 Andrée-Anne Marchand1*
Andrée-Anne Marchand1* Mariève Houle2
Mariève Houle2 Julie O'Shaughnessy1Claude-Édouard Châtillon3,4
Julie O'Shaughnessy1Claude-Édouard Châtillon3,4 Martin Descarreaux5
Martin Descarreaux5- 1Department of Chiropractic, Université du Québec à Trois-Rivières, Trois-Rivières, QC, Canada
- 2Department of Anatomy, Université du Québec à Trois-Rivières, Trois-Rivières, QC, Canada
- 3Department of Neurosurgery, Centre Intégré Universitaire de Santé et de Services Sociaux de la Mauricie-et-du-Centre-du-Québec, Trois-Rivières, QC, Canada
- 4Division of Neurosurgery, Faculty of Medicine, University of Montreal, Trois-Rivières, QC, Canada
- 5Department of Human Kinetics, Université du Québec à Trois-Rivières, Trois-Rivières, QC, Canada
Study Design: Secondary analysis of a randomized controlled trial.
Objective: To identify preoperative physical variables associated with favorable postoperative outcome in individuals undergoing laminectomy or laminotomy for degenerative central lumbar spinal stenosis.
Summary of Background Data: Clinical or condition specific variables have most commonly been studied as predictors of postoperative outcome in lumbar spinal stenosis. If associated to favorable postoperative outcome, modifiable physical variables would inform prehabilitation interventions for patients with degenerative central lumbar spinal stenosis.
Methods: Patients awaiting surgery for central lumbar spinal stenosis were recruited to participate in a randomized controlled trial. Following baseline data collection of demographics, clinical portrait and physical testing, participants were randomized to either 6-week active prehabilitation program or hospital standard care. Complete baseline and postoperative data were obtained from 58 participants which were included in the present analysis. Favorable postoperative outcome was determined based on two outcome measures. Favorable outcome was defined as a decrease of ≥30% on the Numerical Rating Scale for leg pain intensity and a decrease of ≥30% on the Oswestry Disability Index for low back disability. Baseline physical variables were used to conduct binary logistic regression.
Results: Sixty percent of participants were determined as having a favorable postoperative outcome. None of the included physical variables were found to be predictors of a favorable postoperative outcome based on leg pain intensity and low back pain-associated disability [trunk flexors muscle strength (OR = 0.73; 95%CI (0.02–27.12)] lumbar extensors muscle endurance [OR= 1.09; 95%CI (0.95–1.24)] total ambulation time [OR = 1.00 95%CI (0.99–1.01)] lumbar active range of motion in extension [OR = 1.08; 95%CI (0.95–1.23)] and knee extensors muscle strength [OR=1.02; 95%CI (0.98–1.06)].
Conclusion: Results show that none of the investigated variables, all related to low back and lower limbs physical capacity, were predictors of postoperative recovery. Further testing in larger cohort is needed to assess the full potential of physical outcome measures as predictors of postoperative recovery.
Introduction
Lumbar spinal stenosis (LSS) is the most common reason for undergoing lumbar spine surgery in adults over 65 years of age (1). While positive postoperative results support surgical interventions, with reports of patients experiencing rapid symptoms reduction, success rates over time are quite variable (2–8). In fact, one in three individuals will experience little to no benefit from surgery (9) and slightly more than 25% will require revision surgery within the 1-year (10). From a general standpoint, persistence of mild-to-moderate pain and disability up to 5-year should be expected (11, 12).
In the last decade, the perioperative teams have sought means to improve surgical outcomes and as a result, the concept of prehabilitation has emerged. Indeed, prehabilitation is defined as the process by which patients are better prepared to withstand the many stressors associated with surgery ahead of a surgical intervention. Augmentation of functional capacity and physiological reserve is the cornerstone of prehabilitation (13, 14). Therefore, the identification of individuals modifiable risk factors of poor surgical outcome and complications are necessary to tailor efficient prehabilitation interventions.
Recently, our group conducted a randomized controlled clinical trial investigating the effectiveness of exercise-based prehabilitation on improving postoperative recovery in patients awaiting surgery for central LSS compared to hospital standard care (15). While participants in the intervention group showed improvements in numerous clinical and physical outcome measures at the postintervention assessment, between group differences leveled out at the postoperative evaluation and follow-ups with the surgery having a tremendous positive effect on most patients in both groups. Considering that the main goal of prehabilitation is to facilitate recovery and return to baseline functional level, it was deemed important to identify physical predictors of favorable postoperative outcome that could in turn be targeted in future prehabilitation programs. Therefore, the objective of this study was to identify the physical variables associated with favorable postoperative outcomes following laminectomy or laminotomy surgery in patients with central LSS.
Methods
Study Design
This study is a secondary analysis of a randomized controlled trial investigating the effectiveness of exercise-based prehabilitation in patients awaiting surgery for lumbar spinal stenosis. A more detailed methodology regarding subject recruitment and data collection can be found in previous publications resulting from this trial (15, 16). The study protocol was registered (ClinicalTrials.gov: NCT02258672) and published elsewhere (17). Ethics approval for involvement of human participants was obtained through the Université du Québec à Trois-Rivières (UQTR) (CÉR-2014-008-00) and the Centre Intégré Universitaire de Santé et de Services Sociaux de la Mauricie-et-du-Centre-du-Québec (CER-14-204-07.07) institutional review boards. All participants provided written informed consent prior to data collection.
Original Study
Participants
Background information on the original study is provided to establish the current study context. Sixty-eight participants were recruited from the Trois-Rivières regional hospital (Quebec, Canada) during outpatient clinical encounters with members of the neurosurgery team from February 2015 to June 2019. To be included, in the original study patients had to (1) be aged over 18 years, (2) have both clinical and imaging confirmation of degenerative primarily central lumbar spinal stenosis, (3) have opted to undergo decompressive surgery (open or minimally invasive approach), (4) be able to provide written informed consent voluntarily, and (5) to understand and speak fluent French. Potential participants were excluded if they presented with non-degenerative or other than primarily central canal stenosis, inflammatory arthritic conditions, vertebral instability requiring surgical non-instrumental or instrumental fusion, altered cognitive function, or any other conditions that made them unfit to participate in a rehabilitation program as judged by their treating neurosurgeon.
Intervention
In the original study, eligible participants were randomized to either a 6-week prehabilitation program or to hospital standard care. Upon enrollment, participants provided information on demographics, answered baseline self-reported questionnaires and completed physical tests. A detailed description of outcome measures can be found elsewhere (17). All evaluation sessions were conducted at the UQTR biomechanics laboratory and followed a standardized format. Figure 1 presents the timeline of assessments along with data collection for every evaluation time point. Participants randomized to the hospital standard care group did not receive any particular intervention nor were they discouraged from keeping up with current physical activities if any. Participants randomized to the prehabilitation group aimed to meet one-on-one with the kinesiologist three times a week for 6 weeks. Training sessions lasted 30 mins and included a 5-mins warm-up and a set of five exercises designed to improve trunk stabilization, posterior chain muscles strength and endurance, and lower limb and hip muscles strength. A detailed progression of the proposed exercise can be found elsewhere (16). The analysis of the intervention effectiveness on clinical outcomes and physical function showed that despite statistically and clinically significant changes in favor of the prehabilitation group seen at the preoperative assessment these differences were not maintained at the postoperative and follow-up assessments (15).
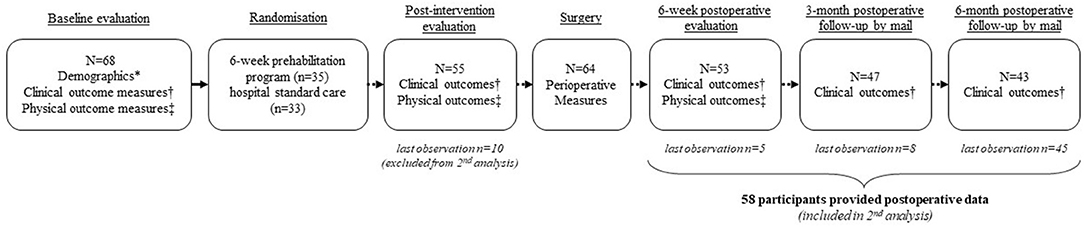
Figure 1. Timeline of outcome assessments and participants flowchart from the original trial. *Demographics included: Age, gender, employment status; variables included in the minimization process (smoking status; disability score ≥41%; presence of diabetes; nerve root motor disturbance confirmed by electrodiagnostic test); number of months since pain first started; presence of comorbidities; previous use of conservative care. †Clinical outcome measures included: Leg pain and low back pain intensity (Numerical Rating Scale); pain dominance (leg or back); low back pain-related disability (Oswestry Disability Index); Quality of life (European Quality of life EQ-5D); Kinesiophobia (Tampa scale of kinesiophobia); Depression (Beck Disability Index); Patients' global impression of change (at the post intervention assessment only). ‡Physical outcome measures included: Active lumbar ranges of motion; Lumbar flexor and extensor muscles maximum isometric voluntary contraction; Lumbar extensor muscles endurance (modified Sorenson test); Knee extensor muscles maximum isometric voluntary contraction; Walking capacities (time to first symptoms and total ambulation time during standardized treadmill evaluation).
Current Study
In the present study, we aimed to identify preoperative physical variables that are associated with favorable postoperative outcomes in a sample of patients who underwent surgery for degenerative central lumbar spinal stenosis. Of the 68 participants originally enrolled in the main trial, 58 provided both baseline and postoperative data and were included in the secondary analysis. Of the 10 participants excluded from this secondary analysis, four opted out of surgery and six did not provide postoperative data. Their baseline characteristics were, however, similar to those of completers. Postoperative outcomes were dichotomized into “favorable” or “unfavorable” based on whether participants reached a clinically meaningful percent change score from baseline in two independent outcome measures (18, 19). Favorable outcome was defined as a decrease of ≥30% from baseline in both leg pain intensity on the Numerical Rating Scale (NRS) and in low back pain-associated disability on the Oswestry Disability Index (ODI) (18, 19). Considering that participants' response rate varied over time, the latest timepoint at which they each provided data was used to determine the postoperative outcome (see Figure 1 for the participants flowchart). Thus, five participants last provided data at the 6-week postoperative evaluation, eight last provided data at the 3-month postoperative follow-up and 45 participants last provided data on the 6-month postoperative follow-up. The 13 participants that did not complete all postoperative follow-ups differed from the 45 completers in that they had lower active range of motion in lumbar extension (−6.5°; p = 0.009) at baseline. This finding is, however, unlikely to explain the loss of these participants to follow-up.
Outcome Measurement
Pain intensity was assessed using an 11-point NRS. Each patient subjectively rated its current level of leg pain on a scale of 0 to 10 (0 being an absence of pain 10 being the worst pain imaginable) (20).
Low back-related disability was measured using the validated French version of the ODI questionnaire (version 2.1a) (21). The ODI comprises 10 questions related to daily activities, including pain intensity, personal care, lifting, walking, sitting, standing, sleeping, sexual life, social life, and traveling. Each question is rated on a scale of zero to five points with a maximum possible score of 50 which in turn is reported as a percentage. Higher scores indicate greater disability.
Physical Variables Measurement
Active lumbar ranges of motion were assessed with a digital inclinometer (Digital Dualer IQ Pro™, Model CM101; JTECH Medical, Midvale, UT, USA) (22). Each range of motion (flexion, extension, right lateral flexion, left lateral flexion) were measured twice and averaged for the analysis.
Lumbar extensor muscles endurance was assessed with a modified version of the Sorenson test using an inclined bench (23). Participants were positioned on a 30° inclined Roman chair, the iliac crest aligned with the chair's border, the upper body maintained in a horizontal position (parallel to the floor) and the arms crossed over the chest. The position was maintained for as long as possible and the test was stopped when participants were either no longer able to maintain a proper horizontal position (as externally judged by the assessor), became too fatigued to continue, or experienced pain. Fatigue was objectively measured using a perceived level of effort using a Borg's Scale (24).
Isometric strength of the knee extensor muscles was assessed using a load cell (Model LSB350; Futek Advanced Sensor Technology Inc., Irvine, CA, USA) (25). Participants sat on a bench with both hips and knees bent at 90°. Three trials were completed for each leg. The highest result of each leg was recorded and averaged for analysis.
Strength of lumbar flexor and extensor muscles was assessed using an isokinetic testing device (LIDO, Loredan Biomedical Inc., Davis, CA, USA) (26). Each measurement was taken three times and averaged for analysis.
Walking capacities were assessed using two components of the exercise treadmill examination: the time to first symptoms (TFS) and the total ambulation time (TAT). Both variables were measured at a walking speed of 1.2 mph, on a 4° inclined ramp. The examination was stopped at the onset of severe symptoms, defined as the level of discomfort that would cause the patient to stop walking in usual life situations.
Data Analysis
Given that in the original study, both groups had similar postoperative improvements, all eligible participants (N = 58) were included regardless of initial group allocation for the present analysis. As the main goal was to identify a set of predictive variables, we did not use imputed data for this study. Each baseline variable was assessed for normality of its distribution using the Shapiro-Wilk test and visual inspection of the corresponding histogram. Means and standard deviations were calculated for continuous variables while proportions were reported for dichotomous variables for the complete sample of participants. Multivariate binary logistic regression was conducted to identify potential predictors of postoperative favorable outcome using baseline physical variables. Because of the small number of cases available for the conduct of the regression analysis, we determined a set of five candidate variables based on their potential to be modified by exercise-based prehabilitation interventions. In addition, leg pain dominance was entered into the regression model, despite not being a physical variable, given that it is known to be the strongest predictor of postoperative recovery. We tested for collinearity with variance inflation factor (VIF) and considered value ≥ 5.0 as indicative of collinearity (27). We controlled for randomization group, leg pain intensity and low back-related disability. Adjustments for overfitting and evaluation of the model were performed by bootstrap. Nagelkerke R2 was used to describe the amount of variation explained by the independent variables in the model. Model results were reported with odds ratios (OR) and 95% confidence intervals (95% CI). All significance tests were two-sided and conducted at a 5% significance level. All statistical analyses were performed using IBM SPSS Statistics version 28 (Armonk, NY: IBM Corp.).
Results
Baseline characteristics for all participants are presented in Table 1. Sixty percent (n = 35) of the sample achieved a favorable outcome as determined by the model prerequisites.
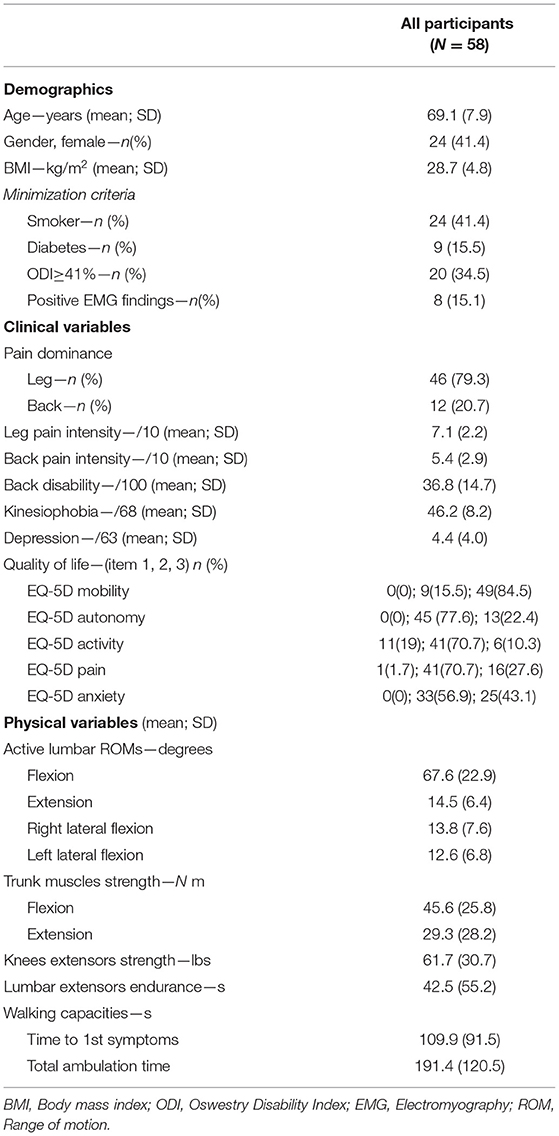
Table 1. Participants' baseline characteristics.
We identified from previous effectiveness analyses (15) the baseline physical variables that were modified by the prehabilitation intervention (i.e., for which between-group significant change was found at the postintervention assessment). These variables were (1) trunk flexors muscle strength; (2) lumbar extensors muscle endurance; (3) total ambulation time (4) lumbar active range of motion in extension; and (5) knee extensors muscle strength. These five physical variables were considered candidate prognostic factors and entered into the regression model along with leg pain dominance. There was no collinearity found between the included variables with VIF values ranging from 1.05 to 2.71. The prediction model retained leg pain dominance as the only significant independent predictor of postoperative favorable outcome. The independent variables explained 29.0% of the model variance. Table 2 presents the multivariate binary logistic regression results.
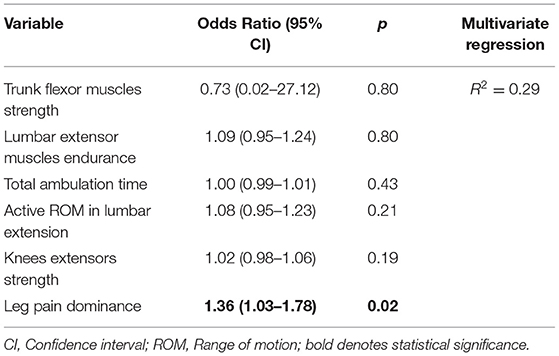
Table 2. Result of the multivariate binary logistic regression analysis.
Discussion
The aim of this study was to identify physical variables associated with favorable postoperative outcome in individuals undergoing decompressive surgery for central lumbar spinal stenosis. This is one of the few studies to investigate whether postoperative favorable outcome based on clinically meaningful difference can be predicted by objectively measured physical variables. Surprisingly, none of the considered physical variables were found to be associated with a favorable postoperative outcome based on leg pain intensity and low back pain-associated disability.
Numerous prognostic factors have been studied in the context of LSS surgery in relation to just as many outcomes. A systematic review of preoperative predictors for LSS surgery have investigated 21 prospective studies and reported on the predictive value of different outcome measures (28). Although there was a clear variation in the number of predictors and outcome measures used, the authors concluded that at 6-month follow-up, preoperative expectations predicted subjective outcome and being a male and of younger age predicted better postoperative walking ability. Furthermore, at 2 to 5-years follow-up, better preoperative walking capacity predicted better postoperative capacity and satisfaction. On the other hand, preoperative depression predicted higher levels of pain, less treatment satisfaction, poorer walking capacity and less global satisfaction (28).
More recently, additional studies have reported on numerous categories of predictors of good but also poor surgical outcomes in LSS. For instance, radiological severity of the stenosis at the laminectomy level was not predictive of surgical outcome at 1 to 5-year after instrumented posterior decompression (29) and at 1-year after surgically implanting interspinous device (30). Conversely, severe central stenosis and single-level central stenosis have been associated with lower pain intensity and higher satisfaction at 2-year follow-up (31).
With regards to clinical outcomes, higher preoperative disability has been described as a predictor of better outcome at 2-year follow-up whereas a history of psychiatric disease have been associated with a worse disability outcome (32). Similarly, depressive symptoms were strong predictors of poorer disability, symptom severity, walking capacity, and health related quality of life outcomes at 1-year follow-up (33, 34). In addition, symptoms duration of more than 33 month has been associated to a less favorable functional outcome at one- and 2-year follow-ups (35) whereas patients with symptoms of fewer than 12-month duration experience significantly better outcomes at 4-year follow-up (36).
With respect to objective physical outcome measures, Lee et al. reported that radiculopathy confirmed by electrodiagnostic study was related to unsuccessful surgical outcomes (37). In addition, Shen et al. reported on the predictive value of hand grip strength and found that higher preoperative values were associated with better surgical outcomes in terms of disability and health status 6-month after spine surgery (38).
To the best of our knowledge very few studies have investigated objective and modifiable physical measures related to the low back or lower limbs to predict surgical outcome. Although self-reported measures may be more easily collected in the clinical setting, objective physical measures offer valuable insight on patients' current level of physical fitness and facilitate the identification of deficits that could then be targeted in prehabilitation programs. Among modifiable physical predictors of postoperative success, isometric trunk extensor strength was reported to be associated with 6-month postoperative 6-mins walk distance in patients undergoing surgery for LSS (12). Furthermore, gait measurements derived from a smart-shoe technology showed promising results for predicting postoperative pain intensity and low back disability outcomes (39). Finally, a preoperative body mass index ≤ 29.1 kg/m2 was reported to be associated with higher surgical success at 2-year follow-up (40) and the presence of skeletal low muscle mass has been shown to be a significant predictor of falls within 12-months of surgery (41).
Variability in predictive value across studies may be attributable to the wide definitions used to define “favorable outcome,” “success” or “satisfaction” following surgery, the inclusion of mixed surgical populations such as the use of complex surgical techniques, the differences in the choice of outcome measures and whether the latter were specific to the target population, and self-reported or objectively measured. The fact that numerous predictors have been identified based on different outcomes suggests that their predictive value may be outcome specific. Therefore, there is a need for a consensus about a core set of relevant outcomes to measure postoperative success in LSS which in turn would increase comparability across studies. Larger studies are needed to assess the full potential of physical variables as predictors of postoperative favorable outcome in patients with lumbar spinal stenosis and to inform the design of more effective prehabilitation programs.
Limitations
Due to losses to follow-up, timing of outcomes measurement differed between participants, and it was therefore not possible to consider the postoperative trajectory as a whole to determine outcome. Determining predictors of outcome based on the combination of two different intervention groups may be viewed as a limitation, but the fact that they both yielded similar postoperative outcomes made the grouping possible. The small sample size resulted in great variability for many predictive variables limiting the power to find significant associations with the postoperative outcome and only a small number of potential predictive variables could be tested. Similarly, the inclusion of participants with low back pain dominance, considered non-optimal surgical candidate as opposed to leg pain dominance, may have affected our ability to identify predictive factors of favorable postoperative outcome.
Conclusion
This study examined physical variables that may influence postoperative outcome in individuals with lumbar spinal stenosis. Results show that none of the investigated variables, all related to low back and lower limbs physical capacity, were predictors of postoperative recovery. Further investigation of modifiable physical variables able to predict surgical outcome in LSS is needed to define efficient prehabilitation interventions for this population.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by the Research Ethics Board of Université du Québec à Trois-Rivières (CÉR-2014-008-00) and the Centre Intégré Universitaire de Santé et de Services Sociaux de la Mauricie-et-du-Centre-du-Québec (CER-14-204-07.07). The patients/participants provided their written informed consent to participate in this study.
Author Contributions
AAM took part in the conceptualization and the design of methodology, conducted the investigation and analyses, and wrote the initial draft. MH was involved in conducting the investigation and reviewing and editing the manuscript. JO and CÉC took part in the conceptualization of the study, provided resources during the data collection, and reviewed the manuscript. MD was responsible for project administration and edited and reviewed the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This study was provided by the Chaire de Recherche Internationale en Santé Neuromusculosquelettique and its partner and the Centre Intégré Universitaire de Santé et de Services Sociaux de la Mauricie-et-du-Centre-du-Québec. The contribution of AAM was supported by the Fonds de recherche du Québec en Santé (FRQS).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Deyo RA, Mirza SK, Martin BI, Kreuter W, Goodman DC, Jarvik JG. Trends, major medical complications, and charges associated with surgery for lumbar spinal stenosis in older adults. JAMA. (2010) 303:1259–65. doi: 10.1001/jama.2010.338
2. Foulongne E, Derrey S, Ould Slimane M, Leveque S, Tobenas AC, Dujardin F, et al. Lumbar spinal stenosis: which predictive factors of favorable functional results after decompressive laminectomy? Neurochirurgie. (2013) 59:23–9. doi: 10.1016/j.neuchi.2012.09.005
3. Amundsen T, Weber H, Nordal HJ, Magnaes B, Abdelnoor M, Lilleas F. Lumbar spinal stenosis: conservative or surgical management?: a prospective 10-year study. Spine (Phila Pa 1976). (2000) 25:1424–35. doi: 10.1097/00007632-200006010-00016
4. Atlas SJ, Keller RB, Wu YA, Deyo RA, Singer DE. Long-term outcomes of surgical and nonsurgical management of lumbar spinal stenosis: 8 to 10 year results from the maine lumbar spine study. Spine (Phila Pa 1976). (2005) 30:936–43. doi: 10.1097/01.brs.0000158953.57966.c0
5. Iguchi T, Kurihara A, Nakayama J, Sato K, Kurosaka M, Yamasaki K. Minimum 10-year outcome of decompressive laminectomy for degenerative lumbar spinal stenosis. Spine (Phila Pa 1976). (2000) 25:1754–9. doi: 10.1097/00007632-200007150-00003
6. Javid MJ, Hadar EJ. Long-term follow-up review of patients who underwent laminectomy for lumbar stenosis: a prospective study. J Neurosurg. (1998) 89:1–7. doi: 10.3171/jns.1998.89.1.0001
7. Jonsson B, Annertz M, Sjoberg C, Stromqvist B. A prospective and consecutive study of surgically treated lumbar spinal stenosis. Part II: five-year follow-up by an independent observer. Spine (Phila Pa 1976). (1997) 22:2938–44. doi: 10.1097/00007632-199712150-00017
8. Stromqvist B, Fritzell P, Hagg O, Jonsson B, Sanden B. Swespine: the Swedish spine register: the 2012 report. Eur Spine J. (2013) 22:953–74. doi: 10.1007/s00586-013-2758-9
9. Hebert JJ, Abraham E, Wedderkopp N, Bigney E, Richardson E, Darling M, et al. Patients undergoing surgery for lumbar spinal stenosis experience unique courses of pain and disability: A group-based trajectory analysis. PLoS ONE. (2019) 14:e0224200. doi: 10.1371/journal.pone.0224200
10. Machado GC, Ferreira PH, Harris IA, Pinheiro MB, Koes BW, van Tulder M, et al. Effectiveness of surgery for lumbar spinal stenosis: a systematic review and meta-analysis. PLoS ONE. (2015) 10:e0122800. doi: 10.1371/journal.pone.0122800
11. Fritsch CG, Ferreira ML, Maher CG, Herbert RD, Pinto RZ, Koes B, et al. The clinical course of pain and disability following surgery for spinal stenosis: a systematic review and meta-analysis of cohort studies. Eur Spine J. (2017) 26:324–35. doi: 10.1007/s00586-016-4668-0
12. Takenaka H, Sugiura H, Kamiya M, Nishihama K, Ito A, Suzuki J, et al. Predictors of walking ability after surgery for lumbar spinal canal stenosis: a prospective study. Spine J. (2019) 19:1824–31. doi: 10.1016/j.spinee.2019.07.002
13. Topp R, Ditmyer M, King K, Doherty K, Hornyak J. The effect of bed rest and potential of prehabilitation on patients in the intensive care unit. AACN Clin Issues. (2002) 13:263–76. doi: 10.1097/00044067-200205000-00011
14. Carli F, Ferreira V. Prehabilitation: a new area of integration between geriatricians, anesthesiologists, exercise therapists. Aging Clin Exp Res. (2018) 30:241–244 doi: 10.1007/s40520-017-0875-8
15. Marchand AA, Houle M, O'Shaughnessy J, Châtillon C, Cantin V, Descarreaux M. Effectiveness of an exercise-based prehabilitation program for patients awaiting surgery for lumbar spinal stenosis: a randomized clinical trial. Sci Rep. (2021) 11:11080. doi: 10.1038/s41598-021-90537-4
16. Marchand AA, Suitner M, O'Shaughnessy J, Châtillon C, Cantin V, Descarreaux M. Feasibility of conducting an active exercise prehabilitation program in patients awaiting spinal stenosis surgery: a randomized pilot study. Sci Rep. (2019) 9:12257. doi: 10.1038/s41598-019-48736-7
17. Marchand AA, Suitner M, O'Shaughnessy J, Chatillon CE, Cantin V, Descarreaux M. Effects of a prehabilitation program on patients' recovery following spinal stenosis surgery: study protocol for a randomized controlled trial. Trials. (2015) 16:483. doi: 10.1186/s13063-015-1009-2
18. Austevoll IM, Gjestad R, Grotle M, Solberg T, Brox JI, Hermansen E, et al. Follow-up score, change score or percentage change score for determining clinical important outcome following surgery? An observational study from the Norwegian registry for Spine surgery evaluating patient reported outcome measures in lumbar spinal stenosis and lumbar degenerative spondylolisthesis. BMC Musculoskelet Disord. (2019) 20:31. doi: 10.1186/s12891-018-2386-y
19. Asher AM, Oleisky ER, Pennings JS, Khan I, Sivaganesan A, Devin CJ, et al. Measuring clinically relevant improvement after lumbar spine surgery: is it time for something new? Spine J. (2020) 20:847–56. doi: 10.1016/j.spinee.2020.01.010
20. Hawker GA, Mian S, Kendzerska T, French M. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res (Hoboken). (2011) 63:S240–52. doi: 10.1002/acr.20543
21. Vogler D, Paillex R. M., Norberg, de Goumoëns P, Cabri J. Validation transculturelle de l'Oswestry disability index en français. Ann de Réadapt Méd Phys. (2008) 51:379–85. doi: 10.1016/j.annrmp.2008.03.006
22. MacDermid JC, Arumugam V, Vincent JI, Payne KL, So AK. Reliability of three landmarking methods for dual inclinometry measurements of lumbar flexion and extension. BMC Musculoskelet Disord. (2015) 16:121. doi: 10.1186/s12891-015-0578-2
23. Champagne A, Descarreaux M, Lafond D. Comparison between elderly and young males' lumbopelvic extensor muscle endurance assessed during a clinical isometric back extension test. J Manipulative Physiol Ther. (2009) 7:521–6. doi: 10.1016/j.jmpt.2009.08.008
24. Borg GA. Psychophysical bases of perceived exertion. Med Sci Sports Exerc. (1982) 14:377–81. doi: 10.1249/00005768-198205000-00012
25. Padulo J, Trajković N, Cular D, Grgantov Z, Madić DM, Di Vico R, et al. Validity and Reliability of Isometric-Bench for Knee Isometric Assessment. Int J Environ Res Public Health. (2020) 17:4326. doi: 10.3390/ijerph17124326
26. Juan-Recio C, López-Plaza D, Barbado Murillo D, García-Vaquero MP, Vera-Garcia FJ. Reliability assessment and correlation analysis of 3 protocols to measure trunk muscle strength and endurance. J Sports Sci. (2018) 36:357–64. doi: 10.1080/02640414.2017.1307439
27. O'brien RM. A caution regarding rules of thumb for variance inflation factors. Qual Quant. (2007) 41:673–90. doi: 10.1007/s11135-006-9018-6
28. Aalto TJ, Malmivaara A, Kovacs F, Herno A, Alen M, Salmi L, et al. Preoperative predictors for postoperative clinical outcome in lumbar spinal stenosis: systematic review. Spine (Phila Pa 1976). (2006) 31:E648–63. doi: 10.1097/01.brs.0000231727.88477.da
29. Alicioglu B, Yilmaz B, Bulakbasi N, Copuroglu C, Yalniz E, Aykac B, et al. Magnetic resonance imaging predictors of surgical outcome in degenerative lumbar spinal stenosis. Jpn J Radiol. (2012) 30:811–8. doi: 10.1007/s11604-012-0125-0
30. Moojen WA, Schenck CD, ALycklama NGJ Jacobs WCH, Van der Kallen, Arts MP, et al. Preoperative MRI in patients with intermittent neurogenic claudication: relevance for diagnosis and prognosis. Spine (Phila Pa 1976). (2018). 43:348–55. doi: 10.1097/BRS.0000000000001301
31. Kuittinen P, Sipola P, Leinonen V, Saari T, Sinikallio S, Savolainen S, et al. Preoperative MRI findings predict two-year postoperative clinical outcome in lumbar spinal stenosis. PLoS ONE. (2014) 9:e106404. doi: 10.1371/journal.pone.0106404
32. Athiviraham A, Wali ZA, Yen D. Predictive factors influencing clinical outcome with operative management of lumbar spinal stenosis. Spine J. (2011) 11:613–7. doi: 10.1016/j.spinee.2011.03.008
33. Sinikallio S, Aalto T, Airaksinen O, Herno A, Kroger H, Viinamaki H. Depressive burden in the preoperative and early recovery phase predicts poorer surgery outcome among lumbar spinal stenosis patients: a one-year prospective follow-up study. Spine (Phila Pa 1976). (2009) 34:2573–8. doi: 10.1097/BRS.0b013e3181b317bd
34. Stull JD, Divi SN, Goyal DKC, Bowles DR, Reyes AA, Bechay J, et al. Preoperative mental health component scoring is related to patient reported outcomes following lumbar fusion. Spine (Phila Pa 1976). (2020) 45:798–803. doi: 10.1097/BRS.0000000000003399
35. Ng LC, Tafazal S, Sell P. The effect of duration of symptoms on standard outcome measures in the surgical treatment of spinal stenosis. Eur Spine J. (2007) 16:199–206. doi: 10.1007/s00586-006-0078-z
36. Radcliff KE, Rihn J, Hilibrand A, DiIorio T, Tosteson T, Lurie JD, et al. Does the duration of symptoms in patients with spinal stenosis and degenerative spondylolisthesis affect outcomes?: analysis of the Spine Outcomes Research Trial. Spine (Phila Pa 1976). (2011) 36:2197–210. doi: 10.1097/BRS.0b013e3182341edf
37. Lee JH, Lee SH. Clinical usefulness of electrodiagnostic study to predict surgical outcomes in lumbosacral disc herniation or spinal stenosis Eur Spine J. (2015) 24:2276–80. doi: 10.1007/s00586-014-3475-8
38. Shen F, Kim HJ, Lee NK, Chun HJ, Chang BS, Lee CK, et al. The influence of hand grip strength on surgical outcomes after surgery for degenerative lumbar spinal stenosis: a preliminary result. Spine J. (2018) 18:2018–24. doi: 10.1016/j.spinee.2018.04.009
39. Lee SI, Campion A, Huang A, Park E, Garst JH, Jahanforouz N, et al. Identifying predictors for postoperative clinical outcome in lumbar spinal stenosis patients using smart-shoe technology. J Neuroeng Rehabil. (2017) 14:77. doi: 10.1186/s12984-017-0288-0
40. Azimi P, Yazdanian T, Shahzadi S, Benzel EC, Azhari S, Nayeb Aghaei H, et al. Cut-off value for body mass index in predicting surgical success in patients with lumbar spinal canal stenosis. Asian Spine J. (2018) 12:1085–91. doi: 10.31616/asj.2018.12.6.1085
Keywords: lumbar spinal stenosis, predictors, physical variables, postoperative outcome, prehabilitation
Citation: Marchand AA, Houle M, O'Shaughnessy J, Châtillon C-É and Descarreaux M (2022) Physical Predictors of Favorable Postoperative Outcomes in Patients Undergoing Laminectomy or Laminotomy for Central Lumbar Spinal Stenosis: Secondary Analysis of a Randomized Controlled Trial. Front. Neurol. 13:848665. doi: 10.3389/fneur.2022.848665
Received: 04 January 2022; Accepted: 15 March 2022;
Published: 15 April 2022.
Edited by:
Giorgio Scivoletto, Santa Lucia Foundation (IRCCS), ItalyReviewed by:
Xuelin Li, University of South China, ChinaNicola Montano, Fondazione Policlinico Universitario Agostino Gemelli IRCCS—Università Cattolica del Sacro Cuore, Italy
Copyright © 2022 Marchand, Houle, O'Shaughnessy, Châtillon and Descarreaux. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Andrée-Anne Marchand, YW5kcmVlLWFubmUubWFyY2hhbmRAdXF0ci5jYQ==