
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurol. , 17 October 2022
Sec. Neuromuscular Disorders and Peripheral Neuropathies
Volume 13 - 2022 | https://doi.org/10.3389/fneur.2022.990802
This article is part of the Research Topic Translational Study for Amyotrophic Lateral Sclerosis Treatment View all 7 articles
 Sven Schröder1†
Sven Schröder1† Mingzhe Wang2†
Mingzhe Wang2† Dandan Sima2†Joana Schröder1,2Xuying Zhu2Xuanlu Zheng2Lin Liu2,3Tingying Li2Qiudong Wang4
Dandan Sima2†Joana Schröder1,2Xuying Zhu2Xuanlu Zheng2Lin Liu2,3Tingying Li2Qiudong Wang4 Thomas Friedemann1*‡
Thomas Friedemann1*‡ Te Liu5*‡
Te Liu5*‡ Weidong Pan2*‡
Weidong Pan2*‡Background: Amyotrophic lateral sclerosis (ALS) is a chronic neurodegenerative disease characterized by gradually increasing damage to the upper and lower motor neurons. However, definitive and efficacious treatment for ALS is not available, and oral intake in ALS patients with bulbar involvement is complicated due to swallowing difficulties.
Hypothesis/purpose: This study investigated whether the external plaster application of the herbal composition Ji-Wu-Li efficiently slows ALS progression because prior studies obtained promising evidence with oral herbal applications.
Study design: The randomized, triple-blinded study compared the efficacy, safety, and tolerability of the application of Ji-Wu-Li plaster (JWLP) with placebo plaster (PLAP).
Methods: In total, 120 patients with definite ALS, clinically probable ALS, or clinically probable laboratory-supported ALS were randomized in a 1:1 ratio to receive JWLP or PLAP. Patients were treated and observed for 20 weeks. The primary outcome was the ALSFRS-R score, while the secondary outcomes were the ALS-SSIT score and weight loss.
Results: The mean±SD decrease in the ALSFRS-R over 20 weeks differed by 0.84 points in a group comparison (JWLP, −4.44 ± 1.15; PLAP, −5.28 ± 1.98; p = 0.005). The mean increase in the ALS-SSIT over 20 weeks differed by 2.7 points in a group comparison (JWLP, 5.361.15; PLAP, 8.06 ± 1.72; p < 0.001). The mean weight loss over 20 weeks differed by 1.65 kg in a group comparison (JWLP, −3.98 ± 2.61; PLAP, −5.63 ± 3.17; p = 0.002). Local allergic dermatitis suspected as causal to the intervention occurred in 10 of 60 participants in the JWLP group and 9 of 60 participants in the PLAP group. Systemic adverse events were mild, temporary, and considered unrelated to the intervention.
Conclusion: The JWLP showed clinical efficacy in the progression of ALS, as measured by the ALSFRS-R, ALS-SSIT, and weight loss in a randomized, placebo-controlled trial. Because skin reactions occurred in both groups, the covering material needs improvement. All of the Ji Wu Li herbal ingredients regulate multiple mechanisms of neurodegeneration in ALS. Hence, JWLP may offer a promising and safe add-on therapy for ALS, particularly in patients with bulbar involvement, but a confirmative long-term multicentre study is required.
Amyotrophic lateral sclerosis (ALS) is a chronic neurodegenerative disease that gradually results in increased damage to the upper and lower motor neurons (1). Its general characteristics include muscle weakness/atrophy in the oropharynx, limbs, or back muscles, dysarthria, dysphagia, eating difficulty, a choking cough, and dyspnoea (2). These features gravely affect the quality of life and may lead to respiratory failure within 3–5 years from disease onset (3, 4).
The pathophysiology of ALS is multifactorial and includes glutamate excitotoxicity (5), neuroinflammation (6), oxidative stress (7, 8), and protein aggregation (9, 10), which lead to mitochondrial dysfunction (8, 11) and apoptosis (12). Axonal transport dysfunction ultimately induces muscle atrophy (13). There is no definitive and efficacious treatment for ALS. The only established drug, riluzole, is mainly effective in the late stages of ALS (14). Moreover, due to adverse events, riluzole discontinuation is necessary for more than 20% of patients (15). Another potential treatment, edaravone, has not been approved in many countries and can only be applied intravenously; it has recently been determined to be ineffective (16). These medications are not reimbursed by insurance in many health systems worldwide.
Hence, inexpensive curative or symptomatic therapies with few adverse effects must be identified. Asian research groups have evaluated herbal medicines derived from Traditional Chinese Medicine (TCM) in animal models of ALS (17). Although the concept of ALS does not exist in TCM, a similar syndrome called “flaccidity syndrome, limpness–or atrophy syndrome” was described in the oldest medicinal book, Huangdi Neijing, in the context of tissue and substance loss (in TCM terms, called “Yin deficiency”) (18). Modern Chinese approaches recommend herbal drugs for ALS that are considered to have tonifying and strengthening properties (19–23).
A prior randomized clinical trial applied this concept with the oral administration of the formulation Jia Wei Si Jun-Zi Tang and found a slowing of the symptom progression of ALS in comparison to riluzole (23). The similar augmented herbal formula Ji Wu Li is a modern formula that has its basis on the classical TCM formula Si Jun Zi from the 12th century (24) and adds four herbs (Astragali Radix, Rhodiola Rosea Radix, Cistanche Radix Herba, Epimedii Herba, Table 1).
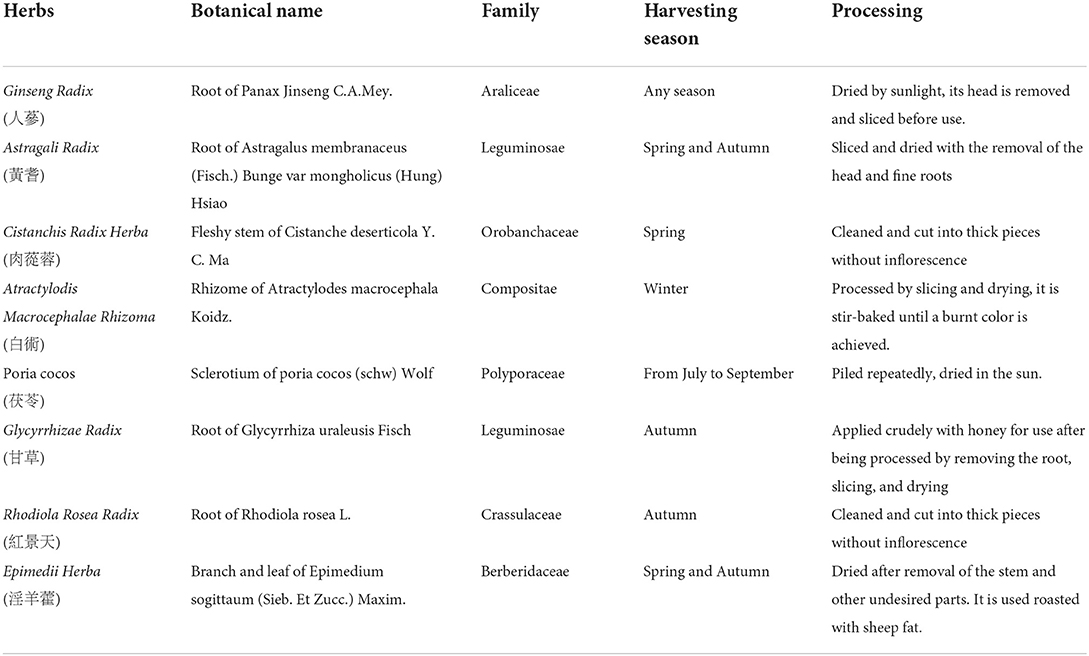
Table 1. Herbal ingredients of the Ji Wu li Plaster.
However, the oral intake of TCM formulations is complicated in patients with dysphagia because herbal extracts require a larger oral intake than concentrated single-component western drugs. Our ALS study team focused on external herbal medicine in the search for a better application method.
The external application of Chinese herbs has a long tradition. Since the fourth century, every TCM therapy book has included a chapter on external herbal therapy (25). Modern application forms for transdermal drug delivery include hot-melt adhesive plasters, which allow drug application directly to the skin (26). Mechanisms of external application of herbs include transdermal micro- and macro absorption, local increment of microcirculation, and adjustment of the neural-endocrine-immune network (27). In general, transdermal application reaches comparable efficacy to oral-dosage forms. However, the transdermal application has advantages because transdermal administration avoids the first-pass effect of metabolism associated with the oral route with improved bioavailability. Transdermal administration allows prolonged release, improving patient adherence and minimizing adverse effects due to lower drug peak concentrations (28, 29).
Hence, we hypothesized that the external application of herbal medicine could have similar promising effects on the progress of ALS as in the oral application form (23). Furthermore, the advantages of the external application (28, 29) could especially become relevant in ALS patients with bulbar involvement. Accordingly, we performed the present placebo-controlled, randomized, triple-blinded ALS-CHEPLA (ALS-Chinese HErbal PLAster) trial. The study aimed to compare the efficacy, safety, and tolerability of the herbal composition Ji-Wu-Li when applied as a plaster (JWLP, Table 1) and placebo plaster (PLAP) in ALS patients. The primary outcome was the Amyotrophic Lateral Sclerosis Rating Scale-Revised (ALSFRS-R) score, a self-reported instrument used to quantify the function of an individual with ALS as the disease progresses. It consists of questions covering gross motor, fine motor, oral motor, and respiratory function and shows good reliability and construct validity (30).
The Ethics Committee (Vote No.: KY-SHSG-2018-540) of Shuguang Hospital, affiliated with the Shanghai University of TCM, approved the study protocol. The study (trial registration number ChiCTR200037353) adhered to the Declaration of Helsinki of 1964 and its later amendments. The full trial protocol can be requested by email from the corresponding author. All patients gave their written informed consent to participate in the study and for data publication.
This single-center, controlled, patient- and observer-blinded, parallel-group randomized trial was conducted at the Department of Neurology within Shuguang Hospital, a specialized center for motor neuron diseases. Interested individuals older than 18 with definite or probable ALS were checked for participation eligibility. Forced vital capacity (FVC) was measured at baseline. In addition, a neurologist obtained a detailed medical history and conducted a neurological examination at baseline and weeks 4, 8, 16, and 20.
According to revised El Escorial criteria, patients with clinically definite ALS, clinically probable ALS, or clinically probable laboratory-supported ALS were eligible for inclusion (31).
We excluded patients with (i) an FVC < 30%; (ii) signs of a significant psychiatric disorder and/or dementia, acute cholecystitis, or bile duct occlusion; (iii) a concomitant condition considered likely to interfere with drug adherence and outcome assessment; (iv) pregnancy; (v) short expected survival due to disease progression; and (vi) participation in other clinical trials.
In total, 138 ALS patients were recruited and checked for eligibility; 120 met the inclusion criteria. Immediately after participants gave their written informed consent and before any study-related procedures were undertaken, site staff obtained a participant identification code. Eligible participants were randomly assigned following stratified randomization procedures (computerized random numbers, Microsoft Excel, 2016) at a 1:1 ratio to receive the JWLP (n = 60) or PLAP (n = 60). Randomization was stratified by sex (yes or no); there was no stratification of patients according to disease onset, age, or respiratory function.
An independent randomization center performed the randomization. They informed the study nurse about the number printed beforehand on the study medication batch, which was then connected to the participant's identification code. To achieve masking of random assignments, PLAP was matched to JWLP by appearance and packaging. Clinicians arranged patient treatment according to the participants' identification codes. The study drug was dispensed at baseline and as needed at study visits. Participants, their families, investigators, site staff, the steering committee, and anyone involved in outcome assessments were masked by these identification codes and randomization.
The JWLP contained 32 g of herbs (Ginseng Radix, Astragalus Radix, Cistanche deserticola Herba, Atractylodis macrocephalae Rhizoma, Poria cocos, Glycyrrhizae Radix, Rhodiola rosea Radix, and Epimedii Herba) in a ratio of 2:6:3:2:2:2:2:2. Table 1 describes the botanical name, plant family, part of the plant, harvesting season, and processing methods. The purified raw herbs were crushed and sieved with an 80-mesh sieve. The materials were mixed with 12-g melt adhesive material [including Styrene-isoprene-styrene tertiary block copolymer (35–50%), Styrene-butadiene-styrene tertiary block copolymer (0–5%), naphthenic hydroxyl-based petroleum fractions (softener, 15–20%), C-5, cyclopentadiene and m-pentadiene (Tackifier 1, 30–40%) and esters formed by the reaction of resin acids with glycerol and pentaerythritol (Tackifier 2, 10–20%)]. To complete the plaster, we covered the self-adhesive patch with a layer of heating particles containing iron powder, salt, and activated carbon. Each plaster weighed about 100 g, including 32 g of herbs, 12 g of melt adhesive material, and 52 g of heating particles. Removal of the sealed cover paper activated the heating particles via contact with air; the particles were not in direct contact with the skin. The particles reached 60°C within 20 min and maintained that temperature for at least 5 h.
The PLAP was prepared similarly (according to HSFA GB2760-2007, CFDA 2006, No. 120). However, a placebo (23 g soybean powder, 23 g starch, 1 g amaranth red, and 1 g carbon black pigment) replaced the herbal material. The shape, color, weight, and heat function of the PLAP were the same as those of the JWLP, and the plasters and packaging were indistinguishable. Figure 1 shows the different layers of the plaster.
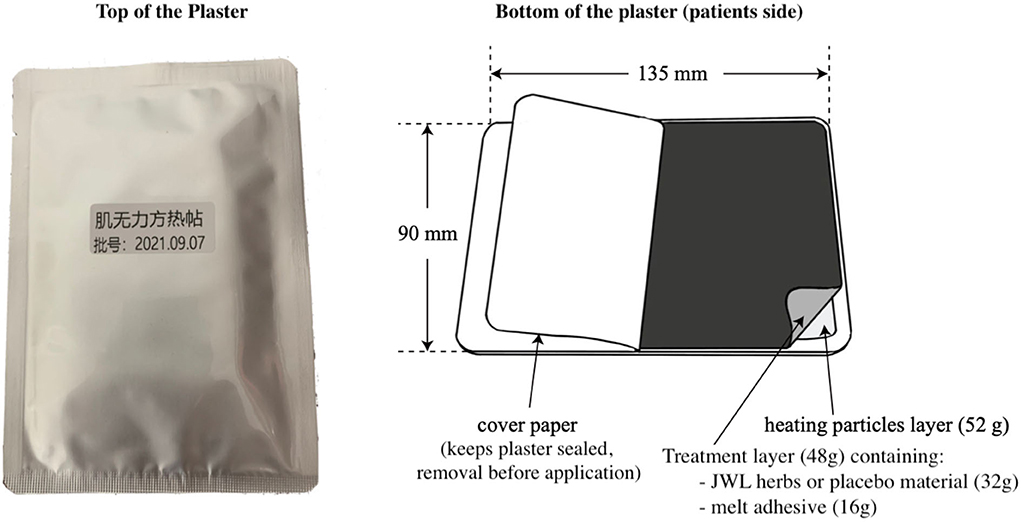
Figure 1. The layers of the Ji-Wu-Li plaster and the placebo.
In the JWLP and PLAP groups, the rectangular 90 × 135-mm plaster was placed on the patient's back in the midline in the depression below the spinous process of the seventh cervical vertebra. Figure 2 demonstrates the plaster position on a patient. The plaster remained in place for 6 h on 6 consecutive days, followed by 1 day of rest to reduce the skin reaction before another cycle of plaster application. The patients continued their regular medical treatment; any treatment changes had to be reported, and no change to a possibly disease-altering therapy was allowed. The description of the quality certificates of the materials of the herbs can be found in the Supplementary material.

Figure 2. Positioning of the JWLP and the PLAP in an ALS patient.
The primary outcome was the ALSFRS-R (30). The minimum score is 0, and the maximum is 48. The lower the score, the more function is affected. A clinical neurologist assessed ALSFRS-R by interviewing the patient at baseline and weeks 4, 8, 16, and 20. The prespecified primary endpoint was 20 weeks from the baseline assessment.
The recently introduced ALS-SSIT (Amyotrophic Lateral Sclerosis Symptom Score in Integrative Treatments) is a clinical score reflecting the quality of life. The higher the score (a maximum score of 40), the more severe the impairment. The ALS-SSIT score has recently been validated to reflect the change in disease severity (32). A clinical neurologist assessed ALS-SSIT by interviewing the patient at baseline and weeks 4, 8, 16, and 20. A study nurse documented the participants' weight with a calibrated scale at each visit at baseline and weeks 4, 8, 16, and 20. Red blood cell count, biochemistry, kidney/liver function, and electrocardiography were assessed at baseline and trial cessation. Safety was evaluated as the prevalence and severity of adverse events and their relationship with the treatment were determined based on the results of laboratory tests, patient reports, and the judgement of the principal investigator.
The sample size was calculated for a two-sided t-test comparing the difference between two independent means using a 1:1 allocation, an alpha of 0.05, and a power of 0.8. An effect size of 0.52 was calculated based on a previous study (TCM group 3.8 ± 4.9 and control group 7.3 ± 8.2) (23). G*Power 3.1.9.4 was used for the sample size calculation. The results revealed that 120 patients were needed, 60 in the control group and 60 in the treatment group.
Statistical analysis followed the intention-to-treat principle. All randomized participants were analyzed. To have an unbiased analysis, we used a complete data set for the primary analysis [JWLP (n = 60), PLAP (n = 60)]. Imputation of missing data followed an individualized decision based on predictive parameters for the missing cases. The ALSRFS-R progression rate (ΔFS' = 48–Total ALSFRS–R score at the assessment on test date/Time from onset of symptoms to assessment on test date) (33) was used to calculate the missing values by carrying the last observed progression rate forward.
Repeated-measures ANOVA was conducted to test the differences among changes in outcomes at baseline and 4, 8, 12, 16, and 20 weeks of treatment for both groups. In addition, differences at baseline and the delta from baseline to endpoint between the JWLP and PLAP were analyzed using the Student's t-test. p-value < 0.05 was considered significant. SPSS 17.0 (IBM, Armonk, NY, USA) was used for statistical analyses. Data are reported as the mean ± standard deviation.
Figure 3 shows the CONSORT flowchart. Between July 2017 and November 2021, 138 consecutive patients were screened for eligibility, of whom 11 were excluded because they did not meet the inclusion criteria or because they met an exclusion criterion. Of the remaining 127 patients, 120 were enrolled in the trial; seven patients declined to participate.
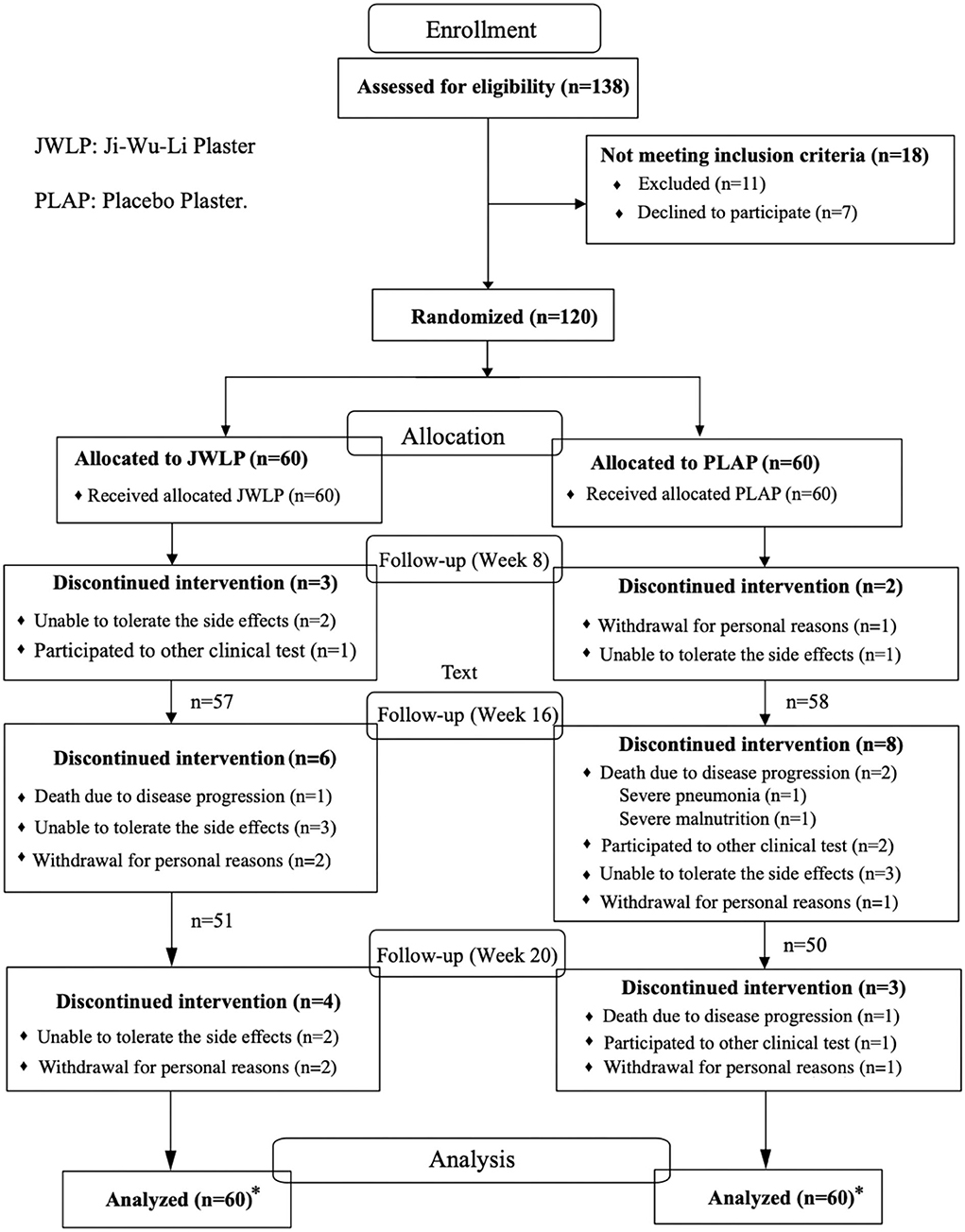
Figure 3. CONSORT flow diagram of the ALS-CHEPAL trial. *Intent-to-treat principle, all randomized participants were analyzed.
All ALS cases were sporadic. There were no significant differences in sex, age, body weight, onset time of morbidity, disease progression, FVC, ALSFRS-R, or ALS-SSIT between the two groups at baseline. Thirty-three participants in the JWLP group and 37 in the PLAP group had involvement of the limbs only, 13 in the JWLP group and 12 in the PLAP group had involvement of the bulbar only, and 14 in the JWLP group and 11 in the PLAP group had involvement of both the limbs and the bulbar region. Table 2 presents the basic characteristics.
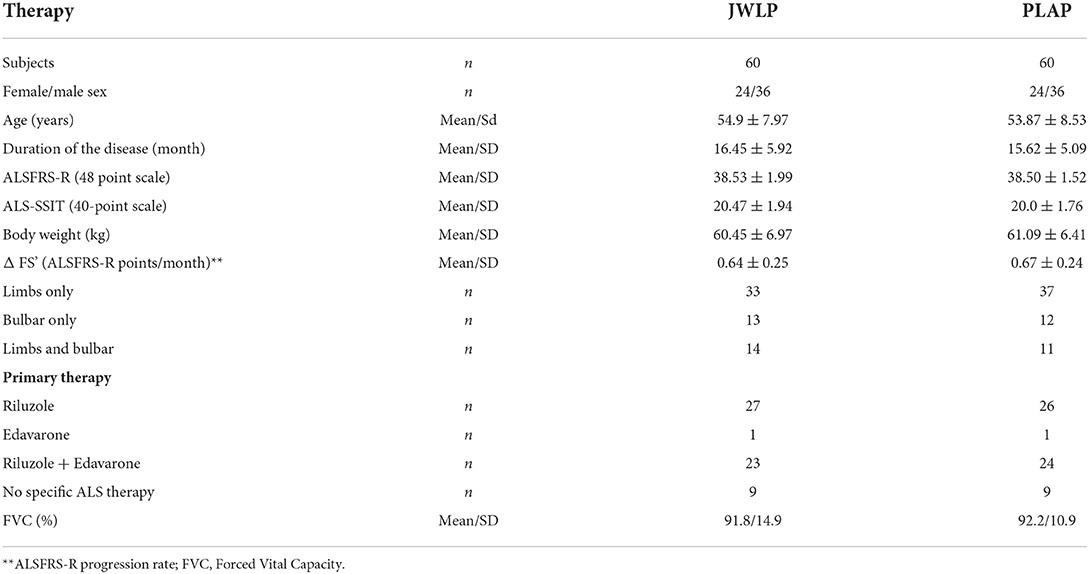
Table 2. Characteristics of the JWLP and PLAP groups.
Forty-seven participants in each group completed the entire 20-week observation period. Discontinuation for personal reasons occurred in four JWLP participants (two before the 16th week and two before the 20th week) and three PLAP participants (one each before the 8th, 16th, and 20th weeks). One JWLP patient (before the 8th week) and one PLAP patient (before the 20th week) decided to participate in another trial. One patient died before the 16th week in the JWLP group, as well as three participants in the PLAP group, two before the 16th week (one for disease progression and one for pneumonia) and one before the 20th week. Discontinuation due to non-tolerable adverse effects occurred in seven JWLP participants (two before the 8th week, three before the 16th week, and two before the 20th week) and four PLAP participants (one before the 8th week and three before the 16th week).
In the JWLP group, the ALSFRS-R continuously declined from baseline (38.53 ± 1.99) to week 4 (37.53 ± 2.35), week 8 (36.34 ± 2.27), week 12 (35.72 ± 2.22), week 16 (35.12 ± 2.24), and week 20 (34.09 ± 2.19). In the PLAP group, the ALSFRS-R also continuously declined from baseline (38.50 ± 1.53) to week 4 (37.60 ± 1.78), week 8 (35.50 ± 1.66), week 12 (34.94 ± 1.68), week 16 (34.24 ± 2.17), and week 20 (33.21 ± 2.30).
The differences between the JWLP and PLAP were −0.03 at baseline (t = 0.09, 95% CI −0.71 to 0.78, p = 0.930), 0.07 after 4 weeks (t = 0.175, 95% CI −0.81 to 0.68, p = 0861), −0.84 after 8 weeks (t = 2.22, 95% CI 0.10 to 1.59, p = 0.027), −0.78 after 12 weeks (t = 2.05, 95% CI 0.03 to 1.52, p = 0.042), −0.87 after 16 weeks (t = 2.30, 95% CI 0.13 to 1.62, p = 0.022) and −0.87 after 20 weeks (t = 2.30, 95% CI 0.26 to 1.43, p = 0.022). Figure 4 summarizes these data. The mean decreases from baseline to the 20th week (Δbaseline to 20th week) were −4.44 ± 1.15 in the JWLP group and −5.28 ± 1.98 in the PLAP group (difference of 0.84 points, p = 0.005).
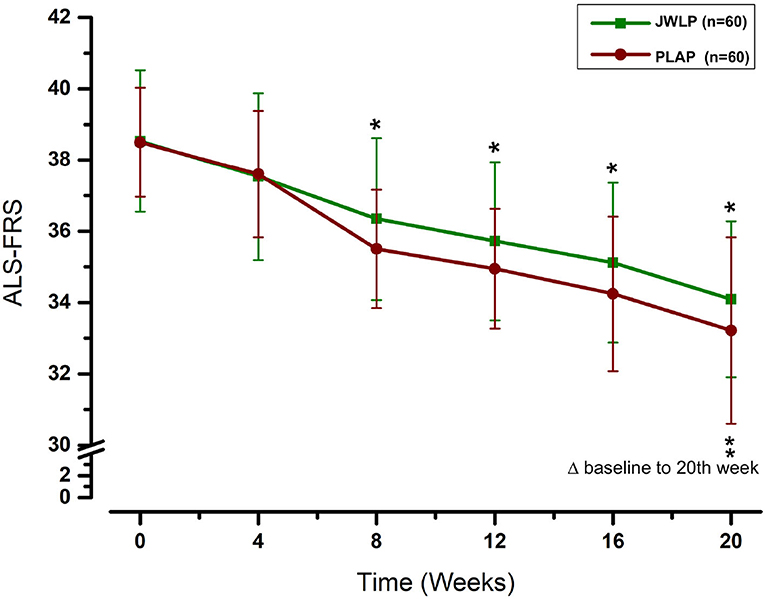
Figure 4. Change over time in the ALSFRS-R over the 20 week trial period. *p < 0.05, **p < 0.01.
In the JWLP group, the ALS-SSIT continuously increased from baseline (20.47 ± 1.94) to week 4 (21.4 ± 2.13), week 8 (23.54 ± 1.82), week 12 (24.22 ± 1.85), week 16 (25.12 ± 1.94), and week 20 (25.83 ± 2.02). In the PLAP group, the ALS-SSIT continuously increased from baseline (20.00 ± 1.76) to week 4 (21.02 ± 1.80), week 8 (24.96 ± 1.87), week 12 (25.91 ± 1.84), week 16 (27.07 ± 2.07), and week 20 (28.06 ± 2.20). The increase in both groups was statistically significant for every 4 weeks compared to the previous score and baseline (p < 0.01).
The differences between the JWLP and PLAP groups were 0.47 at baseline (t = 1.32, 95% CI −0.23 to 1.16, p = 0.188), 0.38 after 4 weeks (t = 1.08, 95% CI −0.31 to 1.08, p = 0.280), −1.42 after 8 weeks (t = 4.01, 95% CI −2.12 to −0.73, p < 0.001), −1.69 after 12 weeks (t = 4.77, 95% CI −2.38 to −0.99, p < 0.001), −1.96 after 16 weeks (t = 5.52, 95% CI −2.65 to −1.26, p < 0.001) and −2.23 after 20 weeks (t = 6.30, 95% CI −2.93 to −1.54, p < 0.001). Figure 5 summarizes these results. The increases in the ALS-SSIT within 20 weeks were 5.36 ± 1.15 points in the JWLP group and 8.06 ± 1.72 points in the PLAP group (difference of 2.7 points, p < 0.001).
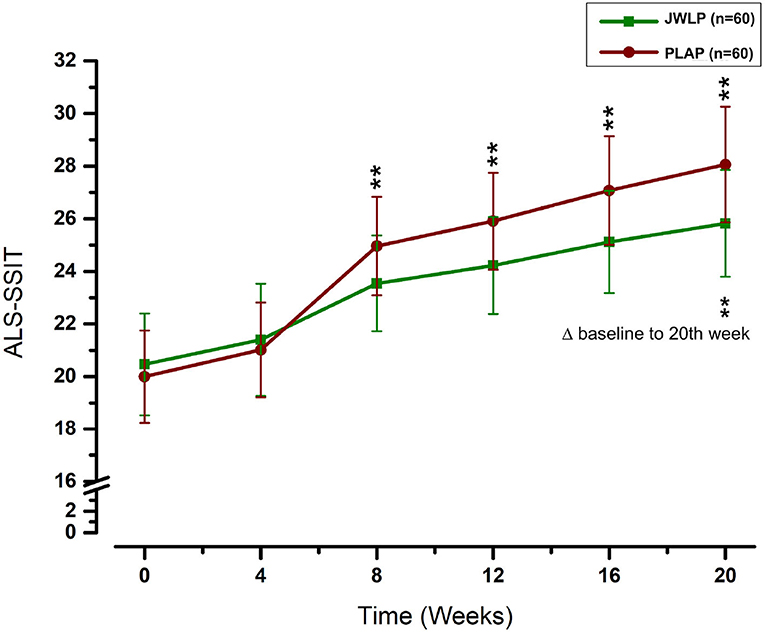
Figure 5. Change over time in the ALS-SITT over the 20 week trial period. **p < 0.01.
In the JWLP group, the mean weight continuously declined from baseline (60.5 ± 6.97) to week 4 (59.58 ± 6.87), week 8 (58.01 ± 6.91), week 12 (57.72 ± 7.15), week 16 (57 ± 7.50), and week 20 (56.58 ± 7.54). In the PLAP group, the weight continuously declined from baseline (61.09 ± 6.41) to week 4 (60.07 ± 6.42), week 8 (58.03 ± 6.30), week 12 (57.37 ± 6.49), week 16 (56.64 ± 6.77), and week 20 (55.46 ± 6.86). The decrease in both groups was statistically significant for every 4 weeks compared to the previous measurement and baseline (p < 0.01). The difference between the JWLP and PLAP was not statistically significant at any measurement point. The mean weight decreases from baseline to week 20 were −3.98 ± 2.61 kg in the JWLP group and −5.63 ± 3.17 kg in the PLAP group (difference of 1.65 kg, p = 0.002). Figure 6 summarizes these findings. The results of the ALSFRS-R, ALSSITT, and weight are summarized in Table 3.
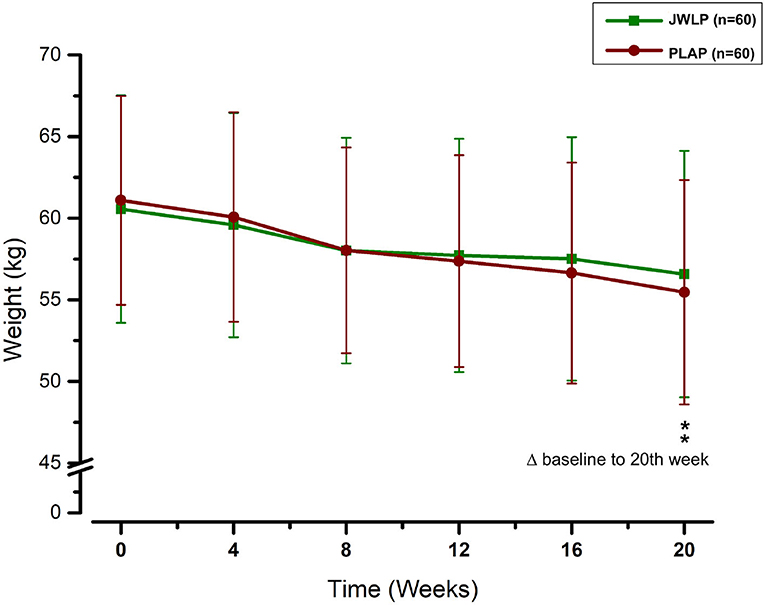
Figure 6. The development of the weight over the 20 week trial period. **p < 0.01.
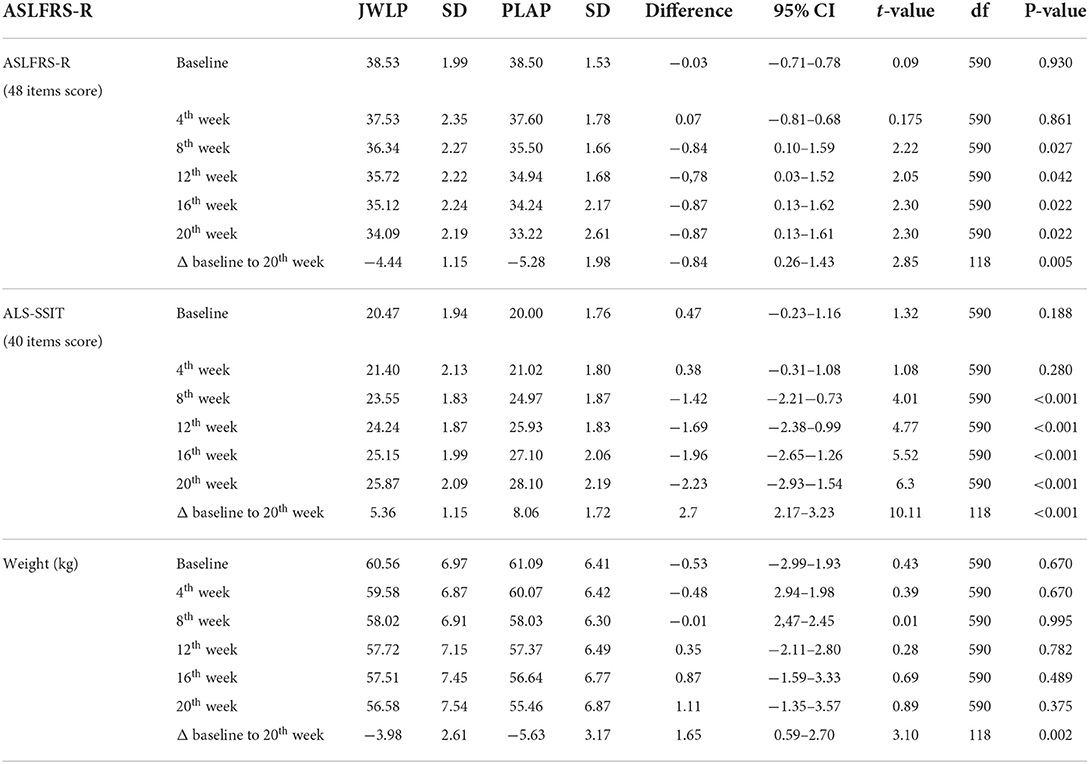
Table 3. ALSFRS-R, ASL-SSIT, and weight over 20 weeks.
Allergic dermatitis under the plaster as an adverse event with a suspected causal relationship to intervention occurred in 10 of 60 JWLP group patients (16, 70%) and 9 of 60 PLAP group patients (8.33%) (df = 2, p = 0.098). Allergic dermatitis, though moderate and local, was not tolerable in seven JWLP participants (11.6%) and five PLAP participants (8.3%) (df = 2, p = 0.34) and caused discontinuation of the therapy (dropout). After cessation of the plaster treatment, all skin symptoms completely recovered and disappeared within weeks.
Temporary mild adverse events (fever, sore throat, nausea, and constipation) occurred in a minority of both groups and were considered unrelated to intervention, or a causal relationship was not assessable. No treatment-related changes in normal blood levels (red blood cells, hemoglobin, haematocrit, platelets, white blood cells, creatinine, blood urea nitrogen, y-glutamyl transferase, alanine aminotransferase, aspartate aminotransferase, and electrolytes), or alterations in the electrocardiogram related to treatment were detected.
Table 4 summarizes the adverse events.
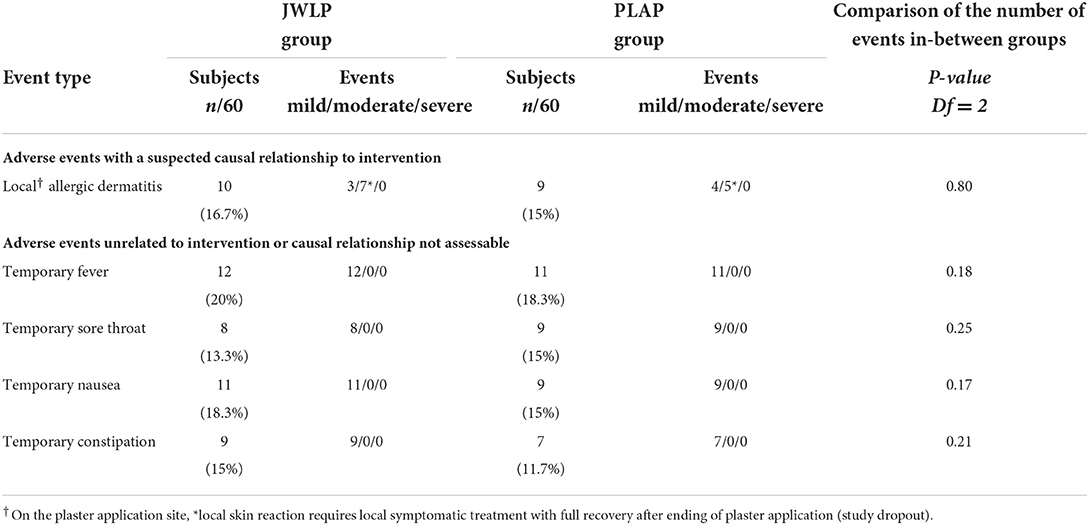
Table 4. Adverse events by MedDRA preferred terms and by treatment group.
To our knowledge, this is the first randomized, controlled, triple-blinded study of external herbal treatment for ALS. We used the ALSFRS-R score as the primary outcome, which is considered the gold standard for the staging and functional measurement of disease progression (34, 35) and comparison with newly proposed scales (36, 37). In our study, the decrease in the ALS-FRS-R was significantly lower in the JWLP group than in the PLAP group from the eighth week until the final examination after 20 weeks.
Additionally, we examined the ALS-SSIT score as a secondary outcome. The ALS-SSIT is focused on patients' quality of life and is approved due to its feasibility, reliability, validity, and sensitivity (38). Like the ALSFRS-R, the difference between the two groups was statistically significant from the eighth week onwards but became more pronounced thereafter until the endpoint. The higher measurement sensitivity of the differences and the focus on the quality of life suggests that the ALS-SSIT should be considered in future ALS studies. Furthermore, we examined weight as an observer-independent marker of cachexia. The mean weight loss for the period of 20 weeks was 1.65 kg higher in the PLAP group than in the JWLP group, which was statistically significant.
One novelty of this study was the introduction of the external application of herbs into ALS treatment. This approach is useful for patients with bulbar involvement. In general, transdermal application has comparable efficacy to oral administration. The mechanisms underlying the external application of herbs include transdermal micro-/macroabsorption, local augmentation of microcirculation, and adjustment of the neural-endocrine-immune network (27). Transdermal application has advantages because it avoids the first-pass effect of metabolism associated with the oral route, leading to improved bioavailability (39, 40).
Furthermore, it allows prolonged release, improves patient adherence, and minimizes adverse effects due to lower drug peak concentrations (29). Transdermal application may avoid gastrointestinal irritation, low absorption, and a short half-life, necessitating frequent dosing. Thus, a lower daily dose can elicit an equivalent therapeutic effect. The most significant disadvantages are the lower permeability of the skin for some herbal ingredients, the slow permeation of hydrophobic ingredients, differences from person to person and with age, and the possibility of local irritation at the application site (26). Skin reactions were the only adverse effects leading to trial cessation in this study. However, the termination rate in the JWLP group was half the rate reported for riluzole, and the adverse events were less severe (15).
Furthermore, the PLAP patients experienced similar skin symptoms. Hence, the adverse effects are partly not medication-generated but a reaction to the plaster material (melt adhesive material) or heat. Therefore, the material needs future improvement, and a periodic change in the plaster position might be an option.
The location of the plaster was chosen for practical considerations because placement in this region does not significantly hinder movement or function. Furthermore, it covers the paravertebral muscles, the trapezius muscle, and the rhomboid, which are well perfused. In addition, the plaster is positioned above reflex areas, which are traditionally considered to have toning and strengthening properties and whose stimulation leads to activation of the thoracic sympathetic trunk with sympathetic afferent neural induction of the increased perfusion of skeletal muscles. This is relevant because the sympathetic nervous system regulates skeletal muscle motor innervation and acetylcholine receptor stability. A progressive decline in sympathetic innervation is frequent in ALS with impaired adaptation to physiological stressors (41).
ALS has multifactorial mechanisms of neurodegeneration that lead to mitochondrial dysfunction (8, 11) and apoptosis (12), with a consequent dysfunction in axonal transport and muscle atrophy (13). The classical pharmacological approach that focuses on a single target of the ingredients can only have limited success (42), as shown for riluzole, which affects glutamate excitotoxicity (43), and edaravone, which affects oxidative stress alone (44)—the herbs of JWL target the pathophysiological mechanism of ALS. Taken together, these herbs target oxidative stress and neuroinflammation and potentially protect against mitochondrial dysfunction and apoptosis. Furthermore, Ginseng Radix, Astragalus Radix, Atractylodis macrocephalae Rhizoma, Glycyrrhizae Radix, Rhodiola rosea Radix, and Epimedii Herba can prevent glutamate excitotoxicity while Ginseng Radix, Astragalus Radix, Glycyrrhizae Radix, and Rhodiola rosea Radix can ameliorate skeletal muscle atrophy (Supplementary Figure 1 summarizes these findings, while Supplementary Tables 1a,b, describe the herbs, their constituents and their mechanisms of action on the targets). Overall, the ingredients of every single herb of JWL have effects on almost all known mechanisms of ALS (45–58). Hence, JWL is a promising combination of herbs that counteracts multiple mechanisms of ALS.
The present study has certain limitations. First, the work was conducted at a single center. A multicentre study is advisable for confirmation. In addition, the study evaluated only 20 weeks. Future studies should confirm the effects in a long-term clinical trial.
Furthermore, the therapeutic concept is based on traditional experience with external applications and herbal studies with oral medications. However, there is limited knowledge on the absorption rate of single ingredients or the pharmacokinetics and pharmacodynamics. Hence, targeted selective animal and human studies are mandatory to substantiate the clinical use of the JWLP in ALS patients.
Nevertheless, while there are not enough established and effective therapies for ALS, there is sufficient knowledge of the toxicology and pharmacovigilance of the single herbs of JWL. Furthermore, their use is well-established, and relevant systemic adverse effects did not occur during this study. Hence, combining TCM formulations with western medicine is an encouraging way to help alleviate symptoms and delay ALS progression.
The JWLP showed clinical efficacy in a randomized, controlled, placebo-controlled trial, measured by the ALSFRS-R, ALS-SSIT, and weight loss. The study revealed no systemic adverse effects. Because skin reactions occurred in the verum and placebo groups, the covering material needs improvement. Hence, JWLP offers a promising add-on therapy for ALS, particularly in patients with bulbar involvement.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding authors.
The studies involving human participants were reviewed and approved by Ethics Committee of Shuguang Hospital Affiliated with the Shanghai University of TCM. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
WP, TLiu, TF, and SS conceived and designed the study and supervised the experiments. MW, DS, JS, XZhe, LL, TLi, and XZhu performed the trial, data collection, literature research, and data analysis. QW and TF performed and controlled the statistical analysis, WP and SS drafted the manuscript. All data were generated in-house and no paper mill was used. All authors corrected the draft manuscript, agreed to be accountable for all aspects of the work, ensuring integrity, and accuracy.
The present study was supported by a grant from the National Natural Science Foundation of China (81373619) and the Clinical Research Plan of Shanghai Shenkang Hospital Development Center (SHDC2020CR2027B). Funding was also received from the Shanghai Municipal Health and Family Planning Commission (ZY3-CCCX-3-3030).
We are grateful to all the study participants for their contributions. We also thank Shanghai NUANYOU Industry Co. Ltd. for preparing and providing the JWLP and PLAP for this study. Supplementary Figure 1 was created with the free version of the Biorender.com.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2022.990802/full#supplementary-material
Supplementary Figure 1. Pharmacological treatment targets in relation to ALS disease mechanism.
Supplementary Table 1a. Antioxidative and anti-inflammatory activities of the main constituents of Ji Wu Li.
Supplementary Table 1b. Neuroprotective and Glutamate excitotoxicity- and muscle atrophy attenuating effects of Ji Wu Li constituents. ABTS, 2,2′-Azino-bis(3-Ethylbenzothiazoline-6-Sulfonic Acid); AChE, Acetylcholinesterase; AIF, apoptosis-inducing factor; AMPK, AMP-activated protein kinase; Bax, Bcl-2-associated X protein; Bcl-2, B-cell lymphoma 2; CARM1, co-activator-associated arginine methyltransferase 1; CAT, Catalase; COX2, Cyclooxygenase-2; DAPK1, Death Associated Protein Kinase 1; DNA, deoxyribonucleic acid; DPPH, 2,2-Diphenyl-1-picrylhydrazyl; ERK, Extracellular-signal Regulated Kinases; GLT-1, Glutamate transporter-1; GPx, Glutathione peroxidase; GSH, Glutathion in its reduced form; GSH-PX, Glutathionperoxidase; GSK3β, Glycogen synthase kinase 3 beta; HSP-16.2, Heat-shock-protein 16.2; Iba1, Ionized calcium-binding adapter molecule 1; IFN-γ, Interferone gamma; IL, Interleukin; I/R, ischemia/reperfusion; iNOS, Inducible nitric oxide synthase; IP-10, interferon-gamma induced protein 10; MDA, Malondialdehyde; MEK, MAPK/ERK Kinase; MMP, Matrix metallopeptidase; mTOR, mammalian Target of Rapamycin; NF-κB, Nuclear factor kappa B; NMDAR, N-Methyl-d-aspartate receptor; NO, Nitric oxide; NOX4, NADPH Oxidase 4; NQO1, NAD(P)H Quinone Dehydrogenase 1; ODG/R, Oxygen glucose deprivation and reperfusion; PCP, Poria cocos polysaccharide; PGE2, Prostaglandin E2; PI3K, Phosphoinositide 3-kinases; PON2, Paraoxonase 2; ROS, Reactive oxygen species; SKP2, S-Phase-kinase-associated-protein; SOD, Superoxide Dismutase; STAT, signal transducer and activator of transcription; S100β, S100 calcium-binding protein B; XOD, xanthine oxidase; TNF-α, Tumor-necrosis-factor-alpha; TXNIP, Thioredoxin-interacting-protein. A Literature search was performed from the databases from inception to February 2022 using MEDLINE, Google Scholar, Cochrane Database, CINHAL, CNKI, and Wanfang Med Online. The keywords “Ginseng Radix, Astragalus Radix, Cistanche deserticola Herba, Atractylodis macrocephalae Rhizoma, Poria cocos, Glycyrrhiza Radix, Rhodiola rosea Radix, Epimedii Herba” AND “neurodegeneration, glutamate excitotoxicity, neuroinflammation, oxidative stress, protein aggregation, mitochondrial dysfunction, axonal transport dysfunction, muscle atrophy, spasticity, and ALS” were used as MeSH terms.
ALS, amyotrophic lateral sclerosis; ALS-CHEPLA, ALS-Chinese HErbal PLAster; JWLP, Ji Wu Li plaster; PLAP, placebo plaster; ALS-SSITS, amyotrophic lateral sclerosis symptom score in integrative treatment scale; ALSFRS-R, amyotrophic lateral sclerosis rating scale-revised; FVC, forced vital capacity; TCM, Traditional Chinese Medicine; EMG, electromyography; CINHAL, Cumulative Index to Nursing and Allied Health Literature; CNKI, China National Knowledge Infrastructure; MeSH, Medical Subject Headings; HSFA, (Chinese) Health Standards for the Use of Food Additives; CFDA, China Food and Drug Administration.
1. Brown RH, Al-Chalabi A. Amyotrophic lateral sclerosis. N Engl J Med. (2017) 377:162–72. doi: 10.1056/NEJMra1603471
2. Kiernan MC, Vucic S, Cheah BC, Turner MR, Eisen A, Hardiman O, et al. Amyotrophic lateral sclerosis. Lancet. (2011) 377:942–55. doi: 10.1016/S0140-6736(10)61156-7
3. Rosa Silva JP, Santiago Júnior JB, dos Santos EL, de Carvalho FO, de França Costa IMP, Mendonça DMF de. Quality of life and functional independence in amyotrophic lateral sclerosis: a systematic review. Neurosci Biobehav Rev. (2020) 111:1–11. doi: 10.1016/j.neubiorev.2019.12.032
4. Niedermeyer S, Murn M, Choi PJ. Respiratory failure in amyotrophic lateral sclerosis. Chest. (2019) 155:401–8. doi: 10.1016/j.chest.2018.06.035
5. Blasco H, Mavel S, Corcia P, Gordon PH. The glutamate hypothesis in ALS: pathophysiology and drug development. Curr Med Chem. (2014) 21:3551–75. doi: 10.2174/0929867321666140916120118
6. McCauley ME, Baloh RH. Inflammation in ALS/FTD pathogenesis. Acta Neuropathol. (2019) 137:715–30. doi: 10.1007/s00401-018-1933-9
7. Singh A, Kukreti R, Saso L, Kukreti S. Oxidative stress: a key modulator in neurodegenerative diseases. Molecules. (2019) 24:1583. doi: 10.3390/molecules24081583
8. Zuo X, Zhou J, Li Y, Wu K, Chen Z, Luo Z, et al. TDP-43 aggregation induced by oxidative stress causes global mitochondrial imbalance in ALS. Nat Struct Mol Biol. (2021) 28:132–42. doi: 10.1038/s41594-020-00537-7
9. Ross CA, Poirier MA. Protein aggregation and neurodegenerative disease. Nat Med. (2004) 10:S10. doi: 10.1038/nm1066
10. Blokhuis AM, Groen EJN, Koppers M, Van Den Berg LH, Pasterkamp RJ. Protein aggregation in amyotrophic lateral sclerosis. Acta Neuropathol. (2013) 125:777–94. doi: 10.1007/s00401-013-1125-6
11. Islam MT. Oxidative stress and mitochondrial dysfunction-linked neurodegenerative disorders. Neurol Res. (2017) 39:73–82. doi: 10.1080/01616412.2016.1251711
12. Ghavami S, Shojaei S, Yeganeh B, Ande SR, Jangamreddy JR, Mehrpour M, et al. Autophagy and apoptosis dysfunction in neurodegenerative disorders. Prog Neurobiol. (2014) 112:24–49. doi: 10.1016/j.pneurobio.2013.10.004
13. De Vos KJ, Hafezparast M. Neurobiology of axonal transport defects in motor neuron diseases: opportunities for translational research? Neurobiol Dis. (2017) 105:283. doi: 10.1016/j.nbd.2017.02.004
14. Fang T, Al Khleifat A, Meurgey J-H, Jones A, Leigh PN, Bensimon G, et al. Stage at which riluzole treatment prolongs survival in patients with amyotrophic lateral sclerosis: a retrospective analysis of data from a dose-ranging study. Lancet Neurol. (2018) 17:416–22. doi: 10.1016/S1474-4422(18)30054-1
15. Inoue-Shibui A, Kato M, Suzuki N, Kobayashi J, Takai Y, Izumi R, et al. Interstitial pneumonia and other adverse events in riluzole-administered amyotrophic lateral sclerosis patients: a retrospective observational study. BMC Neurol. (2019) 19:72. doi: 10.1186/s12883-019-1299-1
16. Witzel S, Maier A, Steinbach R, Grosskreutz J, Koch JC, Sarikidi A, et al. Safety and effectiveness of long-term intravenous administration of edaravone for treatment of patients with amyotrophic lateral sclerosis. JAMA Neurol. (2022) 79:121. doi: 10.1001/jamaneurol.2021.4893
17. Zhou Q, Wang Y, Zhang J, Shao Y, Li S, Wang Y, et al. Fingerprint analysis of Huolingshengji Formula and its neuroprotective effects in SOD1G93A mouse model of amyotrophic lateral sclerosis. Sci Rep. (2018) 8:1668. doi: 10.1038/s41598-018-19923-9
18. Unschuld P. Huang Di Neijing Suwen. Vol. 67. London: University of California Press (2007). p. 1. doi: 10.1525/9780520928497
19. Xu W, Ren H, Zhi H. Effects of kidney-tonifying, spleen-strengthening and liver-soothing method on amyotrophic lateral sclerosis. Acta Univ Tradit Medicalis Sin Pharmacol Shanghai. (2011) 5:46–9. doi: 10.16306/j.1008-861x.2011.05.014
20. Maoxing Y, Peigen Z, Donglin H, Ying L, Jinnan Y, Qihan Z, et al. Innovative therapy of combined chinese and western medicine in the treatment of motor neuron disease:report of 286 cases. Chin J Hyg Rescue. (2018) 4:273–80. doi: 10.3877/cma.j.issn.2095-9133.2018.05.003
21. Xu-ying Z, Hong-zhi Z, Hua-qiang L, Shu-yu Z, Jing C, Jun W, et al. Clinical efficacy and safety evaluation of supplementary sijunzi decoction in treatment of ALS patients with sple-nasthenic syndrome. Clin Misdiagn Misther. (2017) 30:81–7. doi: 10.3969/j.issn.1002-3429.2017.01.028
22. GU Jianxiong, JIANG Yuwen GX. Treatment experience of amyotrophic lateral sclerosis by Professor GU Xizhen from spleen and kidney. Tianjin J Trad Chin. (2020) 37:438–41. doi: 10.11656/j.issn.1672-1519.2020.04.19
23. Pan W, Su X, Bao J, Wang J, Zhu J, Cai D, et al. Open randomized clinical trial on JWSJZ decoction for the treatment of ALS patients. Evidence-Based Complement Altern Med. (2013) 2013:347525. doi: 10.1155/2013/347525
24. Scheid V. Chinese Herbal Medicine : Formulas & Strategies / Volker Scheid (2009). Available online at: http://www.loc.gov/catdir/toc/fy0905/2008943299.html (accessed August 28, 2022).
25. Chen H, Li, D, Han, C,. Chinese External medicine - Chapter 1, History of External Medicine. People's Medical Pub. House (2011). p. 853. Available online at: https://books.google.de/books/about/Chinese_External_Medicine.html?id=wG0QDgAAQBAJ&redir_esc=y (accessed November 27, 2021).
26. Deepthi Venna D, Khan AB. Role of adhesives in transdermal drug delivery: a review. Int J Pharm Sci Res. (2012) 4:3559–64. doi: 10.13040/IJPSR.0975-8232.3(10).3559-64
27. Tian S, Miao M-S. Mechanism of external use of traditional chinese medicine-“three micro-regulations for balance” based on neural-endocrine-immune network. Chin J Exp Tradit Med Formula. (2019) 24:6–12. doi: 10.13422/j.cnki.syfjx.20190436
28. Prausnitz MR, Langer R. Transdermal drug delivery. Nat Biotechnol. (2008) 26:1261–8. doi: 10.1038/nbt.1504
29. Kaestli L-Z, Wasilewski-Rasca A-F, Bonnabry P, Vogt-Ferrier N. Use of transdermal drug formulations in the elderly. Drugs Aging. (2008) 25:269–80. doi: 10.2165/00002512-200825040-00001
30. Cedarbaum JM, Stambler N, Malta E, Fuller C, Hilt D, Thurmond B, et al. The ALSFRS-R: a revised ALS functional rating scale that incorporates assessments of respiratory function. J Neurol Sci. (1999) 169:13–21. doi: 10.1016/S0022-510X(99)00210-5
31. Brooks BR, Miller RG, Swash M, Munsat TL. El Escorial revisited: revised criteria for the diagnosis of amyotrophic lateral sclerosis. Amyotroph Lateral Scler Other Motor Neuron Disord. (2000) 1:293–9. doi: 10.1080/146608200300079536
32. Zheng X, Schröder J, Sima D, Wang M, Wang Q, Pan W. Amyotrophic lateral sclerosis symptom score in integrative treatments (ALS-SSIT) for evaluating therapeutic effect of traditional Chinese medicine: a prospective study. Comput Math Methods Med. (2022) 2022:7594481. doi: 10.1155/2022/7594481
33. Kimura F, Fujimura C, Ishida S, Nakajima H, Furutama D, Uehara H, et al. Progression rate of ALSFRS-R at time of diagnosis predicts survival time in ALS. Neurology. (2006) 66:265–7. doi: 10.1212/01.wnl.0000194316.91908.8a
34. Makary MM, Weerasekara A, Rodham H, Hightower BG, Tseng CEJ, Chan J, et al. Comparison of two clinical upper motor neuron burden rating scales in ALS using quantitative brain imaging. ACS Chem Neurosci. (2021) 12:906–16. doi: 10.1021/acschemneuro.0c00772
35. Eisen A. Motor neurone disease. In:Turner MR, Kiernan MC, , editors. Landmark Papers in Neurology. New York: Oxford University Press (2015). p. 257–88. doi: 10.1093/med/9780199658602.003.0009
36. Bakker LA, Schröder CD, van Es MA, Westers P, Visser-Meily JMA, van den Berg LH. Assessment of the factorial validity and reliability of the ALSFRS-R: a revision of its measurement model. J Neurol. (2017) 264:1413–20. doi: 10.1007/s00415-017-8538-4
37. Fournier CN, Bedlack R, Quinn C, Russell J, Beckwith D, Kaminski KH, et al. Development and validation of the rasch-built overall amyotrophic lateral sclerosis disability scale (ROADS). JAMA Neurol. (2020) 77:480–8. doi: 10.1001/jamaneurol.2019.4490
38. Pan W, Qiudong W, Xuanlu Z, Dandan S, Joana S, Mingzhe W. Performance evaluation of traditional Chinese medicine evaluation scale (ALS-SSIT scale) for therapeutic efficacy in amyotrophic lateral sclerosis. J Neurol Neurorehabilitation. (2021) 17:13–8.
39. Yadav N, Mittal A, Ali J, Sahoo J. Current updates in transdermal therapeutic systems and their role in neurological disorders. Curr Protein Pept Sci. (2020) 22:458–69. doi: 10.2174/1389203721999201111195512
40. Jeong WY, Kwon M, Choi HE, Kim KS. Recent advances in transdermal drug delivery systems: a review. Biomater Res. (2021) 25:1–15. doi: 10.1186/s40824-021-00226-6
41. Rodrigues ACZ, Messi ML, Wang Z-M, Abba MC, Pereyra A, Birbrair A, et al. The sympathetic nervous system regulates skeletal muscle motor innervation and acetylcholine receptor stability. Acta Physiol. (2019) 225:e13195. doi: 10.1111/apha.13195
42. Jaiswal MK. Riluzole and edaravone: a tale of two amyotrophic lateral sclerosis drugs. Med Res Rev. (2019) 39:733–48. doi: 10.1002/med.21528
43. Doble A. The pharmacology and mechanism of action of riluzole. Neurology. (1996) 47:S233–41. doi: 10.1212/WNL.47.6_Suppl_4.233S
44. Guo Z, Wu HT, Li XX, Yu Y, Gu RZ, Lan R, et al. Edaravone protects rat astrocytes from oxidative or neurotoxic inflammatory insults by restoring Akt/Bcl-2/Caspase-3 signaling axis. IBRO reports. (2020) 8:122–8. doi: 10.1016/j.ibror.2020.04.003
45. Zhu J, Shen L, Lin X, Hong Y, Feng Y. Clinical research on traditional chinese medicine compounds and their preparations for amyotrophic lateral sclerosis. Biomed Pharmacother. (2017) 96:854–64. doi: 10.1016/j.biopha.2017.09.135
46. Liu H, Chen W, Lu P, Ma Y, Liang X, Liu Y. Ginsenoside Rg1 attenuates the inflammation and oxidative stress induced by diabetic nephropathy through regulating the PI3K/AKT/FOXO3 pathway. Ann Transl Med. (2021) 9:1789–1789. doi: 10.21037/atm-21-6234
47. Wang C-H, Safwan S, Cheng M-C, Liao T-Y, Cheng L-C, Chen T-A, et al. Protective evaluation of compounds extracted from root of rhodiola rosea L. against methylglyoxal-induced toxicity in a neuronal cell line. Molecules. (2020) 25:2801. doi: 10.3390/molecules25122801
48. Nie A, Chao Y, Zhang X, Jia W, Zhou Z, Zhu C. Phytochemistry and pharmacological activities of wolfiporia cocos (FA Wolf) Ryvarden & Gilb. Front Pharmacol. (2020) 11:505249. doi: 10.3389/fphar.2020.505249
49. Ruqiao L, Yueli C, Xuelan Z, Huifen L, Xin Z, Danjie Z, et al. Rhizoma atractylodis macrocephalae: a review of photochemistry, pharmacokinetics, and pharmacology. Pharmazie. (2020) 75:42–55. doi: 10.1691/ph.2020.9738
50. Richard SA. Exploring the pivotal immunomodulatory and anti-inflammatory potentials of glycyrrhizic and glycyrrhetinic acids. Mediators Inflamm. (2021) 2021:6699560. doi: 10.1155/2021/6699560
51. Wu Y, Wang Z, Du Q, Zhu Z, Chen T, Xue Y, et al. Pharmacological effects and underlying mechanisms of licorice-derived flavonoids. Evid Based Complement Alternat Med. (2022) 2022:9523071. doi: 10.1155/2022/9523071
52. Bratkov VM, Shkondrov AM, Zdraveva PK, Krasteva IN. Flavonoids from the genus astragalus: phytochemistry and biological activity. Pharmacogn Rev. (2016) 10:11–32. doi: 10.4103/0973-7847.176550
53. Sze SCW, Tong Y, Ng TB, Cheng CLY, Cheung HP. Herba epimedii: antioxidative properties and its medical implications. Molecules. (2010) 15:7861–70. doi: 10.3390/molecules15117861
54. Nam SM, Choi JH, Choi S-H, Cho H-J, Cho Y-J, Rhim H, et al. Ginseng gintonin alleviates neurological symptoms in the G93A-SOD1 transgenic mouse model of amyotrophic lateral sclerosis through lysophosphatidic acid 1 receptor. J Ginseng Res. (2021) 45:390–400. doi: 10.1016/j.jgr.2020.04.002
55. Seok YM, Yoo J-M, Nam Y, Kim J, Kim JS, Son J-H, et al. Mountain ginseng inhibits skeletal muscle atrophy by decreasing muscle RING finger protein-1 and atrogin1 through forkhead box O3 in L6 myotubes. J Ethnopharmacol. (2021) 270:113557. doi: 10.1016/j.jep.2020.113557
56. Hu R, Wang M-Q, Liu L-Y, You H-Y, Wu X-H, Liu Y-Y, et al. Calycosin inhibited autophagy and oxidative stress in chronic kidney disease skeletal muscle atrophy by regulating AMPK/SKP2/CARM1 signalling pathway. J Cell Mol Med. (2020) 24:11084–99. doi: 10.1111/jcmm.15514
57. Lee EJ, Shaikh S, Ahmad K, Ahmad SS, Lim JH, Park S, et al. Isolation and characterization of compounds from glycyrrhiza uralensis as therapeutic agents for the muscle disorders. Int J Mol Sci. (2021) 22:876. doi: 10.3390/ijms22020876
Keywords: sporadic amyotrophic lateral sclerosis, RTC, placebo control, herbal plaster, Traditional Chinese Medicine, dysphagia
Citation: Schröder S, Wang M, Sima D, Schröder J, Zhu X, Zheng X, Liu L, Li T, Wang Q, Friedemann T, Liu T and Pan W (2022) Slower progression of amyotrophic lateral sclerosis with external application of a Chinese herbal plaster–The randomized, placebo-controlled triple-blinded ALS-CHEPLA trial. Front. Neurol. 13:990802. doi: 10.3389/fneur.2022.990802
Received: 10 July 2022; Accepted: 13 September 2022;
Published: 17 October 2022.
Edited by:
Jens Schmidt, University Medical Center Göttingen, GermanyReviewed by:
Felipe Patricio, Benemérita Universidad Autónoma de Puebla, MexicoCopyright © 2022 Schröder, Wang, Sima, Schröder, Zhu, Zheng, Liu, Li, Wang, Friedemann, Liu and Pan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Weidong Pan, cGFud2RAbWVkbWFpbC5jb20uY24=; Thomas Friedemann, RnJpZWRlbWFubkB0Y20tYW0tdWtlLmRl; Te Liu, bGl1dGUxOTc5QDEyNi5jb20=
†These authors have contributed equally to this work and share first authorship
‡These authors have contributed equally to this work and share senior authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.