 Natalia Pożarowszczyk1
Natalia Pożarowszczyk1 Iwona Kurkowska-Jastrzębska1Iwona Sarzyńska-Długosz2Maciej Nowak1
Iwona Kurkowska-Jastrzębska1Iwona Sarzyńska-Długosz2Maciej Nowak1 Michał Karliński1*
Michał Karliński1*- 12nd Department of Neurology, Institute of Psychiatry and Neurology, Sobieskiego, Warsaw, Poland
- 2Neurological Rehabilitation Ward, Institute of Psychiatry and Neurology, Sobieskiego, Warsaw, Poland
Introduction: The Modified Rankin Scale (mRS) is the most common tool to quantify post-stroke disability in everyday practice and by certified raters in clinical trials. However, interobserver variability may affect reliability of retrospective observational studies, including clinical registries. Our aim was to assess real-life consistency between neurologists and physical and rehabilitation medicine physicians using mRS to rate post-stroke disability of patients transferred directly from stroke unit (SU) to rehabilitation ward (RW).
Methods: This is a retrospective analysis of 132 consecutive acute stroke patients transferred from single tertiary SU to RW located in the same hospital in Poland. Patients were assessed by one rater from each department at the day of transfer. We distinguished between physicians previously certified in using mRS for clinical trials and not-certified physicians using mRS in everyday practice.
Results: mRS at discharge from SU and on admission to RW was recorded for 105 of 132 patients. The overall agreement was 70.5% (kappa 0.55). Similar agreement was observed in the subset of 30 patients rated by certified physicians in both departments (70.0%, kappa 0.57) and in the subset of 61 patients rated by a pair of certified neurologist and not-certified rehabilitation physician (73.8%, kappa 0.58).
Conclusions: Everyday consistency between raters from SU and RW in using mRS is modest as in previous validation studies. However, it may be considered sufficient for the purpose of observational studies or stroke registries. It emphasizes the need for easily accessible training in conventional mRS or implementation of specialized tools with predefined questions.
Introduction
The modified Rankin Scale (mRS) has been the gold standard for measuring stroke outcome in clinical trials from many years (1–3). As a consequence, it has also become the standard in observational studies and is recommended for everyday use in clinical practice of stroke units and rehabilitation wards all over the world (1–3). This ordinal scale which grades patient's disability from 0 (no symptoms) to 6 (death) is able to capture the whole spectrum of functional states and poses intuitive simplicity (3–5). Despite those major advantages, the issue of significant interobserver variability may lead to end point misclassification and can affect results of clinical studies (6–8).
The attempts to improve the reliability of mRS assessment include the development structured interview, a formal simplified mRS questionnaire (smRSq) and introduction of certification video-based training provided by Glasgow University (trainingcampus.net) (9–12). However, most observational studies and multicenter registries are based on data collected in the course of everyday clinical practice. The assessments are made by attending physicians of different clinical backgrounds who are not always aware of all nuances of mRS and not as dedicated as investigators in clinical trials. This may rise an important question about the bias in retrospective analyses of observational data extracted from clinical records.
Our aim was to assess the real-life consistency between neurologists and physical and rehabilitation medicine (PRM) physicians using mRS to rate post-stroke disability in patients transferred directly from a stroke unit (SU) to a rehabilitation ward (RW).
Methods
This is a retrospective analysis of all consecutive adult acute stroke patients treated in a single tertiary SU from January 2017 to December 2019 and were subsequently transferred to RW located in the same hospital in Warsaw, Poland.
Post-stroke disability was routinely measured using mRS (i) at the discharge from SU by the neurologist or neurologist trainee and (ii) on admission to RW by the specialist in PRM or PRM trainee. Some physicians working in the RW were also specialists in neurology. It is important to note that both mRS assessments were made at the day of transfer which makes significant changes in patients' functional state highly unlikely. The final analysis included only patients having mRS score stated directly in the last observation or discharge note from SU and stated directly in the initial observation or discharge note from RW. There were no exclusion criteria.
We additionally distinguished between (i) physicians who within the last 5 years preceding patients' assessment at least once completed formal mRS certification at trainingcampus.net for the purpose of clinical trials (certified mRS raters) and (ii) physicians who used the scale only as a part of everyday practice (non-certified mRS raters). The authors knew the mRS certification status of involved physicians, as they were either principal investigators (IK-J) or sub-investigators (MK, IS-D) in all stroke trials carried out in both departments within the last 10 years.
Statistical analysis
Categorical variables were presented as a number of valid observations and proportions calculated with exclusion of unknown values from the denominator. Continuous variables were presented as a median with interquartile range (1st quartile to 3rd quartile, Q1–Q3) due to non-normal distribution. Consistency between the raters from SU and the raters from RW was expressed using Cohen's kappa. Considering potential differences in competence, we also planned to calculate the agreement in the following subgroups: (A) certified mRS rater in SU and certified mRS rater in RW; (B) certified mRS rater in SU and non-certified mRS rater in RW; (C) non-certified mRS rater in SU and certified mRS rater in RW; (D) non-certified mRS rater in SU and non-certified mRS rater in RW (Figure 1).

Figure 1. Study population. mRS, modified Rankin scale; RW, rehabilitation ward; SU, stroke unit.
We calculated the proportions of patients who on admission to the RW received mRS score that was either identical, higher or lower than the score given at the discharge from SU. Then we compared the proportions of higher mRS scores at the discharge from SU and on admission to RW. Additional sensitivity analysis was conducted to compare the patients included in the main analysis and the patients excluded due to lack of double mRS assessment made by both SU and RW physicians.
Calculations were carried out using STATISTICA 13.3 software package (TIBCO Software Inc., USA). For comparisons Chi square test, two-tailed Fisher's exact and Mann-Whitney U test were used, as appropriate. P values of <0.05 were considered statistically significant.
Results
During the 24-month study period a total of 132 acute stroke patients were transferred directly from SU to RW, of whom 105 (79.5%) had the mRS score reported both at discharge from SU and on admission to RW. The remaining 27 patients had no information about the mRS score at discharge from SU and therefore were excluded from the main analysis (Figure 1). Compared to the analyzed cohort, excluded patients were significantly more often male (77.8 vs. 49.5%, p = 0.008) and less often discharged from SU by a certified mRS rater (70.4 vs. 86.7%, p = 0.043) (Table 1).
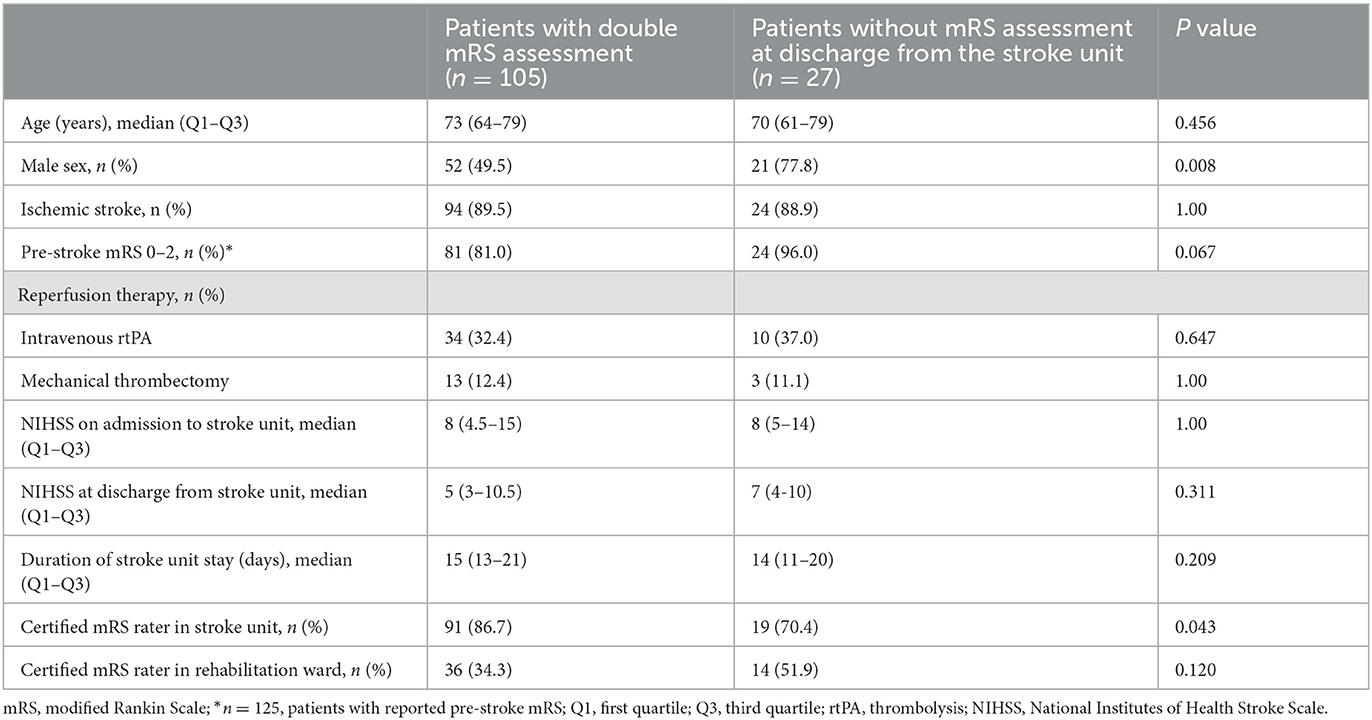
Table 1. Basic characteristics of the analyzed cohort and patients excluded due to lack of double mRS assessment.
Patients from the analyzed cohort had a median age of 73 years, were in 89.5% independent (mRS 0–2) before stroke and were transferred to RW with median of 5 points at National Institutes of Health Stroke Scale (NIHSS) after a median of 15 days of stay in SU (Table 1). The proportion of patients assessed by a certified mRS rater was significantly higher in SU (86.7 vs. 34.3%, p <0.001).
Regardless of raters' certification status, the neurologists discharging from SU and the physicians admitting to RW reported identical mRS scores in 70.5% with Cohen's kappa 0.55 (Table 2). Similar findings were observed in subgroup A (n = 30; 70.0% of identical scores, kappa 0.57) and subgroup B (n = 61, 73.8% of identical scores, kappa 0.58). PRM physicians more often reported higher scores than SU physicians overall (20.0 vs. 9.5%, p = 0.050) and in subgroup A (26.7 vs. 3.3%, p = 0.026), however such difference was not observed in subgroup B (14.8 vs. 11.5%, p = 0.592). The number of cases in subgroups C (n = 6) and subgroup D (n = 8) was too low for detailed reporting and further statistical analysis.
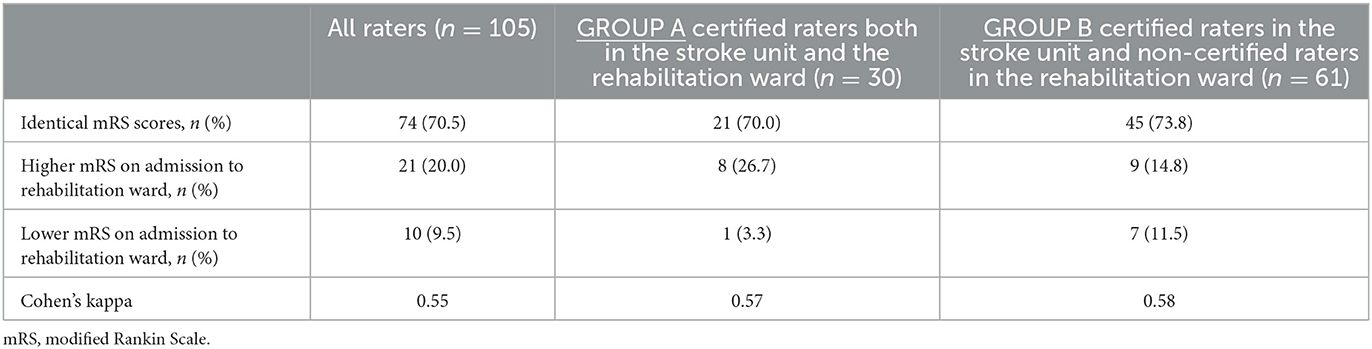
Table 2. Interrater consistency in mRS scoring in stroke unit and rehabilitation ward.
A matrix of mRS scores for subgroups A and B are presented in Table 3 and a matrix of mRS scores incorporating all 132 patients (including cases with not recorded mRS score at discharge from SU) are presented in Table 4.
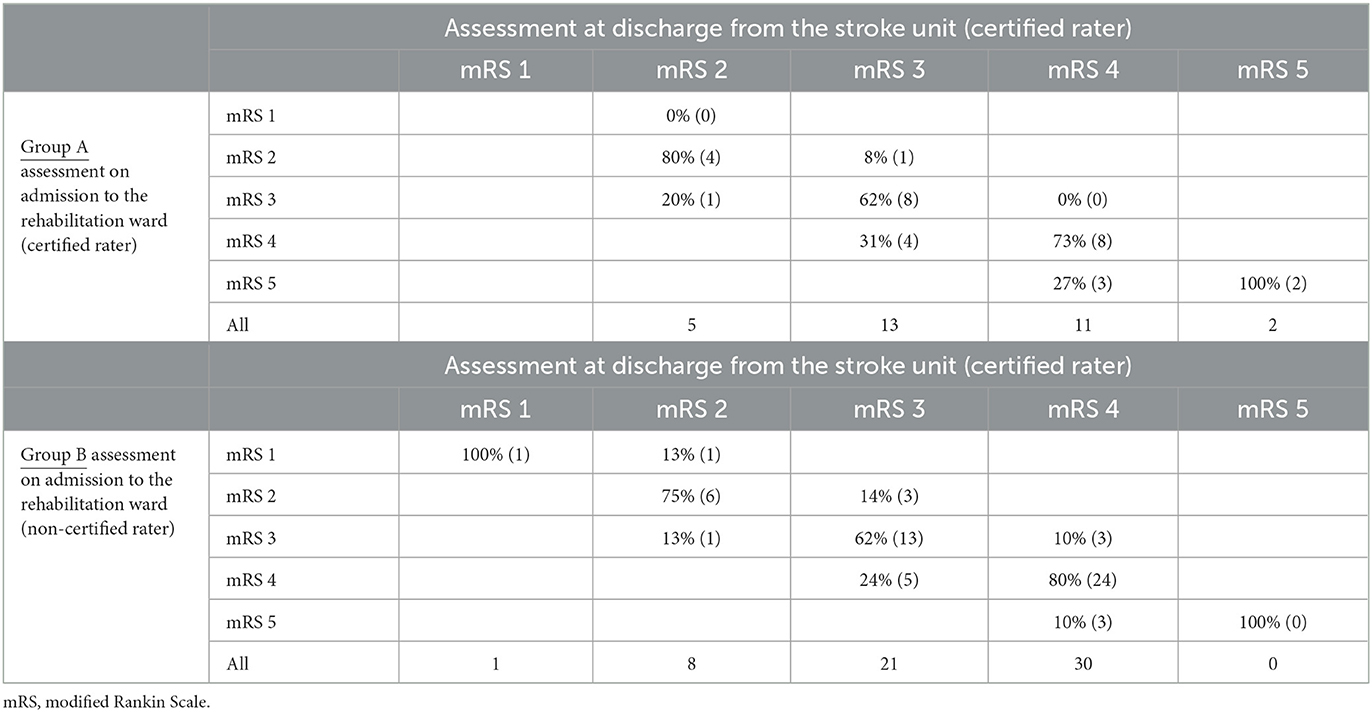
Table 3. Cross tabulation of mRS scores for subgroups of patients depending on the certification status of raters (subgroups A and B).
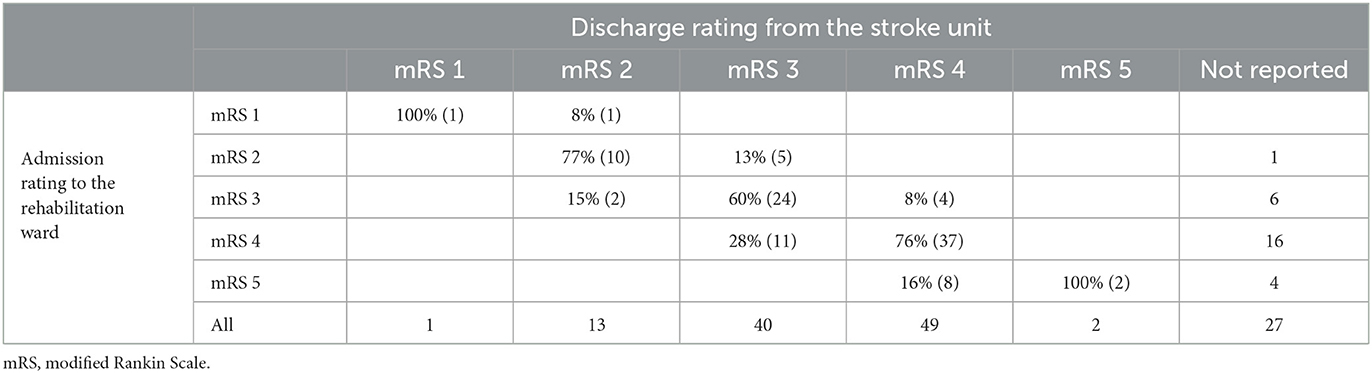
Table 4. Cross tabulation of mRS scores for all analyzed patients.
Discussion
The first version of scale was developed by John Rankin more than 60 years ago and consisted of 5 briefly described states (1 to 5) with no clear criteria for distinguishing between particular levels of disability (11). The scale was modified in the year 1988 by adding grades 0 and 6, which made the scale capable of capturing the whole spectrum of functional states (from no symptoms to death) but still burdened with significant interobserver variability (3, 7, 13, 14).
The first attempts to improve the reliability of mRS assessment included development of simple structured interview and subsequently the development of smRSq (8–10). The smRSq questionnaire includes a few pre-defined yes-or-no questions which helps to distinguish between different levels of post-stroke disability (8–10). The smRSq shows adequate agreement with the standard mRS and it can be useful in standard face-to-face interviews, telephone interviews or in creating online forms. Its reliability is superior to the standard mRS, but still not optimal (10, 11, 15, 16). Another attempt was the introduction of certification video-based training provided by Glasgow University (trainingcampus.net). Unfortunately, the training is available only in English and certification is not free from charge.
Suboptimal consistency of assessment driven by general rules biased by physicians' intuition led to development Rankin Focused Assessment (RFA). The RFA is an independent tool with a checklist that incorporates a detailed structured interview in line with mRS (4). Such form urges the rater to ask all pivotal questions and increases the reliability up to 93% (4, 16). Other proposed approaches to optimize functional assessment after stroke include miFUNCTION scale and utility-weighted mRS (UW-mRS) (16–21).
Unlike previous analyzes addressing the issue of interobserver variability of mRS scoring, our study provides real-life data about performance of physicians using the scale for the purpose of their everyday practice in the early post-acute phase of stroke. All raters were experienced in treating patients after stroke but they represented two different types of clinical background (SU and RW). Their mRS assessments were made with no pressure on precision, that may be exerted by awareness of being a clinical trial investigator or a participant in a validation project. The physicians could use any tool to capture the mRS score. However, knowing the clinical routine in both departments, it may be assumed that they used either smRSq or original mRS, not the RFA. The observed overall consistency of 70.5% with Cohen's kappa 0.55 shown in our study is similar to what has been reported for the smRSq in validation studies (8–12).
Interestingly, the nominal raters' competence understood as obtaining the mRS certificate for the purpose of clinical trials within the few preceding years did not seem to directly improve consistency. This may indicate that the added value of formal training program requires regular retraining or that the precision of certified raters is simply lower in the setting of everyday practice.
We found that the physicians admitting patients to RW had a strong tendency to rate disability higher than the neurologists discharging patients from SU. Noteworthy, this phenomenon was restricted to PRM physicians who completed the certification program. One may hypothesize that SU neurologist (i) tends to concentrate on the disability attributed only to the residual neurological deficits, (ii) only approximates how the patient could handle activities of daily living by observing him in an artificial SU environment and (iii) prefers to see the outcome of SU stay in a positive way. As a consequence, the SU neurologist may involuntarily underestimate the level of disability at discharge from SU.
On the other hand, PRM physician (i) may tend to perceive the patient's functional status in a more complex way including both activity and participation, (ii) is able to see the patient confronting more complex environment and his actual attempts to perform some activities of daily living in RW, and (iii) see the potential for measurable improvement during RW stay. As a consequence, the PRM physician may involuntarily overestimate the level of disability on admission to RW.
This abovementioned one-way skew disappeared when the assessment on admission to RW was done by a non-certified physician. In this subgroup (B) PRM physicians scored disability either higher or lower than the SU neurologists without any pattern. It may indicate that the formal training in mRS equalizes the competence and therefore reveals the background-related cognitive systematic error dependent on the rater background.
Strengths and limitations
The most important strength of the presented study is the fact that it reflects real-life everyday practice. It is important to note that the moderate inconsistency indicates that the mRS reported on admission to RW is not a simple copy of what has been stated in the discharge note from SU. mRS is used as an outcome measure for both acute stroke studies and rehabilitation studies (15, 17). This is the first study that directly compares the mRS assessments between SU and PRM physicians and generates several hypotheses, which may deserve to be addressed in the future.
The retrospective design allowed to collect data unbiased by the awareness of raters that their performance will be externally evaluated or that their imprecise scoring may affect results of an important clinical trial. On the other hand, such method made impossible to decide which mRS assessment is correct in case of disagreement. It should also be noted that RW physicians were aware of the mRS scores given at the discharge from the SU. However, the level of discrepancy may indicate that both assessments were independent.
Transferring post-stroke patients from SU to RW is a common practice in stroke care (22, 23), but our findings refer directly to the subset of patients who require intensive neurological hospital rehabilitation and seem capable of benefiting from RW activities. In our cohort there were almost no patients without or with mild post-stroke disability (only one patient with mRS 1 and no cases with mRS 0) and almost no patients with severe disability (only two cases with mRS 5). Noteworthy, in Poland difficult access to reimbursed outpatient rehabilitation may lead to a higher proportion of patients with mRS 2 stayed in RW than in other health care systems.
The exclusion of a small subgroup of patients due to lack of mRS score stated directly at the time of discharge from SU was unlikely to introduce significant bias. The study accounted for all four combinations of certified and non-certified mRS raters. However, the number of observations was sufficient to perform statistical analysis only in two most important combinations (A and B).
Conclusions
Our findings provide important reassurance that the reliability of mRS assessment made in everyday clinical practice of SU and RW is modest as in the validation studies. Therefore, it may be considered sufficient for the purpose of observational studies or stroke registries.
The tendency among neurologists to underrate disability at discharge from SU or the tendency among PRM physicians to overrate disability on admission to RW is a new observation that deserves further studies. Such studies should include additional reference mRS assessment to identify which physician scores correctly.
It seems reasonable to put additional efforts in improvement the reliability of mRS assessment either by incorporating repeated mRS training in the curriculum of all physicians involved in stroke care or by complementing of using specially designed mRS forms such as the RFA which navigates raters through the pivotal points of the interview.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author contributions
NP conceived and designed the study, collected data, performed statistical analysis, interpreted results, drafted the manuscript, and provided approval of the final version for publication. IK-J, IS-D, and MN interpreted results, revised the manuscript for important intellectual content, and provided approval of the final version for publication. MK conceived and designed the study, performed statistical analysis, interpreted results, revised the manuscript for important intellectual content, and provided approval of the final version for publication. All authors contributed to the article and approved the submitted version.
Funding
The study was supported from the statutory grant of the Institute of Psychiatry and Neurology in Warsaw, Poland for stroke research.
Acknowledgments
The authors would like to acknowledge the multidisciplinary teams of our SU and RW for their dedication to deliver the best available care.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. (2019) 50:e344–418. doi: 10.1161/STR.0000000000000211
2. Błazejewska-Hyzorek B, Członkowska A, Czernuszenko A, Ferens A, Gasecki D, Kazcorowski R, et al. Wytyczne postepowania w udarze mózgu [Polish stroke guidelines]. Pol Przeglad Neuol. (2019) 15:1–164. doi: 10.5603/PPN.2019.0001
3. Banks JL, Marotta CA. Outcomes validity and reliability of the modified Rankin Scale: Implications for Stroke Clinical Trials. Stroke. (2007) 38:1091–6. doi: 10.1161/01.STR.0000258355.23810.c6
4. Saver JL, Filip B, Hamilton S, Yanes A, Craig S, Cho M, et al. Improving the reliability of stroke disability grading in clinical trials and clinical practice: The Rankin Focused Assessment (RFA). Stroke. (2010) 41:992–5. doi: 10.1161/STROKEAHA.109.571364
5. Nunn A, Bath PM, Gray LJ. Analysis of the modified Rankin Scale in randomised controlled trials of acute ischaemic stroke: a systematic review. Stroke Res Treat. (2016) 2016:1–7. doi: 10.1155/2016/9482876
6. Quinn TJ, Dawson J, Walters MR, Lees KR. Variability in modified Rankin scoring across a large cohort of international observers. Stroke. (2008) 39:2975–9. doi: 10.1161/STROKEAHA.108.515262
7. Quinn TJ, Dawson J, Walters MR, Lees KR. Reliability of the modified Rankin Scale. Stroke. (2009) 40:3393–5. doi: 10.1161/STROKEAHA.109.557256
8. Zhao H, Collier J, Quah D, Purvis T, Bernhardt J. The modified Rankin Scale in acute stroke has good inter-rater-reliability but questionable validity. Cerebrovasc Dis. (2010) 29:188–93. doi: 10.1159/000267278
9. Wilson J, Hareendran A, Grant M, Baird T, Schulz U, Muir K, et al. Improving the assessment of outcomes in stroke - use of a structured interview to assign grades on the Modified Rankin scale. Stroke. (2002) 33:2243–6. doi: 10.1161/01.STR.0000027437.22450.BD
10. Bruno A, Akinwuntan AE, Lin C, Close B, Davis K, Baute V, et al. Simplified modified Rankin Scale questionnaire: Reproducibility over the telephone and validation with quality of life. Stroke. (2011) 42:2276–9. doi: 10.1161/STROKEAHA.111.613273
11. Chen X, Li J, Anderson CS, Lindley RI, Hackett ML, Robinson T, et al. Validation of the simplified modified Rankin scale for stroke trials: Experience from the ENCHANTED alteplase-dose arm. Int J Stroke. (2021) 16:222–8. doi: 10.1177/1747493019897858
12. Wilson J, Hareendran A, Hendry A, Potter J, Bone I, Muir K. Reliability of the modified Rankin Scale across multiple raters: benefits of a structured interview. Stroke. (2005) 36:777–81. doi: 10.1161/01.STR.0000157596.13234.95
13. Bath PM, Lees KR, Schellinger PD, Altman H, Bland M, Hogg C, et al. Statistical analysis of the primary outcome in acute stroke trials. Stroke. (2012) 43:1171–8. doi: 10.1161/STROKEAHA.111.641456
14. Rankin J. Cerebral vascular accidents in patients over the age of 60: II. Prognosis Scott Med J. (1957) 2:200–15. doi: 10.1177/003693305700200504
15. Dutta D, Foy C, Ramadurai G, Obaid M, Bruno A. Initial testing of an electronic application of the simplified modified Rankin Scale questionnaire (e-smRSq). J Stroke Cerebrovasc Dis. (2020) 29:1–5. doi: 10.1016/j.jstrokecerebrovasdis.2020.105024
16. Broderick JP, Adeoye O, Elm J. Evolution of the modified Rankin Scale and its use in future stroke trials. Stroke. (2017) 48:2007–12. doi: 10.1161/STROKEAHA.117.017866
17. Dijkland SA, Voormolen DC, Venema E, Roozenbeek B, Polinder S, Haagsma JA, et al. Utility-weighted modifed Rankin scale as primary outcome in stroke trials a simulation study. Stroke. (2018) 49:965–71. doi: 10.1161/STROKEAHA.117.020194
18. Rethnam V, Bernhardt J, Johns H, Hayward KS, Collier JM, Ellery F, et al. Look closer: The multidimensional patterns of post-stroke burden behind the modified Rankin Scale. Int J Stroke. (2021) 16:420–8. doi: 10.1177/1747493020951941
19. Wang X, Moullaali TJ Li Q, Berge E, Robinson TG, Lindley R, et al. Utility-weighted modified Rankin Scale scores for the assessment of stroke outcome: pooled analysis of 20 000+ patients. Stroke. (2020) 51:2411–7. doi: 10.1161/STROKEAHA.119.028523
20. Zerna C, Burley T, Green TL, Dukelow SP, Demchuk AM, Hill MD. Comprehensive assessment of disability post-stroke using the newly developed miFUNCTION scale. Int J Stroke. (2020) 15:167–74. doi: 10.1177/1747493019840933
21. Patel RD, Starkman S, Hamilton S, Craig S, Grace A, Conwit R, et al. The Rankin Focused Assessment—Ambulation: a method to score the modified Rankin Scale with emphasis on walking ability. J Stroke Cerebrovasc Dis. (2016) 25:2172–6. doi: 10.1016/j.jstrokecerebrovasdis.2015.10.030
22. Bagherpour R, Dykstra DD, Barrett AM, Luft AR, Divani AA, A. comprehensive neurorehabilitation program should be an integral part of a comprehensive stroke center. Front Neurol. (2014) 5:57. doi: 10.3389/fneur.2014.00057
Keywords: stroke, modified Rankin Scale, disability, reliability, consistency, outcome assessment
Citation: Pożarowszczyk N, Kurkowska-Jastrzębska I, Sarzyńska-Długosz I, Nowak M and Karliński M (2023) Reliability of the modified Rankin Scale in clinical practice of stroke units and rehabilitation wards. Front. Neurol. 14:1064642. doi: 10.3389/fneur.2023.1064642
Received: 08 October 2022; Accepted: 06 February 2023;
Published: 03 March 2023.
Edited by:
Jean-Claude Baron, University of Cambridge, United KingdomReviewed by:
Hrvoje Budincevic, University Hospital Sveti Duh, CroatiaJosé Alexandre Bachur, University of Franca, Brazil
Copyright © 2023 Pożarowszczyk, Kurkowska-Jastrzębska, Sarzyńska-Długosz, Nowak and Karliński. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Michał Karliński, bWthcmxpbnNraUBpcGluLmVkdS5wbA==