
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurol., 21 April 2023
Sec. Headache and Neurogenic Pain
Volume 14 - 2023 | https://doi.org/10.3389/fneur.2023.1128953
This article is part of the Research TopicCognitive Schemas in Primary Headache DisordersView all 6 articles
 Gülen Güler Aksu1*
Gülen Güler Aksu1* Ozan Kayar2
Ozan Kayar2 Ali Evren Tufan3
Ali Evren Tufan3 Meryem Özlem Kütük4
Meryem Özlem Kütük4 Ayşe Nur Özdağ Acarli5Damla Hazal Sucu6
Ayşe Nur Özdağ Acarli5Damla Hazal Sucu6 Bahar Taşdelen6
Bahar Taşdelen6 Fevziye Toros1
Fevziye Toros1 Aynur Özge7
Aynur Özge7Introduction: Psychotherapies, such as schema therapy, are receiving increasing attention in the management of pediatric headaches. The purpose of this study was to investigate early maladaptive schemas (EMSs) in adolescents with episodic migraine (EM) and chronic migraine (CM).
Methods: This clinic-based, cross-sectional study consisted of 167 adolescents, aged 12–18, who were diagnosed with EM (n = 140) and CM (n = 27). The clinical characteristics of migraine, its accompanying symptoms, EMSs, the interrelationship of EMSs, depression, and anxiety were evaluated. We specifically analyzed psychopathology and abuse history as covariates in this study.
Results: Defectiveness/shame, mistrust/abuse, abandonment/instability, enmeshment/undeveloped self, self-sacrifice, and subjugation schemas were more prevalent in the CM group. In terms of schema domains, the CM group scored significantly higher in disconnection/rejection and other orientations. Psychopathology did not affect the EMS scores, but a history of sexual abuse did. In patients with EM, a relationship was found between the variables of anxiety, depression, and five of the EMS domains. On the other hand, the CM group showed a significant relationship with anxiety, hypervigilance/inhibition, disconnection/rejection, and other orientation domains.
Discussion: This study highlights the value of EMSs, anxiety, and depression in young people with EM and CM. Schema therapy and schema-based therapeutic interventions should be researched, especially in pediatric migraine, as they may potentially prevent the progression to treatment-resistant migraine.
Episodic migraine (EM) and chronic migraine (CM) are two distinct clinical entities in terms of clinical, epidemiologic, sociodemographic, and comorbidity characteristics. Although CM is less common, it is far more debilitating and associated with a reduced quality of life (1), a higher rate of psychiatric and medical comorbidities (2), and an increased economic burden (3) than EM. EM progresses to CM at a rate of 2.5% per year (4). Age, gender, family history of headaches, increased headache frequency, acute medication overuse, obesity, caffeine, and psychopathologies are well-known risk factors for the development of CM (1–3). Psychiatric disorders have a close and complex relationship with headaches, based on a neurobiological and genomic background (5, 6). Anxiety, depression (5), cognitive structures (7, 8), personality traits (9), and coping styles (10) are some of the related psychological factors. Psychological stress and psychopathology may lead to the onset of headaches, the worsening of headache episodes, and the acceleration of headache chronicity (1, 3, 4, 11). However, there are still no clear data on how psychiatric disorders lead to worsening headache episodes or treatment-resistant and treatment-refractory migraine.
Beck emphasized maladaptive schemas, which are basic beliefs about the self, others, and the world (called cognitive schemas), that may lead to vulnerability to psychopathology (7). Young modified and updated Beck's cognitive model to identify different schemas (7, 12). In Young's model, early maladaptive schemas (EMSs) are significantly dysfunctional patterns of beliefs about oneself and one's interactions with others that develop during childhood and are elaborated throughout one's lifetime (12, 13). EMSs are present in all individuals with some degree of certain psychological flexibility but are more extreme and rigid in the presence of psychopathology (12–14). Childhood experiences such as trauma, neglect, abuse, and psychological stress are associated with the development of EMSs (12–14). The connection between EMSs and psychopathology in children and adolescents is less clear. The concept of EMS is still developing and may be fluid at this time (14). Thus, understanding the relationship between EMS, psychopathology, and migraine in the early years of life is crucial.
EMSs may be one of the overlooked underlying core factors in patients with headaches. Accordingly, a quick and accurate diagnosis of migraine in childhood and its contributing factors may help prevent the development of CM in adolescence and later in life (15). The study of EMSs in pediatric migraine seems to be essential. In this way, the progression to resistant migraine may be prevented by improving new and comprehensive treatment modalities, such as psychotherapies. Therefore, we aimed to investigate the following: the headache characteristics of youths with migraine, EMSs in youths with EM and CM, and the relationship between schema domains, anxiety, and depression scores in youths with EM and CM.
This clinic-based, cross-sectional study was conducted as part of an ongoing Turkish Child and Adolescent Headache Database Project conducted by the Department of Child and Adolescent Psychiatry and Neurology at the Faculty of Medicine at Mersin University. This project included the data of patients with headaches who were admitted to the aforementioned Department of Child and Adolescent Psychiatry from 1 January 2004 to 1 April 2021. The inclusion criteria of the study were adolescents aged between 12 and 18 years of age, who were diagnosed with migraine according to the criteria of the International Classification of Headache Disorders, 3rd Edition (ICHD-3), (16) who presented to the center where the study was conducted between 1 November 2013 and 1 April 2021. The patients with organic mental disorders, psychotic disorders, intellectual disabilities, alcohol and substance abuse, symptoms of personality disorders, vision and hearing loss, a history of severe (with loss of consciousness) or recurrent head trauma in the past month, other headache types (e.g., tensiontype headache, secondary headache), with neurological and physical conditions, and the patients with missing data were excluded.
This form was developed by the researchers and included questions about the patient's age, gender, socioeconomic status, parental education level, family structure, marital status, parental psychiatric disorders, and history of abuse.
The questionnaire was developed and partially validated by Ozge et al. to gather data on age, gender, education level, family history of headaches, and headache characteristics (17). The form was administered to the patients by a neurologist (AO), who also performed a thorough neurologic examination and a family interview, if necessary.
The CDI was developed by Kovacs to evaluate depressive symptoms in children between the ages of 6 and 17. It consists of a 27-item scale, and each item is scored between 0 and 2. It has a cutoff score of 19 and a maximum score of 54 (18).
SCARED is used to evaluate anxiety symptoms in children and consists of 41 items. It is a self-report on a 3-point Likert-type scale with scores ranging from 0 to 2 (0: not true or seldom true, 1: somewhat true or occasionally true, and 2: very true or frequently true) (19).
This scale was developed to evaluate EMSs in Turkish children between the ages of 10 and 16 (20). It is a self-report on a 5-point Likert scale with response options for each item ranging from 1 (completely disagree) to 5 (completely agree). The set consists of five schema domains, 97 items, and 15 EMSs. The 15 EMSs and the five schema domains are shown in Figure 1 (20).
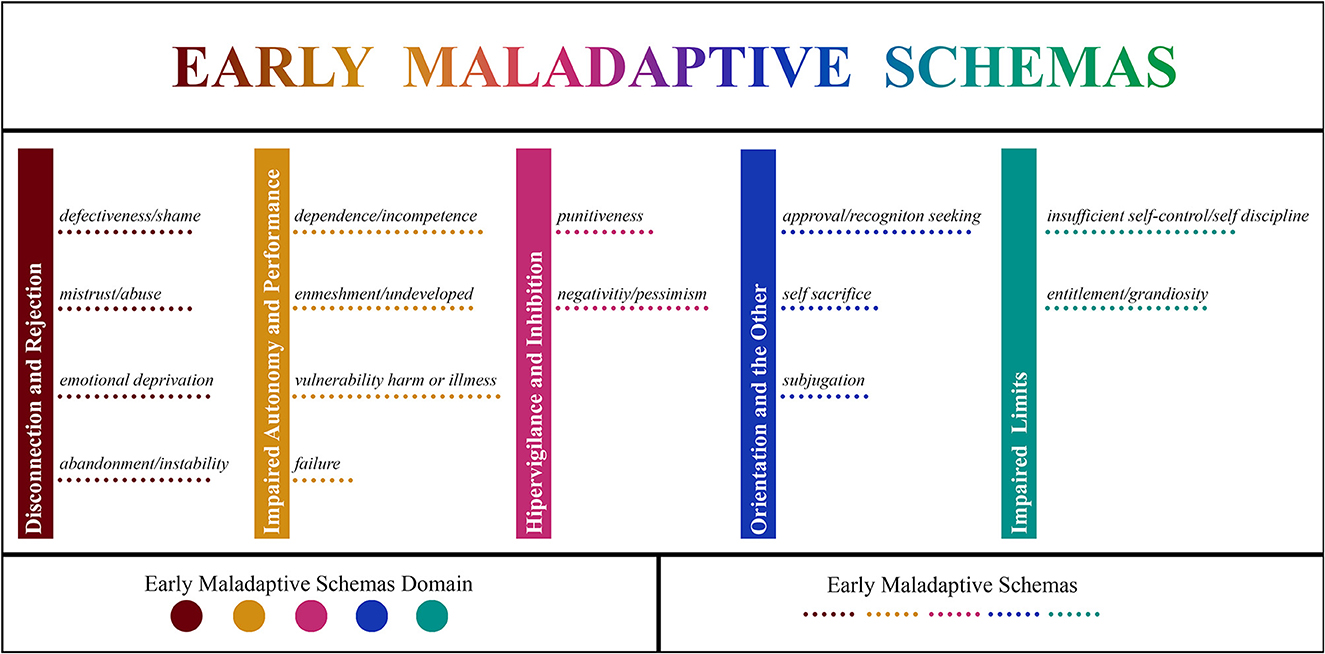
Figure 1. Illustration of 15 early maladaptive schemas and five schema domains consisting of disconnection and rejection, impaired autonomy and performance, hypervigilance and inhibition, impaired limits, and orientation to the others.
A neurological examination was performed for each patient, and the ICHD-3 criteria (16) were used for the classification of headache types. Psychiatric diagnoses were assessed based on unstructured clinical interviews using the diagnostic criteria of the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) (21). Adolescents were asked to complete all paper questionnaires independently in the waiting room of the outpatient clinic. All questionnaires were completed within 25–30 min. Sociodemographic characteristics, clinical characteristics, and accompanying symptoms of migraine and EMSs were analyzed. Furthermore, psychopathology and trauma history were also controlled in the subjects because they might influence the EMSs.
The study was conducted according to the principles of the Declaration of Helsinki and local laws and regulations. Institutional Research Board approval was obtained from the Faculty of Medicine at Mersin University (Number: E-78017789-050.01.04-1659432 Date: 26/05/2021).
The collected information was entered into a database prepared using SPSS version 23.0 (IBM Inc., Armonk, NY). The SPSS 23.0 and JAMOVI 2.0 software packages (the Jamovi project, 2021; https://www.jamovi.org) were used for analyses. Nominal variables were summarized as counts and frequencies, and quantitative data were summarized as either means and standard deviations or medians and interquartile ranges (IQRs), depending on the assumptions of normality. Bivariate comparisons of nominal variables were conducted using the chi-squared test with Yates' and Fisher's exact tests when appropriate. Quantitative variables were compared between groups using the Student's t-test for independent groups or the Mann-Whitney U-test. Schema domains and self-reported depression and anxiety symptoms between youths with EM and CM were compared using MANOVA followed by ANOVA. A history of sexual abuse and the presence of psychopathology were entered as covariates. Stepwise discriminant function analyses were conducted following MANOVA to evaluate the predictive functions of schema domains and self-reported depressive and anxiety symptoms for EM and CM. Relationships between schema domains and self-reported symptoms of depression and anxiety were evaluated using Pearson's correlation analyses. Due to the scarcity of studies on EMSs in adolescents with migraine and the exploratory nature of our study, we did not use correction for multiple comparisons.
Network analyses using EBICglasso were conducted to ascertain the relationships between schema domains and self-reported symptoms in patients with EM and CM. Significance was set at p = 0.05 (two-tailed). Effect sizes for significant findings were also reported.
Out of 800 patients, only 456 patients completed the EMS scale. A total of 193 patients with other headache types, 15 patients with comorbidities, 32 patients with symptoms of personality disorder, five patients with head trauma, two patients with an intellectual disability, one patient with alcohol and substance abuse, and one patient with vision loss were excluded. A total of 40 patients were excluded due to missing data. A total of 167 patients (n = 112, 67.1% female patients) diagnosed as suffering from EM (n = 140, 87.0%) and CM (n = 27, 23.0%) met the study inclusion criteria. The groups were similar in terms of female preponderance (66.4% episodic vs. 70.4% chronic, χ2 = 0.03, p = 0.861, Yates'). Adolescents with EM and CM did not differ significantly in terms of their own and their parents' sociodemographic features. The sociodemographic characteristics of the respondents and their families according to migraine type are illustrated in Table 1.
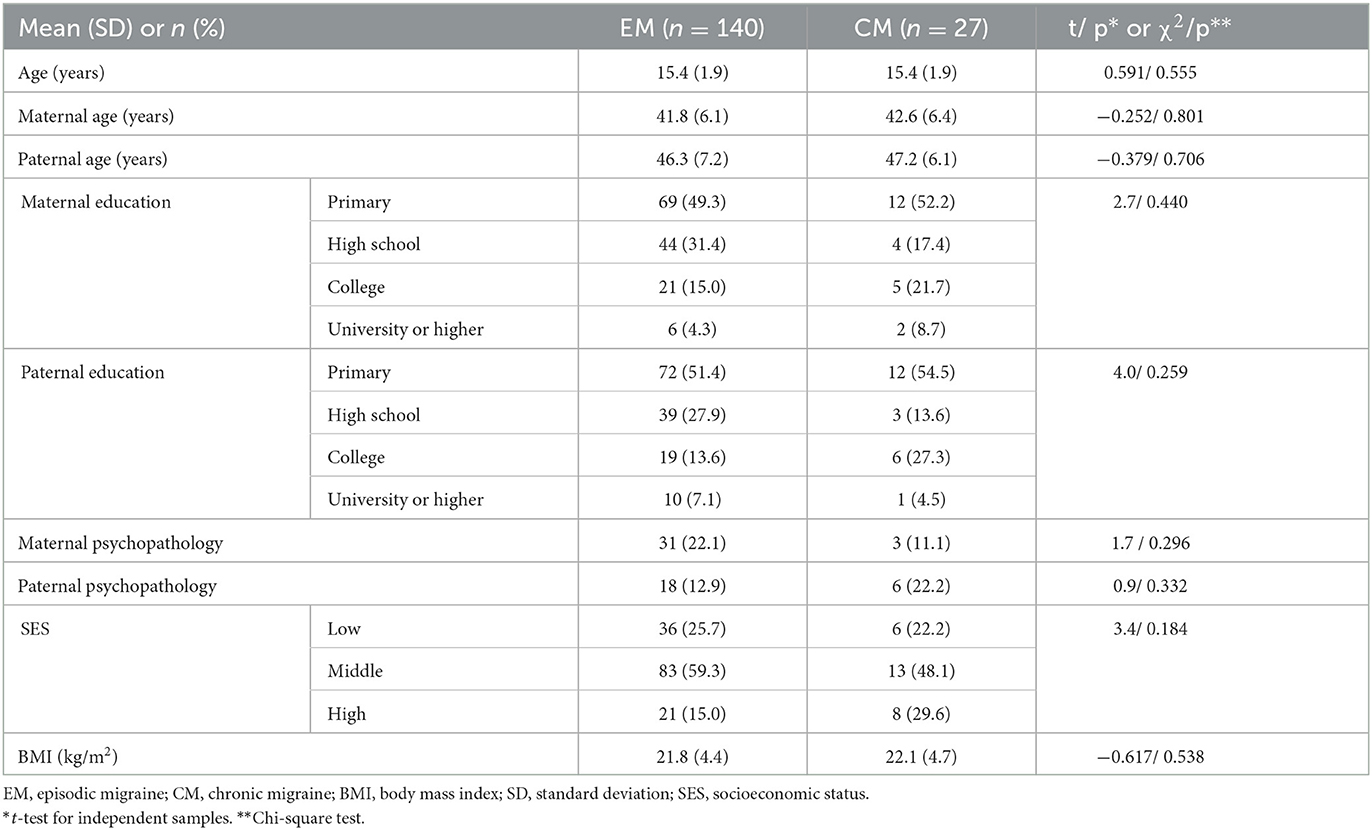
Table 1. Sociodemographic features of the respondents and their families according to migraine type.
More than half of the youths in both groups with EM (n = 72, 51.4%) and CM (n = 16, 59.3%) met the criteria for psychopathology, with no significant difference between the groups (χ2 = 0.29, p = 0.592, Yates'). The diagnoses of adolescents with migraine according to temporal features are illustrated in Table 2.
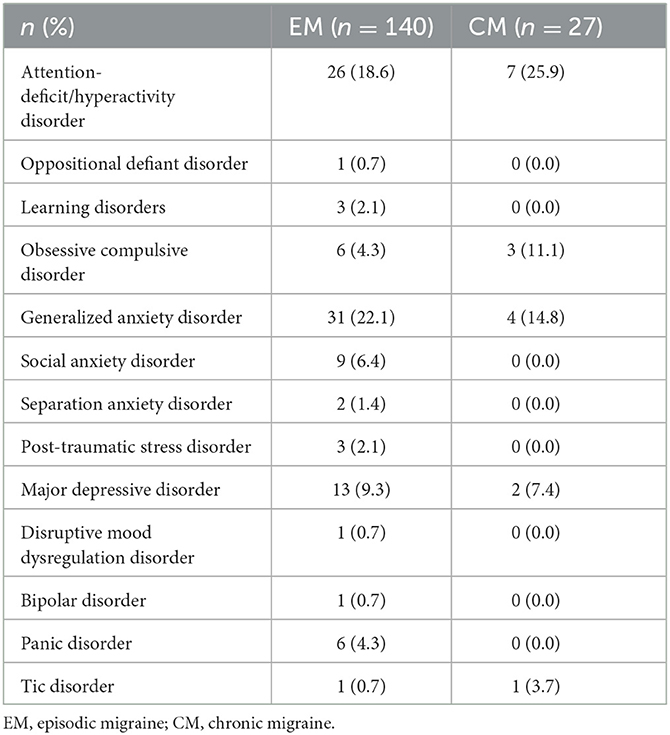
Table 2. Psychiatric diagnoses of the respondents according to migraine type.
For both EM and CM, the median number of diagnoses was 1.0 (IQR = 1.0) with no significant difference between the groups (Mann–Whitney U-test, Z = −0.4, p = 0.697). A history of sexual abuse was reported by five individuals with EM (3.6%); there were no reports of sexual abuse among youths with CM.
Features of pain in youths with EM and CM are illustrated in Table 3.
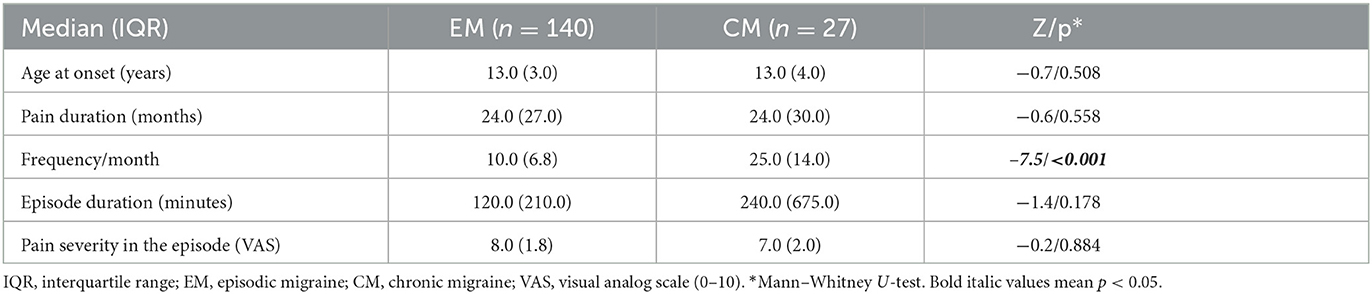
Table 3. Pain features in adolescents with migraine according to type.
In bivariate comparisons, except for the frequency of migraine episodes/month, other pain features did not differ significantly between the groups. Symptoms associated with migraine episodes are illustrated in Table 4.
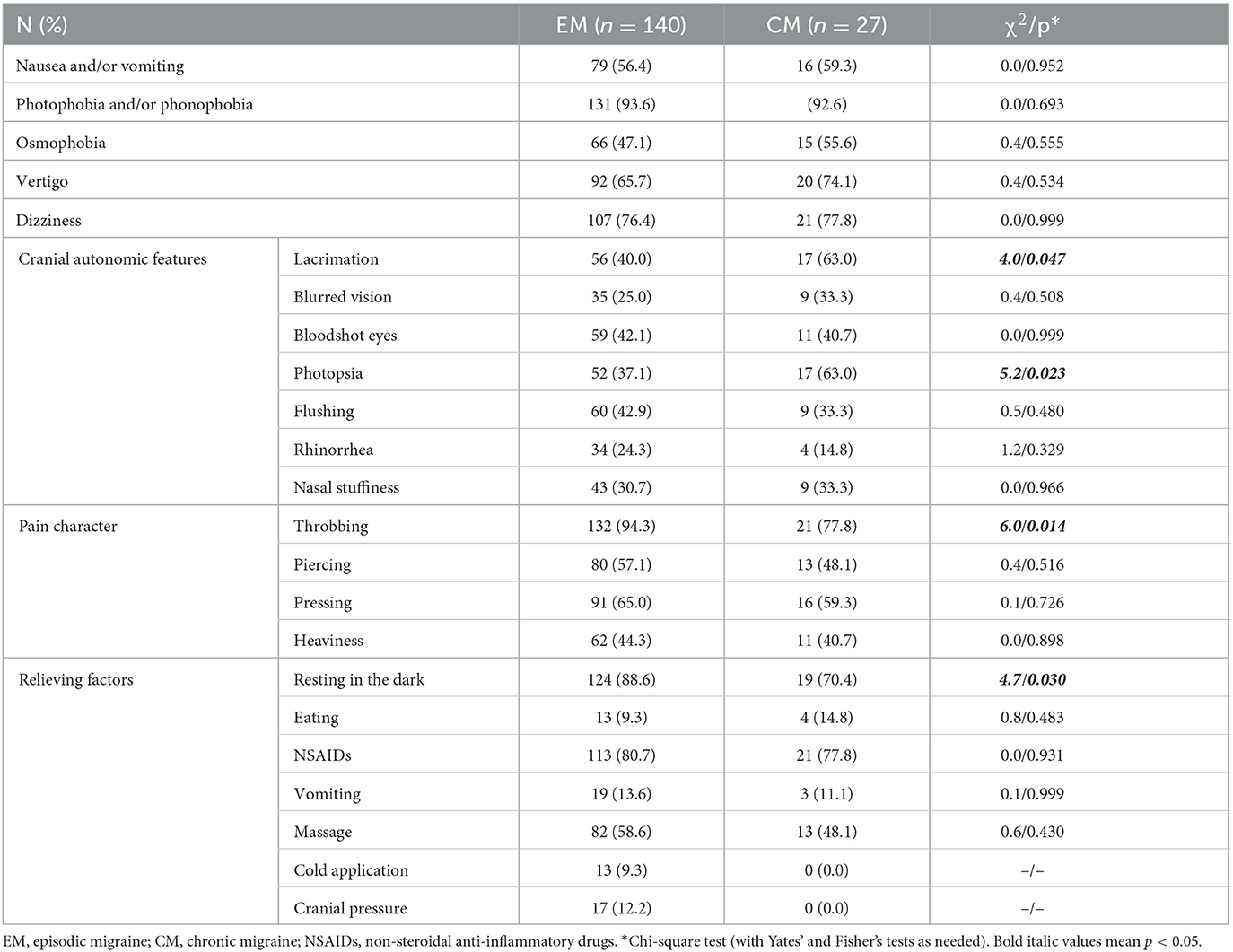
Table 4. Symptoms of migraine episodes according to type.
When the pain characteristics were compared between groups, some autonomic symptoms, such as lacrimation and photopsia, were found to be significantly more frequent in respondents with CM (with small effect sizes, Phi 0.17 and 0.19, respectively). A throbbing pain was reported significantly more frequently in youths with EM (Phi = 0.22). Youths with EM also reported relief from resting in a dark room significantly more frequently than those with CM (Phi = 0.19). Among the adolescents with EM, more than half (n = 92, 55.1%) reported no auras, and the remaining youths experienced auras.
EMSs and schema domains were compared between youths with EM and CM using MANOVA. The covariance matrices were homogenous (Box's M, χ2[28] = 28.3, p = 0.451), and Levene's test showed that the error variances for the emotional deprivation, negativity/pessimism schema, and hypervigilance domains were not equal (p = 0.021, p = 0.002, and p = 0.004, respectively). Therefore, Pillai's trace was used for comparison. Adolescents with EM and CM differed significantly in terms of EMSs and schema domains (F [15.0, 151.0] = 1.9, p = 0.028, partial η2 = 0.16). Follow-up univariate ANOVAs are presented in Table 5.
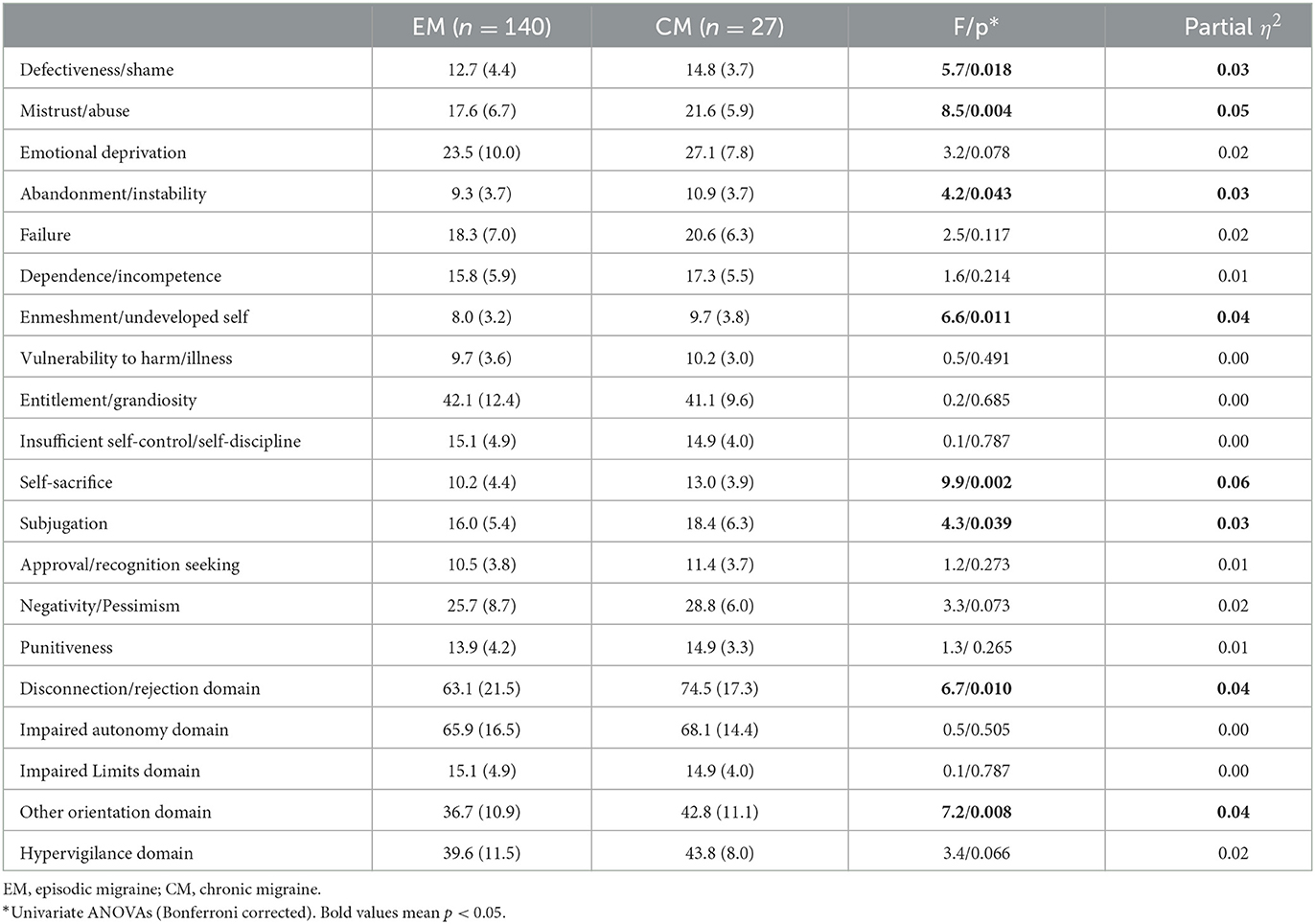
Table 5. Comparison of adolescents with episodic (EM) and chronic migraine (CM) in terms of early maladaptive schemas and schema domains.
In bivariate comparisons, youths with CM scored significantly higher on defectiveness/shame, mistrust/abuse, abandonment/instability, enmeshment/undeveloped self, self-sacrifice, and subjugation schemas. As for the schema domains, adolescents with CM scored significantly higher on disconnection/rejection and other orientation domains (p = 0.01 and p = 0.008, respectively) (Figure 2).

Figure 2. Illustration showing a summary of the EMSs and EMS domain scores from bivariate comparisons between EM and CM.
The inclusion of sexual abuse history and the presence of psychopathology did not affect the difference between the groups in terms of EMS scores (F [15.0, 149.0] = 1.9, p = 0.027, partial η2 = 0.16, Pillai's Trace). The presence of psychopathology did not affect EMS scores (F [15.0, 149.0]=1.2, p = 0.313, partial η2 = 0.10), but sexual abuse history did (F [15.0, 149.0] = 1.8, p = 0.038, partial η2 = 0.15, both Pillai's Trace). Youths with a history of sexual abuse had significantly higher scores on the defectiveness/shame, mistrust/abuse, emotional deprivation, dependence/incompetence, vulnerability to harm/illness, entitlement/grandiosity, self-sacrifice, and negativity/pessimism subscales. They also scored significantly higher on the disconnection/rejection, impaired autonomy, and hypervigilance domains.
Stepwise discriminant function analysis with EMSs revealed just one function involving the other orientation domain (Wilks's λ= 0.96, χ2 = 7.0, p = 0.008). The correlations of the disconnection/rejection (r = 0.73), hypervigilance (r = 0.59), impaired autonomy (r = 0.51), and impaired limit (r = 0.30) domains with the discriminant function were lower. This function was able to correctly classify 99.3% of adolescents with EM and 96.3% of those with CM, for an overall accuracy of 83.8%. When SCARED and CDI scores were entered into a stepwise discriminant function analysis, only one function including SCARED scores emerged (Wilks's λ= 0.94, χ2 = 7.5, p = 0.006). This function correctly classified 100.0% of youth with EM and none of those with CM, for an overall accuracy of 83.8%.
The mean CDI scores for youths with EM and CM were 15.9 (SD = 8.8) and 21.3 (SD = 9.8), respectively. The mean SCARED scores for adolescents with EM and CM were 31.9 (SD = 15.6) and 42.3 (SD = 13.4), respectively. The covariance matrices (Box's M, F [3.0, 14492.9] = 1.1, p = 0.363) and error variances (p = 0.589 and p = 0.375, respectively, Levene's test) were equal. Youths with EM and CM differed significantly in terms of depressive and anxiety symptoms (F [2.0, 131.0] = 4.7, p = 0.011, partial η2 = 0.07, Wilks's λ) with scores for CM being greater. The inclusion of sexual abuse and psychopathology as covariates did not affect the difference between EM and CM (F [2.0, 129.0] = 5.2, p = 0.007, partial η2 = 0.08, Wilks's λ). The presence of sexual abuse did not affect the self-reported depressive and anxiety symptoms (F [2.0, 129.0] = 0.3, p = 0.769, partial η2 = 0.00), but youths with a psychiatric diagnosis had significantly higher scores (F [2.0, 129.0] = 20.5, p < 0.001, partial η2 = 0.24, both Wilks's λ).
In adolescents with EM, age correlated significantly with the impaired limits domain of the EMSs (r = 0.24, p = 0.004). CDI and SCARED scores correlated positively with disconnection/rejection (r = 0.54, p < 0.001 and r = 0.45, p < 0.001, respectively), impaired autonomy (r = 0.38, p < 0.001 and r = 0.27, p = 0.003, respectively), impaired limits (r = 0.41, p < 0.001 and r = 0.23, p = 0.015, respectively), other orientation (r = 0.44, p < 0.001 and r = 0.29, p = 0.002, respectively), and hypervigilance (r = 0.60, p < 0.0001 and r = 0.53, p < 0.001, respectively) domains. When age was controlled, these correlations did not change significantly.
In adolescents with CM, age did not correlate with EMS domains. SCARED scores correlated significantly and positively only with the disconnection/rejection (r = 0.59, p = 0.006), and other orientations (r = 0.45, p = 0.045) domains. There were no significant correlations between CDI scores and EMS domains. When age was controlled, these correlations did not change significantly.
Network analyses with EBICglasso revealed a network of seven nodes with 15/21 non-zero edges for EM (sparsity = 0.29) and seven nodes with 3/21 non-zero edges (sparsity = 0.86) for CM. Centrality and clustering measures per variable for the EM and CM networks are illustrated in Table 6.
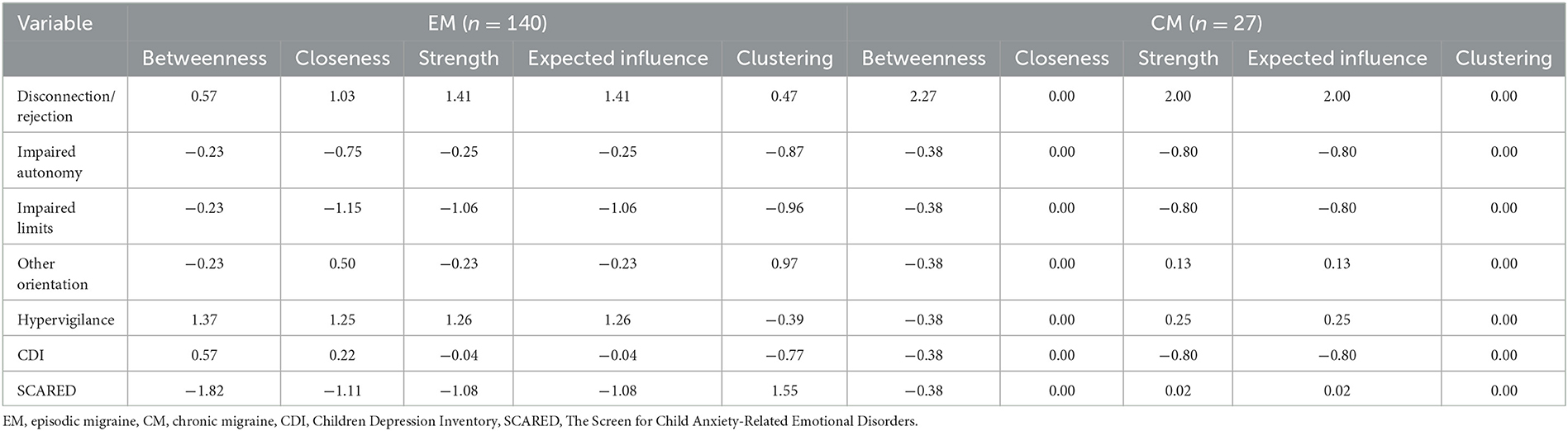
Table 6. Measures of centrality and clustering (Barrat) per variable for adolescents with episodic (EM) and chronic migraine (CM).
Network plots for adolescents with episodic (EM) and chronic (CM) migraine are illustrated in Figures 3, 4, respectively.
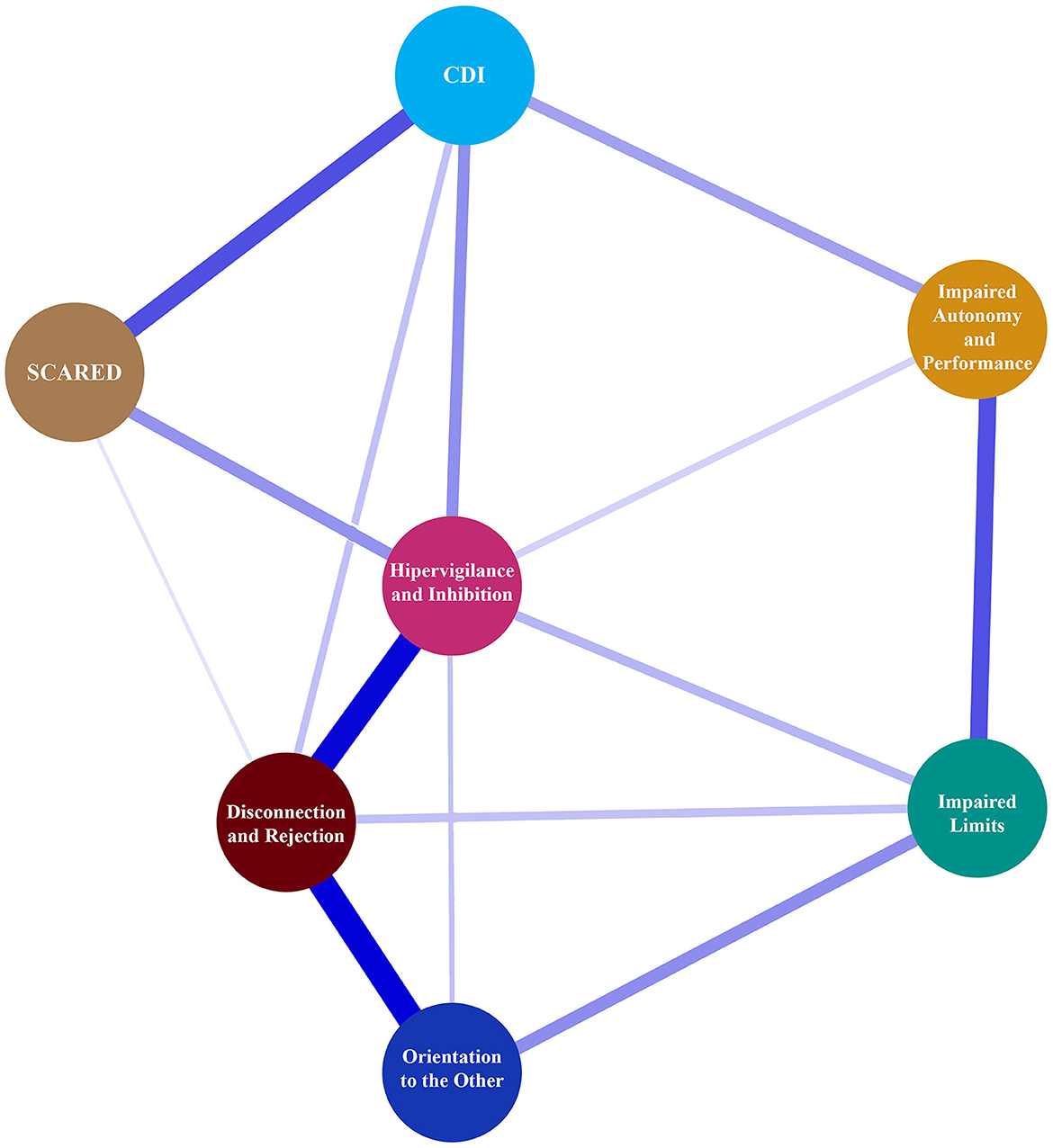
Figure 3. Network plot for adolescents between CDI, SCARED, and EMS domain with episodic migraine.
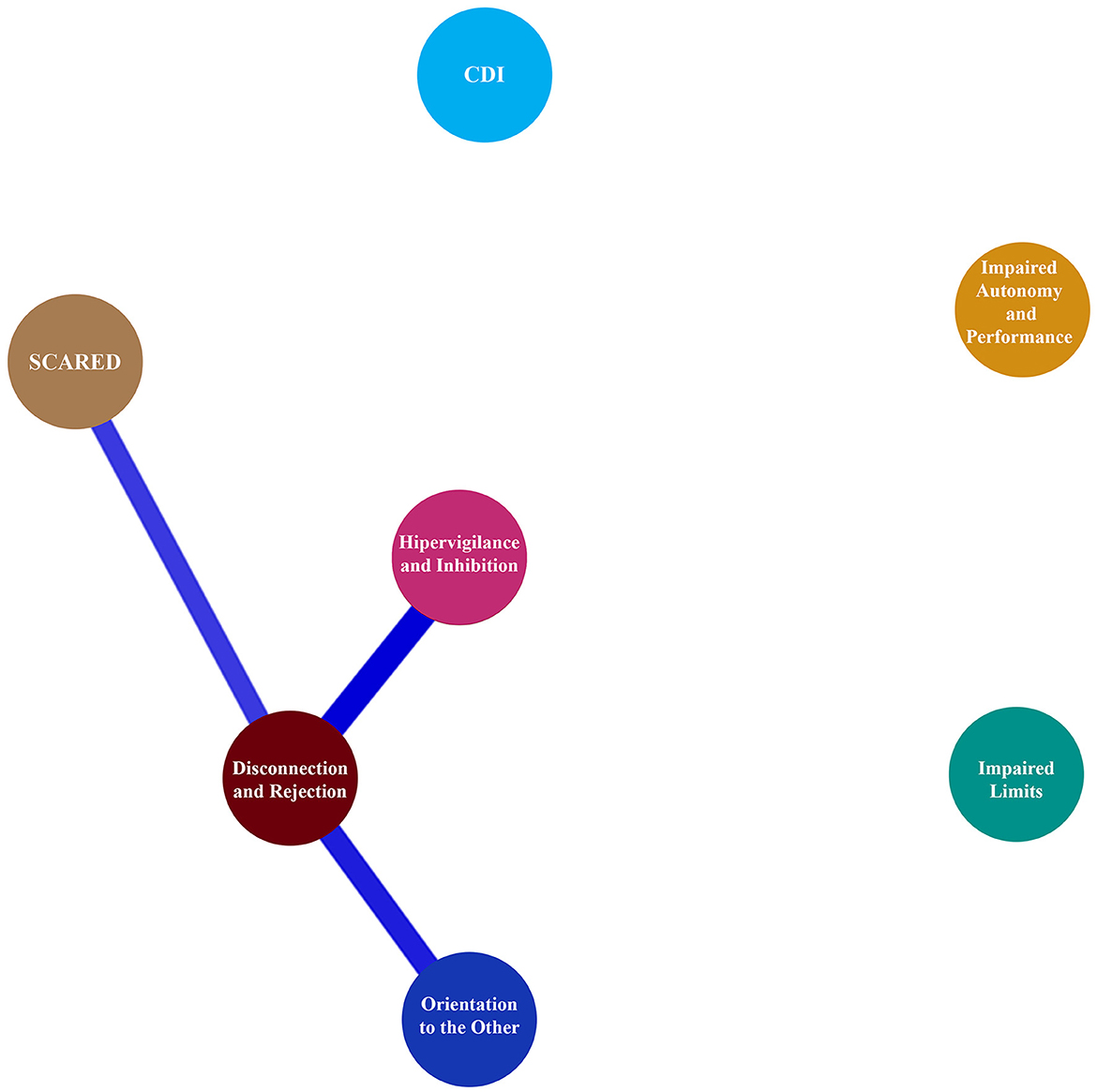
Figure 4. Network plot for adolescents between CDI, SCARED, and EMS domain with chronic migraine.
This study investigated headache characteristics, EMSs, depression, anxiety, and the interrelationship of schema domains and others in adolescents with either EM or CM. The effects of age, current psychopathology, history of sexual abuse, anxiety, and depression on EMSs were also evaluated. Age, gender, sociodemographic characteristics, most pain features, and the core clinical characteristics of migraine did not differ significantly between groups. In bivariate comparisons, disconnection/rejection, other orientation schema domains, defectiveness/shame, mistrust/abuse, abandonment/instability, enmeshment of the undeveloped self, self-sacrifice, and subjugation schemas were more frequent in CM. Discriminant analysis revealed that the other orientation schema domain could correctly classify 99.3% of youths with EM and 96.3% of those with CM, for an overall accuracy of 83.8%. SCARED scores correctly classified 100.0% of youths with EM and none of those with CM, for an overall accuracy of 83.8%. Respondents with CM had higher depression and anxiety scores. In addition, the inclusion of sexual abuse and psychopathology as covariates did not affect the difference between the groups in terms of depressive and anxiety symptoms. Age, anxiety, and depression correlated with most of the EMS domains in adolescents with EM, and the relationship between anxiety, disconnection/rejection, and other orientation schema domains became evident with the migraine chronification.
Dogaheh et al. reported that EMSs and maladaptive coping styles (avoidance and overcompensation), which are used to overcome EMSs but have perpetuating long-term effects, were more common in patients with migraine and tension-type headaches than in a non-clinical group (10, 22). Bashiri Nejadian et al. revealed that EMSs may serve as a basis for emotional and behavioral tendencies and defensive coping styles in patients with migraine (23). Enayatian et al. also found that EMSs and clinical symptoms of migraine were mediated by dysfunctional attitudes (24). There seems to be an under-recognized, multidirectional relationship between EMSs, coping styles, attitudes, psychopathology, and migraine. Although there is an increasing interest in EMSs, the literature is still lacking in detailed studies about the possible role of EMSs in headaches, especially for children and adolescents. To our knowledge, only one study has been conducted to date on EMSs in adults with CM. It has been suggested that EMSs may explain a significant proportion of pain and that schema therapy may be effective in reducing the frequency and severity of headaches in CM (8). We conducted a study evaluating EMSs in adolescents with migraine and found that different EMSs between the sexes may play a role in migraine. It was the first study of EMSs in pediatric migraine (25). This study is also the first to investigate EMSs in episodic and chronic migraine in the pediatric age group.
CM is often transformed from EM, but the majority of people with EM do not develop CM. Many studies have evaluated risk factors to determine who may develop CM. Consistent results point to obesity, high attack frequency, medication overuse, snoring, and stressful life events (2, 4). Depression and anxiety are associated with a high risk of new-onset CM (2). Although there are many studies on stressful life events, depression, anxiety, and other psychiatric comorbidities in migraine, schemas, which are the basic structures of cognition, are understudied in both pediatric and adult migraine. This is the first study of EMSs in CM in adolescents, and the results show that there are different active schemas and schema domains in CM. In the study, sociodemographic/family characteristics, pain features, and the median number of psychopathologies were similar between the groups. Although causal explanations are not possible due to the design of the research, the difference in terms of EMSs in CM between these homogeneous groups is remarkable and merits further investigation into the underlying pathophysiology of CM.
Several studies confirm that psychiatric disorders are frequently seen in migraineurs (2). Mood and anxiety disorders are more commonly reported in CM (2). In our study, more than half of the cases in both groups were accompanied by a psychiatric disorder, showing the importance of psychopathology in migraine at an early age. Although there was no difference in the ratio of psychopathology between the groups, the fact that depressive and anxiety symptoms were high in CM indicates that the foundations of this course were laid at a younger age. Personality traits, childhood maltreatment, attachment, and emotional and behavioral problems are the most studied psychiatric topics in adult migraine (2, 9, 26), but further investigation on pediatric migraine may shed light on pathophysiology and chronification. Multi-center and community-based studies can elucidate the clinical features and accompanying psychopathologies of deeper cognitive structures called schemas in EM and CM, especially in children and adolescents.
Pain characteristics and core clinical features of migraine were not different between the groups. We also examined controversial clinical features, and two of them, lacrimation and photopsia, were more frequent in CM. Few studies have reported that cranial autonomic symptoms (CAS), which are the hallmarks of trigeminal autonomic cephalalgias, may occur in migraine (27). CAS is like a rule in pediatric migraine with a rate as high as 70% based on the ICHD-3 (28). Only one study reported that migraineurs with CAS had longer illness duration and longer headache episodes (29). Another study showed that CAS was related to the higher frequency of migraine attacks in children (30). To date, we have not found any data showing that lacrimation and photopsia are more common in CM. There is a need to investigate the extent of CAS in pediatric CM and its effects on chronicity. According to the results, EMSs associated with CAS may be independent risk factors for progression to treatment-resistant migraine. In early childhood, EMSs may lead to malformed neural networks, and their consequences in the long term may negatively affect mental health and headache courses.
Psychological stress influences the onset, severity, and course of many diseases. Psychological stress and EMSs have been studied in many diseases such as diabetes mellitus, psoriasis, atopic eczema, and irritable bowel syndrome (31–33). Migraine is a stress-related disorder. In this study, the presence of psychiatric disorders did not affect EMS scores, but sexual abuse did, especially in the domains of disconnection/rejection, impaired autonomy, and hypervigilance. The presence of sexual abuse did not affect self-reported depressive and anxiety symptoms, but psychopathologies did. These results suggest that EMSs may not be directly correlated with psychiatric disorder, but that EMSs may be important background factors in EM and CM, independent of psychopathologies. This hypothesis should be addressed with comprehensive longitudinal studies.
A recent review discovered evidence of a link between EMS and adolescent psychopathology. Depression, anxiety, eating pathology, borderline symptomatology, and externalizing behaviors were distinguished by EMSs (14). However, to date, there has been no study of EMSs in young patients with headaches. Tavallaii et al. revealed that divergent schemas were associated with headache pain severity, disability, and affective stress. They stated that the hypervigilance/inhibition domain had a predictive role in CM (8). Later, Ribas et al. confirmed the association between hypervigilance/inhibition and migraine, especially in female patients (34). Another study found that migraine and tension-type headaches were linked to mistrust/abuse, and self-sacrifice schemas in Iranian adults (10). In the current study, which supports previous adult studies, we found that defectiveness/shame, mistrust/abuse, abandonment/instability, enmeshment/undeveloped self, self-sacrifice and subjugation schemas, disconnection/rejection, and other orientations for schema domains were higher in adolescents with CM.
Recently, studies in adults have focused on the relationship between emotional problems, EMS, and migraine. Onen et al. speculated that the self-sacrifice schema may be associated with both depression and migraine (35). Previous studies reported that defensive styles/dysfunctional attitudes were linked to EMSs, emotional and behavioral symptoms, and migraine symptoms (14, 23, 24). According to Dogaheh, a set of EMSs could correctly predict 61% of the overall change in position in tension headaches or migraine groups in adults (10). In our study, the other orientation schema domain could correctly classify 99.3% of youths as EM and 96.3% as CM, for an overall accuracy of 83.8%. SCARED scores correctly classified 100.0% of adolescents with EM and none of those with CM, for an overall accuracy of 83.8%. Network analysis showed that CDI and SCARED scores had a moderately positive correlation with all EMS domains in youths with EM, and these correlations became evident between SCARED scores and disconnection/rejection and other orientation domains in youths with CM. This is important to consider in terms of which features may be unique to CM; further studies may answer this question.
This study has several limitations, including the limited number of patients, especially in the CM group, due to the retrospective design. The single-center, clinic-based, cross-sectional design limits the generalizability of the results. A larger study with a control group and follow-up studies are needed to confirm our findings. EMSs were evaluated using self-report scales, which may lead to reporting and recall bias. We did not use psychometric instruments to assess childhood adversity; instead, we relied on the reports of sexual abuse from respondents and their parents. The strength of this study is that we analyzed the results by taking into account comorbid psychopathology and abuse history. Another strength is that it is the first study to investigate EMSs, emotional factors, and their interrelationships within adolescents with EM and CM.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Faculty of Medicine at Mersin University (Number: E-78017789-050.01.04-1659432 Date: 26/05/2021). Written informed consent from the participants' legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
GG, OK, FT, and AÖzg designed the study and involved in data collection. MK, AT, DS, and BT analyzed the data. GG, AÖzd, OK, and AT wrote the original draft of the manuscript. AT, MK, FT, BT, DS, AÖzd, and AÖzg provided a critical review of the original draft of the manuscript. All authors read and approved the content of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Özge A, Yalin OÖ. Chronic migraine in children and adolescents. Curr Pain Headache Rep. (2016) 20:1–9. doi: 10.1007/s11916-016-0538-z
2. Buse DC, Silberstein SD, Manack AN, Papapetropoulos S, Lipton RB. Psychiatric comorbidities of episodic and chronic migraine. J Neurol. (2013) 260:1960–9. doi: 10.1007/s00415-012-6725-x
3. Manack AN, Buse DC, Lipton RB. Chronic migraine: epidemiology and disease burden. Curr Pain Headache Rep. (2011) 15:70–8. doi: 10.1007/s11916-010-0157-z
4. Bigal ME, Serrano D, Buse D, Scher A, Stewart WF, Lipton RB, et al. Acute migraine medications and evolution from episodic to chronic migraine: a longitudinal population-based study. Headache. (2008) 48:1157–68. doi: 10.1111/j.1526-4610.2008.01217.x
5. Özge A, Genç H, Aksu GG, Uludüz D. Migraine and frontostriatal circuit disorders: What have we learned until now? Neurol Sci Neurophysiol. (2021) 38:81–9. doi: 10.4103/nsn.nsn_9_21
6. Anttila V, Bulik-Sullivan B, Finucane HK, Walters RK, Bras J, Duncan L, et al. Analysis of shared heritability in common disorders of the brain. Science. (2018) 360:eaap8757. doi: 10.1126/science.aap8757
7. Beck AT, Haigh EAP. Advances in cognitive theory and therapy: the generic cognitive model. Annu Rev Clin Psychol. (2014) 10:1–24. doi: 10.1146/annurev-clinpsy-032813-153734
8. Tavallaii A, Naderi Z, Rezaiemaram P, Tavallaii V, Babamohamadi Z, Aghaie M. The relationship between early maladaptive schemas and three dimensions of headache impact in Iranian outpatients with chronic migraine without aura. Int J Behav Sci. (2015) 9:215–23. Available online at: http://www.behavsci.ir/article_67923.html
9. Sotodehasl N, Amirahmadi E, Ghorbani R, Masoudian N. and Samaei, A. Association between personality traits and migraine headache Koomesh. (2019) 21:46–51. Available online at: https://koomeshjournal.semums.ac.ir/browse.php?a_id=4125&sid=1&slc_lang=en
10. Dogaheh ER, Yoosefi A, Kami M. Comparison of maladaptive coping styles in patients with migraine and tension headaches with normal group. Pract Clin Psychol. (2014) 2:211–9. Available online at: http://jpcp.uswr.ac.ir/browse.php?a_code=A-10-1-24&slc_lang=en&sid=1
11. Nash JM, Thebarge RW. Understanding psychological stress, its biological processes, and impact on primary headache. Headache J Head Face Pain. (2006) 46:1377–86. doi: 10.1111/j.1526-4610.2006.00580.x
13. Young JE, Klosko JS, Weishaar ME. Schema therapy: a practitioner's guide. New York: The Guilford Press (2003).
14. Nicol A, Mak AS, Murray K, Walker I, Buckmaster D. The relationships between early maladaptive schemas and youth mental health: a systematic review. Cogn Ther Res. (2020) 44:715–51. doi: 10.1007/s10608-020-10092-6
15. Lipton RB, Silberstein SD. Episodic and chronic migraine headache: breaking down barriers to optimal treatment and prevention. Headache. (2015) 55:103–22. doi: 10.1111/head.12505_2
16. The International Classification of Headache Disorders. Headache classification committee of the international headache society (IHS), 3rd edition. Cephalalgia. (2013). 38:1–211. doi: 10.1177/0333102417738202
17. Ozge A, Bugdayci R, Sasmaz T, Kaleagasi H, Kurt O, Karakell A, et al. The sensitivity and specificity of the case definition criteria in diagnosis of headache: a school-based epidemiological study of 5562 children in Mersin. Cephalalgia. (2002) 22:791–8. doi: 10.1046/j.1468-2982.2002.00467.x
19. Birmaher B, Brent DA, Chiappetta L, Bridge J, Monga S. Baugher. Psychometric properties of the screen for child anxiety related emotional disorders (SCARED): a replication study. J Am Acad Child Adolesc Psychiatry. (1999) 38:1230–6. doi: 10.1097/00004583-199910000-00011
20. Güner O. Psychometric properties and normative values of early maladaptive schema questionnaires set for children and adolescents (SQS). Clin Psychol Psychother. (2017) 24:534–54. doi: 10.1002/cpp.2049
21. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, fifth ed. (2013). doi: 10.1176/appi.books.9780890425596
22. Dogaheh ER, Yoosefi A, Kami M. Early maladaptive schemas in patients with and without migraine and tension headaches. Iran Rehabil J. (2015) 13:7–12. Available online at: http://irj.uswr.ac.ir/browse.php?a_code=A-10-187-1&slc_lang=en&sid=1
23. Bashiri Nejadian A, Babamiri M. and Johari Fard, R. The association between defensive styles and early maladaptive schemas in patients with migraine headaches Iran. J Psychiatry Behav Sci. (2017) 11:e7592. doi: 10.5812/ijpbs.7592
24. Enayatian O, Amiri M, Zarabi Moghadam Z. Investigating the mediating role of dysfunctional attitudes on the rela-tionship between early maladaptive schemas and clinical symptoms in migraine patients. Shenakht J Psychol Psychiatry. (2020) 7:126–40. doi: 10.52547/shenakht.7.1.126
25. Güler Aksu G, Kayar O, Tufan AE, Kütük MÖ, Sucu DH, Taşdelen B, et al. Early maladaptive schemas differing according to sex may contribute to migraine among the youth. Brain Dev. (2022) 44:427–37. doi: 10.1016/j.braindev.2022.04.001
26. Tietjen GE, Brandes JL, Peterlin BL. Eloff A, Dafer, RM, Stein MR, et al. Childhood maltreatment and migraine (Part II) emotional abuse as a risk factor for headache chronification headache. J Head Face Pain. (2010) 50:32–41. doi: 10.1111/j.1526-4610.2009.01557.x
27. Uluduz D, Ayta S, Özge A, Yalin OÖ, Örekici Temel G. ans Taşdelen, B. Cranial autonomic features in Migraine and Migrainous features in cluster headache. Noropsikiyatri Ars. (2018) 55:220–4. doi: 10.5152/npa.2016.19183
28. Gelfand AA, Reider AC, Goadsby PJ. Cranial autonomic symptoms in pediatric migraine are the rule, not the exception. Neurology. (2013) 81:431–6. doi: 10.1212/WNL.0b013e31829d872a
29. Gupta R, Bhatia MS. A report of cranial autonomic symptoms in migraineurs. Cephalalgia. (2007) 27:22–8. doi: 10.1111/j.1468-2982.2006.01237.x
30. Raieli V, Giordano G, Spitaleri C, Consolo F, Buffa D, Santangelo G, et al. Migraine and cranial autonomic symptoms in children and adolescents: a clinical study. J Child Neurol. (2015) 30:182–6. doi: 10.1177/0883073814535494
31. Fathabadi J, Haji Ghorbani Doulabi M, Arjmandnia A, Abidi H, Shalani B, Sadeghi S, et al. Prediction of blood glucose level in patients with type 2 diabetes through early maladaptive schemas. Daneshvar Med. (2020) 28:40–9. Available online at: https://www.magiran.com/paper/2147066/?lang=en
32. Yousefi R. The comparison of early maladaptive schemas and cognitive emotion regulation styles in patient with functional gastrointestinal disorders (FGID) and normal group. Govaresh. (2014) 19:257–64. Available online at: http://govaresh.org/index.php/dd/article/view/1360/1670
33. Mizara A, Papadopoulos L, McBride SR. Core beliefs and psychological distress in patients with psoriasis and atopic eczema attending secondary care: the role of schemas in chronic skin disease. Br J Dermatol. (2012) 166:986–93. doi: 10.1111/j.1365-2133.2011.10799.x
34. Ribas K, Ribas V, Barros S, Ribas VR, Filizola M, Ribas R, et al. The participation of early maladaptive schemas (EMSs) in the perception of pain in patients with migraine: a psychological profile. Dement Neuropsychol. (2018) 12:68–74. doi: 10.1590/1980-57642018dn12-010010
Keywords: adolescent, migraine, episodic, chronic, early maladaptive schemas, psychopathology
Citation: Güler Aksu G, Kayar O, Tufan AE, Kütük MÖ, Özdağ Acarli AN, Sucu DH, Taşdelen B, Toros F and Özge A (2023) Early maladaptive schemas in episodic and chronic migraine in adolescents. Front. Neurol. 14:1128953. doi: 10.3389/fneur.2023.1128953
Received: 21 December 2022; Accepted: 24 March 2023;
Published: 21 April 2023.
Edited by:
Tim P. Jürgens, University Hospital Rostock, GermanyReviewed by:
Gul Karacetin, University of Health Sciences, TürkiyeCopyright © 2023 Güler Aksu, Kayar, Tufan, Kütük, Özdağ Acarli, Sucu, Taşdelen, Toros and Özge. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gülen Güler Aksu, ZHIuZ3VsZW5AaG90bWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.