
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurol. , 15 July 2022
Sec. Multiple Sclerosis and Neuroimmunology
Volume 13 - 2022 | https://doi.org/10.3389/fneur.2022.898741
This article is part of the Research Topic Insights in Multiple Sclerosis and Neuroimmunology: 2021 View all 20 articles
 Girolama Alessandra Marfia1
Girolama Alessandra Marfia1 Diego Centonze2,3
Diego Centonze2,3 Marco Salvetti3,4Elisabetta Ferraro5Valentina Panetta6
Marco Salvetti3,4Elisabetta Ferraro5Valentina Panetta6 Claudio Gasperini7
Claudio Gasperini7 Massimiliano Mirabella8,9*
Massimiliano Mirabella8,9* Antonella Conte10,11
Antonella Conte10,11Background: In multiple sclerosis (MS), bridging therapies are usually administered when switching from one therapy to another. Such treatments generally consist of injectable immunomodulatory drugs (interferon or glatiramer acetate), whose efficacy, safety, and tolerability data are consolidated for use even in fragile patients. We performed a nationwide survey to gather expert opinions regarding the most appropriate use of bridging therapies in MS.
Methods: An independent steering committee of Italian neurologists with expertise in MS treatment identified critical issues in the use of bridging therapies and formulated a questionnaire. This questionnaire was used to conduct a Delphi web survey, involving a panel of Italian neurologists with experience in MS treatment. Their anonymous opinions were collected in three sequential rounds. Consensus was defined as an interquartile range (IQR) ≤2.
Results: Responses were obtained from 38 experts (100%) in all three rounds. Injectable immunomodulatory drugs were considered first-line therapy in patients with mild-to-moderate disease activity and in women planning to become pregnant. In addition, the experts were confident about prescribing these drugs in patients at risk of cancer recurrence, while the panel agreed to discontinue any treatments in patients with uncontrolled cardiovascular or metabolic disorders. Moreover, bridging therapy with injectable immunomodulatory drugs was considered appropriate in order to protect the patient from disease reactivation when a prolonged washout was needed and also while waiting for the completion of the immunization schedule.
Conclusion: The results of this nationwide survey confirm that, among Italian neurologists, there was wide agreement on the use of bridging therapies with injectable immunomodulatory drugs in several conditions in order to minimize the risk of disease reactivation when a prolonged washout was required or when the immunization schedule still needed to be completed in patients planning to become pregnant and in patients at risk of cancer recurrence.
The term “bridging therapy” is used in medicine to indicate a transitional period to another stage of therapy or health. This concept is well-known and widely applicable in the field of transplantation (1, 2) and anticoagulant treatment (e.g., heparin bridge) (3). Therapeutic plasma exchange and intravenous immunoglobulins are examples of rapid but short-acting immunomodulatory treatments used as a bridge while waiting for slower-acting immunosuppressive therapies to become effective in other autoimmune neurologic diseases, such as myasthenia gravis (particularly when glucocorticoid use has to be avoided or minimized).
In multiple sclerosis (MS), bridging therapies may be administered when switching from one therapy to another. Such treatments generally consist of injectable immunomodulatory drugs (interferon or glatiramer acetate), whose efficacy, safety, and tolerability data are consolidated for use even in fragile patients. In the past, monthly pulses of intravenous steroids were suggested as an option to prevent reactivation of MS in subjects switching from natalizumab to alemtuzumab or in patients discontinuing fingolimod (4). Moreover, if the chosen disease-modifying treatment (DMT) could not be administered immediately, due, for example, to persistent leukopenia, a bridging therapy with corticosteroids, interferons, or glatiramer acetate was considered a valid option to fill this treatment gap.
However, while the concept of bridging therapy in MS is relatively new and still not adequately defined in terms of duration, it still might play an important role in MS decision-making strategies. In 2019, interferon labeling was updated to indicate that it could be safely used during pregnancy and breastfeeding, suggesting its potential role as a bridging treatment in female patients with MS with mild disease activity who plan on becoming pregnant in the short term (5–7).
The aim of this survey was to obtain expert opinions on the use of bridging therapies with injectables in MS from 38 Italian neurologists highly qualified in treating MS.
An independent steering committee of seven Italian neurologists with expertise in the treatment of MS identified critical issues concerning bridging therapies and generated a 16-item questionnaire.
This questionnaire was used to conduct a Delphi web survey with an expert panel consisting of 38 neurologists from 25 Italian MS centers.
The Delphi technique is considered an effective way to gain and measure group agreement in healthcare consensus development methods (8). It is an anonymous structured approach that uses repeated administration (rounds) of the same questionnaire given to a panel of experts (8, 9). Anonymity can reduce the effects of status, personality, and group pressure that can arise in meetings and can help resolve several difficulties typically due to group decision dynamics. Questionnaire items are provided by a small group of experts, called the board, and submitted to the entire panel. During the following rounds, the administrator who manages the process, called the facilitator, provides participants with a statistical summary of the responses from all respondents from the previous round and invites the experts to provide reasons if there is no consensus of opinion (9).
Three consensus rounds were executed over nearly 5 months (from December 2019 to April 2020). All responses were aggregated to maintain respondent anonymity. Review and approval of this study by an ethics committee were not necessary since the collected data consisted of neurologist opinions. In each round, the participants were invited to respond by scaling each statement based on the degree of agreement (ranging from 1 = no agreement to 7 = maximum agreement).
The interquartile range (IQR) was used as a measure of the deviation of the individual expert's opinion from the opinion of the whole panel (median value). The IQR is the difference between the 3rd and 1st quartile in which the middle 50% of evaluations were located.
Consensus was defined as an IQR ≤2 and agreement with the statement when the 1st quartile was ≥4. For all 16 questions, the following statistical parameters were calculated: median, 1st and 3rd quartile, and IQR. Stata 16.1 was used for all analyses and graphs.
Responses were obtained from 38 experts (100%) in all three rounds. Between the second and third rounds, 39% and 23% of the respondents changed their responses, respectively. All statements are shown in Table 1.
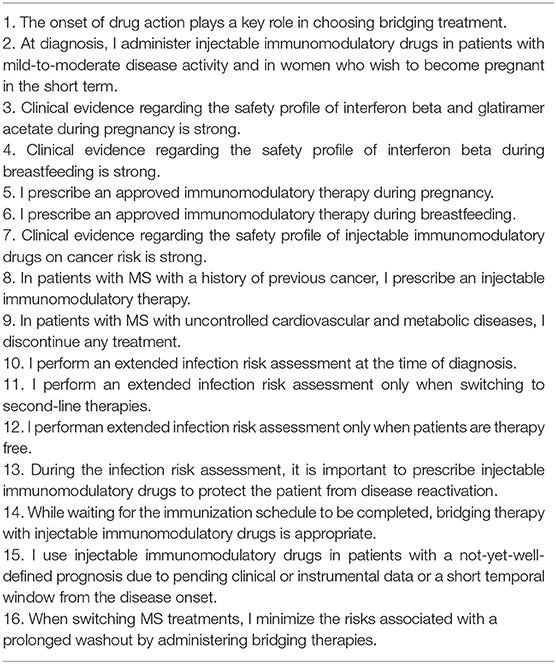
Table 1. A Delphi questionnaire.
High positive consensus was obtained for12 statements, while two statements reached a negative consensus (Items 9 and 12). In one case, the panel disagreed with the statement but did not reach a consensus (Item 11), and, in another case, there was indecision regarding the statement (Item 15; Figures 1, 2, Supplementary Figure S1).
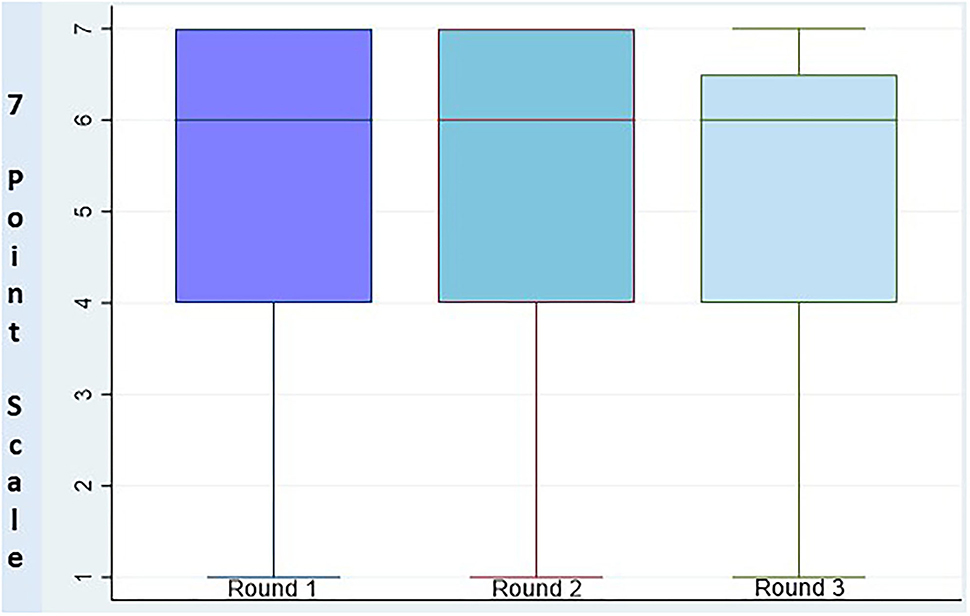
Figure 1. Distribution of responses between rounds.
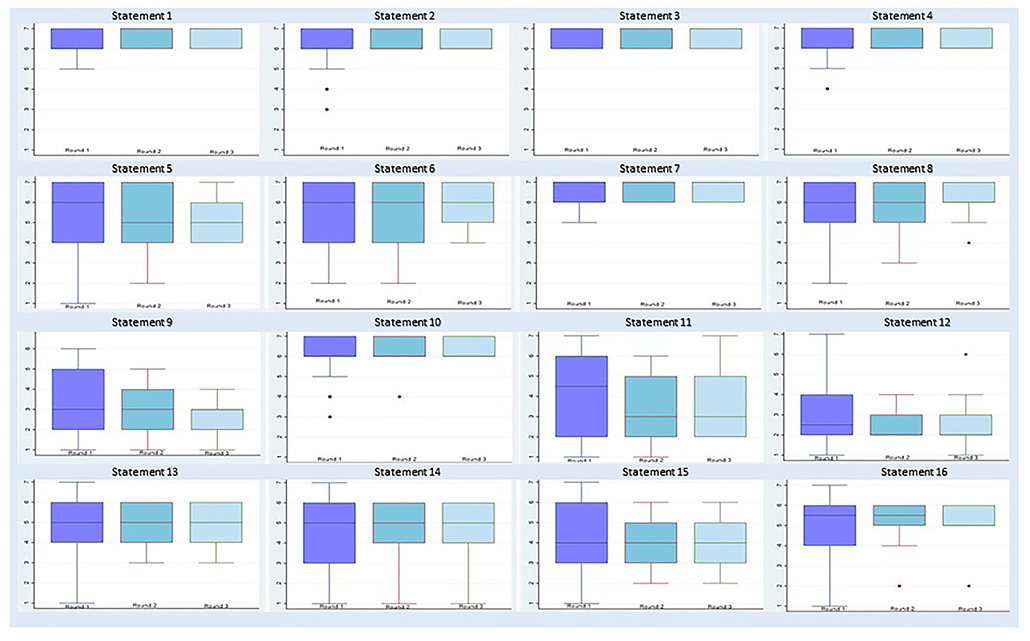
Figure 2. Distribution of responses for each item per round.
The respondents stated that the time necessary for the onset of drug activity played a critical role in choosing a bridging therapy. At the time of diagnosis, injectable immunomodulatory drugs were confirmed to be the first choice in patients with mild-to-moderate disease activity and in women who were planning to become pregnant in the short term. Neurologists agreed that scientific evidence supporting the safety of interferon and glatiramer acetate administration during pregnancy was robust, although the label of glatiramer acetate suggested avoiding its use unless the benefits outweighed the risks. The neurologists also agreed that scientific evidence regarding interferon use during breastfeeding was robust. In clinical practice, they prescribed immunomodulatory treatments approved for pregnancy and breastfeeding in patients who were pregnant or breastfeeding. Moreover, all experts were confident about prescribing injectable immunomodulatory drugs in patients at risk of cancer recurrence.
The respondents stated that they discontinued any immunomodulatory treatment in patients with uncontrolled cardiovascular or metabolic disease.
There was agreement on the statement that an extensive infection risk assessment should be performed at the time of diagnosis. However, a consensus was not reached when they were asked if they actually performed this extensive assessment before switching to second-line therapies (Item 11). It was agreed that an extended infection risk assessment should be performed only in immunosuppressive drug-free patients to avoid the risk of latent infection reactivation and interference with laboratory tests.
During the evaluation of infection risk, the experts highlighted the critical issue of protecting patients from disease reactivation by administering injectable immunomodulatory drugs as a bridging therapy. This behavior was considered appropriate also while waiting for the immunization schedule to be completed.
Item 15 resulted in indecision among neurologic health professionals regarding the use of injectable immunomodulatory drugs in patients with a not-yet-well-defined prognosis due to pending clinical findings and/or instrumental assessment or a short temporal window from the disease onset.
Regarding switching from one DMT to another, the neurologists were in favor of using a bridging therapy in order to minimize the risk of disease reactivation when prolonged washout was required in individual patients. When the various items were discussed, it was clearly intended that bridging therapy duration would outlast the 8–12 weeks required for injectables to be effective (10, 11).
The objective of this Delphi analysis was to obtain consensus on the choice and most appropriate use of bridging therapy in MS. In summary, 14 statements achieved a consensus in the survey. There was positive consensus on 12 statements and negative consensus on two statements.
A rapid onset of action was confirmed to be a critical issue driving the choice of bridging treatment, and this approach may play a key role during the current pandemic period. Interferon beta does not increase the risk linked to SARS-CoV-2, and, indeed, some studies have highlighted the protective effect of this drug as indicated as a potential antiviral treatment of coronavirus-related diseases (COVID-19, MERS, and SARS) (12–17). According to literature data, Italian neurologists participating in this survey consider interferon and glatiramer acetate as first-line treatment in patients with mild-to-moderate disease activity at early stages (18). Although there are no evidence-based guidelines on decision-making in family planning, these first-line treatments are considered appropriate strategies in women with MS who desire to become pregnant in the short term (19).
Until a few years ago, clinical treatment guidelines recommended that injectables, such as interferon be discontinued at pregnancy occurrence (20, 21). However, interferons are now considered safe in pregnancy and have obtained approval for use during pregnancy in Europe (5–7). Moreover, all injectables are no longer contraindicated during breastfeeding according to the recent label updates (2019 for interferons and 2022 for glatiramer acetate). This modified prescription label now allows interferons to be recommended from conception, during the whole gestational period, and while breastfeeding (22). Therefore, a switch to interferon may be considered for female patients with MS on oral first-line DMTs that need to be discontinued due to pregnancy planning (i.e., dimethylfumarate, teriflunomide).
In regard to currently available DMTs, several of which have immunosuppressive effects, screening patients with MS for potential malignancy risk has become crucial, especially in older patients in whom comorbidity risk is higher. Since interferon and glatiramer acetate are considered to have a favorable and well-documented safety profile and were not associated with cancer in clinical trials (23), they tend to be preferred in patients with MS with comorbidities and, in particular, in people at risk of cancer or cancer recurrence. Some disorders, including uncontrolled cardiovascular and metabolic diseases, remain a critical issue and neurologists are less confident in prescribing even injectable DMTs in these conditions due to the perceived overall benefit-risk ratio.
According to prescription label recommendations, screening for chronic infections (e.g., hepatitis B and C, tuberculosis) is required before initiating specific DMTs. Patients who test positive for latent infections must be treated before starting these drugs. In the last few years, however, an extended infection risk assessment has been widely recommended regardless of the DMT product label. To avoid possible false-negative results due to the interference of immunosuppressive drugs, this assessment should be performed in therapy-free patients. Moreover, an extensive infection risk assessment performed at the time of diagnosis in naïve patients may avoid delays in switching to a second-line treatment during the disease course and may help to identify potential subclinical comorbidities. This beneficial approach, however, is not always applied in clinical practice. In light of these considerations, prescribing a bridging therapy with injectable immunomodulatory drugs (with a slightly prevalent use of high-dosage subcutaneous interferon beta) may protect patients from disease reactivation during the evaluation of infection risk or while waiting to complete the immunization schedule, thus minimizing the risks associated with a prolonged washout. Although not detailed, it is worth noting that, for all clinical conditions considered in the Delphi panel, the time interval intended to be covered by bridging therapy outlasted the known interval required for the injectables to be active as DMTs (i.e., longer than 2–3 months).
A limitation of this study is related to the Delphi technique itself; in particular, the opinions reported are those of a select group of experts from a few Italian centers, and their approach may not be representative of Italian neurologists and clinical practice in other countries. Another limitation is related to the type of bridging drugs investigated. We specifically considered bridging with injectables and not bridging when switching from some second-line therapies to prevent rebound or bridging with natalizumab in patients on second-line DMTs in case of pregnancy desire. Thus, expert consensus is still needed regarding the unaddressed bridging of second-line DMTs. More importantly, the present study only evaluated the potential role of injectables used as bridging therapy in specific clinical conditions according to MS neurologists, but it did not address their effectiveness as bridging therapy. Nonetheless, the present Delphi study paves the way toward future clinical studies specifically designed to assess the effectiveness of injectables as bridging therapy for the various clinical conditions identified by the MS expert panel. To our knowledge, this is the first survey based on a panel of experts (neurologists) that has tried to obtain consensus on the use of bridging therapy with injectables in MS management.
The results of this nationwide survey confirm that Italian neurologists agree on the use of bridging therapy with injectable immunomodulatory drugs in several conditions in order to minimize the risk of disease reactivation when a prolonged washout is required or the immunization schedule still needs to be completed in patients who plan on becoming pregnant and in patients at risk of cancer recurrence.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
VP performed the statistical analysis. GM, MM, and AC wrote the first draft of the manuscript. DC, MS, CG, and EF wrote sections of the manuscript. All authors contributed to conception and design of the study, contributed to manuscript revision, read, and approved the submitted version.
The development of this publication was financially supported by Merck Serono Italy, an affiliate of Merck KGaA, Darmstadt, Germany, through an independent medical writing grant. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
The views and opinions described in this publication do not necessarily reflect those of the grantor.
GM received honoraria for speaking, consultation fees, and travel funding from Roche, Almirall, Bayer Schering, Biogen Idec, Merck Serono, Novartis, Sanofi-Genzyme, Mylan, and Teva. She is the principal investigator in clinical trials for Actelion, Biogen Idec, Merck Serono, Mitsubishi, Novartis, Roche, Sanofi-Genzyme, and Teva. DC is an Advisory Board member of Almirall, Bayer Schering, Biogen, GW Pharmaceuticals, Merck Serono, Novartis, Roche, Sanofi-Genzyme, and Teva and received honoraria for speaking or consultation fees from Almirall, Bayer Schering, Biogen, GW Pharmaceuticals, Merck Serono, Novartis, Roche, Sanofi-Genzyme, and Teva. He is also the principal investigator in clinical trials for Bayer Schering, Biogen, Merck Serono, Mitsubishi, Novartis, Roche, Sanofi-Genzyme, and Teva. His preclinical and clinical research was supported by grants from Bayer Schering, Biogen Idec, Celgene, Merck Serono, Novartis, Roche, Sanofi-Genzyme, and Teva. MS reports speaking honoraria and research support from Merck, Sanofi, Novartis, Biogen, Roche, Bristol Myers Squibb. EF has received travel grants from Biogen, Merck, Novartis, Sanofi-Genzyme, and Roche. VP is employed by L'altrastatistica srl – Consultancy & Training, Rome, Italy. CG received a fee as speaker or advisory board by Teva, Novartis, Roche, Merck KGaA, Bayer, Almirall, and Biogen. MM is a scientific advisory board membership of Bayer Schering, Biogen, Sanofi-Genzyme, Merck, Novartis, Teva, Mylan, Almirall. He received consulting and/or speaking fees, research support or travel grants from Almirall, Bayer Schering, Biogen, CSL Behring, Sanofi-Genzyme, Merck, Novartis, Teva, Roche, and Ultragenix. He is principal investigator in clinical trials for Biogen, Merck, Novartis, Roche, Sanofi Genzyme, Teva, Ultragenix, and CSL Behring. AC received research grants or speaking honoraria and board participation from Almirall, Biogen, BMS-Celgene Merck, Novartis, Roche, Sanofi-Genzyme.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors would like to thank the neurologists who participated in the Delphi study: Alessandra Bellacosa, Damiano Paolicelli, RoccoTotaro, Roberta Fantozzi, Fabio Buttari, Paolo Bellantonio, Elisabetta Signoriello, Roberta Lanzillo, Antonio Gallo, Sebastiano Bucello, Paolo Ragonese, Davide Maimone, Giuseppe Fenu, Massimiliano Di Filippo, Doriana Landi, Chiara Buscarinu, Antonio Cortese, Viola Baione, Fabrizia Monteleone, Viviana Nociti, Katrin Plewnia, Cinzia Scandellari, Gabriella Coniglio, Pietro Annovazzi, Cinzia Cordioli, Marinella Clerico, Assunta Bianco, Laura De Giglio, Silvia Romano, Giorgia Mataluni, and Carolina Gabri Nicoletti.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2022.898741/full#supplementary-material
Supplementary Figure S1. Data for each item per round.
1. Prasad MA, Kulik LM. The role of bridge therapy prior to orthotopic liver transplantation. J Natl ComprCancNetw. (2014) 12:1183–90. quiz 1191. doi: 10.6004/jnccn.2014.0113
2. Shigemura N, Gilbert S, Bhama JK, Crespo MM, Zaldonis D, Pilewski JM, et al. Lung transplantation after lung volume reduction surgery. Transplantation. (2013) 96:421–5. doi: 10.1097/TP.0b013e31829853ac
3. Baser O, Supina D, Sengupta N, Wang L. Anticoagulation bridging therapy patterns in patients undergoing total hip or total knee replacement in a US health plan: real-world observations and implications. Am Health Drug Benefits. (2011) 4:240−8.
4. Berger B, Baumgartner A, Rauer S, Mader I, Luetzen N, Farenkopf U, et al. Severe disease reactivation in four patients with relapsing-remitting multiple sclerosis after fingolimod cessation. J Neuroimmunol. (2015)282:118–22. doi: 10.1016/j.jneuroim.2015.03.022
5. European Medicines Agency. Human Medicine European Public Assessment Report (EPAR): Rebif. Available online at: https://www.ema.europa.eu/documents/product-information/rebif-epar-product-information_en.pdf (accessed September 21, 2021).
6. European Medicines Agency. Human Medicine European Public Assessment Report (EPAR): Plegridy. Available online at: https://www.ema.europa.eu/en/documents/product-information/plegridy-epar-product-information_en.pdf (accessed September 21, 2021).
7. European Medicines Agency. Human Medicine European Public Assessment Report (EPAR): Avonex. Available online at: https://www.ema.europa.eu/documents/product-information/avonex-epar-product-information_en.pdf (accessed September 21, 2021).
8. Murphy MK, Black NA, Lamping DL, McKee CM, Sanderson CF, Askham J, et al. Consensus development methods, and their use in clinical guideline development. Health Technol Assess. (1998) 2:i–iv.1–88. doi: 10.3310/hta2030
9. Hasson F, Keeney S, McKenna H. Research guidelines for the Delphi survey technique. J Adv Nurs. (2000) 32:1008–15. doi: 10.1046/j.1365-2648.2000.t01-1-01567.x
10. De Stefano N, Curtin F, Stubinski B, Blevins G, Drulovic J, Issard D, et al. Rapid benefits of a new formulation of subcutaneous interferon beta-1a in relapsing-remitting multiple sclerosis. MultScler. (2010) 16:888–92. doi: 10.1177/1352458510362442
11. Comi G, Filippi M, Wolinsky JS. European/Canadian multicenter, double-blind, randomized, placebo-controlled study of the effects of glatiramer acetate on magnetic resonance imaging–measured disease activity and burden in patients with relapsing multiple sclerosis. European/Canadian Glatiramer Acetate Study Group. Ann Neurol. (2001) 49:290–7. doi: 10.1002/ana.64
12. Sallard E, Lescure FX, Yazdanpanah Y, Mentre F, Peiffer-Smadja N. Type 1 interferons as a potential treatment against COVID-19. Antiviral Res. (2020) 178:104791. doi: 10.1016/j.antiviral.2020.104791
13. Sheahan TP, Sims AC, Leist SR, Schäfer A, Won J, Brown AJ, et al. Comparative therapeutic efficacy of remdesivir and combination lopinavir, ritonavir, and interferon beta against MERS-CoV. Nat Commun. (2020) 11:222. doi: 10.1038/s41467-019-13940-6
14. Mantlo E, Bukreyeva N, Maruyama J, Paessler S, Huang C. Antiviral activities of type I interferons to SARS-CoV-2 infection. Antiviral Res. (2020)179:104811. doi: 10.1016/j.antiviral.2020.104811
15. Hung IF, Lung KC, Tso EY, Liu R, Chung TW, Chu MY, et al. Triple combination of interferon beta-1b, lopinavir-ritonavir, and ribavirin in the treatment of patients admitted to hospital with COVID-19: an open-label, randomised, phase 2 trial. Lancet. (2020) 395:1695–704. doi: 10.1016/S0140-6736(20)31042-4
16. Dastan F, Nadji SA, Saffaei A, Marjani M, Moniri A, Jamaati H, et al. Subcutaneous administration of interferon beta-1a for COVID-19: a non-controlled prospective trial. Int Immunopharmacol. (2020) 85:106688. doi: 10.1016/j.intimp.2020.106688
17. Severa M, Farina C, Salvetti M, Coccia EM. Three decades of interferon-β in multiple sclerosis: can we repurpose this information for the management of SARS-CoV2 infection? Front Immunol. (2020) 11:1459. doi: 10.3389/fimmu.2020.01459
18. Melendez-Torres GJ, Armoiry X, Court R, Patterson J, Kan A, Auguste P, et al. Comparative effectiveness of beta-interferons and glatiramer acetate for relapsing-remitting multiple sclerosis: systematic review and network meta-analysis of trials including recommended dosages. BMC Neurol. (2018) 18:162. doi: 10.1186/s12883-018-1162-9
19. Coyle PK, Oh J, Magyari M, Oreja-Guevara C, Houtchens M. Management strategies for female patients of reproductive potential with multiple sclerosis: an evidence-based review. MultSclerRelatDisord. (2019) 32:54–63. doi: 10.1016/j.msard.2019.04.003
20. Sandberg-Wollheim M, Frank D, Goodwin TM, Giesser B, Lopez-Bresnahan M, Stam-Moraga M, et al. Pregnancy outcomes during treatment with interferon beta-1a in patients with multiple sclerosis. Neurology. (2005) 65:802–6. doi: 10.1212/01.wnl.0000168905.97207.d0
21. Boskovic R, Wide R, Wolpin J, Bauer DJ, Koren G. The reproductive effects of beta interferon therapy in pregnancy: a longitudinal cohort. Neurology. (2005)65:807–11. doi: 10.1212/01.wnl.0000180575.77021.c4
22. Hellwig K, Geissbuehler Y, Sabidó M, Popescu C, Adamo A, Klinger J, et al. Pregnancy outcomes in interferon-beta-exposed patients with multiple sclerosis: results from the European Interferon-beta Pregnancy Registry. JNeurol. (2020) 267:1715–23. doi: 10.1007/s00415-020-09762-y
Keywords: multiple sclerosis, bridging therapy, Delphi survey, MS management, injectable immunomodulatory drugs
Citation: Marfia GA, Centonze D, Salvetti M, Ferraro E, Panetta V, Gasperini C, Mirabella M and Conte A (2022) Bridging Therapies With Injectable Immunomodulatory Drugs in the Management of Multiple Sclerosis: A Delphi Survey of an Italian Expert Panel of Neurologists. Front. Neurol. 13:898741. doi: 10.3389/fneur.2022.898741
Received: 17 March 2022; Accepted: 20 June 2022;
Published: 15 July 2022.
Edited by:
Antonios Bayas, Augsburg University Hospital, GermanyReviewed by:
Vincent Van Pesch, Catholic University of Louvain, BelgiumCopyright © 2022 Marfia, Centonze, Salvetti, Ferraro, Panetta, Gasperini, Mirabella and Conte. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Massimiliano Mirabella, bWFzc2ltaWxpYW5vLm1pcmFiZWxsYUB1bmljYXR0Lml0; orcid.org/0000-0002-7783-114X
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.