
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Neurol., 17 November 2022
Sec. Dementia and Neurodegenerative Diseases
Volume 13 - 2022 | https://doi.org/10.3389/fneur.2022.1024004
 Hope Onohuean1,2*
Hope Onohuean1,2* Abraham Olutumininu Akiyode3Oluwole Akiyode2,4
Abraham Olutumininu Akiyode3Oluwole Akiyode2,4 Sharon Iyobor Igbinoba1,2,5Abdullateef Isiaka Alagbonsi6
Sharon Iyobor Igbinoba1,2,5Abdullateef Isiaka Alagbonsi6Introduction: There is a scarcity of epidemiological data on neurodegenerative diseases (NDs) in East Africa. This meta-analysis provides the regional prevalence of NDs, their contributing factors, and evidence of change over time concerning gender per age or year.
Methods: Articles were retrieved from electronic databases following the PRISMA standard.
Results: Forty-two studies were reviewed, and 25 were meta-analyzed with a random-effects model. The pool estimate proportion of 15.27%, 95% CI (0.09–0.23) (I2 = 98.25%), (Q = 1,369.15, p < 0.0001) among a population of 15,813 male/female and 1,257 with NDs. Epidemiological characteristics associated with NDs include Dyskinesias prevalence 55.4%, 95% CI (13.5; 90.9), I2 (96%) and subsistence farming prevalence 11.3%, 95% CI (5.8; 20.9), I2 (99%). Publication bias by Egger test was (z = 4.1913, p < 0.0001), while rank correlation test using Kendall's model was (tau = 0.1237, p = 0.3873). Heterogeneity (R2 design = 5.23%, p design < 0.0001; R2 size = 52.163%, p size < 0.001; and R2 period = 48.13, p period < 0.0001. Covariates (R2 design + size + period = 48.41%, p < 0.001).
Conclusion: There is a high prevalence of NDs in the East African region, which could impact life expectancy, morbidity, and quality of life. Thus, early screening and regular surveillance could assist in management strategies.
The loss of function in the brain's nerve cells and the peripheral nervous system causes neurodegenerative diseases (NDs). Alzheimer's disease (AD), Parkinson's disease (PD), Huntington's disease (HD), and Lou Gehrig or amyotrophic lateral sclerosis (ALS) are the major neurodegenerative disorders, which are of public health concerns (1–4) and characterized by the inevitable degeneration of specific neuronal clusters (5). This group of illness provides a significant clinical challenge due to its progressive nature (6, 7), in which nerve cells in the brain and peripheral nervous system lose their ability to function over time and eventually die and can only be delayed, not completely stopped, once it has started.
In most surveys around the world, annual incidence rates of NDs are estimated to be 10–15 per 100,000, 2% of which are people over the age of 65 years (8). According to a 2019 estimate, ~50 million individuals worldwide suffered from NDs that resulted in dementia, and this number is expected to rise to 152 million by 2060 (9–11).
In the United States (US), the most prevalent and burdensome neurological illnesses are tension-type headache (TTH) [121.6 (95% UI, 110–133) million people], migraine [68.5 (95% UI, 64–73) million people], stroke [7.8 (95% UI, 7.4–8.2) million people], AD and other dementias [2.9 (95% UI, 2.6–3.2) million people], and spinal cord injuries (SCI) [2.2 (95% UI, 2.0–2.3) million people] (12).
In sub-Saharan Africa, population-based prevalence of PD, ALS, and HD range from 10 to 235 per 100,000, 5 to 15 per 100,000, and 3.5 per 100,000, respectively, while their corresponding hospital-based prevalence are 0.41 to 7.2%, 0.2–8.0 per 1,000, and 0.2 to 46.0 per 100,000, respectively (13). Nevertheless, data on the prevalence and epidemiological potentials of neurological illnesses in the communities are sparse in Sub-Saharan Africa, especially those living in hard-to-reach settlements. In most rural areas, residents often suffer the most due to a lack of knowledge about the symptoms and adequate early diagnosis or medical examinations for these neurological diseases and are left out of the epidemiological survey.
East Africa is a region consisting of many low-income communities that have reported several cases of malaria (14, 15), HIV/AIDs (16, 17), and diarrhea (18–21) infections as well as sporadic multi-drug resistance (22, 23). Various forms of NDs have also been reported to be prevalent in the region. In the Mukono district of Uganda, for instance, the frequencies of peripheral neuropathy (46.2%), chronic headaches (26.4%), epilepsy (8.5%), pain syndromes (7.5%), stroke (6.6%), and tremors/Parkinson disease (3.8%) were reported to be high. Moreover, the crude prevalence rates (95% CI) of stroke, epilepsy, and peripheral neuropathy were reported as 14.3% (8.5–24.1), 13.3% (7.7–22.8), and 33.7% (23.9–47.4), respectively (24). In the rural Hai district of Tanzania, the age-adjusted prevalence per 1,000 of the most common neurological disorders was tremor (48.2), headache (41.8), stroke (23.0), peripheral polyneuropathy (18.6), upper limb mononeuropathy (6.5), and parkinsonism (5.9) (25).
Exploring the epidemiology and factors contributing to the prevalence of NDs is critical for identifying patterns of disease predisposition, environmental clustering, and medication responses mostly at regional, communal, and individual levels (23, 26). The knowledge of whether NDs incidence and/or prevalence is changing would have substantial scientific and therapeutic implications, aside from the need of having accurate, up-to-date numbers for developing services to meet the needs of the population suffering from them.
There is scarce information on the prevalence of neurological disorders and epidemiological potentials in populations of other East African regions to identify research opportunities and suggest preventative or mitigation solutions. Again, there is a lack of presentation of published East African epidemiologically relevant studies. Here, we provide the first epidemiological assessment of major neurological illnesses in the East African region, giving information on the prevalence of such disorders. Thus, a decrease would imply that future rates are partially adjustable and effectively addressing the changeable risk factors could delay, if not completely prevent the illness. The specific objective includes (1) providing regional estimates of NDs prevalence and incidence, (2) investigating factors that contribute to estimating heterogeneity (study location {Countries}, NDs types, study design, sample size, study period), and (3) finding evidence of change in NDs prevalence and/or incidence over time concerning gender per age or year. This research study updates and expands the prior findings on the epidemiology of this condition.
The statement (Appendix 1 Table) of the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) (23, 27) was used in this study. The Boolean keywords in the form of title words or medical subject headings were conducted as a literature search using the electronic databases: PubMed, Web of Science (WOS), SCOPUS span 1980 and November 2021. The keywords, neuro disease or neurodegenerative disease, detail search algorithms, or key terms in the additional information (Appendix 2 Text) were used to assess the prevalence, epidemiology, population, and survey data within the East African region. The datasets were combined on RStudio versions 4.0.5 using the bibliometrix R package (28), while the removal of duplicates and normalization of variables were done using ScientoPy and fBasics R-packages (29), followed by a hand check of the reference lists of all retrieved studies to add any relevant articles. Two reviewers (HO and AOA) did the literature search independently.
Studies that matched the following criteria were included, such as (1) data on the population-based prevalence of NDs or epidemiological and observational studies on NDs reported in East Africa, (2) NDs diagnosis made for both males/females across all ages; (3) Prognosis of NDs based on the opinions of a qualified medical practitioner, electrophysiological test, or medical records indicating a diagnosis of NDs according to the International Classification of Diseases and Codes; (4) full-text articles written in English that are available; (5) Diagnostic and Statistical Manual of Mental Disorders (DSM-IV); (6) Identification and Interventions for Dementia in Elderly Africans (IDEA) screen; (7) International HIV Dementia Scale (IHDS); (8) Montreal Cognitive Assessment test (MoCA); (9) Based on the modified McDonald's criteria.
The following studies were excluded: (1) conference abstracts' documents or meeting abstracts, letters, or reviews; full texts without raw data, total population, positive cases, and duplicate publications; (2) NDs were not based on objective examination or medical records and involved self-reported cases; (3) questionnaires or app technology-based studies; (4) Dementia-associated with the treatment of HIV and other terminal diseases; (4) articles published in languages other than English.
Based on these criteria, two reviewers (H. O. and A. O. A.) independently selected the studies for final inclusion while a third author (S. I.) doubled-check, arbitrated, and resolved disagreements between the two reviewers.
Following the inclusion and exclusion criteria, information on the first author names, publication year, the total population, number of positive cases, country of study, study source, study period, and study type were identified and extracted from results, discussions, figures and tables in the qualified articles as the meta-analysis indices by two investigators independently (HO and AOA) and double-checked by a third investigator (S. I). Afterward, documentation of homogeneity or consistency and heterogeneity across studied populations was done and further statistical analysis was based on requirements for the study as conceptualized by the investigators.
The Newcastle–Ottawa Scale (NOS), proposed by the Agency for Healthcare Research and Quality (AHRQ), was used to assess methodological quality found in (http://www.ohri.ca/programs/clinicalepidemiology/oxford.asp). This rating employs a star system to rate the quality of a study in three areas: study group selection, group comparability, and outcome measurement.
The raw proportions were used to compute the regional population-based NDs prevalence from 27 studies, and the Wilson method was employed to calculate 95% confidence intervals (CIs). The study's random-effects meta-analyses weighting was done by estimating the summary effect size (weighted average proportion) to calculate the pooled effect size based on the individual effect sizes and their sampling variances via the argument method = “DL” (using the restricted maximum-likelihood estimator). To improve the statistical properties, the logit transformation was conducted to get the pooled prevalence since we have a mean proportion of 0.03 across the studies (30). The effects of examined homogeneity or consistency and heterogeneity across studied populations were measured using sensitivity and influence meta-regression analysis of sample size and period. A Forest plot for the overall and the mixed effects model for the between-study variation of subgroups analysis (design, East Africa region (location) as well gender per year/per age distribution were generated. The Funnel plots for comparison of publication bias were conducted according to asymmetry Egger's test for this purpose and further examined for the significance of the bias using the rank correlation test and Kendall's model. All analyses were two-tailed with p < 0.05 level of significance and were conducted in the statistical software R 4.0.5. packages (31, 32).
Our search found a total of 147 NDs articles from the three databases reported in the East African region between 1980 and 2021. After removing duplicates and studies that were not relevant, the abstracts of the remaining studies were read, and 42 articles from different countries in the East African region with possibly relevant studies were reviewed, the details of which are in the flowchart (Figure 1). Thirty-one studies were from Tanzania, five were from Uganda, one from Ethiopia, and five were from Kenya, and they can be found in Supplementary Figure 1. The sample sizes of the studies ranged from 21 to 161,000 males and females in the East Africa regional NDs prevalence estimate. The retrieved age ranged from 32 years to 100 years old at the time of diagnosis, and 42 articles (Table 1) were systematically reviewed while 25 published studies were included in the meta-analysis. Based on the systematic review, a total population of 26,762 were tested for the NDs and a prevalence of a total of 1,629 people (6.09%): male 600 (36.83%) and female 995 (61.08%) were observed. While the gender of 34 positive cases was not identified in the included studies.
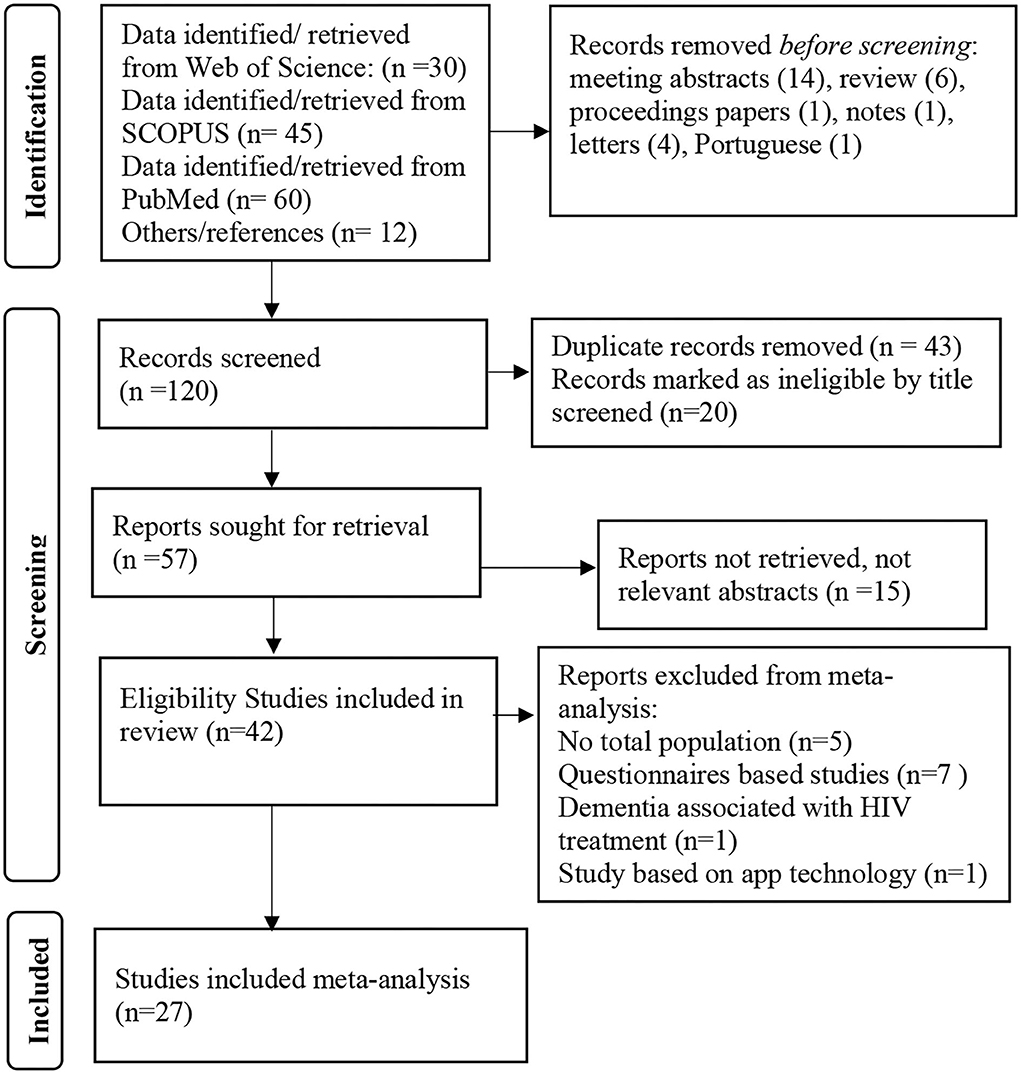
Figure 1. Study selection flowchart.
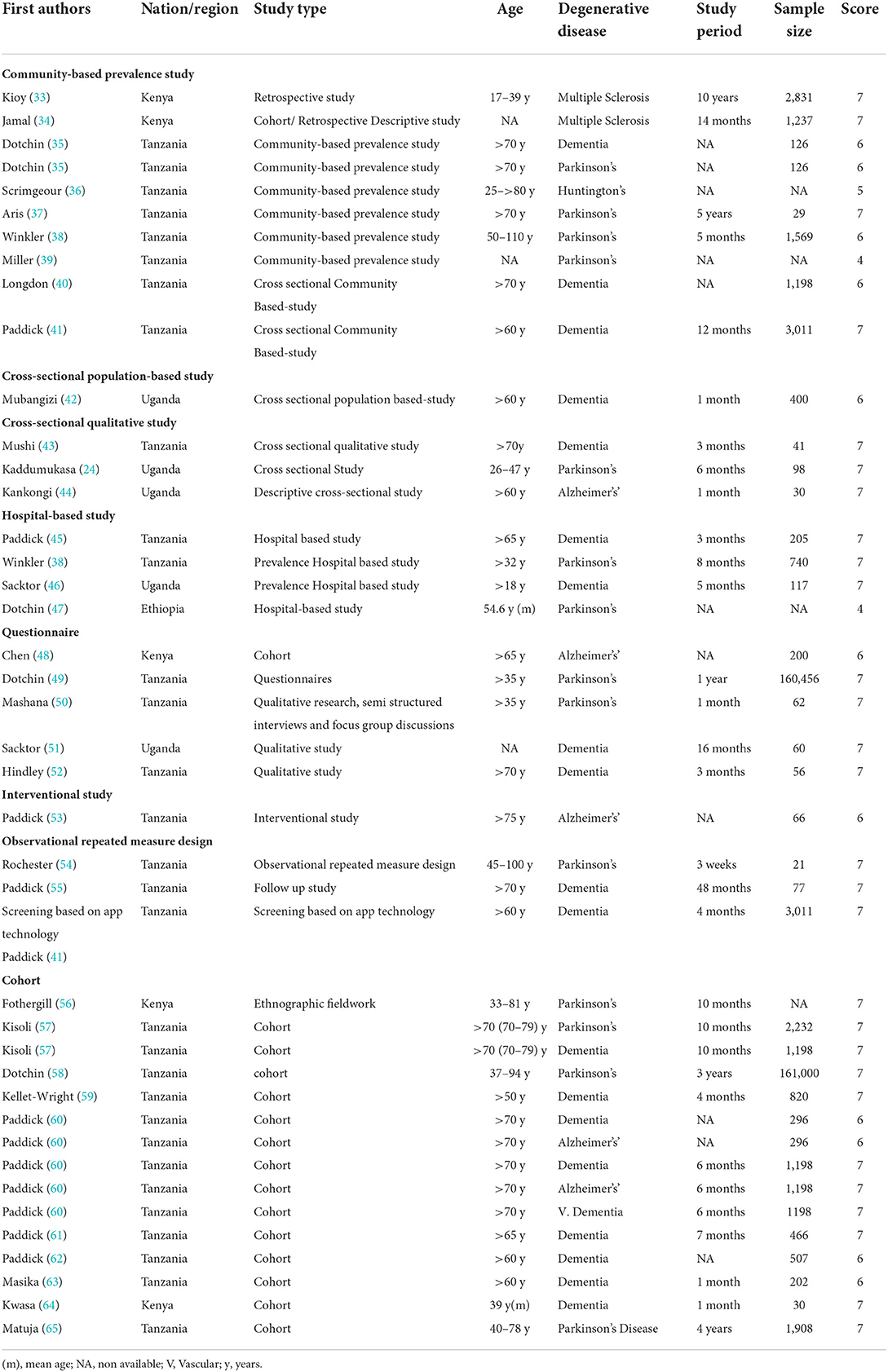
Table 1. Overall characteristics of the included studies.
Supplementary Table 1 show the quality evaluation scores of the included studies, and Table 1 shows the details of the assessment questions in domains for each article. The NOS variables and comparability received no stars to any of the examined studies because comparative studies were not reported in the included publications. For the other studies, quality scores range from 4 to 7. Twenty-eight studies received 7 points, 11 studies received 6 points, a study received 5 points, and 2 studies received 4 points out of the maximum 8 points.
Upon removal of two outer liars in the analysis (35, 61), a total of 15,813 people, both male and female, were included in the 25 studies (33–35, 37, 38, 40–45, 48, 53–55, 57–62, 65, 66), and a prevalence of 7.95% (1,257) was recorded on the regional-based epidemiological potential of NDs. Also, the prevalence of NDs is apparently increasing in females per year and age in this regional meta-analysis, as depicted in Supplementary Figures 1, 2. The design distribution of these studies include cross-sectional study (n = 3), a community-based prevalence study (n = 5), hospital-based study (4), follow up study (1), while regional cohorts (n = 14) included data on the population-based prevalence of NDs in the studied region (Table 1).
The pooled estimate of ND prevalence calculated for the 25 east Africa regional base epidemiological potentials studies is as follows. The pool estimate proportion of 15.27%, 95%CI (0.09–0.23) with an (I2 = 98.25%) by random effect model, implicates a high proportion between studies. A significant Q statistic of (Q = 1369.15, p < 0.0001) was observed, indicating that the included studies do not share a common effect size. Therefore, overall, our NDs prevalence meta-analysis has substantial heterogeneity, as depicted in Figure 2. The evaluation of publication bias by a funnel plot (Supplementary Figure 4) using the Egger test model (P < 0.0001) indicates a significant level of publication bias.
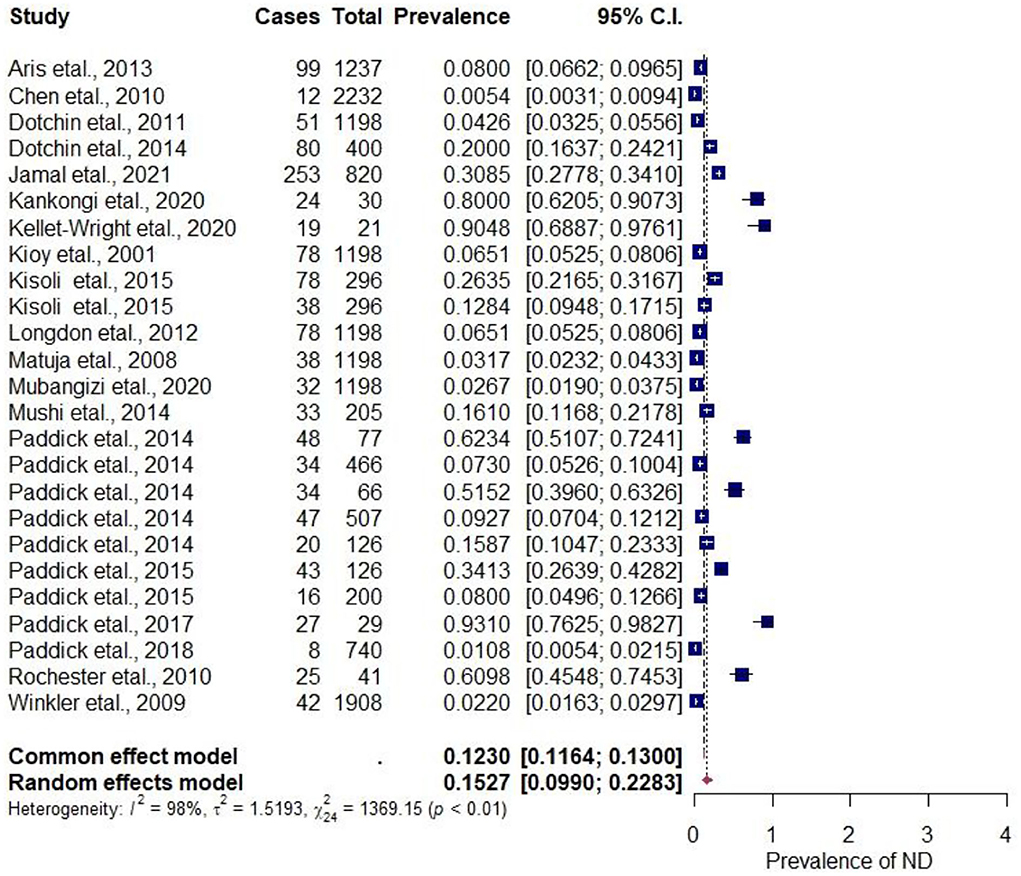
Figure 2. Forest plot for the prevalence of NDs in the regional-based studies.
The Funnel plots were used to determine the publication bias. Each point denotes a separate study on the designated association. The vertical line denotes the mean effect size. However, the points are dispersed asymmetrically, which shows publication bias. While the linear regression test of funnel plot asymmetry using the Egger test signifies a bias (z = 4.1913, p < 0.0001), indicating a significant publication bias (Supplementary Figure 4). On the other hand, the rank correlation test for funnel plot asymmetry using Kendall's model indicates tau = 0.1237 and p = 0.3873.
To examine the probable sources of heterogeneity observed in the visual forest plot and the baseline analysis of the included studies, five definite covariates were investigated. In univariate meta-regression analyses, the countries (Tanzania or Kenya or Uganda) and NDs types (Multiple Sclerosis or Parkinsons or Dementia or Alzheimers) were not significantly associated with the NDz prevalence (p = 0.166; R2 = 0.00%) (p = 0.8464; R2 = 0.00%). However, there was a significant estimate for the covariates analysis of the study design (Cohort or Other), sample size (less or more than 1,000), and study period (months or above 1 year). The R2 (amount of heterogeneity accounted for) and p-values for each covariate estimate are as follows: R2 design = 5.23%, p design < 0.0001; R2 size = 52.163%, p size < 0.001; and R2 period = 48.13, p period < 0.0001, respectively. Additionally, a subsequent multivariate mixed-effects meta-regression model was developed based on the study's (design, size, and period), with each of these variables showing significant associations with the pooled prevalence heterogeneity. These three covariates significantly accounted for 48.41% of the heterogeneity in the ND prevalence estimate (R2 design + size + period = 48.41%, p design + size + period < 0.001).
The potential variations of study design (cohort or others) categorical variables, the others have the highest NDs prevalence estimate 44.94%, CI (0.272–0.640), I2 = 97.21%, to the cohort group 5.60%, CI (0.031–0.099), I2 = 98.49% in Supplementary Figure 3. Subgroup analysis by study size revealed the high NDs prevalence in < 1,000 size 27.97% CI (0.192–0.388), I2 = 96.58% to that of more than 1,000 sample size 3.46%, CI (0.022–0.054) as depicted in Supplementary Figure 4. The study period subgroup analysis reveals the most prevalence in years 22.87% CI (0.105–0.428), I2 = 96.15% to that of study period in months 12.12%, CI (0.069–0.204), I2 = 96.40% as shown in Supplementary Figure 5. For the individual subgroups, variations that were not significantly associated with the NDs prevalence [East Africa region (Kenya or Tanzania or Uganda) in Supplementary Figure 6 and NDs types (Multiple Sclerosis or Parkinsons or Dementia or Alzheimers)] are shown in Figure 3.
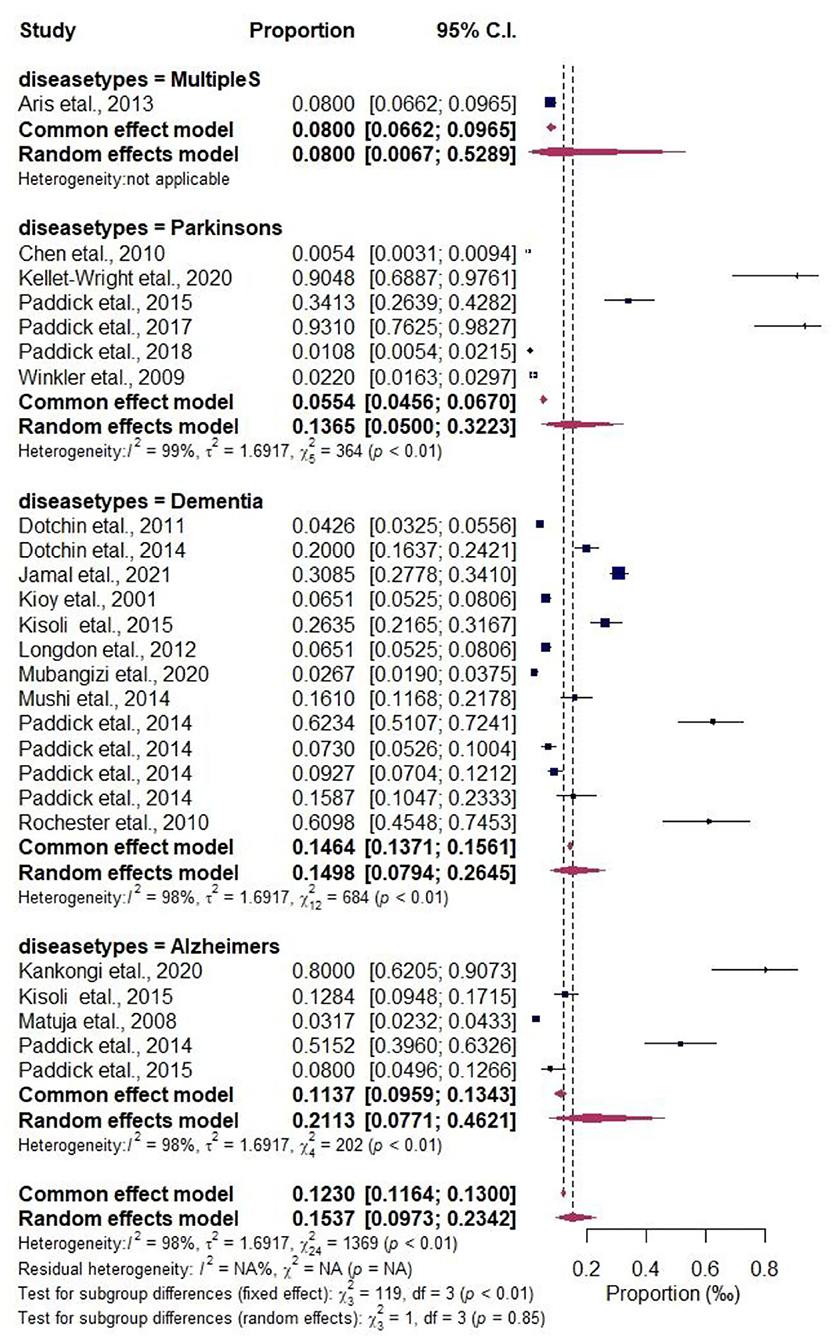
Figure 3. Forest plot of the subgroup analysis by NDs types.
The Forest plots for the subgroup analysis of regional-based NDs prevalence including the subgroup analysis by research period, sample size, and East African countries are shown in Supplementary Figures 5–8. The prevalence of the subcategories according to two epidemiological characteristics including comorbidity and subsistence farming are also shown in Table 2. The comorbidities reported in the included articles by authors categorized as others include (chronic choreoathetosis, progressive dementia) Scrimgeour (36) (abnormalities of sympathetic and parasympathetic functions) Aris et al. (37) (visual disturbances and somatic sensorimotor disturbances) Kioy et al. (33) account for 93.1%, and dyskinesias, spinal cord pathology, HIV, cognitive impairment 55.4, 34.1, 28.2, and 20.1%, respectively. On the other hand, the economic status was categorized into two: subsistence farmers and others such as (workers, retired, student, unemployed, employed, house wife/husband) as reported in the included articles. Subsistence farming accounts for 11.3% prevalence, while others account for 5.7%.
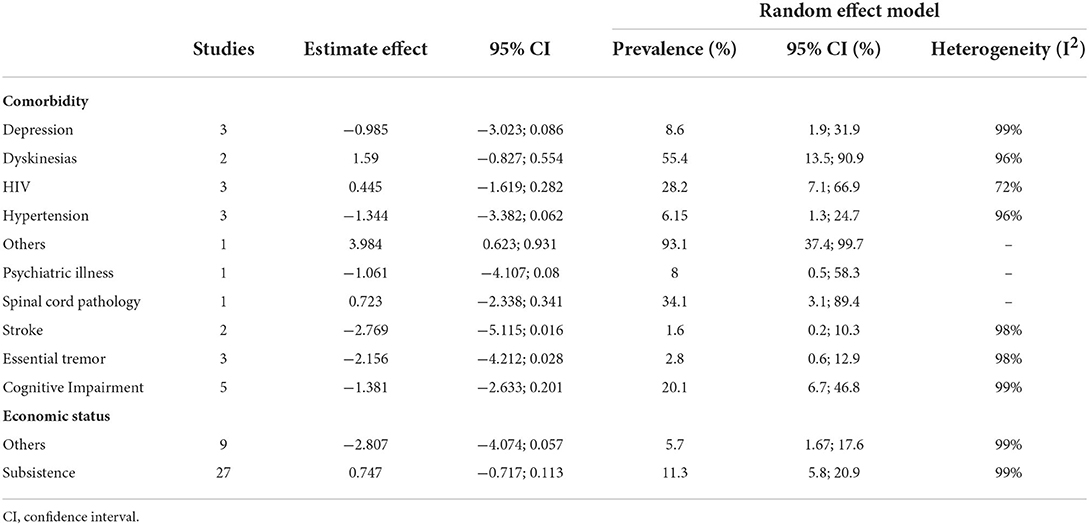
Table 2. Pooled estimates of economic status and comorbidity epidemiological characteristics.
This study aimed to provide scientific evidence on regional estimates of NDs prevalence and incidence; investigate factors that contribute to the estimated heterogeneity (study location {Countries}, ND types, study design, sample size, study period); and find evidence of change in NDs prevalence and/or incidence over time concerning gender per age or year. Overall, our findings indicate a higher regional prevalence of NDs with substantial heterogeneity among the included studies. The covariates analysis of study design, size, and period variables significantly account for the pooled prevalence heterogeneity. Also, there is an increasing occurrence of NDs in females per year and age within the region. These findings are consistent with studies elsewhere (67–72). These systematic review and meta-analysis are the first approach to compile epidemiological data on NDs in the East African region. However, accurately quantifying and comparing the burden of NDs across countries could be challenging due to broad, multicultural, and multiethnic regions. Nevertheless, our findings are informative and describe the prevalent cases or occurrences based on retrospective data from studies that have primarily covered regional populations.
Numerous research work on the geographical distribution of NDs have been conducted around the world with little focus on resources and limited regional-based evaluation. Our study gives thorough, current estimates of the prevalence and important epidemiological aspects of NDs in the East African region. The systematic review revealed 42 studies on epidemiology and its prevalence; Tanzania researchers have shown excellent interest in NDs with 31 (73.8%) of the studies, one (2.4%) from Ethiopia, five (11.9%) from Uganda and five (11.9%) from Kenya, while 25 (59.5%) of the studies was meta-analyzed using a random-effect model.
Our analysis reveals a prevalence of 6.09%, of which females were reported to have the highest proportion (61.08%), while the overall random model pool estimates a prevalence of 7.95%, indicating that NDs are becoming a common disease in the region. The prevalence of NDs in the region designates a public health burden, mounting beyond rare diseases based on WHO (73) and European (74) standards. Rare diseases have a substantially lower population incidence than common disorders resulting in higher demands for disease documentation and more extensive reliance on reliable and thorough epidemiological data (75). This may be due to a lack of public awareness and integrated health systems; the few large-scale epidemiological studies that have been conducted to focus on restricted locations, limited populations, and partial epidemiological variables, resulting in inadequate evidence synthesis and outcomes.
An observable upsurge was seen in the yearly status of the disease in 2020, with the female having the highest, confirming the projection report before 2050 (9–11). Also, studies have implicated age (those above the age of 60), gender (female), family, educational level, and rural living as substantial risk factors for developing NDs (8, 76–78). Moreover, evidence (79) predicts that population aging or growth is a driving factor for individuals affected by dementia worldwide. We are not surprised to see females having the highest gender per year/age distribution, as it is consistent with previous reports that suggest sex differences are a potential biological pathway underlying Alzheimer's disease (79–81). Interestingly, our result shows a growing prevalence from age 45, unlike the well-reported cases of NDs burden from age 65 years. It implies that NDs in the region have undergone a shift that may potentially affect life expectancy. NDs could be cellular or molecular and could be caused by a metabolic deficiency or hereditary/genetic or medical issues such as (alcoholism, tumor, stroke), or toxins, chemicals, and viruses which are more common as people get older (5, 82–85). At the same time, many people living in hard-to-reach limited resources settings do not seek medical help early enough. The absence of diagnostic facilities has aggravated the prevalence of NDs-related illnesses, and many cases remain undiagnosed and unmanaged, putting the population at risk of developing into mortality.
Our study reveals NDs prevalence order of (Dementia 52% > Parkinson's 24% > Alzheimer's 16% > Multiple sclerosis 8%), indicating dementia has been the most reported and widespread NDs in the region. This study is in agreement with the report of Lekoubou et al. (13), where dementia was the most common neurological disorder, and Alzheimer's disease accounted for the majority of cases. Also, the incidence of dementia is increasing in middle and north Africa (86). Investigation implicates dementia to have a lifelong course, with risk aggregating around specific periods and frequently accumulation, sometimes decades before clinical symptoms (87). Some risk factors impact early in life, while others occur later due to environmental interaction (42, 88, 89). Again Ethnic differences associated with biological peril factors, including cerebrovascular disease and cognitive impairment, also contribute to dementia and Alzheimer's disease prevalence in the region (8, 77).
Our sensitivity analysis showed substantial heterogeneity among the studies; however, each country and disease type have no significant contribution to the heterogeneity. Furthermore, study design, sample size, and study period accounted for the significant differences. These could explain the broad prevalence range observed in both population and hospital-based research work for NDs, and the heterogeneity could potentially be due to methodology differences. These disparities in NDs frequency are not limited to East Africa, and the same has also been reported in Europe (90). Because most of the studies were community-based prevalence studies and retrospective descriptive studies where the final diagnosis was not based on pathogenesis and variation in the sample size, we have less clarity in the case of Multiple Sclerosis and Huntington's disease, making comparisons and inferences inaccurate.
Due to the enormous socioeconomic expenses that could amplify the increase of NDs and the disease's complexity in the region, it's critical to identify the risk factors that contribute to the related illness development to establish an effective management approach. In several parts of the world, including East Africa, NDs have shown a quick change that could affect life expectancy.
Epidemiological characteristics, comorbidity, and economic status are also linked to the upsurge of NDs in the East African region. Mainly, dyskinesias, HIV, spinal cord pathology, cognitive impairment, chronic choreoathetosis, and abnormalities of sympathetic and parasympathetic functions are the comorbidities linked to NDs in our findings (33, 34, 37, 43, 46, 48, 51, 91). While the majority of the population's livelihood is subsistence farming, which is implicated in the disease progression (25, 38, 45, 49, 55, 60, 66), the increase in NDs prevalence in East Africa could be attributed to the region's changing lifestyles and social factors, including smoking, drinking, pre-existing medical disorders, or environmental factors like air pollution (92–96).
Epidemiological surveys are critical for developing preventative and management strategies for the region's potential epidemic ill health. Due to the current lack of availability of effective NDs-modifying medications, immediate attempts to limit the disease-increasing projection could focus on disease prevention via interventions to regulate risk factors (97, 98).
Our study is the first of its type in East Africa on neurodegenerative diseases. We are confident it will draw the attention of policymakers to intervention strategies in the region. The epidemiological survey emphasizes the region's circumstances and highlights research priorities. Conversely, we examined a regionally-based population study by including community diverse data sources to suggest clear information about the present burden and risk factors to stakeholders for future preparedness.
The Egger test signifies a publication bias for the occurrence proportion and period prevalence, and publication bias implies possible unpublished research with different findings. Again, combining research from different countries and assessing changes over time is also tricky because of the lack of uniform or specific information. Here, some studies did not provide the total population or cases, specific age and sex, and studies period, and were excluded from the prevalence estimates. Also, our analysis covered only studies published in English. However, two reviewers' thorough assessment of the study's quality and independent data extraction were among the study's strengths.
The findings reveal a possible regional increase in NDs as an implication of common disorders in the region, with significant gaps in the epidemiological drivers. Particularly the occurrence of NDs in low-income sittings requires advances in screening tools and public health efforts in intervention strategies. We recommend to policymakers make provisions for quality healthcare in rural settings to improve early diagnosis and care for the affected individuals.
The original contributions presented in the study are included in the article/Supplementary files, further inquiries can be directed to the corresponding author/s.
HO conceived, designed the study, and drafted the manuscript. HO, AA, and SI conducted the dataset searches. HO and AA extracted and conducted data analysis. All authors read, revised, and approved the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2022.1024004/full#supplementary-material
ND, Neurodegenerative Disease; AD, Alzheimer's disease; PD, Parkinson's disease; HD, Huntington's disease; ALS, Amyotrophic Lateral Sclerosis; US, United States; TTH, Tension-Type Headache; SCI, spinal cord injuries; US, United States; WOS, Web of Science; WHO, World Health Organization.
1. Dugger BN, Dickson DW. Pathology of neurodegenerative diseases. Cold Spring Harbor Perspect Biol. (2017) 9:a028035. doi: 10.1101/cshperspect.a028035
2. Walker L, Stefanis L, Attems J. Clinical and neuropathological differences between Parkinson's disease, Parkinson's disease dementia and dementia with Lewy bodies – current issues and future directions. J Neurochem. (2019) 150:467–74. doi: 10.1111/jnc.14698
3. Jagaraj CJ, Parakh S, Atkin JD. Emerging evidence highlighting the importance of redox dysregulation in the pathogenesis of amyotrophic lateral sclerosis (ALS). Front Cell Neurosci. (2021) 14:581950. doi: 10.3389/fncel.2020.581950
4. Lamptey RNL, Chaulagain B, Trivedi R, Gothwal A, Layek B, Singh J. A review of the common neurodegenerative disorders: current therapeutic approaches and the potential role of nanotherapeutics. Int J Mol Sci. (2022) 23:1851. doi: 10.3390/ijms23031851
5. Muddapu VR, Dharshini SAP, Chakravarthy VS, Gromiha MM. Neurodegenerative diseases – is metabolic deficiency the root cause? Front Neurosci. (2020) 14:213. doi: 10.3389/fnins.2020.00213
6. Gao HM, Hong JS. Why neurodegenerative diseases are progressive: uncontrolled inflammation drives disease progression. Trends Immunol. (2008) 8:472–9. doi: 10.1016/j.it.2008.05.002
7. Hong J-S. O.107 Why neurodegenerative diseases are progressive: uncontrolled inflammation drives disease progression. Parkinsonism Relat Disord. (2009) 15(Suppl. 4):S28–32. doi: 10.1016/S1353-8020(09)70122-1
8. Alzheimer's disease facts and figures. Alzheimer's Dement. (2021) 17:327–406. doi: 10.1002/alz.12328
10. Armstrong R. What causes neurodegenerative disease? Folia Neuropathol. (2020) 58:93–112. doi: 10.5114/fn.2020.96707
11. Chen D, Zhang T, Lee TH. Cellular mechanisms of melatonin: insight from neurodegenerative diseases. Biomolecules. (2020) 10:1158. doi: 10.3390/biom10081158
12. Feigin VL, Vos T, Alahdab F, Amit AML, Bärnighausen TW, Beghi E, et al. Burden of neurological disorders across the US from 1990-2017: a global burden of disease study. JAMA Neurol. (2021) 78:165–76. doi: 10.1001/jamaneurol.2020.4152
13. Lekoubou A, Echouffo-Tcheugui JB, Kengne AP. Epidemiology of neurodegenerative diseases in sub-Saharan Africa: a systematic review. BMC Public Health. (2014) 14:653. doi: 10.1186/1471-2458-14-653
14. Alegana VA, Macharia PM, Muchiri S, Mumo E, Oyugi E, Kamau A, et al. Plasmodium falciparum parasite prevalence in East Africa: updating data for malaria stratification. PLoS Glob Public Health. (2021) 1:e0000014. doi: 10.1371/journal.pgph.0000014
15. Onohuean H, Alagbonsi AI, Usman IM, Iceland Kasozi K, Alexiou A, Badr RH, et al. Annona muricata Linn and Khaya grandifoliola C.DC. Reduce oxidative stress in vitro and ameliorate Plasmodium berghei-induced parasitemia and cytokines in BALB/c mice. J Evidence-Based Integr Med. (2021) 26:2515690X211036669. doi: 10.1177/2515690X211036669
16. WHO. HIV/AIDS. In: WHO: HIV/AIDS (2021). Available online at: https://www.who.int/news-room/fact-sheets/detail/hiv-aids (accessed August 02, 2020).
17. Onohuean H, Aigbogun EO Jr, Igere BE. Meta-synthesis and science mapping analysis of HIV / HPV co-infection : a global perspective with emphasis on Africa. Global Health. (2022) 18:36. doi: 10.1186/s12992-022-00812-w
18. Omona S, Malinga GM, Opoke R, Openy G, Opiro R. Prevalence of diarrhoea and associated risk factors among children under five years old in Pader District, northern Uganda. BMC Infect Dis. (2020) 20:37. doi: 10.21203/rs.2.15318/v2
19. Onohuean H, Okoh AI, Nwodo UU. Epidemiologic potentials and correlational analysis of Vibrio species and virulence toxins from water sources in greater Bushenyi districts, Uganda. Sci Rep. (2021) 11:2242. doi: 10.1038/s41598-021-01375-3
20. Onohuean H. Occurrence, antibiotic susceptibility and genes encoding antibacterial resistance of Salmonella spp. and Escherichia coli from milk and meat sold in markets of Bushenyi District, Uganda. Microbiol Insights. (2022) 15:11786361221088992. doi: 10.1177/11786361221088992
21. Kotloff KL, Nataro JP, Blackwelder WC, Nasrin D, Farag TH, Panchalingam S, et al. Burden and aetiology of diarrhoeal disease in infants and young children in developing countries (the Global Enteric Multicenter Study, GEMS): a prospective, case-control study. Lancet. (2013) 382:209–22. doi: 10.1016/S0140-6736(13)60844-2
22. Ampaire L, Muhindo A, Orikiriza P, Mwanga-Amumpaire J, Bebell L, Boum Y. A review of antimicrobial resistance in East Africa. Afr J Lab Med. (2016) 5:a432. doi: 10.4102/ajlm.v5i1.432
23. Onohuean H, Agwu E, Nwodo UU. Systematic review and meta-analysis of environmental Vibrio species – antibiotic resistance. Heliyon. (2022) 8:e08845. doi: 10.1016/j.heliyon.2022.e08845
24. Kaddumukasa M, Mugenyi L, Kaddumukasa MN, Ddumba E, Devereaux M, Furlan A, et al. prevalence and incidence of neurological disorders among adult Ugandans in rural and urban Mukono district; a cross-sectional study. BMC Neurol. (2016) 16:227. doi: 10.1186/s12883-016-0732-y
25. Dewhurst F, Dewhurst MJ, Gray WK, Aris E, Orega G, Howlett W, et al. The prevalence of neurological disorders in older people in Tanzania. Acta Neurol Scand. (2013) 27:198–207. doi: 10.1111/j.1600-0404.2012.01709.x
26. Fu H, Hardy J, Duff KE. Selective vulnerability in neurodegenerative diseases. Nat Neurosci. (2018) 21:1350–8. doi: 10.1038/s41593-018-0221-2
27. Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Rev Esp Nutr Humana Diet. (2016) 20:148–60. doi: 10.1186/2046-4053-4-1
28. Aria M, Cuccurullo C. bibliometrix : an R-tool for comprehensive science mapping analysis. J Informetr. (2017) 11:959–75. doi: 10.1016/j.joi.2017.08.007
29. Ruiz-Rosero J, Ramirez-Gonzalez G, Viveros-Delgado J. Software survey: ScientoPy, a scientometric tool for topics trend analysis in scientific publications. Scientometrics. (2019) 121: 1165–88. doi: 10.1007/s11192-019-03213-w
30. Lipsey MW, Wilson DB, Lipsey. Practical meta-analysis. Appl Soc Res Methods Series. (2001) 49:1–264. Available online at: https://us.sagepub.com/en-us/nam/practical-meta-analysis/book11092 (accessed May 04, 2022).
32. Balduzzi S, Rücker G, Schwarzer G. How to perform a meta-analysis with R: a practical tutorial. Evid Based Ment Health. (2019) 22:153–60. doi: 10.1136/ebmental-2019-300117
33. Kioy PG. Emerging picture of multiple sclerosis in Kenya. East Afr Med J. (2001) 78:93–6. doi: 10.4314/eamj.v78i2.9096
34. Jamal I, Shah J, Mativo P, Hooker J, Wallin M, Sokhi DS. Multiple sclerosis in Kenya: demographic and clinical characteristics of a registry cohort. Mult Scler J Exp Transl Clin. (2021) 7:205521732110227. doi: 10.1177/20552173211022782
35. Dotchin CL, Paddick SM, Longdon AR, Kisoli A, Gray WK, Dewhurst F, et al. A comparison of caregiver burden in older persons and persons with Parkinson's disease or dementia in sub-Saharan Africa. Int Psychogeriatr. (2014) 26:687–92. doi: 10.1017/S104161021300255X
36. Scrimgeour EM. Huntington's disease in Tanzania. J Med Genet. (1981) 18:200–3. doi: 10.1136/jmg.18.3.200
37. Aris E, Dotchin CL, Gray WK, Walker RW. Autonomic function in a prevalent Tanzanian population with Parkinson's disease and its relationship to disease duration and 5-year mortality. BMC Res Notes. (2013) 6:535. doi: 10.1186/1756-0500-6-535
38. Winkler AS, Tütüncü E, Trendafilova A, Meindl M, Kaaya J, Schmutzhard E, et al. Parkinsonism in a population of northern Tanzania: a community-based door-to-door study in combination with a prospective hospital-based evaluation. J Neurol. (2010) 257:799–805. doi: 10.1007/s00415-009-5420-z
39. Miller N, Mshana G, Msuya O, Dotchin C, Walker R, Aris E. Assessment of speech in neurological disorders: development of a Swahili screening test. S. Afr. J Commun Disord. (2012) 59:27–33. doi: 10.4102/sajcd.v59i1.19
40. Longdon AR, Paddick SM, Kisoli A, Dotchin C, Gray WK, Dewhurst F, et al. The prevalence of dementia in rural Tanzania: a cross-sectional community-based study. Int J Geriatr Psychiatry. (2013) 28:728–37. doi: 10.1002/gps.3880
41. Paddick SM, Yoseph M, Gray WK, Andrea D, Barber R, Colgan A, et al. Effectiveness of app-based cognitive screening for dementia by lay health workers in low resource settings. A validation and feasibility study in Rural Tanzania. J Geriatr Psychiatry Neurol. (2021). 34:613–21. doi: 10.1177/0891988720957105
42. Mubangizi V, Maling S, Obua C, Tsai AC. Prevalence and correlates of Alzheimer ' s disease and related dementias in rural study. BMC Geriatr. (2020) 20:48. doi: 10.1186/s12877-020-1461-z
43. Mushi D, Rongai A, Paddick SM, Dotchin C, Mtuya C, Walker R. Social representation and practices related to dementia in Hai District of Tanzania. BMC Public Health. (2014) 14:260. doi: 10.1186/1471-2458-14-260
44. Kakongi N, Rukundo GZ, Gelaye B, Wakida EK, Obua C, Okello ES. Exploring pathways to Hospital Care for Patients with Alzheimer's disease and related dementias in rural South Western Uganda. BMC Health Serv Res. (2020) 20:1–12. doi: 10.1186/s12913-020-05365-5
45. Paddick SM, Gray WK, Ogunjimi L, Lwezuala B, Olakehinde O, Kisoli A, et al. Validation of the Identification and Intervention for Dementia in Elderly Africans (IDEA) cognitive screen in Nigeria and Tanzania. BMC Geriatr. (2015) 15:53. doi: 10.1186/s12877-015-0040-1
46. Sacktor N, Nakasujja N, Redd AD, Manucci J, Laeyendecker O, Wendel SK, et al. HIV subtype is not associated with dementia among individuals with moderate and advanced immunosuppression in Kampala, Uganda. Metab Brain Dis. (2014) 29:261–8. doi: 10.1007/s11011-014-9498-3
47. Dotchin CL, Msuya O, Walker RW. The challenge of Parkinson's disease management in Africa. Age Ageing. (2007) 36:122–7. doi: 10.1093/ageing/afl172
48. Chen CH, Mizuno T, Elston R, Kariuki MM, Hall K, Unverzagt F, et al. A comparative study to screen dementia and APOE genotypes in an ageing East African population. Neurobiol Aging. (2010) 31:732–40. doi: 10.1016/j.neurobiolaging.2008.06.014
49. Dotchin C, Msuya O, Kissima J, Massawe J, Mhina A, Moshy A, et al. The prevalence of Parkinson's disease in rural Tanzania. Mov Disord. (2008) 23:1567–672. doi: 10.1002/mds.21898
50. Mshana G, Dotchin CL, Walker RW. “We call it the shaking illness”: Perceptions and experiences of Parkinson's disease in rural northern Tanzania. BMC Public Health. (2011) 11:219. doi: 10.1186/1471-2458-11-219
51. Sacktor N, Nakasujja N, Skolasky RL, Rezapour M, Robertson K, Musisi S, et al. HIV subtype D is associated with dementia, compared with subtype A, in immunosuppressed individuals at risk of cognitive impairment in Kampala, Uganda. Clin Infect Dis. (2009) 49:780–6. doi: 10.1086/605284
52. Hindley G, Kissima J, Oates LL, Paddick SM, Kisoli A, Brandsma C, et al. The role of traditional and faith healers in the treatment of dementia in Tanzania and the potential for collaboration with allopathic healthcare services. Age Ageing. (2017) 46:130–7. doi: 10.1093/ageing/afw167
53. Paddick SM, Kisoli A, Mkenda S, Mbowe G, Gray WK, Dotchin C, et al. Adaptation and validation of the Alzheimer's disease assessment scale - cognitive (ADAS-Cog) in a low-literacy setting in sub-Saharan Africa. Acta Neuropsychiatr. (2017) 29:244–51. doi: 10.1017/neu.2016.65
54. Rochester L, Rafferty D, Dotchin C, Msuya O, Minde V, Walker RW. The effect of cueing therapy on single and dual-task gait in a drug naïve population of people with parkinson's disease in Northern Tanzania. Mov Disord. (2010) 25:906–11. doi: 10.1002/mds.22978
55. Paddick SM, Kisoli A, Dotchin CL, Gray WK, Chaote P, Longdon A, et al. Mortality rates in community-dwelling Tanzanians with dementia and mild cognitive impairment: a 4-year follow-up study. Age Ageing. (2015) 44:636–41. doi: 10.1093/ageing/afv048
56. Fothergill-Misbah N, Walker R, Kwasa J, Hooker J, Hampshire K. “Old people problems”, uncertainty and legitimacy: Challenges with diagnosing Parkinson's disease in Kenya. Soc Sci Med. (2021) 282:114148. doi: 10.1016/j.socscimed.2021.114148
57. Kisoli A, Gray WK, Dotchin CL, Orega G, Dewhurst F, Paddick SM, et al. Levels of functional disability in elderly people in Tanzania with dementia, stroke and Parkinson's disease. Acta Neuropsychiatr. (2015) 27:206–12. doi: 10.1017/neu.2015.9
58. Dotchin C, Jusabani A, Walker R. Three year follow up of levodopa plus carbidopa treatment in a prevalent cohort of patients with Parkinson's disease in Hai, Tanzania. J Neurol. (2011) 258:1649–56. doi: 10.1007/s00415-011-5988-y
59. Kellett-Wright J, Flatt A, Eaton P, Urasa S, Howlett W, Dekker M, et al. Screening for HIV-Associated Neurocognitive Disorder (HAND) in adults aged 50 and over attending a government HIV clinic in Kilimanjaro, Tanzania. Comparison of the International HIV Dementia Scale (IHDS) and IDEA Six Item Dementia Screen. AIDS Behav. (2021) 25:542–53. doi: 10.1007/s10461-020-02998-9
60. Paddick SM, Longdon A, Kisoli A, Gray WK, Dotchin CL, Jusabani A, et al. The prevalence of dementia subtypes in rural Tanzania. Am J Geriatr Psychiatry. (2014) 22:1613–22. doi: 10.1016/j.jagp.2014.02.004
61. Paddick SM, Mkenda S, Mbowe G, Kisoli A, Gray WK, Dotchin CL, et al. Cognitive stimulation therapy as a sustainable intervention for dementia in sub-Saharan Africa: feasibility and clinical efficacy using a stepped-wedge design. Int Psychogeriatr. (2017) 29:979–89. doi: 10.1017/S1041610217000163
62. Paddick SM, Lewis EG, Duinmaijer A, Banks J, Urasa S, Tucker L, et al. Identification of delirium and dementia in older medical inpatients in Tanzania: a comparison of screening and diagnostic methods. J Neurol Sci. (2018) 385:156–63. doi: 10.1016/j.jns.2017.12.006
63. Masika GM, Yu DSF, Li PWC, Wong A, Lin, RSY. Psychometrics and diagnostic properties of the Montreal Cognitive Assessment 5-min protocol in screening for Mild Cognitive Impairment and dementia among older adults in Tanzania: A validation study. Int J Older People Nurs. (2021) 16:1–11. doi: 10.1111/opn.12348
64. Kwasa J, Cettomai D, Lwanya E, Osiemo D, Oyaro P, Birbeck GL, et al. Lessons learned developing a diagnostic tool for HIV-associated dementia feasible to implement in resource-limited settings: Pilot testing in Kenya. PLoS ONE. (2012) 7:e32898. doi: 10.1371/journal.pone.0032898
65. Matuja WBP, Aris EA. Motor and non-motor features of Parkinson's disease. East Afr Med J. (2008) 85:3–9. doi: 10.4314/eamj.v85i1.9599
66. Paddick SM, Kisoli A, Longdon A, Dotchin C, Gray WK, Chaote P, et al. The prevalence and burden of behavioural and psychological symptoms of dementia in rural Tanzania. Int J Geriatr Psychiatry. (2015) 30:815–23. doi: 10.1002/gps.4218
67. Doyle P, Brown A, Beral V, Reeves G, Green J. Incidence of and risk factors for motor neurone disease in UK women: a prospective study. BMC Neurol. (2012) 12:25. doi: 10.1186/1471-2377-12-25
68. Fereshtehnejad SM, Vosoughi K, Heydarpour P, Sepanlou SG, Farzadfar F, Tehrani-Banihashemi A, et al. Burden of neurodegenerative diseases in the Eastern Mediterranean Region, 1990–2016: findings from the Global Burden of Disease Study 2016. Eur J Neurol. (2019) 52:70–81. doi: 10.1111/ene.13972
69. Pérez-Carmona N, Fernández-Jover E, Sempere ÁP. Epidemiology of multiple sclerosis in Spain. Rev Neurol. (2019) 69:32–8. doi: 10.33588/rn.6901.2018477
70. Ray Dorsey E, Elbaz A, Nichols E, Abd-Allah F, Abdelalim A, Adsuar JC, et al. Global, regional, and national burden of Parkinson's disease, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. (2018) 17:939–53. doi: 10.1016/S1474-4422(18)30295-3
71. Mao YM, Wang P, Wang XY, Ye DQ. Global public interest and seasonal variations in Alzheimer's disease: evidence from google trends. Front Med. (2021) 8:778930. doi: 10.3389/fmed.2021.778930
72. Piña-Aguilar RE, Simpson SA, Alshatti A, Clarke A, Craufurd D, Dorkins H, et al. 27 years of prenatal diagnosis for Huntington disease in the United Kingdom. Genet Med. (2019) 21:1639–43. doi: 10.1038/s41436-018-0367-z
73. Widdus R. Public-private partnerships for health: their main targets, their diversity, and their future directions. Bull World Health Organiz. (2001) 79:713–20. doi: 10.4324/9781315254227-32
74. Taruscio D, Capozzoli F, Frank C. Rare diseases and orphan drugs. Ann Ist Super Sanita. (2011) 47:83–93. doi: 10.4415/ANN-11-01-17
75. Lin H, Long E, Chen W, Liu Y. Documenting rare disease data in China. Science. (2015) 349:1064. doi: 10.1126/science.349.6252.1064-b
76. Lim U, Wang S, Park SY, Bogumil D, Wu AH, Cheng I, et al. Risk of Alzheimer's disease and related dementia by sex and race/ethnicity: the Multiethnic Cohort Study. Alzheimers Dement. (2021) 18:700–89. doi: 10.1002/alz.12528
77. Manly JJ, Mayeux R. Ethnic differences in Dementia and Alzheimer's disease. In: Critical Perspectives on Racial and Ethnic Differences in Health in Late Life. Washington, DC: National Academies Press (US) (2004). doi: 10.17226/11086
78. Brewster P, Barnes L, Haan M, Johnson JK, Manly JJ, Nápoles AM, et al. Progress and future challenges in aging and diversity research in the United States. Alzheimers Dementia. (2019) 15:995–1003. doi: 10.1016/j.jalz.2018.07.221
79. Nichols E, Steinmetz JD, Vollset SE, Fukutaki K, Chalek J, Abd-Allah F, et al. Estimation of the global prevalence of dementia in 2019 and forecasted prevalence in 2050: an analysis for the Global Burden of Disease Study 2019. Lancet Public Health. (2022) 17:e051496. doi: 10.1002/alz.051496
80. Hohman TJ, Dumitrescu L, Barnes LL, Thambisetty M, Beecham G, Kunkle B, et al. Sex-specific association of apolipoprotein e with cerebrospinal fluid levels of tau. JAMA Neurol. (2018) 78:937–47. doi: 10.1001/jamaneurol.2018.0821
81. Koran MEI, Wagener M, Hohman TJ. Sex differences in the association between AD biomarkers and cognitive decline. Brain Imaging Behav. (2017) 11:205–13. doi: 10.1007/s11682-016-9523-8
82. Anisa, Thahir R, Magfirah N, Baharullah, Ernawati. Counseling and health checks as an effort to prevent degenerative diseases. JCES. (2021) 4:221–8. doi: 10.31764/jces.v4i1.3604
83. Di Renzo L, Gualtieri P, Romano L, Marrone G, Noce A, Pujia A, et al. Role of personalized nutrition in chronic-degenerative diseases. Nutrients. (2019) 11:1707. doi: 10.3390/nu11081707
84. Ames BN, Shigenaga MK, Hagen TM. Oxidants, antioxidants, and the degenerative diseases of aging. Proc Natl Acad Sci USA. (1993) 90:7915–22. doi: 10.1073/pnas.90.17.7915
85. Kaur G, Singh NK. The role of inflammation in retinal neurodegeneration and degenerative diseases. Int J Mol Sci. (2022) 23:386. doi: 10.3390/ijms23010386
86. Bhalla D, Lotfalinezhad E, Amini F, Salmannejad M, Reza Borhani Nezhad V, Rezai Kooshalshah SF, et al. Incidence and Risk profile of dementia in the regions of middle East and North Africa. Neuroepidemiology. (2018) 50:144–52. doi: 10.1159/000487761
87. Whalley LJ, Dick FD, McNeill G. A life-course approach to the aetiology of late-onset dementias. Lancet Neurol. (2006) 5:87–96. doi: 10.1016/S1474-4422(05)70286-6
88. NIH Fogarty International Center. As dementia rises in Africa, urgent need for research - Fogarty International Center @ NIH. Glob Heal Matters Newsl. (2018) 17:8–9. Available online at: https://www.fic.nih.gov/News/GlobalHealthMatters/september-october-2018/Pages/dementia-research-africa.aspx (accessed May 04, 2022).
89. Guerchet M, Mayston R, Lloyd-Sherlock P, Prince M, Aboderin I, Akinyemi R, et al. Dementia in sub-Saharan Africa: challenges and opportunities; Dementia in sub-Saharan Africa: challenges and opportunities. Available online at: www.leahbeach.com (accessed May 04, 2022).
90. Okubadejo NU, Bower JH, Rocca WA, Maraganore DM. Parkinson's disease in Africa: a systematic review of epidemiologic and genetic studies. Mov Disord. (2006) 21:2150–6. doi: 10.1002/mds.21153
91. Dotchin CL, Jusabani A, Walker RW. Non-motor symptoms in a prevalent population with Parkinson's disease in Tanzania. Park Relat Disord. (2009) 15:457–60. doi: 10.1016/j.parkreldis.2008.11.013
92. Erro R, Brigo F, Tamburin S, Zamboni M, Antonini A, Tinazzi M. Nutritional habits, risk, and progression of Parkinson disease. J Neurol. (2018) 265:12–23. doi: 10.1007/s00415-017-8639-0
93. Palacios N. Air pollution and Parkinson's disease - evidence and future directions. Rev Environ Health. (2017) 32:303–13. doi: 10.1515/reveh-2017-0009
94. Brown RC, Lockwood AH, Sonawane BR. Neurodegenerative diseases: an overview of environmental risk factors. Environ Health Perspect. (2005) 13:1250–6. doi: 10.1289/ehp.7567
95. Hecker M, Bühring J, Fitzner B, Rommer PS, Zettl UK. Genetic, environmental and lifestyle determinants of accelerated telomere attrition as contributors to risk and severity of multiple sclerosis. Biomolecules. (2021) 11:1510. doi: 10.3390/biom11101510
96. Leso V, Caturano A, Vetrani I, Iavicoli I. Shift or night shift work and dementia risk: a systematic review. Eur Rev Med Pharmacol Sci. (2021) 17:1527. doi: 10.3390/ijerph17051527
97. Waite LM. Treatment for Alzheimer's disease: has anything changed? Aust Prescr. (2015) 38:60–3. doi: 10.18773/austprescr.2015.018
Keywords: epidemiology, potentials, neurodegenerative diseases, East Africa, meta-analysis
Citation: Onohuean H, Akiyode AO, Akiyode O, Igbinoba SI and Alagbonsi AI (2022) Epidemiology of neurodegenerative diseases in the East African region: A meta-analysis. Front. Neurol. 13:1024004. doi: 10.3389/fneur.2022.1024004
Received: 27 August 2022; Accepted: 18 October 2022;
Published: 17 November 2022.
Edited by:
Sirwan Darweesh, Radboud University Medical Centre, NetherlandsReviewed by:
Oluwafemi Gabriel Oluwole, University of Cape Town, South AfricaCopyright © 2022 Onohuean, Akiyode, Akiyode, Igbinoba and Alagbonsi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hope Onohuean, b25vaHVlYW5AZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.