 Tian Sang
Tian Sang Ying Wang
Ying Wang Ye Wu
Ye Wu Qiao Guan
Qiao Guan ZhiXian Yang
ZhiXian Yang
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurol. , 23 November 2022
Sec. Pediatric Neurology
Volume 13 - 2022 | https://doi.org/10.3389/fneur.2022.957465
Objectives: To investigate neonatal electroencephalography (EEG) background activity and electrographic seizures in patients in the pediatric intensive care unit (PICU) who underwent bedside video-electroencephalography (vEEG) monitoring.
Methods: A total of 232 pediatric patients admitted or transferred to PICU that underwent vEEG monitoring were retrospectively enrolled in this study, and electrographic status epilepticus was observed after vEEG monitoring.
Results: The median age was 1.56 years [95% confidence interval (CI) = 1.12–2.44]. Electrographic seizures occurred in 88 patients (37.9%), out of which 36 cases (40.9%) had electrographic status epilepticus. Prior epileptic encephalopathy diagnosis [odds ratio (OR) = 6.57, 95% CI = 1.91–22.59, p = 0.003], interictal epileptiform discharges (OR = 46.82, 95%CI = 5.31–412.86, p = 0.0005), slow disorganized EEG background (OR = 11.92, 95%CI = 1.31–108.71, p = 0.028), and burst-suppression EEG background (OR = 23.64, 95%CI = 1.71–327.57, p = 0.018) were the risk factors for electrographic seizures' occurrence. Of the 232 patients, the condition of 179 (77.2%) patients improved and they were discharged, 34 cases (14.7%) were withdrawn, and 18 cases (7.8%) died. The in-hospital death rate was 47.6% (10 in 21 cases) in patients with attenuated/featureless, compared to 0/23 with normal EEG background.
Conclusions: Electrographic status epilepticus occurs in more than one-third of patients with electrographic seizures. vEEG is an efficient method to determine electrographic seizures in children. Abnormal EEG background activity is associated with both electrographic seizures' occurrence and unfavorable in-hospital outcomes.
In critically ill patients, epileptic seizures, with the majority being non-convulsive seizures (NCS), may be difficult to detect due to the subtle or the absence of clinical signs (1–5). They can be caused by unhealed status epilepticus (subclinical seizures), acute neurologic impairment (encephalitis, trauma, stroke, and anoxia), and systemic disorders (metabolic disorders, cardiorespiratory disease, poisoning, and sepsis).
Video-electroencephalography (vEEG) monitoring is increasingly being utilized in the identification of epileptic seizures in clinical practice, especially in patients with impaired consciousness (6–9). Electrographic seizures (seizure on EEG) have an estimated occurrence of 20–40% among children who underwent vEEG monitoring in pediatric intensive care unit (PICU) (2, 3, 7, 8, 10). Kirkham et al. (11) reported that either clinical or subclinical seizures are associated with poor survival outcomes in patients in PICU. Meanwhile, studies indicated that the occurrence of status epilepticus in PICU is associated with higher in-hospital mortality (7, 8, 12). EEG has been reported to affect clinical management in about 59% of monitored children, most often by affecting anticonvulsant utilization (13). All these findings inform us that vEEG monitoring in PICU plays an important role in both detecting subclinical seizures and guiding the treatment with anticonvulsants in critically ill patients.
The aim of the present study was to describe current pediatric critical care vEEG utilization using a single-center retrospective study of consecutive patients. According to the continuous vEEG monitoring in PICU, we retrospectively investigated the prevalence of seizures, determined the risk factors for seizures, and further analyzed the association between seizures and clinical outcomes.
From July 2013 to June 2018, this retrospective study was conducted on all consecutive patients who underwent vEEG monitoring in PICU of Peking University First Hospital, China. This study was approved by the Ethics Committee of the Peking University First Hospital, China (No. 2021KY422). If the patient received multiple vEEG monitorings, the vEEG recording with the poorest performance was registered. Patients with a vEEG monitoring of < 4 h were excluded. Premature infants with a gestational age < 44 weeks and term infants < 28 days after birth were excluded.
Demographic and clinical information was gathered from the patients, including age, gender, hospitalized time in PICU, prior diagnosis of epileptic encephalopathy, prior diagnosis of epilepsy, clinical seizures prior to vEEG monitoring, mental status before vEEG monitoring, prior developmental delay or intellectual disability, and acute or systemic disorders. Acute or systemic disorders include neurologic disorder, central nervous system (CNS) infection, autoimmune diseases, sepsis, previous hypoxic ischemic encephalopathy (HIE), other structural brain impairments, mitochondrial encephalomyopathy (ME), and inborn errors of metabolism (IEM).
Bedside vEEG monitoring was performed on each patient using a Nihon Kohden digital video-EEG 1200C instrument (Nihon Kohden, Japan), which consists of an EEG-1200c system program, an isolated power supply unit, an electric J input box, a mini extension junction box, an input converter, a signal switching box, an additional electrical stimulation unit, a light stimulation control unit, a flash lamp, a camera image input unit, a wire assembly, a peripheral capillary oxygen saturation (SpO2) adapter, a reusable pulse oxygen probe, a CO2 sensor, a nose adapter, and digital video software. The sensitivity is 10–1,500 μV/cm. The EEG electrodes were positioned over the scalp according to the International 10–20 System. All individuals also underwent polyelectromyography (PEMG) during the vEEG monitoring. The occurrence and characteristics of seizures, interictal epileptiform discharges, and EEG background were collected from the vEEG recording. Electrographic seizures were recognized according to the description given in a previous literature (14). Electrographic status epilepticus refers to single or recurrent electrographic seizures that last longer than 30 min in any 1 h epoch. Interictal epileptiform discharges refer to sharp/sharp–slow waves, spikes/ spike–slow waves, polyspike slow waves, and paroxysmal fast activity. EEG background activity is categorized as normal/sleep waves, slow/disorganized waves, asymmetric/asynchronous waves, burst-suppression waves, and attenuated/electrical silence waves, and electrographic seizure characteristics are seizure duration, clinical seizure correlate, seizure onset localization, and seizure maximal spread. Moreover, patients received carbamazepine, diazepam, phenytoin sodium, and other drug treatments combined with anti-infection treatment.
In the present study, continuous data were presented as median and 95% confidence intervals (CIs), and categorical data were shown as counts and percentages. The Chi-square (χ2) test and Fisher's exact test were used to analyze the factors associated with electrographic seizures or in-hospital outcomes. The univariate logistic regression model was established to determine the risk factors for electrographic seizures. All parameters that were significant in a univariate logistic regression model were taken into a multivariable logistic regression model in the end. The comparison of age and duration of PICU stay between the electrographic seizure group and the non-electrographic seizure group was performed by using the Mann–Whitney U test. All statistical analyses in the present study were performed using OriginPro Software version 8.5.0 (OriginLab Corporation, Northampton, MA, USA) and MedCalc Statistical Software version 15.2.2 (MedCalc Software bvba, Ostend, Belgium). A value of p < 0.05 was regarded as a statistically significant difference.
A total of 232 children were enrolled in the population, including 128 (55.17%) girls and 104 (44.83%) boys. The median duration of patient stay at the PICU was 7 days (95% CI = 6–9). The median age of the enrolled population was 1.56 ± 0.145 years. The patient age distribution is plotted in Figure 1. There were 195 (84.05%) study individuals who suffered from a neurologic disorder, 27 (11.64%) patients had CNS infection, 14 (6.03%) patients had autoimmune diseases, 28 (12.07%) patients had sepsis, 45 (19.4%) patients had structural brain impairments, 8 (3.45%) patients had previous HIE, 44 (18.97%) patients had IEM or ME, and 71 (30.6%) of patients showed prior developmental delay or intellectual disability. As many as 71.6% (166) of patients received 4 to 8 h of vEEG monitoring, 21.6% (50) of them received 8 to 16 h of vEEG monitoring, and 6.9% (15) patients received longer than 16 h of vEEG monitoring. Of the 232 patients, 26 patients had clinical seizures before being monitored for vEEG (Table 1).
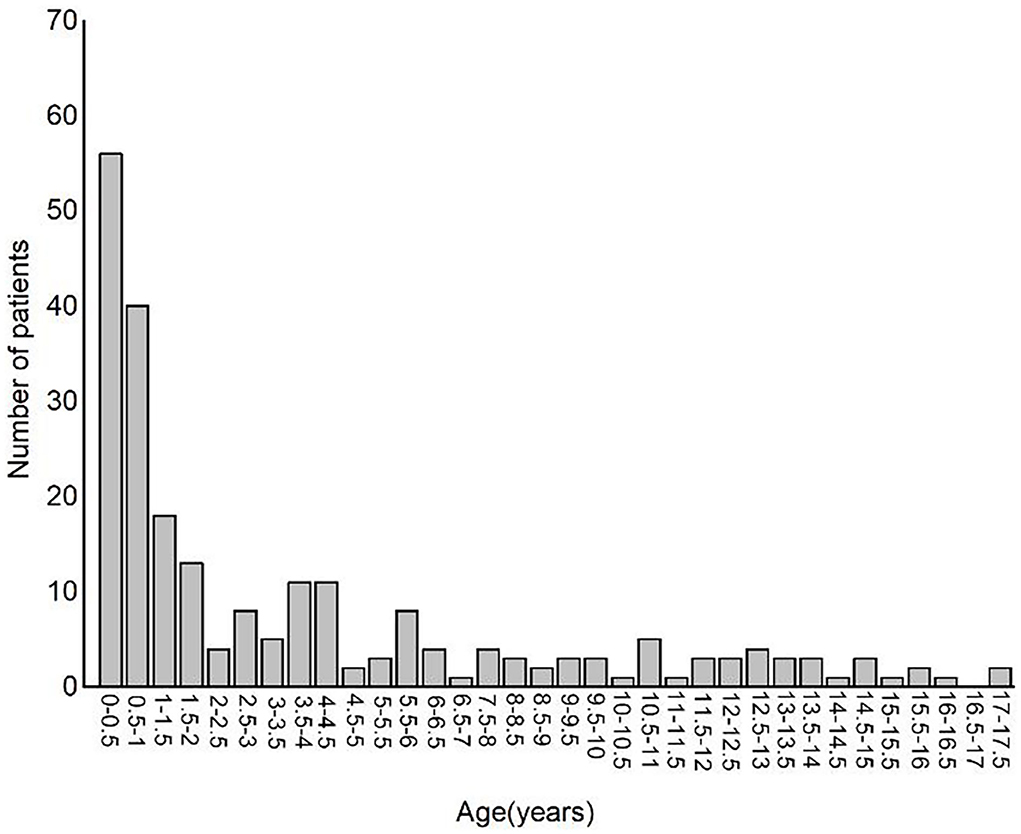
Figure 1. Bar plot showing patient's age distribution.
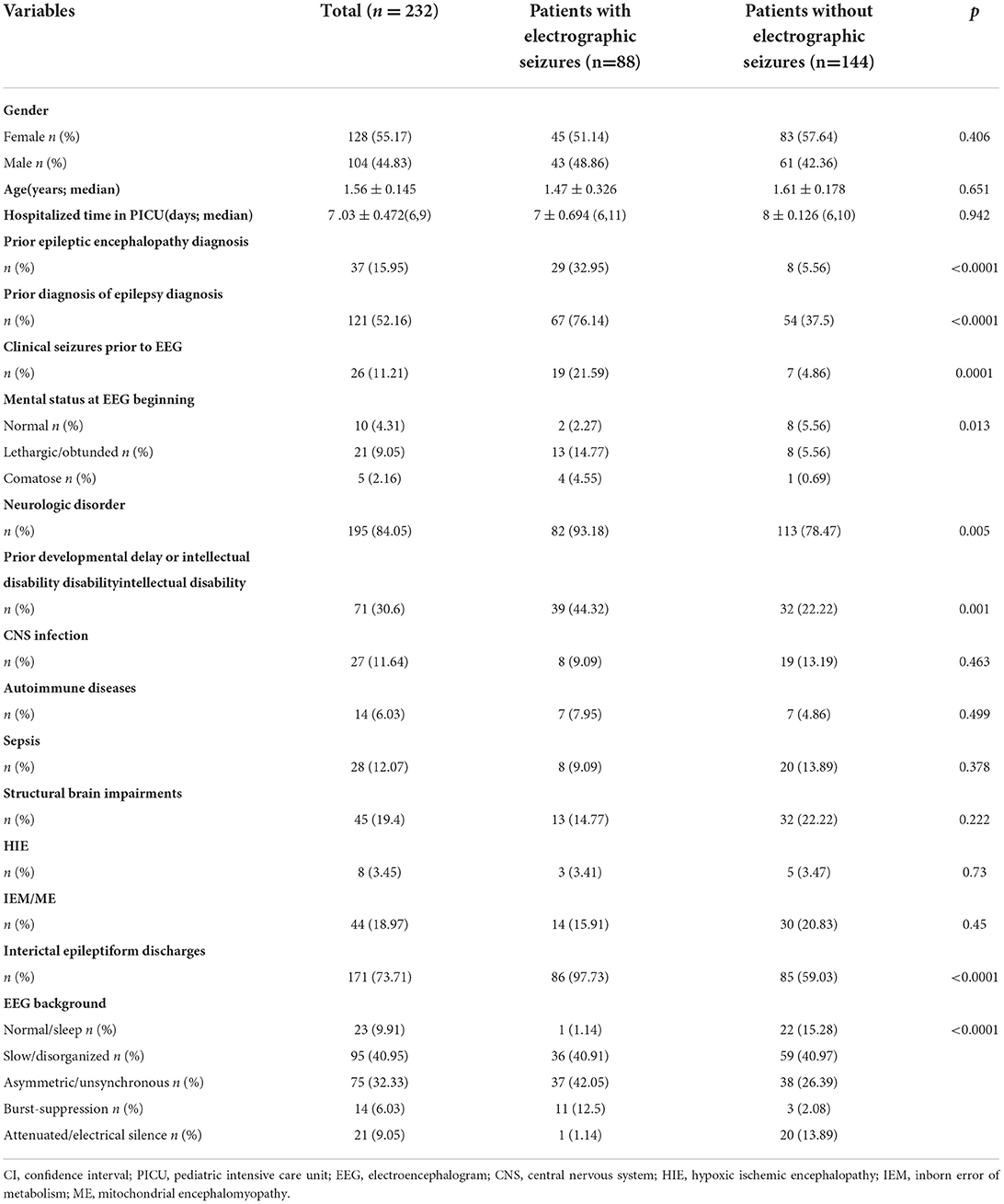
Table 1. General and clinical factors associated with electrographic seizures.
Table 1 shows that the variables used in the chi-square (χ2) test and Fisher's exact test are the significant factors associated with the occurrence of electrographic seizure (p < 0.05): prior epileptic encephalopathy, prior diagnosis of epilepsy, clinical seizures prior to EEG, mental status at EEG onset, neurologic disorder, prior developmental delay or intellectual disability, interictal epileptiform discharges, and EEG background. Clinical parameters that are relevant to electrographic status epilepticus in Table 2 indicated that the primary variables investigated in the study, namely, prior epileptic encephalopathy, prior epilepsy, CNS disorder, and EEG background, were not significantly associated with electrographic status epilepticus (p > 0.05).
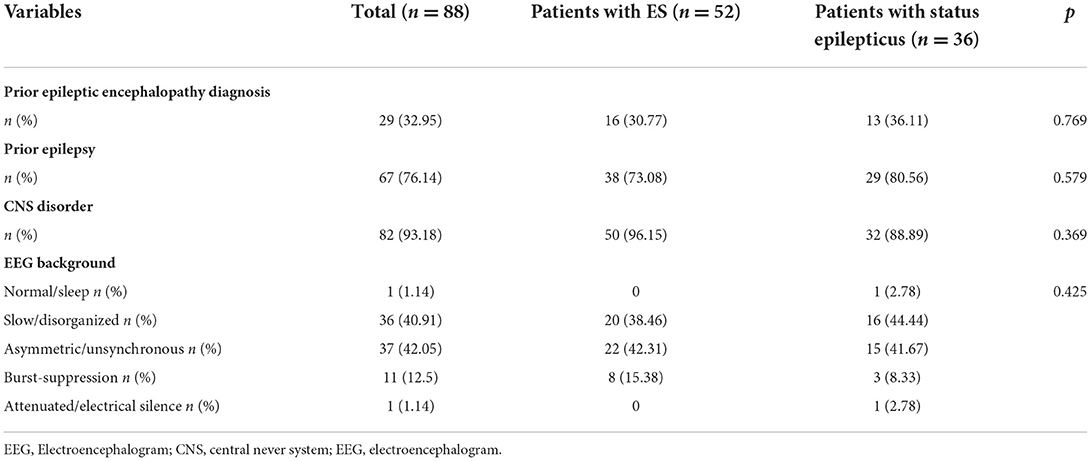
Table 2. Analysis of related factors for status epilepticus in patients with electrographic seizures.
The incidence of electrographic seizure in the population was 37.9% (88 of 232). Therein, 40.9% of (36 of 88) patients with electrographic seizure had electrographic status epilepticus. The characteristics of electrographic seizure are presented in Table 3. In total, 16.13, 27.42, 1.61, and 54.84% of patients were accounted for the seizure duration category of < 1 min, 1 min-5 min, 5–30 min, and >30 min, respectively. In patients with electrographic seizure, 36.36% cases were focal onset, 47.73% cases were multifocal onset, and 15.91% cases were generalized onset. In addition, 61.54% patients with electrographic seizure had bilateral seizure spread localization, 35.9% patients had unilateral seizure spread localization, and 2.56% patients had focal seizure spread localization.
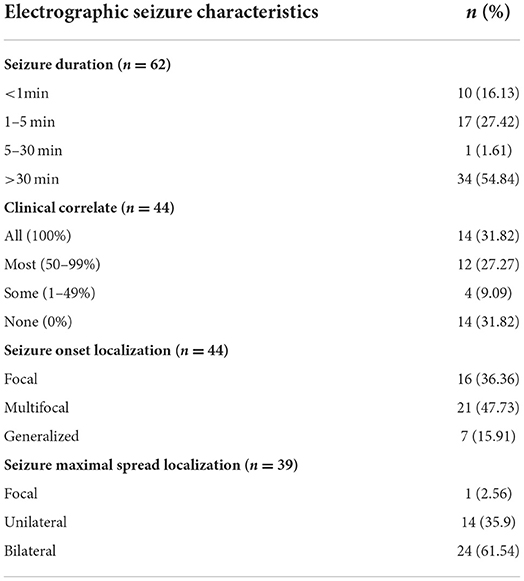
Table 3. Electrographic seizure characteristics of 88 patients.
Furthermore, we explored the risk factors for electrographic seizures in the logistic regression model, as shown in Table 4: prior epileptic encephalopathy (OR = 6.57, 95%CI = 1.91–22.59, p = 0.003), interictal epileptiform discharges (OR = 46.82, 95%CI = 5.31–412.86, p = 0.0005), slow disorganized EEG background (OR = 11.92, 95%CI = 1.31–108.71, p = 0.028), and burst-suppression EEG background (OR = 23.64, 95%CI = 1.71–327.57, p = 0.018).
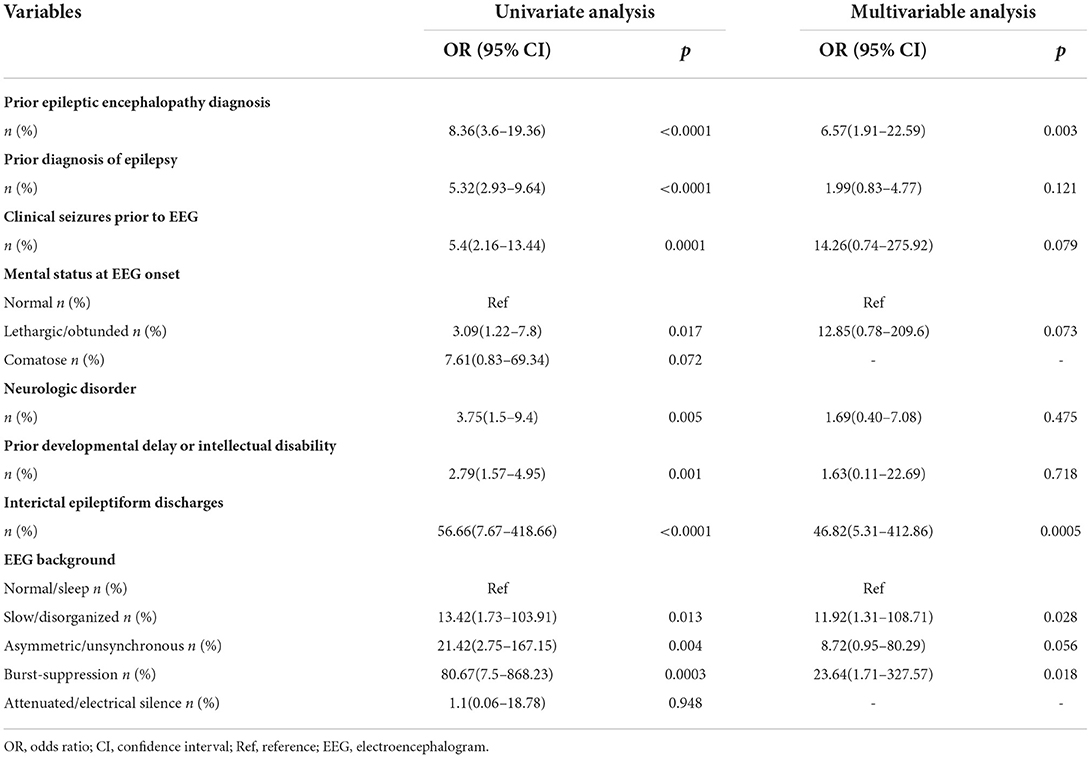
Table 4. Risk factors for electrographic seizures.
In the present study, 77.16% (179 of 232) of patients had improved condition and were discharged from the hospital, 14.66% (34 of 232) of patients had not improved and were voluntarily discharged from the hospital, and 7.76% (18 of 232) of patients died. The associated factors for in-hospital outcomes are presented in Table 5. It was found that clinical variables, such as gender, age, prior epileptic encephalopathy, prior diagnosis of epilepsy, seizure category, neurologic disorder, CNS infection, structural brain impairments, HIE, and interictal epileptiform discharges, were not related to in-hospital outcomes (p > 0.05). Moreover, patients with sepsis and/or abnormal EEG background in PICU were more likely to face an unfavorable in-hospital outcome (p < 0.05).
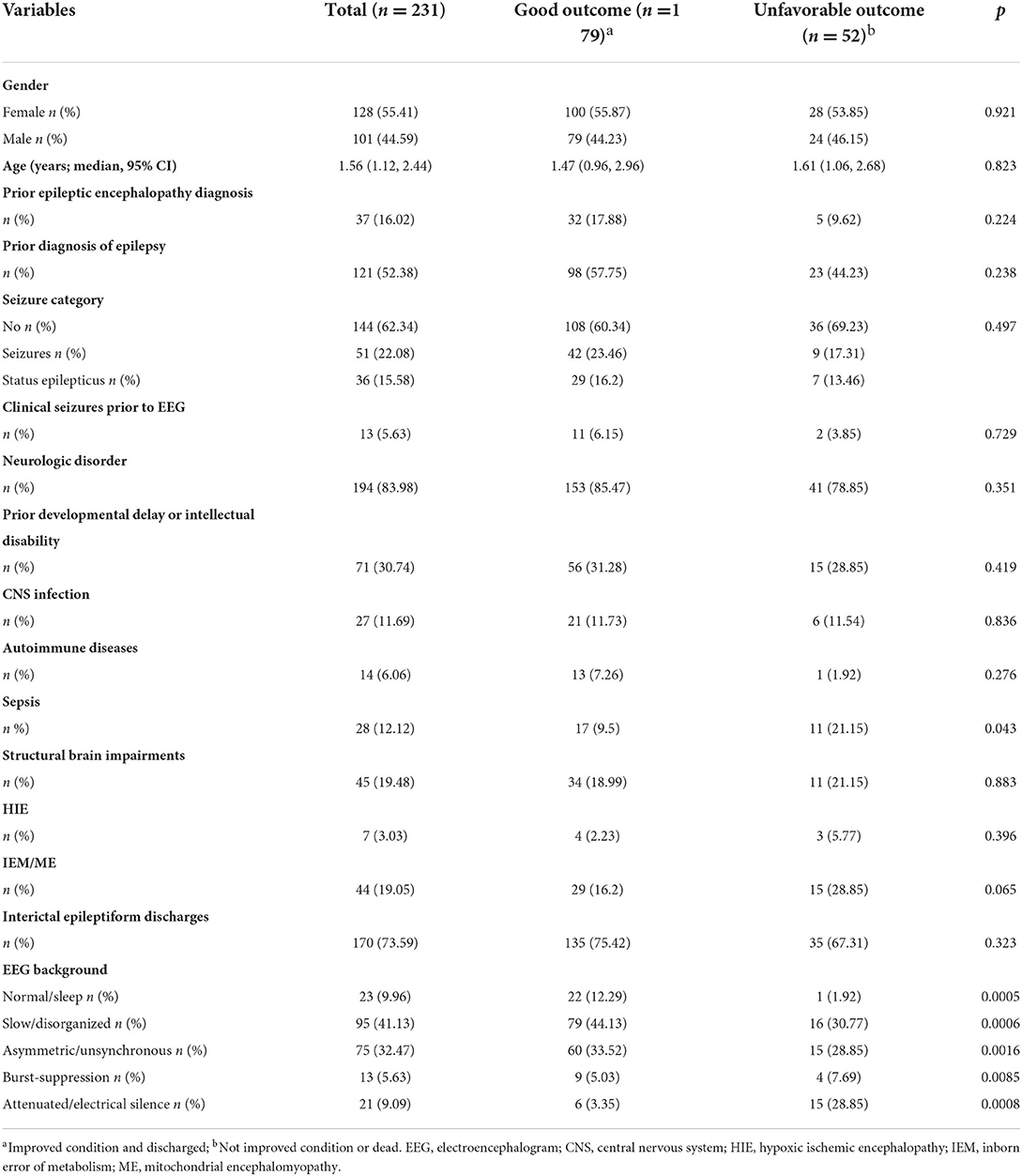
Table 5. Association between clinical variables and in-hospital outcomes.
The present study retrospectively analyzed the occurrence of electrographic seizures and EEG background among 232 children who underwent bedside vEEG monitoring in PICU of a tertiary hospital in China. The results indicate that the incidence of electrographic seizures was 37.9%, of which 40.9% electrographic seizures were status epilepticus. In addition, 88.4% patients had an abnormal initial EEG background.
The categories of admission diagnoses in PICU and the length of ICU stay are quite different from those in an adult or neonatal intensive care unit (ICU). Acute respiratory and cardiac diseases, trauma, and seizures are the most common admission diagnoses in PICU (16, 17). However, in this study, a large proportion of patients had varying degrees of primary neurologic disorder, such as ME, previous HIE, other structural brain impairments, CNS infection, and IEM, with the reasoning put forth that patients with these diseases have a poor mental state and were thus considered eligible for the study. In the present study, the proportion of electrographic seizures in only 31.8% of patients was completely correlated with clinical signs, which illustrated the significance of vEEG monitoring in PICU for the detection of subclinical electrographic seizures. Electrographic seizures without clear clinical signs were regarded as subclinical electrographic seizures in our study. Moreover, a reported research indicated that 75% of critically ill children with electrographic seizures who underwent CEEG have complete non-convulsive seizures (NCS) (2). Another study on seizures in infants also showed that only 21% of seizures detected by EEG are related to clinical signs (15). All these findings revealed that the majority of seizures in critically ill patients are subclinical seizures without obvious clinical signs, which can only be determined by EEG monitoring. Moreover, the recruitment of patients in our study was sequential and had no bias for any specific diagnosis.
The confirmation of risk factors for electrographic seizures can be potential indicators to evaluate the condition of children in PICU and draw different monitoring strategies (18). However, distinguishing patients with a high risk of seizure is of benefit for the best use of limited EEG resources. Prior epileptic encephalopathy, presence of interictal epileptiform discharges, and abnormal initial EEG background are the risk factors for electrographic seizures determined by this study. Clinical and electrographic risk factors for seizures, including clinical seizures, brain impairment induced by multiple reasons, epileptiform discharges, and abnormal EEG background activity, have been identified by several studies (2, 5, 19, 20). Although young age has been regarded as one of the risk factors for seizures in partial studies (5, 7, 8), it is not a significant parameter in some other literature (2, 19, 20). Thus, a study with an age-balanced population can be helpful to illustrate the association between age and electrographic seizures.
Although there is no common opinion regarding the association between electrographic seizures and clinical outcomes, some researchers are striving to prove it. A study on 204 comatose children concluded that seizures are associated with an unfavorable outcome in survivor patients, but not in dead cases (11). Other studies also reported that status epilepticus, but not all epileptic seizure types, is related to higher in-hospital deaths (4, 7, 8, 12, 21, 22). There may be a connection between seizure burden and poor outcomes, but early seizure detection by EEG and effective antiseizure treatment may improve the condition reversely (23). In the present study, sepsis and abnormal EEG background activity are the associated factors for in-hospital unfavorable outcomes such as unimproved condition and death. There is no significant association between seizure presence and unfavorable in-hospital outcomes in current research.
There are several limitations to this study. First, the size of the studied population is insufficient for a comprehensive in-hospital outcome analysis. It is very limited for determining the connection of mortality and electrographic seizures. Second, the population was enrolled in a single institution. Since a large proportion of the study individuals (84.05%) in the PICU had neurologic disorders, an admission-rate bias was present for this research. Third, the limited total durations of vEEG monitoring might not detect electrographic seizures completely. The clinical application of vEEG should consider both the misdiagnosis of abnormal EEG activities and the reasonable use of healthcare medical resource. Fourth, it is possible that substantial bias was introduced into this study, because it is unlikely to monitor patients without neurological symptoms or risk for neurological complications. Future research is necessary to investigate how the early detection of electrographic seizures by vEEG affects the clinical outcomes in critically ill patients.
In conclusion, this study indicates that the occurrence of electrographic seizures is over one-third of the population in PICU. vEEG is an efficient method to determine electrographic seizures in children. Abnormal EEG background activities are indicators both for the occurrence of electrographic seizures and for unimproved condition or even in-hospital deaths.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
The studies involving human participants were reviewed and approved by the Ethics Committee of Peking University First Hospital (2021KY422). Written informed consent to participate in this retrospective study was not considered necessary by the Ethics Committee.
YWu and YWa were the guarantors of integrity of the entire study and undertook study design. YWu gave the definition of intellectual content and undertook manuscript review. QG and ZY gave data acquisition. TS undertook data analysis, statistical analysis, and manuscript preparation and editing. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Towne AR, Waterhouse EJ, Boggs JG, Garnett LK, Brown AJ, Smith JR, et al. Prevalence of nonconvulsive status epilepticus in comatose patients. Neurology. (2000) 54:340–5. doi: 10.1212/WNL.54.2.340
2. Jette N, Claassen J, Emerson RG, Hirsch LJ. Frequency and predictors of nonconvulsive seizures during continuous electroencephalographic monitoring in critically ill children. Arch Neurol. (2006) 63:1750–5. doi: 10.1001/archneur.63.12.1750
3. Shahwan A, Bailey C, Shekerdemian L, Harvey AS. The prevalence of seizures in comatose children in the pediatric intensive care unit: a prospective video-EEG study. Epilepsia. (2010) 51:1198–204. doi: 10.1111/j.1528-1167.2009.02517.x
4. Abend NS, Gutierrez-Colina AM, Topjian AA, Zhao H, Guo R, Donnelly M, et al. Nonconvulsive seizures are common in critically ill children. Neurology. (2011) 76:1071–7. doi: 10.1212/WNL.0b013e318211c19e
5. Williams K, Jarrar R, Buchhalter J. Continuous video-EEG monitoring in pediatric intensive care units. Epilepsia. (2011) 52:1130–6. doi: 10.1111/j.1528-1167.2011.03070.x
6. Privitera M, Hoffman M, Moore JL, Jester D. EEG detection of nontonic-clonic status epilepticus in patients with altered consciousness. Epilepsy Res. (1994) 18:155–66. doi: 10.1016/0920-1211(94)90008-6
7. Abend NS, Arndt DH, Carpenter JL, Chapman KE, Cornett KM, Gallentine WB, et al. Electrographic seizures in pediatric ICU patients: cohort study of risk factors and mortality. Neurology. (2013) 81:383–91. doi: 10.1212/WNL.0b013e31829c5cfe
8. Abend NS, Chapman KE, Gallentine W, Goldstein J, Hyslop AE, Loddenkemper T, et al. Electroencephalographic monitoring in the pediatric intensive care unit. Curr Neurol Neurosci Reports. (2013) 13:330. doi: 10.1007/s11910-012-0330-3
9. Bozarth XL, McGuire J, Novotny E. Current Status of continuous electroencephalographic monitoring in critically ill children. Pediatr Neurol. (2019) 101:11–7. doi: 10.1016/j.pediatrneurol.2019.07.012
10. Alehan FK, Morton LD, Pellock JM. Utility of electroencephalography in the pediatric emergency department. J Child Neurol. (2001) 16:484–7. doi: 10.1177/088307380101600704
11. Kirkham FJ, Wade AM, McElduff F, Boyd SG, Tasker RC, Edwards M, et al. Seizures in 204 comatose children: incidence and outcome. Intensive Care Med. (2012) 38:853–62. doi: 10.1007/s00134-012-2529-9
12. Topjian AA, Gutierrez-Colina AM, Sanchez SM, Berg RA, Friess SH, Dlugos DJ, et al. Electrographic status epilepticus is associated with mortality and worse short-term outcome in critically ill children. Crit Care Med. (2013) 41:215–23. doi: 10.1097/CCM.0b013e3182668035
13. Sanchez SM, Carpenter J, Chapman KE, Dlugos DJ, Gallentine WB, Giza CC, et al. Pediatric ICU EEG monitoring: current resources and practice in the United States and Canada. J Clin Neurophysiol Am Electroencephal Soc. (2013) 30:156–60. doi: 10.1097/WNP.0b013e31827eda27
14. Young GB, Jordan KG, Doig GS. An assessment of nonconvulsive seizures in the intensive care unit using continuous EEG monitoring: an investigation of variables associated with mortality. Neurology. (1996) 47:83–9. doi: 10.1212/WNL.47.1.83
15. Clancy RR, Legido A, Lewis D. Occult neonatal seizures. Epilepsia. (1988) 29:256–61. doi: 10.1111/j.1528-1157.1988.tb03715.x
16. Ruttimann UE, Patel KM, Pollack MM. Length of stay and efficiency in pediatric intensive care units. J Pediatr. (1998) 133:79–85. doi: 10.1016/S0022-3476(98)70182-9
17. Khilnani P, Sarma D, Singh R, Uttam R, Rajdev S, Makkar A, et al. Demographic profile and outcome analysis of a tertiary level pediatric intensive care unit. Indian J Pediat. (2004) 71:587–91. doi: 10.1007/BF02724117
18. Gutierrez-Colina AM, Topjian AA, Dlugos DJ, Abend NS. Electroencephalogram monitoring in critically ill children: indications and strategies. Pediatr Neurol. (2012) 46:158–61. doi: 10.1016/j.pediatrneurol.2011.12.009
19. McCoy B, Sharma R, Ochi A, Go C, Otsubo H, Hutchison JS, et al. Predictors of non-convulsive seizures among critically ill children. Epilepsia. (2011) 52:1973–8. doi: 10.1111/j.1528-1167.2011.03291.x
20. Greiner HM, Holland K, Leach JL, Horn PS, Hershey AD, Rose DF, et al. Nonconvulsive status epilepticus: the encephalopathic pediatric patient. Pediatrics. (2012) 129:e748–55. doi: 10.1542/peds.2011-2067
21. Lambrechtsen FA, Buchhalter JR. Aborted and refractory status epilepticus in children: a comparative analysis. Epilepsia. (2008) 49:615–25. doi: 10.1111/j.1528-1167.2007.01465.x
22. Abend NS. Electrographic status epilepticus in children with critical illness: Epidemiology and outcome. Epilepsy and behavior: EandB. (2015) 49:223–7. doi: 10.1016/j.yebeh.2015.03.007
Keywords: electroencephalography, electrographic seizures, status epilepticus, PICU, EEG background
Citation: Sang T, Wang Y, Wu Y, Guan Q and Yang Z (2022) VEEG monitoring and electrographic seizures in 232 pediatric patients in ICU at a tertiary hospital in China. Front. Neurol. 13:957465. doi: 10.3389/fneur.2022.957465
Received: 31 May 2022; Accepted: 07 September 2022;
Published: 23 November 2022.
Edited by:
Maurizio Elia, IRCCS Oasi Maria SS, ItalyReviewed by:
Aglaia Vignoli, University of Milan, ItalyCopyright © 2022 Sang, Wang, Wu, Guan and Yang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ying Wang, Ynl3YW5neWluZzFAMTI2LmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.