 Tim J. Hallenberger
Tim J. Hallenberger Raphael Guzman
Raphael Guzman Leo H. Bonati2,4
Leo H. Bonati2,4 Ladina Greuter
Ladina Greuter
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Neurol. , 20 December 2022
Sec. Stroke
Volume 13 - 2022 | https://doi.org/10.3389/fneur.2022.1054106
Introduction: Treatment for spontaneous supratentorial intracerebral haemorrhage (SSICH) is limited and consist of either best medical treatment (BMT) or surgical hematoma evacuation. Treatment methods and choice of surgical technique are debated, and so far, no clear advantage of endoscopic surgery (ES) over conventional craniotomy (CC) or BMT was shown. The aim of this systematic review and meta-analysis was to investigate the differences in outcome, morbidity, and mortality between ES and CC or BMT.
Methods: We systematically searched Embase and PubMed databases for randomised controlled trials comparing ES to CC or BMT. The primary outcome was favourable functional outcome after 6 months. Secondary outcomes were morbidity and mortality rates and duration of surgery.
Results: Seven articles were eligible for the outcome analysis with 312 subjects in the control (216 CC, 96 BMT) and 279 in the treatment group (ES). Compared to BMT, ES showed significantly improved favourable functional outcome (RR 1.93 [1.12; 3.33], p = 0.02) and mortality rates (RR 0.63 [0.44; 0.90], p = 0.01). No significant difference in favourable functional outcome and mortality was seen in ES compared to CC (RR 2.13 [0.01; 737], p = 0.35; RR 0.42 [0.17; 1.05], p = 0.06). ES showed significantly lower morbidity (RR 0.41 [0.29; 0.58], p < 0.01), and overall infection rates (RR 0.33 [0.20; 0.54], p < 0.01) compared to CC. Duration of surgery was significantly shorter for ES compared to CC (SMD −3.17 [−4.35; −2.00], p < 0.01).
Conclusion: ES showed significantly improved favourable functional outcome and mortality rates compared to BMT while showing reduced length of surgery and lower complication rates compared to CC. Therefore, ES appears a promising approach for treatment of SSICH justifying further prospective trials.
Systematic review registration: PROSPERO, identifier: CRD42020181018.
Spontaneous supratentorial intracerebral haemorrhage (SSICH) accounts for approximately 9–27% of all strokes, affecting more than 5 million people worldwide annually (1). In total of 60–70% are caused by hypertension and 5–20% are related to amyloid angiopathy and other non-structural reasons (2, 3). It is most commonly located in the basal ganglia but can also be of lobar origin (4, 5). Clinical outcome is often poor and known to be influenced by the primary hematoma volume, hematoma expansion, neurotoxic metabolites, as well as oedema (4). SSICH is associated with a 30-day mortality rate of up to 40% (6–9). Current treatment recommendations can be divided into best medical treatment (BMT), which is a combination of early SSICH diagnosis, strict blood pressure control, reversal of anticoagulation and in-patient management in dedicated stroke units or intensive care units, or into surgical evacuation of the hematoma (10, 11). The mainstay of surgical treatment is a reduction of the hematoma volume resulting in a reduction of the mass effect and prevention of secondary neurotoxic injury caused by haemoglobin breakdown metabolites (4, 12). Surgical hematoma evacuation can be achieved through conventional craniotomy (CC) or minimal invasive surgery (MIS), including hematoma reduction through catheter-based infusion of rtPA and endoscopic surgery (ES) (10, 11, 13). Decompressive craniectomy might reduce mortality in patients suffering mass effect due to severe SSICH by simply reducing intracranial pressure without evacuation of the clot (10). Despite several large randomised controlled trials (RCTs) comparing various surgical techniques to BMT, current treatment recommendations and guidelines are lacking consensus on whether, and if so, which surgical treatment should be applied in SSICH (10, 13–17). Over the years, several different systematic reviews with meta-analyses were carried out comparing various MIS techniques to CC or BMT, most recently by Scaggiante et al. (18), Yao et al. (19), Nam et al. (20), Zhao et al. (21), Guo et al. (22), Li et al. (23), Sondag et al. (24), and Hou et al. (25). Despite also reporting ES as main surgical technique or as a technique in a subgroup analysis, all previous works either mixed ES with other MIS techniques as the experimental group or compared ES to both BMT and CC as a combined comparator, effectively creating a mixture of different treatments in the control group, possibly limiting the generalizability of the results (18–24). The aim of this systematic review and meta-analysis was to investigate endoscopic hematoma evacuation in comparison to either CC and BMT separately regarding functional clinical outcome, morbidity, and mortality.
We used a search string with the keywords “spontaneous intracerebral haemorrhage” and “endoscopic surgery” in both PubMed and Embase databases including studies published until the 1st of June 2020 (Supplementary Figure 1). After removal of duplicates, titles and abstracts of remaining articles were reviewed by two of the authors independently (TJH and LG). In a second step, full text publications of selected abstracts were independently reviewed by the same authors, based on which a final list of eligible studies was compiled. The reference lists of the final articles were searched manually for further eligible studies. In case of disagreement on the inclusion of a study a third researcher (JS) took a final decision. Data were extracted from the included studies by two researchers (TJH, LG) and compiled to a final data set for analysis.
We included RCTs fulfilling the following criteria:
1) Inclusion of spontaneous supratentorial ICH confirmed by imaging.
2) Comparison of ES to either BMT or CC.
3) Inclusion of patients >18 years of age.
4) Written in English.
We excluded studies according to the following criteria:
1) Inclusion of patients with a secondary hematoma due to a tumour, vascular lesion or malformation or traumatic causes.
2) Description of other forms of MIS than ES (e.g., stereotactic aspiration or catheter lysis).
3) Not an RCT.
The primary outcome measure was favourable functional outcome at 6 months. Favourable functional outcome was defined as a modified Rankin Scale (mRS) of 0–3 points, a Barthel Index (BI) of ≥70 or an Activity of Daily Living (ADL) score of 1–3, respectively and a Glasgow Outcome Scale (GOS) of 4–5 Points. Due to inconsistency of the reported outcome measures among the studies, we chose to use the four most frequently reported scores to assess favourable functional outcome. Thresholds for the BI and ADL were chosen in accordance with the literature and the current consensus (26–28). For the GOS, scores 4 and 5 were chosen as they are quite similar to mRS 1–3 (29).
Secondary outcomes were mortality, morbidity, postoperative residual hematoma volume (defined as the hematoma volume after intervention in millilitres), hematoma evacuation rate (defined as the difference of hematoma volume before and after surgery calculated as percentage), and the duration of surgery (in minutes). Morbidity consisted of re-bleeding, seizure, revision surgery, and infection (including pulmonary infection, surgical site infection (SSI), and central nervous system (CNS) infections). We compared ES to CC and BMT individually. The pooled outcome analysis for hematoma evacuation rate, postoperative hematoma volume and the temporal evolution of mortality rates was initially not planned in the protocol but was added as exploratory analyses.
We used the revised Risk of Bias (RoB 2) tool to evaluate the included studies (30). The RoB 2 tool is the recommended tool to assess risk of bias in RCTs by the Cochrane Collaboration and covers all aspect of trial design, conduct and reporting (30). Quality assessment was carried out independently by two authors (TJH and LG) and compared thereafter. This review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (31) and was registered at PROSPERO under the registration number CRD42020181018. No ethical approval was needed for the present study.
Relative risk ratio (RR) was used as an effect measurement for the pooled outcomes. Confidence intervals (CI) and p-values were calculated for each outcome. Results with p<0.05 were considered statistically significant. To identify influential studies distorting the primary outcome, a leave-one-out analysis was performed. If low heterogeneity (I2<50%) was present, we used fixed-effects models, while otherwise the random-effects models were used. Forest plots were generated for each outcome parameter to evaluate publication bias. All statistical analyses were done using R statistical software (version 4.0.2, 2020, The R foundation, U.S.A) using the dmetar package (32).
A total of 932 articles were identified of which seven met the eligibility criteria, with a total of 591 patients, 312 subjects (52.8%) in the control group (216 subjects with CC and 96 subjects with BMT) and 279 subjects (47.2%) in the treatment group (ES) (Figure 1). ES was compared to BMT in three studies (33–35) and to CC in four studies, respectively (36–39) (Table 1). One RCT comparing ES to BMT to develop a modified intracerebral haemorrhage score and identify optimal cut-offs for surgical vs. conservative treatment in basal ganglia haemorrhage was reviewed and excluded since the primary outcome of the respective study did not compare the treatment modalities itself but rather when to apply them based on the score (40).
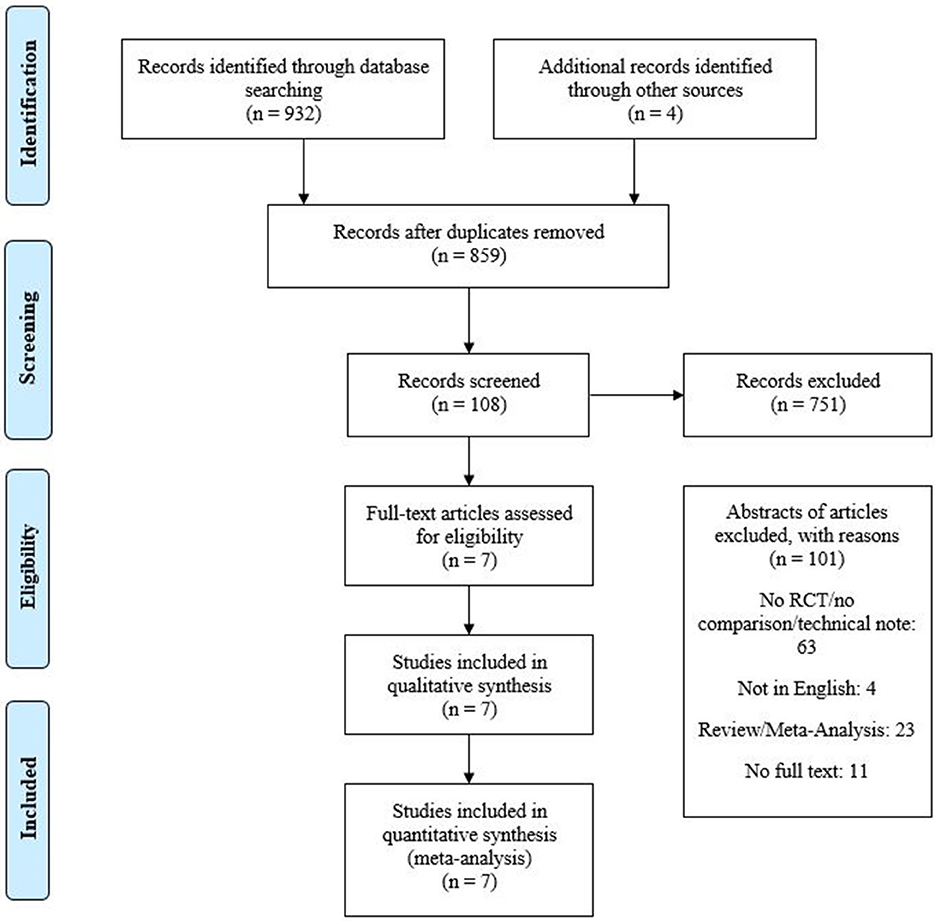
Figure 1. Flowchart of the study selection process according to the PRISMA guidelines.
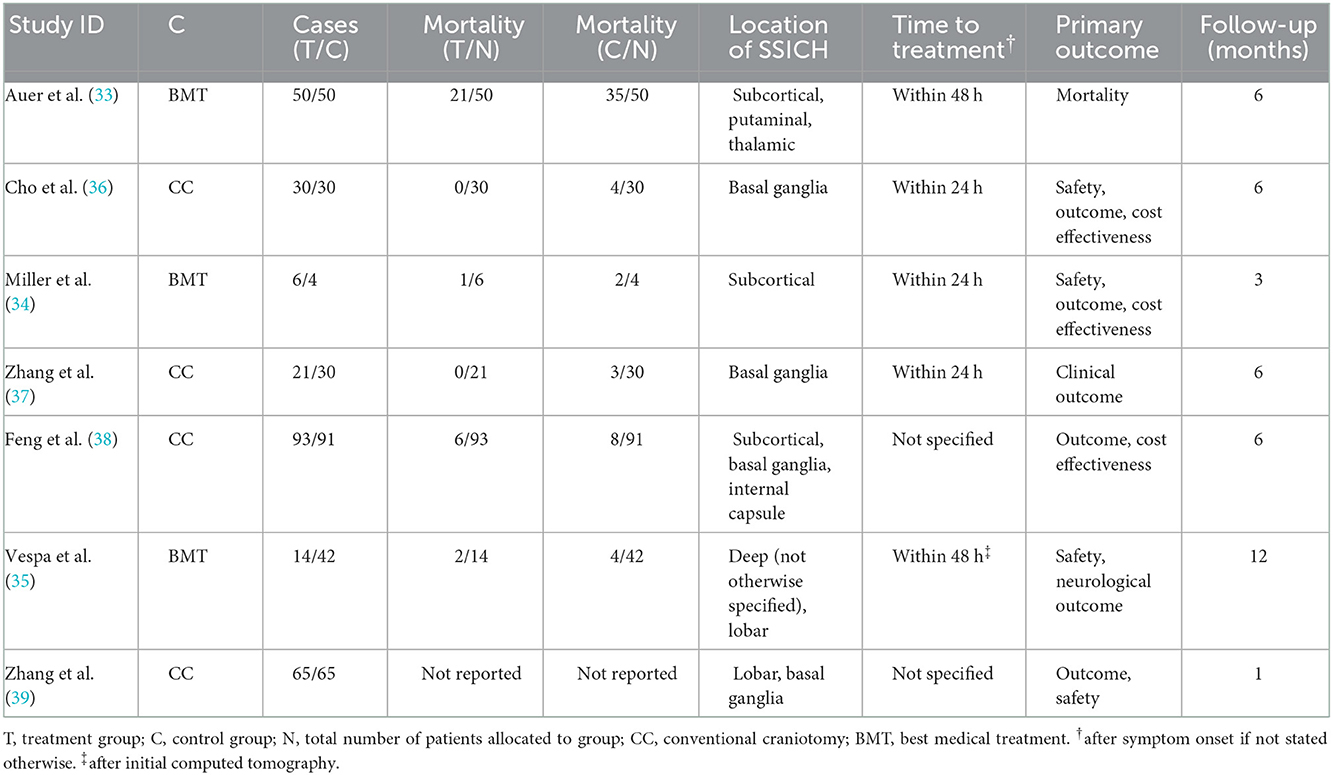
Table 1. Characteristics of the included studies.
Favourable functional outcome 6 months after treatment was reported in five of the seven included studies showing an overall rate of 38.3% (33, 35, 37, 38). ES showed a statistically significant higher rate of favourable functional outcome compared to BMT (p = 0.02, Table 2, Figure 2A). No significantly influential study was identified for ES vs. BMT after the “leave-one-out” method. Comparing ES to CC, a non-significant higher favourable functional outcome rate for ES with a moderate to high heterogeneity was observed (p = 0.35, Table 2, Figure 2B). After applying the “leave-one-out” method, Feng et al. (38) was identified as the influential study for ES vs. CC, however no pooled outcome analysis was possible as only one study remained for the analysis (37).
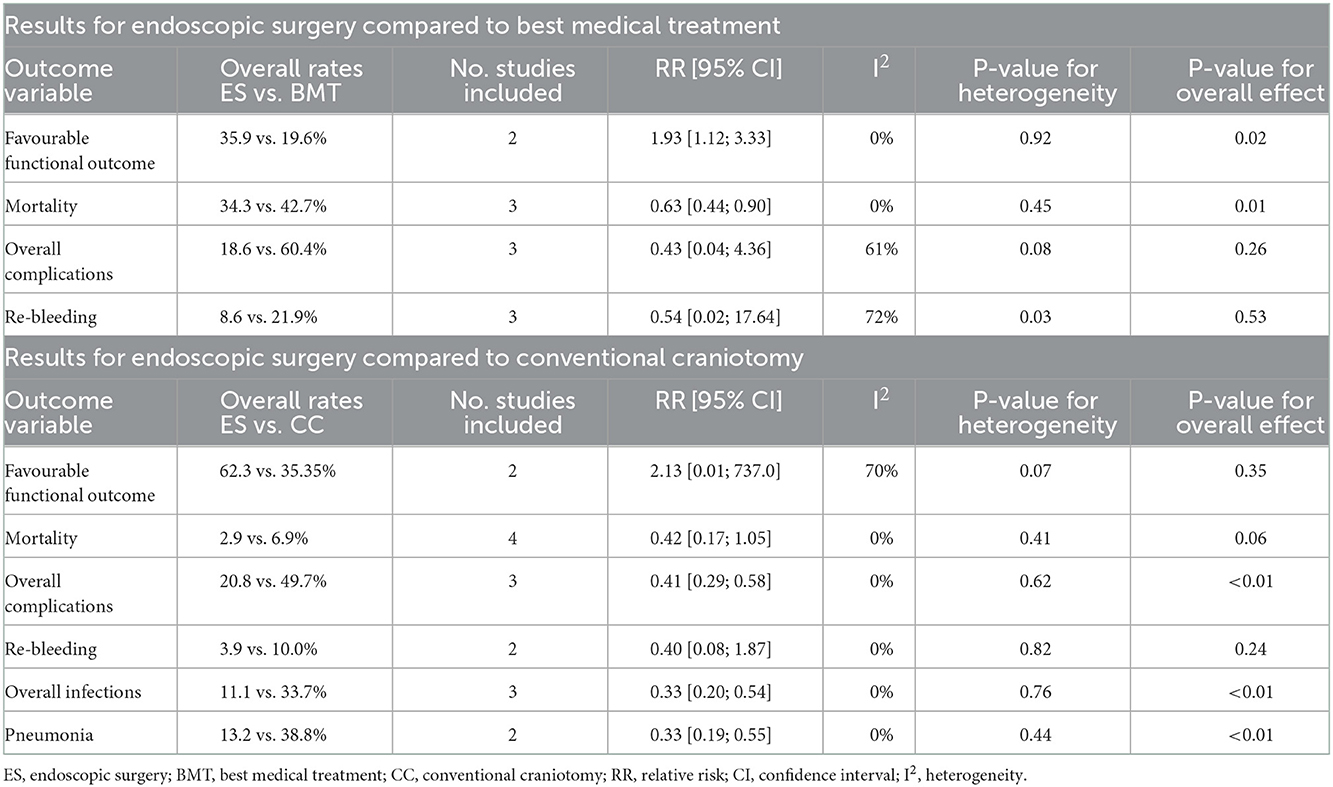
Table 2. Results of the meta-analysis for ES compared to BMT and CC.

Figure 2. (A) Forest plots of favourable functional outcome endoscopic surgery (ES) vs. best medical treatment (BMT). (B) Favourable functional outcome ES vs. CC. (C) Mortality rates ES vs. BMT. (D) Mortality rates ES vs. CC.
Mortality was reported in all of the included studies showing an overall rate of 21.7% (33–39). A significantly lower rate of mortality was observed for ES compared to BMT (p = 0.01, Table 2, Figure 2C). ES compared to CC showed a non-significantly lower mortality rate (p = 0.06, Table 2, Figure 2D). Mortality for ES was reported in four studies. Auer et al. reported a mortality rate of 42% (21/50), Miller et al. of 20% (1/6), Vespa et al. of 14% (2/14) and Feng et al. of 6% (6/93) for ES (33–35, 38). Cho et al., Zhang et al., and Zhang et al. reported no fatalities for ES (37, 39, 40). Mortality for CC was reported in three studies. Cho et al. reported a mortality rate of 13% (4/30), Zhang et al. of 10% (3/30) and Feng et al. of 9% (8/91) (37, 38, 40). Zhang et al. reported no fatalities (39). Mortality for BMT was reported in three studies. Auer et al. reported mortality rates of 70% (35/50), Miller et al. of 50% (2/4) and Vespa et al. of 10% (4/42) (33–35).
Morbidity was reported in six out of seven studies (33–38). Overall complication rate was 37.4% and significantly lower in ES than in CC (p < 0.01, Table 2, Supplementary Figure 2B). In contrast to BMT, ES showed a lower rate of overall complications but did not reach statistical significance (p = 0.26, Table 2, Supplementary Figure 2A).
Re-bleeding rate was reported in five studies (33–37). The overall re-bleeding rate was 11.1% and when ES was compared to CC or BMT no significant difference was observed (p = 0.24 and p = 0.53 respectively, Table 2, Supplementary Figures 3A, B).
The overall infection rate was 25.5% and was reported in four studies (35–38). Comparing ES to CC, a significantly lower rate of overall infections (p < 0.01, Table 2, Supplementary Figure 3C) and a lower rate of pneumonia (p < 0.01, Table 2, Supplementary Figure 3D) was observed. Regarding CNS infections and surgical site infections (SSI), no pooled outcome analysis was possible as only one study per control group reported these outcome measures (35–37).
Seizure rates were reported in two out of seven studies with a total rate of 26.0% (35, 38). However, no pooled outcome analysis was possible, because the two studies reporting seizure rates, each belonged to a different control group (35, 38).
Three of the included seven studies [one being compared to BMT (35)] analysed the postoperative hematoma volume [7.89 ml (±6.53) for ES vs. 15.02 ml (±10.06) for CC] while five studies [one being compared to BMT (34)] compared the hematoma evacuation rate [86.02% (±10.53) for ES vs. 77.6% (±4.79) for CC] after intervention (34–39). No difference in the hematoma evacuation rate nor the postoperative hematoma volume was found when comparing ES to CC with significant heterogeneity was observed (p = 0.07 and p = 0.44 respectively, Table 3, Supplementary Figures 4A, B).
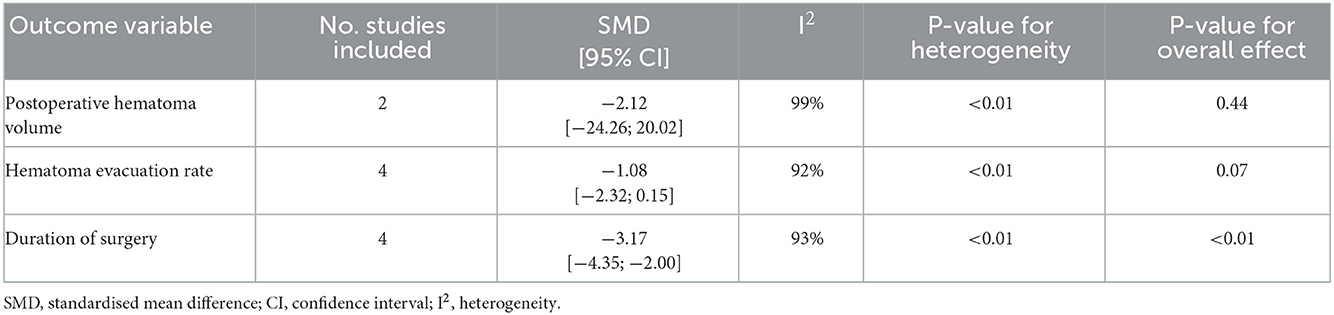
Table 3. Results of the meta-analysis for ES compared to CC.
Duration of surgery was reported in four studies (36–39). ES had an average duration of surgery of 123.39 (±36.62) minutes in contrast to 273.78 (±85.55) minutes for CC. Pooled outcome analysis showed significantly shorter duration of surgery for ES vs. CC with significant heterogeneity (p < 0.01, Table 3, Supplementary Figure 4C).
Time to surgery was similar among the different studies (Table 1). All but two (38, 39) reported a treatment window, which was within 72 h (33–39). Three studies (34, 36, 37) defined a maximum treatment window of 24 h while two studies (33, 35) allowed a treatment window of 48 h. However, most patients in the latter two studies, were treated within 18–29 h after symptom onset (34, 35, 37). Only one of the included studies, reported “ultra-early” clot evacuation, in which patients were treated within the first 60–100 min after hospital admission (36). Due to the similarity of the described treatment windows in the included studies, no pooled outcome analysis was conducted. A regression analysis between time to treatment and mortality showed no significant association (p = 0.891) (34–36).
We assessed a low overall risk of bias in two studies (35, 38), an intermediate risk of bias in four studies (34, 36, 37, 39), and a high risk of bias in one study (33). Risk of bias analysis for the included studies is shown in Figure 3.
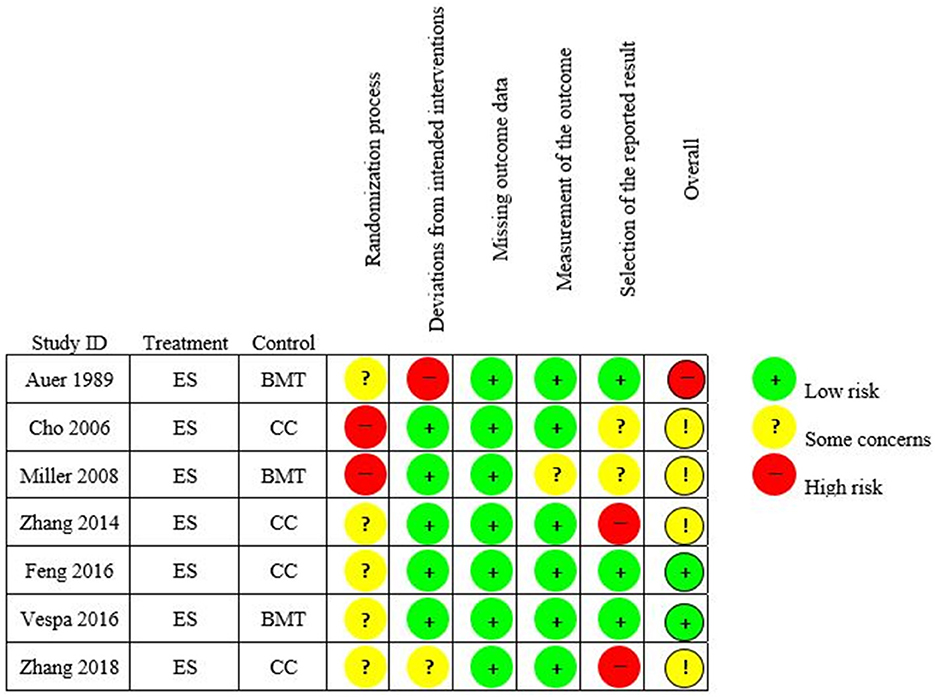
Figure 3. Risk of bias analysis (Rob-2) traffic light plot for the included studies.
Our meta-analysis of the existing RCTs comparing endoscopic surgery additionally to best medical treatment to conventional craniotomy or best medical treatment alone (ES to CC or BMT) in the treatment of spontaneous supratentorial intracerebral haemorrhage (SSICH) showed that ES had a significantly higher rate of favourable functional outcome and lower 6-month mortality rate compared to BMT. Overall morbidity was significantly lower for ES compared to CC. A significantly shorter duration of surgery and non-significant smaller postoperative hematoma volume was observed for ES in contrast to CC.
Several large RCTs were conducted in the past decades investigating surgical treatment of SSICH (13–15, 17), but the role of surgery in SSICH has remained controversial (10, 16). The STICH trial included various forms of SSICH, including deep-seated and intraventricular haematomas, for which the surgeon had uncertainty concerning the choice of treatment, while STICH II only included superficial lobar haemorrhages (14, 15). However, both the STICH and STICH II trial failed to show superiority of surgical hematoma evacuation compared to BMT concerning favourable functional outcome (14, 15). In the STICH trial, 75% of all hematomas were evacuated by craniotomy and microscopic hematoma removal, while only 7% of the hematomas were evacuated endoscopically (14).
Endoscopic surgery for SSICH was first proposed by Auer et al. (33). According to their publication, the benefit of ES regarding functional recovery and mortality rates applied only to a specific subgroup of younger and healthier patients with small hematomas (33). In the past decades, several other MIS methods, including stereotactic clot aspiration, minimally invasive catheter evacuation and lysis therapy (MISTIE) or minimally invasive puncture surgery (MIPS), were compared to BMT but all failed to show a significant difference in favourable functional primary outcome analysis (11, 17). Furthermore, different meta-analyses were carried out comparing various MIS techniques to CC or BMT, resulting in different results for the respective techniques (18–25). These publications analyse mostly RCTs but also prospective and retrospective cohort studies. Further, they report ES either as main surgical technique or as a subgroup analysis but compare it to both BMT and CC combined, effectively creating a mixture of different treatments in the control group possibly limiting the generalizability of the results (18–25). To our knowledge, we present the first meta-analysis including solely RCTs of ES compared to either CC or BMT separately for the treatment of SSICH.
Our results showed a significantly higher rate of favourable functional outcome (mRS ≤ 3) for ES compared to BMT. A network meta-analysis by Guo et al. (22) comparing four interventions (BMT, ES, CC and minimally invasive puncture surgery), also observed a higher rate of favourable functional outcome in the ES group than in the BMT group. However, favourable functional outcome was defined differently in their meta-analysis with a cut off of mRS ≤ 2 (22). The observed difference in favourable functional outcome of ES and BMT might be due to a faster hematoma evacuation achieved with surgery, reducing the mass effect and disposing of neurotoxic hematoma metabolites. These were shown to negatively affect the cerebral tissue and induce brain oedema and apoptosis due to formation of reactive oxygen species (4). We assume that the evacuation of blood itself influences the outcome more than the surgical method chosen, and therefore no difference in favourable functional outcome between ES and CC was observed. However, ES is less invasive than CC, resulting in less injury of the surrounding brain tissue and shorter surgery time, which might lead to better surgical results (41).
Based on our data ES showed reduced mortality rates when compared to BMT. However, compared to CC no statistically significant difference was reached. This might indicate that hematoma evacuation, irrespective of the surgical technique, could reduce mortality by treating the mass effect, which ultimately can cause death if left untreated (4). In accordance with our results, Yao et al. described a significantly lower mortality rate for ES compared to BMT but also to CC in their meta-analysis (19). Contrary to our analysis, Yao et al. also included retrospective cohort studies and other forms of MIS and thus had a bigger sample size, which could lead to a higher heterogeneity in their data and the reported difference in outcome (19). We observed decreasing mortality rates for ES over time in the included studies (6–42%), while the mortality rates for BMT and CC remained unchanged around 43 and 8% over the time span of the different studies. We assume, that the decrease of mortality rates over time could be due to the growing experience and technological advances in ES over the years. In our analysis, we observed higher percentages of mortality in ES vs. BMT compared to ES vs. CC which could be either due to the higher number of patients included in the analysis of ES vs. CC (425) compared to ES vs. BMT (166) or due to the high mortality rate in Auer et al. (33).
Overall morbidity for ES described within the literature is rather low (8–10%) (36–38). This could be due to the improved intracavitary vision during ES. ES allows clot removal under full visual sight, and through a minimal invasive approach which could lead to the observed higher evacuation rate of ES compared to CC (42). Additionally, improved vision could not only lead to a more efficient evacuation of the clot but also improved haemostasis. In our analysis, no significant difference between ES and CC was observed concerning evacuation rates.
A common complication after SSICH are infections with reported rates of 23–38% (43, 44). We observed a significantly lower rate of any kind of infection in ES compared to CC. However, since data on the comparison of surgical site and CNS infections within the included reports is limited, most of the observed effect is attributable to reduced rates of extracranial infections. Nevertheless, ES potentially leads to less surgical site infections due to the smaller incision or the observed significantly shorter duration of surgery for ES. As proposed by Patir et al. in a prospective study, a prolonged surgery time (>4 h) significantly increases the rate of postoperative infections in neurosurgical patients (45). Hence, keeping the surgical time short appears to be of paramount importance for these patients, as severe infection could lead to worse outcome in these already frail patients.
In accordance with the well-known treatment paradigm “time is brain” in ischemic stroke, it was shown that earlier hematoma evacuation (within 24 h) could lead to a 2.8 times higher rate of functional independence compared to a prolonged evacuation period (>72 h) (18, 46). This was also suggested by a subgroup analysis of MISTIE III, which showed a trend towards better outcome in early hematoma evacuation (within 36 h) compared to later evacuation (>36 h) (17). To note, however, that ultra-early hematoma evacuation (< 4–7 h after symptom onset) was shown to be associated with a significantly higher risk of re-bleeding and a higher rate of mortality (47–49). From all the included studies only one reported ultra-early clot evacuation and no higher re-bleeding rate was observed (36). The worse outcome in ultra-early surgery could be due to diffuse bleeding and due to the poorly controlled hypertension within the 1st h after SSICH, which make a thorough haemostasis challenging. However, the literature is controversial on this topic (50). Early hematoma evacuation (after 12–24 h) is probably beneficial for achieving a good outcome in SSICH; however, further well-designed trials are needed to determine the optimal timing for surgery.
Despite conducting a systematic review and meta-analysis based solely on RCTs, this study presents some limitations. First, we observed substantial heterogeneity in the analysis of several endpoints, many of which included only few studies. Given, that much of the variance of those outcomes is likely attributable to differences in the studies themselves, the absence of difference between groups must be interpreted carefully since it might not represent the absence of a true treatment difference. Second, the primary outcome (favourable functional outcome) was reported in four different outcome measures and was measured at different time points which introduces a risk of bias and limits comparison (27, 28). Third, based on the available data, we were not able to compare the outcome between lobar and non-lobar, eloquent and non-eloquent as well as deep seated and superficial seated bleedings. This limits our results when it comes to these different type of bleedings. Forth, data concerning CNS infections and SSI was sparse. Therefore, infection rates within the analysis include intra- and extracranial infections, while the true outcome of CNS infections and SSI remains elusive. Further, we only searched two of the existing databases (PubMed and Embase) and only included studies in English, which carries a risk for selection bias. The described evolution of mortality rates for ES spans over several decades with varying technical expertise and should therefore be interpreted with care. Lastly, this study is not impervious to publication bias due to possible unpublished negative results, which are not included in this meta-analysis. However, to our knowledge, this is the first meta-analysis based on RCTs solely comparing ES (and not any other forms of MIS), to CC and BMT separately.
To conclude, based on our pooled analysis, ES has a significantly higher rate of favourable functional outcome and lower rate of mortality compared to BMT. Further, ES showed significantly lower overall complication rate, shorter surgery time, and non-significant higher hematoma evacuation rates compared to CC. ES seems to be a promising approach in the treatment of SSICH. Nevertheless, further sufficiently powered prospective trials analysing the benefit of early ES over BMT and other surgical treatment modalities for SSICH are warranted.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Conception and design: JS, LB, RG, and LG. Data curation, analysis, and interpretation of data: TH and LG. Statistical analysis and drafting the manuscript: TH, LG, and JS. Study supervision: LB, RG, and JS. Funding acquisition: LB. Critically revising the manuscript: All authors.
Funding for the current project was provided by the Swiss Heart Foundation (FF19092). The funders had no involvement with the study design, collection, analysis, interpretation of the data and the decision to submit the paper for publication.
TH receives a joint MD PhD Scholarship by the Swiss National Science Foundation and the Swiss Academy for Medical Sciences (SNF 323630_207030).
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2022.1054106/full#supplementary-material
BMT, Best medical treatment; CC, Conventional Craniotomy; ES, Endoscopic surgery; MIS, Minimally invasive surgery.
1. Feigin VL, Lawes CM, Bennett DA, Barker-Collo SL, Parag V. Worldwide stroke incidence and early case fatality reported in 56 population-based studies: a systematic review. Lancet Neurol. (2009) 8:355–69. doi: 10.1016/S1474-4422(09)70025-0
2. Biffi A, Greenberg SM. Cerebral amyloid angiopathy: a systematic review. J Clin Neurol. (2011) 7:1–9. doi: 10.3988/jcn.2011.7.1.1
3. Flower O, Smith M. The acute management of intracerebral hemorrhage. Curr Opin Crit Care. (2011) 17:106–14. doi: 10.1097/MCC.0b013e328342f823
4. Xi G, Keep RF, Hoff JT. Mechanisms of brain injury after intracerebral haemorrhage. Lancet Neurol. (2006) 5:53–63. doi: 10.1016/S1474-4422(05)70283-0
5. Rychen J, O'Neill A, Lai LT, Bervini D. Natural history and surgical management of spontaneous intracerebral hemorrhage: a systematic review. J Neurosurg Sci. (2020) 64:558–70. doi: 10.23736/S0390-5616.20.04940-1
6. Dennis MS. Outcome after brain haemorrhage. Cerebrovasc Dis. (2003) 16:9–13. doi: 10.1159/000069935
7. Feigin VL, Lawes CMM, Bennett DA, Anderson CS. Stroke epidemiology: a review of population-based studies of incidence, prevalence, case-fatality in the late 20th century. Lancet Neurol. (2003) 2:43–53. doi: 10.1016/S1474-4422(03)00266-7
8. Krishnamurthi RV, Feigin VL, Forouzanfar MH, Mensah GA, Connor M, Bennett DA, et al. Global and regional burden of first-ever ischaemic and haemorrhagic stroke during 1990-2010: findings from the Global Burden of Disease Study 2010. Lancet Glob Health. (2013) 1:e259–81. doi: 10.1016/S2214-109X(13)70089-5
9. Poon MT, Fonville AF, Al-Shahi Salman R. Long-term prognosis after intracerebral haemorrhage: systematic review and meta-analysis. J Neurol Neurosurg Psychiatry. (2014) 85:660–7. doi: 10.1136/jnnp-2013-306476
10. Hemphill III JC, Greenberg SM, Anderson CS, Becker K, Bendok BR, Cushman M, et al. Guidelines for the Management of Spontaneous Intracerebral Hemorrhage: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke. (2015) 46:2032–60. doi: 10.1161/STR.0000000000000069
11. Cordonnier C, Demchuk A, Ziai W, Anderson CS. Intracerebral haemorrhage: current approaches to acute management. Lancet. (2018) 392:1257–68. doi: 10.1016/S0140-6736(18)31878-6
12. Huang FP, Xi G, Keep RF, Hua Y, Nemoianu A, Hoff JT, et al. Brain edema after experimental intracerebral hemorrhage: role of hemoglobin degradation products. J Neurosurg. (2002) 96:287–93. doi: 10.3171/jns.2002.96.2.0287
13. Hanley DF, Thompson RE, Muschelli J, Rosenblum M, McBee N, Lane K, et al. Safety and efficacy of minimally invasive surgery plus alteplase in intracerebral haemorrhage evacuation (MISTIE): a randomised, controlled, open-label, phase 2 trial. Lancet Neurol. (2016) 15:1228–37. doi: 10.1016/S1474-4422(16)30234-4
14. Mendelow AD, Gregson BA, Fernandes HM, Murray GD, Teasdale GM, Hope DT, et al. Early surgery versus initial conservative treatment in patients with spontaneous supratentorial intracerebral haematomas in the International Surgical Trial in Intracerebral Haemorrhage (STICH): a randomised trial. Lancet. (2005) 365:387–97. doi: 10.1016/S0140-6736(05)70233-6
15. Mendelow AD, Gregson BA, Rowan EN, Murray GD, Gholkar A, Mitchell PM, et al. Early surgery versus initial conservative treatment in patients with spontaneous supratentorial lobar intracerebral haematomas (STICH II): a randomised trial. Lancet. (2013) 382:397–408. doi: 10.1016/S0140-6736(13)60986-1
16. Steiner T, Al-Shahi Salman R, Beer R, Christensen H, Cordonnier C, Csiba L, et al. European Stroke Organisation (ESO) guidelines for the management of spontaneous intracerebral hemorrhage. Int J Stroke. (2014) 9:840–55. doi: 10.1111/ijs.12309
17. Hanley DF, Thompson RE, Rosenblum M, Yenokyan G, Lane K, McBee N, et al. Efficacy and safety of minimally invasive surgery with thrombolysis in intracerebral haemorrhage evacuation (MISTIE III): a randomised, controlled, open-label, blinded endpoint phase 3 trial. Lancet. (2019) 393:1021–32. doi: 10.1016/S0140-6736(19)30195-3
18. Scaggiante J, Zhang X, Mocco J, Kellner CP. Minimally Invasive Surgery for Intracerebral Hemorrhage. Stroke. (2018) 49:2612–20. doi: 10.1161/STROKEAHA.118.020688
19. Yao Z, Hu X, You C, He M. Effect and feasibility of endoscopic surgery in spontaneous intracerebral hemorrhage: A systematic review and meta-analysis. World Neurosurg. (2018) 113:348–356.e2. doi: 10.1016/j.wneu.2018.02.022
20. Nam TM, Kim YZ. A meta-analysis for evaluating efficacy of neuroendoscopic surgery versus craniotomy for supratentorial hypertensive intracerebral hemorrhage. J Cerebrovasc Endovasc Neurosurg. (2019) 21:11–7. doi: 10.7461/jcen.2019.21.1.11
21. Zhao XH, Zhang SZ, Feng J, Li ZZ, Ma ZL. Efficacy of neuroendoscopic surgery versus craniotomy for supratentorial hypertensive intracerebral hemorrhage: A meta-analysis of randomized controlled trials. Brain Behav. (2019) 9:e01471. doi: 10.1002/brb3.1471
22. Guo G, Pan C, Guo W, Bai S, Nie H, Feng Y, et al. Efficacy and safety of four interventions for spontaneous supratentorial intracerebral hemorrhage: a network meta-analysis. J Neurointerv Surg. (2020). doi: 10.1136/neurintsurg-2019-015362
23. Li M, Mu F, Su D, Han Q, Guo Z, Chen T, et al. Different surgical interventions for patients with spontaneous supratentorial intracranial hemorrhage: A network meta-analysis. Clin Neurol Neurosurg. (2020) 188:105617. doi: 10.1016/j.clineuro.2019.105617
24. Sondag L, Schreuder F, Boogaarts HD, Rovers MM, Vandertop WP, Dammers R, et al. Neurosurgical Intervention for Supratentorial Intracerebral Hemorrhage. Ann Neurol. (2020) 88:239–50. doi: 10.1002/ana.25732
25. Hou D, Lu Y, Wu D, Tang Y, Dong Q. Minimally invasive surgery in patients with intracerebral hemorrhage: A meta-analysis of randomized controlled trials. Front Neurol. (2021) 12:789757. doi: 10.3389/fneur.2021.789757
26. Granger CV, Dewis LS, Peters NC, Sherwood CC, Barrett JE. Stroke rehabilitation: analysis of repeated Barthel index measures. Arch Phys Med Rehabil. (1979) 60:14–7.
27. Uyttenboogaart M, Stewart RE, Vroomen PC, De Keyser J, Luijckx GJ. Optimizing cutoff scores for the Barthel index and the modified Rankin scale for defining outcome in acute stroke trials. Stroke. (2005) 36:1984–7. doi: 10.1161/01.STR.0000177872.87960.61
28. Lee SY, Kim DY, Sohn MK, Lee J, Lee SG, Shin YI, et al. Determining the cut-off score for the Modified Barthel Index and the Modified Rankin Scale for assessment of functional independence and residual disability after stroke. PLoS ONE. (2020) 15:e0226324. doi: 10.1371/journal.pone.0226324
29. Jennett B, Bond M. Assessment of outcome after severe brain damage. Lancet. (1975) 1:480–4. doi: 10.1016/S0140-6736(75)92830-5
30. Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. (2019) 366:l4898. doi: 10.1136/bmj.l4898
31. Moher D, Liberati A, Tetzlaff J, Altman DG, The PG. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. (2009) 6:e1000097. doi: 10.1371/journal.pmed.1000097
32. Harrer M, Cuijpers P, Furukawa TA, Ebert DD. Doing Meta-Analysis in R: A Hands-on Guide. Chapman and Hall/CRC: PROTECT Lab Erlangen. (2019).
33. Auer LM, Deinsberger W, Niederkorn K, Gell G, Kleinert R, Schneider G, et al. Endoscopic surgery versus medical treatment for spontaneous intracerebral hematoma: a randomized study. J Neurosurg. (1989) 70:530–5. doi: 10.3171/jns.1989.70.4.0530
34. Miller CM, Vespa P, Saver JL, Kidwell CS, Carmichael ST, Alger J, et al. Image-guided endoscopic evacuation of spontaneous intracerebral hemorrhage. Surg Neurol. (2008) 69:441–6. doi: 10.1016/j.surneu.2007.12.016
35. Vespa P, Hanley D, Betz J, Hoffer A, Engh J, Carter R, et al. ICES (Intraoperative stereotactic computed tomography-guided endoscopic surgery) for brain hemorrhage: a multicenter randomized controlled trial. Stroke. (2016) 47:2749–55. doi: 10.1161/STROKEAHA.116.013837
36. Cho DY, Chen CC, Chang CS, Lee WY, Tso M. Endoscopic surgery for spontaneous basal ganglia hemorrhage: comparing endoscopic surgery, stereotactic aspiration, craniotomy in noncomatose patients. Surg Neurol. (2006) 65:547–55. discussion 555-6. doi: 10.1016/j.surneu.2005.09.032
37. Zhang HZ, Li YP, Yan ZC, Wang XD, She L, Wang XD, et al. Endoscopic evacuation of basal ganglia hemorrhage via keyhole approach using an adjustable cannula in comparison with craniotomy. Biomed Res Int. (2014) 2014:898762. doi: 10.1155/2014/898762
38. Feng Y, He J, Liu B, Yang L, Wang Y. Endoscope-assisted keyhole technique for hypertensive cerebral hemorrhage in elderly patients: a randomized controlled study in 184 patients. Turk Neurosurg. (2016) 26:84–9. doi: 10.5137/1019-5149.JTN.12669-14.0
39. Zhang J, Lu S, Wang S, Zhou N, Li G. Comparison and analysis of the efficacy and safety of minimally invasive surgery and craniotomy in the treatment of hypertensive intracerebral hemorrhage. Pakistan J Medical Sciences. (2018) 34:578–82. doi: 10.12669/pjms.343.14625
40. Cho DY, Chen CC, Lee WY, Lee HC, Ho LH. A new Modified Intracerebral Hemorrhage Score for treatment decisions in basal ganglia hemorrhage-a randomized trial. Crit Care Med. (2008) 36:2151–6. doi: 10.1097/CCM.0b013e318173fc99
41. de Oliveira Manoel AL. Surgery for spontaneous intracerebral hemorrhage. Crit Care. (2020) 24:45. doi: 10.1186/s13054-020-2749-2
42. Xinghua X, Xiaolei C, Fangye L, Xuan Z, Qun W, Guochen S, et al. Effectiveness of endoscopic surgery for supratentorial hypertensive intracerebral hemorrhage: a comparison with craniotomy. J Neurosurg. (2017) 128:553–9. doi: 10.3171/2016.10.JNS161589
43. Lord AS, Langefeld CD, Sekar P, Moomaw CJ, Badjatia N, Vashkevich A, et al. Infection after intracerebral hemorrhage: risk factors and association with outcomes in the ethnic/racial variations of intracerebral hemorrhage study. Stroke. (2014) 45:3535–42. doi: 10.1161/STROKEAHA.114.006435
44. Murthy SB, Moradiya Y, Shah J, Merkler AE, Mangat HS, Iadacola C, et al. Nosocomial Infections and Outcomes after Intracerebral Hemorrhage: A Population-Based Study. Neurocrit Care. (2016) 25:178–84. doi: 10.1007/s12028-016-0282-6
45. Patir R, Mahapatra AK, Banerji AK. Risk factors in postoperative neurosurgical infection. A prospective study. Acta Neurochir. (1992) 119:80–4. doi: 10.1007/BF01541786
46. Kellner CP, Song R, Ali M, Nistal DA, Samarage M, Dangayach NS, et al. Time to evacuation and functional outcome after minimally invasive endoscopic intracerebral hemorrhage evacuation. Stroke. (2021) 52:e536–9. doi: 10.1161/STROKEAHA.121.034392
47. Morgenstern LB, Demchuk AM, Kim DH, Frankowski RF, Grotta JC. Rebleeding leads to poor outcome in ultra-early craniotomy for intracerebral hemorrhage. Neurology. (2001) 56:1294–9. doi: 10.1212/WNL.56.10.1294
48. Ovesen C, Christensen AF, Krieger DW, Rosenbaum S, Havsteen I, Christensen H, et al. Time course of early postadmission hematoma expansion in spontaneous intracerebral hemorrhage. Stroke. (2014) 45:994–9. doi: 10.1161/STROKEAHA.113.003608
49. Wang YF, Wu JS, Mao Y, Chen XC, Zhou LF, Zhang Y. The optimal time-window for surgical treatment of spontaneous intracerebral hemorrhage: result of prospective randomized controlled trial of 500 cases. In: Cerebral Hemorrhage. (2008) p. 141–145. doi: 10.1007/978-3-211-09469-3_29
Keywords: endoscopy, intracerebral haemorrhage, neurosurgery, meta-analysis, outcome
Citation: Hallenberger TJ, Guzman R, Bonati LH, Greuter L and Soleman J (2022) Endoscopic surgery for spontaneous supratentorial intracerebral haemorrhage: A systematic review and meta-analysis. Front. Neurol. 13:1054106. doi: 10.3389/fneur.2022.1054106
Received: 26 September 2022; Accepted: 05 December 2022;
Published: 20 December 2022.
Edited by:
Gabriel Broocks, University of Hamburg, GermanyReviewed by:
Mukesch Johannes Shah, University of Freiburg, GermanyCopyright © 2022 Hallenberger, Guzman, Bonati, Greuter and Soleman. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jehuda Soleman,  SmVodWRhLnNvbGVtYW5AZ21haWwuY29t
SmVodWRhLnNvbGVtYW5AZ21haWwuY29t
†These authors have contributed equally to this work and share last authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.