
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurol., 18 August 2022
Sec. Neurotrauma
Volume 13 - 2022 | https://doi.org/10.3389/fneur.2022.941829
 Bianca Miarka1
Bianca Miarka1 Dany A. Sobarzo Soto2*
Dany A. Sobarzo Soto2* Esteban A. Aedo-Muñoz3
Esteban A. Aedo-Muñoz3 Clóvis A. Maurício1
Clóvis A. Maurício1 Vanessa T. Müller1
Vanessa T. Müller1 Nicola L. Bragazzi4
Nicola L. Bragazzi4 Ciro José Brito5
Ciro José Brito5This research study verified the technical–tactical actions during the mixed martial arts (MMA) fights to generate serious enough injury to stop the MMA round, determining technical-tactical potential risk factors for injury in official MMA combats, according to Concussion or Resignation per Submission. A total of 990 rounds with concussions and 627 resignations per submission were considered with severe injury (i.e., a fight ended by a doctor or referee). All injuries were diagnosed and managed by attending ringside physicians during the MMA fights and rounds and had a continuous technical–tactical behavior analysis, p ≤ 0.05. The leading cause of concussion was due to head trauma (~90%), with higher dependence on head strikes scored actions. Comparisons between Concussion and Resignation per Submission combats demonstrated differences between distance head strikes actions [13(6,25) vs. 9(4,18) frequencies], clinch head strikes actions [1(0;4) vs. 1(0;3) frequencies], ground head strikes actions [1(0;8) vs. 2(0;10) frequencies] and takedowns actions [0(0;1) vs. 1(0;2) frequencies]. This information may provide significant evidence regarding the doctor stoppage in concussion combats and when it could be called by officials supervising MMA.
Technical–tactical behavior analysis has been applied to study actions during mixed martial arts (MMA) tournaments and produced accurate recordings of movement patterns during this combat modality (1, 2). MMA fights are typically decided using strategic methods with an intentional goal to cause a discontinuance of the combat either by submission (verbal or physical signal of wish to discontinue the combat), knockout (KO), or technical knockout (TKO) due to judge decision after an allotted amount of time has elapsed (3). Fights may also end because of athlete retirement, forfeit, disqualification, or TKO by doctor stoppage (4, 5). The specific actions during the rounds are considered acyclic with open tasks involving aggressive strikes (punches, kicks, knees, and elbow attacks), as well as grappling actions (tackles, twists, and projections using legs) and submissions on the ground, such as chokes and joint locks (6) that can produce acute and chronic severe injuries (7, 8). Studies regarding the mechanism and seriousness of injuries (9) predominantly connected with technical-tactical actions are essential to understanding the interaction of these variables with a severe injury during MMA combats (7, 10).
There has been increased interest in concussion incidence (10–13) risk factors (14) and types of injuries in MMA (15, 16). Preceding results have indicated that the incidence of head traumas ranges between 58 and 78% of all injuries (17), highlighting maxillofacial traumas (18, 19). Studies also have reported all-cause injury incidence rates ranging from 23.6 in 100 fight participations to 28.6 in 100 fight participations in MMA (20). These values are equivalent to reports for taekwondo (4, 21, 22), karate (23, 24), kickboxing (25, 26) and boxing (27, 28). Bernick et al. (29) indicated a mean of 0.061 concussions (0.047 for boxers and 0.085 for MMA) per minute of combat time.
Concussions are present in different sports, as the pooled incidence of concussions per 1,000 younger athlete exposures (AEs) across 12 sports (football, rugby, hockey, lacrosse, soccer, basketball, baseball, softball, wrestling, field hockey, track, taekwondo, volleyball, and cheerleading) in 13 studies using a random-effects model was 0.23 (95% CI 0.19 to 0.28) (30). The three sports with the highest incidence rates were rugby (4.18 AEs), hockey (1.2 AEs), and American football (0.53 AEs) (30). Lowest incidence rates occurred in volleyball (0.03 AEs), baseball (0.06 AEs) and cheerleading (0.07 AEs). Long-term clinical cognitive consequences were shown, as 1,513 retired professional football players had ≥1 and 597 ≥ = 3 concussions with a prevalence of mild cognitive impairment (31). Moreover, in comparing former university athletes with 24.00 ± 4.55 concussions vs. the control group with 0 concussions, former athletes showed reduced semantic verbal fluency, reduced recognition, and delayed recall (32). In addition, after a concussion ending-fight, despite the indications in the rules of striking combat to prevent risks associated with concussion, ~40% of amateur fighters reported returning to competition or training on the same day a head trauma was sustained. This percentage is double that found in boxing, as ~20% of boxers endorsed hiding symptoms of head trauma from coaches and medical providers (27). However, grappling athletes had a high concussion prevalence, Brazilian jiu-jitsu demonstrated 25.2% (33) and wrestling had a 19.5% of concussion prevalence (34) during training and tournaments. In terms of injury severity patterns, a consecutive case series using professional data from post-fight medical checkups recommended that knockouts (KOs) and TKOs in MMA seem to be connected with a long time of post-combat medical suspensions and brain trauma reports (7, 35).
The fighters in MMA are constantly projecting, kicking, or striking at each other with extreme power to debilitate their opponent and claim victory. Considering such a high participation rate in MMA (4), athlete safety is the highest priority. Moreover, the moments of exposure during the bout in which fighters become more susceptible to trauma are unknown during combats ended by concussion or resignation by submission. Previous studies have observed injury incidence in MMA and found lacerations and concussion head injuries to be the most common MMA injuries (4, 9, 35). Although the concussion occurs in striking and grappling actions, the possibility of ending the round by resignation instead of targeting the head is essential to reduce the possibility of chronological effects of concussions in athletes. In addition, performance analysis of MMA combats can demonstrate technical variability in what makes the MMA event commercial.
At most competitions, the medical staff stands on hand to manage care for athletes who suffer injury. This effort at making violent, inherently unsafe combat as safe as possible has stopped abundant competitors from suffering trauma (4). These devastating injuries have been inflicted because an injured athlete can continue fighting (4, 35). A TKO by doctor stoppage occurs when a fight is stopped through a subjective analysis because of a competitor's inability to logically or safely defend himself/herself (36). Preceding rates of KOs and TKOs have drawn the attention of the scientific community (37) given the probably debilitating acute and chronic effects associated with concussions and repetitive traumatic brain trauma (9, 26). To date, no one knows a real enough number of strikes for a doctor to stop TKO in professional fights. This analysis could reduce acute and chronic injury caused by excessive attacks, particularly in the head (12, 38).
Shin et al. (39) scanned 155 boxing and mixed martial arts fighters using diffusion tensor imaging (DTI) and demonstrated that the number of KOs in MMA athletes is prognostic of microstructural injury in the brain. Chronic traumatic encephalopathy was recently associated with MMA after a middle-aged male case exhibited memory impairment, mood, and behavioral changes after years of competition (7, 27).
In contrast, Stellpflug et al. (40) described an analysis of 5,834 fights in 538 Ultimate Fighting Championship™ (UFC™) events, finding 1,186 fight-ending grappling submissions (chokes and non-chokes) and 904 fight-ending choke holds. The 904 fight-ending choke holds comprise 15.5% of the total fight outcomes and 76.2% of the total grappling submissions. Almost half (444–49.1%) of the chokes were rear-naked chokes, and most fight-ending chokes culminated in voluntary submission. Preceding studies have also suggested a relation between chronic traumatic encephalopathy and repeated traumatic brain injuries in striking combats, such as boxing, taekwondo, and kickboxing (9, 11). There is substantial debate over appropriate preventive approaches to decrease the burden of traumatic brain injuries in MMA fighters (7, 9, 28). Thus, this study aimed to verify actions associated with concussion and resignation by submission (locks and chokes) during MMA fights, which could generate serious enough injury to stop the fight.
This retrospective epidemiological study adhered to the guidelines of the Strengthening the Reporting of Observational Studies in Epidemiology Statement (41). We created a protocol (Table 1) based on previous studies that assessed injury factors (8, 20, 42) and behavior technical-tactical patterns (1, 43, 44), which were incorporated into the assessment and validation analysis (45, 46). Next, a stratified selection and comparison of MMA rounds with and without injury were done in the MMA championships (6, 24, 47). The study conforms to the World Medical Association Code of Ethics (approved by the local ethics advisory board).
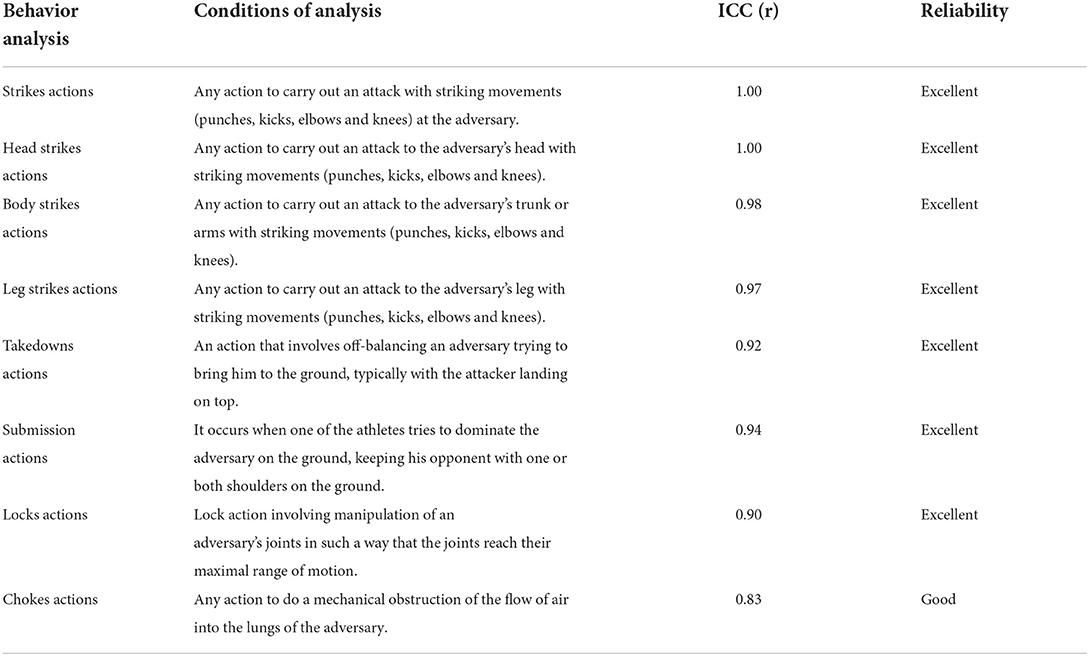
Table 1. Criteria of technical-tactical analysis from MMA performances and intraclass coefficient of correlations.
The present study considered 1,617 MMA rounds stratified from events between 2014 (after anti-doping policies increased, followed by the introduction of the U.S. Anti-doping Agency as the official anti-doping agency of the UFC™ in 2015) and 2019 (before the Pandemic COVID-19) of 635 athletes from UFC™ championships. The present study stratified all rounds from the total amount that resulted in severe injury considering a fight stoppage performed by a doctor or referee. A total of 990 rounds with concussions and 627 resignations by submission combats were considered with severe injury. The inclusion criteria were to have a round ending with resignation by submission or concussion by KO, TKO, or doctor stoppage during the MMA fight. The videos were obtained and selected at https://www.ufc.com.br/watch/library. All records had sufficient quality with high definition and were taken from a landscape view of the complete UFC™ octagon. Exclusion criteria concerned matches in which the end of the fight was a draw or no result, or finished due to unforeseen circumstances such as illegal actions. The study was previously approved by the local ethics (2014/61) and research committee and completed within the guidelines set forth in the Declaration of Helsinki.
All injury was diagnosed and managed by attending ringside physicians during the MMA fights, as the injury was recorded at the discretion of attending ringside doctors (15). Injury described in the official event records were coded according to the Orchard Sports Injury Classification System (OSICS, version 10.8), following previous reports (5, 48). The fights were analyzed using a previously developed protocol (9, 12) (Table 1) by five analysts who determined the frequency of striking and grappling actions (6, 49–51). There is typically a mean (min-max) of 2 (1–5) rounds with 264 s (6–315 s) in an MMA fight (52–54).
For performance analysis, two experts in Mixed Martial Arts analyzed 10 videos randomly selected from an amount of 635 MMA combats that were analyzed and reanalyzed 24 h later. All evaluators had ≥20 years of experience and competed at the national level. The inter-observer reliability correlation between measurements obtained for each model was verified by the interclass correlation (ICC) (2). A preceding study (55) indicated the following criteria for ICC inter-rater agreement measures: Less than.40 as poor; between.40 and.59 as fair; between.60 and.74 as good; and between.75 and 1.00 as excellent. The inter-observer reliability correlation between measurements obtained an agreement classified as “excellent” for all variables, and is shown in Table 1. Video analyzes were performed after reliability results, following criteria described in Table 1.
The Kolmogorov–Smirnov test (K–S) was used to determine the normal distribution of the data. Descriptive data of frequency of dependent variables are presented as median, first quartile (1Q), and third quartile (3Q). The Mann–Whitney test was applied for the non-parametric data to compare the effects of Concussion vs. Resignation by Submission combats. Afterward, the effect size for non-parametric analysis was calculated, defined as ES = Z/√N, where ES represented the effect size, Z was derived from the conversion of the Wilcoxon test, and N was the total number of observations. The analysis considered ES-values as small (ES < 0.10), medium (ES < 0.30), or large effect size (ES < 0.50). The significance level of p ≤ 0.05 was used. All analyses were conducted using the SPSS 20.0 program for Windows.
No effects were observed for severe trauma (excluding concussion and the resignation submission) between Concussion and Resignation by Submission combats (p = 0.155). In concussion combats, 0.2% demonstrated ankle injury, 0.4% knee injury, 0.8% leg injury, 0.2% rib injury, and 0.4% arm injury, while resignation by submission combats showed 0.3% of calf slicer, 0.3% of face crank, 0.3% of straight armbar injury, 0.3% standing rear-naked choke injury, 5.7% undefined submissions injury, 0.6% triangle armbar injury, and 0.3% of von flue choke injury.
From the total concussion vs. resignation by submission combats, 36.6 vs. 35.2% ended during the 1st round, 38.6 vs. 36% ended during the 2nd round, and 24.8 vs. 28.7% ended during the last round. No effects were observed in the ending round comparison (p = 0.214) between concussion and resignation by submission combats. Table 2 shows striking and grappling actions: round comparisons of Concussion and Resignation by Submission groups by each round.
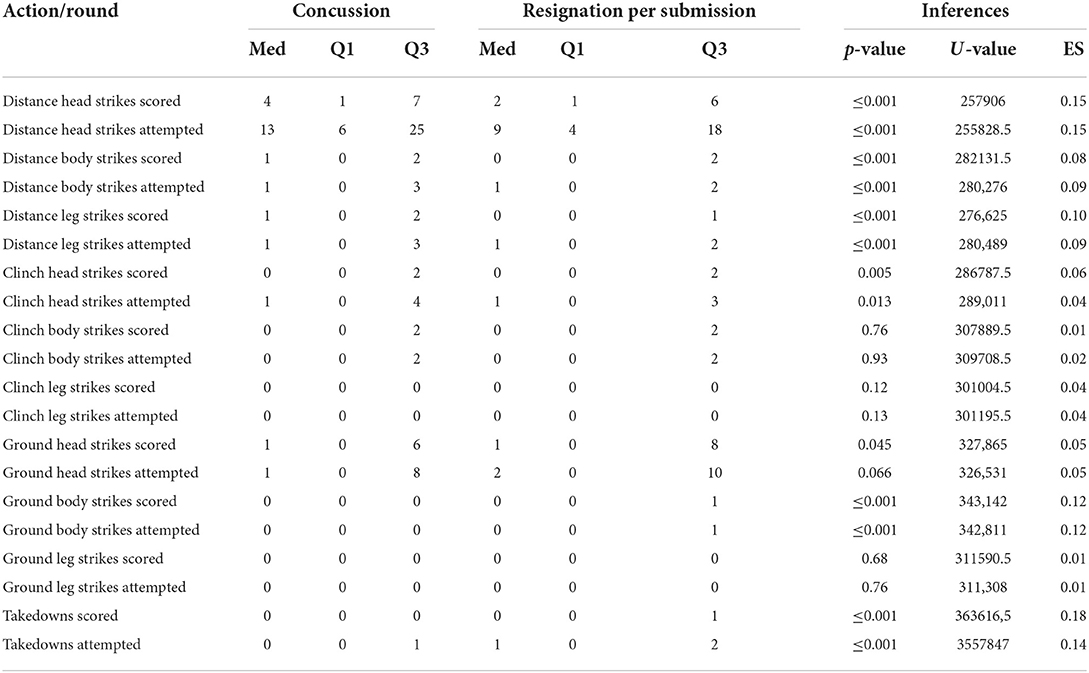
Table 2. Striking and grappling actions compared by concussion and resignation per submission groups by round.
Table 3 shows submission actions: round comparisons of Concussion and Resignation by Submission combats.
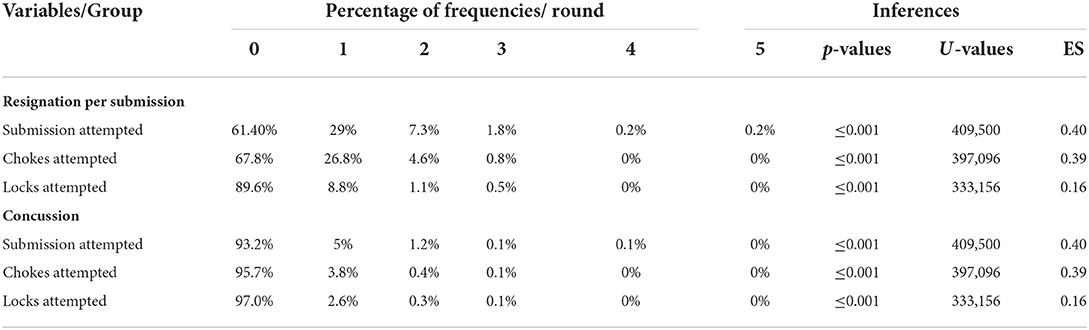
Table 3. Submission actions compared by concussion and resignation per submission groups.
Regarding the ending target, significant differences were observed between concussion and resignation by submission combats (U = 10335.00, p ≤ 0.001), concussion combats demonstrated that 90.7% of all combats had the head as the final target, 2.6% undefined target, 2.6% body, and 0.4% leg, while the resignation by submission group had 99% of undefined target, 0.3% body, and 0.6% target on the head (p ≤ 0.001). Table 4 shows the ending techniques associated with concussion or resignation by submission combats.
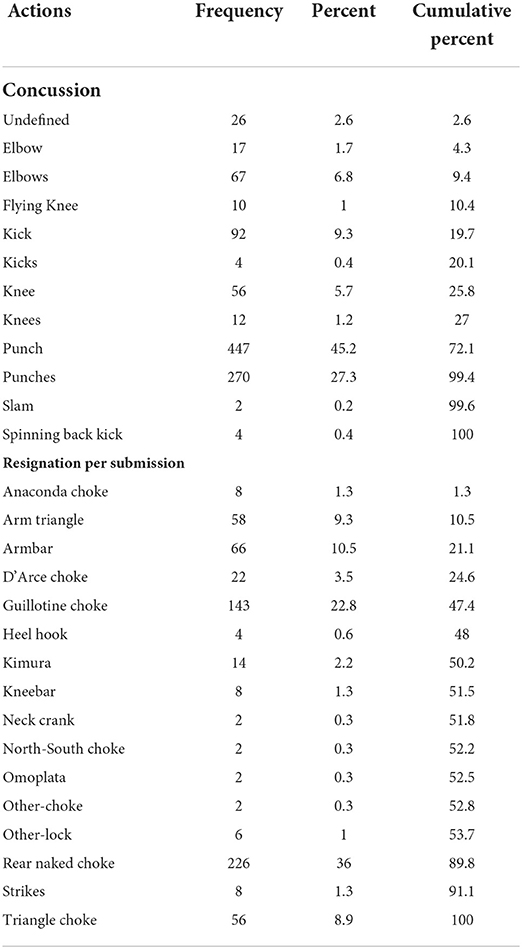
Table 4. Ending technique in frequency, percent and cumulative percent, according to concussion or resignation per submission groups.
The present study's primary purpose was to describe the injury aspects and action demands of MMA rounds with particular reference to rounds stopped by concussion or submission due to injuries determined by the ringside doctor. The main descriptive results in concussion combats showed that ~90% of fight stoppages were caused by head trauma, with striking head actions being the leading cause of all injuries, while the submissions group had 0.6 fights finished from head trauma. The descriptive analysis demonstrated a prevalence of head and neck injury, with the potential for severe injuries in combats finalized by concussion, particularly to the brain, which is persistent in MMA (56). Significant effects were observed between groups in takedowns, and distance and ground striking actions.
The present trauma results of MMA concussions indicated the need for concussion rules changes and, if it occurs, monitoring the recovery with biomarkers. Concussion rounds had ~60% more striking actions than resignation by submission. There could be a maximum count of distance or sequential head strikes attacks by round in MMA rules, this brings more dynamism to the MMA fight because the athletes would have to make attacks in different directions (e.g., legs or body), more defenses and improve their reaction time. Moreover, after concussion occurrence, athletes have to be neurologically monitored (57). Bishop and Neary (57) assessed prefrontal cortex oxygenation after concussion using near-infrared spectroscopy, which showed oxygenation changes in the brain. Previous research also demonstrated that MMA fighters exhibited reduced concentration, memory, and processing speed relative to the control group in neuropsychological testing coupled with a decrease of thinning in the left middle and superior frontal gyrus and reduced cortical thinning in the left posterior cingulate gyrus and right occipital cortex (7, 38, 58). Post-fighting scores were expressively worse for fighters with head trauma during the fight (17). A past study found anomalies in MMA fighters having different brain structures, but it seems that the thalamus and caudate are the most affected (17). The reduced performance in verbal memory, processing speed, and psychomotor speed is regularly established in investigations with fighters (17, 47). Head trauma could be a risk factor for the development of neurodegenerative conditions (11, 17, 26, 39, 56), and it may be one of the probable causes of chronic traumatic encephalopathy (16). The present results can be used to reduce the impact caused by more harmful techniques.
Concussions and blunt force trauma are a significant concern in contact and combat sports (36, 47, 59). One study detected a higher incidence of concussions involving loss of consciousness in MMA athletes and boxing athletes (~4 and ~7%) (35). Studies have shown that musculoskeletal injuries such as sprains, dislocations, and fractures in other combat sports, such as taekwondo (5), karate (24), wrestling (4), and judo (42) with fewer injury coming from lacerations, abrasions, cuts, or epistasis which induce blood loss than MMA data which demonstrated ~80% of injury with lacerations (8).
Elite athletes demonstrate 2–5 times more traumatic injuries than non-elite fighters (24). This result is probably due to helmets and the prohibition of specific techniques such as elbow strikes (22). Previous research also shows that striking sports have a typical distribution of injury by anatomic region (4, 15) and is similar to that demonstrated in our study. The head/neck was the most frequently injured anatomical region in MMA (~65%), boxing (~85%), karate (~75%), and kickboxing (~55%), whereas the lower and upper limbs were the most common anatomical regions in taekwondo (~50%) and judo (~50%) (15). Head trauma in MMA has also been associated with temporomandibular disorders because of the intensity and duration of training needed for professional competitions (18, 19).
Upper eyelid and eyebrow lacerations of fighters are recurrent and troublesome during MMA fights given the effect of hemorrhage from facial injury on the fighter's vision and in turn their ability to continue fighting (48). Findings have demonstrated one mutual action among all injury cases: head strike scoring actions. This data reveals that many basic techniques could be essential to winning, but under combat conditions and are related to severe injury (60). A past study indicated that injuries in doctor stoppage situations occurred in specific attacks that emerged when the fighter performed groundwork combat with an increase in the submission, lock, and choke actions (8). Thus, strength and conditioning coaches should be aware of the increase in the frequency of critical actions from the technical-tactical round differences, especially of striking defenses, and takedown training could focus on high-speed defenses and attacks while in a fatigued state, simulating the metabolic demands and tactical necessities of the final round (1, 2). Previous research indicates that the most common conclusion to MMA combat is a technical knockout followed by a submission (14).
Regarding limitations of the present study, it only included data from MMA contests sanctioned by UFC™ fights, limiting the generalizability of the reported data. This study did not adopt a strict operational injury definition for pragmatic reasons, following previously published research (9, 48). Moreover, the injury recording was at the discretion of the attending ringside physicians. Therefore, it is possible that several traumas that occurred were not recorded (48). This fact may result in underestimating the actual risk of severe injury, while potentially overestimating the relative proportion of more severe injuries, such as fractures. Indeed, knowledge of the present results is essential to establish technical and tactical strategies, as defeated fighters have 3 × more risk of injury than winners, and athletes in fights ending by KO or TKO have 2 × the risk of injury as fighters in fights ending in submission (20, 48). Moreover, the present data agree with the previous findings regarding the incidence of injury sustained in MMA and boxing (4, 28, 36). As MMA rules have to be constantly concerned with greater emphasis on safety (3, 4), supplementary priority could be given to maneuvers that do not involve high concussion risk and blow to the head. Furthermore, studies on the impact attenuation of protective headgear in martial arts did not support this suggestion (61). Indeed, the headgear may increase aggressive fighting (15, 62–65), and it could increase judge tolerance before stopping a fight.
This study focused on verifying what kind of technical and tactical actions occurred during the rounds to generate serious enough injury to stop the fight. With this data, it is possible to summarize how and when fighters are predisposed to severe injury in MMA, as well as to develop suggestions for rules which may allow a technical knockout to be declared based on an objective performance analysis measurement, such as a specific number of unrequited attacks per round time.
The information gained from this study enhances the mechanisms of injury during an MMA fight and the situational factors involved. Concussions associated with blunt force trauma to the head were the main worries in MMA fighters, and the present data demonstrated that more than 90% of serious injuries occurred to the head, with striking head actions, such as sequential kicks, elbows, isolated knee, and punches, being the main factors. The rates of strikes on the head per round are higher than those reported in other combats; this outcome is associated with the risk of brain injuries, and severe injury provoking doctor stoppage, as the athlete does not show cognitive and physical function to continue the combat. These findings suggest a rule change to stimulate grappling actions instead of targeting the opponent's head. Future advances in MMA injury prevention will only be achieved if study efforts are concentrated on understanding the implementation context (i.e., technical–tactical analysis) for injury prevention and continuing to build the database for the efficacy and effectiveness of training interventions.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
This study was financed in part by the Fundação de Amparo à Pesquisa do Rio de Janeiro (FAPERJ) [Grant# E# 26/202.810/2019(247397)].
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Kirk C, Hurst HT, Atkins S. Measuring the workload of mixed martial arts using accelerometry, time motion analysis and lactate. Int J Perform Anal Sport. (2015) 15:359–70. doi: 10.1080/24748668.2015.11868798
2. Miarka B, Vecchio FB, Camey S, Amtmann J. Comparisons technical-tactical and time-motion analysis of mixed martial arts by outcomes. J Strength Cond Res. (2016) 30:1975–84. doi: 10.1519/JSC.0000000000001287
3. Fernandes JR, Dal Bello F, Duarte MADB, De Carvalho PH, Queiroz ACC, Brito CJ, et al. Effect of rule changes on technical-tactical actions correlated with injury incidence in professional mixed martial arts. J Physic Educ Sport. (2018) 18:1713–21. doi: 10.7752/jpes.2018.03250
4. Bromley SJ, Drew MK, Talpey S, McIntosh AS, Finch CF. A systematic review of prospective epidemiological research into injury and illness in Olympic combat sport. Br J Sports Med. (2018) 52:8–16. doi: 10.1136/bjsports-2016-097313
5. Lystad RP, Graham PL, Poulos RG. Epidemiology of training injuries in amateur taekwondo athletes: a retrospective cohort study. Biol Sport. (2015) 32:213–8. doi: 10.5604/20831862.1150303
6. James LP, Haff GG, Kelly VG, Beckman EM. Towards a determination of the physiological characteristics distinguishing successful mixed martial arts athletes: a systematic review of combat sport literature. Sports Med. (2016) 46:1525–51. doi: 10.1007/s40279-016-0493-1
7. Lim LJH, Ho RCM, Ho CSH. Dangers of mixed martial arts in the development of chronic traumatic encephalopathy. Int J Environ Res Public Health. (2019) 16:254. doi: 10.3390/ijerph16020254
8. Miarka B, Dal Bello F, Brito CJ, Del Vecchio FB, Amtmann J, Chamari K. A 12-year cohort study of doc-stoppage in professional mixed martial arts. Int J Sports Physiol Perform. (2019) 14:606–611. doi: 10.1123/ijspp.2017-0131
9. Hutchison MG, Lawrence DW, Cusimano MD, Schweizer TA. Head trauma in mixed martial arts. Am J Sports Med. (2014) 42:1352–8. doi: 10.1177/0363546514526151
10. Follmer B, Dellagrana RA, Zehr EP. Head trauma exposure in mixed martial arts varies according to sex and weight class. Sports Health. (2019) 11:280–5. doi: 10.1177/1941738119827966
11. Hubbard R, Stringer G, Peterson K, Vaz Carneiro MRF, Finnoff JT, Savica R. The King-Devick test in mixed martial arts: the immediate consequences of knock-outs, technical knock-outs, and chokes on brain functions. Brain Inj. (2019) 33:349–54. doi: 10.1080/02699052.2018.1553068
12. Lawrence DW, Hutchison MG, Cusimano MD, Singh T, Li L. Interrater agreement of an observational tool to code knockouts and technical knockouts in mixed martial arts. Clin J Sport Med. (2014) 24:397–402. doi: 10.1097/JSM.0000000000000047
13. Merino J, Whelan BM, Finch E. Examining the occurrence and outcomes of concussion and mTBI in mixed martial arts athletes: a systematic review. Phys Sportsmed. (2022) 12:1–11. doi: 10.1080/00913847.2022.2061836
14. Bledsoe GH, Hsu EB, Grabowski JG, Brill JD, Li G. Incidence of injury in professional mixed martial arts competitions. J Sports Sci Med. (2006) 5:136–42. Available online at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3863915/
15. Lystad RP. Epidemiology of injuries in full-contact combat sports. Australas Epidemiol. (2015) 22:14.
16. Verduyn C, Bjerke M, Duerinck J, Engelborghs S, Peers K, Versijpt J, et al. CSF and blood neurofilament levels in athletes participating in physical contact sports: a systematic review. Neurology. (2021) 96:705–15. doi: 10.1212/WNL.0000000000011750
17. Schlegel P, Novotny M, Valis M, Klimova B. Head injury in mixed martial arts: a review of epidemiology, affected brain structures and risks of cognitive decline. Phys Sportsmed. (2021) 49:371–80. doi: 10.1080/00913847.2021.1885966
18. Sifuentes-Cervantes JS, Yamamoto-Valenzuela K, Autran-Martínez J, Castro-Núñez J, Guerrero LM. Maxillofacial trauma in the ultimate fighting championship. J Oral Maxillofac Surg. (2021) 79:1921.e1–1921.e7. doi: 10.1016/j.joms.2021.05.009
19. Freiwald HC, Schwarzbach NP, Wolowski A. Effects of competitive sports on temporomandibular dysfunction: a literature review. Clin Oral Investig. (2021) 25:55–65. doi: 10.1007/s00784-020-03742-2
20. Ngai KM, Levy F, Hsu EB. Injury trends in sanctioned mixed martial arts competition: a 5-year review from 2002 to 2007. Br J Sports Med. (2008) 42:686–9. doi: 10.1136/bjsm.2007.044891
21. Pieter W, Fife GP, O'Sullivan DM. Competition injuries in taekwondo: a literature review and suggestions for prevention and surveillance. Br J Sports Med. (2012) 46:485–91. doi: 10.1136/bjsports-2012-091011
22. Pieter W, Rostami M, Ziaee V. An addendum to injury rates in Iranian taekwondo athletes; a prospective study. Asian J Sports Med. (2010) 1:117–21. doi: 10.5812/asjsm.34865
23. Augustovicova D, Lystad RP, Arriaza R. Time-Loss injuries in karate: a prospective cohort study of 4 consecutive world karate championships. Orthop J Sports Med. (2019) 7:2325967119865866. doi: 10.1177/2325967119865866
24. Pieter W. Competition injury rates in young karate athletes. Sci Sports. (2010) 25:32–38. doi: 10.1016/j.scispo.2009.07.001
25. Slimani M, Chaabene H, Miarka B, Franchini E, Chamari K, Cheour F. Kickboxing review: anthropometric, psychophysiological and activity profiles and injury epidemiology. Biol Sport. (2017) 34:185–96. doi: 10.5114/biolsport.2017.65338
26. Zazryn TR, Finch CF, McCrory P. A 16-year study of injuries to professional kickboxers in the state of Victoria, Australia. Br J Sports Med. (2003) 37:448–51. doi: 10.1136/bjsm.37.5.448
27. Bennett LL, Arias JJ, Ford PJ, Bernick C, Banks SJ. Concussion reporting and perceived knowledge of professional fighters. Phys Sportsmed. (2019) 47:295–300. doi: 10.1080/00913847.2018.1552481
28. Jensen AR, Maciel RC, Petrigliano FA, Rodriguez JP, Brooks AG. Injuries sustained by the mixed martial arts athlete. Sports health. (2017) 9:64–9. doi: 10.1177/1941738116664860
29. Bernick C, Hansen T, Ng W, Williams V, Goodman M, Nalepa B, et al. Concussion occurrence and recognition in professional boxing and MMA matches: toward a concussion protocol in combat sports. Phys Sportsmed. (2020) 49:469–75. doi: 10.1080/00913847.2020.1856631
30. Pfister T, Pfister K, Hagel B, Ghali WA, Ronksley PE. The incidence of concussion in youth sports: a systematic review and meta-analysis. Br J Sports Med. (2015) 50:292–7. doi: 10.1136/bjsports-2015-094978
31. Guskiewicz KM, Marshall SW, Bailes, McCrea J M, Cantu C, Randolh C, et al. Association between recurrent concussion and late-life cognitive impairment in retired professional football players. Neurosurgery. (2005) 57:719–26. doi: 10.1227/01.NEU.0000175725.75780.DD
32. Tremblay S, De Beaumont L, Henry LC, Boulanger Y, Evans AC, Bourgouin P, et al. Sports concussions and aging: a neuroimaging investigation. Cereb Cortex. (2013) 23:1159–66. doi: 10.1093/cercor/bhs102
33. Spano, Risucci M DA, Etienne M, Petersen KH. Epidemiology of sports related concussion in Brazilian Jiu-Jitsu: a cross-sectional study. Sports. (2019) 7:53. doi: 10.3390/sports7020053
34. Bell L, Paskus T, Hainline B. Self-Reported Concussion among NCAA Student Athletes Executive Summary. Indianapolis, IN: NCAA (2014).
35. Karpman S, Reid P, Phillips L, Qin Z, Gross DP. Combative sports injuries: an edmonton retrospective. Clin J Sport Med. (2015) 26:332–4. doi: 10.1097/JSM.0000000000000235
36. Buse GJ. No holds barred sport fighting: a 10-year review of mixed martial arts competition. Br J Sports Med. (2006) 40:169–72. doi: 10.1136/bjsm.2005.021295
37. Miarka B, Coswig VS, Vecchio FBD, Brito CJ, Amtmann J. Comparisons of time-motion analysis of mixed martial arts rounds by weight divisions. Int J Perform Anal Sport. (2015) 15:12. doi: 10.1080/24748668.2015.11868861
38. Mayer AR, Ling JM, Dodd AB, Gasparovic C, Klimaj SD, Meier TB. A longitudinal assessment of structural and chemical alterations in mixed martial arts fighters. J Neurotrauma. (2015) 32:1759–67. doi: 10.1089/neu.2014.3833
39. Shin W, Mahmoud S, Sakaie K, Banks S, Lowe M, Phillips M, et al. Diffusion measures indicate fight exposure–related injury to cerebral white matter in boxers and mixed martial arts fighters. Am J Neuroradiol. (2014) 35:285–90. doi: 10.3174/ajnr.A3676
40. Stellpflug SJ, Menton WH, LeFevere RC. Analysis of the fight-ending chokes in the history of the Ultimate Fighting Championship™ mixed martial arts promotion. Phys Sportsmed. (2020) 50:60–3. doi: 10.1080/00913847.2020.1866958
41. Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP, et al. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. PLoS Med. (2007) 4:e296. doi: 10.1371/journal.pmed.0040296
42. Pocecco E, Ruedl G, Stankovic N, Sterkowicz S, Del Vecchio FB, Gutierrez-Garcia C, et al. Injuries in judo: a systematic literature review including suggestions for prevention. Br J Sports Med. (2013) 47:1139–43. doi: 10.1136/bjsports-2013-092886
43. James LP, Robertson S, Haff GG, Beckman EM, Kelly VG. Identifying the performance characteristics of a winning outcome in elite mixed martial arts competition. J Sci Med Sport. (2017) 20:296–301. doi: 10.1016/j.jsams.2016.08.001
44. Miarka B, Brito CJ, Amtmann J. Performance probabilities and outcome effects in technical–tactical factors with bout phase changes of mixed martial arts. Int J Perform Anal Sport. (2017) 17:510–20. doi: 10.1080/24748668.2017.1360103
45. Chaabene H, Franchini E, Miarka B, Selmi MA, Mkaouer B, Chamari K. Time-motion analysis and physiological responses to karate official combat sessions: is there a difference between winners and defeated karatekas? Int J Sports Physiol Perform. (2014) 9:302–8. doi: 10.1123/ijspp.2012-0353
46. Moran RW, Schneiders AG, Major KM, Sullivan SJ. How reliable are functional movement screening scores? A systematic review of rater reliability. Br J Sports Med. (2016) 50:527–36. doi: 10.1136/bjsports-2015-094913
47. Thomas RE, Thomas BC. Systematic review of injuries in mixed martial arts. Phys Sportsmed. (2018) 46:155–67. doi: 10.1080/00913847.2018.1430451
48. Lystad RP, Gregory K, Wilson J. The epidemiology of injuries in arts a systematic review and meta-analysis. Orthop J Sports Med. (2014) 2:2325967113518492. doi: 10.1177/2325967113518492
49. Brito CJ, Miarka B, de Durana ALD, Fukuda DH. Home advantage in judo: analysis by the combat phase, penalties and the type of attack. J Hum Kinet. (2017) 57:213–20. doi: 10.1515/hukin-2017-0062
50. Slimani M, Chaabene H, Miarka B, Chamari K. the activity profile of elite low-kick kickboxing competition. Int J Sports Physiol Perform. (2017) 12:182–9. doi: 10.1123/ijspp.2015-0659
51. Tornello F, Capranica L, Chiodo S, Minganti C, Tessitore A. Time-motion analysis of youth Olympic Taekwondo combats. J Strength Cond Res. (2013) 27:223–8. doi: 10.1519/JSC.0b013e3182541edd
52. Antonietto NR, Bello FD, Carrenho Queiroz AC, Berbert de Carvalho PH, Brito CJ, Amtmann J, et al. Suggestions for professional mixed martial arts training with pacing strategy and technical-tactical actions by rounds. J Strength Cond Res. (2019) doi: 10.1519/JSC.0000000000003018. [Epub ahead of print].
53. Dal Bello F, Brito CJ, Amtmann J, Miarka B. Ending MMA combat, specific grappling techniques according to the type of the outcome. J Hum Kinet. (2019) 67:271–80. doi: 10.2478/hukin-2018-0081
54. Ghoul N, Tabben M, Miarka B, Tourny C, Chamari K, Coquart J. Mixed martial arts induces significant fatigue and muscle injury Up to 24 hours post-combat. J Strength Cond Res. (2019) 33:1570–9. doi: 10.1519/JSC.0000000000002078
55. Cicchetti DV. Guidelines, criteria, and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Psychol Assess. (1994) 6:284. doi: 10.1037/1040-3590.6.4.284
56. O'Keeffe E, Kelly E, Liu Y, Giordano C, Wallace E, Hynes M, et al. Dynamic blood-brain barrier regulation in mild traumatic brain injury. J Neurotrauma. (2019) 37:347–56. doi: 10.1089/neu.2019.6483
57. Bishop S, Neary PJ. Assessing prefrontal cortex oxygenation after sport concussion with near-infrared spectroscopy. Clin Physiol Funct Imaging. (2018) 38:573–85. doi: 10.1111/cpf.12447
58. Cuningham J, Broglio SP, O'Grady M, Wilson F. History of sport-related concussion and long-term clinical cognitive health outcomes in retired athletes: a systematic review. J Athletic Training. (2020) 55:132–58. doi: 10.4085/1062-6050-297-18
59. Ochs CP, Kay MC, Register-Mihalik JK. The effect of concussive injury on individual game performance in professional collision-sport athletes. J Sport Rehabil. (2019) 28:769–73. doi: 10.1123/jsr.2018-0168
60. Dos Santos DA, Miarka B, Dal Bello F, Queiroz ACC, de Carvalho PHB, Brito CJ, et al. 10 years on time-motion and motor actions of paired mixed martial arts athletes. Int J Sports Physiol Perform. (2019) 14:399–402. doi: 10.1123/ijspp.2018-0566
61. O'Sullivan DM, Fife GP. Impact attenuation of protective boxing and taekwondo headgear. Euro J Sports Sci. (2016) 16:1219–25. doi: 10.1080/17461391.2016.1161073
62. Menger R, Menger A, Nanda A. Rugby headgear and concussion prevention: misconceptions could increase aggressive play. Neurosurg Focus. (2016) 40:E12. doi: 10.3171/2016.1.FOCUS15615
63. Lystad RP. Injuries to professional and amateur kickboxing contestants: a 15-year retrospective cohort study. Orthop J Sports Med. (2015) 3:2325967115612416. doi: 10.1177/2325967115612416
64. Miarka B, Brito CJ, Moreira DG, Amtmann J. Differences by ending-rounds and other rounds in time-motion analysis of mixed martial arts: implications for assessment and training. J Strength Cond Res. (2017) 32:534–44. doi: 10.1519/JSC.0000000000001804
65. Ultimate Fighting Championship,. UFC library. (2022). Available online at: https://www.ufc.com.br/watch/library.~
Keywords: neurology, trauma, time and motion studies, risk factors, injury, rehabilitation
Citation: Miarka B, Soto DAS, Aedo-Muñoz EA, Maurício CA, Müller VT, Bragazzi NL and Brito CJ (2022) Concussion vs. resignation by submission: Technical–tactical behavior analysis considering injury in mixed martial arts. Front. Neurol. 13:941829. doi: 10.3389/fneur.2022.941829
Received: 11 May 2022; Accepted: 22 July 2022;
Published: 18 August 2022.
Edited by:
Kelly Russell, University of Manitoba, CanadaReviewed by:
Samuel Stellpflug, Regions Hospital, United StatesCopyright © 2022 Miarka, Soto, Aedo-Muñoz, Maurício, Müller, Bragazzi and Brito. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dany A. Sobarzo Soto, ZGFueXNvYmFyem9Ac2FudG90b21hcy5jbA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.