 Fkrte Kebede Woldetsadik1
Fkrte Kebede Woldetsadik1 Tesfa Kassa1
Tesfa Kassa1 Workagegnehu Hailu Bilchut2
Workagegnehu Hailu Bilchut2 Alemu kassaw Kibret1
Alemu kassaw Kibret1 Yisak Girma Guadie1
Yisak Girma Guadie1 Getachew Azeze Eriku1*
Getachew Azeze Eriku1*- 1Department of Physiotherapy, School of Medicine, College of Medicine and Health Science, University of Gondar, Gondar, Ethiopia
- 2Department of Internal Medicine, School of Medicine, College of Medicine and Health Science, University of Gondar, Gondar, Ethiopia
Introduction: Stroke is a global health problem, causing significant morbidities and mortalities in both developing and developed countries. Patients living with chronic diseases like hypertension are at a high risk of stroke. Approximately 80% of strokes could be prevented with necessary preventive practices. There is scarce evidence in the preventive practices in Ethiopia, particularly in the study area. Therefore, this study aimed to assess knowledge and prevention practices related to stroke among hypertensive patients at the University of Gondar comprehensive specialized hospital, northwest Ethiopia.
Methods: An institution-based cross-sectional study was conducted among 393 hypertensive patients at the University of Gondar Comprehensive Specialized Hospital from May 1st to June 30th, 2021. The study participants were selected by a systematic random sampling technique. A semi-structured and interviewer-administered questionnaire was used to collect data. The data was entered into EPI Info version 7.2.1 and analyzed with SPSS version 23.0. Binary logistic regression analyses were undertaken to identify associated factors. The level of significance was determined using the adjusted odds ratio (AOR) with its 95% CI at a p-value of 0.05.
Results: Participants in this study had adequate knowledge of stroke and good prevention practices in 40.7% (95% CI: 35.9, 45.5) and 51.7% (95 CI: 46.8, 56.5) of cases, respectively. Attending secondary education and above 4.6 (95% CI: 2.08, 10.17), knowing someone who has had a stroke 13.17 (95% CI: 7.3, 23.77), and physical activity 4.05 (95% CI: 2.23, 7.36) were all significantly associated with adequate stroke knowledge. Furthermore, educational status (attending primary education 2.61 (95% CI: 1.44, 4.73) and secondary education and above 3.75 (95% CI: 1.99, 7.05), being an urban dweller 9.65 (95% CI: 5.04, 18.44), duration of hypertension 1.9 (95% CI: 1.15, 3.14), knowing someone with a stroke 2.27 (95% CI: 1.30, 3.93), and physical activity 1.76 (95% CI: 1.03, 3.01) were associated with good stroke prevention practices.
Conclusion: The proportion of participants with good-related knowledge and prevention practice is relatively good.
Background
Stroke is the leading cause of significant mortality and disability worldwide (1). Globally, stroke is the second leading cause of death with 6.5 million deaths and the third leading cause of death and disability combined, after neonatal disorders and ischemic heart disease with 143 million disability adjusted life years (DALYs) (2, 3). In 2019, there were 101 million prevalent cases of stroke and 12.2 million incident stroke cases globally (1).
Despite the tremendous progress and improvement in evidence-based stroke management, the burden of stroke has rapidly increased over the past three decades (4) and it has shifted from developed to low- and middle-income countries (4, 5). Several factors have been identified as contributing to this burden shift, including aging population, population growth, and increased burden of cardiovascular diseases, changing disease patterns, rapid socio-demographic and lifestyle changes, and health care (6, 7). Currently, 75.2% of all stroke deaths and 81.1% of the total DALYs lost due to stroke occur in developing countries (5, 8, 9). The mortality rate from stroke in sub-Saharan Africa (SSA) is five times higher compared to developed countries (1, 10). The prevalence of ischemic and hemorrhagic strokes in Ethiopia was 31.5 and 18.3%, respectively, with 50.2% having an undetermined type of stroke (11). Stroke, therefore, has emerged as a major public health priority in developing countries (7).
Stroke has a significant impact on physical, mental, and social wellbeing of the individual life (12). It not only affects the individual, but it also places a caregiver burden on family members, and the direct cost of stroke management and indirect loss of productivity from both the affected individual and their caregivers is enormous, resulting in a high social burden (13, 14).
Although healthcare providers may know the prevention of stroke and control the major risk factors, patients' lack of knowledge about risk factors for experiencing new events of stroke is a contributing factor to poor adherence to medical advice and treatment (15). Whereas, awareness of stroke risk factors and warning signs is important for stroke prevention and seeking care for hypertensive patients, ultimately reducing the occurrence of stroke (16). Patients living with chronic non-communicable diseases like hypertension are at high risk of developing strokes (17). Almost half of the stroke survivors were diagnosed with hypertension, and one fifth of them died in the hospital (18). In Ethiopia, hypertension is the most commonly reported risk factor for stroke, accounting for 37.1% of all stroke risk factors. Hemorrhagic stroke (45.1%) is more prevalent than ischemic stroke (37.6%) (11).
The knowledge of stroke warning signs and risk factors has been found to be important for early treatment of stroke (19) and prevention of stroke, which reduces mortality due to stroke and improves prognosis for stroke survivors (20). To a large extent, stroke is a preventable condition, there are many modifiable risk factors of stroke (21). Prevention strategies that focus on modifiable factors such as hypertension, diabetes mellitus, smoking, unhealthy diet, and sedentary physical activity practices can reduce the stroke burden by up to 80% (22, 23).
Even though early identification of stroke warning signs and risk factors is essential for stroke prevention and early management, there is low level of knowledge in the general population (24, 25). The studies done in Ethiopia investigated only the warning signs, risk factors, and prevention knowledge of stroke (26–28). Furthermore, no research has investigated the stroke prevention practices of hypertensive patients. To fill this knowledge and prevention practice gap, this study aimed to determine the knowledge, prevention practice, and associated factors of stroke among hypertension patients in the University of Gondar comprehensive specialized hospital.
Methods and Materials
Study Design, Setting and Period
An institutional-based cross-sectional study was conducted from May 1st to Jun 30th, 2021 at the University of Gondar Comprehensive Specialized Hospital (UoGCSH), Gondar city, northwest Ethiopia. Gondar city is the administrative city of central Gondar zone which is found in Amhara region and located 738 km from Addis Abeba and 175 km from Bahir dar which is the capital city of the region. UOGCSH is a specialized hospital in the Gondar area providing a tertiary level health care services as a major referral center for more than 7 million people from the surrounding areas. The UOGCSH has an outpatient department that provides follow-up services for chronic disease including hypertension, stroke and diabetes.
Study Population and Eligibility Criteria
Hypertensive patients who have been attending a chronic care follow-up clinic at UOGCSH during the data collection period were included in this study. Patients with hypertension who had previously experienced a transient ischemic attack or stroke, critically ill patients, underlying severe mental illness, or were unable to provide the necessary information on their own were excluded.
Sample Size Determination and Sampling Procedure
The sample size was determined using the single population proportion formula with the assumption of a 95% level of confidence and a 10% marginal error (d). With the assumption of a 50% proportion of hypertensive patients who have good knowledge and prevention practices toward stroke, there is no similar study on stroke prevention practice done in a similar area.
Where n = the required sample size for the study.
d 2 = margin of tolerable sampling error commonly used 0.05.
Z = is 1.96 for 95%.
Among the two-sample sizes calculated, the larger sample size, which is 385, has been selected.
The required sample size is 424, with a 10% non-response rate.
The hospital records showed there were about 250 to 270 hypertensive patients in the outpatient's clinic every week. Thereafter, the skipping interval (Kth) was calculated by dividing the 1-month report by the calculated sample size (1,040/424), resulting in 2. The study participants were selected randomly using a lottery method. Finally, a systematic random sampling technique was used to select all eligible study participants.
Data Collection Procedure and Tool
The data was collected using an interviewer-administered structured questionnaire adapted from previous literature (14, 26, 27, 29), which contained socio-demographic, clinical, and lifestyle characteristics, stroke knowledge items, and stroke prevention practice items.
The knowledge section comprises 16 questions assessing the warning signs and risk factors related knowledge toward stroke with three possible responses: “Yes” or “No;” “I don't know;” and scores of 1 or 0 respectively. Participants who answered correctly to 16 stroke knowledge related questions, scored equal to or more than the mean value, were defined as having adequate stroke knowledge (27). The stroke prevention part consists of 9 questions with three possible responses: “Yes” or “No;” “I don't know;” and scores 1 or 0 respectively. Participants who answered 9 questions correctly or had a score greater than or equal to the mean score were considered to have good stroke prevention practice (27).
Usual Alcohol Consumption
A person who drinks alcohol on a regular basis (more than 6 days per week). According to World Health Organization (WHO) alcohol drinking guidelines, a woman should not drink more than two drinks per day, a man should not drink more than three drinks per day, and 1 day per week should be alcohol-free.
Physically Active
Participants engaged in moderate physical activity, including walking, for at least 150 min/week and fewer than 150 min/week were considered to be physically inactive (26).
Data Quality Assurance and Processing
The questionnaire was pretested on 5% of the sample size of hypertension patients who had follow-up at Felege Hiwot comprehensive specialized hospital. The questionnaire was modified to enhance the consistency of understanding by the respondents as well as by the data collector. The data was collected by 3 trained physiotherapists. The data collectors were trained by the primary investigator about the general purpose of the study and data collection procedures. The questionnaire was translated from English to Amharic by language experts, then translated back to English during data analysis.
Data Analysis
Data were cleaned, coded and entered Epi info version 7.2.1 and exported to SPSS version 23.0. Descriptive statistics were summarized in percentage and frequency. The statistical analysis using binary logistic regression was done to determine the candidate variables for multivariable logistic regression at p-value < 0.2. Then, variables having p-value < 0.05 at 95% in multivariable logistic regression were statistically significant.
Ethical Consideration
Ethical clearance was obtained from the ethical review committee of the school of medicine under the delegation of the University of Gondar Institutional review board. Before data collection, the purpose of this study, potential indirect benefit, and right to refuse were explained to each participant. After that, written informed consent is taken from each study participant. Information was recorded anonymously, and confidentiality was assured throughout the data collection.
Results
Socio Demographic Characteristics of Hypertensive Patients
Out of the total 424 study participants, 393 participated in the study, with a response rate of 92.7%. The age of the participants ranged from 27 to 93 years, with a mean age of 57.6 (SD 11.39) years. More than half of the participants were female, and nearly half of the participants were found between the ages of 50 and 65. The majority of the participants (71.5%) resided in the urban areas (Table 1).
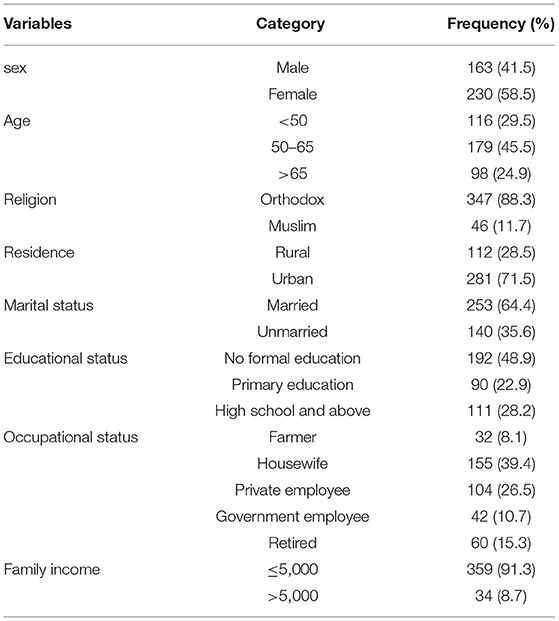
Table 1. Socio-demography of participants attending in chronic illness follow-up Clinic of University of Gondar Comprehensive Specialized Hospital, Northwest, Ethiopia, 2021 (n = 393).
Clinical and Behavioral Characteristics of Hypertensive Patients
Almost half (49.4%) of the participants had a history of hypertension for the last 5 years, and more than one third of the participants had concomitant diabetes mellitus. Nearly one third of the participants knew someone with one stroke and was physically active (Table 2).
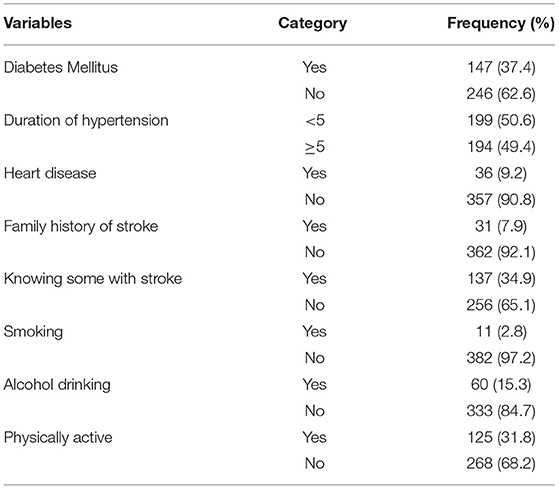
Table 2. Clinical and behavioral characteristics of participants attending in chronic illness follow-up Clinic of University of Gondar Comprehensive Specialized Hospital, Northwest, Ethiopia, 2021 (n = 393).
General Knowledge of Hypertensive Patients About Stroke
More than half of the participants 220 (56%) have never heard of stroke, and only a quarter of the participants 99 (25.2%) regraded stroke is a brain disease, while approximately 57 (14.5%) believed in homeopathic treatment for stroke. Some misconceptions have been observed, such as 21 (5%) believing that stroke was contagious, while 43 (10.9%) believed that it was caused by sin. Only 133 (33.8%) agreed that e stroke can be avoided. While one-third of 130 people (33.1%) accepted that stroke was a disease in the Elderly.
Knowledge of the Warning Signs of Stroke Among Hypertensive Patients
More than half the participants (58.1%) had no any stroke warning signs. The warning signs of stroke identified by one third of the participants (37.4%) as sudden onset of half body weakness, followed by sudden onset of loss of consciousness (27.7%), sudden onset of speech problems (22.4%), sudden onset of memory loss (19.4%), and sudden onset of double vision (18.6%) (Table 3).
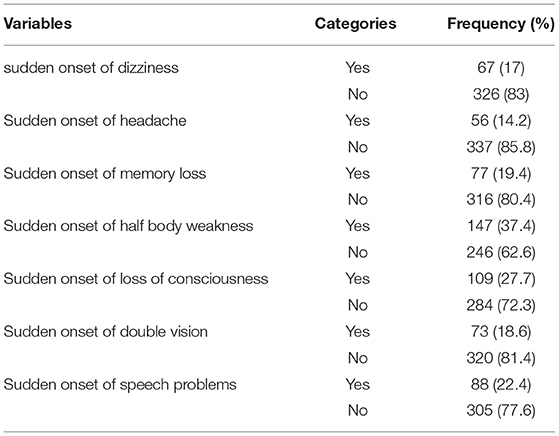
Table 3. Stroke warning sign/symptom of patients attending in chronic illness follow-up Clinic of University of Gondar Comprehensive Specialized Hospital, Northwest, Ethiopia, 2021 (n = 393).
Knowledge of Risk Factors of Stroke Among Hypertensive Patients
Nearly half of the participants (46.1%) didn't know any of the listed stroke risk factors. The common risk factors identified by the study participants were hypertension (48.1%), followed by alcohol consumption (38.2%), hypercholesterolemia (36.1%), physical inactivity (33.8%), obesity (33.3%), smoking (28%), and diabetes mellitus (23.2%) (Table 4).
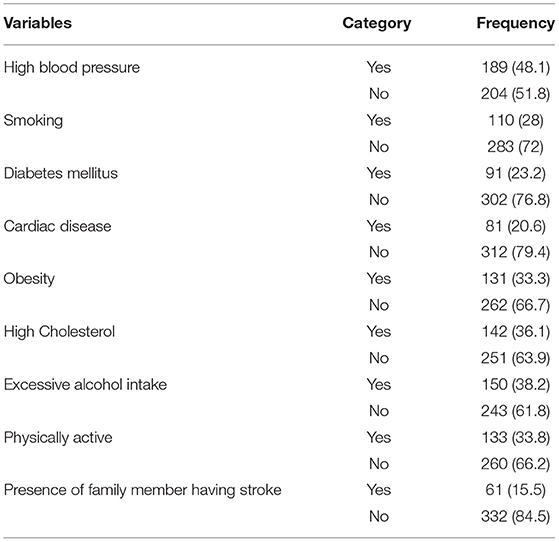
Table 4. Stroke risk factors of patients attending in chronic illness follow-up Clinic of University of Gondar Comprehensive Specialized Hospital, Northwest, Ethiopia, 2021 (n = 393).
Knowledge of Hypertensive Patients Toward Stroke
Out of 393 participants, 40.7% (160) (95% CI: 35.9, 45.5) of the study participants had adequate knowledge toward stroke warning signs and risk factors.
Prevention Practice of Hypertensive Patients Toward Stroke
In our study, 51.7% (95% CI: 46.8, 56.5) of the participants had good stroke prevention practice. The majority of the participants avoided or quite smoking and reduced alcohol consumption by 97.7 and 89.6%, respectively, whereas almost three-quarters of the participants reduced salt consumption (72%) and attended their regular clinic follow-up (75%). However, only 19.8% consumed fruits and vegetables, 36.6% engaged in regular physical activity, and 42.2% avoided fatty foods (Table 5).
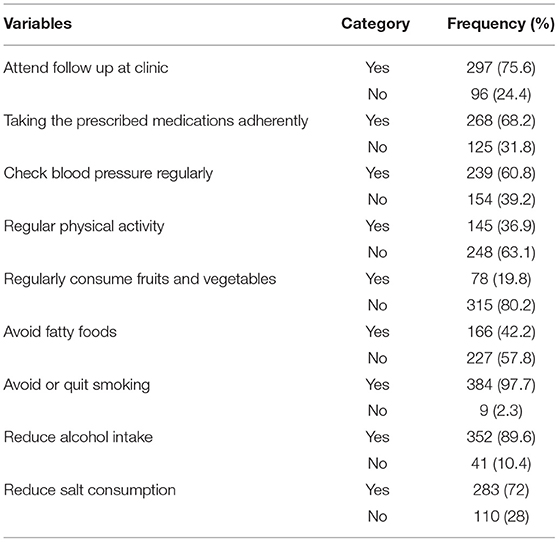
Table 5. Stroke prevention practice of patients attending in chronic illness follow-up Clinic of University of Gondar Comprehensive Specialized Hospital, Northwest, Ethiopia, 2021 (n = 393).
Factors Associated With Knowledge of Hypertensive Patients Toward Stroke
Sex, age, educational status, occupation, place of residence, household monthly income, knowing someone with stroke, and physical activity were entered into multivariable analysis. Adequate stroke knowledge was significantly associated with formal education, knowing someone with stroke and physical activity.
Educational status was directly related to stroke-related knowledge in hypertensive patients. Hypertensive patients with high school or above had 4.6 times the odds of having adequate stroke knowledge compared to those with no formal education [AOR = 4.6 (95% CI: 2.08, 10.17)]. Hypertensive patients who knew someone with a stroke had 13.17 times the odds of having adequate stroke knowledge compared to those hypertensive patients who didn't know anyone had a stroke [AOR = 13.17 (95% CI: 7.3, 23.77)]. Hypertensive patients who are physically active had 4.05 times the odds of having adequate stroke knowledge compared to those who are physically inactive [AOR = 4.05 (95% CI: 2.23, 7.37)] (Table 6).
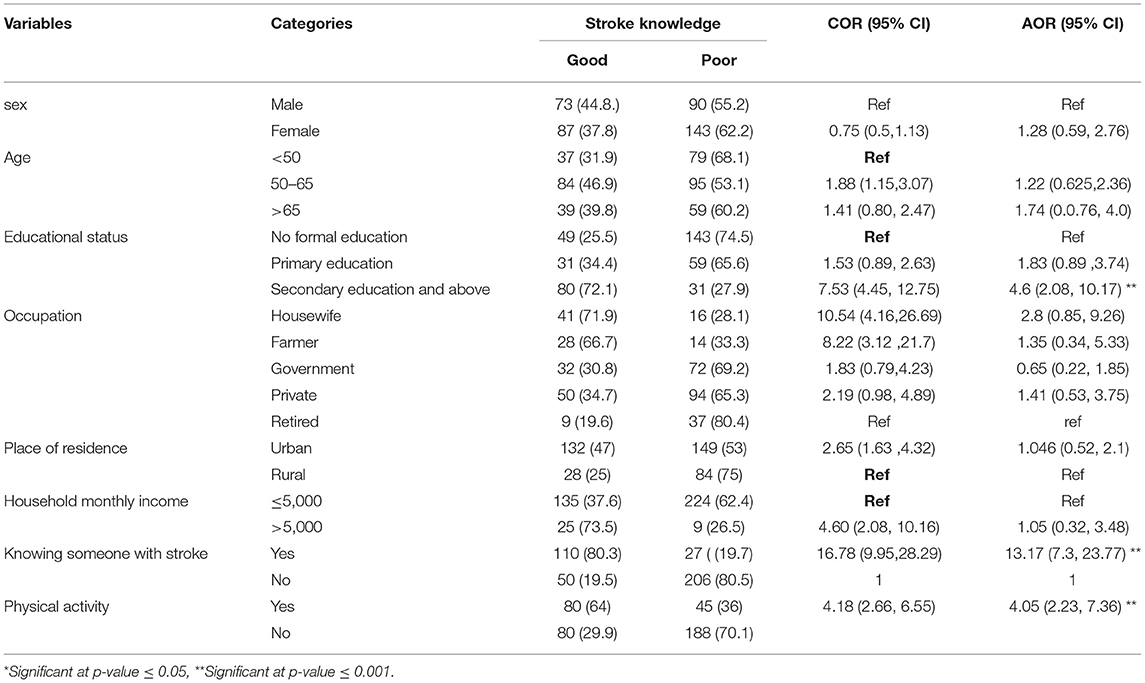
Table 6. Factors associated with stroke knowledge in hypertensive patients attending in chronic illness follow-up clinic of University of Gondar Comprehensive Specialized Hospital, Northwest, Ethiopia, 2021 (n = 393).
Factors Associated With Prevention Practice of Hypertensive Patients Toward Stroke
Like knowledge, multiple variables found to be affected the stroke prevention practice of hypertensive patients. Educational status, place of residence, duration of hypertension, knowing someone with stroke and physical activity were significantly associated with good stroke prevention practice in multivariable logistic regression.
Hypertensive patients with primary education [AOR = 2.61 (95% CI: 1.44, 4.73)] and secondary or higher education [AOR = 3.75 (95% CI: 1.99, 7.05)] had 2.61 times and 3.75 times respectively, the odds of engaging in good stroke prevention practices compared to hypertensive patients with no formal education. Hypertensive patients residing in urban areas had 9.65 times the odds of engaging in good stroke prevention practices compared to those living in rural areas [AOR = 9.65 (95% CI: 5.04, 18.44)]. Hypertensive patients who had <5 years of duration of hypertension had 1.9 times the odds of engaging in good stroke prevention practices compared to participants who had 5 year or above duration of hypertension (AOR = 1.9, 95% CI:1.15,3.14).
Hypertensive patients who knew someone with a stroke had 2.27 times the odds of engaging in good stroke prevention practices compared to those hypertensive patients who didn't know anyone had a stroke (AOR = 2.27:95% CI: 1.3, 3.93). Hypertensive patients who are physically active had 1.76 times the odds of engaging in good stroke prevention practices compared to those who are physically inactive (AOR = 1.76, 95% CI: 1.03, 3.01) (Table 7).
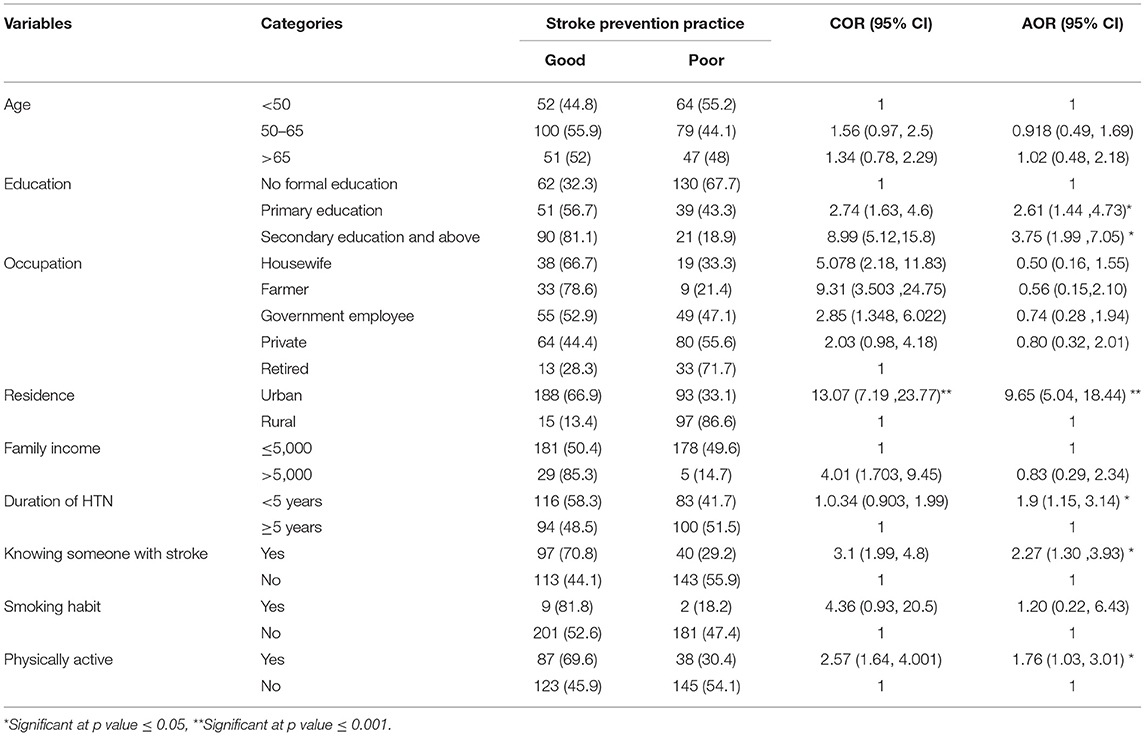
Table 7. Factors associated with stroke prevention practices in hypertensive patients attending in chronic illness follow-up clinic of University of Gondar Comprehensive Specialized Hospital, Northwest, Ethiopia, 2021 (n = 393).
Discussion
The study aimed to assess the knowledge of stroke, prevention practice and associated factors among patients with hypertension in the University of Gondar comprehensive specialized hospital, Gondar, Ethiopia.
The finding of this study revealed that more than one third of the participants (40.7%) had adequate knowledge about stroke, which is higher than the finding of previous studies in Ethiopia [Debre-Tabor, 24.9 % (27), 15% (28), Bahir dar, 18.3% (26)], and India, 24% (30). The possible explanation for differences in the prevalence of stroke knowledge among hypertensive patients could be the criteria used to define stroke knowledge. In the study done in Bahir Dar, the number of warning signs and risk factors mentioned were used to define adequate stroke knowledge, whereas in the study done in Debre Tabor, the stroke knowledge was measured by the stroke warning signs (28) and prevention practices (27) separately. However, this finding is lower than the study conducted in Nigeria 70.3%) (14), India, 66.7% (31). This could be due to a difference in the socio-demography of the study populations. One of the possible reasons might be the fact that only half of the participants in our study had formal education, whereas three-quarters of the participants in a study done in Nigeria had formal education.
More than half (51.7%) of the participants had good prevention practice for stroke. In contrast with the previous literature, a higher prevalence of good stroke prevention practice than stroke knowledge has been reported in our study. A possible explanation could be that hypertensive patients may be exposed to health education regarding common non-communicable diseases, including stroke, which have similar prevention practices, but they may not identify the specific prevention methods for stroke.
The most recognized warning signs of stroke in our study were the sudden occurrence of half body weakness, loss of consciousness, and speech problems. Participants also identified hypertension as a risk factor for stroke. Alcohol consumption and hypercholesterolemia were the subsequent risk factors identified. This is in agreement with the study done in Morocco where the most frequently identified warning signs and risk factors were sudden weakness of the arm, leg or face and hypertension, respectively (25).
In multivariable logistic regression analysis; higher educational status, knowing someone with stroke and being physically active were significantly associated with good stroke knowledge.
In the present study, education was significantly associated with having adequate stroke knowledge. Hypertensive patients who had secondary education, and above were more than four times more likely to have adequate stroke knowledge. This was concordant with the findings of a range of studies in which high educational level had been the most associated factor with adequate knowledge of stroke in hypertensive patients in Ethiopia (26, 28, 29), and Nigeria (14, 32) Morocco (25), and Beirut (33). This may be due to the fact that individuals who have a higher educational level may have more interaction with society and have easy access to health-related information from various sources like the internet, news, books, magazines, and literature as compared with individuals who have no formal education, which is supported by the systematic reviews reporting that educational status has a significant impact on cardiovascular disease knowledge in SSA populations (24, 34). Furthermore, a similar study conducted on the general population revealed that a low educational level is associated with poor stroke knowledge (35).
In this study, knowing someone with a stroke was one of the predictors of stroke knowledge among hypertensive patients. Those who knew someone who had a stroke were 13.17 times more likely than their counterparts to have adequate stroke-related knowledge. This is consistent with the findings of studies conducted in Addis Abeba, Ethiopia (36), Nigeria (32) and Morocco (25). However, this finding is inconsistent with the findings of a study conducted on hypertensive patients in Pakistan, which found that knowing someone who had a stroke was not associated with knowing about stroke risk factors or warning signs (37). The odds of hypertensive patients who knew someone who had a stroke were 2.27 times more likely to engage in good stroke prevention practice than those of hypertensive patients who didn't know anyone had a stroke. A possible explanation could be that family, friends and the community could be the primary sources of information regarding strokes. This is supported by the study done in South Asian populations, which found that lack of reliable sources of information was identified as a significant determinant factor for adequate knowledge of stroke.
This study revealed that the odds of physically active participants having adequate knowledge of stroke were 4.06 times higher compared to those who were physically inactive. Physically active participants were 1.76 times more likely than physically inactive participants to have adequate stroke preventive practices. Our findings are supported by the report from Hungary (38). A possible explanation could be that health-conscious people are more likely to engage in beneficial health behaviors like regular exercise because they tend to have a better understanding of their health, pay attention to individual health problems, and then take healthy measures to ensure their personal health. Having a higher educational level, being an urban resident, knowing someone with a stroke, and being physically active were significantly associated with good stroke prevention practice.
Participants with higher educational status were more likely to have good stroke prevention practice. Participants who completed primary and high school and above had a higher stroke prevention practice than study participants who had no formal education by 2.61 and 3.75, respectively. A similar finding was reported by a systematic review which reported that poor stroke prevention practices were related to low educational levels (24). The explanation could be that patients who have at least completed primary education may have a better chance of exposure to different communication media like magazines, leaflets, books, and the internet. The other predictor of stroke prevention practices was residence. Urban residences were 9.65 times more likely to have good stroke prevention practice than those in rural areas. This could explain why the majority of educated hypertensive patients live in cities.
Limitation of the Study
Since the study was institutional based and excluded hospitalized patients, generalization of the findings to the general population is limited; Also, since it was confined to a public hospital, hypertensive patients with higher economic status and education may have had follow-up at another private hospital and the study did not assess them. Furthermore, the study used close-ended questions. This might have limited the participant's responses regarding their knowledge and prevention practices. The hypertensive patient's attitudes toward stroke prevention were not assessed in this study.
Conclusion
The proportion of participants with good stroke-related knowledge and prevention practice was good. Being physically active, having a higher educational level, and knowing someone who has had a stroke were all significantly associated with adequate stroke knowledge. While, having a formal education, knowing someone with a stroke, being an urban dweller, having a short duration of hypertension, and being physically active were significantly associated with good stroke prevention practices.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethical Review Committee of the School of Medicine under the delegation of the University of Gondar Institutional Review Board. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
FKW contributed to the conception of the research, study design, data collection, data entering, analysis, interpretation of data, drafting the work, and writing and review of the manuscript. GAE contributed to the conception, study design, analysis, and writing and review of the manuscript. TK, WB, AKK, and YGG contributed to the study design, analysis, and review of the research. All the authors read and approved the final manuscript to be submitted for publication.
Funding
This research has been funded by the University of Gondar, Gondar, Ethiopia.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Feigin VL, Stark BA, Johnson CO, Roth GA, Bisignano C, Abady GG, et al. Global, regional, and national burden of stroke and its risk factors, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet Neurol. (2021) 20:795–820. doi: 10.1016/S1474-4422(21)00252-0
2. Global regional and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories 1990-2017: 1990-2017: a systematic analysis for the global burden of disease study 2017. Lancet. (2018) 392:1859–922. doi: 10.1016/S0140-6736(18)32335-3
3. Krishnamurthi RV, Ikeda T, Feigin VL. Global, regional and country-specific burden of ischaemic stroke, intracerebral haemorrhage and subarachnoid haemorrhage: a systematic analysis of the global burden of disease study 2017. Neuroepidemiology. (2020) 54:171–9. doi: 10.1159/000506396
4. Duncan PW, Bushnell C, Sissine M, Coleman S, Lutz BJ, Johnson AM, et al. Comprehensive stroke care and outcomes: time for a paradigm shift. Stroke. (2021) 52:385–93. doi: 10.1161/STROKEAHA.120.029678
5. Feigin VL, Krishnamurthi RV, Parmar P, Norrving B, Mensah GA, Bennett DA, et al. Update on the global burden of ischemic and hemorrhagic stroke in 1990-2013: the GBD 2013 study. Neuroepidemiology. (2015) 45:161–76. doi: 10.1159/000441085
6. Akinyemi RO, Brainin M. The African stroke organization - a new dawn for stroke in Africa. Nat Rev Neurol. (2021) 17:127–8. doi: 10.1038/s41582-021-00456-1
7. Kalkonde YV, Alladi S, Kaul S, Hachinski V. Stroke prevention strategies in the developing world. Stroke. (2018) 49:3092–7. doi: 10.1161/STROKEAHA.118.017384
8. Connor MD, Walker R, Modi G, Warlow CP. Burden of stroke in black populations in sub-Saharan Africa. Lancet Neurol. (2007) 6:269–78. doi: 10.1016/S1474-4422(07)70002-9
9. Gutefeldt K, Hedman CA, Thyberg ISM, Bachrach-Lindström M, Arnqvist HJ, Spångeus A. Disability and Rehabilitation. (2020). p. 1–7. doi: 10.1155/2020/4172635
10. Johnson W, Onuma O, Owolabi M, Sachdev S. Stroke: a global response is needed. Bull World Health Organ. (2016) 94:634–a. doi: 10.2471/BLT.16.181636
11. Baye M, Hintze A, Gordon-Murer C, Mariscal T, Belay GJ, Gebremariam AA, et al. Stroke characteristics and outcomes of adult patients in Northwest Ethiopia. Front Neurol. (2020) 11:428. doi: 10.3389/fneur.2020.00428
12. Zemed A, Nigussie Chala K, Azeze Eriku G, Yalew Aschalew A. Health-related quality of life and associated factors among patients with stroke at tertiary level hospitals in Ethiopia. PLoS ONE. (2021) 163:e0248481 doi: 10.1371/journal.pone.0248481
13. Warlow C, Sudlow C, Dennis M, Wardlaw J, Sandercock P. Stroke. Lancet. (2003) 362:1211–24. doi: 10.1016/S0140-6736(03)14544-8
14. Arisegi SA, Awosan KJ, Oche MO, Sabir AA, Ibrahim MT. Knowledge and practices related to stroke prevention among hypertensive and diabetic patients attending specialist hospital, Sokoto, Nigeria. Pan Afr Med J. (2018) 29:63. doi: 10.11604/pamj.2018.29.63.13252
15. Zeng Y, He GP, Yi GH, Huang YJ, Zhang QH, He LL. Knowledge of stroke warning signs and risk factors among patients with previous stroke or TIA in China. J Clin Nurs. (2012) 21:2886–95. doi: 10.1111/j.1365-2702.2012.04118.x
16. Stroebele N, Müller-Riemenschneider F, Nolte CH, Müller-Nordhorn J, Bockelbrink A, Willich SN. Knowledge of risk factors, and warning signs of stroke: a systematic review from a gender perspective. Int J Stroke. (2011) 6:60–6. doi: 10.1111/j.1747-4949.2010.00540.x
17. Kupferman JC, Zafeiriou DI, Lande MB, Kirkham FJ, Pavlakis SG. Stroke and hypertension in children and adolescents. J Child Neurol. (2017) 32:408–17. doi: 10.1177/0883073816685240
18. Alene M, Assemie MA, Yismaw L, Ketema DB. Magnitude of risk factors and in-hospital mortality of stroke in Ethiopia: a systematic review and meta-analysis. BMC Neurol. (2020) 20:309. doi: 10.1186/s12883-020-01870-6
19. Krishnamurthi RV, Barker-Collo S, Barber PA, Tippett LJ, Dalrymple-Alford JC, Tunnage B, et al. Community knowledge and awareness of stroke in New Zealand. J Stroke Cerebrovasc Dis. (2020) 29:104589. doi: 10.1016/j.jstrokecerebrovasdis.2019.104589
20. Shobha N, Buchan AM, Hill MD. Thrombolysis at 3-4. 5 hours after acute ischemic stroke onset–evidence from the Canadian alteplase for stroke effectiveness study (CASES) registry. Cerebrovasc Dis. (2011) 31:223–8. doi: 10.1159/000321893
21. Krishnamurthi RV, Feigin VL. 14 Global Burden of Stroke. Stroke E-Book: Pathophysiology, Diagnosis, and Management. (2021). p. 163. doi: 10.1016/B978-0-323-69424-7.00014-4
22. O'Donnell MJ, Xavier D, Liu L, Zhang H, Chin SL, Rao-Melacini P, et al. Risk factors for ischaemic and intracerebral haemorrhagic stroke in 22 countries (the INTERSTROKE study): a case-control study. Lancet. (2010) 376:112–23. doi: 10.1016/S0140-6736(10)60834-3
23. Mayosi BM, Lawn JE, van Niekerk A, Bradshaw D, Abdool Karim SS, Coovadia HM. Health in South Africa: changes and challenges since 2009. Lancet. (2012) 380:2029–43. doi: 10.1016/S0140-6736(12)61814-5
24. Melak AD, Wondimsigegn D, Kifle ZD. Knowledge, prevention practice and associated factors of stroke among hypertensive and diabetic patients–a systematic review. Risk Manag Healthc Policy. (2021) 14:3295. doi: 10.2147/RMHP.S324960
25. Kharbach A, Obtel M, Achbani A, Bouchriti Y, Hassouni K, Lahlou L, et al. Level of knowledge on stroke and associated factors: a cross-sectional study at primary health care centers in Morocco. Ann Global Health. (2020) 86:83. doi: 10.5334/aogh.2885
26. Abate AT, Bayu N, Mariam TG. Hypertensive patients' knowledge of risk factors and warning signs of stroke at felege hiwot referral hospital, Northwest Ethiopia: a cross-sectional study. Neurol Res Int. (2019) 2019:8570428. doi: 10.1155/2019/8570428
27. Tibebu NS, Emiru TD, Tiruneh CM, Nigat AB, Abate MW, Demelash AT. Knowledge on prevention of stroke and its associated factors among hypertensive patients at debre tabor general hospital: an institution-based cross-sectional study. Risk Manag Healthc Policy. (2021) 14:1681–8. doi: 10.2147/RMHP.S303876
28. Nigat AB, Abate MW, Demelash AT, Tibebu NS, Tiruneh CM, Emiru TD, et al. Knowledge on stroke warning signs and associated factors among hypertensive patients, Northwest Ethiopia: an institution-based cross-sectional study. Vasc Health Risk Manag. (2021) 17:721. doi: 10.2147/VHRM.S333394
29. Workina A, Kebede S, Fekadu C, Wubetie Snr A. Knowledge of risk factors and warning signs of stroke among patients with heart disease at Tikur Anbessa specialized hospital. Open Access Emerg Med. (2021) 13:57–66. doi: 10.2147/OAEM.S291648
30. Sinha R, Verma P, Rohilla KK, Kalyani CV. Hypertensive patients knowledge, attitude and practice for stroke prevention in Uttarakhand, India. Commun Med. (2020) 11:385–9. doi: 10.5455/njcm.20201002015318
31. Venkatesh U, Srivastava D. Knowledge, attitude and practice in relation to stroke: comparative study between hypertensive and non-hypertensive patients attending a tertiary care centre in Gorakhpur, Uttar Pradesh. India J Med Sci Clin Res. (2016) 4:15014–21. doi: 10.18535/jmscr/v4i12.116
32. Wahab KW, Kayode OO, Musa OI. Knowledge of stroke risk factors among Nigerians at high risk. J Stroke Cerebrovasc Dis. (2015) 24:125–9. doi: 10.1016/j.jstrokecerebrovasdis.2014.07.053
33. Khalil HM, Lahoud N. Knowledge of stroke warning signs, risk factors, and response to stroke among lebanese older adults in Beirut. J Stroke Cerebrovasc Dis. (2020) 29:104716. doi: 10.1016/j.jstrokecerebrovasdis.2020.104716
34. Boateng D, Wekesah F, Browne JL, Agyemang C, Agyei-Baffour P, Aikins Ad-G, et al. Knowledge and awareness of and perception towards cardiovascular disease risk in sub-Saharan Africa: a systematic review. PLoS ONE. (2017) 12:e0189264. doi: 10.1371/journal.pone.0189264
35. Chang T, Ibrahim S, Ranasinghe HM, Mihirini A, Weerasinghe D, Vithanage TDP, et al. Knowledge of stroke, its warning symptoms, risk factors and treatment among the general public and general practitioners in a South Asian population. J Stroke Cerebrovasc Dis. (2020) 29:104760. doi: 10.1016/j.jstrokecerebrovasdis.2020.104760
36. Bacha D, Abera H. Knowledge, attitude and self-care practice towards control of hypertension among hypertensive patients on follow-up at st. Paul's hospital, Addis Ababa. Ethiop J Health Sci. (2019) 29:421–30. doi: 10.4314/ejhs.v29i4.2
37. Dar NZ, Khan SA, Ahmad A, Maqsood S. Awareness of stroke and health-seeking practices among hypertensive patients in a tertiary care hospital: a cross-sectional survey. Cureus. (2019) 11:e4774. doi: 10.7759/cureus.4774
Keywords: stroke, knowledge, practice, hypertension, Ethiopia
Citation: Woldetsadik FK, Kassa T, Bilchut WH, Kibret Ak, Guadie YG and Eriku GA (2022) Stroke Related Knowledge, Prevention Practices and Associated Factors Among Hypertensive Patients at University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia, 2021. Front. Neurol. 13:839879. doi: 10.3389/fneur.2022.839879
Received: 20 December 2021; Accepted: 17 March 2022;
Published: 19 April 2022.
Edited by:
Jean-Claude Baron, University of Cambridge, United KingdomReviewed by:
Hui Jan Tan, National University of Malaysia, MalaysiaRiyadh K. Lafta, Al-Mustansiriya University, Iraq
Copyright © 2022 Woldetsadik, Kassa, Bilchut, Kibret, Guadie and Eriku. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Getachew Azeze Eriku, Z2V0YWNoZXdhemV6ZTQzQGdtYWlsLmNvbQ==