 Zihua He
Zihua He Jinmei Li
Jinmei Li- Department of Neurology, West China Hospital, Sichuan University, Chengdu, China
Epilepsy is a chronic neurological disorder associated with severe social and psychological effects, and most epilepsy patients often report at least one comorbidity. Accumulating evidence have suggested that lacosamide, a new generation of anti-seizure medications, may exhibit efficacy in the management of both epilepsy and its related comorbidities. Therefore, this narrative review aimed to elucidate the recent advancements regarding the therapeutic role of lacosamide in epilepsy-associated comorbidities. The possible pathophysiological mechanisms between epilepsy and epilepsy-associated comorbidities have been also partially described. Whether lacosamide improves cognitive and behavioral functions in patients with epilepsy has not been conclusively established. Some studies support that lacosamide may alleviate anxiety and depression in epilepsy patients. In addition, lacosamide has been found to be safe and effective in the treatment of epilepsy in people with intellectual disabilities, epilepsy of cerebrovascular etiology, and epilepsy associated with brain tumors. Moreover, lacosamide treatment has demonstrated fewer side effects on other systems. Hence, future larger and higher quality clinical studies are needed to further explore both the safety and efficacy of lacosamide in the treatment of epilepsy-associated comorbidities.
1. Introduction
Epilepsy is a clinically complicated syndrome and a commonly diagnosed neurological disorder. In addition to seizures, a high proportion of patients also develop comorbidities. It has been found that ~50% of adult patients with active epilepsy have comorbid conditions, including somatic as well mental comorbidities, with anxiety and depression being the most common psychiatric comorbidities. A number of previous studies have reported that about 16–23 and 18–22% of patients with epilepsy (PWE) suffered from comorbid depression and anxiety disorders, respectively, with the prevalence of the former in patients with recurrent seizures being as high as 55%. The presence of the psychiatric comorbidities can increase the recurrence, mortality, and severely affect the quality of life in PWE (1–4). Likewise, the various somatic comorbidities can complicate antiepileptic therapy and increase the medical and social burden.
Anti-seizure medications (ASMs) are currently being used as the main treatment for epilepsy. Epilepsy-associated comorbidities have a crucial impact on the treatment decisions, and some ASMs may also influence these comorbidities (5). Consequently, in clinical practice, it is necessary to screen and diagnose the different comorbidities in a timely and accurate manner. This can aid to comprehensively assess the necessity, safety, as well as feasibility of the treatment, which can facilitate the selection of appropriate treatment plan, individualize the therapy based on the etiology and significantly improve the symptoms in PWE (6, 7).
The new ASM lacosamide has been approved for the management of patients with partial-onset seizures because to its effectiveness, safety and tolerability (8–13). The seizures are primarily caused by abnormal excess or synchronization of the neuronal activity (14). The voltage-gated sodium channels (VGSCs) are activated during the membrane depolarization and play a crucial role in the generation and transmission of action potentials in the neurons by controlling the flow of sodium ions across the cell membrane (15). Abnormal activity of VGSCs has been found to closely linked with the pathophysiology of epilepsy (16). In contrast to the conventional sodium channel blocking ASMs (i.e., phenytoin and carbamazepine, etc.), it has been postulated that lacosamide can selectively increase the slow inactivation of VGSCs, thereby controlling the pathophysiological neuronal hyperexcitability by regulating the long-term availability of sodium channels (17–19). Electrophysiologic studies have shown that lacosamide can alter the slow inactivation voltage curve toward hyperpolarization and significantly accelerate the slow inactivation state of VGSCs (20–22). In addition, lacosamide can enhance the slow inactivation of VGSCs at potentials close to the resting membrane potential of the neurons, thus inhibiting action potential generation and neuronal firing (22). Moreover, another recent in vitro study has suggested that lacosamide can bind to fast-inactivated states of VGSCs similarly to other sodium channel blockers, but with slower binding and unbinding kinetics (23). Abnormal axon sprouting can lead to the rewiring of neuronal circuits, which can also contribute to epileptic seizures (24, 25). Collapsin response mediator protein-2 (CRMP2) is a cytoplasmic protein that is expressed mainly in neurons and oligodendrocytes, and can mediate the neuronal polarity, neurite outgrowth and axonal growth (26). Lacosamide may also regulate CRMP2 in an indirect functional interaction to prevent the formation of excitatory synaptic connections in epileptogenesis (5, 27, 28). In addition, to enhance the pharmacological effects, lacosamide can be combined with a variety of ASMs or non-ASMs due to the modest influence of drug-drug interactions during the metabolism (29). In recent years, lacosamide has also been found to have substantial positive effects on multiple epilepsy-associated comorbidities, and thus may lead to novel strategies for the clinical treatment options (3, 29).
2. Epilepsy-associated comorbidities
Epilepsy-associated comorbidities can increase the risk of seizures by up to tenfold, thus suggesting that epilepsy and epilepsy-associated comorbidities share diverse pathophysiological mechanisms (30). Certain comorbidities can induce epilepsy by direct or indirect mechanisms (1), and epilepsy or antiepileptic treatment might also trigger or promote some comorbidities (31). In addition, some shared risk factors or genetics can contribute to the development of epilepsy-associated comorbidities (1, 32).
2.1. The shared pathophysiological mechanisms between epilepsy and epilepsy-associated comorbidities
The common pathophysiological mechanisms of epilepsy and psychiatric disorders involve several complex aspects, including neurotransmitter alterations, hypothalamus-pituitary-adrenal axis (HPA) dysfunction, network/structural abnormalities, and inflammation (30). In PWE or animal models, a decrease in the monoamine neurotransmitters, such as dopamine, 5-hydroxytryptamine, and norepinephrine, can be observed (33), and deficiencies in these neurotransmitters can contribute to the development of diverse psychiatric conditions (34). Amino acid neurotransmitters, such as glutamate and gamma-aminobutyric acid (GABA), also play key roles in normal neuronal signaling, and abnormalities in glutamatergic signaling have been found to be the common pathological basis for the central nervous system related diseases (35). In preclinical experiments, dysregulation of HPA has been observed in animal models of depression as well as status epilepticus (36), and seizure-induced HPA dysfunction can increase the risk of comorbid depression (32). Comorbid psychiatric disorders have been found to be more common in frontal or temporal lobe epilepsy and are associated with abnormal network activity, including abnormalities in the hippocampus and structural changes in the amygdala (36). Disruptions of hippocampal neuron formation can directly increase the susceptibility to psychiatric disorders, while seizures can lead to altered hippocampal neuroplasticity (36, 37). Moreover, hippocampal sclerosis may affect cognition by modulating the reorganization of the cortical area connections (38). It has been reported that up to 90% of temporal lobe epilepsy patients with amygdala enlargement have comorbid depression, and amygdala volume is also closely associated with the mood disorders in PWE (39). Brain-derived neurotrophic factor (BDNF) exhibits a significant pathophysiological role in depression, and it has been suggested that BDNF might enhance seizure susceptibility by inducing the synaptic plasticity (40). Furthermore, inflammatory signaling may be involved in abnormal cerebral development, and the inflammatory factor IL-1β can contribute to epilepsy and major depression by increasing excitation (34).
2.2. Management of epilepsy-associated comorbidities
2.2.1. Screening and evaluation for comorbid psychiatric disorders in epilepsy
Psychiatric comorbidities in PWE are often under-treated because of their late detection (7). Therefore, early identification as well as screening can facilitate prompt intervention, and provide greater medical benefit for PWE (1). The International League Against Epilepsy (ILAE) recommends using the Generalized Anxiety Disorder 7-item scale (GAD-7) as a primary screening scale. Moreover, the Hospital Anxiety and Depression Scale (HADS), the Neurologic Disorders Depression Inventory for Epilepsy (NDDI-E), and the Patient Health Questionnaire (PHQ) can also be employed to screen for anxiety or depression in PWE (7). Attention deficit hyperactivity/impulsivity disorder (ADHD) is one of the most commonly associated comorbidities in children affected with epilepsy, and the ILAE recommends the Strengths and Difficulties Questionnaire (SDQ) as a potential screening tool (level B) (41).
2.2.2. Epilepsy-associated comorbidities and selection of ASMs
The objectives of treatment for epilepsy-associated comorbidities should focus on the positively controlling seizures, as well as reasonable interventions for comorbidities should be developed that can improve the patients' quality of life (4). As research progresses, it has been found that ASMs might have different psychiatric or psychological effects on patients, including the psychiatric and behavioral side effects (PBSEs) (42, 43). Some ASMs have no cognitive effects on PWE (e.g., gabapentin, and lamotrigine), whereas phenytoin sodium, topiramate, and zonisamide can adversely affect the cognition (44). In terms of the mood state, topiramate, zonisamide, and levetiracetam might have negative effects, whereas lacosamide is considered to have generally positive impact but occasionally adverse effects on the mood (44). Levetiracetam and zonisamide are associated with higher risk for PBSEs than other ASMs, although the potential mechanisms are unclear (45). In addition, there may be a cross-sensitivity between the different ASMs, i.e., one ASM causing PBSEs might simultaneously increase the risk of PBSEs associated with another ASM, which also requires attention in the clinical applications (46).
Overall, the selection of ASMs in the treatment of epilepsy-associated comorbidities need to be comprehensively considered in the benefits and risks, considering various issues such as efficacy, adverse effects, drug-drug interactions, giving priority to ASMs that can also be beneficial for the management of the comorbidities (4).
3. Effects of lacosamide treatment on the cognitive and behavioral functions in different populations
3.1. In children and adolescents
Epilepsy can increase the risk of cognitive impairment. It has been established that underlying neuropathology, seizure types, and the administration of ASMs can all have major impact on patients' cognitive abilities (47). Lacosamide is well tolerated and may have potentially positive effects on social, behavioral, and motor function while controlling seizures in children with epilepsy (48–54). Grosso et al. recruited 8 children (aged 8–16) with epileptic syndromes who had continuous spike and waves during slow sleep in a study. It was observed that after at least 12 months of follow-up, two of the five who responded to lacosamide efficacy had improved cognitive performance (55). An open label prospective study enrolled 79 children (aged 5–15) with epilepsy and evaluated the potential effect of lacosamide on behavior by Connor's Comprehensive Behavioral Rating Scales. The results indicated that adjunctive lacosamide significantly reduced the frequency of seizures and concurrently improved the patients' behavior (49). However, Farkas conducted a 16-week randomized, double-blind, placebo-controlled study to evaluate adjunctive lacosamide for the treatment of partial-onset seizures in children and adolescents. Behavioral and cognitive function were evaluated using the Achenbach Child Behavior Checklist (Achenbach CBCL) and the Behavior Rating Inventory for Executive Functioning (BRIEF). They found that behavioral and cognitive function scores were generally steady and similar in both groups (13). ADHD is a common comorbidity in children affected with epilepsy (56), and certain ASMs, such as valproic acid, possess the potential to induce or exacerbate ADHD symptoms (57, 58). Lacosamide is considered to have a possible positive or at least neutral effect on the behavioral control in ADHD, despite lack of validation of adequate evidence (59).
3.2. In adults
Long-term treatment with lacosamide is also well tolerated and efficacious in adult PWE, and has no significant negative effects on cognition (29, 60). However, whether it improves cognitive function remains controversial. A prospective, open-label study recruited 33 patients (aged 16–74, mean: 37 years) to evaluate the possible efficacy of lacosamide in PWE. Interestingly, lacosamide group demonstrated faster reaction times for processing the relevant information (61). Moreover, in another retrospective longitudinal study, 94 epilepsy patients were enrolled in order to compare the cognitive and behavioral effects of lacosamide and perampanel [age at first assessment: lacosamide: 40.70 (14.51), perampanel: 43.33 (11.92); mean (standard deviation)]. The Lacosamide group showed significant improvements in executive functions and memory, without a substantial increase in the self-reported aggression or irritability (60). Biton et al. pooled data from three RCTs of adjunctive lacosamide treatment for partial-onset seizures in adults. Within the permitted dose range (200 and 400 mg/day dose groups combined), the incidence of cognitive-related treatment-emergent adverse events (TEAEs) was comparable in the lacosamide and placebo groups (odds ratio: 1.3, 95% confidence interval: 0.7–2.4) and increased with lacosamide dose (62). In a prospective, open-label research with 34 adult patients with refractory epilepsy, there were no significant differences in the composite ratings of cognition or mood/quality of life before and after 6 months of treatment with lacosamide (63). In addition, several studies have demonstrated the safety and efficacy of lacosamide in elderly patients with epilepsy (64–68). However, there are currently insufficient data available regarding the cognition, mood, and quality of life of elderly patients taking lacosamide (69).
In summary, although the adverse effects of lacosamide on cognition appear to be minimal (47), it remains unclear whether it improves cognitive function in PWE. Recent experiments in animal models of epilepsy have confirmed that the strong neuroprotective effects of long-term lacosamide treatment in rats with combined neuronal damage and behavioral comorbidities (70). Future evidence from more high-quality RCTs is required to expand the in-depth understanding of this field (the details about the included clinical trials are presented in Table 1).
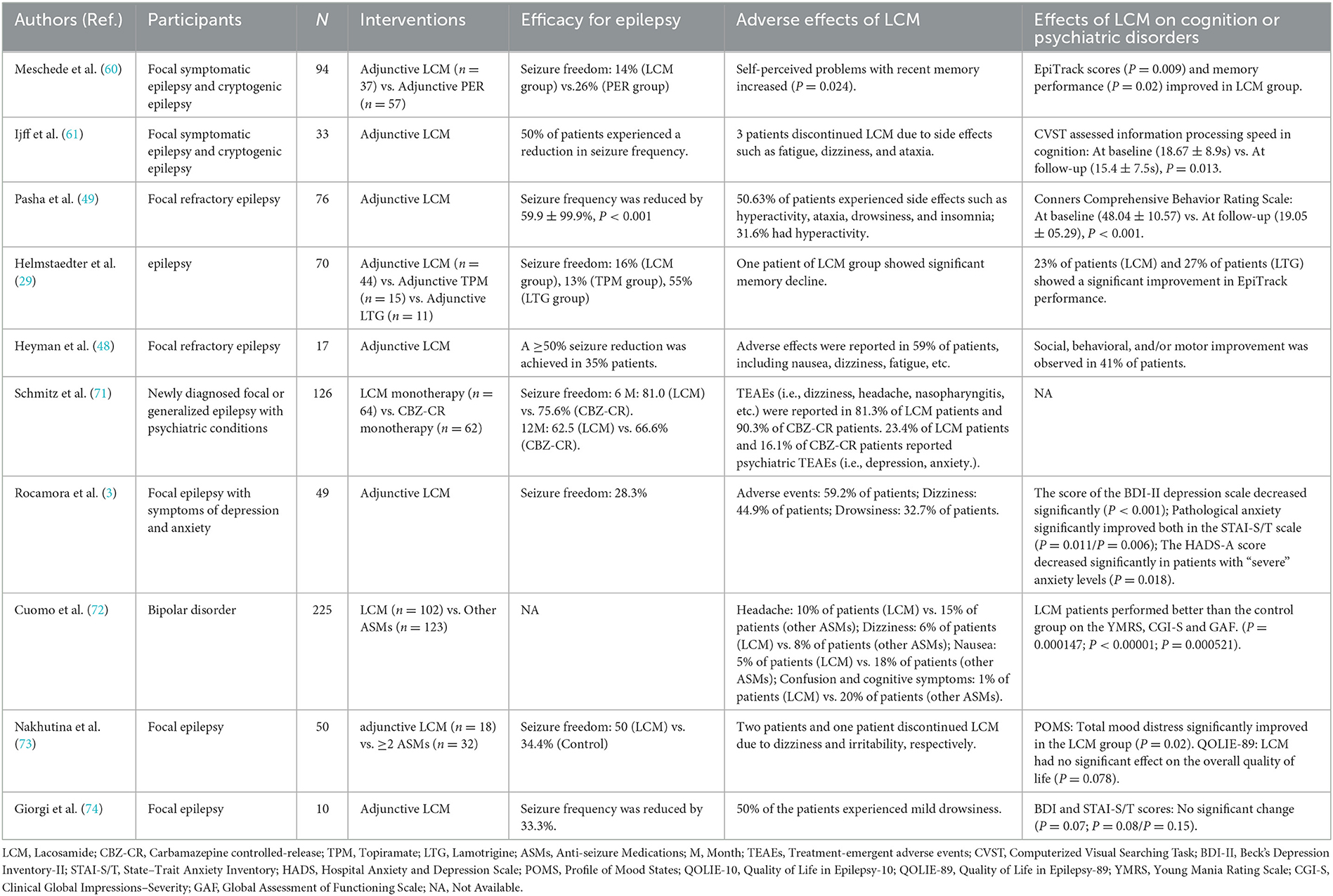
Table 1. Summaries of clinical trials on the effects of lacosamide treatment in epilepsy and psychiatric disorders.
4. Effects of lacosamide treatment on epilepsy-associated anxiety and depression
In recent years, researchers have explored the effects of lacosamide on anxiety and depression in PWE. A post hoc analysis of a large randomized controlled trial SP0993 revealed that the efficacy of lacosamide monotherapy was comparable to that of carbamazepine controlled-release (CBZ-CR) in a subgroup of epilepsy patients with comorbid psychiatric disorders, such as anxiety, depression, and insomnia (71). Moreover, in patients with partial-onset seizures, the treatment of epilepsy with lacosamide also may improv anxiety, depression as well as quality of life without worsening indicators of sleep quality and fatigue (3, 73, 74). In addition, lacosamide improved mania, anxiety, depression, and global functioning in the short term when used for the treatment of patients with bipolar disorder compared to other ASMs (72).
However, whether lacosamide can positively affect mood disorders in PWE remains controversial, with some studies suggesting that it has no significant effect on the mood or can exhibit only positively affects patients with major depressive symptoms at the baseline (75), but it is unlikely to have a negative impact and no serious safety concerns have been reported. Under standard clinical treatment conditions, the incidence of the cardiovascular and psychiatric adverse events associated with lacosamide is minimal, which was identical to the incidence of treatment discontinuation owing to adverse events (76). Therefore, it might still be a safe and effective treatment option for PWE with psychiatric comorbidities (the details of the included clinical trials are presented in Table 1).
5. Effects of lacosamide treatment on epilepsy patients with intellectual disability
The prevalence of the comorbid epilepsy in people with intellectual disability (PWID) ranges from 20 to 30% and increases with severity of intellectual disability (ID). It has been established that ~16% of people with epilepsy also have some degree of ID, which is significantly higher than the prevalence of <1% in the overall population (77–79). The patients with such comorbidities might exhibit more complicated neuropsychiatric characteristics that can impair the treatment outcomes, exacerbate clinical management challenges, and raise the risk of mortality (80, 81).
Brenner et al. (82) included 132 patients with refractory epilepsy in PWID in study whose primary endpoint variables were the retention rates of lacosamide which were estimated by the Kaplan-Meier method. The results showed that the retention rates were 64% at 1 year, 57% at 2 years, and 56% at 3 years, and that ID and seizure severity did not affect the continued use of the drug. However, except for a high incidence of behavior-related side effects, other adverse events were similar to those reported in the previous studies in the general population. Overall, the findings of this study concluded that lacosamide may be effective and safe for the management of epilepsy patients in PWID. In addition, another non-interventional, single-center study reported evaluating the efficacy of lacosamide in patients with ID and drug-resistant epilepsy. The results showed improved Clinical Global Impression scale in 61% of patients, with retention rates of 71 and 65% at 12 and 24 months, respectively, thus suggesting that adjunctive lacosamide may be a suitable antiepileptic treatment option for ID patients (83).
6. Effects of lacosamide treatment on the post-stroke epilepsy and brain tumor-related epilepsy
Stroke is a common cause of epilepsy in the elderly population, with seizure rates ranging from 3.3–3.8 to 7–14% following ischemic and hemorrhagic strokes, respectively (84–87). Seizures in the stroke patients may be caused by distinct mechanisms such as release of cytotoxic neurotransmitter leading to the neuronal hyperexcitability and deposition of gliosis and hemosiderin (88). Seizures are also prevalent in patients affected with brain tumors, with a risk of 60–100% for low-grade gliomas and 40–60% for glioblastomas (89).
According to the findings of a small observational study, 50% of elderly patients with post-stroke non-convulsive status epilepticus (NCSE) displayed controlled epileptic activity within 45–60 min of intravenous lacosamide treatment, with no recurrence and adverse effects reported over a 24-h period. This finding confirmed that lacosamide was safe and effective, thus suggesting that it has the potential to become the drug of choice for the prevention and treatment of post-stroke NCSE in the elderly (90). In a prospective study compared with the historical control group, it was concluded that the clinical efficacy of lacosamide as an add-on therapy might be superior to the historical group treated with levetiracetam in patients with brain tumor-related epilepsy, without affecting the mood and quality of life (91). Rosenow et al. (92) analyzed the efficacy of lacosamide in epilepsy patients of cerebrovascular etiology based on three large clinical studies and reported that the monotherapy efficacy of lacosamide was numerically superior to carbamazepine-CR, with a higher proportion of lacosamide patients being seizure-free after 6 and 12 months of therapy than carbamazepine-CR patients. These observations suggested that lacosamide may be useful for the treatment of epilepsy with cerebrovascular etiology.
7. Effects of lacosamide treatment for epilepsy on other systems
In addition to the aforementioned disorders, several common somatic comorbidities of epilepsy include the cardiovascular, musculoskeletal, respiratory, and nutritional disorders (93, 94). Traditional ASMs (e.g., carbamazepine) have a high potential for drug-drug interactions, negatively affect the lipid metabolism and can elevate the levels of various cardiac markers (95). Therefore, epilepsy-associated comorbidities can also restrict the options for epilepsy treatment (44). Among the newer ASMs, lacosamide can display relatively less interactions with other drugs, and studies have shown that it also has fewer respiratory effects, with nasopharyngitis being a frequent adverse event (7.2–17.2% occurrence) (8, 96). It has been reported that the drug does not prolong the QTc interval or adversely affect the heart rate in adult patients with partial-onset seizures and the maximum recommended dose (400 mg/day) of adjunctive lacosamide is not significantly associated with cardiac effects, except for small changes in PR interval without any major symptomatic consequences (97). It has also been found that favorable changes in the hormones and lipid levels can be observed in PWE after the lacosamide treatment (98).
8. Common adverse effects of lacosamide treatment
In all clinical studies, dizziness is the most common adverse effect of lacosamide (99, 100). In randomized, double-blind, placebo-controlled studies, the incidence of dizziness associated with lacosamide ranged from 23.1 to 25.9%, compared to 8–9.2% for placebo (101, 102). A 3-year follow-up of 473 PWE suggested a final dizziness rate of 26.4% (103). Another typical TEAE of lacosamide is headache. Ben-Menachem et al. (104) conducted a long-term trial of 116 patients on open-label treatment, with a median exposure duration of 854 days, and headache incidence was 9.4%. In another double-blind study with a median exposure time of 630 days, 15.1% of participants in the lacosamide group experienced headaches (96). Vision-related adverse effects such as diplopia are thought to be associated with sodium channel blockers (105). Rosenow et al. (106) recruited 376 patients and found a 13.8% incidence of diplopia over the course of 3 years. Nausea/vomiting and somnolence are also common side effect associated with lacosamide treatment (12, 107). A meta-analysis revealed that the incidence of nausea/vomiting was 9.3% (108). Long-term follow-up showed a range of 6.1% to 8.7% somnolence occurrence (96, 103). The above-mentioned frequent side events are more likely to occur during the first 3 months of treatment, and the majority are well-tolerated (100). It is noteworthy that between 0.4 and 1.7% of lacosamide-treated individuals experienced suicidal ideation or behavior (62, 101, 109). Although there is no evidence to suggest that lacosamide increases the risk of suicide-related events more than other ASMs, caution is still necessary (100).
9. Conclusions
The complex pathogenesis and clinical manifestations of epilepsy, as well as the propensity to acquire various comorbidities simultaneously can pose significant challenge to application of optimal therapy and increase the clinical burden. Different ASMs can also exacerbate or induce epilepsy-associated comorbidities along with their anti-epileptic effects. Consequently, numerous considerations are needed while selecting a suitable pharmacological treatment strategy. The current findings support that lacosamide may have substantial positive effects on multiple comorbidities without exhibiting serious safety concerns and may provide some reference for clinical treatment. Future studies with larger sample sizes or in specific subgroups of patients are also expected to further validate and demonstrate the influence of lacosamide on the clinical benefit in epilepsy patients with different comorbidities.
Author contributions
ZH drafted the manuscript. JL conceptualized and designed the study and revised the manuscript. Both authors contributed to the article and approved the submitted version.
Funding
This study was supported by the National Natural Science Foundation of China (grant 82071459) and the Institute of Brain Science and Brain-inspired Technology of West China Hospital, Sichuan University (grant ZYJC21001).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Keezer MR, Sisodiya SM, Sander JW. Comorbidities of epilepsy: current concepts and future perspectives. Lancet Neurol. (2016) 15:106–15. doi: 10.1016/S1474-4422(15)00225-2
2. Campbell C, Cavalleri GL, Delanty N. Exploring the genetic overlap between psychiatric illness and epilepsy: a review. Epilepsy Behav. (2020) 102:106669. doi: 10.1016/j.yebeh.2019.106669
3. Rocamora R, Ley M, Molins A, Toledo M, Sansa G, Bertol V, et al. Effect of lacosamide on depression and anxiety symptoms in patients with focal refractory epilepsy: a prospective multicenter study. Epilepsy Behav. (2018) 79:87–92. doi: 10.1016/j.yebeh.2017.10.032
4. Kanner AM. Management of psychiatric and neurological comorbidities in epilepsy. Nat Rev Neurol. (2016) 12:106–16. doi: 10.1038/nrneurol.2015.243
5. Rogawski MA, Tofighy A, White HS, Matagne A, Wolff C. Current understanding of the mechanism of action of the antiepileptic drug lacosamide. Epilepsy Res. (2015) 110:189–205. doi: 10.1016/j.eplepsyres.2014.11.021
6. Mula M. Epilepsy and psychiatric comorbidities: drug selection. Curr Treat Options Neurol. (2017) 19:44. doi: 10.1007/s11940-017-0483-0
7. Fiest KM, Patten SB, Jetté N. Screening for depression and anxiety in epilepsy. Neurol Clin. (2016) 34:351–61. doi: 10.1016/j.ncl.2015.11.003
8. Husain A, Chung S, Faught E, Isojarvi J, McShea C, Doty P. Long-term safety and efficacy in patients with uncontrolled partial-onset seizures treated with adjunctive lacosamide: results from a phase iii open-label extension trial. Epilepsia. (2012) 53:521–8. doi: 10.1111/j.1528-1167.2012.03407.x
9. Fountain NB, Krauss G, Isojarvi J, Dilley D, Doty P, Rudd GD. Safety and tolerability of adjunctive lacosamide intravenous loading dose in lacosamide-naive patients with partial-onset seizures. Epilepsia. (2013) 54:58–65. doi: 10.1111/j.1528-1167.2012.03543.x
10. Wechsler RT Li G, French J, O'Brien TJ, D'Cruz O, Williams P, et al. Conversion to lacosamide monotherapy in the treatment of focal epilepsy: results from a historical-controlled, multicenter, double-blind study. Epilepsia. (2014) 55:1088–98. doi: 10.1111/epi.12681
11. Runge U, Arnold S, Brandt C, Reinhardt F, Kuhn F, Isensee K, et al. A noninterventional study evaluating the effectiveness and safety of lacosamide added to monotherapy in patients with epilepsy with partial-onset seizures in daily clinical practice: the vitoba study. Epilepsia. (2015) 56:1921–30. doi: 10.1111/epi.13224
12. Vossler DG, Wechsler RT, Williams P, Byrnes W, Therriault S, Group A-MS. Long-term exposure and safety of lacosamide monotherapy for the treatment of partial-onset (focal) seizures: results from a multicenter, open-label trial. Epilepsia. (2016) 57:1625–33. doi: 10.1111/epi.13502
13. Farkas V, Steinborn B, Flamini JR, Zhang Y, Yuen N, Borghs S, et al. Efficacy and tolerability of adjunctive lacosamide in pediatric patients with focal seizures. Neurology. (2019) 93:e1212–e26. doi: 10.1212/WNL.0000000000008126
14. Devinsky O, Vezzani A, O'Brien TJ, Jette N, Scheffer IE, de Curtis M, et al. Epilepsy. Nat Rev Dis Primers. (2018) 4:18024. doi: 10.1038/nrdp.2018.24
15. Xu L, Ding X, Wang T, Mou S, Sun H, Hou T. Voltage-gated sodium channels: structures, functions, and molecular modeling. Drug Discov Today. (2019) 24:1389–97. doi: 10.1016/j.drudis.2019.05.014
16. Mantegazza M, Curia G, Biagini G, Ragsdale DS, Avoli M. Voltage-gated sodium channels as therapeutic targets in epilepsy and other neurological disorders. Lancet Neurol. (2010) 9:413–24. doi: 10.1016/S1474-4422(10)70059-4
17. Cawello W, Stockis A, Andreas JO, Dimova S. Advances in epilepsy treatment: lacosamide pharmacokinetic profile. Ann N Y Acad Sci. (2014) 1329:18–32. doi: 10.1111/nyas.12513
18. Carona A, Bicker J, Silva R, Fonseca C, Falcao A, Fortuna A. Pharmacology of lacosamide: from its molecular mechanisms and pharmacokinetics to future therapeutic applications. Life Sci. (2021) 275:119342. doi: 10.1016/j.lfs.2021.119342
19. Licko T, Seeger N, Zellinger C, Russmann V, Matagne A, Potschka H. Lacosamide treatment following status epilepticus attenuates neuronal cell loss and alterations in hippocampal neurogenesis in a rat electrical status epilepticus model. Epilepsia. (2013) 54:1176–85. doi: 10.1111/epi.12196
20. Errington AC, Stöhr T, Heers C, Lees G. The investigational anticonvulsant lacosamide selectively enhances slow inactivation of voltage-gated sodium channels. Mol Pharmacol. (2008) 73:157–69. doi: 10.1124/mol.107.039867
21. Sheets PL, Heers C, Stoehr T, Cummins TR. Differential block of sensory neuronal voltage-gated sodium channels by lacosamide [(2r)-2-(Acetylamino)-N-Benzyl-3-Methoxypropanamide], lidocaine, and carbamazepine. J Pharmacol Exp Ther. (2008) 326:89–99. doi: 10.1124/jpet.107.133413
22. Niespodziany I, Leclère N, Vandenplas C, Foerch P, Wolff C. Comparative study of lacosamide and classical sodium channel blocking antiepileptic drugs on sodium channel slow inactivation. J Neurosci Res. (2013) 91:436–43. doi: 10.1002/jnr.23136
23. Jo S, Bean BP. Lacosamide inhibition of Nav17 voltage-gated sodium channels: slow binding to fast-inactivated states. Mol Pharmacol. (2017) 91:277–86. doi: 10.1124/mol.116.106401
24. Sanchez RM, Ribak CE, Shapiro LA. Synaptic connections of hilar basal dendrites of dentate granule cells in a neonatal hypoxia model of epilepsy. Epilepsia. (2012) 53:98–108. doi: 10.1111/j.1528-1167.2012.03481.x
25. Kourdougli N, Pellegrino C, Renko JM, Khirug S, Chazal G, Kukko-Lukjanov TK, et al. Depolarizing Γ-aminobutyric acid contributes to glutamatergic network rewiring in epilepsy. Ann Neurol. (2017) 81:251–65. doi: 10.1002/ana.24870
26. Zhang JN, Koch JC. Collapsin response mediator protein-2 plays a major protective role in acute axonal degeneration. Neural Regen Res. (2017) 12:692–5. doi: 10.4103/1673-5374.206631
27. Wilson SM, Xiong W, Wang Y, Ping X, Head JD, Brittain JM, et al. Prevention of posttraumatic axon sprouting by blocking collapsin response mediator protein 2-mediated neurite outgrowth and tubulin polymerization. Neuroscience. (2012) 210:451–66. doi: 10.1016/j.neuroscience.2012.02.038
28. Wolff C, Carrington B, Varrin-Doyer M, Vandendriessche A, Van der Perren C, Famelart M, et al. Drug binding assays do not reveal specific binding of lacosamide to collapsin response mediator protein 2 (Crmp-2). CNS Neurosci Ther. (2012) 18:493–500. doi: 10.1111/j.1755-5949.2012.00313.x
29. Helmstaedter C, Witt JA. The longer-term cognitive effects of adjunctive antiepileptic treatment with lacosamide in comparison with lamotrigine and topiramate in a naturalistic outpatient setting. Epilepsy Behav. (2013) 26:182–7. doi: 10.1016/j.yebeh.2012.11.052
30. Maguire J. Mechanisms of psychiatric comorbidities in epilepsy. Curr Top Behav Neurosci. (2022) 55:107–44. doi: 10.1007/7854_2020_192
31. Zaccara G. Neurological comorbidity and epilepsy: implications for treatment. Acta Neurol Scand. (2009) 120:1–15. doi: 10.1111/j.1600-0404.2008.01146.x
32. Hooper A, Paracha R, Maguire J. Seizure-induced activation of the hpa axis increases seizure frequency and comorbid depression-like behaviors. Epilepsy Behav. (2018) 78:124–33. doi: 10.1016/j.yebeh.2017.10.025
33. Akyuz E, Polat AK, Eroglu E, Kullu I, Angelopoulou E, Paudel YN. Revisiting the role of neurotransmitters in epilepsy: an updated review. Life Sci. (2021) 265:118826. doi: 10.1016/j.lfs.2020.118826
34. Mazarati A, Sankar R. Common mechanisms underlying epileptogenesis and the comorbidities of epilepsy. Cold Spring Harb Perspect Med. (2016) 6:798. doi: 10.1101/cshperspect.a022798
35. Barker-Haliski M, White HS. Glutamatergic mechanisms associated with seizures and epilepsy. Cold Spring Harb Perspect Med. (2015) 5:a022863. doi: 10.1101/cshperspect.a022863
36. Colmers PLW, Maguire J. Network dysfunction in comorbid psychiatric illnesses and epilepsy. Epilepsy Curr. (2020) 20:205–10. doi: 10.1177/1535759720934787
37. Johnson AC Li Z, Orfila JE, Herson PS, Cipolla MJ. Hippocampal network dysfunction as a mechanism of early-onset dementia after preeclampsia and eclampsia. Prog Neurobiol. (2021) 199:101938. doi: 10.1016/j.pneurobio.2020.101938
38. Campo P, Garrido MI, Moran RJ, Maestu F, Garcia-Morales I, Gil-Nagel A, et al. Remote effects of hippocampal sclerosis on effective connectivity during working memory encoding: a case of connectional diaschisis? Cereb Cortex. (2012) 22:1225–36. doi: 10.1093/cercor/bhr201
39. Lv RJ, Sun ZR, Cui T, Guan HZ, Ren HT, Shao XQ. Temporal lobe epilepsy with amygdala enlargement: a subtype of temporal lobe epilepsy. BMC Neurol. (2014) 14:194. doi: 10.1186/s12883-014-0194-z
40. Isgor C, Pare C, McDole B, Coombs P, Guthrie K. Expansion of the dentate mossy fiber-Ca3 projection in the brain-derived neurotrophic factor-enriched mouse hippocampus. Neuroscience. (2015) 288:10–23. doi: 10.1016/j.neuroscience.2014.12.036
41. Auvin S, Wirrell E, Donald KA, Berl M, Hartmann H, Valente KD, et al. Systematic review of the screening, diagnosis, and management of adhd in children with epilepsy. Consensus paper of the task force on comorbidities of the ilae pediatric commission. Epilepsia. (2018) 59:1867–80. doi: 10.1111/epi.14549
42. Strzelczyk A, Schubert-Bast S. Psychobehavioural and cognitive adverse events of anti-seizure medications for the treatment of developmental and epileptic encephalopathies. CNS Drugs. (2022) 21:1–33. doi: 10.1007/s40263-022-00955-9
43. Mammì A, Ferlazzo E, Gasparini S, Bova V, Neri S, Labate A, et al. Psychiatric and behavioural side effects associated with perampanel in patients with temporal lobe epilepsy: a real-world experience. Front Neurol. (2022) 13:839985. doi: 10.3389/fneur.2022.839985
44. Sen A, Jette N, Husain M, Sander JW. Epilepsy in older people. Lancet. (2020) 395:735–48. doi: 10.1016/S0140-6736(19)33064-8
45. Chen B, Choi H, Hirsch LJ, Katz A, Legge A, Buchsbaum R, et al. Psychiatric and behavioral side effects of antiepileptic drugs in adults with epilepsy. Epilepsy Behav. (2017) 76:24–31. doi: 10.1016/j.yebeh.2017.08.039
46. Chen B, Choi H, Hirsch LJ, Legge A, Buchsbaum R, Detyniecki K. Cross-sensitivity of psychiatric and behavioral side effects with antiepileptic drug use. Seizure. (2018) 62:38–42. doi: 10.1016/j.seizure.2018.09.014
47. Li KY, Huang LC, Chang YP, Yang YH. The effects of lacosamide on cognitive function and psychiatric profiles in patients with epilepsy. Epilepsy Behav. (2020) 113:107580. doi: 10.1016/j.yebeh.2020.107580
48. Heyman E, Lahat E, Levin N, Berkovitch M, Gandelman-Marton R. Preliminary efficacy and safety of lacosamide in children with refractory epilepsy. Eur J Paediatr Neurol. (2012) 16:15–9. doi: 10.1016/j.ejpn.2011.08.007
49. Pasha I, Kamate M, Suresh DK. Safety of lacosamide in children with refractory partial epilepsy. Saudi Pharm J. (2015) 23:556–61. doi: 10.1016/j.jsps.2015.01.006
50. Casas-Fernández C, Martínez-Bermejo A, Rufo-Campos M, Smeyers-Durá P, Herranz-Fernández JL, Ibáñez-Micó S, et al. Efficacy and tolerability of lacosamide in the concomitant treatment of 130 patients under 16 years of age with refractory epilepsy: a prospective, open-label, observational, multicenter study in Spain. Drugs R D. (2012) 12:187–97. doi: 10.2165/11636260-000000000-00000
51. Pasha I, Kamate M, Didagi SK. Efficacy and tolerability of lacosamide as an adjunctive therapy in children with refractory partial epilepsy. Pediatr Neurol. (2014) 51:509–14. doi: 10.1016/j.pediatrneurol.2014.07.004
52. Grosso S, Parisi P, Spalice A, Verrotti A, Balestri P. Efficacy and safety of lacosamide in infants and young children with refractory focal epilepsy. Eur J Paediatr Neurol. (2014) 18:55–9. doi: 10.1016/j.ejpn.2013.08.006
53. Ferreira JA, Le Pichon JB, Abdelmoity AT, Dilley D, Dedeken P, Daniels T, et al. Safety and tolerability of adjunctive lacosamide in a pediatric population with focal seizures: an open-label trial. Seizure. (2019) 71:166–73. doi: 10.1016/j.seizure.2019.05.016
54. Okanishi T, Fujii Y, Sakuma S, Shiraishi H, Motoi H, Yazaki K, et al. Lacosamide monotherapy for the treatment of childhood epilepsy with centrotemporal spikes. Brain Dev. (2022) 44:380–5. doi: 10.1016/j.braindev.2022.02.005
55. Grosso S, Parisi P, Giordano L, di Bartolo R, Balestri P. Lacosamide efficacy in epileptic syndromes with continuous spike and waves during slow sleep (Csws). Epilepsy Res. (2014) 108:1604–8. doi: 10.1016/j.eplepsyres.2014.08.021
56. Russ SA, Larson K, Halfon N, A. national profile of childhood epilepsy and seizure disorder. Pediatrics. (2012) 129:256–64. doi: 10.1542/peds.2010-1371
57. Glauser TA, Cnaan A, Shinnar S, Hirtz DG, Dlugos D, Masur D, et al. Ethosuximide, valproic acid, and lamotrigine in childhood absence epilepsy. N Engl J Med. (2010) 362:790–9. doi: 10.1056/NEJMoa0902014
58. Glauser TA, Cnaan A, Shinnar S, Hirtz DG, Dlugos D, Masur D, et al. Ethosuximide, valproic acid, and lamotrigine in childhood absence epilepsy: initial monotherapy outcomes at 12 months. Epilepsia. (2013) 54:141–55. doi: 10.1111/epi.12028
59. Verrotti A, Moavero R, Panzarino G, Di Paolantonio C, Rizzo R, Curatolo P. The challenge of pharmacotherapy in children and adolescents with epilepsy-adhd comorbidity. Clin Drug Investig. (2018) 38:1–8. doi: 10.1007/s40261-017-0585-1
60. Meschede C, Witt JA, Rademacher M, von Wrede RD, Elger CE, Helmstaedter C. Evaluating the longer-term cognitive effects of adjunctive perampanel compared to lacosamide in a naturalistic outpatient setting. Seizure. (2018) 58:141–6. doi: 10.1016/j.seizure.2018.04.015
61. DM IJ, van Veenendaal TM, Majoie HJ, de Louw AJ, Jansen JF, Aldenkamp AP. Cognitive effects of lacosamide as adjunctive therapy in refractory epilepsy. Acta Neurol Scand. (2015) 131:347–54. doi: 10.1111/ane.12372
62. Biton V, Gil-Nagel A, Isojarvi J, Doty P, Hebert D, Fountain NB. Safety and tolerability of lacosamide as adjunctive therapy for adults with partial-onset seizures: analysis of data pooled from three randomized, double-blind, placebo-controlled clinical trials. Epilepsy Behav. (2015) 52(Pt A):119–27. doi: 10.1016/j.yebeh.2015.09.006
63. Lancman ME, Fertig EJ, Trobliger RW, Perrine K, Myers L, Iyengar SS, et al. The effects of lacosamide on cognition, quality-of-life measures, and quality of life in patients with refractory partial epilepsy. Epilepsy Behav. (2016) 61:27–33. doi: 10.1016/j.yebeh.2016.04.049
64. Sierra-Marcos A, Bermejo PE, Manso Calderón R, Gutiérrez-Álvarez AM, Jiménez Corral C, Sagarra Mur D. Lacosamide for epileptic seizures in patients with co-morbidities and unusual presentations of epilepsy. CNS Drugs. (2011) 25:17–26. doi: 10.2165/1159573-S0-000000000-00000
65. Baulac M, Rosenow F, Toledo M, Terada K, Li T, De Backer M, et al. Efficacy, safety, and tolerability of lacosamide monotherapy vs. controlled-release carbamazepine in patients with newly diagnosed epilepsy: a phase 3, randomised, double-blind, non-inferiority trial. Lancet Neurol. (2017) 16:43–54. doi: 10.1016/S1474-4422(16)30292-7
66. Rainesalo S, Mäkinen J, Raitanen J, Peltola J. Clinical management of elderly patients with epilepsy; the use of lacosamide in a single center setting. Epilepsy Behav. (2017) 75:86–9. doi: 10.1016/j.yebeh.2017.07.045
67. Sarkis RA, Nicolas J, Lee JW. Tolerability of lacosamide or zonisamide in elderly patients with seizures. Seizure. (2017) 49:1–4. doi: 10.1016/j.seizure.2017.04.010
68. Del Bianco C, Placidi F, Liguori C, Mari L, Ulivi M, Ornello R, et al. Long-term efficacy and safety of lacosamide and levetiracetam monotherapy in elderly patients with focal epilepsy: a retrospective study. Epilepsy Behav. (2019) 94:178–82. doi: 10.1016/j.yebeh.2019.02.022
69. Rohracher A, Kalss G, Kuchukhidze G, Neuray C, Leitinger M, Höfler J, et al. New anti-seizure medication for elderly epilepsy patients: a critical narrative review. Expert Opin Pharmacother. (2021) 22:621–34. doi: 10.1080/14656566.2020.1843636
70. Shishmanova-Doseva M, Atanasova D, Uzunova Y, Yoanidu L, Peychev L, Marinov P, et al. Effects of lacosamide treatment on epileptogenesis, neuronal damage and behavioral comorbidities in a rat model of temporal lobe epilepsy. Int J Mol Sci. (2021) 22:4667. doi: 10.3390/ijms22094667
71. Schmitz B, Dimova S, Zhang Y, Chellun D, De Backer M, Gasalla T. Tolerability and efficacy of lacosamide and controlled-release carbamazepine monotherapy in patients with newly diagnosed epilepsy and concomitant psychiatric conditions: post hoc analysis of a prospective, randomized, double-blind trial. Epilepsy Res. (2020) 159:106220. doi: 10.1016/j.eplepsyres.2019.106220
72. Cuomo I, Piacentino D, Kotzalidis GD, Lionetto L, De Filippis S. Lacosamide in bipolar disorder: a 30-day comparison to a retrospective control group treated with other antiepileptics. Psychiatry Clin Neurosci. (2018) 72:864–75. doi: 10.1111/pcn.12784
73. Nakhutina L, Kunnakkat SD, Coleman M, Lushbough C, Arnedo V, Soni N, et al. Effects of adjunctive lacosamide on mood and quality of life in patients with epilepsy. Epilepsy Behav. (2017) 73:90–4. doi: 10.1016/j.yebeh.2017.05.001
74. Giorgi FS, Pizzanelli C, Pelliccia V, Di Coscio E, Maestri M, Guida M, et al. A clinical-eeg study of sleepiness and psychological symptoms in pharmacoresistant epilepsy patients treated with lacosamide. Epilepsy Res Treat. (2013) 2013:593149. doi: 10.1155/2013/593149
75. Toniolo S, Di Lorenzo F, Bozzali M, Yogarajah M. The impact of lacosamide on mood disorders in adult patients with epilepsy: a systematic review. Epilepsy Behav. (2020) 111:107179. doi: 10.1016/j.yebeh.2020.107179
76. Steinhoff BJ, Eckhardt K, Doty P, De Backer M, Brunnert M, Schulze-Bonhage A, et al. Long-term noninterventional safety study of adjunctive lacosamide therapy in patients with epilepsy and uncontrolled partial-onset seizures. Epilepsy Behav. (2016) 58:35–43. doi: 10.1016/j.yebeh.2016.02.041
77. Bowley C, Kerr M. Epilepsy and intellectual disability. J Intellect Disabil Res. (2000) 44(Pt 5):529–43. doi: 10.1046/j.1365-2788.2000.00270.x
78. Morgan CL, Baxter H, Kerr MP. Prevalence of epilepsy and associated health service utilization and mortality among patients with intellectual disability. Am J Ment Retard. (2003) 108:293–300. doi: 10.1352/0895-8017(2003)108<293:POEAAH>2.0.CO;2
79. Forsgren L, Beghi E, Oun A, Sillanpää M. The epidemiology of epilepsy in europe: a systematic review. Eur J Neurol. (2005) 12:245–53. doi: 10.1111/j.1468-1331.2004.00992.x
80. Devinsky O, Asato M, Camfield P, Geller E, Kanner AM, Keller S, et al. Delivery of epilepsy care to adults with intellectual and developmental disabilities. Neurology. (2015) 85:1512–21. doi: 10.1212/WNL.0000000000002060
81. Nickels KC, Zaccariello MJ, Hamiwka LD, Wirrell EC. Cognitive and neurodevelopmental comorbidities in paediatric epilepsy. Nat Rev Neurol. (2016) 12:465–76. doi: 10.1038/nrneurol.2016.98
82. Brenner J, Majoie HJM, van Beek S, Carpay JA. The retention of lacosamide in patients with epilepsy and intellectual disability in three specialised institutions. Seizure. (2017) 52:123–30. doi: 10.1016/j.seizure.2017.09.017
83. Kleist A, Kerling F, Hamer H, Winterholler M. Lacosamide in patients with intellectual disability and refractory epilepsy. Acta Neurol Belg. (2019) 119:423–30. doi: 10.1007/s13760-019-01098-3
84. Wang JZ, Vyas MV, Saposnik G, Burneo JG. Incidence and management of seizures after ischemic stroke: systematic review and meta-analysis. Neurology. (2017) 89:1220–8. doi: 10.1212/WNL.0000000000004407
85. Feher G, Gurdan Z, Gombos K, Koltai K, Pusch G, Tibold A, et al. Early seizures after ischemic stroke: focus on thrombolysis. CNS Spectr. (2020) 25:101–13. doi: 10.1017/S1092852919000804
86. Naidech AM, Garg RK, Liebling S, Levasseur K, Macken MP, Schuele SU, et al. Anticonvulsant use and outcomes after intracerebral hemorrhage. Stroke. (2009) 40:3810–5. doi: 10.1161/STROKEAHA.109.559948
87. De Herdt V, Dumont F, Hénon H, Derambure P, Vonck K, Leys D, et al. Early seizures in intracerebral hemorrhage: incidence, associated factors, and outcome. Neurology. (2011) 77:1794–800. doi: 10.1212/WNL.0b013e31823648a6
88. Quirins M, Dussaule C, Denier C, Masnou P. Epilepsy after stroke: definitions, problems and a practical approach for clinicians. Rev Neurol. (2019) 175:126–32. doi: 10.1016/j.neurol.2018.02.088
89. Vecht CJ, Kerkhof M, Duran-Pena A. Seizure prognosis in brain tumors: new insights and evidence-based management. Oncologist. (2014) 19:751–9. doi: 10.1634/theoncologist.2014-0060
90. Belcastro V, Vidale S, Pierguidi L, Sironi L, Tancredi L, Striano P, et al. Intravenous lacosamide as treatment option in post-stroke non convulsive status epilepticus in the elderly: a proof-of-concept, observational study. Seizure. (2013) 22:905–7. doi: 10.1016/j.seizure.2013.07.011
91. Maschio M, Zarabla A, Maialetti A, Fabi A, Vidiri A, Villani V, et al. Quality of life, mood and seizure control in patients with brain tumor related epilepsy treated with lacosamide as add-on therapy: a prospective explorative study with a historical control group. Epilepsy Behav. (2017) 73:83–9. doi: 10.1016/j.yebeh.2017.05.031
92. Rosenow F, Brandt C, Bozorg A, Dimova S, Steiniger-Brach B, Zhang Y, et al. Lacosamide in patients with epilepsy of cerebrovascular etiology. Acta Neurol Scand. (2020) 141:473–82. doi: 10.1111/ane.13230
93. Aaberg KM, Bakken IJ, Lossius MI, Lund Soraas C, Haberg SE, Stoltenberg C, et al. Comorbidity and childhood epilepsy: a nationwide registry study. Pediatrics. (2016) 138:921. doi: 10.1542/peds.2016-0921
94. Arya R, Gillespie CW, Cnaan A, Devarajan M, Clark P, Shinnar S, et al. Obesity and overweight as cae comorbidities and differential drug response modifiers. Neurology. (2016) 86:1613–21. doi: 10.1212/WNL.0000000000002611
95. Lopinto-Khoury C, Mintzer S. Antiepileptic drugs and markers of vascular risk. Curr Treat Options Neurol. (2010) 12:300–8. doi: 10.1007/s11940-010-0080-y
96. Ben-Menachem E, Grebe HP, Terada K, Jensen L, Li T, De Backer M, et al. Long-term safety and efficacy of lacosamide and controlled-release carbamazepine monotherapy in patients with newly diagnosed epilepsy. Epilepsia. (2019) 60:2437–47. doi: 10.1111/epi.16381
97. Rudd GD, Haverkamp W, Mason JW, Wenger T, Jay G, Hebert D, et al. Lacosamide cardiac safety: clinical trials in patients with partial-onset seizures. Acta Neurol Scand. (2015) 132:355–63. doi: 10.1111/ane.12414
98. Elger CE, Rademacher M, Brandt C, Elmoufti S, Dedeken P, Eckhardt K, et al. Changes in hormone and lipid levels in male patients with focal seizures when switched from carbamazepine to lacosamide as adjunctive treatment to levetiracetam: a small phase iiib, prospective, multicenter, open-label trial. Epilepsy Behav. (2016) 62:1–5. doi: 10.1016/j.yebeh.2016.05.023
99. Fattore C, Perucca E. Novel medications for epilepsy. Drugs. (2011) 71:2151–78. doi: 10.2165/11594640-000000000-00000
100. Li J, Sun M, Wang X. The adverse-effect profile of lacosamide. Expert Opin Drug Saf. (2020) 19:131–8. doi: 10.1080/14740338.2020.1713089
101. Hong Z, Inoue Y, Liao W, Meng H, Wang X, Wang W, et al. Efficacy and safety of adjunctive lacosamide for the treatment of partial-onset seizures in Chinese and Japanese adults: a randomized, double-blind, placebo-controlled study. Epilepsy Res. (2016) 127:267–75. doi: 10.1016/j.eplepsyres.2016.08.032
102. Vossler DG, Knake S, O'Brien TJ, Watanabe M, Brock M, Steiniger-Brach B, et al. Efficacy and safety of adjunctive lacosamide in the treatment of primary generalised tonic-clonic seizures: a double-blind, randomised, placebo-controlled trial. J Neurol Neurosurg Psychiatry. (2020) 91:1067–75. doi: 10.1136/jnnp-2020-323524
103. Inoue Y, Liao W, Wang X, Du X, Tennigkeit F, Sasamoto H, et al. Safety and efficacy of adjunctive lacosamide in chinese and japanese adults with epilepsy and focal seizures: a long-term, open-label extension of a randomized, controlled trial. Epilepsy Res. (2021) 176:106705. doi: 10.1016/j.eplepsyres.2021.106705
104. Ben-Menachem E, Dominguez J, Szász J, Beller C, Howerton C, Jensen L, et al. Long-term safety and tolerability of lacosamide monotherapy in patients with epilepsy: results from a multicenter, open-label trial. Epilepsia Open. (2021) 6:618–23. doi: 10.1002/epi4.12522
105. Zaccara G, Giovannelli F, Maratea D, Fadda V, Verrotti A. Neurological adverse events of new generation sodium blocker antiepileptic drugs. Meta-analysis of randomized, double-blinded studies with eslicarbazepine acetate, lacosamide and oxcarbazepine. Seizure. (2013) 22:528–36. doi: 10.1016/j.seizure.2013.03.016
106. Rosenow F, Kelemen A, Ben-Menachem E, McShea C, Isojarvi J, Doty P. Long-term adjunctive lacosamide treatment in patients with partial-onset seizures. Acta Neurol Scand. (2016) 133:136–44. doi: 10.1111/ane.12451
107. Hmaimess G, Sabbagh S, Dirani M, Hotait M, Beydoun AA, Nasreddine W. Efficacy and tolerability of treatment with lacosamide in children: postmarketing experience from the middle east. Seizure. (2020) 79:75–9. doi: 10.1016/j.seizure.2020.04.016
108. Yang C, Peng Y, Zhang L, Zhao L. Safety and tolerability of lacosamide in patients with epilepsy: a systematic review and meta-analysis. Front Pharmacol. (2021) 12:694381. doi: 10.3389/fphar.2021.694381
Keywords: epilepsy, lacosamide, anti-seizure medications, epilepsy comorbidities, psychiatric disorders
Citation: He Z and Li J (2023) The therapeutic effects of lacosamide on epilepsy-associated comorbidities. Front. Neurol. 14:1063703. doi: 10.3389/fneur.2023.1063703
Received: 07 October 2022; Accepted: 02 March 2023;
Published: 16 March 2023.
Edited by:
Sara Gasparini, Magna Græcia University, ItalyReviewed by:
Ayataka Fujimoto, Seirei Hamamatsu General Hospital, JapanCopyright © 2023 He and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jinmei Li, bGlqaW5tZWlAd2Noc2N1LmNu