 Bettina Scheffler
Bettina Scheffler Florian Schimböck2
Florian Schimböck2 Jacob Spallek
Jacob Spallek Christian Kopkow
Christian Kopkow
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
STUDY PROTOCOL article
Front. Neurol., 27 July 2022
Sec. Neurorehabilitation
Volume 13 - 2022 | https://doi.org/10.3389/fneur.2022.828521
Objective: Evidence-based guidelines are important for informing clinical decision-making and improving patient outcomes. There is inconsistent usage of guidelines among physical therapists involved in stroke rehabilitation, suggesting the existence of a gap between theory and practice. Addressing the German guideline “evidence-based rehabilitation of mobility after stroke (ReMoS),” the aims of this project are (1) to describe the current physical therapy practice within the context of stroke rehabilitation in Germany, (2) to evaluate barriers and facilitators of guideline usage, (3) to develop, and (4) to pilot test a theory-based, tailored implementation intervention for the benefit of guideline recommendations.
Materials and Methods: This study uses a stepwise mixed methods approach for implementing a local guideline. A self-reported online questionnaire will be used to survey the current physical therapy practice in stroke rehabilitation. The same survey and systematic-mixed methods review will be used to evaluate the barriers and facilitators of guideline usage quantitatively. Semi-structured interviews will add a qualitative perspective on factors that influence ReMoS guideline implementation. The Behavior Change Wheel and Theoretical Domains Framework will be used to support the development of a tailored implementation intervention which will be pilot tested in a controlled study. Patient and physical therapy-related outcomes, as well as the appropriateness, such as acceptance and feasibility of the tailored implementation intervention, will be analyzed.
Conclusion: This will be the first endeavor to implement a guideline in German stroke rehabilitation with a focus on changing care provider behavior based on the knowledge of current practice and determining factors using a tailored and theory-based intervention.
In comparison with other diseases, mortality among people after stroke is the second highest of all causes in Europe and the world (1). Stroke typically occurs among older people, but its prevalence among younger adults is also rising (2–4). In the German population, about 2.5% of all adults have already suffered a stroke, and about 200,000 new cases occur every year (5–7). Among neurological disorders, stroke causes 41.2% of the global burden of diseases and is among the most common causes of long-term disability worldwide (8, 9). At about 28 billion euros, Germany contributes 63% of the total disease-related costs of stroke in Europe (10). For the affected individuals, stroke can result in multifaceted dysfunctions (11, 12) and can lead to an impaired physical and mental quality of life over the long term (13). In particular, limitations of motor skills often follow a stroke, and these are crucial for a dependent living with the disease (14, 15). Restoring mobility after stroke is a relevant rehabilitation goal for affected individuals, but only 53% of patients will be able to walk independently outdoors after a stroke (16–20).
Clinical guidelines are defined as “statements that include recommendations intended to optimize patient care. These statements are informed by a systematic review of evidence and an assessment of the benefits and costs of alternative care options” (21). Although guideline-based motor rehabilitation after stroke has been shown to be effective and important for those affected, physiotherapy has been found to deviate from the recommended practice (22–27). Possible reasons for non-adherence to guidelines in acute stroke rehabilitation may be related to healthcare professionals', patients', and healthcare institutions' characteristics, the complexity of some recommended therapies, or complexities in the guidelines themselves (28). In terms of the mobility of patients with stroke, Donnellan et al. noted that guidelines were not specific enough with regard to the performance of the recommended intervention (29). For the purposes of stroke rehabilitation, several guidelines have become available (30). Neurologists and physical therapists of the German Society of Neurorehabilitation (Deutsche Gesellschaft für Neurorehabilitation—DGNR) developed the interdisciplinary “rehabilitation of mobility after stroke (ReMoS)” guideline, which was first published in 2015 by the “Working Group of Scientific Medical Societies” (Arbeitsgemeinschaft Wissenschaftlicher Medizinischer Fachgesellschaften—AWMF) (31). According to the AWMF classification, the ReMoS guideline is considered an “S2e guideline” which implies that the guideline development process is based on a systematic literature search and a systematic selection and appraisal of the evidence. Considering the adverse events and the clinical applicability, the authors recommend therapy goal-directed interventions for improving walking ability, walking speed, walking distance, and the balance of individuals with sub-acute and chronic stroke (31). As the greatest potential for functional recovery in patients with stroke can be expected during the 1st months after disease onset (32), only recommendations for the sub-acute phase during the first 6 months are focused upon here (Supplementary Material 1).
Since the ReMoS guideline was disseminated via passive dissemination strategies, and as its publication was not supported by a specific implementation strategy, a gap between theory and practice is to be expected (33, 34). As such, the aims are (1) to describe the current physical therapy practice for stroke rehabilitation in Germany, (2) to evaluate barriers and facilitators of guideline usage, (3) to develop, and (4) to pilot test a theory-based implementation intervention for the benefit of ReMoS guideline recommendations.
This project is divided into four phases guided by the Behavior Change Wheel (BCW) and Theoretical Domains Framework (TDF), which yield a stepwise mixed methods approach to understand and facilitate the use of the ReMoS guideline (Figure 1).
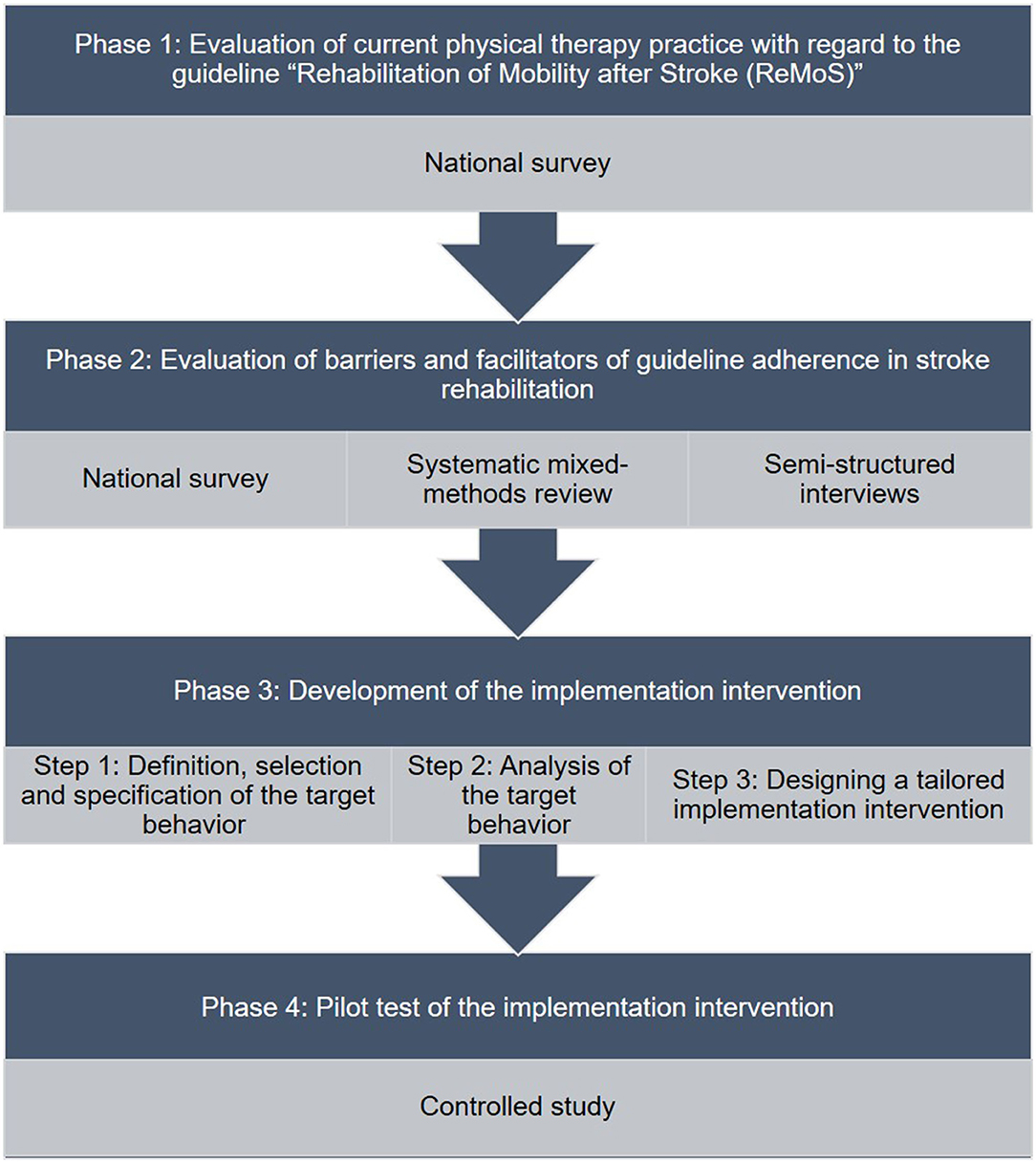
Figure 1. Flow chart of study phases.
Adoption of clinical practice guidelines by healthcare providers and behavioral changes toward their use is needed to ensure implementation of the guidelines. Theories and frameworks can facilitate the identification of determining factors and can guide the development of tailored implementation interventions. The selection of implementation frameworks should be based on empirical evidence, the applicability within a specific setting, explanatory power, and on the priorities of clinical practice and health policy (35, 36). Although BCW and TDF are comparatively new implementation frameworks, they have already been used to understand and promote adherence to guidelines in healthcare in general (37–39) and specifically within the field of neurorehabilitation (35, 40–42). Both aim to support behavioral changes among healthcare professionals and enable them to become involved in the whole process (43). The BCW was developed from 19 behavioral change frameworks for guiding diagnosis and intervention development with respect to behavioral problems. The core of the BCW forms the “capabilities, opportunities, and motivation—behavior (COM-B)” system (44). To acquire a deeper understanding of a behavior, the TDF, consisting of 14 domains (Knowledge; Skills; Social/Professional Role and Identity; Beliefs about Capabilities; Optimism; Beliefs about Consequences; Reinforcement; Intentions; Goals; Memory, Attention and Decision Processes; Environmental Context and Resources; Social Influences; Emotions; Behavioural regulation), was amended to the COM-B system (45). When a detailed understanding of the targeted behavior is assured, behavioral change techniques will be chosen from a matrix to design the tailored implementation intervention (46, 47).
An implementation shall eventually take place in the “Elbland Rehabilitationsklinik” in Großenhain, Germany (see Figure 1, Phase 3–4). This clinic is a part of the “Regional Working Group Reha Saxony” [Landesarbeitsgemeinschaft Reha Sachsen (LARS) e.V.] and provides capacity for up to 100 multidisciplinary rehabilitation and 25 weaning beds. Following acute care, people after stroke and other neurological diseases receive further care, as regulated by the Federal Working Group for Rehabilitation (Bundesarbeitsgemeinschaft für Rehabilitation, BAR) with regard to the severity of the disease and the rehabilitation goals (48).
Since the education of physical therapists in Germany is or has been mostly performed at vocational schools and not at higher education institutions, and since clinical decision-making depends on prescriptions from physicians, knowledge of and adherence to guidelines on the part of the physical therapist is assumed to be limited (49). A nationwide open, anonymous, online survey will be conducted to evaluate the current physical therapy practice in stroke rehabilitation in Germany, as well as to assess adherence to the ReMoS guideline recommendations and other related factors. The reporting of the survey methods and results shall follow the “Strengthening the Reporting of Observational Studies in Epidemiology (STROBE)” statement and the “Checklist for Reporting Results of Internet E-Surveys (CHERRIES)” (50, 51).
The survey will be prepared using the browser-based software “LimeSurvey” and shall consist of three sections with open and closed questions. The first section will include questions for the self-reported use of ReMoS guideline recommendations for the sub-acute phase after stroke, which are relevant to the field of action of physiotherapists. Participants shall rate the frequency of use of the recommended interventions as “never,” “sometimes,” “often,” and “always.” The second section shall relate to barriers and facilitators of guideline use on the basis of the “The Barriers and Facilitators Assessment Instrument” (52). In the third section, sociodemographic data shall be queried. The preliminary version will be drafted according to the recommendations by Dillman et al., and shall be reviewed by the study team and the ReMoS working group (53). Pretesting will be conducted using a convenient sample of physical therapists to check for technical functioning and feasibility using the cognitive technique known as “post-interview probing” (54). The survey will be open to (1) trained physical therapists, who (2) currently work in sub-acute stroke rehabilitation in Germany, and who have (3) sufficient reading and writing abilities in the German language. Information on the purpose and extent of the survey as well as the means of data storage shall be provided in advance. Participation will be voluntary, and no incentives shall be offered. If participants leave their e-mail address with the intention to participate in further study sections, these shall be stored separately from the survey data. To access the survey, every participant must approve written informed consent and self-reported eligibility criteria. An adaptive answering system shall be used to limit the burden on participants. Snowball sampling will be used to disseminate the access link to the online-survey via e-mail, a QR code, and social media. The data will be analyzed descriptively using R and R Studio version 1.0.143 (or newer versions of “The R Project for Statistical Computing,” Vienna, Austria) for all questionnaires that are answered at least in part (confirmation of the eligibility criteria and one further item). Each survey item will be analyzed using descriptive statistics as appropriate. Guideline adherence will be defined as 80% of the participants complying with the ReMoS guideline recommendations either “always” or “often” (55).
International insights to barriers and facilitators of guideline use in stroke rehabilitation will be acquired by conducting a systematic review according to the guideline for mixed methods systematic reviews from the Joanna Briggs Institute (JBI) (56). The trial registration number on PROSPERO is CRD42020160258. The “Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)” statement will guide the reporting of the review (57).
The aims of this review are (1) to synthesize barriers and facilitators of guideline adherent physical therapy and (2) to identify at which level physical therapy is performed according to clinical practice guidelines within the context of stroke rehabilitation. The Cochrane Database of Systematic Reviews, the Cochrane Central Register of Controlled Trials, MEDLINE/PubMed, the Physiotherapy Evidence Database (PEDro), and the Database of Research Into Stroke (DORIS) will all be screened for published studies. Additionally, study protocols will be searched in clinicalTrials.gov, clinicaltrialsregister.eu, and the German Clinical Trials Register. Studies published or registered in the English or German language are considered eligible for inclusion. Studies that will be included are (1) reports on physical therapy during inpatient or outpatient stroke rehabilitation, which (2) present barriers or facilitators of the guideline adherent to physical therapy (3) and/or refer to the level of physiotherapy guideline adherence as an outcome, or which feature either a qualitative or quantitative study design or a mixed methods design that allows a clear extraction of quantitative and qualitative components. Studies investigating the abovementioned outcomes during the acute phase after stroke will not be included. Eligible articles will be independently screened by two reviewers. If any disagreements occur, a third reviewer will be consulted. Full texts will be managed using the JBI “System for the Unified Management, Assessment and Review of Information (SUMARI)” (58). An adapted version of the “JBI Mixed Methods Data Extraction Form following a Convergent Integrated Approach” will be used. If there are any missing information, the corresponding author of the primary study will be contacted. Included studies will be appraised using the “Mixed Methods Appraisal Tool” (59). To analyze the primary outcome regarding barriers and facilitators, a convergent-integrated approach will be used. The above approach enables the synthesis and integration of quantitative and qualitative study results by converting quantitative data into a qualitative format (60).
Semi-structured interviews are used to provide a qualitative approach to acquiring additional understanding of the factors influencing the ReMoS guideline under the conditions of the German healthcare system. The reporting will follow the “Consolidated criteria for reporting qualitative research (COREQ)” paradigm (61).
A convenient sample of at least 10 physical therapists in Germany will be recruited by e-mail invitations given out to inpatient and outpatient rehabilitation facilities, via social media, on the website of a professional association, and via professional contacts. To gather a broad range of information, a diverse sample will be recruited with respect to gender, age, professional education level, duration of working experience, professional role, and healthcare setting (inpatient or outpatient rehabilitation). An interview guide will be drafted, revised by the study team, and pilot tested (Supplementary Material 2). The interviews will focus on factors influencing guideline usage in daily physical therapy practice and shall be conducted in the German language. Probing questions related to the TDF domains will be used to acquire further information. Interviews will be conducted either in a one-on-one setting, personally, or via phone/video call and shall take no longer than 45 min to complete. Participants shall receive and approve a written informed consent before taking part in the interviews and the interview guide shall also be provided in advance. The first author will conduct the interviews, unless it transpires that she has a personal relationship with the interviewees. All interviews shall be audio recorded and transcribed verbatim. Sociodemographic data shall be collected afterward. Data collection and storage shall be done pseudonymously. Transcripts from the interviews will be returned to the participants if desired for revision within 2 weeks. For data management and analysis, MAXQDA Analytics Pro (release 20.0.08 or later) shall be used. Inductive thematic analysis will be used to develop themes (62). Two team members shall carry out the initial coding of data from the first interview independently. The coding scheme shall be consented to and the first author shall code all the other interviews iteratively. Finally, the themes will be mapped against the TDF and shall be identified as barriers or facilitators with respect to ReMoS guideline usage.
Results from the earlier study components (survey, systematic-mixed methods review, and semi-structured interviews) shall lead to a list of candidate target behaviors, which might potentially influence the usage of the ReMoS guideline. Members of the “Elbland Rehabilitationsklinik” in Großenhain, Germany, the study team, and the ReMoS working group shall rank the candidate target behaviors independently as to whether they appear to be promising in terms of their impact on ReMoS guideline usage, their likelihood of being changed, their spillover effect on related behaviors, and whether they seem to be easily measurable. Out of the top-ranked candidate factors, one or two shall be chosen as target behavior(s). The target behavior(s) shall then be specified further (who, when, where, how often, and with whom, see Figure 1: Phase 3, Step 1).
Focus groups shall be queried to study target behavior(s) regarding their occurrence and to identify what needs to be changed within a specific setting (see Figure 1: Phase 3, Step 2). The reporting of this study component shall follow the “Consolidated criteria for reporting qualitative research (COREQ)” document (61).
Two to three focus groups with 6–10 participants taken from a relevant sample of, e.g., management, administration, and health professionals of the “Elbland Rehabilitationsklinik,” shall be implemented (63). Participants who shall be sought are (1) ≥18 years old and (2) directly or indirectly involved in the target behavior(s). Mixed groups shall be invited to promote diversity and represent a wide range of opinions/information levels and to keep the burden for the clinicians as low as possible. The moderated focus groups shall be queried during the working hours in the clinic environment on the basis of a semi-structured discussion guide. The guide shall be developed with open-ended questions to determine what needs to be changed regarding the target behavior. The focus groups shall be audio recorded and a member of the study team shall make field notes. All participants shall receive and approve a written informed consent before taking part in the group discussion and shall be asked to provide sociodemographic information. The focus group discussions shall be transcribed and managed using the software MAXQDA Analytics Pro (release 20.0.08 or later). Thematic analyses shall spawn themes according to the TDF, and the results shall allow a “behavior diagnosis” to assist in the development of a tailored implementation intervention to improve the use of the ReMoS guideline (62).
The development process for the tailored implementation intervention shall be undertaken according to the BCW guidance and in close collaboration between stakeholders of “Elbland Rehabilitationsklinik” and the study team (see Figure 1: Phase 3, Step 3).
Regarding the Affordability, Practicability, (cost-) Effectiveness, Acceptability, Side-effects/Safety and Equity (APEASE) criteria, appropriate intervention functions (e.g., education, environmental restructuring, enablement, feedback, persuasion, or training) to address findings from focus groups shall be selected in discussions (44). Since an intervention design at the policy level is beyond the scope of this project, policy categories shall not be considered to be relevant as recommended by the BCW guidance. Most appropriate behavior change techniques (e.g., feedback regarding behavior, verbal persuasion, or social support) that match the selected intervention functions shall be selected from the Behavior Change Theory Taxonomy, v1 (BCTTV1) after appraisal consistent with the APEASE criteria (44). Finally, the mode of delivery (e.g., via face-to-face or remote mode, individual or group mode) shall be chosen. The reporting of the final implementation intervention shall follow a structured scheme (64).
A controlled study design will aim to evaluate the effectiveness, appropriateness, acceptability, and feasibility of both the tailored implementation intervention and the implementation process in order to improve ReMoS guideline usage (65). The trial was registered on the German Clinical Trials Register with the number DRKS00019024. The reporting of this study will follow the “Standards for Reporting Implementation Studies (StaRI)” statement (66).
Routine practice shall be monitored in a single-center design in the “Elbland Rehabilitationsklinik” over a control period of 6 months. During this time, healthcare professionals shall not receive any instructions to change their habits or follow the ReMoS guideline recommendations any differently than they had before. Afterward, the implementation phase including the tailored implementation intervention shall be carried out (6 weeks). This will then be followed by a further monitoring period of 6 months. The implementation intervention shall be provided to all therapists involved in motor rehabilitation, regardless of whether they participate in the study.
Healthcare professionals shall be eligible for participation if they are (1) ≥18 years old, (2) trained therapists providing motor rehabilitation, and (3) continuously employed during the study period. Patients will be eligible to participate if they are (1) ≥18 years old, (2) diagnosed primarily with stroke, and (3) having improvement in mobility as one of their activity-related rehabilitation goals. Reasons for exclusion include other diseases of organ systems that negatively impact on motor rehabilitation (e.g., other severe neurological or musculoskeletal conditions, acute renal or cardiac diseases and other pre-existing disorders that potentially reduce the rehabilitation potential). A study nurse shall screen patients for eligibility. Written informed consent shall be provided and approved before the start of the study for each participant. Primary implementation outcomes will be the German versions of the Acceptability of Intervention Measure (AIM), the Intervention Appropriateness Measure (IAM), the Feasibility of Intervention Measure (FIM), and ReMoS guideline adherence (healthcare professional level) (67). Secondarily recommended core-outcomes will be used for further evaluation at the patient level within 1 week after the start of rehabilitation, at the week of discharge, and 6 months after discharge for the health-related quality of life among people with stroke (PROMIS® Scale v1.2 - Global Health) (68–70). Recruitment and retention rate as well as compliance with the intervention protocol shall be evaluated at the study feasibility level (71). As the present study represents a pilot study for testing the feasibility, acceptability, applicability, and possible effectiveness of a targeted implementation intervention, the number of cases required to determine significant effects has not been determined beforehand. Data analysis as well as the blinding of patients, healthcare providers, and assessors will not be possible because of the controlled before-after experimental design and the active intervention measures. In order to reduce the risk of systematic bias, staff and patients will only be informed in detail about the content and objectives of the implementation study if this is explicitly requested (72). A between-group analysis will be used to evaluate pre-post changes to indicate whether the intervention is successful with regard to the primary healthcare professional and patient outcome.
Studies have been conducted both internationally and in Germany on the implementation of the guidelines for and changes to stroke rehabilitation, although with uncertain effects (73–76). Although the ReMoS guideline was first published in 2015, knowledge of the guideline is lacking in Germany, as is its usage. Since the release of the guideline was not accompanied by a tailored dissemination or implementation strategy, this project aims to pilot test a tailored implementation intervention for the purposes of promoting this guideline.
As we attempt to implement the ReMoS guideline, our first task is to explore current physical therapy practice and to describe a hypothetical rift between guideline recommendations and current clinical practice. Based on a comprehensive study of determining factors, where multiple methods have been used, a tailored theory-based implementation intervention is to be designed in close collaboration with stakeholders. This will be done using the BCW guide (44) and will be tested in a controlled study for feasibility and possible effects on clinical practice and patient outcomes.
As a restricted implementation of recommended interventions can contribute toward avoidable disabilities and indeed harm (77), guideline implementation is relevant for any health condition (78, 79) and for any healthcare profession (80, 81). Barriers to guideline-compliant practice have been found to be individual, external, or guideline related, and these have been studied both in general (82–84) and in specific circumstances (85, 86). Knowledge of existing barriers, as well as the use of theoretical underpinning of behavioral change, is recommended to develop promising strategies for addressing the factors that determine guideline adherence (87). Even so, different frameworks are used in healthcare implementation research (88, 89), meaning heterogeneous results have been observed regarding effectiveness (90–92). With regard to physical therapy practice specifically, multifaceted and tailored interventions seem to be the most promising types (43, 93, 94).
The BCW and TDF have been successfully applied to develop and tailor implementation interventions by healthcare professionals in the context of stroke rehabilitation (41, 42, 95, 96). Two recent studies from Australia have given grounds for optimism regarding the design of tailored interventions, guided by the BCW and TDF in the field of guideline implementation of stroke rehabilitation. Both studies reported the feasibility and acceptance of the intervention and Jolliffe et al. cited a possible effect on guideline adherence in the hands of occupational and physical therapists (75, 97).
Neurorehabilitation services in Germany differ from others both in Europe and the world, which will probably impact on current practice, perceived barriers, and facilitators, the applicability of the implementation intervention, and the transferability of our results. The reasons underlying this might lie with the specifics of the respective rehabilitation systems and the comparatively low proportion of academically trained physiotherapists in Germany (98).
Despite the effort we expended on selecting the theoretical underpinnings, issues might still arise. Both the BCW and the TDF are validated and commonly used in implementation research, but to date, only the BCTTV1 has been translated into German (47). Here, a systematic procedure is used, but subjective and pragmatic decisions are still required. Further issues might also arise due to the design of the study components, since results rely in part on self-reported data and on limited blinding modalities and are subject to possible contamination.
The project outlined here will be the first to a use a behavioral change approach to promote guideline adherent practice among healthcare professionals working in stroke rehabilitation in Germany. We will gain an understanding of ReMoS guideline usage, the factors that determine usage, and the feasibility of a tailored implementation intervention to change clinical practice. In addition, this project shall also inform recruitment, retention, and the power of future studies to evaluate the actual effect of the intervention using a randomized study design. Understanding of current practice and theory will guide this project toward implementing a local guideline in an inpatient stroke rehabilitation setting. This study shall provide information on the feasibility of a tailored implementation intervention, possible outcomes for clinical practice and patients, and the realization of future effectiveness studies.
All authors have contributed to the study concept and design. BS and CK conceived the study, substantially contributed to the development of the study design, have given relevant intellectual input, and drafted the manuscript. AS, KR, FS, and JS gave input relating to the development of the study design. All authors read, improved, and approved the final manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors respectfully acknowledge the past and present support by the members of the ReMoS working group of the Deutsche Gesellschaft für Neurorehabilitation e.V., namely Christian Dohle, Jochen Quintern, Susanne Saal, Klaus Martin Stephan, Reina Tholen, and Heike Wittenberg.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2022.828521/full#supplementary-material
AIM, Acceptability of Intervention Measure; APEASE, Affordability, Practicability, (cost-) Effectiveness, Acceptability, Side-effects/Safety and Equity; AWMF, Arbeitsgemeinschaft Wissenschaftlicher Medizinischer Fachgesellschaften; BAR, Bundesarbeitsgemeinschaft für Rehabilitation; BCW, Behavior Change Wheel; BCTTV1, Behavior Change Theory Taxonomy (v1); CHERRIES, Checklist for Reporting Results of Internet E-Surveys; COM-B, Capabilities, Opportunities and Motivation-Behavior; COREQ, Consolidated criteria for reporting qualitative research; DGNR, Deutsche Gesellschaft für Neurorehabilitation; DORIS, Database of Research Into Stroke; FIM, Feasibility of Intervention Measure; IAM, Intervention Appropriateness Measure; JBI, Joanna Briggs Institute; LARS, Landesarbeitsgemeinschaft Reha Sachsen; PEDro, Physiotherapy Evidence Database; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; PROMIS, Patient-Reported Outcomes Measurement Information System; ReMoS, Rehabilitation of Mobility after Stroke; StaRI, Standards for Reporting Implementation Studies; STROBE, Strengthening the Reporting of Observational Studies in Epidemiology; SUMARI, System for the Unified Management, Assessment and Review of Information; TDF, Theoretical Domains Framework.
1. World Health Organization. Global Health Estimates 2016: Deaths by Cause, Age, Sex, by Country and by Region, 2000-2016. Geneva: World Health Organization (2018).
2. Bejot Y, Bailly H, Durier J, Giroud M. Epidemiology of stroke in Europe and trends for the 21st century. Presse Medicale. (1983) 45:e391–e8. doi: 10.1016/j.lpm.2016.10.003
3. Ekker MS, Verhoeven JI, Vaartjes I, van Nieuwenhuizen KM, Klijn CJM, de Leeuw FE. Stroke incidence in young adults according to age, subtype, sex, and time trends. Neurology. (2019) 92:e2444–e54. doi: 10.1212/WNL.0000000000007533
4. Thrift AG, Thayabaranathan T, Howard G, Howard VJ, Rothwell PM, Feigin VL, et al. Global stroke statistics. Int J Stroke. (2017) 12:13–32. doi: 10.1177/1747493016676285
5. Busch M, Kuhnert R. 12-Month prevalence of stroke or chronic consequences of stroke in Germany. J Health Monitor. (2017) 2:64–9. doi: 10.17886/RKI-GBE-2017-019
6. Thiele I, Linseisen J, Heier M, Holle R, Kirchberger I, Peters A, et al. Time trends in stroke incidence and in prevalence of risk factors in Southern Germany, 1989 to 2008/09. Sci Rep. (2018) 8:11981. doi: 10.1038/s41598-018-30350-8
7. Robert-Koch-Institut. Wie steht es um unsere Gesundheit? Berlin: Robert Koch-Institut, Epidemiologie und Gesundheitsberichterstattung (2015). doi: 10.17886/rkipubl-2015-003-2
8. GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet. (2018) 392:1789–858. doi: 10.1016/S0140-6736(18)32279-7
9. Wafa HA, Wolfe CDA, Emmett E, Roth GA, Johnson CO, Wang Y. Burden of stroke in Europe: thirty-year projections of incidence, prevalence, deaths, and disability-adjusted life years. Stroke. (2020) 51:2418–27. doi: 10.1161/STROKEAHA.120.029606
10. Luengo-Fernandez R, Violato M, Candio P, Leal J. Economic burden of stroke across Europe: a population-based cost analysis. Eur Stroke J. (2020) 5:17–25. doi: 10.1177/2396987319883160
11. Corbetta M, Ramsey L, Callejas A, Baldassarre A, Hacker CD, Siegel JS, et al. Common behavioral clusters and subcortical anatomy in stroke. Neuron. (2015) 85:927–41. doi: 10.1016/j.neuron.2015.02.027
12. Feigin VL, Vos T, Nichols E, Owolabi MO, Carroll WM, Dichgans M, et al. The global burden of neurological disorders: translating evidence into policy. Lancet Neurol. (2020) 19:255–65. doi: 10.1016/S1474-4422(19)30411-9
13. Crichton SL, Bray BD, McKevitt C, Rudd AG, Wolfe CD. Patient outcomes up to 15 years after stroke: survival, disability, quality of life, cognition and mental health. J Neurol Neurosurg Psychiatry. (2016) 87:1091–8. doi: 10.1136/jnnp-2016-313361
14. Langhorne P, Coupar F, Pollock A. Motor recovery after stroke: a systematic review. Lancet Neurol. (2009) 8:741–54. doi: 10.1016/S1474-4422(09)70150-4
15. Cohen JW, Ivanova TD, Brouwer B, Miller KJ, Bryant D, Garland SJ. Do performance measures of strength, balance, and mobility predict quality of life and community reintegration after stroke? Arch Phys Med Rehabil. (2018) 99:713–9. doi: 10.1016/j.apmr.2017.12.007
16. Harris JE, Eng JJ. Goal priorities identified through client-centred measurement in individuals with chronic stroke. Physiotherapy Canada. (2004) 56:171–6. doi: 10.2310/6640.2004.00017
17. Lord SE, McPherson K, McNaughton HK, Rochester L, Weatherall M. Community ambulation after stroke: how important and obtainable is it and what measures appear predictive? Arch Phys Med Rehabil. (2004) 85:234–9. doi: 10.1016/j.apmr.2003.05.002
18. Pollock A, Baer G, Campbell P, Choo PL, Forster A, Morris J, et al. Physical rehabilitation approaches for the recovery of function and mobility following stroke. Cochr Database Systemat Rev. 2014:Cd001920. doi: 10.1002/14651858.CD001920.pub3
19. Rudberg AS, Berge E, Laska AC, Jutterström S, Näsman P, Sunnerhagen KS, et al. Stroke survivors' priorities for research related to life after stroke. Top Stroke Rehabil. (2021) 28:153–8. doi: 10.1080/10749357.2020.1789829
20. Shum ST, Chiu JK, Tsang CP, Wong CH, Tsang RC, Ma SL, et al. Predicting walking function of patients one month poststroke using modified Rivermead mobility index on admission. J Stroke Cerebrovasc Dis. (2014) 23:2117–21. doi: 10.1016/j.jstrokecerebrovasdis.2014.03.023
21. Institute of Medicine. Clinical practice guidelines we can trust. In: Graham R, Mancher M, Wolman DM, Greenfield S, Steinberg E, editors, Washington, DC: The National Academies Press (2011). p. 290.
22. Ajimsha MS, Kooven S, Al-Mudahka N. Adherence of physical therapy with clinical practice guidelines for the rehabilitation of stroke in an active inpatient setting. Disabil Rehabil. (2019) 41:1855–62. doi: 10.1080/09638288.2018.1449257
23. Johnston J, Mudge S, Kersten P, Jones A. Physiotherapy alignment with guidelines for the management of stroke in the inpatient setting. N Zeal J Physiother. (2013) 41:102–11.
24. Otterman NM, van der Wees PJ, Bernhardt J, Kwakkel G. Physical therapists' guideline adherence on early mobilization and intensity of practice at dutch acute stroke units: a country-wide survey. Stroke. (2012) 43:2395–401. doi: 10.1161/STROKEAHA.112.660092
25. English C, Bayley M, Hill K, Langhorne P, Molag M, Ranta A, et al. Bringing stroke clinical guidelines to life. Int J Stroke. (2019) 14:337–9. doi: 10.1177/1747493019833015
26. Eng JJ, Bird ML, Godecke E, Hoffmann TC, Laurin C, Olaoye OA, et al. Moving stroke rehabilitation research evidence into clinical practice: consensus-based core recommendations from the Stroke Recovery and Rehabilitation Roundtable. Int J Stroke. (2019) 2019:1747493019873597. doi: 10.1177/1747493019873597
27. Pogrebnoy D, Dennett A. Exercise programs delivered according to guidelines improve mobility in people with stroke: a systematic review and meta-analysis. Arch Phys Med Rehabil. (2019). doi: 10.1016/j.apmr.2019.06.015
28. Baatiema L, Otim ME, Mnatzaganian G, de-Graft Aikins A, Coombes J, Somerset S. Health professionals' views on the barriers and enablers to evidence-based practice for acute stroke care: a systematic review. Implement Sci. (2017) 12:74. doi: 10.1186/s13012-017-0599-3
29. Donnellan C, Sweetman S, Shelley E. Health professionals' adherence to stroke clinical guidelines: a review of the literature. Health Policy. (2013) 111:245–63. doi: 10.1016/j.healthpol.2013.05.002
30. Platz T. Evidence-based guidelines and clinical pathways in stroke rehabilitation-an international perspective. Front Neurol. (2019) 10:200. doi: 10.3389/fneur.2019.00200
31. Saal DQ, Wittenberg ST. S2e-Leitlinie ≫Rehabilitation der Mobilität nach Schlaganfall (ReMoS)≪ Kurzfassung der Konsensusversion. Neurol Rehabil. (2015) 21:179–84. doi: 10.14624/NR201509.001
32. Smith MC, Byblow WD, Barber PA, Stinear CM. Proportional recovery from lower limb motor impairment after stroke. Stroke. (2017) 48:1400–3. doi: 10.1161/STROKEAHA.116.016478
33. Grimshaw JM, Thomas RE, MacLennan G, Fraser C, Ramsay CR, Vale L, et al. Effectiveness and efficiency of guideline dissemination and implementation strategies. Health Technol Assess. (2004) 8:1–72. doi: 10.3310/hta8060
34. Grol R. Successes and failures in the implementation of evidence-based guidelines for clinical practice. Medical Care. (2001) 39(8 Suppl 2):Ii46-54. doi: 10.1097/00005650-200108002-00003
35. Birken SA, Powell BJ, Shea CM, Haines ER, Alexis Kirk M, Leeman J, et al. Criteria for selecting implementation science theories and frameworks: results from an international survey. Implement Sci. (2017) 12:124. doi: 10.1186/s13012-017-0656-y
36. Wensing M, Oxman A, Baker R, Godycki-Cwirko M, Flottorp S, Szecsenyi J, et al. Tailored Implementation For Chronic Diseases (TICD): a project protocol. Implement Sci. (2011) 6:103. doi: 10.1186/1748-5908-6-103
37. Jolliffe L, Hoffmann T, Lannin NA. Increasing the uptake of stroke upper limb guideline recommendations with occupational therapists and physiotherapists. A qualitative study using the Theoretical Domains Framework. Austr Occup Ther J. (2019) 2019:12599. doi: 10.1111/1440-1630.12599
38. Murphy K, O'Connor DA, Browning CJ, French SD, Michie S, Francis JJ, et al. Understanding diagnosis and management of dementia and guideline implementation in general practice: a qualitative study using the theoretical domains framework. Implement Sci. (2014) 9:31. doi: 10.1186/1748-5908-9-31
39. Shrubsole K, Worrall L, Power E, O'Connor DA. Barriers and facilitators to meeting aphasia guideline recommendations: what factors influence speech pathologists' practice? Disabil Rehabil. (2019) 41:1596–607. doi: 10.1080/09638288.2018.1432706
40. Lynch EA, Mudge A, Knowles S, Kitson AL, Hunter SC, Harvey G. “There is nothing so practical as a good theory”: a pragmatic guide for selecting theoretical approaches for implementation projects. BMC Health Serv Res. (2018) 18:857. doi: 10.1186/s12913-018-3671-z
41. Connell LA, McMahon NE, Redfern J, Watkins CL, Eng JJ. Development of a behaviour change intervention to increase upper limb exercise in stroke rehabilitation. Implement Sci. (2015) 10:34. doi: 10.1186/s13012-015-0223-3
42. Loft MI, Martinsen B, Esbensen BA, Mathiesen LL, Iversen HK, Poulsen I. Strengthening the role and functions of nursing staff in inpatient stroke rehabilitation: developing a complex intervention using the Behaviour Change Wheel. Int J Qual Stud Health Well-being. (2017) 12:1392218. doi: 10.1080/17482631.2017.1392218
43. Prior M, Guerin M, Grimmer-Somers K. The effectiveness of clinical guideline implementation strategies–a synthesis of systematic review findings. J Eval Clin Pract. (2008) 14:888–97. doi: 10.1111/j.1365-2753.2008.01014.x
44. Michie S, Atkins L, West R. The Behaviour Change Wheel. A Guide To Designing Interventions. London: Silverback Publishing (2014).
45. Cane J, O'Connor D, Michie S. Validation of the theoretical domains framework for use in behaviour change and implementation research. Implement Sci. (2012) 7:37. doi: 10.1186/1748-5908-7-37
46. Michie S, Richardson M, Johnston M, Abraham C, Francis J, Hardeman W, et al. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: building an international consensus for the reporting of behavior change interventions. Ann Behav Med. (2013) 46:81–95. doi: 10.1007/s12160-013-9486-6
47. Göhner W, Küffner R, Schagg D, Faller H, Reush A. Behavior Change Techniques Taxonomy version 1 –Deutsche Übersetzung der Taxonomie von Michie et al., 2013. (2016). Available online at: www.zentrum-patientenschulung.de
48. Schupp W. Konzept einer zustands- und behinderungsangepassten Behandlungs- und Rehabilitationskette in der neurologischen und neurochirurgischen Versorgung in Deutschland (“Phasenmodell”). Nervenarzt. (1995) 66:907–14.
49. Konrad R, Konrad A, Geraedts M. [Physiotherapy Education in Germany: Ready for Direct Access?] Gesundheitswesen. Bundesverband der Arzte des Offentlichen Gesundheitsdienstes. (2017) 79:e48–55. doi: 10.1055/s-0035-1559708
50. Eysenbach G. Improving the quality of Web surveys: the Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J Med Internet Res. (2004) 6:e34. doi: 10.2196/jmir.6.3.e34
51. von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: guidelines for reporting observational studies. Int J Surg. (2014) 12:1495–9. doi: 10.1016/j.ijsu.2014.07.013
52. Peters MAJ, Harmsen M, Laurant MGH, Wensing M. Ruimte voor verandering? Knelpunten en mogelijkheden voor verandering in de patiëntenzorg [Room for improvement? Barriers to and facilitators for improvement of patient care] Nijmengen: Centre for Quality of Care Research (WOK). Radboud: University Nijmegen Medical Centre. (2002).
53. Christian DS. Internet, Phone, Mail, and Mixed-Mode Surveys: The Tailored Design Method. Hoboken, NJ: John Wiley & Sons (2014).
54. Willis GB, Artino AR Jr. What do our respondents think we're asking? using cognitive interviewing to improve medical education surveys. J Graduate Medical Educ. (2013) 5:353–6. doi: 10.4300/JGME-D-13-00154.1
55. Bahns C, Happe L, Thiel C, Kopkow C. Physical therapy for patients with low back pain in Germany: a survey of current practice. BMC Musculoskelet Disord. (2021) 22:563. doi: 10.1186/s12891-021-04422-2
56. Lizarondo L, Stern C, Carrier J, Godfrey C, Rieger K, Salmond S, et al. Chapter 8: Mixed methods systematic reviews. In: Aromataris E, Munn Z, editors, Joanna Briggs Institute Reviewer's Manual. Adelaide, SA: The Joanna Briggs Institute (2017). Available online at: https://reviewersmanual.joannabriggs.org/ (accessed December 2021).
57. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. (2009) 6:e1000097. doi: 10.1371/journal.pmed.1000097
58. Munn Z, Aromataris E, Tufanaru C, Stern C, Porritt K, Farrow J, et al. The development of software to support multiple systematic review types: the Joanna Briggs Institute System for the Unified Management, Assessment and Review of Information (JBI SUMARI). Int J Evid Based Healthc. (2019) 17:36–43. doi: 10.1097/XEB.0000000000000152
59. Hong QN, Gonzalez-Reyes A, Pluye P. Improving the usefulness of a tool for appraising the quality of qualitative, quantitative and mixed methods studies, the Mixed Methods Appraisal Tool (MMAT). J Eval Clin Pract. (2018) 24:459–67. doi: 10.1111/jep.12884
60. Stern C, Lizarondo L, Carrier J, Godfrey C, Rieger K, Salmond S, et al. Methodological guidance for the conduct of mixed methods systematic reviews. JBI Evid Synth. (2020) 18:2108–18. doi: 10.11124/JBISRIR-D-19-00169
61. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. (2007) 19:349–57. doi: 10.1093/intqhc/mzm042
62. Clarke V, Braun V. Successful Qualitative Research: A Practical Guide for Beginners. Newcastle upon Tyne: Sage (2013).
63. Guest G, Namey E, McKenna K. How many focus groups are enough? Building an evidence base for nonprobability sample sizes. Field Methods. (2017) 29:3–22. doi: 10.1177/1525822X16639015
64. Proctor EK, Powell BJ, McMillen JC. Implementation strategies: recommendations for specifying and reporting. Implement Sci. (2013) 8:139. doi: 10.1186/1748-5908-8-139
65. Curran GM, Bauer M, Mittman B, Pyne JM, Stetler C. Effectiveness-implementation hybrid designs: combining elements of clinical effectiveness and implementation research to enhance public health impact. Med Care. (2012) 50:217–26. doi: 10.1097/MLR.0b013e3182408812
66. Pinnock H, Barwick M, Carpenter CR, Eldridge S, Grandes G, Griffiths CJ, et al. Standards for Reporting Implementation Studies (StaRI): explanation and elaboration document. BMJ Open. (2017) 7:e013318. doi: 10.1136/bmjopen-2016-013318
67. Weiner BJ, Lewis CC, Stanick C, Powell BJ, Dorsey CN, Clary AS, et al. Psychometric assessment of three newly developed implementation outcome measures. Implement Sci. (2017) 12:108. doi: 10.1186/s13012-017-0635-3
68. Kwakkel G, Lannin NA, Borschmann K, English C, Ali M, Churilov L, et al. Standardized measurement of sensorimotor recovery in stroke trials: consensus-based core recommendations from the stroke recovery and rehabilitation roundtable. Neurorehabil Neural Repair. (2017) 31:784–92. doi: 10.1177/1545968317732662
69. Moore JL, Potter K, Blankshain K, Kaplan SL, O'Dwyer LC, Sullivan JE, et al. Core set of outcome measures for adults with neurologic conditions undergoing rehabilitation: a clinical practice guideline. J Neurol Phys Ther. (2018) 42:174–220. doi: 10.1097/NPT.0000000000000229
70. Salinas J, Sprinkhuizen SM, Ackerson T, Bernhardt J, Davie C, George MG, et al. An international standard set of patient-centered outcome measures after stroke. Stroke. (2016) 47:180–6. doi: 10.1161/STROKEAHA.115.010898
71. Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Developing and evaluating complex interventions: the new Medical Research Council guidance. BMJ. (2008) 337:a1655. doi: 10.1136/bmj.39486.541725.80
72. Hutton JL, Eccles MP, Grimshaw JM. Ethical issues in implementation research: a discussion of the problems in achieving informed consent. Implement Sci. (2008) 3:52. doi: 10.1186/1748-5908-3-52
73. Schnoor M, Meyer T, Suttorp N, Raspe H, Welte T, Schäfer T. Development and evaluation of an implementation strategy for the German guideline on community-acquired pneumonia. Qual Saf Health Care. (2010) 19:498–502. doi: 10.1136/qshc.2008.029629
74. Diermayr G, Schomberg M, Greisberger A, Elsner B, Gronwald M, Salbach NM. Task-oriented circuit training for mobility in outpatient stroke rehabilitation in Germany and Austria: a contextual transferability analysis. Phys Ther. (2020) 2020:pzaa053. doi: 10.1093/ptj/pzaa053
75. Jolliffe L, Hoffmann T, Churilov L, Lannin NA. What is the feasibility and observed effect of two implementation packages for stroke rehabilitation therapists implementing upper limb guidelines? A cluster controlled feasibility study. BMJ Open Qual. (2020) 9:954. doi: 10.1136/bmjoq-2020-000954
76. Cahill LS, Carey LM, Lannin NA, Turville M, Neilson CL, Lynch EA, et al. Implementation interventions to promote the uptake of evidence-based practices in stroke rehabilitation. Cochr Database Systemat Rev. (2020) 2020:CD012575.pub2. doi: 10.1002/14651858.CD012575.pub2
77. Glasziou P, Straus S, Brownlee S, Trevena L, Dans L, Guyatt G, et al. Evidence for underuse of effective medical services around the world. Lancet. (2017) 390:169–77. doi: 10.1016/S0140-6736(16)30946-1
78. Ebben RHA, Siqeca F, Madsen UR, Vloet LCM, Van Achterberg T. Effectiveness of implementation strategies for the improvement of guideline and protocol adherence in emergency care: a systematic review. BMJ Open. (2018) 8:17575. doi: 10.1136/bmjopen-2017-017572
79. Tomasone JR, Chaudhary R, Brouwers MC. Effectiveness of guideline dissemination and implementation strategies on health care professionals' behaviour and patient outcomes in the cancer care context: a systematic review protocol. Syst Rev. (2015) 4:113. doi: 10.1186/s13643-015-0100-9
80. Miao M, Power E, O'Halloran R. Factors affecting speech pathologists' implementation of stroke management guidelines: a thematic analysis. Disabil Rehabil. (2015) 37:674–85. doi: 10.3109/09638288.2014.932444
81. Reynolds SS, Murray LL, McLennon SM, Bakas T. Implementation of a stroke competency program to improve nurses' knowledge of and adherence to stroke guidelines. J Neurosci Nurs. (2016) 48:328–35. doi: 10.1097/JNN.0000000000000237
82. Francke AL, Smit MC, de Veer AJ, Mistiaen P. Factors influencing the implementation of clinical guidelines for health care professionals: a systematic meta-review. BMC Med Inform Decis Mak. (2008) 8:38. doi: 10.1186/1472-6947-8-38
83. Fischer F, Lange K, Klose K, Greiner W, Kraemer A. Barriers and strategies in guideline implementation-a scoping review. Healthcare. (2016) 4:30036. doi: 10.3390/healthcare4030036
84. Correa VC, Lugo-Agudelo LH, Aguirre-Acevedo DC, Contreras JAP, Borrero AMP, Patiño-Lugo DF, et al. Individual, health system, and contextual barriers and facilitators for the implementation of clinical practice guidelines: a systematic metareview. Health Res Pol Syst. (2020) 18:74. doi: 10.1186/s12961-020-00588-8
85. Juckett LA, Wengerd LR, Faieta J, Griffin CE. Evidence-based practice implementation in stroke rehabilitation: a scoping review of barriers and facilitators. Am J Occup Therapy. (2020) 74:1–14. doi: 10.5014/ajot.2020.035485
86. Paci M, Faedda G, Ugolini A, Pellicciari L. Barriers to evidence-based practice implementation in physiotherapy: a systematic review and meta-analysis. Int J Qual Health Care. (2021) 33:1–13. doi: 10.1093/intqhc/mzab093
87. Hakkennes S, Dodd K. Guideline implementation in allied health professions: a systematic review of the literature. Qual Saf Health Care. (2008) 17:296–300. doi: 10.1136/qshc.2007.023804
88. Liang L, Bernhardsson S, Vernooij RW, Armstrong MJ, Bussieres A, Brouwers MC, et al. Use of theory to plan or evaluate guideline implementation among physicians: a scoping review. Implement Sci. (2017) 12:26. doi: 10.1186/s13012-017-0557-0
89. Romney W, Bellows DM, Tavernite JP, Salbach N, Deutsch JE. Knowledge translation research to promote behavior changes in rehabilitation: use of theoretical frameworks and tailored interventions: a scoping review. Arch Phys Med Rehabil. (2021). doi: 10.1016/j.apmr.2021.01.076
90. Spoon D, Rietbergen T, Huis A, Heinen M, van Dijk M, van Bodegom-Vos L, et al. Implementation strategies used to implement nursing guidelines in daily practice: a systematic review. Int J Nurs Stud. (2020) 111:103748. doi: 10.1016/j.ijnurstu.2020.103748
91. Kovacs E, Wang X, Strobl R, Grill E. Economic evaluation of guideline implementation in primary care: a systematic review. Int J Qual Health Care. (2020) 32:1–11. doi: 10.1093/intqhc/mzz059
92. Murrell JE, Pisegna JL, Juckett LA. Implementation strategies and outcomes for occupational therapy in adult stroke rehabilitation: a scoping review. Implement Sci. (2021) 16:1–26. doi: 10.21203/rs.3.rs-229354/v1
93. van der Wees PJ, Jamtvedt G, Rebbeck T, de Bie RA, Dekker J, Hendriks EJ. Multifaceted strategies may increase implementation of physiotherapy clinical guidelines: a systematic review. Aust J Physiother. (2008) 54:233–41. doi: 10.1016/S0004-9514(08)70002-3
94. Zadro JR, O'Keeffe M, Allison JL, Lembke KA, Forbes JL, Maher CG. Effectiveness of implementation strategies to improve adherence of physical therapist treatment choices to clinical practice guidelines for musculoskeletal conditions: systematic review. Phys Ther. (2020) 100:1516–41. doi: 10.1093/ptj/pzaa101
95. McCluskey A, Massie L, Gibson G, Pinkerton L, Vandenberg A. Increasing the delivery of upper limb constraint-induced movement therapy post-stroke: a feasibility implementation study. Aust Occup Ther J. (2020) 2020:12647. doi: 10.1111/1440-1630.12647
96. Connell LA, McMahon NE, Tyson SF, Watkins CL, Eng JJ. Mechanisms of action of an implementation intervention in stroke rehabilitation: a qualitative interview study. BMC Health Serv Res. (2016) 16:534. doi: 10.1186/s12913-016-1793-8
97. Shrubsole K, Worrall L, Power E, O'Connor DA. The Acute Aphasia IMplementation Study (AAIMS): a pilot cluster randomized controlled trial. Int J Lang Commun Disord. (2018) 53:1021–56. doi: 10.1111/1460-6984.12419
Keywords: guideline, implementation, stroke, allied health professionals, rehabilitation
Citation: Scheffler B, Schimböck F, Schöler A, Rösner K, Spallek J and Kopkow C (2022) Tailored GuideLine Implementation in STrokE Rehabilitation (GLISTER) in Germany. Protocol of a Mixed Methods Study Using the Behavior Change Wheel and the Theoretical Domains Framework. Front. Neurol. 13:828521. doi: 10.3389/fneur.2022.828521
Received: 03 December 2021; Accepted: 17 June 2022;
Published: 27 July 2022.
Edited by:
Alessandra Solari, IRCCS Carlo Besta Neurological Institute Foundation, ItalyReviewed by:
Christoph Heesen, University Medical Center Hamburg-Eppendorf, GermanyCopyright © 2022 Scheffler, Schimböck, Schöler, Rösner, Spallek and Kopkow. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bettina Scheffler, YmV0dGluYS5zY2hlZmZsZXJAYi10dS5kZQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.