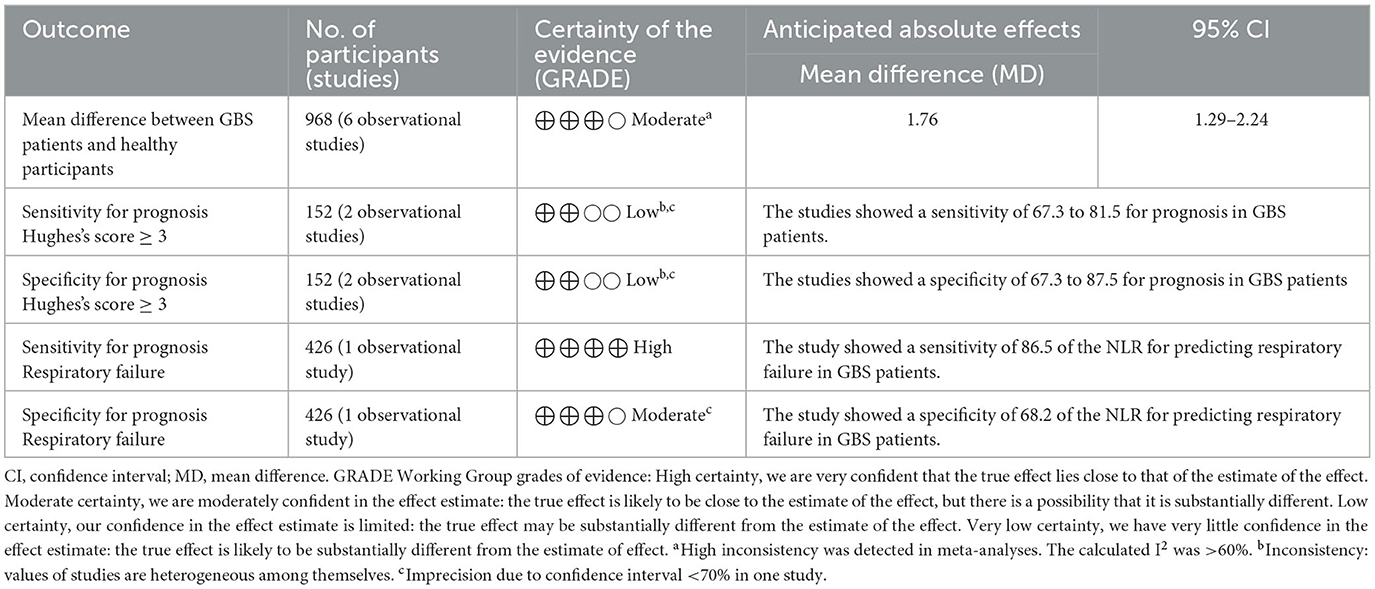
Table 3. Summary of findings.
Our results revealed a higher mean NLR in GBS patients compared to healthy controls. Furthermore, we found that NLR could be a prognostic factor for disability and respiratory failure.
Our pooled analysis showed that mean NLR was significantly higher in GBS patients than in healthy patients. These results were not altered by any study or by studies reporting case-control matching as our sensitivity analysis demonstrates. This agrees with previous reviews that evaluated the NLR in other autoimmune diseases. Olsson et al. (8) evaluated 4 case-control studies and found that the NLR was higher in patients with MS than in healthy controls. Similarly, Paliogiannis et al. (33) reported that a meta-analysis of 12 studies showed a higher values NLR (SMD = 0.69, 95% CI 0.53–1.85, p < 0.001) in patients with psoriasis than in healthy patients. In turn, Erre et al. (34) and Ma et al. (35) reported similar results for rheumatoid arthritis (SMD = 0.79, 95% CI 0.55–1.03; p < 0.001) and systemic lupus erythematosus (SMD = 1.004, 95% CI = 0.781–1.227, P < 0.001), respectively. This would show that high NLR values could differentiate between autoimmune diseases and healthy persons. The biological mechanism that would explain these relationship between NLR and GBS, is the increase of immune cells such as neutrophils, macrophages, dendritic cells and T cells in response to peripheral nerve injury (36).
Despite its importance and novelty, the presence of systematic reviews about NLR and its prognosis in neurological diseases, specifically autoimmune diseases, is limited. Olsson et al. (8) reported five studies that evaluated NLR as a prognostic factor in multiple sclerosis. Among these, one reported that high NLR (>3.9) was an independent predictor of disability progression (p = 0.001). Also, Guzel et al. (37) reported that a cut-off point of 4.52 (sensitivity: 96.1%; specificity: 57.1%) in multiple sclerosis patients have a discriminatory capacity for disability [Expanded Disability Status Scale (EDSS) ≥ 5]. These results were similar to our results in patients with GBS where the cut-off points were 4.40 (sensitivity: 81.5%; specificity: 87.5%) and 3.05 (sensitivity: 67.3%; specificity: 67.3%) for disability (Hughes ≥ 3). This is also supported by an observational study in which 34 patients with autoimmune encephalitis presented a cut-off value of 4.82 (sensitivity: 78%; specificity: 88%) to predict severity defined as Modified Rankin Scale (mRS) score > 3 (13). This can be explained by the presence of serum low-density neutrophils (LDN), which are immature and degranulated cells with immunomodulatory capacity that are prematurely mobilized from the bone marrow (38, 39). These LDNs secrete higher levels of proinflammatory cytokines, including interleukin 10 and interferon 21 (40). Levels of this cell type have been correlated with poor prognosis in patients with GBS (41). However, despite the findings, the pathological levels of NLR for different diseases have not yet been standardized, with a possible range of normality being between 0.78 and 3.53 (42).
Otherwise, one of our included studies also evaluated the ability of NLR to predict respiratory failure in patients with GBS with a cut-off point of 3.5 (sensitivity: 86.5%; specificity: 68.2%). According to Moisa et.al. (43), NLR with a cut-off point > 2 was found to predict the need for mechanical ventilation and >11 for mortality at 48 h after admission to ICU in patients with severe or critical pneumonia due to COVID-19. Nair et al. (44) also reported a cut-off point of 4.6 (sensitivity: 79.2%; specificity: 62.3%) for ventilatory assistance 24 h after admission to ICU, which is supported by an SR where the NLR cut-off points ranged from 3.3 to 5.9 predicted a severe COVID-19 condition defined as present respiratory failure (45). As mentioned above, the correlation between NLR and a worse prognosis in GBS could be because neutrophils are one of the first lines of response to peripheral nerve injury so it proliferates within the first hours of trauma (46). This would make the NLR more susceptible to any poor prognosis with respect to other biomarkers.
According to GRADE approach, the certainty of evidence from the NLR was moderate in GBS patients vs. healthy controls due to high heterogeneity between studies. In our subgroup analysis by GBS diagnostic criteria, it was possible to observe differences in effect size and heterogeneity. This aspects should be expanded in future studies, in addition to taking into account the Brighton criteria (47), since only one study reported using them (6). Finally, we recommend conducting studies that use the NLR for the differential diagnosis of other polyneuropathies (chronic inflammatory demyelinating polyradiculoneuropathy, metabolic diseases, toxicity, others).
Certainty for sensitivity and specificity for poor prognosis (Hughes ≥ 3) was low due to heterogeneity and imprecision. Therefore, prospective studies with long-term follow-up are needed to determine optimal cut-off point taking into account the different prognosis of axonal and demyelinating GBS (48, 49). In addition, since majority of included studies was realized in one country (Turkey), it is recommended to analyze the NLR in different GBS populations due there are variations in clinical patterns and severity between Europe/America and Asia (50). On the other hand, the modified Erasmus GBS Outcome Score (mEGOS) is a validated tool that predicts short- and long-term disability with clinical variables that are easy to obtain at admission (51), so the NLR could be added to that tool for better prognostic accuracy. Regarding the prognosis of respiratory failure, the evidence was moderate based on a single large size cohort; however, there are no data about the time in which this failure will be established so more studies are recommended to evaluate the NLR as a prognostic of early requirement of mechanic ventilation. Like mEGOS, there is a validated tool that predicts respiratory failure (EGRIS) based on three simple variables (52, 53), so NLR could also be a biomarker to take into account due to its similar characteristics.
NLR is not only an indicator of systemic inflammation but can also serve as an early warning of a pathological state or process (54). For neurological diseases, it has demonstrated clinical utility in assessing the activity or prognosis of diseases such as multiple sclerosis (8). Our results show that the NLR was significantly higher in GBS patients with respect to healthy patients and that, in turn, it was also a poor prognostic factor. The early identification of GBS patients with poor prognosis could benefit them since they can be treated with different doses, although this is not yet conclusive (55, 56). In addition, determine who will have respiratory failure may allow early intubation and reduce the risk of early-onset pneumonia (57). Several biomarkers associated with GBS such as cerebrospinal lipids (58) or IL-8 have been reported to differentiate GBS from chronic inflammatory demyelinating polyneuropathy (CIDP) (59).However, the clinical importance of NLR lies in the simplicity of its performance, its low cost, its availability in routine examinations and its easy acceptance by physicians and patients. Therefore, if its role is confirmed with more and better studies, it should be recommended for its diagnostic and prognostic application.
There are some limitations to this systematic review. First, most of the studies were retrospective in nature, so their results could be prone to confounding. In addition, most on the included studies were realized in only one country (Turkey) so it's necessary to analyze the NLR values of other GBS patients from different parts of the world, to seek for variations in clinical patterns and severity. Also, there was significant heterogeneity among the included articles in our meta-analysis. However, our results were strengthened by sensitivity analyzes performed. Our study also has strengths. This is the first systematic review that evaluates the clinical significance of NLR in the diagnosis and prognosis of GBS. Second, we conducted a comprehensive systematic search without language or time restrictions. Finally, we performed an assessment of the certainty of our results using the GRADE criteria.
Based on the evidence available, with moderate certainty, mean NLR is higher in GBS patients compared to healthy controls. Furthermore, with low and moderate certainty, we found that NLR could be a prognostic factor for disability and respiratory failure, respectively. Future prospective studies in different regions with long-term follow-up are required to determine optimal cut-off values considering the possibility of including NLR in validated prognostic tools.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
MC-L: drafting/revision of the manuscript for content, including medical writing for content, study concept or design, and analysis or interpretation of data. CQ-V and CA-D: drafting/revision of the manuscript for content, including medical writing for content, major role in the acquisition of data, and study concept or design. CC-B, MP-G, and NM-Q: drafting/revision of the manuscript for content, including medical writing for content, and major role in the acquisition of data. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2023.1153690/full#supplementary-material
1. van den Berg B, Walgaard C, Drenthen J, Fokke C, Jacobs BC, van Doorn PA. Guillain-Barré syndrome: pathogenesis, diagnosis, treatment and prognosis. Nat Rev Neurol. (2014) 10:469–82. doi: 10.1038/nrneurol.2014.121
2. Sejvar JJ, Baughman AL, Wise M, Morgan OW. Population incidence of Guillain-Barré syndrome: a systematic review and meta-analysis. Neuroepidemiology. (2011) 36:123–33. doi: 10.1159/000324710
3. Bragazzi NL, Kolahi AA, Nejadghaderi SA, Lochner P, Brigo F, Naldi A, et al. Global, regional, and national burden of Guillain-Barré syndrome and its underlying causes from 1990 to 2019. J Neuroinflammation. (2021) 18:264. doi: 10.1186/s12974-021-02319-4
4. Kuwabara S, Yuki N. Axonal guillain-barré syndrome: concepts and controversies. Lancet Neurol. (2013) 12:1180–8. doi: 10.1016/S1474-4422(13)70215-1
5. Jasti AK, Selmi C, Sarmiento-Monroy JC, Vega DA, Anaya JM, Gershwin ME. Guillain-Barré syndrome: causes, immunopathogenic mechanisms and treatment. Expert Rev Clin Immunol. (2016) 12:1175–89. doi: 10.1080/1744666X.2016.1193006
6. Ozdemir HH. Analysis of the albumin level, neutrophil-lymphocyte ratio, and platelet-lymphocyte ratio in Guillain-Barré syndrome. Arq Neuropsiquiatr. (2016) 74:718–22. doi: 10.1590/0004-282X20160132
7. Rodríguez Y, Rojas M, Pacheco Y, Acosta-Ampudia Y, Ramírez-Santana C, Monsalve DM, et al. Guillain-barré syndrome, transverse myelitis and infectious diseases. Cell Mol Immunol. (2018) 15:547–62. doi: 10.1038/cmi.2017.142
8. Olsson A, Gustavsen S, Gisselø Lauridsen K, Chenoufi Hasselbalch I, Sellebjerg F, Bach Søndergaard H, et al. Neutrophil-to-lymphocyte ratio and CRP as biomarkers in multiple sclerosis: a systematic review. Acta Neurol Scand. (2021) 143:577–86. doi: 10.1111/ane.13401
9. Leonhard SE, Mandarakas MR, Gondim FAA, Bateman K, Ferreira MLB, Cornblath DR, et al. Diagnosis and management of guillain-barré syndrome in ten steps. Nat Rev Neurol. (2019) 15:671–83. doi: 10.1038/s41582-019-0250-9
10. Mayeux R. Biomarkers: potential uses and limitations. NeuroRx. (2004) 1:182–8. doi: 10.1602/neurorx.1.2.182
11. Mondello S, Salama MM, Mohamed WMY, Kobeissy FH. Editorial: biomarkers in Neurology. Front Neurol. (2020) 11:190. doi: 10.3389/fneur.2020.00190
12. Ballman KV. Biomarker: predictive or prognostic? J Clin Oncol. (2015) 33:3968–71. doi: 10.1200/JCO.2015.63.3651
13. Zeng Z, Wang C, Wang B, Wang N, Yang Y, Guo S, et al. Prediction of neutrophil-to-lymphocyte ratio in the diagnosis and progression of autoimmune encephalitis. Neurosci Lett. (2019) 694:129–35. doi: 10.1016/j.neulet.2018.12.003
14. Ji Z, Liu G, Guo J, Zhang R, Su Y, Carvalho A, et al. The neutrophil-to-lymphocyte ratio is an important indicator predicting in-hospital death in AMI patients. Front Cardiovasc Med. (2021) 8:706852. doi: 10.3389/fcvm.2021.706852
15. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
16. Hughes RA, Newsom-Davis JM, Perkin GD, Pierce JM. Controlled trial prednisolone in acute polyneuropathy. Lancet. (1978) 2:750–3. doi: 10.1016/S0140-6736(78)92644-2
17. van Koningsveld R, Steyerberg EW, Hughes RA, Swan AV, van Doorn PA, Jacobs BC, et al. clinical prognostic scoring system for Guillain-Barré syndrome. Lancet Neurol. (2007) 6:589–94. doi: 10.1016/S1474-4422(07)70130-8
18. Mendoza-Chuctaya G, Montesinos-Segura R, Agramonte-Vilca M, Aguirre-Tenorio L. Características y prevalencia de partos domiciliarios en un distrito rural de la sierra del perú, 2015-2016. Rev Chil Obstet Ginecol. (2018) 83:377–85. doi: 10.4067/s0717-75262018000400377
19. Ulloque-Badaracco JR, Ivan Salas-Tello W, Al-Kassab-Córdova A, Alarcón-Braga EA, Benites-Zapata VA, Maguiña JL, et al. Prognostic value of neutrophil-to-lymphocyte ratio in COVID-19 patients: a systematic review and meta-analysis. Int J Clin Pract. (2021) 75:e14596. doi: 10.1111/ijcp.14596
20. Bedel C, Korkut M, Hospital R. The clinical significance of neutrophil lymphocyte ratio, monocyte lymphocyte ratio and platelet lymphocyte ratio in patients with guillain-barré syndrome. Haydarpaşa Numune Med J. (2021) 61:341–5. doi: 10.14744/hnhj.2019.38233
21. Ethemoglu O, Calik M. Effect of serum inflammatory markers on the prognosis of adult and pediatric patients with Guillain-Barré syndrome. Neuropsychiatr Dis Treat. (2018) 14:1255–60. doi: 10.2147/NDT.S162896
22. Geyik S, Bozkurt H, Neyal M, Yigiter R, Kuzudisli S, Kul S, et al. The clinical significance of the neutrophil-to-lymphocyte ratio in patients with Guillain-Barré syndrome independent of infection. Med Sci Discov. (2016) 3:305–11. doi: 10.17546/msd.90383
23. Hashim NA, Mohamed WS, Emad EM. Neutrophil–lymphocyte ratio and response to plasmapheresis in Guillain–Barré syndrome: a prospective observational study. Egypt J Neurol Psychiatry Neurosurg. (2020) 56:17. doi: 10.1186/s41983-020-0154-z
24. Huang Y, Ying Z, Quan W, Xiang W, Xie D, Weng Y, et al. The clinical significance of neutrophil-to-lymphocyte ratio and monocyte-to-lymphocyte ratio in Guillain-Barré syndrome. Int J Neurosci. (2018) 128:729–35. doi: 10.1080/00207454.2017.1418342
25. Gümüşyayla S, Vural G. The predictive value of neutrophil-lymphocyte ratio in disability of gullain-barr? syndrome. Bakirköy Tip Dergisi. (2019) 15:187. doi: 10.4274/BTDMJB.galenos.2019.20171214071335
26. Sahin S, Cinar N, Karsidag S. Are cerebrospinal fluid protein levels and plasma neutrophil/lymphocyte ratio associated with prognosis of guillain barré syndrome? Neurol Int. (2017) 9:7032. doi: 10.4081/ni.2017.7032
27. Tunç A. Early predictors of functional disability in Guillain-Barré Syndrome. Acta Neurol Belg. (2019) 119:555–9. doi: 10.1007/s13760-019-01133-3
28. Ning P, Yang B, Yang X, Huang H, Shen Q, Zhao Q, et al. Lymphocyte-based ratios for predicting respiratory failure in Guillain-Barré syndrome. J Neuroimmunol. (2021) 353:577504. doi: 10.1016/j.jneuroim.2021.577504
29. Guyatt GH, Thorlund K, Oxman AD, Walter SD, Patrick D, Furukawa TA, et al. GRADE guidelines: 13. preparing summary of findings tables and evidence profiles-continuous outcomes. J Clin Epidemiol. (2013) 66:173–83. doi: 10.1016/j.jclinepi.2012.08.001
30. Murad MH, Mustafa RA, Schünemann HJ, Sultan S, Santesso N. Rating the certainty in evidence in the absence of a single estimate of effect. Evid Based Med. (2017) 22:85–7. doi: 10.1136/ebmed-2017-110668
31. Schünemann H, Brozek J, Guyatt G, Oxman A. GRADE Handbook for Grading Quality of Evidence and Strength of Recommendation 2008. Available online at: https://gdt.gradepro.org/app/handbook/handbook.html
32. Huguet A, Hayden JA, Stinson J, McGrath PJ, Chambers CT, Tougas ME, et al. Judging the quality of evidence in reviews of prognostic factor research: adapting the GRADE framework. Syst Rev. (2013) 2:71. doi: 10.1186/2046-4053-2-71
33. Paliogiannis P, Satta R, Deligia G, Farina G, Bassu S, Mangoni AA, et al. Associations between the neutrophil-to-lymphocyte and the platelet-to-lymphocyte ratios and the presence and severity of psoriasis: a systematic review and meta-analysis. Clin Exp Med. (2019) 19:37–45. doi: 10.1007/s10238-018-0538-x
34. Erre GL, Paliogiannis P, Castagna F, Mangoni AA, Carru C, Passiu G, et al. Meta-analysis of neutrophil-to-lymphocyte and platelet-to-lymphocyte ratio in rheumatoid arthritis. Eur J Clin Invest. (2019) 49:e13037. doi: 10.1111/eci.13037
35. Ma L, Zeng A, Chen B, Chen Y, Zhou R. Neutrophil to lymphocyte ratio and platelet to lymphocyte ratio in patients with systemic lupus erythematosus and their correlation with activity: a meta-analysis. Int Immunopharmacol. (2019) 76:105949. doi: 10.1016/j.intimp.2019.105949
36. Hagen KM, Ousman SS. The neuroimmunology of Guillain-Barré Syndrome and the potential role of an aging immune system. Front Aging Neurosci. (2021) 12:613628. doi: 10.3389/fnagi.2020.613628
37. Guzel I, Mungan S, Oztekin ZN, Ak F. Is there an association between the Expanded Disability Status Scale and inflammatory markers in multiple sclerosis? J Chin Med Assoc. (2016) 79:54–7. doi: 10.1016/j.jcma.2015.08.010
38. Morisaki T, Goya T, Ishimitsu T, Torisu M. The increase of low density subpopulations and CD10 (CALLA) negative neutrophils in severely infected patients. Surg Today. (1992) 22:322–7. doi: 10.1007/BF00308740
39. Ng LG, Ostuni R, Hidalgo A. Heterogeneity of neutrophils. Nat Rev Immunol. (2019) 19:255–65. doi: 10.1038/s41577-019-0141-8
40. Rahman S, Sagar D, Hanna RN, Lightfoot YL, Mistry P, Smith CK, et al. Low-density granulocytes activate T cells and demonstrate a non-suppressive role in systemic lupus erythematosus. Ann Rheum Dis. (2019) 78:957–66. doi: 10.1136/annrheumdis-2018-214620
41. Ren K, Yang A, Lu J, Zhao D, Bai M, Ding J, et al. Association between serum low-density neutrophils and acute-onset and recurrent Guillain-Barré syndrome. Brain Behav. (2022) 12:e2456. doi: 10.1002/brb3.2456
42. Forget P, Khalifa C, Defour JP, Latinne D, Van Pel MC, De Kock M. What is the normal value of the neutrophil-to-lymphocyte ratio? BMC Res Notes. (2017) 10:12. doi: 10.1186/s13104-016-2335-5
43. Moisa E, Corneci D, Negoita S, Filimon CR, Serbu A, Negutu MI, et al. Dynamic changes of the neutrophil-to-lymphocyte ratio, systemic inflammation index, and derived neutrophil-to-lymphocyte ratio independently predict invasive mechanical ventilation need and death in critically Ill COVID-19 patients. Biomedicines. (2021) 9:1656. doi: 10.3390/biomedicines9111656
44. Nair PR, Maitra S, Ray BR, Anand RK, Baidya DK, Subramaniam R. Neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio as predictors of the early requirement of mechanical ventilation in COVID-19 patients. Indian J Crit Care Med. (2020) 24:1143–4. doi: 10.5005/jp-journals-10071-23663
45. Yang AP, Liu JP, Tao WQ, Li HM. The diagnostic and predictive role of NLR, d-NLR and PLR in COVID-19 patients. Int Immunopharmacol. (2020) 84:106504. doi: 10.1016/j.intimp.2020.106504
46. Liu JA, Yu J, Cheung CW. Immune actions on the peripheral nervous system in pain. Int J Mol Sci. (2021) 22:1448. doi: 10.3390/ijms22031448
47. Fokke C, van den Berg B, Drenthen J, Walgaard C, van Doorn PA, Jacobs BC. Diagnosis of Guillain-Barré syndrome and validation of Brighton criteria. Brain. (2014) 137:33–43. doi: 10.1093/brain/awt285
48. Arami MA, Yazdchi M, Khandaghi R. Epidemiology and characteristics of Guillain-Barré syndrome in the northwest of Iran. Ann Saudi Med. (2006) 26:22–7. doi: 10.5144/0256-4947.2006.22
49. Tian J, Cao C, Li T, Zhang K, Li P, Liu Y, et al. Electrophysiological subtypes and prognostic factors of Guillain-Barre Syndrome in Northern China. Front Neurol. (2019) 10:714. doi: 10.3389/fneur.2019.00714
50. Doets AY, Verboon C, van den Berg B, Harbo T, Cornblath DR, Willison HJ, et al. Regional variation of Guillain-Barré syndrome. Brain. (2018) 141:2866–77. doi: 10.1093/brain/awy232
51. Doets AY, Lingsma HF, Walgaard C, Islam B, Papri N, Davidson A, et al. Predicting outcome in Guillain-Barré Syndrome: international validation of the modified erasmus GBS outcome score. Neurology. (2022) 98:e518–32. doi: 10.1212/WNL.0000000000013139
52. Doets AY, Walgaard C, Lingsma HF, Islam B, Papri N, Yamagishi Y, et al. International validation of the erasmus Guillain-Barré Syndrome respiratory insufficiency score. Ann Neurol. (2022) 91:521–31. doi: 10.1002/ana.26312
53. Malaga M, Rodriguez-Calienes A, Marquez-Nakamatsu A, Recuay K, Merzthal L, Bustamante-Paytan D, et al. Predicting mechanical ventilation using the egris in Guillain-Barré Syndrome in a Latin American country. Neurocrit Care. (2021) 35:775–82. doi: 10.1007/s12028-021-01218-z
54. Zahorec R. Neutrophil-to-lymphocyte ratio, past, present and future perspectives. Bratisl Lek Listy. (2021) 122:474–88. doi: 10.4149/BLL_2021_078
55. van Koningsveld R, Schmitz PI, Meché FG, Visser LH, Meulstee J, van Doorn PA. Effect of methylprednisolone when added to standard treatment with intravenous immunoglobulin for Guillain-Barré syndrome: randomised trial. Lancet. (2004) 363:192–6. doi: 10.1016/S0140-6736(03)15324-X
56. Walgaard C, Jacobs BC, Lingsma HF, Steyerberg EW, van den Berg B, Doets AY, et al. Second intravenous immunoglobulin dose in patients with Guillain-Barré syndrome with poor prognosis (SID-GBS): a double-blind, randomised, placebo-controlled trial. Lancet Neurol. (2021) 20:275–83. doi: 10.1016/S1474-4422(20)30494-4
57. Orlikowski D, Sharshar T, Porcher R, Annane D, Raphael JC, Clair B. Prognosis and risk factors of early onset pneumonia in ventilated patients with Guillain-Barré syndrome. Intensive Care Med. (2006) 32:1962–9. doi: 10.1007/s00134-006-0332-1
58. Péter M, Török W, Petrovics-Balog A, Vígh L, Vécsei L, Balogh G. Cerebrospinal fluid lipidomic biomarker signatures of demyelination for multiple sclerosis and Guillain-Barré syndrome. Sci Rep. (2020) 10:18380. doi: 10.1038/s41598-020-75502-x
Keywords: Guillain-Barre syndrome, NLR, neutrophil to lymphocyte ratio, diagnosis, prognosis
Citation: Cabanillas-Lazo M, Quispe-Vicuña C, Cruzalegui-Bazán C, Pascual-Guevara M, Mori-Quispe N and Alva-Diaz C (2023) The neutrophil-to-lymphocyte ratio as a prognostic biomarker in Guillain-Barre syndrome: a systematic review with meta-analysis. Front. Neurol. 14:1153690. doi: 10.3389/fneur.2023.1153690
Received: 29 January 2023; Accepted: 03 May 2023;
Published: 02 June 2023.
Edited by:
Stefania Mondello, University of Messina, ItalyReviewed by:
Vitalie Lisnic, Nicolae Testemitanu State University of Medicine and Pharmacy, MoldovaCopyright © 2023 Cabanillas-Lazo, Quispe-Vicuña, Cruzalegui-Bazán, Pascual-Guevara, Mori-Quispe and Alva-Diaz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Carlos Alva-Diaz, YWx2YWNhcmxAY3JlY2UudXNzLmVkdS5wZQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.