 Xueming Fan
Xueming Fan Guojing Fu
Guojing Fu Liuding Wang
Liuding Wang Wei Shen
Wei Shen Yunling Zhang
Yunling Zhang- Xiyuan Hospital, China Academy of Chinese Medical Sciences, Beijing, China
Background: Tension-type headache (TTH) is the most prevalent headache in the clinical practice, leading to impaired social activities, work-related disability, and heavy financial burdens. Previous studies have described possible inducement, potential pathophysiology, and clinical management of TTH; however, due to the lack of attention, literature involving bibliometric analysis is sporadic. Therefore, this study aimed to explore the current hotspots and future directions of the TTH field by bibliometric analysis.
Methods: By using CiteSpace and VOSviewer, literature regarding TTH between 2002 and 2021 from the Web of Science database was summarized and extracted. Annual publication trend, the most productive countries/regions and institutions, distribution of categories, co-citation of journals and references, and co-occurrence of keywords were analyzed.
Results: A total of 3,379 publications were included in the final visualization, indicating a stable trend in current research and a lack of breakthroughs over the past decades. These studies were mainly conducted in 120 countries/regions led by the United States and more than 600 institutions. Four eternal core themes were identified in TTH, including neurosciences, nursing, developmental psychology, and general/internal medicine. Cephalalgia ranked first, with the highest number of literature, and is the most influential journal in this area. Keyword analysis demonstrated that the similarities and differences between migraine and TTH, epidemiological studies, clinical double-blind trials, and potential populations have become key issues in the TTH field.
Conclusion: TTH has received less attention and breakthroughs in the past 20 years. To promote coordinated development between regions to fight headaches, cooperation and exchanges between countries and institutions are essential in the future. Relevant studies about headaches in children and adolescents, inducing factors such as emotional triggers and sleep disorders, concomitant diseases, possible pathogenesis, and headache treatments, are in the spotlight in recent years. This study offers a powerful roadmap for further research in this field.
Introduction
Headache is a critical factor in increasing the global burden of disease (1), and tension-type headache (TTH) occurs in 42% of the adult population with an active headache disorder (2), which is a major factor that affects the disability-adjusted life-years of young and middle-aged people (3). TTH is the most common form of primary headache (4); typically, pain is often described as a pressing or tightening sensation of mild-to-moderate intensity in the bilateral regions of the head (5, 6). Based on headache frequency, TTH can be divided into three subtypes, namely, infrequent episodic, frequent episodic, and chronic TTH; infrequent episodic TTH has little effect on individuals with rare medical services, whereas chronic TTH is often associated with work-related disability and difficult treatment (5, 7). The lifetime prevalence of TTH in the general population ranges from 30 to 78% (8), with a higher incidence in female than in male patients (9). TTH has a huge effect on emotions, daily work, and general living activities, which not only leads to impaired social activities (10), such as a considerable number of work absences (11), but also brings a heavy economic burden to society (12). The potential pathophysiology of TTH remains poorly understood, and previous studies have reported that peripheral and central mechanisms play an important role in this process (13). Multimodal management is tailored for each patient with TTH according to different clinical symptoms and may include various therapies such as pharmacotherapy, behavioral therapies, and healthy lifestyle habits (5). Despite the widespread prevalence and considerable disability of TTH, a more comprehensive bibliometric analysis remains unavailable due to the lack of attention in this area.
To indicate critical issues in future studies, bibliometric analysis can reveal the current research status in a given field based on statistical and mathematical methods of publications (14). By using computerized analytic techniques, bibliometric analysis can estimate the most influential authors, journals, countries, departments, and institutions in a research area to identify publications that have influenced clinical practice and developed research ideas (15–17). The bibliometric analysis software, such as CiteSpace and VOSviewer, typically use scientific publications as input and generate an interactive visual network for statistical analysis (18). CiteSpace is a Java application that provides a progressive visual exploration of highly cited publications, frontier development in the current area, and emerging trends of research topics through knowledge discovery in bibliographic databases (19, 20). VOSviewer constructs bibliometric maps of influential authors, journals, and keywords in co-citation or co-occurrence analysis, with powerful functions and a user-friendly interface (21). These software have become important scientific mapping tools in the medical area, illuminating development trends and forecasts research outlook in a given field (22). Using the CiteSpace and VOSviewer software, this study was conducted to uncover the valuable insights and explore research hotspots of TTH over the past 20 years.
Materials and methods
Data collection
Citation data were retrieved from the Science Citation Index Expanded (SCI-expanded) of the Web of Science Core Collection database as of 17 January 2022. Considering the tremendous development of TTH in recent years, the search keyword was set to “tension-type headache” with a time span of 20 years from 2002 to 2021. Full records and cited references of publications were downloaded directly from the database, and document types were limited to articles or reviews.
Data analysis
CiteSpace 5.8 R3 was adopted to generate visualization analysis and characteristic mapping, including a cooperation map of countries/regions and institutions, distribution of categories, number of citations, and keyword analysis. VOSviewer 1.6.17 was used to optimize unaesthetic diagrams. Moreover, the latest H-index, SCImago Institutions and Journal Rank, and Impact Factor were added for a clear and integrated analysis. ArcGIS 10.8 was applied to examine the national distribution of publications.
Results
A total of 3,497 records were extracted from the database and 118 irrelevant articles were excluded, including 92 proceedings papers, 24 early access, and two book chapters. The remaining 3,379 records were exported for visualization analysis, of which 2,672 articles accounted for 79.08% of the total, followed by 707 reviews (20.92%). The retrieval process is presented in Figure 1.
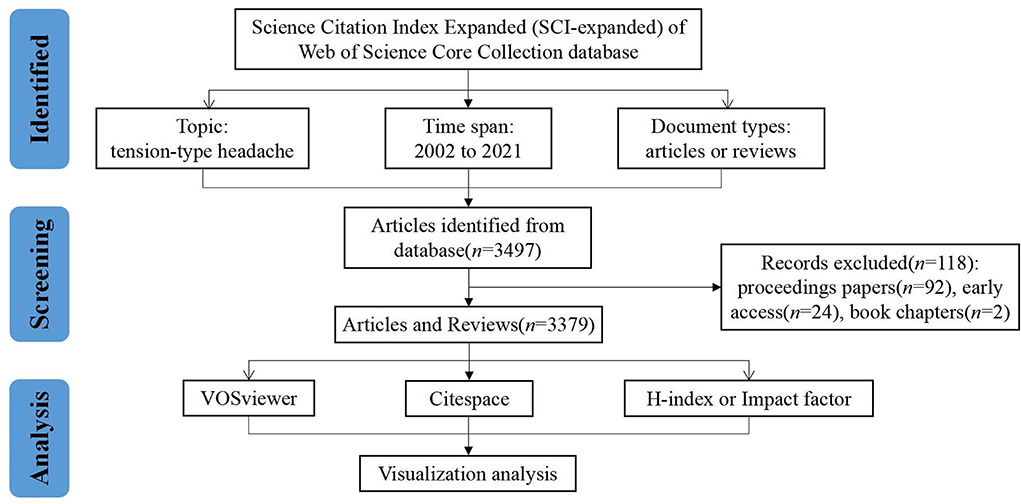
Figure 1. Flowchart of literature selection.
Annual publication outputs
The number of articles published in a specific period directly reflects the development trend of research in this field. As shown in Figure 2, despite the overall upward trend, publication growth on the topic of TTH can be divided into two periods, a rapid growth phase in the first decade and a slow phase in the second decade. From 2002 to 2009, publication outputs increased steadily year by year, but the volume fluctuated greatly from 2010 to 2021.
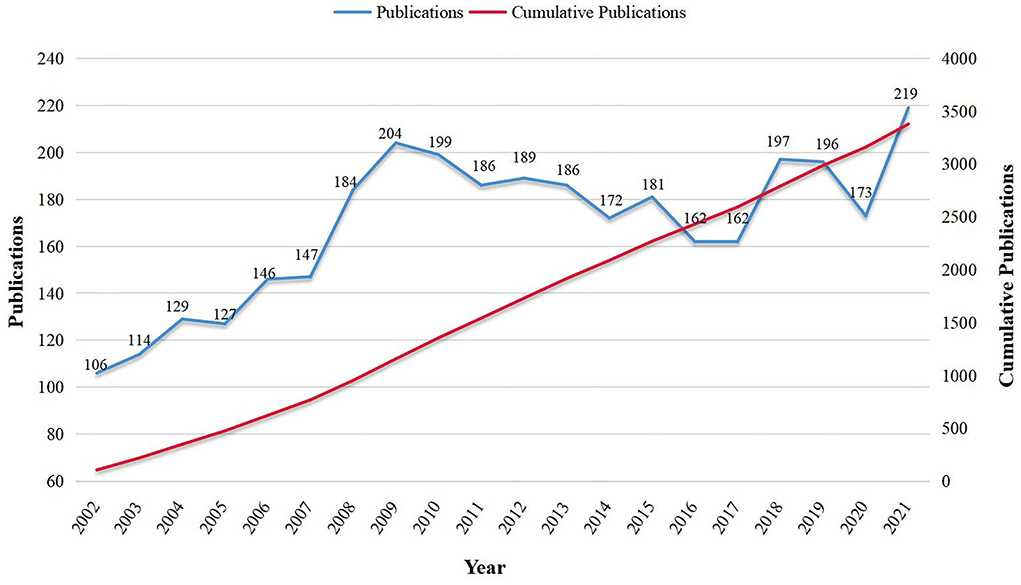
Figure 2. Publication trend of tension-type headache over the past 20 years.
Cooperation map of countries/regions
TTH research has been conducted in 120 countries/regions over the past 20 years (Figure 3A). In North America, the United States ranked first with 794 articles, followed by Italy and Germany in Europe with 439 and 426 publications, respectively. These countries contributed over one-third of the total number of publications and were labeled as three central research forces in this area. Denmark, the United Kingdom, and Spain in Europe, as well as Turkey in Asia, with more than 200 publications, will have great development space in the future. Besides, 76 countries (63.33% of the total) have <10 articles since 2002, and many countries/regions are still blank in this area.
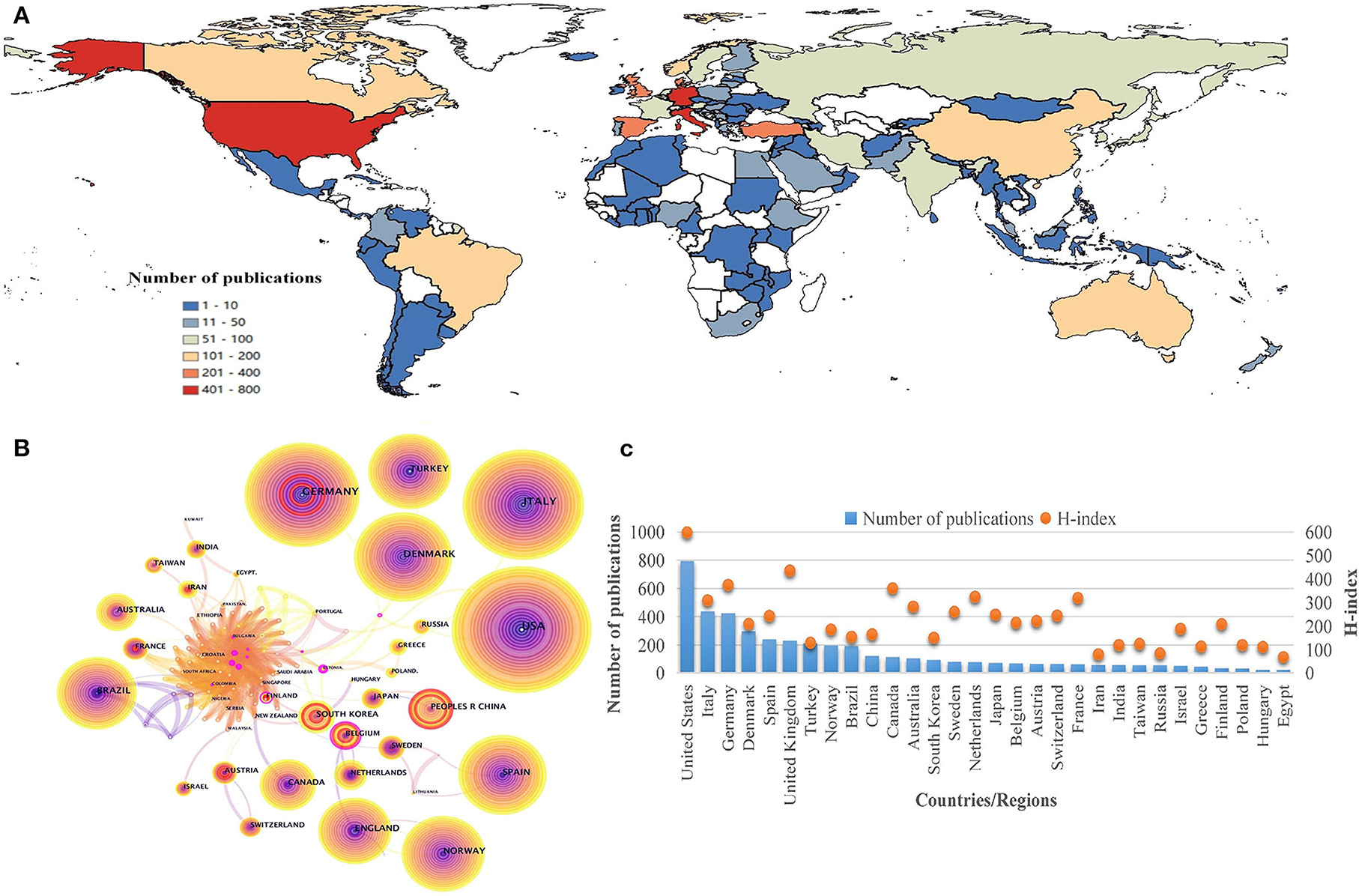
Figure 3. Geographical distribution and cooperation map of countries/regions in tension-type headache: (A) geographical heat map of publications; (B) co-occurrence network of countries/regions; (C) number of publications and H-index of countries/regions.
Nodes in CiteSpace were selected to obtain the cooperation network map of countries/regions (Figure 3B). The node size represents the overall number of publications, and the lines between them indicate the cooperation relationship. Red nodes manifest the frequency burst, while pink rimmed nodes refer to those with high centrality, highlighting the importance of nodes in network (23). Germany, China, Belgium, South Korea, Sweden, and Austria have seen an increase in the number of publications over a certain period, speculating that they may have made innovative discoveries in TTH research. The H-index is a valuable indicator aimed at evaluating scientific influence of disciplines. Compared with other indexes, H-index can be more accurate in predicting future research achievement (24). By searching the H-index of the neurology field (Figure 3C), the United States has the highest score of 598, identifying its obvious advantage and outstanding contribution to TTH. The United Kingdom (436), Germany (375), and Canada (361) also made significant achievements in this area.
Cooperation map of institutions
More than 600 institutions have explored TTH research over the past 20 years (Figure 4A). Among them, the University of Copenhagen in Denmark ranked first with 150 articles published, indicating its strong scientific ability in this area. The Universidad Rey Juan Carlos in Spain (115), Norwegian University of Science and Technology in Norway (103), and Aalborg University in Denmark (91) have also made significant contributions. Besides, the Universidade de São Paulo in Brazil, Imperial College London in the United Kingdom, and Universita Degli Studi di Roma La Sapienza in Italy have experienced a rapid increase in a certain period, indicating a breakthrough in these institutions. The SCImago Institutions Rankings in Medicine provide data references for scientific impact of institutions (25). Harvard University (1), Harvard Medical School (2), and the University of Washington (16) in the United States, as well as Medizinische Universitat Wien in Austria (121), have made vital contributions to TTH research field (Figure 4B).
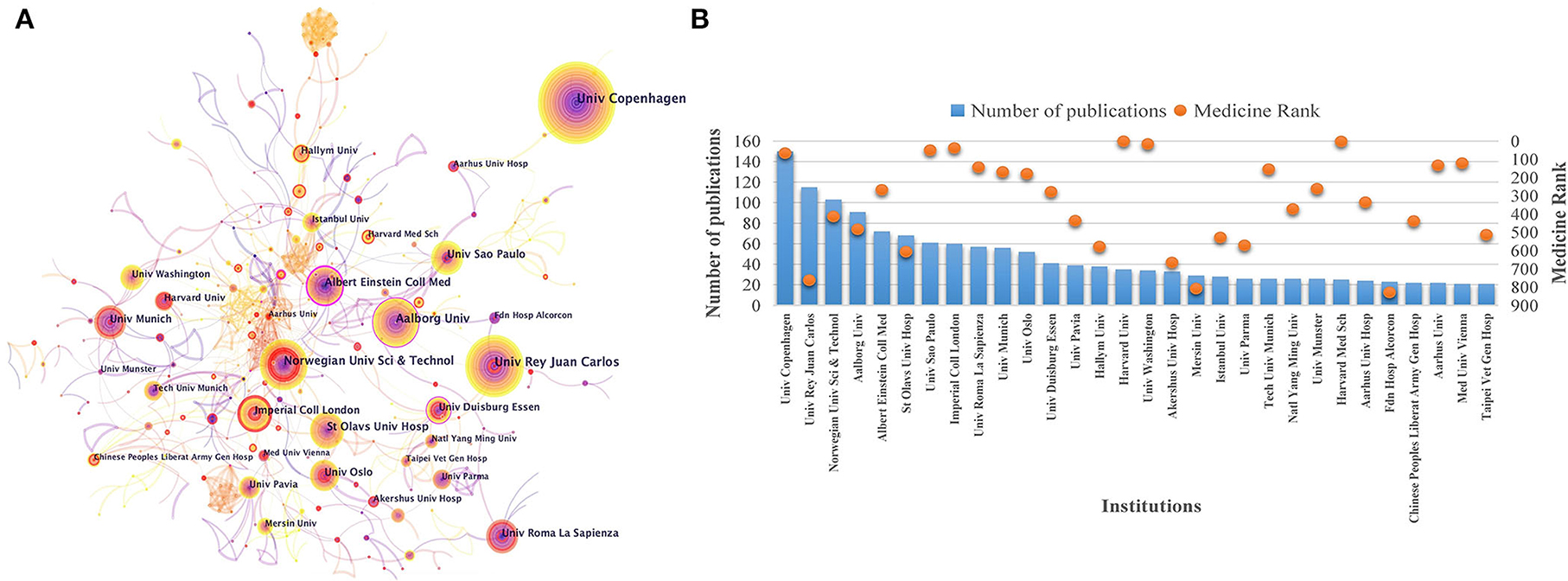
Figure 4. Cooperation maps of institutions in tension-type headache: (A) co-occurrence network of institutions; (B) number of publications and SCImago rank of institutions.
Distribution of categories
To visualize changes in interdisciplinary situations in the TTH field, the alluvial diagram was adopted to highlight and summarize the structural variation of Web of Science categories (Figure 5). The network is displayed as vertical stacks connected by streamlines that joint modules containing the same nodes. The height changes of the streamlines are proportional to the aggregated flow of nodes in the connected modules (26). Structural changes from one period to the next are represented by mergers and divergences, with different categories plotted in different colors. The interdisciplinary change has been ongoing from 13 modules in 2002–2003 to 14 modules in 2020–2021. The modules represented by neurosciences, healthcare sciences/services, genetics/heredity, biology, and general/internal medicine are gradually summarized into the four eternal core themes led by neurosciences, nursing, developmental psychology, and general/internal medicine. Besides, physics, plant sciences, and public environmental/occupational health as newly emerging themes are in the spotlight in recent years.
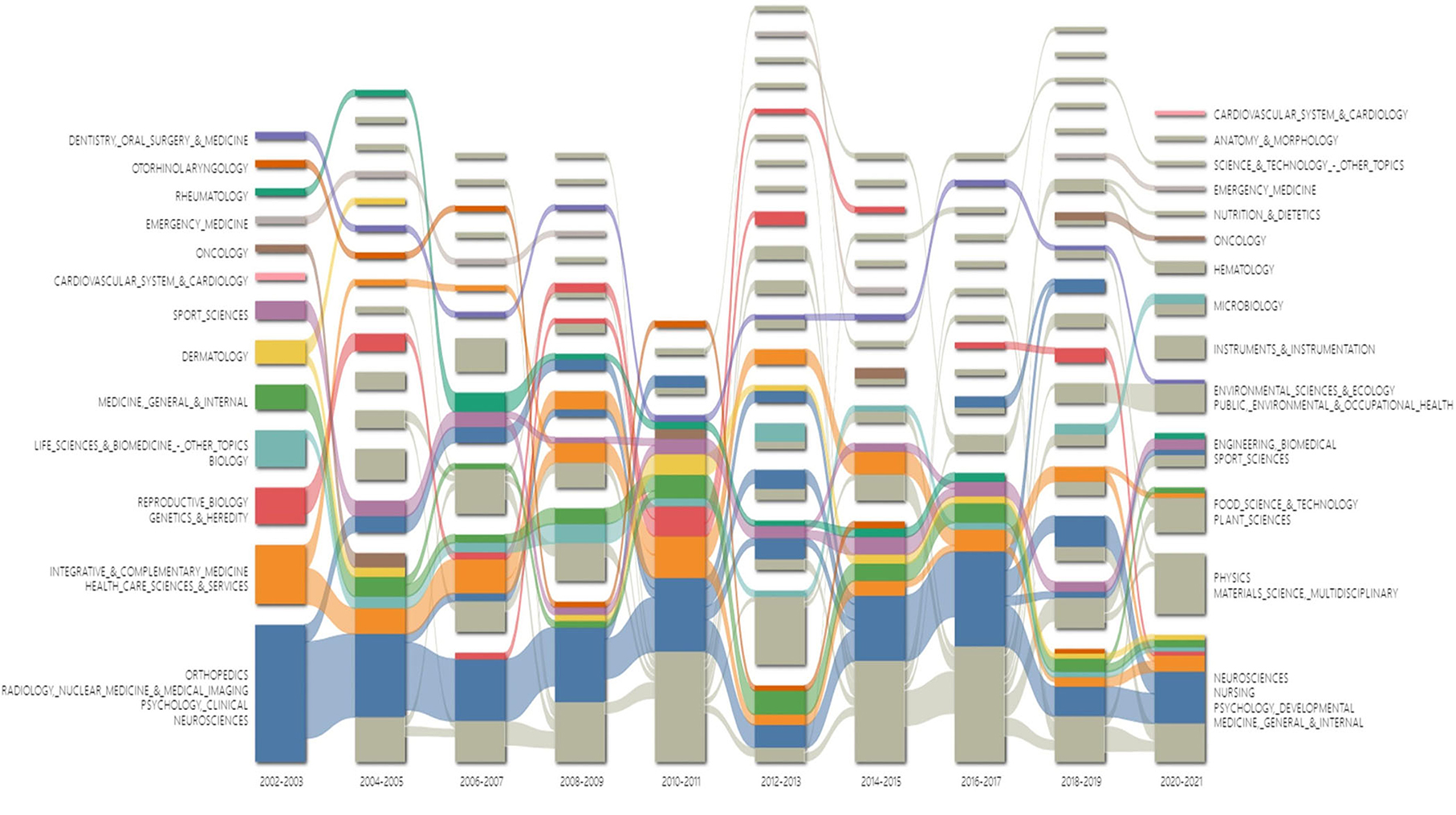
Figure 5. Alluvial diagram of categories in tension-type headache during 2002–2021.
The statistical indicators of the top 15 categories are listed in Table 1, indicating that TTH is a multidisciplinary research area. Neurosciences and neurology ranked first with 2,339 articles published since 2002, followed by clinical neurology with 1,296 articles. Although the number of publications is much lower than the top categories, public environmental/occupational health, and pediatrics have high betweenness centrality, indicating their critical position in this field.
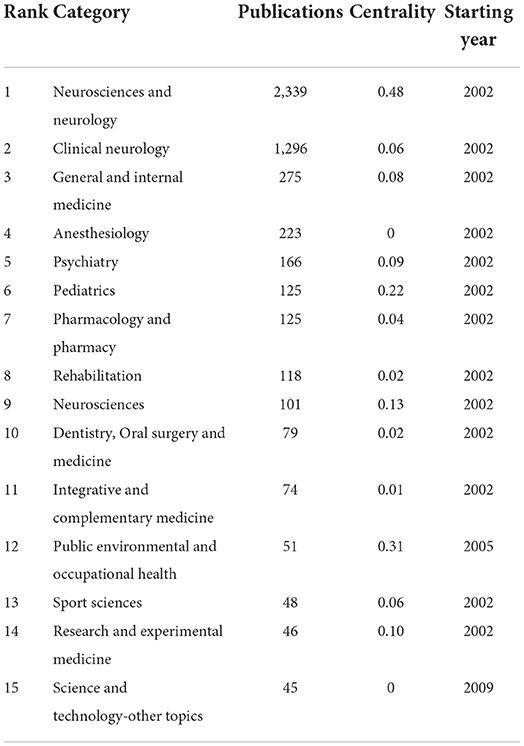
Table 1. Top 15 categories in the tension-type headache field.
Journal and co-cited journals
A total of 620 journals reported research in TTH, and the top 15 are presented in Table 2. Cephalalgia ranks first with 419 publications (12.40%), followed by Headache (364, 10.77%) and Journal of Headache and Pain (264, 7.81%). Among the top 15 academic journals, five are from the United States, four from the United Kingdom, and two from Italy, showing a strong research foundation in these countries. Six journals have an impact factor >5, including Neurology (11.800), Journal of Headache and Pain (8.588), Pain (7.926), European Journal of Neurology (6.288), Cephalalgia (6.075), and Headache (5.311). SCImago Journal Rankings measure the scientific impact, influence, and prestige of journals based on the average number of weighted citations (27). Eight journals (Cephalalgia, Headache, Journal of Headache and Pain, Pain, Neurology, European Journal of Pain, European Journal of Neurology, and Frontiers in Neurology) are considered of Q1 quality with far-reaching development prospects.
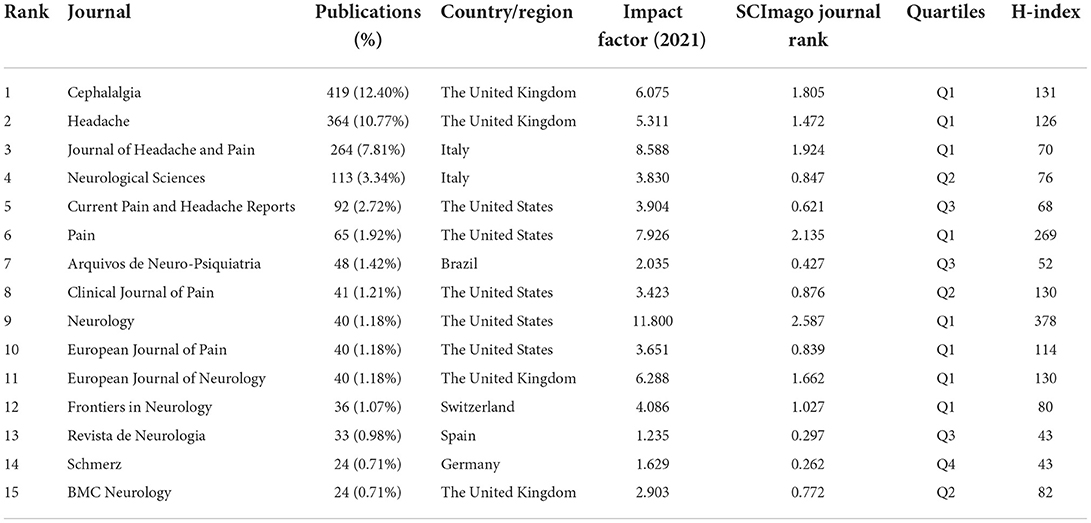
Table 2. Top 15 journals in the tension-type headache field.
The influence of journals in a particular research field depends on the number of co-citations, i.e., when two articles published in different journals were cited in a third article of another journal. The analysis was performed in VOSviewer (Figure 6). The clusters were generated based on citation links and were marked with different colors. The size of the node indicates the co-citated number of journals, and the lines between them represent the co-citation relationship. Cephalalgia, hosted by SAGE Publications Ltd in the United Kingdom, is the most influential journal with 3,345 citations, indicating the highest recognition and authority in the TTH area. Compared with journal analysis, in the top co-cited journals, six of 15 have an impact factor >10, including Lancet (202.731), JAMA – Journal of the American Medical Association (157.335), Lancet Neurology (59.935), Brain (15.255), Journal of Neurology, Neurosurgery and Psychiatry (13.654), and Neurology (11.800), which demonstrated that the theoretical sources of TTH articles are of high quality.
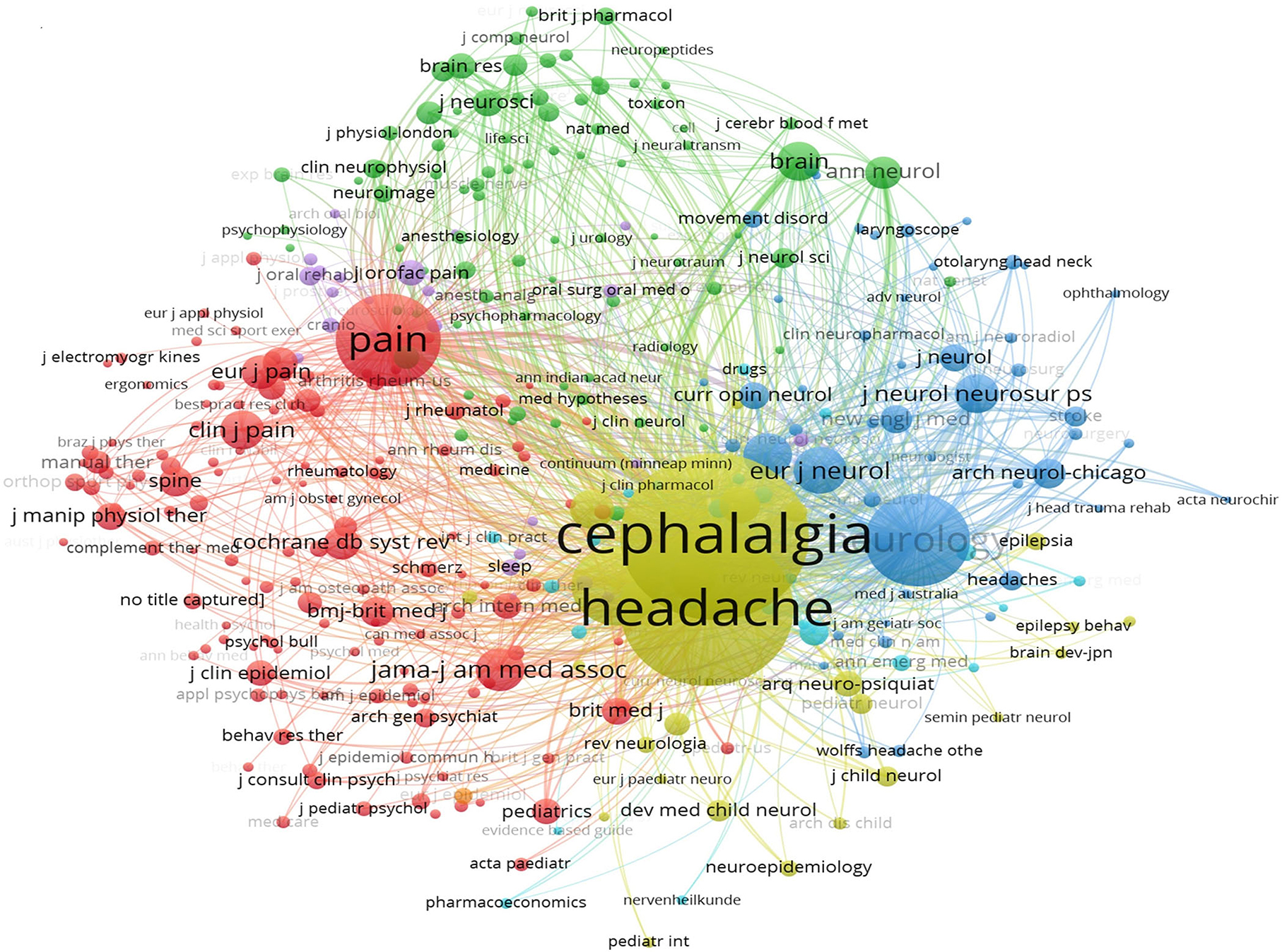
Figure 6. Co-cited journals in tension-type headache.
Co-cited references
A total of 1,420 co-cited references were analyzed, and the top 15 are listed in Table 3. The review “Migraine pathophysiology and its clinical implications” (28) in Cephalalgia ranked first with 374 citations. Other references were cited between 40 and 300 times. In addition, topics covered by highly co-cited references include epidemiological studies, clinical guidelines, and progress reports. The top 15 co-cited references were all published in journals with an impact factor >5, and five were in top journals, including two in Lancet (202.731) and three in Lancet Neurology (59.935).
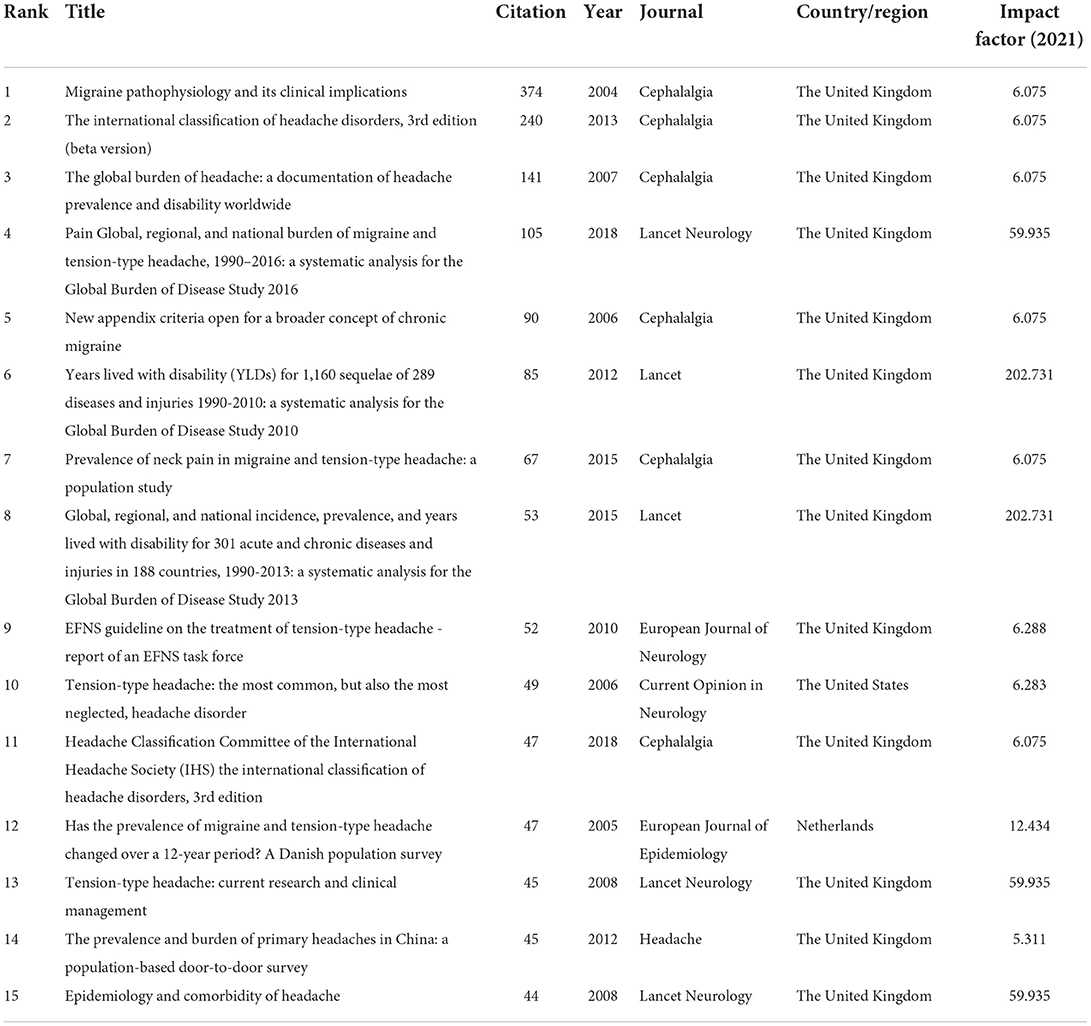
Table 3. Top 15 co-cited references in the tension-type headache field.
Co-cited network and cluster analysis of references was conducted in CiteSpace (Figure 7). Color corresponds to the year in which the publications appeared, and the depth of the color represents time. All references were divided into 24 clusters with active co-citation relationships between them, including pain sensitivity (#3), chronic daily headache (#9), acupuncture (#16), trigger points (#19), botulinum toxin a (#22), and amitriptyline (#21). Clusters located in the upper part of the figure are lighter in color, indicating that calcitonin gene-related peptide (CGRP), insomnia, child and adolescent headache, trigger factors, and magnesium are research hotspots in recent years.

Figure 7. Co-cited networks and cluster diagrams of references in tension-type headache.
Keyword analysis
Keyword analysis provided a typical overview of research topics, reflecting the hotspots and directions in a particular field. The network mapping of high-frequency keywords was performed in VOSviewer (Figure 8A). The keyword “tension-type headache” ranked first with 2,171 times, which is consistent with the research topic. In addition, the top high-frequency keywords included migraine (1,042), prevalence (850), double-blind (398), epidemiology (393), and population (377), leading to speculations that identifying similarities and differences between migraine and TTH, strengthening epidemiological research, conducting clinical double-blind trials, and searching potential population have become key issues in the TTH area.
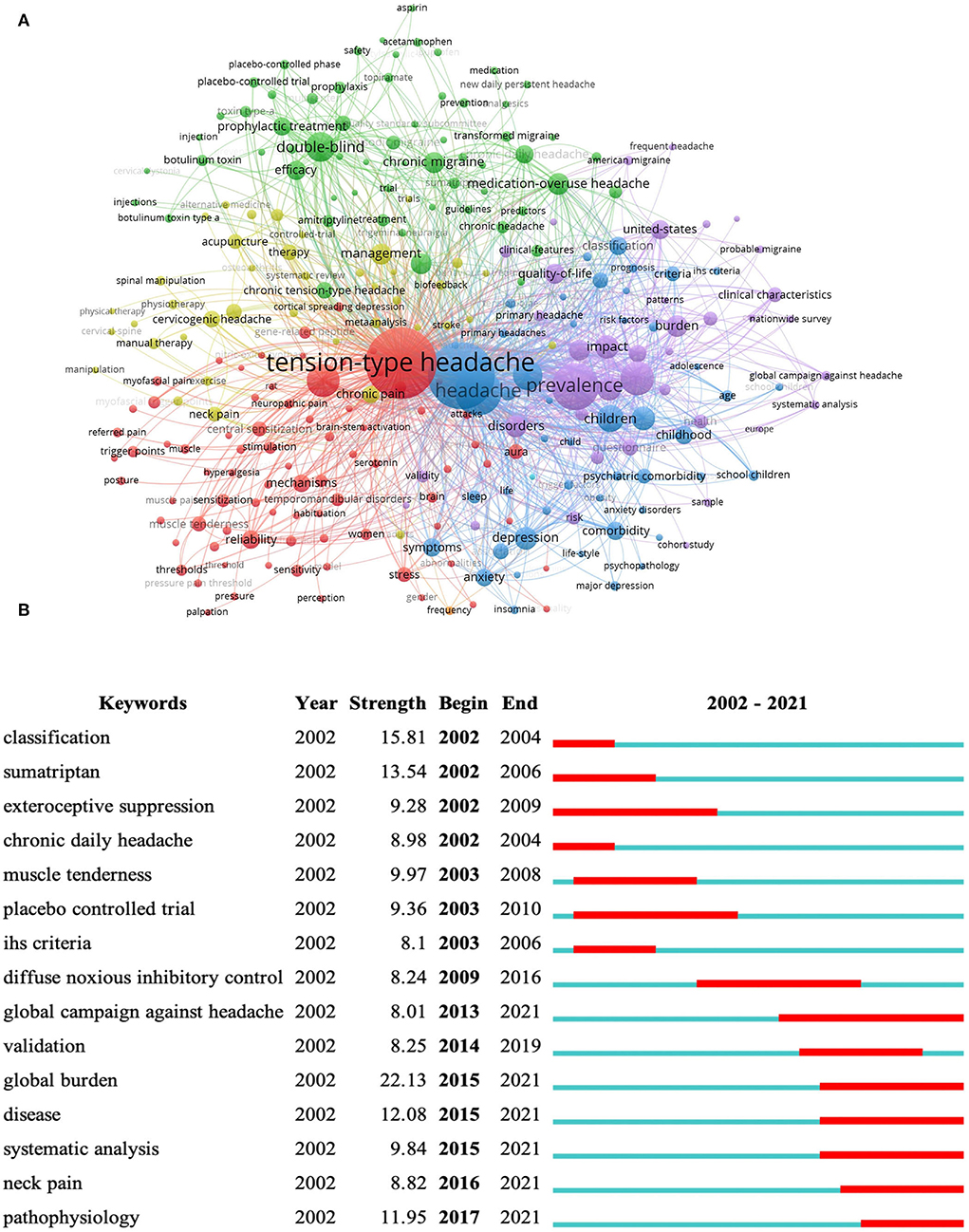
Figure 8. Keyword analyses in tension-type headache: (A) co-occurrence network of keywords; (B) top 15 keywords with the strongest citation bursts.
Keywords with citation bursts indicate the rapid increase in research topics in a given period and highlight the possible research priorities in the near future. The top 15 with the strongest citation bursts were identified in CiteSpace (Figure 8B). Keywords such as classification (15.81, 2002–2004), muscle tenderness (9.97, 2003–2008), exteroceptive suppression (9.28, 2002–2009), and International Headache Society (IHS) criteria (8.1, 2003–2006) inferred that the classification criteria of the subtypes and mechanism of peripheral stimulation were the hotspots of TTH in the first 10 years; while keywords like global burden (22.13, 2015–2021), pathophysiology (11.95, 2017–2021), diffuse noxious inhibitory control (8.24, 2009–2016), and global campaign against headache (8.01, 2013–2021) manifested that the globalization of TTH damage and pathogenesis of central sensitization have become the focus of current research in the TTH field.
Besides, to better illustrate the current hotspots and future directions, this study conducted manual statistics based on the top five keywords in each classification, including potential population, induction factors, concomitant diseases, possible pathogenesis, and clinical therapies (Figure 9).
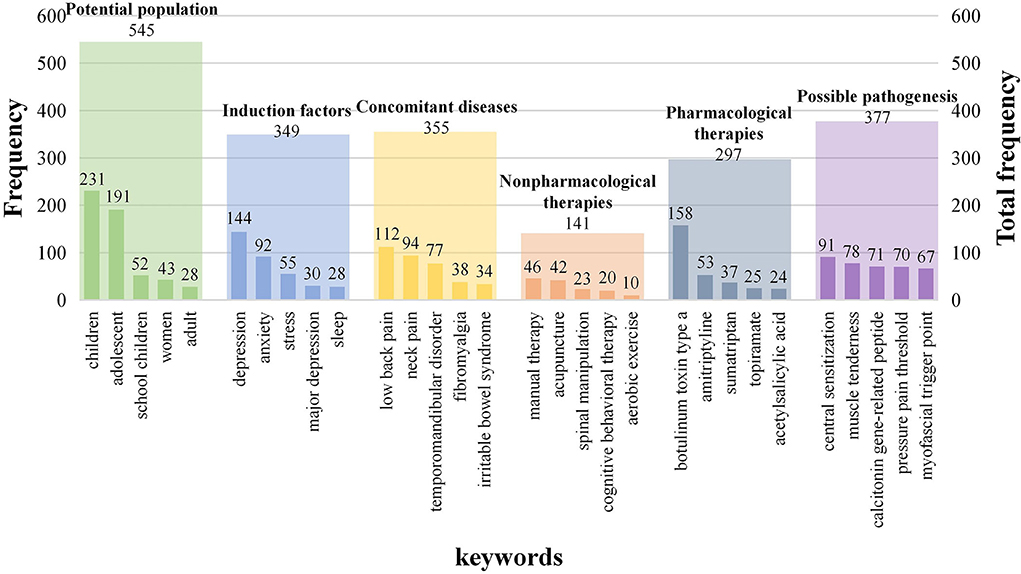
Figure 9. Keyword analyses in five dimensions.
Discussion
General information
As regards annual publication outputs, the trend of literature published from 2002 to 2021 went through two growth stages, publications in 2021 were just 2.07 times over 2002, manifesting a stable trend in current research and a lack of breakthroughs over the past decades. The finding that most patients with TTH rarely seek medical help compared with migraines or other type of headaches is probably the main reason that this area of research received less attention from health authorities, clinical researchers, or professional pharmacologists (5, 29); and as a result, TTH has made little progress since the early 2010s.
On the cooperation networks of countries and institutions, although TTH studies have been conducted in 120 countries led by the United States and more than 600 institutions, most regions still lacked study data in the area. This phenomenon can be explained from two aspects. The social perception of headache damage is at low level in developing countries, leading to less investment in research funds. In addition, due to brain drain, backward technology, and lack of frontiers, the majority of publications on headache disorders still come from developed countries (30–32). Such uneven development among regions revealed that the negative effects of TTH have not received widespread attention. Although coordinated development between regions and institutions remains inadequate, the current cooperation between countries indicated an active relationship. Lifting The Burden, a UK-registered charity organization, established an official relationship with the World Health Organization to conduct the Global Campaign against Headache (33), which, to a certain extent, promotes the mutual collaboration between countries and institutions (34).
TTH is a multidisciplinary development research field. Previous studies identified that TTH is at a relatively high risk of developing ischemic stroke (35), health nursing delivering treatments efficiently to patients, and will substantially reduce the ill-health burden of headache (36); similarly, emotional factors are potential causes of unfavorable prognosis and outcomes from the preventive treatment in headache (37). Population-based studies have manifested that anxiety and depression are more common in patients with TTH (38, 39), which lead to an increase in headache frequency and play a relevant role in the association between pain interference and burden (40). Therefore, psychological therapies can reduce emotional burden and relieve headache symptoms in patients. This explains the critical role of nursing and developmental psychology in the TTH field. In addition, the prevalence of TTH among children and adolescents ranges from 10 to 25% (41), resulting in impaired daily activities and absence from school (42). Understanding the mechanism of headache and finding specific drugs for treatment may help reduce the incidence of pain and the occurrence of concomitant diseases in children and adolescents. Besides, stress-related headaches usually lead to inefficient work during attacks (43), thus a leisurely work environment probably contributes to the alleviation. Although the number of publications is much lower than the top categories, public environmental/occupational health and pediatrics have also attracted widespread attention in TTH.
Cephalalgia ranks first with most literature and is the most influential journal in the area, with the most citation reviews of migraine pathophysiology. Considering that the pathogenesis of TTH remains unclear, most researchers tend to endorse peripheral and central sensitization, which is independent of headache types, demonstrating the clinical similarity of various forms of chronic headache (44). In other words, the mechanism of migraine may have certain reference in TTH, which is perhaps the main reason that such studies are most cited in the TTH area.
Hotspots and frontiers
In view of the current research situation of the TTH field, the following suggestions are provided for future research hotspots based on reference and keyword analysis.
About the potential population. Although the prevalence of TTH assorted between countries and regions due to differences in study methods and demographic characteristics (45), the peak arose in adults aged 35–39 years, and the percentage of disability-adjusted life-years was high in children and adolescents (32). Headache has been a common grievance in childhood, and younger children seem to be more sensitive to pain stimulation (46). In spite of the symptoms of TTH being not different from those in adults, the duration of attack can be shorter and more variable (47). Headache in children and adolescents should be the priority of future research; in addition to the tremendous impact on daily life and learning, sufficient attention should be paid to whether severe and frequent headaches over a long period of time can lead to mental impairment in children or even to various diseases caused by pain sensitivity in adulthood.
About the induction factors. The role of psychological factors associated with TTH has long been the focus of headache investigation (48). The high depression or anxiety score at baseline was strongly associated with a substantially increased risk of headache (49). Besides, individuals with TTH often complain of sleep disturbances. Previous studies have demonstrated that insomnia, insufficient sleep, and poor sleep quality can result in TTH, with an increased risk of chronic form (50). The association between headaches and emotions or sleep may be bidirectional, but the potential effects are unclear, and whether targeted preventive measures have definite benefits for both psychological and sleep factors need to be further explored.
About the concomitant diseases. The characteristics of temporomandibular disorders are often accompanied by symptoms that are not directly related to the functioning of joints, such as TTH (51). The positive intersections had been reported in previous studies, namely, resulting in higher headache frequency and the Headache Impact Test (HIT-6) scores, and the occurrence of chronic headache (52). Fibromyalgia is a chronic pain syndrome of unknown etiology that appears to be prevalent in patients with TTH (53). When a headache occurs, its severity is associated with increased fibromyalgia symptoms, including frequent headaches, anxiety, pericranial tenderness, physical performance, and sleep disturbances (54, 55). Central sensitization is an important part of the abnormal endogenous pain regulation and somatic hypersensitivity, which is highly similar to the underlying pathogenesis of headache, indicating that TTH is the main cause of comorbidities. However, somatic pain such as back and neck pain in some individuals may be strongly associated with a lower pericranial pressure pain threshold, leading to a view that central sensitization may be a consequence of comorbidity rather than a cause (56). Clarifying the relationship between TTH and comorbidities may help understand the pathogenesis. The collaboration of a multidisciplinary clinical team may have significant benefits for the treatment of TTH, which should be the focus of future research.
About the non-pharmacological therapies. Non-drug treatments for TTH are widely used as a supplement or substitute to medical treatment. Manual therapy is a physical treatment used by practitioners to treat musculoskeletal pain and disability (57). Previous analysis manifested that despite the low certainty of evidence, manual therapy has potential positive effects on headache frequency and quality of life (58). Besides, acupuncture, which originated in China, is a therapy that involves inserting thin needles into the skin at specific points; it is used in many countries to treat headaches. Given its low side effects and high patient acceptance, acupuncture demonstrated significant improvement in pain measures, disability index, quality of life, and psychological status (59, 60). The Cochrane Database of Systematic Reviews acknowledged the potential of acupuncture as a valuable therapy for frequent episodic or chronic TTH (61). In addition, cognitive behavioral therapy is an effective strategy for reducing headache episodes over time (62). Previous studies have demonstrated that cognitive behavioral therapy is associated with a better reduction in pain intensity, mood, headache-related disability, and quality of life (63), forming a valid option for the prevention of headaches at a young age (41, 64). Nevertheless, because of the inevitable unblinded method and detection bias in experimental process, the intervention effect on headache might be overestimated. Therefore, large and high-quality studies are needed to clarify the efficacy.
About the pharmacological therapies. The dominant opinion on the underlying mechanism of botulinum toxin is to inhibit the release of peripheral neurotransmitters or inflammatory mediators, with a secondary effect on the central sensitization, preventing the progression to chronic TTH (65). Several studies have identified that chronic TTH could benefit from the use of botulinum toxin-based on careful patient selection, specific injection patterns, and clear treatment targets (66). Although there are studies indicated that compared with placebo, botulinum toxin was not associated with chronic TTH (67). Such contradictory findings are probably related to their exclusion criteria, and further studies are warranted to determine the efficacy. In the preventive treatment of TTH, the tricyclic antidepressant amitriptyline is the only drug that has proven to be effective, leading to rapid reduction in headache activity, use of analgesic medications, and headache-related disability (68). However, multiple side effects caused by amitriptyline such as dry mouth, drowsiness, dizziness, obstipation, and weight gain may hamper the treatment effectiveness (69). Acetylsalicylic acid (aspirin) is among the most commonly used drugs for the management of pain symptomatologies (70). In frequent episodic TTH, aspirin provided some effects in adults with acute headaches of moderate or severe intensity. Nevertheless, owing to the limited quantity and quality of evidence, such benefit should be interpreted with caution in clinical practice (71). Therefore, the treatment of TTH is still the focus and difficulty of clinical research, and there is an urgent need to develop specific pharmacological management with higher efficacy and fewer side effects.
About the possible pathogenesis. The pathogenesis of TTH mainly focuses on peripheral and central sensitization, but the specific mode of action remains unclear. CGRP is considered as a pain-signaling neuropeptide and a potent vasodilator (72). Previous studies have indicated that the plasma levels of CGRP are normal in patients with chronic TTH and are not associated with the headache status (73). However, considering the pathophysiological importance of CGRP, whether TTH can be treated with monoclonal antibodies targeting CGRP or its receptor-like migraine requires various studies to elucidate this issue, and further research is needed to explore the differences between migraine and TTH.
Limitations
Although CiteSpace and VOSviewer have become important mapping tools in the medical field, bibliometric analysis cannot replace system retrieval because of methodological limitations. First, the publications retrieved only included articles and reviews in the Web of Science database, ignoring contributions from other forms of publications. The limitation of the retrieval strategy may lead to the uncertainty of research conclusions. Second, bibliometric analyses generally focus on the influence of a publication rather than on the quality; the inclusion of low-quality articles may affect analysis results. Finally, a unified standard is still lacking in bibliometric analysis; different types of publications may have more appropriate research methods. Disease research should consider complicated factors, which cannot be quantified in simple diagrams and need to be discussed in future research.
Conclusion
Despite the lack of attention and breakthroughs in the past decades, TTH has vital research value and broad development prospects and urgently needs cooperation and exchanges between countries and institutions. Relevant studies about headaches in children and adolescents, inducing factors such as emotional and sleep, concomitant diseases, and clinical management related to central sensitization, are in the spotlight in recent years, which are also the hotspot of future research.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
XF conceived and designed this study, retrieved the articles, collected the data, and drafted the manuscript. XF, GF, and LW analyzed the data and drew the maps. WS and YZ directed the research. All authors contributed to the article and approved the final manuscript.
Funding
This research was supported by the Capital Health Research and Development of Special (No. 2020-2-4173), Scientific and Technological Innovation Project of China Academy of Chinese Medical Sciences (No. CI2021B006), Innovation Team and Talents Cultivation Program of National Administration of Traditional Chinese Medicine (No. ZYYCXTD-C-202007), and the National TCM Leading Personnel Support Program [NATCM Personnel and Education Department (2018)] (No. 12).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Vos T, Lim SS, Abbafati C, Abbas KM, Abbasi M, Abbasifard M, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the global burden of disease study 2019. Lancet. (2020) 396:1204–22. doi: 10.1016/S0140-6736(20)30925-9
2. Stovner L, Hagen K, Jensen R, Katsarava Z, Lipton R, Scher A, et al. The global burden of headache: a documentation of headache prevalence and disability worldwide. Cephalalgia. (2007) 27:193–210. doi: 10.1111/j.1468-2982.2007.01288.x
3. Jha RP. Global, regional, and national burden of neurological disorders, 1990-2016: a systematic analysis for the global burden of disease study 2016. Lancet Neurol. (2019) 18:459–80.
4. Robbins MS. Diagnosis and management of headache: a review. JAMA. (2021) 325:1874–85. doi: 10.1001/jama.2021.1640
5. Ashina S, Mitsikostas DD, Lee MJ, Yamani N, Wang SJ, Messina R, et al. Tension-type headache. Nat Rev Dis Primers. (2021) 7:24. doi: 10.1038/s41572-021-00257-2
6. Steiner TJ, Jensen R, Katsarava Z, Linde M, MacGregor EA, Osipova V, et al. Aids to management of headache disorders in primary care (2nd edition): on behalf of the european headache federation and lifting the burden: the global campaign against headache. J Headache Pain. (2019) 20:57. doi: 10.1186/s10194-018-0899-2
7. Jensen RH. Tension-type headache - the normal and most prevalent headache. Headache. (2018) 58:339–45. doi: 10.1111/head.13067
8. Arnold M. Headache classification committee of the international headache society (IHS) the international classification of headache disorders, 3rd edition. Cephalalgia. (2018) 38:1–211. doi: 10.1177/0333102417738202
9. Lyngberg AC, Rasmussen BK, Jørgensen T, Jensen R. Incidence of primary headache: a danish epidemiologic follow-up study. Am J Epidemiol. (2005) 161:1066–73. doi: 10.1093/aje/kwi139
10. Monzani L, Espí-López GV, Zurriaga R, Andersen LL. Manual therapy for tension-type headache related to quality of work life and work presenteeism: secondary analysis of a randomized controlled trial. Complement Ther Med. (2016) 25:86–91. doi: 10.1016/j.ctim.2016.01.008
11. Bendtsen L, Evers S, Linde M, Mitsikostas DD, Sandrini G, Schoenen J. Efns guideline on the treatment of tension-type headache - report of an efns task force. Eur J Neurol. (2010) 17:1318–25. doi: 10.1111/j.1468-1331.2010.03070.x
12. Steiner TJ, Stovner LJ, Katsarava Z, Lainez JM, Lampl C, Lantéri-Minet M, et al. The impact of headache in Europe: principal results of the Eurolight project. J Headache Pain. (2014) 15:31. doi: 10.1186/1129-2377-15-31
13. Steel SJ, Robertson CE, Whealy MA. Current understanding of the pathophysiology and approach to tension-type headache. Curr Neurol Neurosci Rep. (2021) 21:56. doi: 10.1007/s11910-021-01138-7
14. Guler AT, Waaijer CJ, Palmblad M. Scientific workflows for bibliometrics. Scientometrics. (2016) 107:385–98. doi: 10.1007/s11192-016-1885-6
15. Wilson M, Sampson M, Barrowman N, Doja A. Bibliometric analysis of neurology articles published in general medicine journals. JAMA Netw Open. (2021) 4:e215840. doi: 10.1001/jamanetworkopen.2021.5840
16. Brandt JS, Hadaya O, Schuster M, Rosen T, Sauer MV, Ananth CV, et al. Bibliometric analysis of top-cited journal articles in obstetrics and gynecology. JAMA Netw Open. (2019) 2:e1918007. doi: 10.1001/jamanetworkopen.2019.18007
17. Ramos MB, Teixeira MJ, Preul MC, Spetzler RF, Figueiredo EG A A bibliometric study of the most cited reports in central nervous system arteriovenous malformations. World Neurosurg. (2019) 129:261–8. doi: 10.1016/j.wneu.2019.06.048
18. Chen C, Hu Z, Liu S, Tseng H. Emerging trends in regenerative medicine: a scientometric analysis in citeSpace. Expert Opin Biol Ther. (2012) 12:593–608. doi: 10.1517/14712598.2012.674507
19. Liu S, Sun YP, Gao XL, Sui Y. Knowledge domain and emerging trends in Alzheimer's disease: a scientometric review based on citespace analysis. Neural Regen Res. (2019) 14:1643–50. doi: 10.4103/1673-5374.255995
20. Chen C. Searching for intellectual turning points: progressive knowledge domain visualization. Proc Natl Acad Sci U S A. (2004) 101:5303–10. doi: 10.1073/pnas.0307513100
21. van Eck NJ, Waltman L. Software survey: VOSviewer, a computer program for bibliometric mapping. Scientometrics. (2010) 84:523–38. doi: 10.1007/s11192-009-0146-3
22. Mojgani P, Jalali M, Keramatfar A. Bibliometric study of traumatic brain injury rehabilitation. Neuropsychol Rehabil. (2022) 32:51–68. doi: 10.1080/09602011.2020.1796714
23. Synnestvedt MB, Chen C, Holmes JH. CiteSpace II: visualization and knowledge discovery in bibliographic databases. AMIA Annu Symp Proc. (2005) 2005:724–8.
24. Hirsch JE. Does the H-index have predictive power? Proc Natl Acad Sci U S A. (2007) 104:19193–8. doi: 10.1073/pnas.0707962104
25. Bornmann L, de Moya Anegón F, Leydesdorff L. The new excellence indicator in the world report of the SCImago institutions rankings 2011. J Informetr. (2012) 6:333–5. doi: 10.1016/j.joi.2011.11.006
26. Rosvall M, Bergstrom CT. Mapping change in large networks. PLoS ONE. (2010) 5:e8694. doi: 10.1371/journal.pone.0008694
27. Falagas ME, Kouranos VD, Arencibia-Jorge R, Karageorgopoulos DE. Comparison of SCImago journal rank indicator with journal impact factor. FASEB J. (2008) 22:2623–8. doi: 10.1096/fj.08-107938
28. Silberstein SD. Migraine pathophysiology and its clinical implications. Cephalalgia. (2004) 24:2–7. doi: 10.1111/j.1468-2982.2004.00892.x
29. Fumal A, Schoenen J. Tension-type headache: current research and clinical management. Lancet Neurol. (2008) 7:70–83. doi: 10.1016/S1474-4422(07)70325-3
30. Mateen FJ, Dua T, Steiner T, Saxena S. Headache disorders in developing countries: research over the past decade. Cephalalgia. (2008) 28:1107–14. doi: 10.1111/j.1468-2982.2008.01681.x
31. Martelletti P, Haimanot RT, Láinez MJ, Rapoport AM, Ravishankar K, Sakai F, et al. The global campaign (GC) to reduce the burden of headache worldwide. The international team for specialist education (ITSE). J Headache Pain. (2005) 6:261–3. doi: 10.1007/s10194-005-0202-1
32. Stovner LJ, Nichols E, Steiner TJ, Abd-Allah F, Abdelalim A, Al-Raddadi RM. Global, regional, and national burden of migraine and tension-type headache, 1990-2016: a systematic analysis for the global burden of disease study 2016. Lancet Neurol. (2018) 17:954–76. doi: 10.1016/S1474-4422(18)30322-3
33. Steiner TJ. Lifting the burden: the global campaign against headache. Lancet Neurol. (2004) 3:204–5. doi: 10.1016/S1474-4422(04)00703-3
34. Stovner LJ, Al JM, Birbeck GL, Gururaj G, Jensen R, Katsarava Z, et al. The methodology of population surveys of headache prevalence, burden and cost: principles and recommendations from the global campaign against headache. J Headache Pain. (2014) 15:5. doi: 10.1186/1129-2377-15-5
35. Tsai CL, Chou CH, Lee PJ, Yin JH, Chen SY, Lin CC, et al. The potential impact of primary headache disorders on stroke risk. J Headache Pain. (2016) 17:108. doi: 10.1186/s10194-016-0701-2
36. Steiner TJ, Jensen R, Katsarava Z, Stovner LJ, Uluduz D, Adarmouch L, et al. Structured q1 headache services as the solution to the ill-health burden of headache: 1. Rationale and description. J Headache Pain. (2021) 22:78. doi: 10.1186/s10194-021-01265-z
37. Probyn K, Bowers H, Caldwell F, Mistry D, Underwood M, Matharu M, et al. Prognostic factors for chronic headache: a systematic review. Neurology. (2017) 89:291–301. doi: 10.1212/WNL.0000000000004112
38. Song TJ, Cho SJ, Kim WJ, Yang KI, Yun CH, Chu MK. Anxiety and depression in tension-type headache: a population-based study. PLoS ONE. (2016) 11:e165316. doi: 10.1371/journal.pone.0165316
39. Ashina S, Bendtsen L, Buse DC, Lyngberg AC, Lipton RB, Jensen R. Neuroticism, depression and pain perception in migraine and tension-type headache. Acta Neurol Scand. (2017) 136:470–6. doi: 10.1111/ane.12751
40. Fuensalida-Novo S, Palacios-Ceña M, Fernández-Muñoz JJ, Castaldo M, Wang K, Catena A, et al. The burden of headache is associated to pain interference, depression and headache duration in chronic tension type headache: a 1-year longitudinal study. J Headache Pain. (2017) 18:119. doi: 10.1186/s10194-017-0829-8
41. Anttila P. Tension-type headache in childhood and adolescence. Lancet Neurol. (2006) 5:268–74. doi: 10.1016/S1474-4422(06)70376-3
42. Albers L, Straube A, Landgraf MN, Filippopulos F, Heinen F, von Kries R. Migraine and tension type headache in adolescents at grammar school in Germany - burden of disease and health care utilization. J Headache Pain. (2015) 16:534. doi: 10.1186/s10194-015-0534-4
43. Lin KC, Huang CC, Wu CC. Association between stress at work and primary headache among nursing staff in Taiwan. Headache. (2007) 47:576–84. doi: 10.1111/j.1526-4610.2007.00759.x
44. Filatova E, Latysheva N, Kurenkov A. Evidence of persistent central sensitization in chronic headaches: a multi-method study. J Headache Pain. (2008) 9:295–300. doi: 10.1007/s10194-008-0061-7
45. Deuschl G, Beghi E, Fazekas F, Varga T, Christoforidi KA, Sipido E, et al. The burden of neurological diseases in Europe: an analysis for the global burden of disease study 2017. Lancet Public Health. (2020) 5:e551–67. doi: 10.1016/S2468-2667(20)30190-0
46. Lautenbacher S, Peters JH, Heesen M, Scheel J, Kunz M. Age changes in pain perception: a systematic-review and meta-analysis of age effects on pain and tolerance thresholds. Neurosci Biobehav Rev. (2017) 75:104–13. doi: 10.1016/j.neubiorev.2017.01.039
47. Straube A, Andreou A. Primary headaches during lifespan. J Headache Pain. (2019) 20:35. doi: 10.1186/s10194-019-0985-0
48. Torelli P, Abrignani G, Castellini P, Lambru G, Manzoni GC. Human psyche and headache: tension-type headache. Neurol Sci. (2008) 29 (Suppl 1):S93–5. doi: 10.1007/s10072-008-0896-3
49. Hagen K, Stovner LJ, Zwart JA. Time trends of major headache diagnoses and predictive factors. Data from three nord-trøndelag health surveys. J Headache Pain. (2020) 21:24. doi: 10.1186/s10194-020-01095-5
50. Cho SJ, Song TJ, Chu MK. Sleep and tension-type headache. Curr Neurol Neurosci Rep. (2019) 19:44. doi: 10.1007/s11910-019-0953-8
51. Pihut M, Ferendiuk E, Szewczyk M, Kasprzyk K, Wieckiewicz M. The efficiency of botulinum toxin type a for the treatment of masseter muscle pain in patients with temporomandibular joint dysfunction and tension-type headache. J Headache Pain. (2016) 17:29. doi: 10.1186/s10194-016-0621-1
52. Tchivileva IE, Ohrbach R, Fillingim RB, Lin FC, Lim PF, Arbes SJ, et al. Clinical, psychological, and sensory characteristics associated with headache attributed to temporomandibular disorder in people with chronic myogenous temporomandibular disorder and primary headaches. J Headache Pain. (2021) 22:42. doi: 10.1186/s10194-021-01255-1
53. Kleykamp BA, Ferguson MC, McNicol E, Bixho I, Arnold LM, Edwards RR, et al. The prevalence of psychiatric and chronic pain comorbidities in fibromyalgia: an acttion systematic review. Semin Arthritis Rheum. (2021) 51:166–74. doi: 10.1016/j.semarthrit.2020.10.006
54. de Tommaso M, Federici A, Serpino C, Vecchio E, Franco G, Sardaro M, et al. Clinical features of headache patients with fibromyalgia comorbidity. J Headache Pain. (2011) 12:629–38. doi: 10.1007/s10194-011-0377-6
55. de Tommaso M, Sardaro M, Serpino C, Costantini F, Vecchio E, Prudenzano MP, et al. Fibromyalgia comorbidity in primary headaches. Cephalalgia. (2009) 29:453–64. doi: 10.1111/j.1468-2982.2008.01754.x
56. Ashina S, Lipton RB, Bendtsen L, Hajiyeva N, Buse DC, Lyngberg AC, et al. Increased pain sensitivity in migraine and tension-type headache coexistent with low back pain: a cross-sectional population study. Eur J Pain. (2018) 22:904–14. doi: 10.1002/ejp.1176
57. Chaibi A, Russell MB. Manual therapies for primary chronic headaches: a systematic review of randomized controlled trials. J Headache Pain. (2014) 15:67. doi: 10.1186/1129-2377-15-67
58. Krøll LS, Callesen HE, Carlsen LN, Birkefoss K, Beier D, Christensen HW, et al. Manual joint mobilization techniques, supervised physical activity, psychological treatment, acupuncture and patient education for patients with tension-type headache. A systematic review and meta-analysis. J Headache Pain. (2021) 22:96. doi: 10.1186/s10194-021-01298-4
59. Georgoudis G, Felah B, Nikolaidis PT, Papandreou M, Mitsiokappa E, Mavrogenis AF, et al. The effect of physiotherapy and acupuncture on psychocognitive, somatic, quality of life, and disability characteristics in the patients. J Pain Res. (2018) 11:2527–35. doi: 10.2147/JPR.S178110
60. Schiller J, Karst M, Kellner T, Zheng W, Niederer D, Vogt L, et al. Combination of acupuncture and medical training therapy on tension type headache: results of a randomized controlled pilot study. Cephalalgia. (2021) 41:879–93. doi: 10.1177/0333102421989620
61. Linde K, Allais G, Brinkhaus B, Fei Y, Mehring M, Shin BC, et al. Acupuncture for the prevention of tension-type headache. Cochrane Database Syst Rev. (2016) 4:D7587. doi: 10.1002/14651858.CD007587.pub2
62. Klausen SH, Rønde G, Tornøe B, Bjerregaard L. Non-pharmacological interventions addressing pain, sleep, and quality of life in children and adolescents with primary headache: a systematic review. J Pain Res. (2019) 12:3437–59. doi: 10.2147/JPR.S216807
63. Probyn K, Bowers H, Mistry D, Caldwell F, Underwood M, Patel S, et al. Non-pharmacological self-management for people living with migraine or tension-type headache: a systematic review including analysis of intervention components. BMJ Open. (2017) 7:e16670. doi: 10.1136/bmjopen-2017-016670
64. Andrasik F, Grazzi L, Sansone E, D'Amico D, Raggi A, Grignani E. Non-pharmacological approaches for headaches in young age: an updated review. Front Neurol. (2018) 9:1009. doi: 10.3389/fneur.2018.01009
65. Matak I, Lacković Z. Botulinum toxin A, brain and pain. Prog Neurobiol. (2014) 119-120:39–59. doi: 10.1016/j.pneurobio.2014.06.001
66. Freund B, Rao A. Efficacy of botulinum toxin in tension-type headaches: a systematic review of the literature. Pain Pract. (2019) 19:541–51. doi: 10.1111/papr.12773
67. Jackson JL, Kuriyama A, Hayashino Y. Botulinum toxin a for prophylactic treatment of migraine and tension headaches in adults: a meta-analysis. JAMA. (2012) 307:1736–45. doi: 10.1001/jama.2012.505
68. Holroyd KA, O'Donnell FJ, Stensland M, Lipchik GL, Cordingley GE, Carlson BW. Management of chronic tension-type headache with tricyclic antidepressant medication, stress management therapy, and their combination: a randomized controlled trial. JAMA. (2001) 285:2208–15. doi: 10.1001/jama.285.17.2208
69. Bendtsen L. Drug and nondrug treatment in tension-type headache. Ther Adv Neurol Disord. (2009) 2:155–61. doi: 10.1177/1756285609102328
70. Farinelli I, Martelletti P. Aspirin and tension-type headache. J Headache Pain. (2007) 8:49–55. doi: 10.1007/s10194-006-0357-4
71. Derry S, Wiffen PJ, Moore RA. Aspirin for acute treatment of episodic tension-type headache in adults. Cochrane Database Syst Rev. (2017) 1:D11888. doi: 10.1002/14651858.CD011888.pub2
72. Schuster NM, Rapoport AM. New strategies for the treatment and prevention of primary headache disorders. Nat Rev Neurol. (2016) 12:635–50. doi: 10.1038/nrneurol.2016.143
Keywords: bibliometric analysis, CiteSpace, network, tension-type headache, VOSviewer
Citation: Fan X, Fu G, Wang L, Shen W and Zhang Y (2022) A bibliometric analysis and visualization of tension-type headache. Front. Neurol. 13:980096. doi: 10.3389/fneur.2022.980096
Received: 28 June 2022; Accepted: 08 August 2022;
Published: 31 August 2022.
Edited by:
Chirstian Wöber, Medical University of Vienna, AustriaReviewed by:
Federica Galli, Sapienza University of Rome, ItalyMin Kyung Chu, Yonsei University Health System, South Korea
Copyright © 2022 Fan, Fu, Wang, Shen and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wei Shen, Njc2NjY1NzA5QHFxLmNvbQ==; Yunling Zhang, eXVubGluZ3poYW5nMjAwNEAxNjMuY29t