 Samar S. Ayache
Samar S. Ayache Nicolas Serratrice
Nicolas Serratrice Georges N. Abi Lahoud
Georges N. Abi Lahoud Moussa A. Chalah
Moussa A. Chalah- 1EA4391 Excitabilité Nerveuse and Thérapeutique, Université Paris Est Créteil, Créteil, France
- 2Department of Clinical Neurophysiology, DMU FIxIT, Henri Mondor University Hospital, Assistance Publique-Hôpitaux de Paris (APHP), Créteil, France
- 3Department of Spine Surgery, Centre Médico Chirurgical Bizet, Paris, France
- 4Institut de la Colonne Vertébrale et des Neurosciences (ICVNS), Centre Médico Chirurgical Bizet, Paris, France
Fatigue is the most commonly reported symptom in patients with multiple sclerosis (MS). It is a worrisome, frequent, and debilitating manifestation that could occur at any time during the course of MS and in all its subtypes. It could engender professional, familial, and socioeconomic consequences and could severely compromise the patients' quality of life. Clinically, the symptom exhibits motor, cognitive, and psychosocial facets. It is also important to differentiate between perceived or subjective self-reported fatigue and fatigability which is an objective measure of decrement in the performance of cognitive or motor tasks. The pathophysiology of MS fatigue is complex, and its management remains a challenge, despite the existing body of literature on this matter. Hence, unraveling its neural mechanisms and developing treatment options that target the latter might constitute a promising field to explore. A PubMed/Medline/Scopus search was conducted to perform this review which aims (a) to reappraise the available electrophysiological studies that explored fatigue in patients with MS with a particular focus on corticospinal excitability measures obtained using transcranial magnetic stimulation and (b) to assess the potential utility of employing neuromodulation (i.e., non-invasive brain stimulation techniques) in this context. A special focus will be put on the role of transcranial direct current stimulation and transcranial magnetic stimulation. We have provided some suggestions that will help overcome the current limitations in upcoming research.
Introduction
Multiple sclerosis (MS) is one of the most common neurological diseases and a serious cause of disability in young adults. Its natural course is characterized by recurrent relapses and progressive functional decline (1). With disease evolution, patients could accumulate several neurological dysfunctions, including motor deficit, sensory dysfunction, and sphincter disorders, among others (2). In addition, they could suffer from several “silent” “non-motor” complications, such as fatigue, pain, emotional manifestations, and cognitive dysfunctions (3).
Over the last two decades, MS symptoms have preoccupied the scientific community, and tremendous efforts have been made to understand the reasons behind their development and the modalities of their treatments. Among these symptoms, fatigue constitutes a real enigma and has given rise to collective awareness. Although the last few years have shown a growing literature on the characterization, pathophysiology, and treatment of MS fatigue, this symptom continues to challenge the medical and research societies of its difficult-to-treat nature and its resistance to the available pharmacological solutions. Hence, in this review, we will start with a definition of MS fatigue by highlighting the difference between fatigue and fatiguability. Then, we will give an overview of its underlying pathophysiological mechanisms. There will be particular focus on the application of the neurophysiological techniques in this domain. Afterward, we will address the place of non-invasive brain stimulation (NIBS) interventions in the treatment of this symptom.
Fatigue in MS
MS fatigue is very common; it could impact the lives of 75–90% of patients suffering from this disease (2, 4). It deeply affects their professional, social, and familial domains and could result in significant health costs and, therefore, should not be neglected (5, 6). For all these reasons, understanding this symptom and adopting novel therapeutic approaches have become more important than ever before.
To start, the definition of fatigue has been a source of confusion for several years. On the one hand, the terms “tiredness,” “malaise,” and “motor weakness” have been interchangeably used by patients to describe their fatigue; on the other hand, care providers have sometimes perceived fatigue as a lack of self-motivation. Toward the end of the 90's, a consensus was set by the MS Council for Clinical Practice Guidelines and has ended this debate (7). According to this council, MS fatigue corresponds to “a subjective lack of physical and/or mental energy that is perceived by the individual or caregiver to interfere with usual and desired activities.” Currently, it is recommended to adopt this definition as has been thoroughly discussed in Mills and Young's study (8). In the same perspective of this definition, the intensity of MS fatigue is temperature-dependent in a way that hot or cold temperatures would worsen or alleviate fatigue, respectively. This aspect differentiates it from the “classical” tiredness encountered in healthy individuals.
In addition to the importance of setting a clear definition of fatigue, it is important to stress the difference between subjective or perceived self-reported fatigue and fatigability. While the former reflects a subjective experience that is classically tested by self-administered questionnaires, the latter reflects a performance decrement during the execution of a task and is usually evaluated with various cognitive or physical exercises.
Fatigue is a multifaceted symptom and consists of three domains: the physical, psychosocial, and cognitive domains. Thus, when patients complain about fatigue, the clinician or researcher should understand whether they feel this fatigue in the three domains or whether it only concerns one domain, for instance, the cognitive one. For this reason, some of the self-rated questionnaires that have been developed to diagnose and follow up on this complaint included questions dedicated to the assessment of several aspects of MS fatigue. For instance, the Modified Fatigue Impact Scale (MFIS), one of the most widely used scales, includes 21 questions that examine the three facets of fatigue (i.e., the physical, psychosocial, and cognitive ones) (7). In a similar manner, the Fatigue Scale for Motor and Cognitive Functions includes 20 questions and assesses two dimensions of MS fatigue as its name implies (9). Other scales assess one dimension of fatigue (e.g., the physical dimension), such as the 9-item Fatigue Severity Scale, which is one of the first tools developed to be used in PwMS (10), while others such as the Visual Analog Scale [VAS, (11)] provide a global assessment of this symptom [For a review refer to (1)].
Moreover, when talking about MS fatigue, it is pertinent to distinguish between primary fatigue, which is related to disease-specific mechanisms, and secondary fatigue, which could rather be attributed to comorbidities (motor symptoms, psychiatric manifestations, other medical conditions, or treatments adverse events) (1).
Selection Criteria
Research was done following PRISMA guidelines using computerized databases (PubMed/MEDLINE, Scopus) (12). An independent review was conducted by two of the authors (SSA and MAC) in order to identify original research articles published in English and French languages at any time till November 2021. The following key terms were used: (“MS” OR “multiple sclerosis”) AND (“fatigue”) AND (“non-invasive brain stimulation” OR “NIBS” OR “transcranial magnetic stimulation” OR “TMS” OR “theta burst stimulation” OR “TBS” OR “motor evoked potential” OR “MEP” OR “cortical excitability” OR “corticospinal excitability” OR “intracortical inhibition” OR “intracortical facilitation” OR “silent period” OR “interhemispheric inhibition” OR “transcranial direct current stimulation” OR “tDCS” OR “transcranial random noise stimulation” OR “tRNS”). In order to look for additional sources, the bibliographical references of the retrieved articles were also scanned.
Pathophysiology of Fatigue in MS
Clinical, neuropsychological, neuroanatomical, neuroimmune, and neurophysiological studies attempted to explore this multidimensional symptom. From a clinical perspective, the relationship between fatigue and physical disability appears to be inconsistent; MS fatigue seems to occur in all disease subtypes (4). From a neuropsychological viewpoint, fatigue could be associated with specific emotions, thoughts, and behaviors according to a cognitive-behavioral model proposed by van Kessel and Moss-Morris (13). In addition, this symptom could be associated with emotional factors, with which it may have bidirectional relationships and may share common biological substrates (14). In terms of neuroanatomy, inconsistencies exist regarding conventional measures (e.g., lesion load, global brain atrophy), but more advanced neuroimaging modalities (e.g., tractography, normal-appearing white matter, regional brain volumes and lesion load, brain activity, and functional connectivity at rest or during task performance) have unraveled a cortico-striato-thalamo-cortical loop related to MS fatigue (15–19). The exploration of neuroimmune and neuroendocrine axes has yielded scarce findings linking MS fatigue to some peripheral proinflammatory cytokines (20–22), while the relationship between this symptom and other outcomes were inconsistent {i.e., cerebrospinal fluid markers, orexin-A system, hypothalamus-pituitary-adrenal axis (20, 21, 23, 24), or absent [peripheral T cell populations or markers of inflammation (25, 26)]} [for reviews see (14)]. Finally, neurophysiology also constitutes a discipline that addresses MS fatigue in terms of pathophysiology and management as will be developed in the following sections.
Nibs to Explore and Manage Fatigue in MS
Modulating the activity of brain regions and circuits continues to be a fascinating scientific field and a source of inspiration for researchers worldwide. The story began in the previous century when scientists first tested the impact of a weak electric current on the functioning of neural networks in animals and discovered that the application of a polarizing current on the scalp results in various effects on cortical activity. Afterward, much research has taken place across the world, and the fruit of this long investment has resulted in the development of the various NIBS techniques that we currently have at our disposal. Among these techniques, two are particularly interesting and have been the subject of many scientific investigations into different pathologies. The first is based on a famous law of biophysics—Faraday's law (the law of electromagnetic induction)—, while the second rather uses a weak electric current. These are, respectively, the transcranial magnetic stimulation (TMS) and the transcranial direct current stimulation (tDCS) techniques (27–30).
Neurophysiology of Fatigue in MS Using NIBS
As stated previously, TMS finds its roots in an ancient law of biophysics—the Faraday law. In fact, this law paved the way for the development of what has now become the rescue solution to some crippling neuropsychiatric manifestations, such as depression and neuropathic pain (29). Briefly, Faraday demonstrated that making an electric current flow in a conductive element would induce a magnetic field; the latter could in its turn induce an electric field in another conductive element placed nearby. Hence, applying a magnetic field on the scalp would diffuse toward the underlying cortical networks and would stimulate the corresponding nervous fibers (29).
The first clinical development of TMS served for the study of pyramidal motor conductions, using the technique known as motor evoked potentials (MEP). Performing MEP remains the most common application of TMS (31). This technique uses unique shocks applied to the skull to stimulate the pyramidal cortical neurons and to the spine to activate the nerve roots. A surface electromyographic recording is made at the level of the muscles of interest and the parameters (i.e., latency and amplitude) of the evoked responses are generally measured. Central motor conduction time (CMCT) is another TMS parameter used in clinical settings and reflects the time the nerve impulses take to travel from the motor cortex to the spinal motor neurons. It could be measured by subtracting the MEP latency obtained from spinal magnetic stimulation (also known as peripheral motor conduction time) from TMS-evoked MEP latency (32). Its lengthening may arise from a degeneration or a demyelination affecting the fastest-conducting cortico-motoneuronal fibers (33). Prolonged MEP latency was found to be a significant predictor of fatigue severity (34) while CMCT seems to be unrelated to this symptom (35).
Apart from obtaining conventional MEP, TMS has other important applications such as studying cortical excitability, which assesses different processes of regulation and execution of motor commands using paradigms of single and double cortical pulses. The parameters measured (i.e., motor thresholds (MT), short-interval intracortical inhibition (SICI) and intracortical facilitation (ICF), cortical silent period (CSP), interhemispheric inhibition (IHI), cerebello-cortical inhibition, among others) provide information on neuronal modulation circuits using well-characterized GABAergic, glutamatergic, or cholinergic neurotransmission (32, 33). Excitability paradigms have been widely used to examine the pathophysiological processes behind several neurological and psychiatric symptoms, among which stands MS fatigue.
To start, concerning single-pulse parameters, no correlation was found between fatigue severity and resting MT (rMT) (36, 37), a parameter that reflects the excitability of the corticomotor neuronal membrane, including the spinal level. It corresponds to the stimulation intensity, as a percentage of the maximal stimulator output, that yields MEP of at least 50 μV amplitude on a fully relaxed muscle in 5 out of 10 trials (32, 33). The CSP is another single-pulse parameter that reflects cortical (GABA-B) and spinal inhibitions (e.g., Renshaw cells, IA inhibitory interneurons) (32, 33). It could last up to 300 ms and corresponds to the interruption of voluntary muscular activity in a muscle of interest by applying a TMS pulse over the contralateral motor cortex. Prolonged CSP was found to be associated with fatigue severity in one study (38) but not in another one (37). Such discrepancy could be related to the clinical and methodological differences between both studies, such as the cohorts' disease characteristics (predominantly relapsing–remitting vs. progressive disease, respectively) and the adapted fatigue measures (VAS vs. MFIS, respectively).
Besides single-pulse measures, double-pulse measures could also be used. Some of them consist of applying a first subthreshold conditioning stimulus (whose intensity is below the rMT) that would inhibit or facilitate the response of a second suprathreshold stimulus (whose intensity is above the rMT) delivered to the same cortical site depending on the interstimulus interval (ISI) (32). For instance, applying short (≤ 6 ms) and long (≥7 ms) ISI could yield SICI and ICF which respectively, reflects GABA-A and glutamatergic transmissions. IHI represents another double-pulse measure that consists of conditioning the response of a suprathreshold stimulus by applying a suprathreshold stimulus over the contralateral motor site, and reflects GABAergic transcallosal activity (32). Three works have explored SICI in the context of MS fatigue and found low (36), high (37), or similar (39) pattern of inhibition in fatigued PwMS compared to non-fatigued PwMS and/or healthy controls (HC). In addition, in these three works, no significant group difference (or correlation) was obtained in terms of fatigue and ICF. Moreover, one of the three works included an IHI assessment and found no correlation between this measure and fatigue severity (37).
Some studies also explored the neurophysiological correlates of MS fatigue during motor task performance and tested the relationship of this symptom with movement preparation or execution phases. Some reported positive findings linking MS fatigue to movement-related TMS outcomes. Premovement MEP facilitation which is a normal finding following a motor task was found to be significantly reduced in fatigued PwMS compared to their non-fatigued counterparts and HC (39–41). This finding was correlated with frontal lesion load (39), motor performance decay [decrease in movement rate, (40)], and fatigue severity (39), suggesting a relationship between MS fatigue and abnormalities involving cerebral networks devoted to movement preparation. In addition, higher MEP amplitude was observed with contralateral hand grip following the fatiguing task in HC and non-fatigued PwMS but not in fatigued PwMS. This finding might suggest an involvement of callosal dysfunction in MS fatigue (42). Moreover, fatigue severity seems to be correlated with the time required for the rMT to reach the pre-exercise level (36). Conversely, no group difference in post-exercise MEP facilitation was found between non-fatigued and fatigued PwMS (43).
The second other major application of TMS is the realization of repetitive TMS (rTMS). Briefly, this method consists of delivering trains of stimulation at various frequencies and requiring specific machines (27, 29). Data on rTMS effects derive from numerous studies performed in healthy individuals, in whom low and high frequency (LF and HF) rTMS, respectively led to reduction and augmentation of MEP size. Hence, LF-rTMS and HF-rTMS have been perceived as inhibitory and facilitatory interventions. However, this viewpoint is simplistic, and it is now known that this dichotomy is no more valid since rTMS effects also depend on the baseline excitatory state of the nervous circuits; a state that would vary between individuals and even in the same subject at different moments of the day, it would also vary between healthy networks and those affected by various pathologies. Even more, several studies have documented that the augmentation/reduction of MEP amplitude after the application of HF/LF rTMS over the precentral cortex [i.e., the primary motor cortex (M1)] may be due to a decrease/increase of the GABA mediated inhibitory control of the corticospinal circuit rather than a direct modulation of the motor cortex excitability. Thus, what is perceived as “facilitatory” protocol (HF rTMS) could be in fact “inhibitory” (decrease in the functioning of the GABA interneurons) and vice versa. Other factors that can impact rTMS effects include age, drugs, and genetic factors, among others [For review, please refer to (27)].
In addition to the “classical” rTMS paradigms, a particular form of rTMS has been recently developed, the so-called theta burst stimulation (TBS). It consists of applying bursts (three pulses per burst at 50 Hz) in a repetitive manner at theta frequency (at 5 Hz) (44). TBS could induce changes in corticospinal excitability and the nature of such changes depends on the way the bursts are applied. Continuous and intermittent TBS (cTBS and iTBS) could lead to long-term depression-like and long-term potentiation-like effects, respectively (44).
Concerning rTMS and MS fatigue pathophysiology, it is worth noting here that some study protocols have tested the effects of 5-Hz rTMS over MEP outcomes in PwMS. In one study, MEP outcomes did not significantly differ between fatigued and non-fatigued PwMS, with both patient groups showing an increase in MEP amplitude following the intervention (39). In another study, the expected increase in MEP size was not obtained in fatigued PwMS, an increment that was found in their non-fatigued counterparts and in HC (45). Methodological differences could partly account for the observed changes as the second study included an attentional task (instructions to focus attention on the hand corresponding to stimulation); in addition, as aforementioned, inter-individual variability in terms of the baseline cortical excitability level could be behind such a discrepancy. One should note that the second study also assessed the impact of paired-associative stimulation (peripheral nerve stimulation followed by 5-Hz rTMS) on MEP amplitude and yielded similar findings (i.e., no change in MEP amplitude in fatigued PwMS) (45).
As for TBS, it is worth mentioning that no single study has applied this technique to explore the underlying mechanisms of MS fatigue. Its future application in this context could unveil additional mechanisms incriminated in the generation of this symptom. Table 1 summarizes the neurophysiological studies that explored MS fatigue.
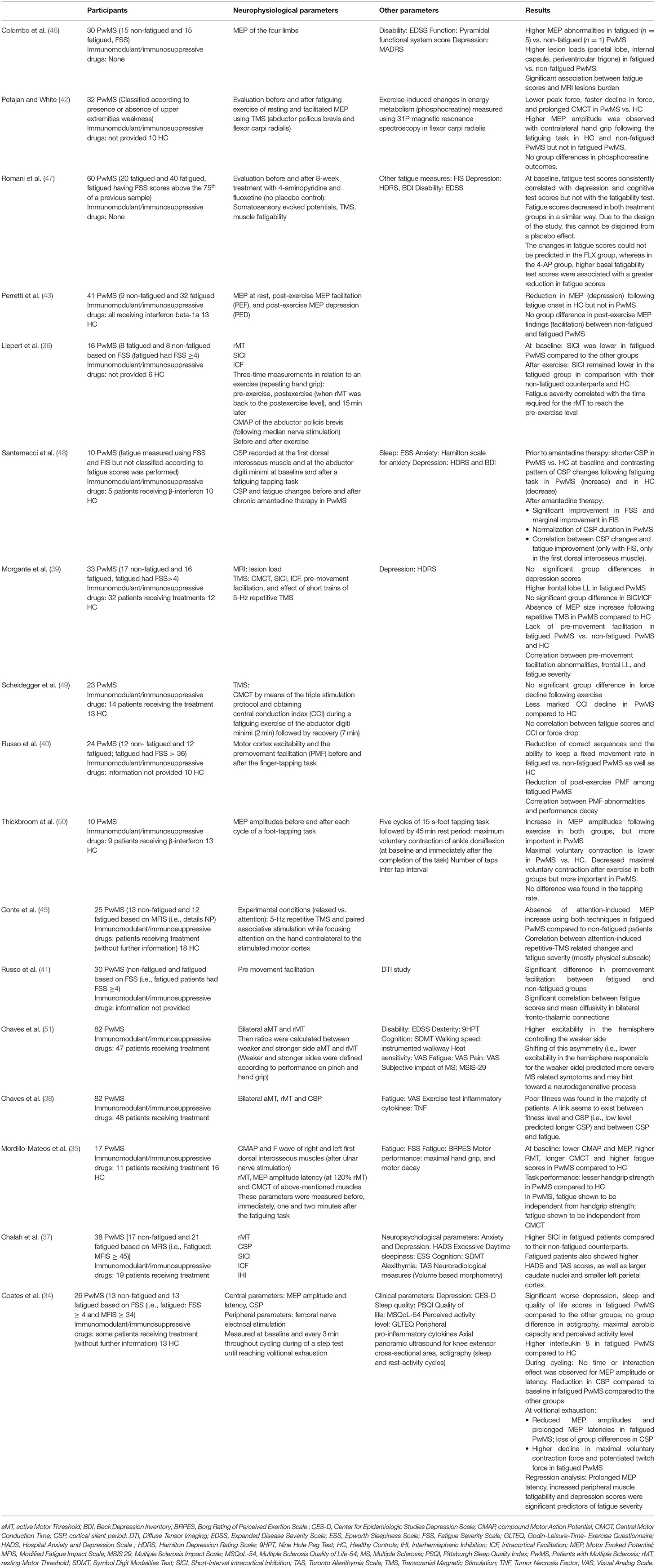
Table 1. Summary of studies on neurophysiological parameters in MS fatigue.
Treatment of Fatigue in MS Using NIBS
As stated previously, MS fatigue is perceived as a multidimensional construct, thus its management requires a personalized strategy that should address each of its dimensions. In this setting, various therapeutic interventions have been tried including pharmacological and non-pharmacological approaches. Concerning the pharmacological solutions, there is a vast array of literature on this topic, with numerous molecules being tested over the last years and only few having benefited from an in-depth evaluation. This includes amantadine hydrochloride, modafinil, pemoline, carnitine, and potassium channels blockers. Although all these drugs have demonstrated promising results in some studies, other works have failed to document any amelioration of fatigue and have thus questioned their place in the management of this symptom. Moreover, in a recent randomized, placebo-controlled, double-blind trial that compared the effects of amantadine, modafinil, and methylphenidate on MS fatigue, the studied drugs were not significantly superior to placebo in terms of efficacy and engendered more frequent adverse effects (52). Description of the mechanisms of action of these drugs and results of the corresponding studies falls outside the scope of this review [for more details, please refer to (1)].
In what concerns non-pharmacological alternatives, numerous therapies have been assessed so far and have led to some encouraging results, as has been demonstrated with exercise, whole body cryostimulation (53), cognitive behavioral therapies (CBT) (54), and NIBS (55). As mentioned in the introduction, in this review, we will only focus on the latter techniques (i.e., NIBS), the remaining does not match the main purpose of the current review.
As stated previously, tDCS is a NIBS technique that relies on the administration of a feeble electric current through two saline-soaked sponge electrodes, an anode and a cathode, placed on the scalp and connected to a battery-driven stimulator (28). The choice of the electrodes' place and polarity depends on the intended effects. This approach has been shown to be beneficial in several neurological and psychological problems, such as neuropathic pain, anxiety, and depression, to set a few. Therefore, its application in PwMS, and particularly in the context of fatigue, has been the focus of several research teams. The majority of studies that assessed the effects of tDCS on subjective or perceived self-reported MS fatigue adopted a crossover randomized (or pseudorandomized) design, were double-blinded and sham-controlled, and consisted of applying an anodal stimulation over the left dorsolateral prefrontal cortex (DLPFC), the right posterior parietal cortex, the bilateral sensorimotor cortex, the bilateral motor, or the bilateral primary somatosensory cortex. The current used was of weak intensity, ranging from 1.5 to 2 mA; and the session duration varied between 15 and 20 min. While results from bilateral somatosensory cortex/bilateral motor cortex stimulation were encouraging (56–59); those of left DLPFC were controversial, with two studies showing negative results (60, 61) and two others documenting positive outcomes (62, 63). Such a discrepancy seems to be due to the difference in the current intensity [current intensity: 1.5 mA in (60) vs. 2 mA in (62, 63)] and the number of stimulation sessions [3 in (61) and 5 in (62, 63)] across the abovementioned studies. This point of view could be supported by the data of a recent work where robust anti-fatigue effects were seen after the left DLPFC and left M1 stimulation, with more lasting fatigue reduction observed following the former condition (64).
As for the posterior parietal cortex (62) and the bilateral sensorimotor cortex (of hand area) (57), results should be interpreted with caution since they are based on two studies only, and further investigations are needed before drawing any formal conclusion.
Regarding fatigability, cognitive and motor fatigability have been investigated in three studies, two of them tested the impact of one anodal session [over the right parietal cortex in (65) and over the left DLPFC in (66)] on cognitive performance during a particular task [visual task in (65), and measurement of P300 in (66)] and one work assessed the effects of 5 consecutive anodal sessions over M1 on a cluster of symptoms including pain, subjective fatigue, and motor fatigability (67). It has been shown that delivering anodal stimulation over the left DLPFC or the right parietal cortex could counteract cognitive fatigability and prevent decrement in cognitive performance (reflected by prolonged reaction time). On the other hand, anodal stimulation of M1 would result in a decrease in motor fatigability (of the contralateral leg), as well as an amelioration of subjective fatigue and pain.
All the previously reported studies have addressed the short-lasting effects of tDCS and its feasibility over a short period of time (sessions were performed over 1 or 2 weeks). However, to suggest this innovative technique as a therapeutic solution for PwMS, we need to maintain its effectiveness over time; such maintenance requires repetition of the sessions, and this has been addressed in some case studies where sessions (14–19 sessions) were repeated over 4 weeks and ensured a long-term reduction of fatigue and amelioration of cognitive functions as well as the mood state (68, 69).
Although the results of these trials are interesting, a limitation should be considered. In fact, health providers are dealing with a fragile population, thus suggesting to this population that recurrent traveling to the care facilities is a real challenge. Often, these patients are either disabled and/or have a busy personal or professional schedule, which should be taken into consideration. Hence, the best solution would be by organizing a home-based therapy. The feasibility and efficacy of the latter have been tested by Charvet et al., and it has been documented that remotely supervised tDCS sessions are safe, could be coupled with computer-based cognitive training programs, and would help in alleviating fatigue and improving cognitive performance (70).
Besides tDCS, other neuromodulation approaches have been also tried in the setting of MS fatigue. However, the literature is limited to few studies. Two of them have explored the potential role of transcranial random noise stimulation (tRNS) in the treatment of fatigue and three of them have evaluated the place of rTMS or TBS in this context.
Transcranial random noise stimulation yielded beneficial antifatigue effects in one study (71) but not in the other one (72). Compared to Palm and colleagues, Salemi and colleagues had a different study design (crossover vs. parallel arms, respectively), applied a larger number of sessions (3 vs. 10, respectively), and targeted a different cortical site (left DLPFC vs. M1 of the dominant side or contralateral to the most affected limb, respectively).
Transcranial random noise stimulation/theta burst stimulation studies targeted different cortical sites and were applied alone or in combination with exercise or physical therapy. Some of these studies suggested promising findings that are worth replicating in future trials (73–76). Briefly, with regards to rTMS, 10–18 sessions applied at 5–20 Hz over M1 bilaterally, with or without physical therapy, resulted in significant fatigue reduction (74, 75). As for TBS, the existing literature on the matter consisted of iTBS protocols. Ten sessions of such intervention, combined with exercise or physical therapy, did not significantly affect fatigue when applied over the cerebellum or M1 bilaterally (75, 76) but yielded antifatigue effects when applied over M1 contralateral to the most spastic limb (73). The latter protocol applied without concomitant exercise did not significantly reduce fatigue compared to the sham (73). Here, it is worth stating that the considered iTBS studies primarily focused on MS spasticity, fatigue being included as a secondary outcome. Therefore, the effects of iTBS on primary MS fatigue merit to be further addressed. Details of NIBS application in MS fatigue are presented in Table 2.
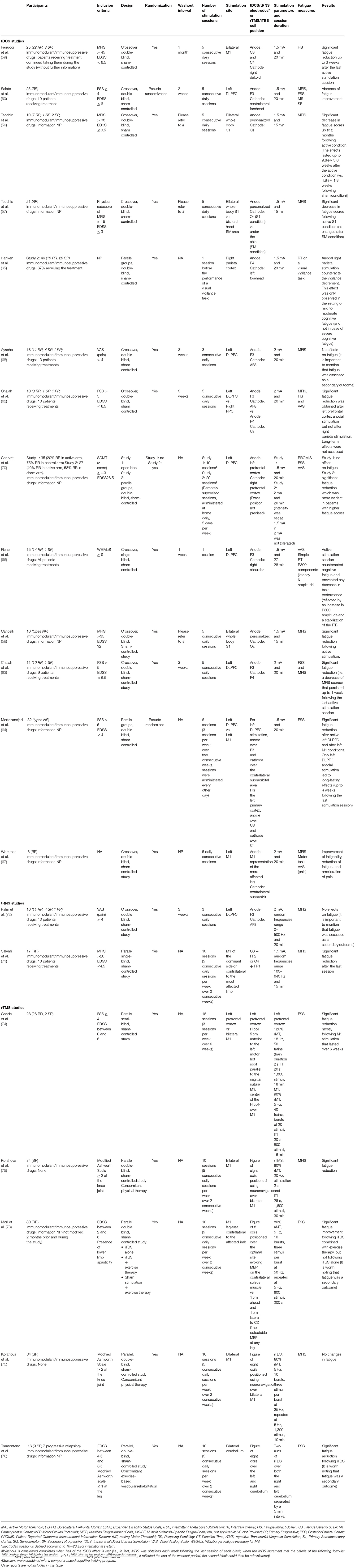
Table 2. Summary of NIBS studies in MS fatigue.
Conclusion
This review explored the potential role of neurophysiology in the exploration and modulation of fatigue in PwMS. First, in terms of pathophysiology, the available studies that included intracortical excitability and corticospinal excitability outcomes yielded inconsistent findings. For instance, while fatigue was correlated with SICI/CSP (GABA-mediated outcomes) in some studies, such a correlation was not found in other studies. The included studies were cross-sectional; they assessed fatigue using different scales and included PwMS suffering from different disease subtypes. This highlights the relevance of longitudinally studying the dynamics of these parameters across the disease course and subtypes and their relationships with fatigue. In addition, considering secondary factors to fatigue and taking into consideration the symptom cluster in the covariate analysis would also be of help (3). Besides tackling the previously mentioned differences (subjected or perceived self-reported fatigue vs. fatigability, primary vs. secondary), the temporal dimension of fatigue merits to be considered. In this perspective, Palotai and colleagues longitudinally assessed PwMS and suggested different types of fatigue (sustained fatigue vs. one time-point fatigue vs. reversible fatigue), which seem to differ in brain imaging findings (brain parenchymal fraction, T2 lesion volume) (77), a finding that might also apply to corticospinal excitability parameters.
Second, in terms of tDCS, the data altogether suggest promising tDCS effects obtained on MS fatigue. The current challenge remains to find the best parameters to optimize treatment effects (e.g., applying a higher number of sessions, selecting the best cortical target, selecting the best return electrode location, designing patient-tailored electrodes, increasing the current intensity up to 4 mA) (56, 57, 68, 69, 78). As stated with neurophysiological exploration, it would be helpful to consider the temporal dynamics of fatigue and the symptom cluster when assessing the mediators of response to tDCS. It is noteworthy that, when it comes to either exploring or modulating MS fatigue using NIBS techniques, a confounder that needs to be considered or accounted for is the pharmacological profile of the recruited cohorts. For instance, some medications (e.g., disease-modifying therapies, symptomatic treatments) might modify the corticospinal excitability in PwMS (79). In addition, some treatments (e.g., sodium channel blockers, calcium channel blockers, medications that act on neurotransmitters pathways) may also affect the tDCS effects on corticospinal excitability (80). The relationship between the treatment status and the considered outcomes (e.g., SICI, ICF, IHI, CSP, or fatigue improvement) warrants further investigation since this was rarely or not tackled in previous studies.
Third, studying the effects of tDCS on corticospinal excitability would provide further insights into the neurophysiological mechanisms of fatigue and the antifatigue mechanisms of action of tDCS (57, 68).
Finally, home-based tDCS will provide a solution for physically disabled PwMS. The application of psychotherapies (e.g., CBT-based online interventions) and pharmacotherapy might yield synergistic effects (81). Such an approach constitutes a domain that remains to be explored in this context.
Author Contributions
SA and MC: conceptualization and methodology. MC, NS, GA, and SA: data analysis, writing—original draft preparation, and writing—review and editing. SA: supervision. All authors have read and agreed to the published version of the manuscript.
Conflict of Interest
SA declares having received compensation from ExoNeural Network AB, Sweden. MC declares having received compensation from Janssen Global Services LLC, ExoNeural Network AB, Sweden, and Ottobock, France.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Ayache SS, Chalah MA. Fatigue in multiple sclerosis - insights into evaluation and management. Neurophysiol Clin. (2017) 47:139–71. doi: 10.1016/j.neucli.2017.02.004
2. Noseworthy JH, Lucchinetti C, Rodriguez M, Weinshenker BG. Multiple sclerosis. N Engl J Med. (2000) 343:938–52. doi: 10.1056/NEJM200009283431307
3. Ayache SS, Chalah MA. Fatigue and affective manifestations in multiple sclerosis-a cluster approach. Brain Sci. (2019) 10:10. doi: 10.3390/brainsci10010010
4. Chalah MA, Riachi N, Ahdab R, Créange A, Lefaucheur JP, Ayache SS. Fatigue in multiple sclerosis: neural correlates and the role of non-invasive brain stimulation. Front Cell Neurosci. (2015) 9:460. doi: 10.3389/fncel.2015.00460
5. Le H, Ken-Opurum J, Maculaitis M, Sheehan J. Comorbidity and economic burdens of fatigue among patients with Relapsing-remitting multiple sclerosis in the United States [Poster Presentation]. MS Virtual 2020 Joint ACTRIMS-ECTRIMS meeting. Multiple Sclerosis Journal. Thousand Oaks, CA: SAGE (2020).
6. Oliva Ramirez A, Keenan A, Kalau O, Worthington E, Cohen L, Singh S. Prevalence and burden of multiple sclerosis-related fatigue: a systematic literature review. BMC Neurol. (2021) 21:468. doi: 10.1186/s12883-021-02396-1
7. Multiple sclerosis council for clinical practice guidelines. Fatigue and Multiple Sclerosis: Evidence-Based Management Strategies for Fatigue in Multiple Sclerosis. Washington, DC; Paralyzed Veterans of America (1998).
8. Mills RJ, Young CA. A medical definition of fatigue in multiple sclerosis. QJM. (2008). 101:49–60. doi: 10.1093/qjmed/hcm122
9. Penner IK, Raselli C, Stöcklin M, Opwis K, Kappos L, Calabrese P. The Fatigue Scale for Motor and Cognitive Functions (FSMC): validation of a new instrument to assess multiple sclerosis-related fatigue. Mult Scler. (2009) 15:1509–17. doi: 10.1177/1352458509348519
10. Krupp LB, LaRocca NG, Muir-Nash J, Steinberg AD. The fatigue severity scale. Application to patients with multiple sclerosis and systemic lupus erythematosus. Arch Neurol. (1989) 46:1121–3. doi: 10.1001/archneur.1989.00520460115022
11. Kos D, Nagels G, D'Hooghe MB, Duportail M, Kerckhofs E. A rapid screening tool for fatigue impact in multiple sclerosis. BMC Neurol. (2006) 6:27. doi: 10.1186/1471-2377-6-27
12. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.31222/osf.io/v7gm2
13. van Kessel K, Moss-Morris R. Understanding multiple sclerosis fatigue: a synthesis of biological and psychological factors. J Psychosom Res. (2006) 61:583–5. doi: 10.1016/j.jpsychores.2006.03.006
14. Chalah MA, Ayache SS. Is there a link between inflammation and fatigue in multiple sclerosis? J Inflamm Res. (2018) 11:253–64. doi: 10.2147/JIR.S167199
15. Calabrese M, Rinaldi F, Grossi P, Mattisi I, Bernardi V, Favaretto A, et al. Basal ganglia and frontal/parietal cortical atrophy is associated with fatigue in relapsing-remitting multiple sclerosis. Mult Scler. (2010) 16:1220–8. doi: 10.1177/1352458510376405
16. Stefancin P, Govindarajan ST, Krupp L, Charvet L, Duong TQ. Resting-state functional connectivity networks associated with fatigue in multiple sclerosis with early age onset. Mult Scler Relat Disord. (2019) 31:101–5. doi: 10.1016/j.msard.2019.03.020
17. Arm J, Ribbons K, Lechner-Scott J, Ramadan S. Evaluation of MS related central fatigue using MR neuroimaging methods: scoping review. J Neurol Sci. (2019) 400:52–71. doi: 10.1016/j.jns.2019.03.007
18. Capone F, Collorone S, Cortese R, Di Lazzaro V, Moccia M. Fatigue in multiple sclerosis: the role of thalamus. Mult Scler. (2020) 26:6–16. doi: 10.1177/1352458519851247
19. Palotai M, Guttmann CR. Brain anatomical correlates of fatigue in multiple sclerosis. Mult Scler. (2020) 26:751–64. doi: 10.1177/1352458519876032
20. Heesen C, Nawrath L, Reich C, Bauer N, Schulz KH, Gold SM. Fatigue in multiple sclerosis: an example of cytokine mediated sickness behaviour? J Neurol Neurosurg Psychiatry. (2006) 77:34–9. doi: 10.1136/jnnp.2005.065805
21. Gold SM, Krüger S, Ziegler KJ, Krieger T, Schulz KH, Otte C, et al. Endocrine and immune substrates of depressive symptoms and fatigue in multiple sclerosis patients with comorbid major depression. J Neurol Neurosurg Psychiatry. (2011) 82:814–8. doi: 10.1136/jnnp.2010.230029
22. Pokryszko-Dragan A, Frydecka I, Kosmaczewska A, Ciszak L, Bilińska M, Gruszka E, et al. Stimulated peripheral production of interferon-gamma is related to fatigue and depression in multiple sclerosis. Clin Neurol Neurosurg. (2012) 114:1153–8. doi: 10.1016/j.clineuro.2012.02.048
23. Papuć E, Stelmasiak Z, Grieb P, Paweł G, Rejdak K. CSF hypocretin-1 concentrations correlate with the level of fatigue in multiple sclerosis patients. Neurosci Lett. (2010) 474:9–12. doi: 10.1016/j.neulet.2010.02.062
24. Constantinescu CS, Niepel G, Patterson M, Judd A, Braitch M, Fahey AJ, et al. Orexin A (hypocretin-1) levels are not reduced while cocaine/amphetamine regulated transcript levels are increased in the cerebrospinal fluid of patients with multiple sclerosis: no correlation with fatigue and sleepiness. J Neurol Sci. (2011) 307:127–31. doi: 10.1016/j.jns.2011.04.024
25. Giovannoni G, Thompson AJ, Miller DH, Thompson EJ. Fatigue is not associated with raised inflammatory markers in multiple sclerosis. Neurology. (2001) 57:676–81. doi: 10.1212/WNL.57.4.676
26. Adamczyk-Sowa M, Sowa P, Adamczyk J, Niedziela N, Misiolek H, Owczarek M, et al. Effect of melatonin supplementation on plasma lipid hydroperoxides, homocysteine concentration and chronic fatigue syndrome in multiple sclerosis patients treated with interferons-beta and mitoxantrone. J Physiol Pharmacol. (2016) 67:235–42.
27. Lefaucheur JP, André-Obadia N, Antal A, Ayache SS, Baeken C, Benninger DH, et al. Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS). Clin Neurophysiol. (2014) 125:2150–206. doi: 10.1016/j.clinph.2014.05.021
28. Lefaucheur JP, Antal A, Ayache SS, Benninger DH, Brunelin J, Cogiamanian F, et al. Evidence-based guidelines on the therapeutic use of transcranial direct current stimulation (tDCS). Clin Neurophysiol. (2017) 128:56–92. doi: 10.1016/j.clinph.2016.10.087
29. Lefaucheur JP, Aleman A, Baeken C, Benninger DH, Brunelin J, Di Lazzaro V, et al. Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS): an update (2014-2018). Clin Neurophysiol. (2020) 131:474–528. doi: 10.1016/j.clinph.2019.11.002
30. Rossi S, Antal A, Bestmann S, Bikson M, Brewer C, Brockmöller J, et al. Safety and recommendations for TMS use in healthy subjects and patient populations, with updates on training, ethical and regulatory issues: expert guidelines. Clin Neurophysiol. (2021) 132:269–306. doi: 10.1016/j.clinph.2020.10.003
31. Rossini PM, Berardelli A, Deuschl G, Hallett M, Maertens de Noordhout AM, Paulus W, et al. Applications of magnetic cortical stimulation. The international federation of clinical neurophysiology. Electroencephalogr Clin Neurophysiol Suppl. (1999) 52:171–85.
32. Rossini PM, Burke D, Chen R, Cohen LG, Daskalakis Z, Di Iorio R, et al. Non-invasive electrical and magnetic stimulation of the brain, spinal cord, roots and peripheral nerves: Basic principles and procedures for routine clinical and research application. An updated report from an IFCN Committee. Clin Neurophysiol. (2015) 126:1071–107. doi: 10.1016/j.clinph.2015.02.001
33. Groppa S, Oliviero A, Eisen A, Quartarone A, Cohen LG, Mall V, et al. A practical guide to diagnostic transcranial magnetic stimulation: report of an IFCN committee. Clin Neurophysiol. (2012) 123:858–82. doi: 10.1016/j.clinph.2012.01.010
34. Coates KD, Aboodarda SJ, Krüger RL, Martin T, Metz LM, Jarvis SE, et al. Multiple sclerosis-related fatigue: the role of impaired corticospinal responses and heightened exercise fatigability. J Neurophysiol. (2020) 124:1131–43. doi: 10.1152/jn.00165.2020
35. Mordillo-Mateos L, Soto-Leon V, Torres-Pareja M, Peinado-Palomino D, Mendoza-Laiz N, Alonso-Bonilla C, et al. Fatigue in multiple sclerosis: general and perceived fatigue does not depend on corticospinal tract dysfunction. Front Neurol. (2019) 10:339. doi: 10.3389/fneur.2019.00339
36. Liepert J, Mingers D, Heesen C, Bäumer T, Weiller C. Motor cortex excitability and fatigue in multiple sclerosis: a transcranial magnetic stimulation study. Mult Scler. (2005) 11:316–21. doi: 10.1191/1352458505ms1163oa
37. Chalah MA, Kauv P, Créange A, Hodel J, Lefaucheur JP, Ayache SS. Neurophysiological, radiological and neuropsychological evaluation of fatigue in multiple sclerosis. Mult Scler Relat Disord. (2019) 28:145–52. doi: 10.1016/j.msard.2018.12.029
38. Chaves AR, Kelly LP, Moore CS, Stefanelli M, Ploughman M. Prolonged cortical silent period is related to poor fitness and fatigue, but not tumor necrosis factor, in multiple sclerosis. Clin Neurophysiol. (2019) 130:474–83. doi: 10.1016/j.clinph.2018.12.015
39. Morgante F, Dattola V, Crupi D, Russo M, Rizzo V, Ghilardi MF, et al. Is central fatigue in multiple sclerosis a disorder of movement preparation? J Neurol. (2011) 258:263–72. doi: 10.1007/s00415-010-5742-x
40. Russo M, Crupi D, Naro A, Avanzino L, Buccafusca M, Dattola V, et al. Fatigue in patients with multiple sclerosis: from movement preparation to motor execution. J Neurol Sci. (2015) 351:52–7. doi: 10.1016/j.jns.2015.02.031
41. Russo M, Calamuneri A, Cacciola A, Bonanno L, Naro A, Dattola V, et al. Neural correlates of fatigue in multiple sclerosis: a combined neurophysiological and neuroimaging approach (R1). Arch Ital Biol. (2017) 155:142–51. doi: 10.12871/00039829201735
42. Petajan JH, White AT. Motor-evoked potentials in response to fatiguing grip exercise in multiple sclerosis patients. Clin Neurophysiol. (2000) 111:2188–95. doi: 10.1016/S1388-2457(00)00469-7
43. Perretti A, Balbi P, Orefice G, Trojano L, Marcantonio L, Brescia-Morra V, et al. Post-exercise facilitation and depression of motor evoked potentials to transcranial magnetic stimulation: a study in multiple sclerosis. Clin Neurophysiol. (2004) 115:2128–33. doi: 10.1016/j.clinph.2004.03.028
44. Huang YZ, Rothwell JC, Chen RS, Lu CS, Chuang WL. The theoretical model of theta burst form of repetitive transcranial magnetic stimulation. Clin Neurophysiol. (2011) 122:1011–8. doi: 10.1016/j.clinph.2010.08.016
45. Conte A, Li Voti P, Pontecorvo S, Quartuccio ME, Baione V, Rocchi L, et al. Attention-related changes in short-term cortical plasticity help to explain fatigue in multiple sclerosis. Mult Scler. (2016) 22:1359–66. doi: 10.1177/1352458515619780
46. Colombo B, Martinelli Boneschi F, Rossi P, Rovaris M, Maderna L, Filippi M, et al. MRI and motor evoked potential findings in nondisabled multiple sclerosis patients with and without symptoms of fatigue. J Neurol. (2000) 247:506–9. doi: 10.1007/s004150070148
47. Romani A, Bergamaschi R, Candeloro E, Alfonsi E, Callieco R, Cosi V. Fatigue in multiple sclerosis: multidimensional assessment and response to symptomatic treatment. Mult Scler. (2004) 10:462–8. doi: 10.1191/1352458504ms1051oa
48. Santarnecchi E, Rossi S, Bartalini S, Cincotta M, Giovannelli F, Tatti E, et al. Neurophysiological correlates of central fatigue in healthy subjects and multiple sclerosis patients before and after treatment with amantadine. Neural Plast. (2015) 2015:616242. doi: 10.1155/2015/616242
49. Scheidegger O, Kamm CP, Humpert SJ, Rösler KM. Corticospinal output during muscular fatigue differs in multiple sclerosis patients compared to healthy controls. Mult Scler. (2012) 18:1500–6. doi: 10.1177/1352458512438722
50. Thickbroom GW, Sacco P, Faulkner DL, Kermode AG, Mastaglia FL. Enhanced corticomotor excitability with dynamic fatiguing exercise of the lower limb in multiple sclerosis. J Neurol. (2008) 255:1001–5. doi: 10.1007/s00415-008-0818-6
51. Chaves AR, Wallack EM, Kelly LP, Pretty RW, Wiseman HD, Chen A, et al. Asymmetry of brain excitability: a new biomarker that predicts objective and subjective symptoms in multiple sclerosis. Behav Brain Res. (2019) 359:281–91. doi: 10.1016/j.bbr.2018.11.005
52. Nourbakhsh B, Revirajan N, Morris B, Cordano C, Creasman J, Manguinao M, et al. Safety and efficacy of amantadine, modafinil, and methylphenidate for fatigue in multiple sclerosis: a randomised, placebo-controlled, crossover, double-blind trial. The Lancet Neurology. (2021) 20:38–48. doi: 10.1016/S1474-4422(20)30354-9
53. Miller E, Kostka J, Włodarczyk T, Dugué B. Whole-body cryostimulation (cryotherapy) provides benefits for fatigue and functional status in multiple sclerosis patients. A case-control study. Acta Neurol Scand. (2016) 134:420–6. doi: 10.1111/ane.12557
54. Chalah MA, Ayache SS. Cognitive behavioral therapies and multiple sclerosis fatigue: a review of literature. J Clin Neurosci. (2018) 52:1–4. doi: 10.1016/j.jocn.2018.03.024
55. Ayache SS, Chalah MA. Transcranial direct current stimulation: a glimmer of hope for multiple sclerosis fatigue? J Clin Neurosci. (2018) 55:10–12. doi: 10.1016/j.jocn.2018.06.002
56. Tecchio F, Cancelli A, Cottone C, Zito G, Pasqualetti P, Ghazaryan A, et al. Multiple sclerosis fatigue relief by bilateral somatosensory cortex neuromodulation. J Neurol. (2014) 261:1552–8. doi: 10.1007/s00415-014-7377-9
57. Tecchio F, Cancelli A, Cottone C, Ferrucci R, Vergari M, Zito G, et al. Brain plasticity effects of neuromodulation against multiple sclerosis fatigue. Front Neurol. (2015) 6:141. doi: 10.3389/fneur.2015.00141
58. Ferrucci R, Vergari M, Cogiamanian F, Bocci T, Ciocca M, Tomasini E, et al. Transcranial direct current stimulation (tDCS) for fatigue in multiple sclerosis. NeuroRehabilitation. (2014) 34:121–7. doi: 10.3233/NRE-131019
59. Cancelli A, Cottone C, Giordani A, Migliore S, Lupoi D, Porcaro C, et al. Personalized, bilateral whole-body somatosensory cortex stimulation to relieve fatigue in multiple sclerosis. Mult Scler. (2018) 24:1366–74. doi: 10.1177/1352458517720528
60. Saiote C, Goldschmidt T, Timäus C, Steenwijk MD, Opitz A, Antal A, et al. Impact of transcranial direct current stimulation on fatigue in multiple sclerosis. Restor Neurol Neurosci. (2014) 32:423–36. doi: 10.3233/RNN-130372
61. Ayache SS, Palm U, Chalah MA, Al-Ani T, Brignol A, Abdellaoui M, et al. Prefrontal tDCS decreases pain in patients with multiple sclerosis. Front Neurosci. (2016) 10:147. doi: 10.3389/fnins.2016.00147
62. Chalah MA, Riachi N, Ahdab R, Mhalla A, Abdellaoui M, Créange A, et al. Effects of left DLPFC versus right PPC tDCS on multiple sclerosis fatigue. J Neurol Sci. (2017) 372:131–7. doi: 10.1016/j.jns.2016.11.015
63. Chalah MA, Grigorescu C, Padberg F, Kümpfel T, Palm U, Ayache SS. Bifrontal transcranial direct current stimulation modulates fatigue in multiple sclerosis: a randomized sham-controlled study. J Neural Transm. (2020) 127:953–61. doi: 10.1007/s00702-020-02166-2
64. Mortezanejad M, Ehsani F, Masoudian N, Zoghi M, Jaberzadeh S. Comparing the effects of multi-session anodal trans-cranial direct current stimulation of primary motor and dorsolateral prefrontal cortices on fatigue and quality of life in patients with multiple sclerosis: a double-blind, randomized, sham-controlled trial. Clin Rehabil. (2020) 34:1103–11. doi: 10.1177/0269215520921506
65. Hanken K, Bosse M, Möhrke K, Eling P, Kastrup A, Antal A, et al. Counteracting fatigue in multiple sclerosis with right parietal anodal transcranial direct current stimulation. Front Neurol. (2016) 7:154. doi: 10.3389/fneur.2016.00154
66. Fiene M, Rufener KS, Kuehne M, Matzke M, Heinze HJ, Zaehle T. Electrophysiological and behavioral effects of frontal transcranial direct current stimulation on cognitive fatigue in multiple sclerosis. J Neurol. (2018) 265:607–17. doi: 10.1007/s00415-018-8754-6
67. Workman CD, Kamholz J, Rudroff T. Transcranial direct current stimulation (tDCS) for the treatment of a Multiple Sclerosis symptom cluster. Brain Stimul. (2020) 13:263–4. doi: 10.1016/j.brs.2019.09.012
68. Ayache SS, Lefaucheur JP, Chalah MA. Long term effects of prefrontal tDCS on multiple sclerosis fatigue: a case study. Brain Stimul. (2017) 10:1001–2. doi: 10.1016/j.brs.2017.05.004
69. Chalah MA, Lefaucheur JP, Ayache SS. Long-term effects of tDCS on fatigue, mood and cognition in multiple sclerosis. Clin Neurophysiol. (2017) 128:2179–80. doi: 10.1016/j.clinph.2017.08.004
70. Charvet LE, Dobbs B, Shaw MT, Bikson M, Datta A, Krupp LB. Remotely supervised transcranial direct current stimulation for the treatment of fatigue in multiple sclerosis: results from a randomized, sham-controlled trial. Clin Neurophysiol. (2018) 24:1760–9. doi: 10.1177/1352458517732842
71. Salemi G, Vazzoler G, Ragonese P, Bianchi A, Cosentino G, Croce G, et al. Application of tRNS to improve multiple sclerosis fatigue: a pilot, single-blind, sham-controlled study. J Neural Transm. (2019) 126:795–9. doi: 10.1007/s00702-019-02006-y
72. Palm U, Chalah MA, Padberg F, Al-Ani T, Abdellaoui M, Sorel M, et al. Effects of transcranial random noise stimulation (tRNS) on affect, pain and attention in multiple sclerosis. Restor Neurol Neurosci. (2016) 34:189–99. doi: 10.3233/RNN-150557
73. Mori F, Ljoka C, Magni E, Codecà C, Kusayanagi H, Monteleone F, et al. Transcranial magnetic stimulation primes the effects of exercise therapy in multiple sclerosis. J Neurol. (2011) 258:1281–7. doi: 10.1007/s00415-011-5924-1
74. Gaede G, Tiede M, Lorenz I, Brandt AU, Pfueller C, Dörr J, et al. Safety and preliminary efficacy of deep transcranial magnetic stimulation in MS-related fatigue. Neurol Neuroimmunol. NeuroInflammation. (2017) 5:e423. doi: 10.1212/NXI.0000000000000423
75. Korzhova J, Bakulin I, Sinitsyn D, Poydasheva A, Suponeva N, Zakharova M, et al. High-frequency repetitive transcranial magnetic stimulation and intermittent theta-burst stimulation for spasticity management in secondary progressive multiple sclerosis. Eur J Neurol. (2019) 26:680–e44. doi: 10.1111/ene.13877
76. Tramontano M, Grasso MG, Soldi S, Casula EP, Bonnì S, Mastrogiacomo S, et al. Cerebellar intermittent theta-burst stimulation combined with vestibular rehabilitation improves gait and balance in patients with multiple sclerosis: a preliminary double-blind randomized controlled trial. Cerebellum. (2020) 19:897–901. doi: 10.1007/s12311-020-01166-y
77. Palotai M, Cavallari M, Healy BC, Guttmann CR. A novel classification of fatigue in multiple sclerosis based on longitudinal assessments. Mult Scler. (2020) 26:725–34. doi: 10.1177/1352458519898112
78. Workman CD, Fietsam AC, Ponto LLB, Kamholz J, Rudroff T. Individual cerebral blood flow responses to transcranial direct current stimulation at various intensities. Brain Sci. (2020) 10:855. doi: 10.3390/brainsci10110855
79. Ayache SS, Chalah MA. Cortical excitability changes: a mirror to the natural history of multiple sclerosis? Neurophysiol Clin. (2017) 47:221–3. doi: 10.1016/j.neucli.2017.02.001
80. McLaren ME, Nissim NR, Woods AJ. The effects of medication use in transcranial direct current stimulation: a brief review. Brain Stimul. (2018) 11:52–8. doi: 10.1016/j.brs.2017.10.006
Keywords: multiple sclerosis, fatigue, neuromodulation, corticospinal excitability, tDCS, TMS, tRNS
Citation: Ayache SS, Serratrice N, Abi Lahoud GN and Chalah MA (2022) Fatigue in Multiple Sclerosis: A Review of the Exploratory and Therapeutic Potential of Non-Invasive Brain Stimulation. Front. Neurol. 13:813965. doi: 10.3389/fneur.2022.813965
Received: 12 November 2021; Accepted: 28 March 2022;
Published: 28 April 2022.
Edited by:
Giancarlo Comi, San Raffaele Hospital (IRCCS), ItalyReviewed by:
Giulia Paparella, Mediterranean Neurological Institute Neuromed (IRCCS), ItalyLauren Krupp, New York University, United States
Copyright © 2022 Ayache, Serratrice, Abi Lahoud and Chalah. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Samar S. Ayache, c2FtYXJheWFjaGVAZ21haWwuY29t; Moussa A. Chalah, bW91c3NhY2hhbGFoQGdtYWlsLmNvbQ==