
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Neurol., 06 March 2023
Sec. Epilepsy
Volume 14 - 2023 | https://doi.org/10.3389/fneur.2023.1132106
 Jimmy Li1,2*
Jimmy Li1,2* Cassandra C. Areal1Dènahin Hinnoutondji Toffa2,3Daphné Citherlet2Charles Deacon1
Cassandra C. Areal1Dènahin Hinnoutondji Toffa2,3Daphné Citherlet2Charles Deacon1 Didier Jutras-Aswad2,4Mark Robert Keezer2,3,5,6
Didier Jutras-Aswad2,4Mark Robert Keezer2,3,5,6 Dang Khoa Nguyen2,3,6
Dang Khoa Nguyen2,3,6Objective: The use of medical cannabis among people with epilepsy (PWE) has been garnering increasing interest. In this scoping review, we aimed to summarize the literature on recreational/non-medical cannabis (NMC) use in PWE, focusing on the experience, habits, and beliefs of PWE regarding NMC.
Methods: Four databases (OVID Medline, OVID Embase, Ovid APA PsycInfo, and Web of Science) were searched for studies describing NMC use in PWE. NMC was defined as cannabis products procured from sources other than by prescription. Studies that consisted in original research and that detailed the experience, habits, and/or beliefs of PWE regarding NMC use were included in the analysis. Data pertaining to study identification, demographics, NMC use, and epilepsy characteristics were extracted. Descriptive statistical analyses and reflexive thematic analyses were performed to map these data.
Results: In total, 3,228 records were screened, and 66 were included for analysis: 45 had mainly adult samples, whereas 21 had mainly pediatric samples. Most studies were published after 2010, originated from the USA, and were cross-sectional. The median number of PWE using cannabis in these studies was 24.5 (1–37,945). No studies showcased elderly PWE, and most had predominantly Caucasian samples. The lifetime prevalence of NMC use in PWE was variable, ranging between 0.69 and 76.8%. Factors frequently associated with NMC use in PWE were male sex, younger adult age, and lower education status. Children with epilepsy took NMC primarily for seizure control, using high CBD/THC ratios, and only orally. Adults with epilepsy took NMC for various reasons including recreationally, using variable CBD/THC ratios, and predominantly through smoking. The majority of PWE across all studies perceived that NMC aided in seizure control. Other aspects pertaining to NMC use in PWE were rarely reported and often conflicting.
Conclusion: The literature on NMC use in PWE is sparse and heterogeneous, with many salient knowledge gaps. Further research is necessary to better understanding the experience, habits, and beliefs of PWE pertaining to NMC.
Cannabis, also commonly referred to as marijuana, is most often derived from the Cannabis sativa plant and has been used for millennia for recreational, medicinal, and spiritual purposes (1). Historically, cannabis was categorized as an illegal substance in many Western countries (2). In the last decades, however, cannabis has seen a rise in interest in developed countries due to its potential medicinal qualities (2, 3). Research on the medicinal properties of cannabis has pushed many administrative bodies to authorize prescribing medical marijuana for certain disorders, such as epilepsy (3). In the last years, an increasing number of jurisdictions have either decriminalized or legalized non-medical cannabis (NMC) use, making cannabis more available for the general population (2).
Although there is debate on how many active compounds are present in cannabis, trans-Δ-9-tetrahydrocannabinol (THC) and cannabidiol (CBD) are the most described. The psychoactive properties of cannabis are mostly mediated by THC (1). While CBD has clearly been shown to have anti-seizure properties, contradictory pro-convulsant and anti-seizure effects have been reported for THC (4, 5). Four landmark randomized controlled trials (RCTs) have notably demonstrated the anti-seizure benefits of CBD in Lennox-Gastaut syndrome, Dravet syndrome, and tuberous sclerosis. In response, the US Food and Drug Administration (FDA) approved Epidiolex, an oral CBD solution, for the treatment of these three syndromes (3, 6–9). Although Epidiolex is not yet approved in many parts of the world, the evidence surrounding the anti-seizure properties of CBD has prompted an increased demand for high CBD and low THC cannabis oils among individuals with refractory epilepsy (4).
Although medical cannabis is now more readily available in many developed countries, its price point limits its use by many people with epilepsy (PWE). In the US, for instance, Epidiolex is estimated to cost tens of thousands of dollars yearly (4). As recent research on cannabis in epilepsy has mostly focused on medical cannabis despite it not being readily available for PWE in many countries, the following question arises: what is known about the use of NMC in PWE? The prevalence of PWE consuming NMC is not well-described, although some studies report that more than half of PWE consume cannabis, with many basing their consumption on cannabis' role in seizure control (10, 11). This reasoning is not trivial since NMC (with often non-negligible THC content) has not been shown to be an efficacious anti-seizure agent and, while it is used without significant negative consequences by many, it has been associated with various harmful health effects (12). Achieving a better understanding of the various factors underpinning NMC consumption in PWE should be a research priority, especially given its potentially hazardous effects on health and the currently limited availability of medical cannabis in many countries.
The protocol for this review was registered on the Open Science Framework platform (10.17605/OSF.IO/C5E74) and follows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) reporting guideline (13). A scoping review is defined as “a form of knowledge synthesis that addresses an exploratory research question aimed at mapping key concepts, types of evidence, and gaps in research related to a defined area or field by systematically searching, selecting, and synthesizing existing knowledge” (14). The aim of broadly mapping a body of literature is one of the key aspects differentiating a scoping review from a systematic review, which rather aims to answer a set of defined questions by critically appraising the literature. Though both types of review require a similar rigorous, transparent methodology, a scoping review will usually screen for multiple different study designs and will not task itself with quality assessment (15).
This scoping review sought to answer the following research question: “What is known about the consumption of NMC in PWE?” More broadly, we aimed to summarize the nature, extent, and range of the available research on the subject, identify relevant knowledge gaps, and offer recommendations for future research (16). NMC was defined as all cannabis products, in any form (e.g., whole plant or oil), that are procured from sources other than by prescription from a medical professional (e.g., legal market, if applicable, or illicit vendors). As such, even if a cannabis product was used by an individual for a “self-medicating” purpose (e.g., for seizure control), if this product was not prescribed by a medical professional, it was still considered NMC. The term “recreational cannabis,” which can be thought of as interchangeable with NMC, was not employed in this review, as it may infer that the cannabis product is used only recreationally, whereas it may in fact be used mainly for its perceived health benefits.
All authors revised and contributed to the search strategy. A health sciences librarian reviewed the search strategy and offered adjustments, and a consensus was eventually reached to search the following databases: OVID Medline, OVID Embase, OVID APA PsycInfo, and Web of Science (17). Free-text terms were combined in various manners with controlled vocabulary terms (when applicable) to search for research reporting on humans. These search terms were inspired from previous research investigating strategies for identifying citations on epilepsy and cannabis (18, 19). The full search strategy, including sources of gray literature, is available in Supplementary Table S1. No restrictions were placed on language or time of publication. Online translation services were employed when feasible for studies written in languages other than English, French, and Spanish. We employed a “snowballing” method by which the reference lists of up to 20 selected literature reviews on cannabis use in epilepsy were manually reviewed for additional works of interest. All citations were imported in the Covidence online platform, which was used for the study selection phase. Duplicate citations were automatically removed by the Covidence platform, and duplicates that remained were manually identified during the study selection phase.
Two reviewers (J.L. and C.C.A.) independently screened titles and abstracts on the Covidence platform for works pertaining to the use of NMC in PWE. At this stage, citations were included if they explicitly described NMC consumption in PWE or if they described cannabis consumption in PWE without enough information to determine if the cannabis was medical or non-medical. Citations explicitly only describing medical cannabis use in PWE (e.g., studies in which patients with epilepsy are offered CBD products by the investigators), only describing the drug mechanisms of cannabis, only involving non-human subjects, or consisting in duplicates were excluded. No restriction was placed on study type. Full-text articles were then independently reviewed by the same two reviewers (J.L. and C.C.A.) using the Covidence platform. At this stage, citations were included if they described the experience, habits, and/or beliefs of PWE in relation to NMC use. Citations were excluded if they only pertained to medical cannabis use, if they only described the drug mechanisms of cannabis in epilepsy, if they consisted in duplicate citations, or if they were not original research. Any disagreement between the two reviewers were resolved through discussion, with third party (D.H.T.) intervention as necessary.
Data were independently extracted from the works having passed the selection phase by one reviewer (J.L.) using an Excel spreadsheet. A second reviewer (C.C.A.) verified the data extraction form, and disagreements were handled through discussion with a third party (D.H.T.) when needed. The following information was extracted when available:
a. Publication identification: first author, title, publication year, publication origin, journal/conference of publication, publication type, and potentially significant funding/conflicts of interest.
b. Study characteristics: sample, study aim, sample type, number of study participants in total (e.g., number of PWE in total if only a subset used NMC), and number of PWE using NMC.
c. Demographics (of PWE using NMC): age, sex, education status, comorbidities, socio-economic standing, and marital status.
d. Epilepsy data: age of onset, epilepsy type (focal-onset vs. generalized-onset), epilepsy syndrome, and antiseizure medication (ASM) use.
e. NMC data: experience with NMC (prevalence of consumers among PWE or of epilepsy among consumers, factors independently associated with consumption, dependency on NMC, consequences of consumption on physical, mental, and social spheres), habits with NMC (type of NMC consumed, administration method, dose of CBD and THC in NMC, frequency of consumption, time since start of consumption, age at first consumption, source of acquisition, product pricing), and beliefs in relation to NMC (goals for consumption, information sources, general knowledge of cannabis, opinion on regulatory policies, and perceived benefits and drawbacks of consumption on seizure control or other aspects of livelihood).
Data were synthesized using Excel. Our analysis comprised a numerical component, wherein data were synthesized using descriptive statistical methods, and a thematic component, wherein data were qualitatively analyzed for themes using a reflexive approach (20). Descriptive statistical analyses were used to synthesize findings from adult studies and pediatric studies separately. Numerical data are presented as medians (range) and count (proportions), where appropriate. All descriptive statistical analyses were performed using R.
A total of 4,182 records were identified using the search strategy in Supplementary Table S1. With 953 records being flagged as duplicates by Covidence, 3,228 records underwent the title/abstract screening phase. A total of 121 records passed this phase and underwent full-text screening. Of these records, the reference lists of 20 selected literature reviews were manually examined for additional works of interest. No additional works of interest were detected. With 55 records being excluded from the full-text screening phase, 66 records were included in the final analysis (2, 4, 10, 11, 21–82). The data selection flowchart is presented in Figure 1.
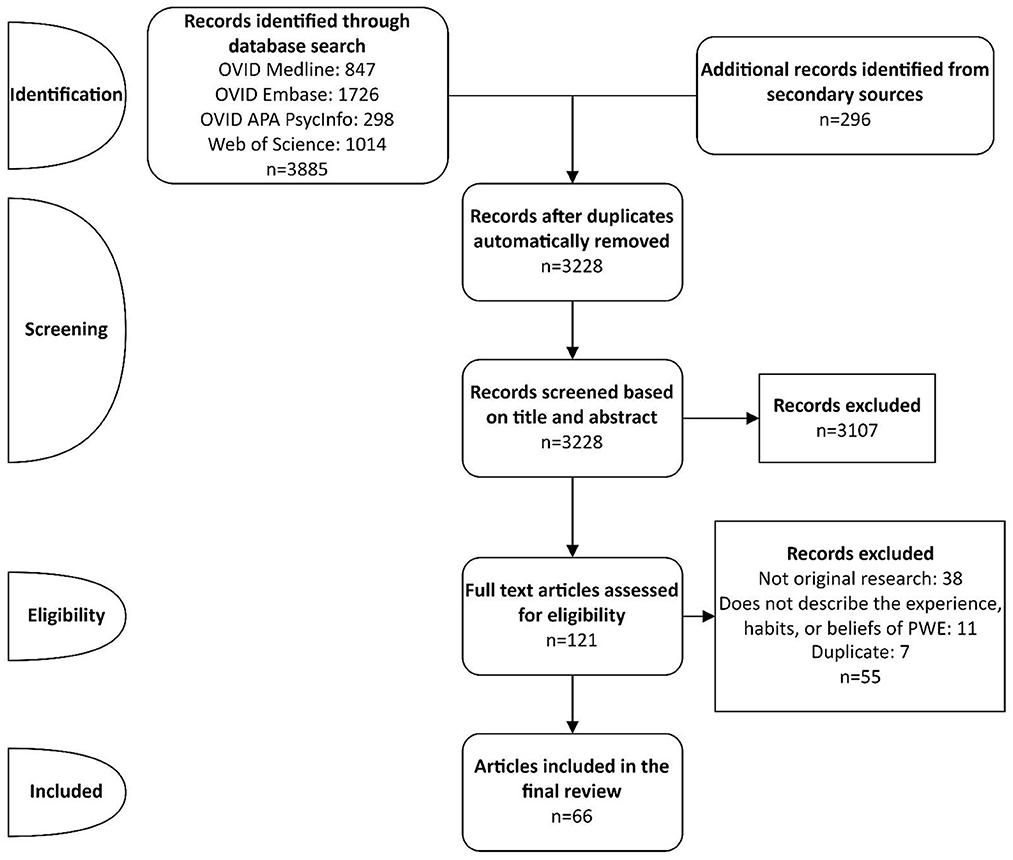
Figure 1. Data selection flowchart.
Table 1 lists the studies included in this review and provides a summary of their sample and primary aim. Table 2 presents in detail the publication identification and study characteristics of all 66 included studies whilst providing separate information for adult and pediatric studies. Supplementary Table S2 presents how many times each variable of interest (demographic, epilepsy, and NMC data) is explored across all included studies and between adult and pediatric studies. Figure 2 consists in a visual summary of the topics/variables touched upon by each study, taking the form of a “heatmap.” An in-depth exploration of all variables of interest measured across all included studies is provided in Supplementary Table S3.
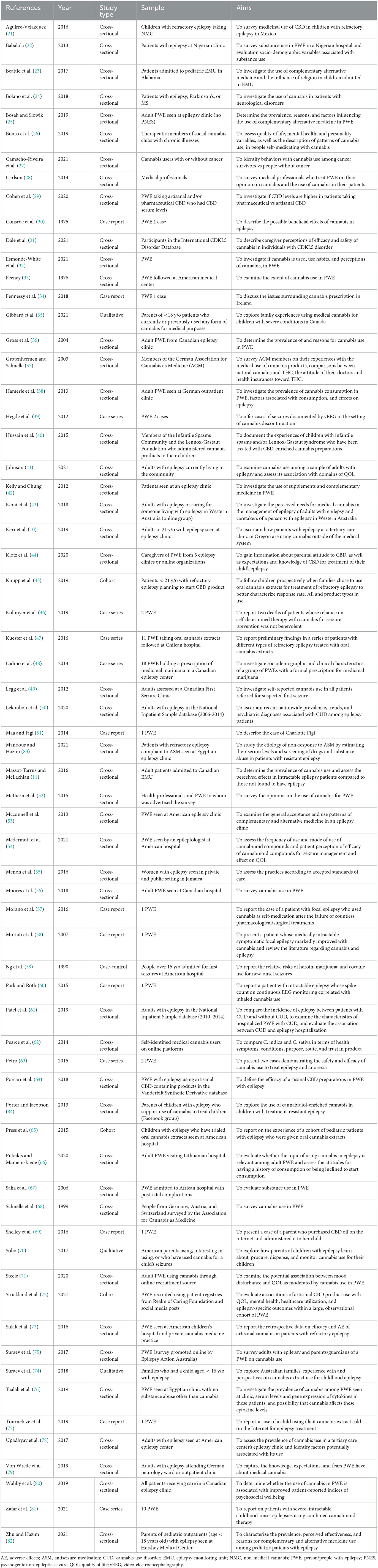
Table 1. Summary of the study types, samples, and aims of included studies.
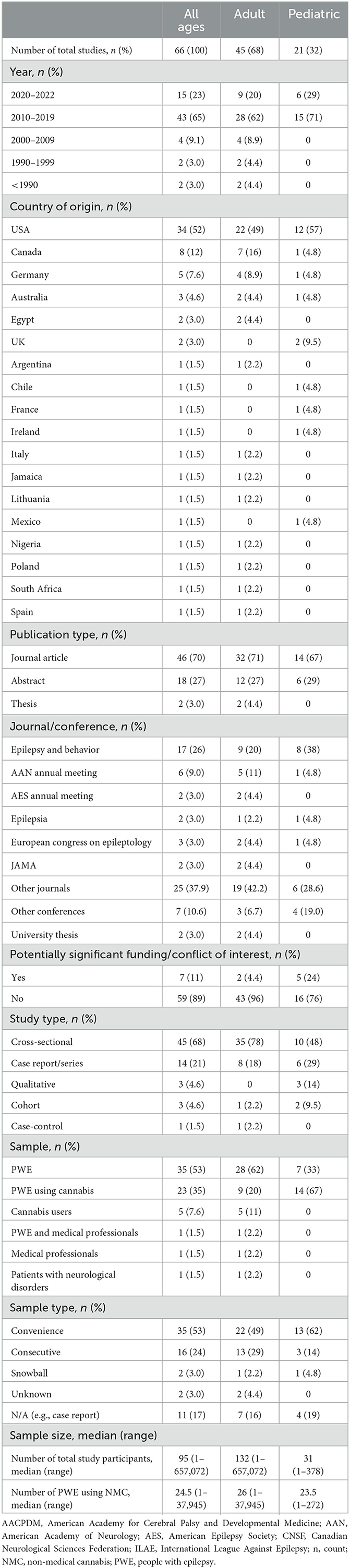
Table 2. Publication identification and study characteristics between adult and pediatric studies.
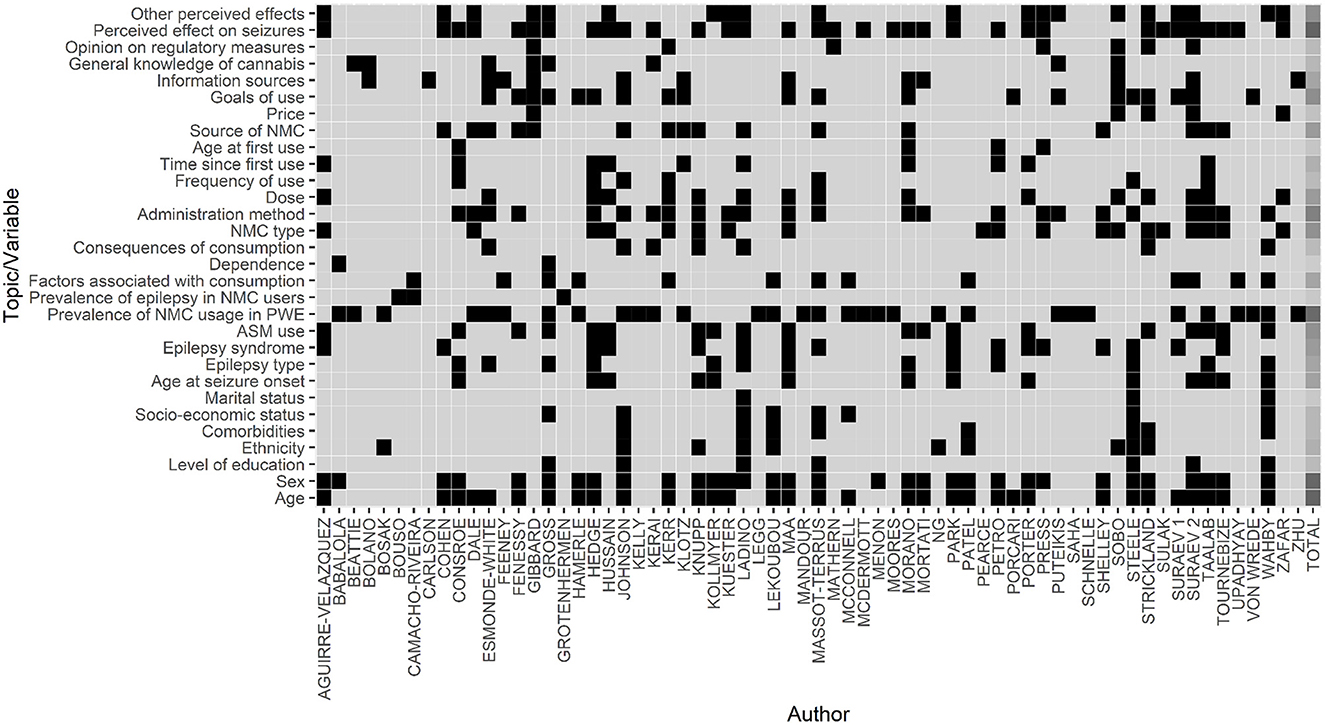
Figure 2. Heatmap of topics discussed in each included study. This figure consists of a heatmap summarizing which topics were discussed in each included study. The x-axis represents the studies that were included in this scoping review, as identified with the first author. The y-axis represents all the topics that we searched for in each study (see Section 2.4. Data extraction for more information). A black square at the junction between a study (x-axis) and a topic (y-axis) indicates that that topic was discussed in that study. A light gray square at that same junction would indicate that that topic was not discussed in that study. The last column represents the sum of the times each topic was discussed by all authors. In this last column, a square takes on a darker shade of gray as the topic is more “popular” (i.e., it was discussed in more publications). For instance, the perceived effect of seizures was a topic that was discussed in many studies, whereas the age at first use of cannabis was rarely discussed. ASM, anti-seizure medication; NMC, non-medical cannabis; PWE, people with epilepsy.
The following section is summarized in Table 1. Of the 66 included studies, 45 (68%) included only or mostly (i.e., >50%) adult participants (10, 11, 22, 24–28, 30, 32, 33, 36–39, 41–43, 46, 48–50, 52–63, 66–68, 71, 72, 75, 76, 78–80, 83), whereas 21 (32%) included only or mostly (i.e., >50%) pediatric participants (21, 23, 29, 31, 34, 35, 40, 44, 45, 47, 51, 64, 65, 69, 70, 73, 74, 77, 81, 82, 84). Most studies (88%), both adult and pediatric, were published after 2010 (10, 11, 21–29, 31, 32, 34, 35, 38–58, 60–66, 69–84). Most studies originated from the USA (52%) (10, 23, 27–31, 33, 39–42, 45, 46, 50–54, 58–65, 70–73, 78, 84), Canada (12%) (11, 21, 32, 36, 48, 49, 80), and Germany (7.6%) (21, 37, 38, 44, 68, 79). Most studies consisted in journal articles (68%) (10, 21, 23, 25–28, 30, 31, 33–40, 43–46, 48, 50–53, 57–59, 61, 62, 64–68, 70, 72–77, 79, 80, 84). The most popular journal was Epilepsy & Behavior, which published 17 (24%) studies in total (10, 11, 23, 25, 31, 39, 40, 44, 46, 53, 64, 65, 67, 72, 73, 75, 79, 84). Studies were most frequently cross-sectional (68%) (10, 11, 21–29, 31–33, 36–38, 40–44, 49, 50, 52–56, 61, 62, 64, 66–68, 71, 73, 75, 76, 78–80, 82–84) or case reports/series (21%) (30, 34, 39, 46–48, 51, 57, 58, 60, 63, 68, 77, 81). A few studies were qualitative (4.6%) (35, 70, 74) or longitudinal (6.1%) (45, 59, 65, 72). Most studies had samples consisting in PWE (71%) (10, 11, 21–23, 25, 30–34, 36, 38, 39, 41–44, 46, 49–51, 53–61, 63, 66, 67, 69, 70, 72, 74–83), though some specifically gathered samples of PWE who were known to use cannabis (17%) (29, 35, 40, 45, 47, 48, 64, 65, 71, 73, 84), and others gathered samples of cannabis consumers, searching for PWE among these consumers (7.6%) (26, 27, 37, 62, 68). Only non-random sampling methods were used; most frequently, convenience sampling (53%) (21, 24, 27, 29, 31–33, 35–37, 40, 41, 43–45, 48, 50, 52–55, 61, 62, 64, 67, 68, 71–75, 78, 81, 82, 84) was employed. The median sample size was 95 participants, but the range (1–657,072) was extremely wide due to the inclusion of case reports and two nationwide patient registry studies (50, 61). The median number of PWE using NMC was 24.5, once again with a very wide range (1–37,945) for the same reasons.
Among the 20 studies providing explicit information on the age of adult PWE using NMC, all studies presented mean ages between 18 and 40 years or focused primarily on this age group (10, 11, 30, 32, 36, 38, 39, 41, 46, 53, 57, 58, 60, 61, 63, 71, 72, 74, 76, 80). As for pediatric studies, reported mean ages varied between 3 years and 11 years (21, 29, 31, 34, 45, 47, 51, 64, 69, 74, 77, 84). Sex was relatively balanced among pediatric studies, though in 14 out of 21 adult studies, there were slightly-to-moderately male-predominant samples (22, 30, 38, 39, 48, 50, 57, 58, 60, 61, 63, 71, 76, 80). In the seven studies detailing level of education, three had adult samples with mostly high school levels of education (36, 48, 80), three had adult samples with mostly post-secondary education (11, 41, 71), and one had a pediatric sample with most children attending mainstream schooling or special education classes (74). Ethnicity was explored in ten studies, with nine of these studies having predominantly Caucasian samples (25, 41, 45, 48, 50, 61, 70–72). Comorbidities were detailed in only eight studies, all of which were predominantly adult studies that explored various psychiatric comorbidities (11, 41, 48, 50, 61, 71, 72, 80). Socio-economic standing was rarely explored, though when it was, the method by which it was presented was variable, with some studies detailing employment rates and others mentioning median household income (11, 36, 41, 48, 50, 53, 71, 80). Marital status was only explored in three studies, two of which had participants who were predominantly single (48, 80), and one of which had participants who were predominantly married (71).
Age at epilepsy onset was touched upon in 14 studies and was lower than 40 years in all but one case series (11, 30, 36, 39, 40, 45, 46, 51, 57, 60, 71, 74, 76, 77, 80, 84). Of the 13 studies reporting epilepsy type, four had samples with predominantly generalized-onset epilepsy (30, 32, 51, 60), and eight had samples with predominantly focal-onset epilepsy (36, 39, 48, 57, 63, 71, 76, 80). One other study consisted in a description of two cases, one of which had generalized-onset epilepsy and the other of which has focal-onset epilepsy (46). A total of 16 studies explored epilepsy syndromes; all nine pediatric studies had samples composed of children with epileptic encephalopathies though in variable proportions (21, 29, 40, 45, 51, 65, 69, 77, 84). The seven remaining adult studies detailed various epilepsy syndromes, such as idiopathic generalized epilepsy and temporal lobe epilepsy, without a clear pattern (11, 39, 48, 60, 63, 71, 75). One of these studies described psychogenic non-epileptic seizures in its sample (11). Use of ASMs was heterogeneously described in 19 studies, with some studies detailing the exact ASMs used, some indicating the proportion of PWE on polytherapy and monotherapy, and others specifying the number of failed ASM trials before NMC was begun (21, 30, 34, 36, 39, 40, 45, 46, 48, 51, 57, 58, 60, 72, 74, 76, 77, 80, 84). Given this heterogeneity, it was impossible to determine which ASMs were most frequently used. When the exact ASMs used were reported, these included phenytoin, phenobarbital, carbamazepine, zonisamide, levetiracetam, clobazam, topiramate, clonazepam, valproate, and vigabatrin (30, 39, 46, 51, 57, 58, 60, 77).
The lifetime prevalence of NMC use in PWE ranged between 0.69 and 76.8% and can be visualized in Figure 3. When studies provided prevalence estimates without clearly specifying what type of prevalence they were (i.e., lifetime vs. active), their prevalence estimates were presumed to be lifetime prevalence. The active prevalence of NMC use in PWE ranged between 3.19 and 57.7% and can be visualized in Supplementary Figure S1. Two studies reported prevalence of “cannabis use disorder,” which were categorized as forms of active prevalence (50, 61). The prevalence of epilepsy in cannabis consumers was detailed in three adult studies reporting 7.2, 5.1, and 2.1%, respectively (26, 27, 37). Thirteen studies evaluated factors that were independently associated with cannabis use in PWE (10, 11, 27, 33, 36, 38, 50, 53, 61, 74, 75, 78, 80). The factors that were most frequently reported were as follows: younger adult (10, 11, 33, 38, 50, 53, 61, 78), male sex (10, 11, 38, 50, 61, 78, 80), and lower level of education (11, 78, 80). Dependence was only detailed in two studies, which characterized 1.4 and 3% of their respective sample of PWE as being dependent on cannabis (22, 36). Consequences of NMC consumption on mental, physical, and social spheres were variably detailed in seven studies (32, 41, 43, 45, 48, 72, 80). Recurrent consequences included stigma (32, 43) and higher levels of depression (41, 80), though one study also reported lower levels of depression (72).

Figure 3. Lifetime prevalence of NMC use in PWE. This barchart presents the lifetime prevalence of NMC use in PWE for each publication for which this information was available. Gray bars represent prevalence calculated from adult samples, whereas orange bars represent prevalence calculated from pediatric samples. Confidence intervals are provided, as calculated using an α-error of 0.05.
A total of 19 studies presented information on the type of NMC consumed by PWE (10, 21, 31, 39, 40, 45, 47, 51, 62, 63, 65, 69, 70, 72–74, 77, 81). The 14 pediatric studies all reported predominantly CBD-based NMC (21, 31, 40, 45, 47, 51, 65, 69, 70, 72–74, 77, 81), whereas the five adult studies reported more mixed findings (10, 39, 62, 63, 76), with one study even reporting that up to 82.5% of its participants used NMC of unknown composition (76). As for NMC administration methods, in all nine pediatric studies, NMC was primarily taken orally (31, 34, 45, 47, 51, 65, 69, 74, 77), whereas in nine of the 15 adult studies, NMC was predominantly smoked (10, 11, 30, 39, 41, 48, 71, 76, 80). The 16 studies exploring NMC dosage presented their data in vastly different methods (e.g., mg/kg/day, g/day, weekly, per consumption), rendering direct comparisons between studies unachievable (10, 11, 21, 32, 39, 40, 45, 48, 51, 57, 70, 72, 74, 76, 81, 84). Seven adult studies detailed the frequency of NMC use; in these studies, participants mostly used NMC daily or at least multiple times per week (10, 11, 30, 39, 41, 71, 76). No data on the frequency of NMC use could be directly extractable from the pediatric studies. The time since the start of NMC consumption and the age at which NMC consumption began were rarely stated and, when stated, yielded varying results (21, 30, 39, 40, 44, 48, 57, 63, 65, 76). Sources of NMC acquisition were listed in 17 studies and included, to varying degrees, the following: medical/recreational dispensaries, online shops, street vendors, friends and family, pharmacies, and homegrown NMC (10, 11, 29, 31, 32, 34, 35, 41, 44, 45, 48, 57, 69, 75–77). Only five studies detailed the price of NMC acquisition; each price was presented in a different currency in different time periods, rendering comparisons between studies difficult due to inflation (35, 70, 72, 74, 81).
In the eight pediatric studies reporting on the goals of NMC consumption, seizure control was overwhelmingly the primary objective (34, 35, 44, 51, 64, 70, 74, 82). In contrast, in the 13 adult studies reporting on the goals of NMC consumption, seizure control and recreational use were both often cited as primary objectives (10, 11, 32, 36, 38, 39, 41, 57, 66, 71, 72, 75, 79). Across 11 studies, information sources for NMC were variable and included word-to-mouth, traditional/social media, and health professionals (24, 28, 32, 33, 35, 41, 44, 51, 57, 58, 70, 74). Variable proportions of participants discussed their NMC use with health professionals (24, 28, 32, 33, 41, 44, 51, 74). In half of studies exploring general knowledge of cannabis, participants had the general conception that NMC was more natural and/or safer than antiseizure medications (32, 35, 43, 66). Seven studies explored PWE's opinions on regulatory policies, but these opinions touched upon different aspects of NMC regulation and were too heterogeneous to be aptly summarized (10, 35, 52, 65, 70, 72, 74). Of the 33 studies detailing the perceived effects of NMC on seizures, 32 reported some beneficial effects on seizure control (10, 11, 21, 29–31, 34–36, 38–41, 45, 47, 48, 51, 54, 56–58, 60, 63, 65, 72–76, 78, 81, 84), whereas nine reported some detrimental effects on seizure control (11, 21, 29, 31, 38, 40, 65, 72, 74, 76). In only two of these nine studies did more participants perceive NMC to be detrimental than beneficial on seizure control (29, 38). As for other potential effects of NMC, ten studies reported varying rates of adverse effects, most commonly increased/decreased appetite, somnolence, various gastrointestinal symptoms, and irritability, (11, 21, 29, 31, 36, 40, 46, 65, 74, 84), whilst 14 studies mentioned various other benefits, such as improved mood, better sleep, lower levels of stress, and higher levels of alertness (11, 21, 31, 35, 36, 40, 47, 48, 65, 72, 74, 75, 81, 84).
In the last years, there has been a steady rise in interest in the use of cannabis in epilepsy, with many studies reporting that CBD extracts may provide beneficial effects for seizure control (2, 3). In several countries, medical, pharmaceutical-grade cannabis may be prescribed by health professionals for seizure control in specific populations of PWE (2). Notwithstanding, personal experience and anecdotal accounts support the notion that a significant portion of PWE acquire cannabis by other means and that many of these PWE use cannabis in the hopes that it may diminish their seizure frequency and severity. This phenomenon is compounded by the fact that recreational cannabis itself is also being legalized in many parts of the world, and cannabis may therefore be more easily accessible in these areas regardless of its medical or recreational use (2). In addition, where cannabis is still bought from illicit vendors, one may question the quality and components of these cannabis products, as their production and distribution are not standardized (85). In this scoping review, we summarized what is known in the literature about the use of NMC (i.e., cannabis not obtained by prescription nor through special access programs) in PWE, focusing primarily on the lived experience, habits, and beliefs of these people regarding NMC. In the following sections, we will further analyze the literature and highlight knowledge gaps that may benefit from more research.
The evidence surrounding NMC use in PWE can be characterized as somewhat sparse and heterogeneous, with studies presenting varying samples, diverse aims, mostly low sample sizes, and differing outcome measures. The literature can naturally be divided into studies with adult samples and those with pediatric samples. Few relevant studies were published before the year 2000 (30, 33, 58, 59, 67, 68); no relevant pediatric studies were published before 2010, which may reflect how interest in cannabis use in children is more recent than in adults. Western countries were predominantly represented in the literature (10, 11, 21, 23, 25–34, 36–46, 48–54, 58–66, 68–75, 77–81, 84), and very little is known about NMC use in PWE from African, Middle Eastern, Central/Southern American, and Asian countries. Efforts should be made to obtain more data on the subject from non-Western countries. Regarding sample size, only two studies, which were nationwide patient registry studies (that unfortunately shared to some extent the same sample), had sample sizes in the 100,000s (50, 61). Otherwise, two studies had sample sizes of ~900 (75, 83), and every other study had samples sized at < 500 individuals. Oftentimes, PWE who used NMC only consisted in a subset of the overall sample and were therefore in even lower numbers. The majority of studies were cross-sectional by design (10, 11, 21–29, 31–33, 36–38, 40–44, 49, 50, 52–56, 61, 62, 64, 66–68, 71, 73, 75, 76, 78–80, 82–84), with only a few qualitative or longitudinal studies (35, 45, 65, 70, 74). Although cross-sectional studies appear to be a quick, cost-efficient way of evaluating PWE's experience with NMC, they may also be plagued by significant selection biases and response biases, especially when considering that studies may have been conducted in locations or in time periods where/when cannabis use was more stigmatized. Longitudinal or qualitative studies may provide different types of information whilst subverting some of the biases inherent to cannabis surveys, and more studies using these designs should be performed.
In terms of demographics, there seems to be a male preponderance for NMC use in adults with epilepsy (10, 11, 22, 30, 38, 39, 48, 50, 57, 58, 60, 61, 63, 71, 76, 78, 80). Such a finding, if confirmed, would probably reflect a general preponderance that men have for cannabis use vs. women (86). There are also slightly more cases of epilepsy in men than in women (87). Similarly, several adult studies suggested that a younger age may be associated with cannabis use in epilepsy (10, 11, 33, 38, 50, 53, 61, 78), though this may once more reflect an association that is independent of epilepsy itself (88). Interestingly, there is no literature focusing specifically on NMC use in elderly PWE. This constitutes a major knowledge gap, especially given the high prevalence of epilepsy in the elderly and the effects of cannabis on cognition (89, 90). In addition, little is known about NMC use in non-Caucasian PWE, as almost all studies that reported their sample's ethnicity reported a Caucasian predominance (25, 41, 45, 48, 50, 61, 70–72). The education level, comorbidities, socio-economic standing, and marital status of PWE using NMC were rarely explored, though some studies suggested associations between cannabis use in PWE and lower levels of education (11, 78, 80), psychiatric comorbidities (61, 80), a lower socio-economic standing (50, 53), and being single (80). To confirm these associations would require larger, more robust epidemiological studies.
Regarding the age at seizure onset, the type of epilepsy (focal- vs. generalized-onset), and the epilepsy syndromes at play, these data should always be disclosed in future research, mostly for better between-study comparability. We note no pattern from the literature regarding these factors, other than the fact that pediatric studies often presented samples of individuals with epileptic encephalopathies (21, 29, 40, 45, 51, 65, 69, 77, 84). No study specifically mentioned if children with tuberous sclerosis complex were included. How NMC use in individuals with epileptic encephalopathies evolves through time and particularly through adulthood remains poorly understood. Finally, data on ASM use was heterogeneously reported; how many failed ASMs were used before NMC was begun, which ASMs are most often taken with NMC, and how does the use of other ASMs evolve once NMC is begun all remain open questions. More data on ASMs would also allow for a better evaluation of the proportion of people with pharmacoresistant vs. pharmacosensitive epilepsy using NMC.
The prevalence of NMC use in PWE was extremely variable and depended upon the study populations at hand and methodological factors. Most studies reported lifetime prevalence of NMC use in PWE grossly between 10 and 40% (25, 31, 33, 38, 43, 44, 49, 53, 54, 59, 66, 67, 75, 76, 78–80, 82). The two largest studies (with sample sizes several 100,000s larger than every other study) reported prevalence of NMC use in PWE of < 10%, though these were prevalence for “cannabis use disorder” in people hospitalized with epilepsy (50, 61). As a matter of fact, in many studies, the type of prevalence being reported (e.g., lifetime cannabis use, active cannabis use, cannabis use only after epilepsy diagnosis) was ambiguous. Future studies exploring the prevalence of NMC use in PWE should carefully distinguish the type of prevalence they are studying. Very few studies reported the prevalence of epilepsy in cannabis consumers, and this may represent an avenue for future research (26, 27, 37). The consequences of NMC use on mental, physical, and social spheres were rarely explored, though recurrent themes included feelings of being stigmatized (32, 43) and depressed mood (41, 80). Given the prevalence of mood disorders in PWE, how cannabis consumption interacts with this association would be important to clarify (91, 92). Interestingly, though some studies used self-reported outcome scales to measure mood and quality of life (41, 45, 71, 72, 80), no study has used formal neuropsychological tests to evaluate the impact of NMC on PWE. Measures of dependence were almost never addressed in the literature and would be important to evaluate in future studies.
The main type of NMC used varied between pediatric and adult studies; children appeared to mostly use oral CBD extracts (21, 31, 40, 45, 47, 51, 65, 69, 70, 72–74, 77, 81), whereas adults used NMC with various CBD-THC compositions (10, 39, 62, 63, 76). The route of administration in adults was also much more varied, although smoking seemed to be a recurrent, predominant route (10, 11, 30, 39, 41, 48, 71, 76, 80). This difference in NMC use between age groups can probably be explained by the fact that children used NMC primarily for seizure control (34, 35, 44, 51, 64, 70, 74, 82), whereas adults often used NMC for recreational purposes as well (10, 11, 32, 36, 38, 39, 41, 57, 66, 71, 75, 79). No clear correlation between NMC type, NMC administration route, and goals of consumption has been established yet, and this potential association could benefit from confirmatory studies. The sources of NMC acquisition included both legal and illicit routes and were highly variable (10, 11, 29, 32, 34, 35, 41, 44, 45, 48, 57, 69, 75–77). More research on the importance and implications of illicit cannabis vendors in PWE should be done, especially given the potential variability in the quality of the cannabis sold by these vendors (85). Information on NMC dosage, frequency of consumption, and pricing was sparse and heterogeneous. The age at which PWE began consuming NMC was rarely explored, representing another significant knowledge gap. In the case of PWE consuming NMC for seizure control, it would be interesting to investigate if they had a history of recreational cannabis use before beginning NMC for seizure control. Ultimately, more research will simply need to be conducted which systematically evaluates the habits of PWE regarding their NMC use. Care will need to be taken to present data in a manner that can be readily compared between studies.
PWE receive information on NMC from various sources, many non-medical. These sources included the internet, social media (e.g., Facebook), traditional media (e.g., TV broadcasts), and friends and family (24, 28, 32, 33, 35, 41, 44, 51, 57, 58, 70, 74). On a public health standpoint, further investigation of PWE's sources of information—especially social media where information may be largely unregulated (93)—may help design awareness campaigns and targeted knowledge sharing strategies. Many PWE did not disclose their NMC use to their physicians, yet the reasons why this occurred are not well-understood (24, 28, 32, 33, 41, 44, 51, 74). Feelings of stigma or of being unsupported by physicians have been cited as barriers to disclosure (32, 35). PWE's general knowledge of cannabis and opinions on regulatory policies were not often explored, though there did seem to be a conception that cannabis was more natural than ASMs (32, 35, 43, 66). The majority of PWE across all studies perceived that NMC aided in seizure control as well as in other domains, such as cognition, sleep, mood, and anxiety (10, 11, 21, 29–31, 34–36, 38–41, 45, 47, 48, 51, 54, 56–58, 60, 63, 65, 72–76, 78, 81, 84). On numerous occasions, being able to wean off other ASMs was cited as an extra benefit of NMC use (11, 21, 29, 31, 36, 40, 46, 65, 74, 84), which begs the question of what proportion of PWE perceive NMC as an add-on therapy rather than a replacement therapy and vice versa. The perceived benefits of NMC use were probably distorted by confirmation biases, and further research should be carried out to distinguish between the objective and subjective effects of NMC as well as to explore what factors could predict a greater bias.
This scoping review featured some limitations. Firstly, given the sheer scope of this study, decisions had to be made to not explore certain variables that may have been interesting to explore. For example, the concomitant/past use of ketogenic diet, vagus nerve stimulation, and epilepsy surgeries could have been searched for in this review. Likewise, though this scoping review focused exclusively on PWE who used NMC, other populations could have been studied. For example, in the screening phase of this review, many studies focusing on healthcare professionals' experience with PWE using NMC were excluded. A future review tackling this subset of studies could yield interesting findings. Secondly, certain variables, such as opinions on regulatory policies, were in hindsight a bit vague and yielded wide-ranging results. Separating these variables into sub-topics would perhaps have enhanced the between-study comparability at the expense of feasibility. Finally, some may argue that the inclusion of case reports/series as primary sources of evidence renders our final interpretations less robust; however, the inclusion of these studies also allowed for a more comprehensive portrayal of the literature.
In this scoping review, we summarized the body of literature surrounding NMC use in PWE, with emphasis on PWE's experience, habits, and beliefs concerning NMC. Overall, the literature can be summarized as heterogeneous and mostly populated by small, cross-sectional studies for which selection, participation, and confirmation biases are of concern. Though some topics are better explored than others, significant knowledge gaps exist throughout the literature and include (but are not limited to) the use of NMC in PWE from non-Western countries, the patterns of use of other ASMs in concomitance with NMC, NMC consumption in elderly PWE, the NMC consumption patterns of PWE (including the influence of illicit vendors), the barriers to the disclosure of NMC use to physicians, the comorbidities and characteristics of consumers vs. non-consumers, and the neuropsychological effects of NMC consumption in PWE. We hope our work may encourage researchers to address these gaps through high-quality research. We equally hope to encourage researchers to explore the landscape of NMC use in other neurological conditions, such as multiple sclerosis, Alzheimer's disease, and amyotrophic lateral sclerosis.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
JL: study design, data collection, data analysis, and drafting. CA: data collection and data analysis. DT: data collection and manuscript revision. DC and CD: manuscript revision. DJ-A and MK: study design and manuscript revision. DN: study design, manuscript revision, and principal investigator. All authors contributed to the article and approved the submitted version.
DJ-A reports research grants for investigator-initiated studies from government entities (Ministère de la Santé et des Services Sociaux du Québec, Health Canada, Canadian Institutes of Health Research, Fonds de Recherche Québec – Santé). DJ-A receives payment for expert testimony at the Ministère de la justice du Québec. DJ-A is a board member for Grand Chemin and the Mental Health Commission of Canada. DJ-A has received study materials for clinical trials from Cardiol Rx and Tetra Biopharma for clinical trials funded by the Quebec government. DJ-A's salary was supported by the Fonds de Recherche Québec—Santé. MK reports unrestricted educational grants from UCB and Eisai, research grants for investigator-initiated studies from UCB and Eisai as well as from government entities (Canadian Institutes of Health Research, Fonds de Recherche Québec—Santé), academic institutions (Centre Hospitalier de l'Université de Montréal), and foundations (TD Bank, TSC Alliance, Savoy Foundation, Quebec Bio-Imaging Network). MK's salary was supported by the Fonds de Recherche Québec—Santé. DN reports unrestricted educational grants from UCB, Eisai, Liva Nova, Pendopharm, Paladin Labs, and Sunovion; research grants for investigator-initiated studies from UCB and Eisai as well as from government entities (Canadian Institutes of Health Research, Fonds de Recherche Québec—Santé, Natural Sciences and Engineering Research Council), academic institutions (Centre Hospitalier de l'Université de Montréal), and foundations (TD Bank, Savoy Foundation, Quebec Bio-Imaging Network). DN's salary was supported by Canada Research Chair Program.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2023.1132106/full#supplementary-material
1. Breijyeh Z, Jubeh B, Bufo SA, Karaman R, Scrano L. Cannabis: a toxin-producing plant with potential therapeutic uses. Toxins. (2021) 13:117. doi: 10.3390/toxins13020117
2. Carter A. A North American history of cannabis use in the treatment of epilepsy. J Clin Neurophysiol. (2020) 37:35–8. doi: 10.1097/WNP.0000000000000644
3. Thomas RH, Cunningham MO. Cannabis and epilepsy. Pract Neurol. (2018) 18:465–71. doi: 10.1136/practneurol-2018-002058
4. Appendino JP, Boelman C, Brna PM, Burneo JG, Claassen CS, Connolly MB, et al. Position statement on the use of medical cannabis for the treatment of epilepsy in Canada. Can J Neurol Sci. (2019) 46:645–52. doi: 10.1017/cjn.2019.282
5. O'Connell BK, Gloss D, Devinsky O. Cannabinoids in treatment-resistant epilepsy: a review. Epilepsy Behav. (2017) 70(Pt B):341–8. doi: 10.1016/j.yebeh.2016.11.012
6. Devinsky O, Cross JH, Laux L, Marsh E, Miller I, Nabbout R, et al. Trial of cannabidiol for drug-resistant seizures in the dravet syndrome. N Engl J Med. (2017) 376:2011–20. doi: 10.1056/NEJMoa1611618
7. Devinsky O, Patel AD, Cross JH, Villanueva V, Wirrell EC, Privitera M, et al. Effect of cannabidiol on drop seizures in the lennox-gastaut syndrome. N Engl J Med. (2018) 378:1888–97. doi: 10.1056/NEJMoa1714631
8. Thiele EA, Marsh ED, French JA, Mazurkiewicz-Beldzinska M, Benbadis SR, Joshi C, et al. Cannabidiol in patients with seizures associated with lennox-gastaut syndrome (gwpcare4): a randomised, double-blind, placebo-controlled phase 3 trial. Lancet. (2018) 391:1085–96. doi: 10.1016/S0140-6736(18)30136-3
9. Thiele EA, Bebin EM, Bhathal H, Jansen FE, Kotulska K, Lawson JA, et al. Add-on cannabidiol treatment for drug-resistant seizures in tuberous sclerosis complex: a placebo-controlled randomized clinical trial. JAMA Neurol. (2021) 78:285–92. doi: 10.1001/jamaneurol.2020.4607
10. Kerr A, Walston V, Wong VS, Kellogg M, Ernst L. Marijuana use among patients with epilepsy at a tertiary care center. Epilepsy Behav. (2019) 97:144–8. doi: 10.1016/j.yebeh.2019.05.037
11. Massot-Tarrus A, McLachlan RS. Marijuana Use in adults admitted to a canadian epilepsy monitoring unit. Epilepsy Behav. (2016) 63:73–8. doi: 10.1016/j.yebeh.2016.08.002
12. Lowe DJE, Sasiadek JD, Coles AS, George TP. Cannabis and mental illness: a review. Eur Arch Psychiatry Clin Neurosci. (2019) 269:107–20. doi: 10.1007/s00406-018-0970-7
13. Tricco AC, Lillie E, Zarin W, O'Brien KK, Colquhoun H, Levac D, et al. Prisma extension for scoping reviews (Prisma-Scr): checklist and explanation. Ann Intern Med. (2018) 169:467–73. doi: 10.7326/M18-0850
14. Colquhoun HL, Levac D, O'Brien KK, Straus S, Tricco AC, Perrier L, et al. Scoping reviews: time for clarity in definition, methods, and reporting. J Clin Epidemiol. (2014) 67:1291–4. doi: 10.1016/j.jclinepi.2014.03.013
15. Peters MD, Godfrey CM, Khalil H, McInerney P, Parker D, Soares CB. Guidance for conducting systematic scoping reviews. Int J Evid Based Healthc. (2015) 13:141–6. doi: 10.1097/XEB.0000000000000050
16. Levac D, Colquhoun H, O'Brien KK. Scoping studies: advancing the methodology. Implement Sci. (2010) 5:69. doi: 10.1186/1748-5908-5-69
17. Bramer WM, Rethlefsen ML, Kleijnen J, Franco OH. Optimal database combinations for literature searches in systematic reviews: a prospective exploratory study. Syst Rev. (2017) 6:245. doi: 10.1186/s13643-017-0644-y
18. Bui KA, Abdaem J, Muccilli A, Gore GC, Keezer MR. Improving the quality of systematic reviews of neurological conditions: an assessment of current practice and the development and validation of six new search strategies. Eur J Neurol. (2018) 25:1477–85. doi: 10.1111/ene.13758
19. Filippini G, Minozzi S, Borrelli F, Cinquini M, Dwan K. Cannabis and cannabinoids for symptomatic treatment for people with multiple sclerosis. Cochrane Database Syst Rev .(2022) 5:CD013444. doi: 10.1002/14651858.CD013444.pub2
20. Braun V, Clarke V. Reflecting on reflexive thematic analysis. Qualit Res Sport Exerc Health .(2019) 11:589–97. doi: 10.1080/2159676X.2019.1628806
21. Aguirre-Velazquez CG. Report from a survey of parents regarding the use of cannabidiol (medicinal cannabis) in Mexican children with refractory epilepsy. Neurol Res Int. (2017) 2017:2985729. doi: 10.1155/2017/2985729
22. Babalola EO. Pattern of psychoactive substance use among people living with epilepsy in southwestern Nigeria. Epilepsia. (2014) 2:160. doi: 10.5455/jbh.20130921013013
23. Beattie JF, Thompson MD, Parks PH, Jacobs RQ, Goyal M. Caregiver-reported religious beliefs and complementary and alternative medicine use among children admitted to an epilepsy monitoring unit. Epilepsy Behav. (2017) 69:139–46. doi: 10.1016/j.yebeh.2017.01.026
24. Bolano C, Vazquez G, Couto B, Claverie CS, Thomson A. What do we think patients know about cannabis in neurological diseases? In: Neurology Conference: 70th Annual Meeting of the American Academy of Neurology, AAN. Los Angeles, CA (2018). Vol. 90(15 Suppl. 1).
25. Bosak M, Slowik A. Use of complementary and alternative medicine among adults with epilepsy in a university epilepsy clinic in Poland. Epilepsy Behav. (2019) 98(Pt A):40–4. doi: 10.1016/j.yebeh.2019.06.004
26. Bouso JC, Jimenez-Garrido D, Ona G, Woznica D, Dos Santos RG, Hallak JEC, et al. Quality of life, mental health, personality and patterns of use in self-medicated cannabis users with chronic diseases: a 12-month longitudinal study. Phytother Res. (2020) 34:1670–7. doi: 10.1002/ptr.6639
27. Camacho-Rivera M, Islam JY, Rodriguez DL, Vidot DC. Cannabis use among cancer survivors amid the Covid-19 pandemic: results from the Covid-19 cannabis health study. Cancers. (2021) 13:3495. doi: 10.3390/cancers13143495
28. Carlson C. Cbd and Marijuana: Q-pulse survey. Epilepsy Curr. (2014) 14:291–6. doi: 10.5698/1535-7597-14.5.291
29. Cohen N, Conry J, Schreiber J. Keep off the grass: artisanal versus pharmaceutical cannabidiol in pediatric refractory epilepsy patients. In: Neurology Conference: 72nd Annual Meeting of the American Academy of Neurology, AAN. Wolters Kluwer (2020). Vol. 94(15 Suppl.).
30. Consroe PF, Wood GC, Buchsbaum H. Anticonvulsant nature of marihuana smoking. JAMA. (1975) 234:306–7. doi: 10.1001/jama.234.3.306
31. Dale T, Downs J, Wong K, Leonard H. The perceived effects of cannabis products in the management of seizures in Cdkl5 deficiency disorder. Epilepsy Behav. (2021) 122:108152. doi: 10.1016/j.yebeh.2021.108152
32. Esmonde-White C, Arts J, Marti AS. Marijuana use in individuals with epilepsy post-legalization in Canada. Epilepsia. (2021) 62(Suppl. 3):167. doi: 10.1111/epi.17079
33. Feeney DM. Marihuana Use among epileptics. JAMA. (1976) 235:1105. doi: 10.1001/jama.1976.03260370015003
34. Fennessy P, Murphy L, Crowe S. Cannabis oil in an irish children's critical care unit. Ir Med J. (2018) 111:807.
35. Gibbard M, Mount D, Rassekh SR, Siden HH. Family attitudes about and experiences with medical cannabis in children with cancer or epilepsy: an exploratory qualitative study. CMAJ Open. (2021) 9:E563–9. doi: 10.9778/cmajo.20200212
36. Gross DW, Hamm J, Ashworth NL, Quigley D. Marijuana use and epilepsy: prevalence in patients of a tertiary care epilepsy center. Neurology. (2004) 62:2095–7. doi: 10.1212/01.WNL.0000127623.03766.75
37. Grotenhermen F, Schnelle M. Survey on the medical use of cannabis and Thc in Germany. J Cannabis Ther. (2003) 3:17–40. doi: 10.1300/J175v03n02_03
38. Hamerle M, Ghaeni L, Kowski A, Weissinger F, Holtkamp M. Cannabis and other illicit drug use in epilepsy patients. Eur J Neurol. (2014) 21:167–70. doi: 10.1111/ene.12081
39. Hegde M, Santos-Sanchez C, Hess CP, Kabir AA, Garcia PA. Seizure exacerbation in two patients with focal epilepsy following marijuana cessation. Epilepsy Behav. (2012) 25:563–6. doi: 10.1016/j.yebeh.2012.09.024
40. Hussain SA, Zhou R, Jacobson C, Weng J, Cheng E, Lay J, et al. Perceived efficacy of cannabidiol-enriched cannabis extracts for treatment of pediatric epilepsy: a potential role for infantile spasms and lennox-gastaut syndrome. Epilepsy Behav. (2015) 47:138–41. doi: 10.1016/j.yebeh.2015.04.009
41. Johnson K. Understanding Marijuana use as a treatment option for people with epilepsy: use, attitudes, and quality of life. Dissert Abstracts Int Sect B Sci Eng. (2022) 83:1–107.
42. Kelly KM, Chung SS. The use of supplements and complementary medicine in patients with epilepsy. Epilepsy Curr. (2013) 1:111.
43. Kerai A, Sim TF, Emmerton L. Medical cannabis: a needs analysis for people with epilepsy. Complement Ther Clin Pract. (2018) 33:43–8. doi: 10.1016/j.ctcp.2018.08.003
44. Klotz KA, Schonberger J, Nakamura L, San Antonio-Arce V, Bast T, Wiemer-Kruel A, et al. Expectations and knowledge of cannabidiol therapy for childhood epilepsy - a German caregiver survey. Epilepsy Behav. (2020) 111:107268. doi: 10.1016/j.yebeh.2020.107268
45. Knupp KG, Rice JD, Helmkamp LJ, Galinkin J, Sempio C, Jost K, et al. Prospective evaluation of oral cannabis extracts in children with epilepsy. Seizure. (2019) 72:23–7. doi: 10.1016/j.seizure.2019.09.007
46. Kollmyer DM, Wright KE, Warner NM, Doherty MJ. Are there mortality risks for patients with epilepsy who use cannabis treatments as monotherapy? Epilepsy Behav Case Rep. (2019) 11:52–3. doi: 10.1016/j.ebcr.2018.11.007
47. Kuester G, Gazmuri AM, Ahumada A, Bobadilla P. Clinical response to oral cannabis extracts in severe refractory epilepsy: preliminary experience in Chilean patients. Epilepsia. (2016) 57(Suppl. 2):147–8. doi: 10.1111/epi.13609
48. Ladino LD, Hernandez-Ronquillo L, Tellez-Zenteno JF. Medicinal marijuana for epilepsy: a case series study. Can J Neurol Sci. (2014) 41:753–8. doi: 10.1017/cjn.2014.37
49. Legg K, Crocker CE, Moeller JJ, Pohlmann-Eden B. Marijuana use in first seizure patients: the halifax adult first seizure clinic experience. Epilepsy Curr. (2013) 1:220.
50. Lekoubou A, Fox J, Bishu KG, Ovbiagele B. Trends in documented cannabis use disorder among hospitalized adult epilepsy patients in the United States. Epilepsy Res. (2020) 163:106341. doi: 10.1016/j.eplepsyres.2020.106341
51. Maa E, Figi P. The case for medical marijuana in epilepsy. Epilepsia. (2014) 55:783–6. doi: 10.1111/epi.12610
52. Mathern GW, Beninsig L, Nehlig A. Fewer specialists support using medical marijuana and cbd in treating epilepsy patients compared with other medical professionals and patients: result of epilepsia's survey. Epilepsia. (2015) 56:1–6. doi: 10.1111/epi.12843
53. McConnell BV, Applegate M, Keniston A, Kluger B, Maa EH. Use of complementary and alternative medicine in an urban county hospital epilepsy clinic. Epilepsy Behav. (2014) 34:73–6. doi: 10.1016/j.yebeh.2014.03.011
54. McDermott D, Fetrow K, Biesecker K, Coulter I, Thompson J. Investigation of the differential impact of cannabinoid compounds on seizure frequency and quality of life in patients with epilepsy. In: Neurology Conference: 73rd Annual Meeting of the American Academy of Neurology, AAN. Wolters Kluwer (2021). Vol. 96(15 SUPPL. 1).
55. Menon U, Williams M, Grindley T, Morgan O, Ali A. Womenand epilepsy: a review of practices in the public and private setting in Jamaica, 2012–2015. Epilepsia. (2016) 57(Suppl. 2):70.
56. Moores G, Lockey A, Attar A. High times? Prevalence and perceptions of marijuana use among patients with epilepsy. Can J Neurol Sci. (2018) 45(Suppl. 2):S10. doi: 10.1017/cjn.2018.121
57. Morano A, Cifelli P, Nencini P, Antonilli L, Fattouch J, Ruffolo G, et al. Cannabis in epilepsy: from clinical practice to basic research focusing on the possible role of Cannabidivarin. Epilepsia Open. (2016) 1:145–51. doi: 10.1002/epi4.12015
58. Mortati K, Dworetzky B, Devinsky O. Marijuana: an effective antiepileptic treatment in partial epilepsy? A case report and review of the literature. Rev. (2007) 4:103–6.
59. Ng SK, Brust JC, Hauser WA, Susser M. Illicit drug use and the risk of new-onset seizures. Am J Epidemiol. (1990) 132:47–57. doi: 10.1093/oxfordjournals.aje.a115642
60. Park H, Roth J. Impact of inhaled marijuana on ceeg spike count in a 33-year-old man with idiopathic epilepsy: a case report. In: Neurology Conference: 67th American Academy of Neurology Annual Meeting, AAN. Washington, DC: Wolters Kluwer (2015). Vol. 84(SUPPL. 14).
61. Patel RS, Mekala HM, Tankersley WE. Cannabis use disorder and epilepsy: a cross-national analysis of 657 072 hospitalized patients. Am J Addict. (2019) 28:353–60. doi: 10.1111/ajad.12898
62. Pearce DD, Mitsouras K, Irizarry KJ. Discriminating the effects of cannabis sativa and cannabis indica: a web survey of medical cannabis users. J Altern Complement Med. (2014) 20:787–91. doi: 10.1089/acm.2013.0190
63. Petro D. Cannabis use in epilepsy and anorexia-two “N-of-One” trials. In: Neurology Conference: 67th American Academy of Neurology Annual Meeting, AAN. Washington, DC: Wolters Kluwer (2015). Vol. 84(SUPPL. 14).
64. Porcari GS, Fu C, Doll ED, Carter EG, Carson RP. Efficacy of artisanal preparations of cannabidiol for the treatment of epilepsy: practical experiences in a tertiary medical center. Epilepsy Behav. (2018) 80:240–6. doi: 10.1016/j.yebeh.2018.01.026
65. Press CA, Knupp KG, Chapman KE. Parental reporting of response to oral cannabis extracts for treatment of refractory epilepsy. Epilepsy Behav. (2015) 45:49–52. doi: 10.1016/j.yebeh.2015.02.043
66. Puteikis K, Mameniskiene R. Use of cannabis and its products among patients in a tertiary epilepsy center: a cross-sectional survey. Epilepsy Behav. (2020) 111:107214. doi: 10.1016/j.yebeh.2020.107214
67. Saha SK, Nel M, Prinsloo EA. Profile and associated factors for re-admitted epileptic patients with complications in a South African Hospital. Cent Afr J Med. (2006) 52:35–8.
68. Schnelle M, Grotenhermen F, Reif M, Gorter RW. [Results of a standardized survey on the medical use of cannabis products in the german-speaking area]. Forsch Komplementarmed. (1999) 6(Suppl. 3):28–36. doi: 10.1159/000057154
69. Shelley K, Wright S, Wyton S, Concannon B, Agrawal S, Philip S, et al. When the drugs don't work. Dev Med Child Neurol. (2016) 58(Suppl. 1):44. doi: 10.1111/dmcn.12998
70. Sobo EJ. Parent use of cannabis for intractable pediatric epilepsy: everyday empiricism and the boundaries of scientific medicine. Soc Sci Med. (2017) 190:190–8. doi: 10.1016/j.socscimed.2017.08.003
71. Steele KL. Exploring mood and quality of life of people with epilepsy who use cannabis: is more cannabis use related to better outcome? DissertAbstracts Int Sect B Sci Eng. (2021) 82:1–110.
72. Strickland JC, Jackson H, Schlienz NJ, Salpekar JA, Martin EL, Munson J, et al. Cross-sectional and longitudinal evaluation of cannabidiol (Cbd) product use and health among people with epilepsy. Epilepsy Behav. (2021) 122:108205. doi: 10.1016/j.yebeh.2021.108205
73. Sulak D, Saneto R, Goldstein B. The current status of artisanal cannabis for the treatment of epilepsy in the United States. Epilepsy Behav. (2017) 70(Pt B):328–33. doi: 10.1016/j.yebeh.2016.12.032
74. Suraev A, Lintzeris N, Stuart J, Kevin RC, Blackburn R, Richards E, et al. Composition and use of cannabis extracts for childhood epilepsy in the Australian community. Sci Rep. (2018) 8:10154. doi: 10.1038/s41598-018-28127-0
75. Suraev AS, Todd L, Bowen MT, Allsop DJ, McGregor IS, Ireland C, et al. An Australian nationwide survey on medicinal cannabis use for epilepsy: history of antiepileptic drug treatment predicts medicinal cannabis use. Epilepsy Behav. (2017) 70(Pt B):334–40. doi: 10.1016/j.yebeh.2017.02.005
76. Taalab YM, Mohammed WF, Helmy MA, Othman AAA, Darwish M, Hassan I, et al. Cannabis influences the putative cytokines-related pathway of epilepsy among egyptian epileptic patients. Brain Sci. (2019) 9:332. doi: 10.3390/brainsci9120332
77. Tournebize J, Gibaja V, Fresse A, Dautriche A, Verney C, Goirand F, et al. Use of cannabis extracts sold on the internet for child epilepsy: a case report in France. Fund Clin Pharmacol. (2019) 33(Suppl. 1):87. doi: 10.1111/fcp.12470
78. Upadhyay R, Ouyang B, McNulty M. Majority of epileptic marijuana users perceive decreased seizure frequency. In: Neurology Conference: 69th American Academy of Neurology Annual Meeting, AAN. Boston, MA: Wolters Kluwer (2017). Vol. 88(16 Suppl. 1).
79. von Wrede R, Moskau-Hartmann S, Amarell N, Elger CE, Helmstaedter C. Knowledge, expectations and fears of cannabis use of epilepsy patients at a tertiary epilepsy center. Epilepsy Behav. (2019) 99:106458. doi: 10.1016/j.yebeh.2019.106458
80. Wahby S, Karnik V, Brobbey A, Wiebe S, Sajobi T, Josephson CB. Cannabis use is both independently associated with and mediates worse psychosocial health in patients with epilepsy. J Neurol Neurosurg Psychiatry. (2019) 90:945–51. doi: 10.1136/jnnp-2018-319780
81. Zafar R, Schlag A, Nutt D. Ending the pain of children with severe epilepsy? an audit of the impact of medical cannabis in 10 patients. Brain Neurosci Adv. (2021) 5:200–1. doi: 10.1177/2050324520974487
82. Zhu Z, Mittal R, Walser SA, Lehman E, Kumar A, Paudel S, et al. Complementary and alternative medicine (Cam) use in children with epilepsy. J Child Neurol. (2022) 37:334–9. doi: 10.1177/08830738211069790
83. Mandour R, Hazim M. Drug and substance abuse in refractory epilepsy. J Neurol Sci. (2021) 83:169. doi: 10.1016/j.jns.2021.119185
84. Porter BE, Jacobson C. Report of a parent survey of cannabidiol-enriched cannabis use in pediatric treatment-resistant epilepsy. Epilepsy Behav. (2013) 29:574–7. doi: 10.1016/j.yebeh.2013.08.037
85. Botelho D, Boudreau A, Rackov A, Rehman A, Phillips B, Hay C, et al. Analysis of Illicit and Legal Cannabis Products for a Suite of Chemical and Microbial Contaminants. Canada: New Brunswick Research and Productivity Council (2021).
86. Cuttler C, Mischley LK, Sexton M. Sex differences in cannabis use and effects: a cross-sectional survey of cannabis users. Cannabis Cannabinoid Res. (2016) 1:166–75. doi: 10.1089/can.2016.0010
87. McHugh JC, Delanty N. Epidemiology and classification of epilepsy: gender comparisons. Int Rev Neurobiol. (2008) 83:11–26. doi: 10.1016/S0074-7742(08)00002-0
88. Mauro PM, Carliner H, Brown QL, Hasin DS, Shmulewitz D, Rahim-Juwel R, et al. Age differences in daily and nondaily cannabis use in the United States, 2002–2014. J Stud Alcohol Drugs. (2018) 79:423–31. doi: 10.15288/jsad.2018.79.423
89. Sen A, Jette N, Husain M, Sander JW. Epilepsy in older people. Lancet. (2020) 395:735–48. doi: 10.1016/S0140-6736(19)33064-8
90. Curran HV, Freeman TP, Mokrysz C, Lewis DA, Morgan CJ, Parsons LH. Keep off the grass? Cannabis, cognition and addiction. Nat Rev Neurosci. (2016) 17:293–306. doi: 10.1038/nrn.2016.28
91. Fiest KM, Dykeman J, Patten SB, Wiebe S, Kaplan GG, Maxwell CJ, et al. Depression in epilepsy: a systematic review and meta-analysis. Neurology. (2013) 80:590–9. doi: 10.1212/WNL.0b013e31827b1ae0
92. Li J, Ledoux-Hutchinson L, Toffa DH. Prevalence of bipolar symptoms or disorder in epilepsy: a systematic review and meta-analysis. Neurology. (2022). doi: 10.1212/WNL.0000000000200186
Keywords: cannabis (marijuana), seizure, epilepsy, tetrahydrocannabinol (THC), cannabidiol (CBD), scoping review
Citation: Li J, Areal CC, Toffa DH, Citherlet D, Deacon C, Jutras-Aswad D, Keezer MR and Nguyen DK (2023) Use of non-medical cannabis in epilepsy: A scoping review. Front. Neurol. 14:1132106. doi: 10.3389/fneur.2023.1132106
Received: 26 December 2022; Accepted: 13 February 2023;
Published: 06 March 2023.
Edited by:
Miguel A. Pozo García, Faculty of Medicine (UCM), SpainReviewed by:
Barbara Mostacci, IRCCS Institute of Neurological Sciences of Bologna (ISNB), ItalyCopyright © 2023 Li, Areal, Toffa, Citherlet, Deacon, Jutras-Aswad, Keezer and Nguyen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jimmy Li, amltbXkubGlAdW1vbnRyZWFsLmNh
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.