 Fei Zhang
Fei Zhang Hong Jiang2
Hong Jiang2 Gang Zhao
Gang Zhao
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurol. , 25 April 2023
Sec. Neuromuscular Disorders and Peripheral Neuropathies
Volume 14 - 2023 | https://doi.org/10.3389/fneur.2023.1081440
This article is part of the Research Topic Surgical Treatment of Peripheral Neuropathic Pain, Peripheral Nerve Tumors, and Peripheral Nerve Injury View all 25 articles
Background: Over the years, endoscopic carpal tunnel release (ECTR) has gained significant interest as an alternative to surgery. However, no consensus has been reached on the necessity of postoperative wrist immobilization. This study aims to compare the outcomes of wrist immobilization for a period of 2 weeks to immediate wrist mobilization after ECTR.
Methods: A total of 24 patients with idiopathic carpal tunnel syndrome undergoing dual-portal ECTR from May 2020 to Feb 2022 were enrolled and randomly divided into two groups postoperatively. In one group, patients wore a wrist splint for 2 weeks. In another group, wrist mobilization was allowed immediately after surgery. The two-point discrimination test (2PD test); the Semmes–Weinstein monofilament test (SWM test); the occurrence of pillar pain, digital and wrist range of motion (ROM); grip and pinch strength; the visual analog score (VAS), the Boston Carpal Tunnel Questionnaire (BCTQ) score; the Disabilities of the Arm, Shoulder, and Hand (DASH) score; and complications were evaluated at 2 weeks and 1, 2, 3, and 6 months after the surgery.
Results: All 24 subjects finished this study with no dropouts. During the early follow-up, patients with wrist immobilization demonstrated lower VAS scores, lower occurrence of pillar pain, and higher grip and pinch strength compared with the immediate mobilization group. No significant difference was obtained between these two groups in terms of the 2PD test, the SWM test, digital and wrist ROM, BCTQ, and the DASH score. In total, two patients without splints reported transient scar discomfort. No one complained of neurapraxia, injury of the flexor tendon, median nerve, and major artery. At the final follow-up, no significant difference was found in any parameters between both groups. The local scar discomfort mentioned above disappeared and left no serious sequela.
Conclusion: Wrist immobilization during the early postoperative period demonstrated significant pain alleviation along with stronger grip and pinch strength. However, wrist immobilization yielded no obvious superiority regarding clinical outcomes at the final follow-up.
Carpal tunnel syndrome (CTS) is the most common peripheral compressive neuropathy worldwide (1). Carpal tunnel release (CTR) represents an alternative approach indicated when conventional intervention fails or symptoms recur (2). The surgery can be undergone via the traditional open or endoscopic approach (3–5). Although endoscopic carpal tunnel release (ECTR) yields similar clinical outcomes compared to open release, ECTR has gained significant attention worldwide for its improved aesthetics and fast recovery (5–9).
However, postoperative immobilization is still subject to much controversy. Earlier studies showed comparable outcomes and even worse prognosis of splint immobilization after open release compared with initial active motion (10–19). According to the 2016 American Academy of Orthopedic Surgeons (AAOS) evidence-based guidelines, postoperative immobilization yields no benefit (20). There are no valid data and associated criteria on splint immobilization after ECTR until now. This study sought to evaluate the outcomes of splint immobilization or initial active motion after ECTR and assess the significance of postoperative wrist immobilization.
This study was approved by the Ethics Committee of WuXi No.9 People's Hospital Affiliated to Soochow University. All subjects provided informed consent before this study started.
Outpatients at the WuXi No.9 People's Hospital Affiliated to Soochow University from May 2020 to Feb 2022 diagnosed with CTS clinically or by electrodiagnostic testing were recruited in our study. Inclusion criteria were severe idiopathic CTS with an electromyography (EMG) test and failure of conventional intervention or symptom recurrence. We defined severe CTS according to the AAEM grading criteria: prolonged median motor and sensory distal latencies, with either an absent SNAP or mixed NAP or low amplitude or absent thenar CMAP. Needle examination often reveals fibrillations, reduced recruitment, and motor unit potential changes (21). Exclusion criteria were slight or moderate CTS, mass-like cyst in the carpal tunnel, other wrist disorders, such as arthritis, wrist fracture within 3 months, CTS revision, and local skin or subcutaneous tissue disorders. Ultimately, 24 subjects according to the inclusion and exclusion criteria were enrolled and randomly divided into two groups, each containing 12 subjects. In total, five subjects had bilateral CTS and received ECTR concomitantly.
All subjects received one sealed envelope prepared by a person who was not involved in this trial after inclusion. The envelope contained the subject's sequential number and group and was opened just before the skin preparation of the surgical area. All subjects underwent dual-portal ECTR by the same operator. After surgery, one group was provided with a plaster splint put in the volar side of the wrist and half of the forearm and wrapped with bandage gauze. The wrist was immobilized in the neutral position for 2 weeks while the metacarpophalangeal joint and elbow could be moved immediately after surgery. Thereafter, the splint and bandage were removed after 2 weeks at the outpatient. For another group, an elastic bandage was applied to cover the incision, with no limitation of active wrist motion. All subjects were discharged on the first or second postoperative day with no analgesics and were required to visit the outpatient clinic five times at 2 weeks and 1, 2, 3, and 6 months.
Outcome parameters contained the 2PD test, SWM tests, the occurrence of pillar pain, digital and wrist range of motion, grip and pinch strength, VAS for pain, BCTQ, DASH score, and complications. All data were measured and recorded by an independent therapist with the Jamar® Hand Evaluation kit.
Sensibility testing was measured by the 2PD and SWM tests. The 2PD test was used to evaluate the threshold capacity to distinguish two different pressure points applied on the fingertip via a particular discriminator. The SWM test was used to evaluate the touch threshold of the fingertip via five standardized filaments (size 2.83, size 3.61, size 4.31, size 4.56, and size 6.65; size 2.83 represents normal sensibility, and size 6.65 represents no protective sensibility). The tactile senses of the first to fourth digital fingertips were measured three times, and the median value was obtained.
Postoperative pain was assessed by VAS and the occurrence of pillar pain. VAS of the wrist was measured during active motion without any load with a 100 mm visual analog scale ranging from 0 to 10 (0: absence of pain and 10: worst pain).
Postoperative strength was measured by the grip and pinch strength. Grip strength was measured in a seated position with the shoulder and wrist in a neutral position, with the elbow in a 90-degree flexed position, using the Jamar dynamometer. Key pinch strength measured the pressure between the thumb pad and the middle phalanx of the index digit with a pinch gauge dynamometer. All tests were measured three times, and the best value was recorded to decrease bias.
Postoperative flexibility was assessed by digital and wrist ROM. Each digital ROM was measured with a finger goniometer, and the interphalangeal joint of thumb value was recorded for further comparison. Wrist ROM during flexion and extension was measured in a seated position with elbow flexion and the hand placed in a resting position using a wrist goniometer.
Postoperative self-evaluation was measured by the BCTQ and DASH questionnaire. The BCTQ consists of two scales: a symptom severity scale (BCTQ-S) and a functional status scale (BCTQ-F) (22, 23). The former section contained 11 items with a score between 1 and 5 (one means normal and five means serious symptom), whereas the latter section included eight items regarding physical function with a score between 1 and 5 (one means no difficulty and five means that subject cannot perform the activity). The average value of each section was recorded for further comparison. The DASH questionnaire contained 30 items with a score between 1 and 5 (one means no difficulty and five means inability). The score was calculated with the formula [(Sum of n responses)/n – 1] * 25 and recorded for further comparison (24).
Data were analyzed using SPSS software, v.25 (IBM SPSS Statistics 25, USA). Digital and wrist ROM and grip and pinch strength were analyzed using a Student's t-test. Data were expressed in the form of mean ± standard deviation. The 2PD test, SWM test, VAS, BCTQ, and DASH score were analyzed with Wilcoxon's rank sum test. Non-parametric data were expressed as median values. The occurrence of pillar pain was analyzed with the Fisher exact test. Data were expressed in the form of occurrence. The level of significance was set at a P-value of < 0.05.
The outcome measures were assessed in all subjects, and none were lost during the follow-up period. The subjects exhibited a female predominance (n = 18, 75%) aged 26–82 years old. The duration of symptoms ranged from 1 to 120 months. In addition to gender, there was no significant difference between the two groups regarding demographic data (Table 1).
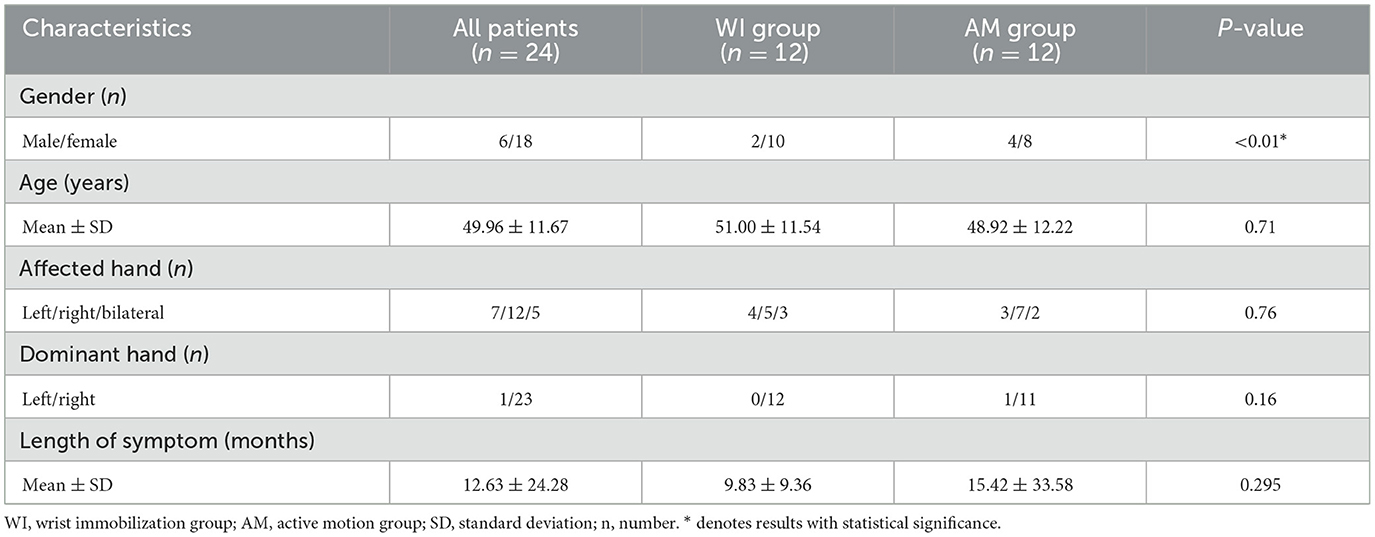
Table 1. Group characteristics.
The 2PD and SWM tests showed an apparent improvement compared with preoperative values although no significant difference was found between both groups at each time point. Moreover, the wrist immobilization group yielded better VAS and lower occurrence of pillar pain compared with the wrist mobilization motion group at 2 weeks postoperatively. No difference in pillar pain was observed at 1 month postoperatively. In addition, nearly 80% of subjects were pain-free at the final follow-up in both cohorts. Moreover, grip and pinch strength decreased in early follow-up and got restored to preoperative levels at 2 months postoperatively. At 3 months postoperatively and the final follow-up, strength was slightly stronger than preoperative values in both groups. When these two groups were compared, the wrist immobilization group showed stronger grip and pinch strength than the wrist mobilization group at 2 weeks postoperatively. Subsequently, the strength of both groups was comparable. Digital and wrist ROM showed no obvious difference between preoperative and final follow-up and in both cohorts at any time. For the BCTQ and DASH questionnaire, both groups showed decreased scores at 2 weeks postoperatively and returned to preoperative levels at 1 month. Although the DASH scores of wrist immobilization at 1 month were greater, the difference showed no statistical significance. In total, two subjects in the wrist mobilization group complained of scar discomfort in the distal wound during early follow-up, which disappeared at 1 month postoperatively. No severe complications, including wound dehiscence, lesion of the superficial palmar arch, or median nerve, occurred during the whole follow-up. All data are shown in Tables 2–5.
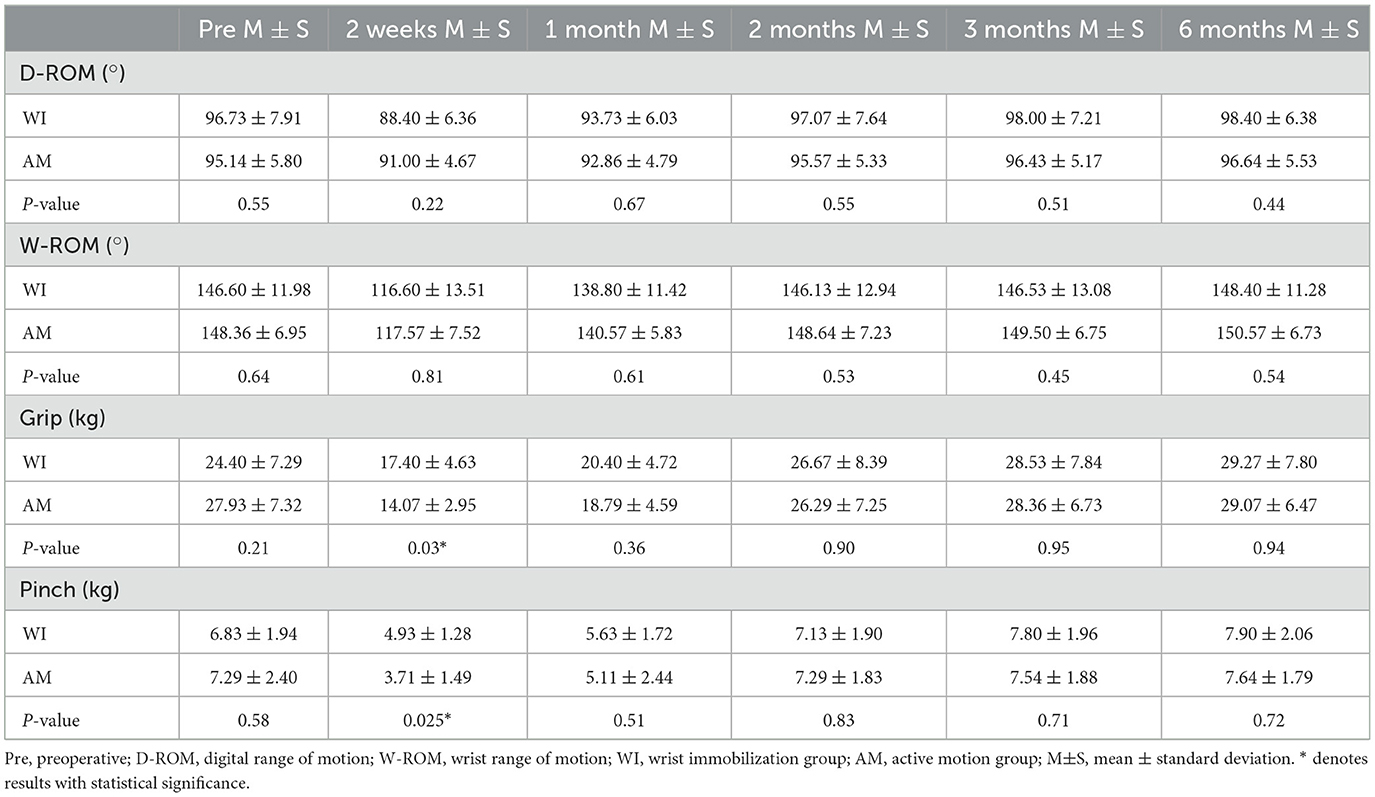
Table 2. Outcome measures of strength and flexibility.
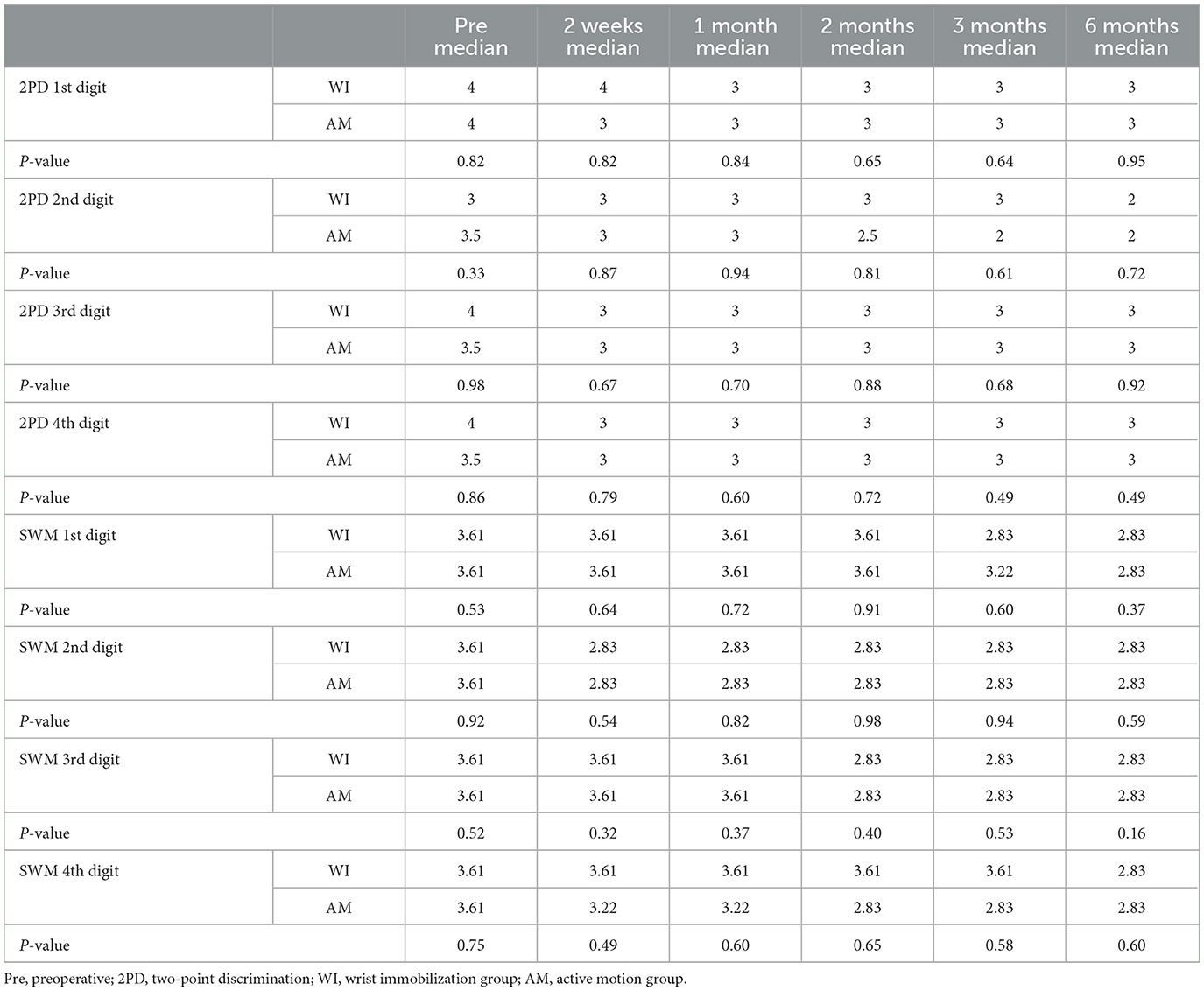
Table 3. Outcome measures of sensibility.
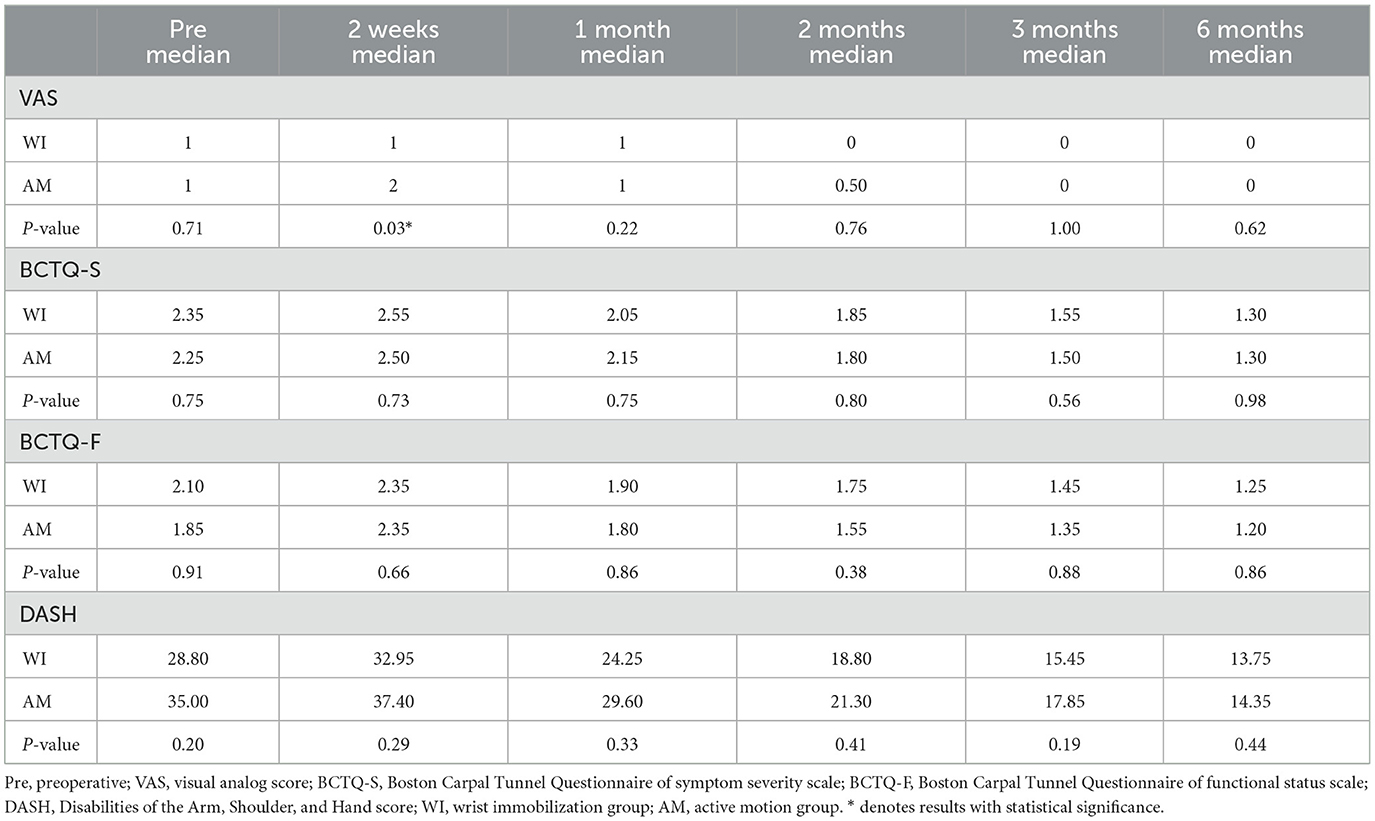
Table 4. Outcome measures of VAS and self-evaluation.
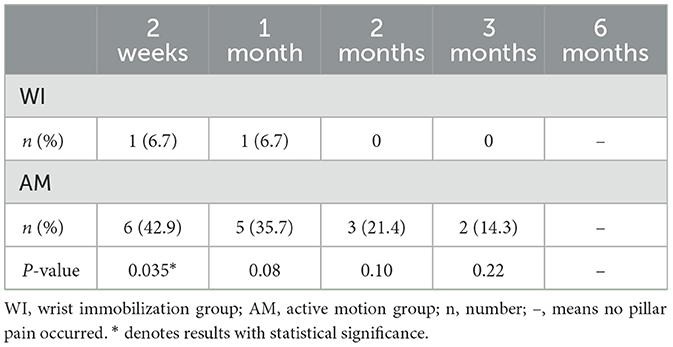
Table 5. Outcome measures regarding the occurrence of pillar pain.
This study assessed postoperative outcome measures of wrist immobilization for 2 weeks following ECTR, compared to active mobilization with no restriction. Our results demonstrated that wrist immobilization significantly improved postoperative pain and strength rehabilitation at early follow-up, whereas there was no significant difference between the two groups regarding postoperative sensibility, flexibility, and self-evaluation. Interestingly, there was no significant difference between both groups in any outcome measure at the final follow-up.
ECTR has increasingly become popular worldwide (1–3). Though significant emphasis has been put on the strengths and limitations between ECTR and open carpal tunnel release (OCTR) (5–8), the postoperative protocol has been largely understudied. To minimize the complications, some surgeon traditionally immobilizes the wrist in question for 1–4 weeks after OCTR (25, 26). An increasing body of evidence suggests that wrist immobilization following OCTR is ineffective and adversely affects postoperative rehabilitation (10–13, 16, 17, 19). However, relevant study concerning wrist immobilization following ECTR is rare. The published literature does not recommend wrist immobilization or not after ECTR. Due to a lack of thorough understanding, some trials allowed initial mobilization while others recommended a plaster splint casting at early stages with variable duration of immobilization (from 48 h to 2 weeks) (14, 15, 18).
In this study, the outcome measures of sensibility improved sustainably in both groups, especially 1 month after ECTR, consistent with the literature. All patients benefited from ECTR and showed no obvious indication of incomplete release. Moreover, the sensibility of both groups at every time point was comparable, which suggested compressive nerve recovery after release was not disturbed by external splint casting.
Postoperative pain peaked at 2 weeks and was initially alleviated at 1 month after ECTR in both groups. At 2 weeks after ECTR, the wrist immobilization group exhibited better outcomes in VAS and pillar pain occurrence than the active motion group. Although pillar pain occurrence between the two groups differed by almost 30% at 1 month postoperatively, this difference did not reach statistical significance, which might be attributed to inadequate sample size. Subsequently, the two groups showed comparable outcomes regarding postoperative pain and achieved satisfactory results at the final follow-up. This difference could be related to stimulation by tiny subcutaneous hematoma and palmar cutaneous branches (27). The premature active motion can reportedly delay nerve recovery and swelling regression. In contrast, wrist immobilization for 2 weeks favored alleviation of the micro-circumstances and relief of nerve edema.
The change in postoperative strength showed a similar tendency to postoperative pain (13, 28). It took nearly 2 months for both groups to recover normal strength, which could provide a reference for the therapist to formulate accurate postoperative physiotherapy. As stated, the wrist immobilization group yielded greater strength than the active motion group at 2 weeks after ECTR. Various factors accounted for this difference although postoperative pain was the predominant cause. After pain alleviation and wound healing, wrist strength got improved 1 month after ECTR. At the final follow-up, the strength of both groups was stronger than the baseline, which was attributed to the recovery of the median nerve and the corresponding innervated muscles.
Postoperative flexibility and self-evaluation demonstrated no significant difference between these two groups in the whole follow-up. The DASH outcome measures at 2 weeks after ECTR was superior in the wrist immobilization group although this difference was not significant. This finding implied that pain and slight strength did not influence the daily routine.
No severe complications like bowstringing of the flexor tendons occurred, which showed the safety of ECTR. In total, two subjects in the wrist mobilization group complained of scar discomfort, which got worse during grip. Moreover, they both felt discomfortable with a scar on the palm rather than the forearm. Despite a lack of theoretical support, we considered that premature active motion, especially grip, would stimulate the cutaneous nerve in this region and cause discomfort.
The outcome measures of ECTR in this study are in accordance with the literature (29–32). This is the first study to compare the outcome of wrist immobilization and active motion after ECTR, which provides novel insights. Earlier studies have demonstrated little value of wrist immobilization after OCTR, and the outcomes even worsened with early immobilization. As already mentioned, splint casting would weaken the strength and cause stiffness of the wrist, which in turn delayed rehabilitation (13). However, we found that wrist immobilization is necessary for the early stage and contributes to symptom relief at 2 weeks postoperatively. This discrepancy may be attributed to the difference in the surgical technique. Due to the limited visualization, ECTR was considered with a higher risk of nerve damage compared with OCTR (5). Early immobilization may contribute to the recovery of the nerve. However, this damage is almost reversible and transient, and the symptoms will relieve with time pass in both groups. Further studies should be carried out to explain this discrepancy clearly.
Several limitations in this study should be given attention. First, the sample size was relatively small, which could easily cause bias and error. Moreover, this is a single-center study, and the findings only represent this single-center, which limits the generalization of our conclusions. Some outcome measures assessed are subjective, while objective outcome measures, such as EMG, were not analyzed. Hence, further multiple-center studies with large sample sizes are warranted for a more comprehensive investigation of outcome measures.
Wrist immobilization for 2 weeks contributes to pain alleviation and improved grip and pinch strength during early follow-up. It brings no significant benefits in terms of improvement of sensibility, flexibility, and self-evaluation. At the final follow-up, wrist immobilization yielded no obvious significance compared with initial active motion. Therefore, wrist immobilization for 2 weeks is warranted after ECTR of idiopathic carpal tunnel syndrome.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding authors.
The studies involving human participants were reviewed and approved by Ethics Committee of WuXi No. 9 People's Hospital Affiliated to SooChow University. The patients/participants provided their written informed consent to participate in this study.
GZ and YR designed this study. HJ, ZL, HY, QZ, and JM worked on data acquisition. FZ and HJ created tables and charts. FZ analyzed the data and drafted this manuscript. GZ revised and finished this manuscript. All authors contributed to the article and approved the submitted version.
This study was supported by the Subsidy Program for Young and Middle-aged Top Talents of Wuxi Municipal Health Commission, the Postdoctoral Research Funding Program of Jiangsu Province (2020Z359), and the Binhu Medical Expert Team of “Light of Binhu Program”.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Joshi A, Patel K, Mohamed A, Oak S, Zhang MH, Hsiung H, et al. Carpal tunnel syndrome: pathophysiology and comprehensive guidelines for clinical evaluation and treatment. Cureus. (2022) 14:e27053. doi: 10.7759/cureus.27053
2. Genova A, Dix O, Saefan A, Thakur M, Hassan A. Carpal tunnel syndrome: a review of literature. Cureus. (2020) 12:e7333. doi: 10.7759/cureus.7333
3. Hacquebord JH, Chen JS, Rettig ME. Endoscopic carpal tunnel release: techniques, controversies, and comparison to open techniques. J Am Acad Orthop Surg. (2022) 30:292–301. doi: 10.5435/JAAOS-D-21-00949
4. Wu YX, Yin H, Lin JY, Jiang HJ, Han F, Liu SD, et al. Our 15-year experience of complications of Chow's technique for endoscopic carpal tunnel releasing. Neurol Res. (2022) 44:761–5. doi: 10.1080/01616412.2022.2051134
5. Shin EK. Endoscopic versus open carpal tunnel Release. Curr Rev Musculoskelet Med. (2019) 12:509–14. doi: 10.1007/s12178-019-09584-0
6. Williamson ERC, Vasquez Montes D, Melamed E. Multistate comparison of cost, trends, and complications in open versus endoscopic carpal tunnel release. Hand. (2021) 16:25–31. doi: 10.1177/1558944719837020
7. Miles MR, Shetty PN, Bhayana K, Yousaf IS, Sanghavi KK, Giladi AM. Early outcomes of endoscopic versus open carpal tunnel release. J Hand Surg Am. (2021) 46:868–76. doi: 10.1016/j.jhsa.2021.04.030
8. Michelotti BM, Vakharia KT, Romanowsky D, Hauck RM. A prospective, randomized trial comparing open and endoscopic carpal tunnel release within the same patient. Hand. (2020) 15:322–6. doi: 10.1177/1558944718812129
9. Koong DP, An VVG, Nandapalan H, Lawson RD, Graham DJ, Sivakumar BS. Open versus single- or dual-portal endoscopic carpal tunnel release: a meta-analysis of randomized controlled trials. Hand. (2022). doi: 10.1177/15589447221075665 [Epub ahead of print].
10. Isaac SM, Okoro T, Danial I, Wildin C. Does wrist immobilization following open carpal tunnel release improve functional outcome? A literature review. Curr Rev Musculoskelet Med. (2010) 3:11–7. doi: 10.1007/s12178-010-9060-9
11. Martins RS, Siqueira MG, Simplício H. Wrist immobilization after carpal tunnel release: a prospective study. Arq Neuropsiquiatr. (2006) 64(3a):596–9. doi: 10.1590/S0004-282X2006000400013
12. Shalimar A, Nor-Hazla MH, Arifaizad A, Jamari S. Splinting after carpal tunnel release: does it really matter? Malays Orthop J. (2015) 9:41–6. doi: 10.5704/MOJ.1507.011
13. Svegard J, Nordvall Persson A, Zetterlund C, Alkner B. Comparison of use of plaster casting versus elastic bandage following carpal tunnel release: a randomized controlled study. J Rehabil Med. (2021) 53:jrm00168. doi: 10.2340/16501977-2788
14. Bury TF, Akelman E, Weiss AP. Prospective, randomized trial of splinting after carpal tunnel release. Ann Plast Surg. (1995) 35:19–22. doi: 10.1097/00000637-199507000-00004
15. Logli AL, Bear BJ, Schwartz EG, Korcek KJ, Foster BJ. A prospective, randomized trial of splinting after minicarpal tunnel release. J Hand Surg Am. (2018) 43:775.e1–8. doi: 10.1016/j.jhsa.2018.01.016
16. Cook AC, Szabo RM, Birkholz SW, King EF. Early mobilization following carpal tunnel release. A prospective randomized study. J Hand Surg Br. (1995) 20:228–30. doi: 10.1016/S0266-7681(05)80057-9
17. Finsen V, Andersen K, Russwurm H. No advantage from splinting the wrist after open carpal tunnel release. A randomized study of 82 wrists. Acta Orthop Scand. (1999) 70:288–92. doi: 10.3109/17453679908997810
18. Cebesoy O, Kose KC, Kuru I, Altinel L, Gul R, Demirtas M. Use of a splint following open carpal tunnel release: a comparative study. Adv Ther. (2007) 24:478–84. doi: 10.1007/BF02848769
19. Bhatia R, Field J, Grote J, Huma H. Does splintage help pain after carpal tunnel release? J Hand Surg Br. (2000) 25:150. doi: 10.1054/jhsb.2000.0365
20. Graham B, Peljovich AE, Afra R, Cho MS, Gray R, Stephenson J, et al. The American Academy of Orthopaedic Surgeons evidence-based clinical practice guideline on: management of carpal tunnel syndrome. J Bone Joint Surg Am. (2016) 98:1750–4. doi: 10.2106/JBJS.16.00719
21. Stevens JC. Aaem minimonograph #26: the electrodiagnosis of carpal tunnel syndrome. American Association of Electrodiagnostic Medicine. Muscle Nerve. (1997) 20:1477–86. doi: 10.1002/(sici)1097-4598(199712)20:12<1477::aid-mus1>3.0.co;2-5
22. Mahmood B, Chongshu C, Qiu X, Messing S, Hammert WC. Comparison of the Michigan hand outcomes questionnaire, Boston carpal tunnel questionnaire, and promis instruments in carpal tunnel syndrome. J Hand Surg Am. (2019) 44:366–73. doi: 10.1016/j.jhsa.2018.10.031
23. Lo IN, Hsu PC, Huang YC, Yeh CK, Yang YC, Wang JC. Dynamic ultrasound assessment of median nerve mobility changes following corticosteroid injection and carpal tunnel release in patients with carpal tunnel syndrome. Front Neurol. (2021) 12:710511. doi: 10.3389/fneur.2021.710511
24. Angst F, Schwyzer HK, Aeschlimann A, Simmen BR, Goldhahn J. Measures of adult shoulder function: Disabilities of the Arm, Shoulder, and Hand Questionnaire (DASH) and Its Short Version (Quickdash), Shoulder Pain and Disability Index (SPADI), American Shoulder and Elbow Surgeons (ASES) Society Standardized Shoulder Assessment Form, Constant (Murley) Score (CS), Simple Shoulder Test (SST), Oxford Shoulder Score (OSS), Shoulder Disability Questionnaire (SDQ), and Western Ontario Shoulder Instability Index (WOSI). Arthritis Care Res. (2011) 63:S174–88. doi: 10.1002/acr.20630
25. McDowell D, Garwood M, Barnes D, Minott M. Endoscopic carpal tunnel release in Jamaica–seven years experience. West Indian Med J. (2012) 61:158–62.
26. Chen Z, Liu J, Yuan TB, Cai DW, Wang XX, Qin J. Comparison of clinical outcomes between open and modified endoscopic release for carpal tunnel syndrome. Exp Ther Med. (2021) 22:861. doi: 10.3892/etm.2021.10293
27. Mujadzic T, Friedman HI, Mujadzic MM, Gober C, Chen E, Atwez A, et al. Modified carpal tunnel release: a new approach to minimizing pillar pain. Ann Plast Surg. (2021) 86(6S Suppl 5):S503–9. doi: 10.1097/SAP.0000000000002885
28. Schroeder J, Malige A, Rodriguez W, Liongson F, Matullo K. Outcomes of endoscopic carpal tunnel release surgery with home guided hand therapy versus no hand therapy: a prospective randomized controlled trial after endoscopic carpal tunnel release. Hand. (2022). doi: 10.1177/15589447221122824. [Epub ahead of print].
29. Teh KK, Gunasagaran J, Choo CH, Ahmad TS. A novel supraretinacular endoscopic carpal tunnel release: surgical technique, clinical efficacy and safety (a series of 48 consecutive cases). J Hand Surg Glob Online. (2021) 3:329–34. doi: 10.1016/j.jhsg.2021.06.011
30. Sato K, Murakami K, Mimata Y, Takahashi G, Doita M. Supraretinacular endoscopic carpal tunnel release: a safe alternative method for treatment of carpal tunnel syndrome. J Orthop Surg. (2021) 29:2309499021993407. doi: 10.1177/2309499021993407
31. Wellington I, Cusano A, Ferreira JV, Parrino A. WALANT technique versus sedation for endoscopic carpal tunnel release. Hand. (2023) 18:214–21. doi: 10.1177/15589447211003180
32. Oertel J, Schroeder HW, Gaab MR. Dual-portal endoscopic release of the transverse ligament in carpal tunnel syndrome: results of 411 procedures with special reference to technique, efficacy, and complications. Neurosurgery. (2006) 59:333–40. discussion 40. doi: 10.1227/01.NEU.0000223500.25131.99
Keywords: carpal tunnel syndrome, median nerve, transverse carpal ligament, endoscopic carpal tunnel release, immobilization
Citation: Zhang F, Jiang H, Lu Z, Yang H, Zhang Q, Mi J, Rui Y and Zhao G (2023) The significance of wrist immobilization for endoscopic carpal tunnel release. Front. Neurol. 14:1081440. doi: 10.3389/fneur.2023.1081440
Received: 27 October 2022; Accepted: 30 March 2023;
Published: 25 April 2023.
Edited by:
Hui Lu, Zhejiang University, ChinaCopyright © 2023 Zhang, Jiang, Lu, Yang, Zhang, Mi, Rui and Zhao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gang Zhao, emhhb2dhbmdtZEBzdWRhLmVkdS5jbg==; Yongjun Rui, d3hzd2tyeWpAMTYzLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.