
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Neurol., 31 January 2022
Sec. Dementia and Neurodegenerative Diseases
Volume 12 - 2021 | https://doi.org/10.3389/fneur.2021.805135
 Gregory D. Scott1,2*
Gregory D. Scott1,2* Moriah R. Arnold3
Moriah R. Arnold3 Thomas G. Beach4
Thomas G. Beach4 Christopher H. Gibbons5
Christopher H. Gibbons5 Anumantha G. Kanthasamy6Russell M. Lebovitz7Afina W. Lemstra8Leslie M. Shaw9
Anumantha G. Kanthasamy6Russell M. Lebovitz7Afina W. Lemstra8Leslie M. Shaw9 Charlotte E. Teunissen10
Charlotte E. Teunissen10 Henrik Zetterberg11,12,13,14,15Angela S. Taylor16
Henrik Zetterberg11,12,13,14,15Angela S. Taylor16 Todd C. Graham16
Todd C. Graham16 Bradley F. Boeve17Stephen N. Gomperts18Neill R. Graff-Radford19
Bradley F. Boeve17Stephen N. Gomperts18Neill R. Graff-Radford19 Charbel Moussa20
Charbel Moussa20 Kathleen L. Poston21Liana S. Rosenthal22
Kathleen L. Poston21Liana S. Rosenthal22 Marwan N. Sabbagh23
Marwan N. Sabbagh23 Ryan R. Walsh24
Ryan R. Walsh24 Miriam T. Weber25
Miriam T. Weber25 Melissa J. Armstrong26
Melissa J. Armstrong26 Jee A. Bang27Andrea C. Bozoki28Kimiko Domoto-Reilly29
Jee A. Bang27Andrea C. Bozoki28Kimiko Domoto-Reilly29 John E. Duda30,31
John E. Duda30,31 Jori E. Fleisher32Douglas R. Galasko33
Jori E. Fleisher32Douglas R. Galasko33 James E. Galvin34
James E. Galvin34 Jennifer G. Goldman35Samantha K. Holden36Lawrence S. Honig37
Jennifer G. Goldman35Samantha K. Holden36Lawrence S. Honig37 Daniel E. Huddleston38
Daniel E. Huddleston38 James B. Leverenz39
James B. Leverenz39 Irene Litvan33Carol A. Manning40
Irene Litvan33Carol A. Manning40 Karen S. Marder37Alexander Y. Pantelyat41
Karen S. Marder37Alexander Y. Pantelyat41 Victoria S. Pelak42
Victoria S. Pelak42 Douglas W. Scharre43
Douglas W. Scharre43 Sharon J. Sha21Holly A. Shill23
Sharon J. Sha21Holly A. Shill23 Zoltan Mari44
Zoltan Mari44 Joseph F. Quinn45,46†
Joseph F. Quinn45,46† David J. Irwin47,48,49,50†
David J. Irwin47,48,49,50†The Lewy Body Dementia Association (LBDA) held a virtual event, the LBDA Biofluid/Tissue Biomarker Symposium, on January 25, 2021, to present advances in biomarkers for Lewy body dementia (LBD), which includes dementia with Lewy bodies (DLBs) and Parkinson's disease dementia (PDD). The meeting featured eight internationally known scientists from Europe and the United States and attracted over 200 scientists and physicians from academic centers, the National Institutes of Health, and the pharmaceutical industry. Methods for confirming and quantifying the presence of Lewy body and Alzheimer's pathology and novel biomarkers were discussed.
The Lewy Body Dementia Association (LBDA) Research Centers of Excellence presented a virtual symposium on biomarkers for consideration in clinical trials on January 25, 2021. The goals were to identify biomarkers that may be useful as inclusion criteria and as outcome measures in clinical trials in Lewy body dementia (LBD) which is a major opportunity to improve clinical trials for these individuals (1). The discussion was confined to biomarkers in body fluids and tissues and did not extend to other modalities such as neuroimaging. Given that the majority of people with LBD harbor both Lewy body and Alzheimer's disease (AD) pathology (2–5), options for identifying and quantifying the presence of each of these types of pathology were reviewed. Novel biomarkers for related disease processes such as endolysosomal trafficking were also evaluated. Although the focus of the symposium was to assess candidate biomarkers for potential use in clinical trials, the role of biomarkers in disease pathophysiology was also considered.
Two modalities for detecting pathologic alpha-synuclein were discussed: seeded aggregation assays (SAAs) and immunohistochemical detection of pathologic alpha-synuclein (Table 1). SAAs, also described as protein misfolding cyclic amplification (PMCA) or real-time quaking-induced conversion (RT-QuIC) assays, amplify small amounts of aggregated protein in body fluids or tissue homogenates in an iterative process of aggregation and partial disaggregation (6). Such assays have become a focus of alpha-synuclein biomarker research since measurement of total, phosphorylated, and oligomeric alpha-synuclein in cerebrospinal fluid (CSF) and serum has to date failed to demonstrate acceptable diagnostic value (14). SAAs are well developed as a clinically useful assay in prion disease, and several laboratories have now adapted the methods for detecting aggregated alpha-synuclein in biofluids (15–18). Dr. Lebovitz described published studies documenting that the specificity and sensitivity of the PMCA assay in CSF samples from clinically diagnosed individuals with Parkinson's disease (PD) is >90% (6, 17, 19). In dementia with Lewy bodies (DLBs), seeding activity is significantly increased over PD, so it is perhaps not surprising that test specificity and sensitivity are also >90% for individuals with DLB vs. controls and individuals with DLB vs. nonsynucleinopathies (16, 20, 21). Furthermore, certain diseases not typically classified as synucleinopathies have been shown to possess subtypes with incidental findings of Lewy body pathology. Previous studies utilizing SAA report that clinically diagnosed patients with AD were found to have aggregated synuclein in CSF in 5/14 cases (36%) (19). Until now, SAAs have been assessed only in clinically-diagnosed cases; however, evaluation of diagnostic value in pathologically confirmed individuals is underway.
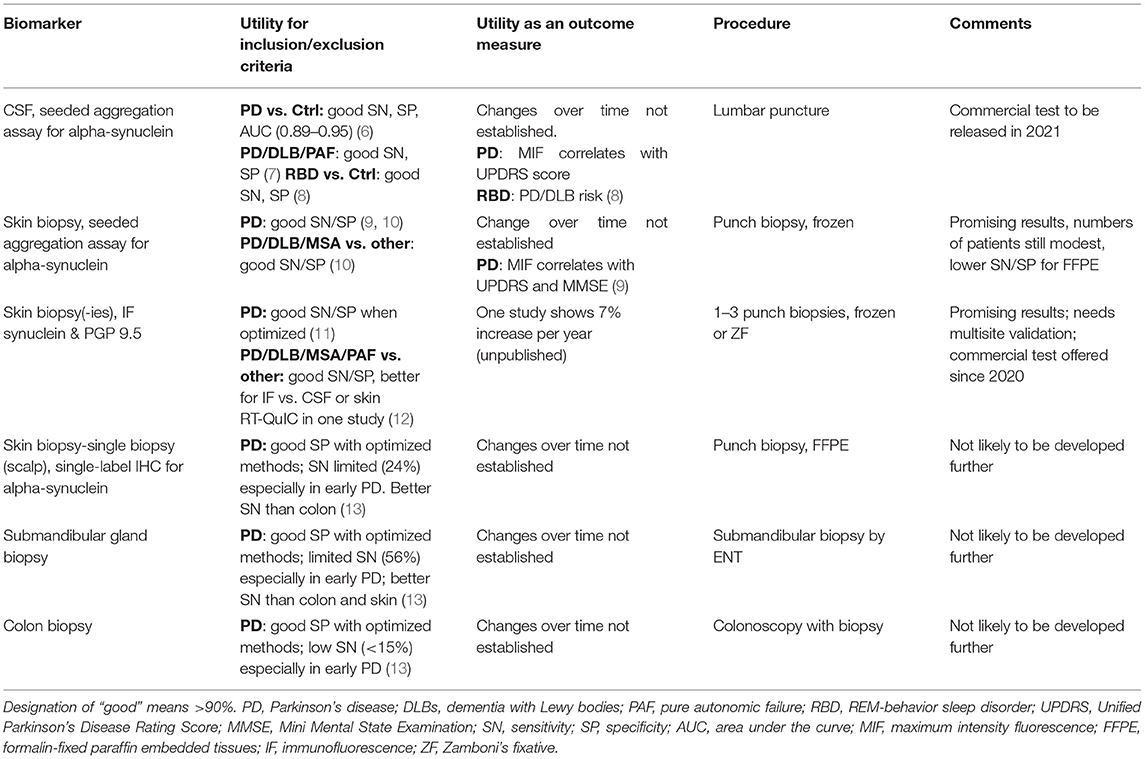
Table 1. Fluid and tissue biomarkers of alpha-synuclein pathology.
In a cohort of 120 patients with a majority of AD clinical diagnoses, the PMCA assay, using antemortem CSF samples, correctly identified Lewy body pathology with a sensitivity of 61.5% and a specificity of 100%, when compared to autopsy findings (unpublished). Interestingly, when broken down by Lewy body distribution, people with AD who harbored Lewy bodies mainly in the amygdala at autopsy were detected only 13% (2/15) of the time with the PMCA assay, suggesting that this assay may not be suitable for certain subtypes of LBD (unpublished). Patients clinically diagnosed with PD or DLB and had autopsy-confirmed Lewy body pathology tested positive by the PMCA assay 4/4 (100%) and 6/8 (75%), respectively (unpublished). Quantitative aspects of the assays (e.g., time to amplification, maximal fluorescence) still require further testing. Data examining these metrics across individuals of advancing disease state (measured by postmortem alpha-synuclein), within individuals longitudinally, and with larger sample sizes are ongoing and are needed to demonstrate clinical utility.
Dr. Beach provided a history of efforts since 2007 to develop immunohistochemical detection of pathologic alpha-synuclein in peripheral tissues as a biomarker of PD. Initial studies in colon biopsies were limited by high false-positive rates and poor interrater reliability, but subsequent multicenter studies concluded that these problems could be addressed by the screening of multiple candidate methods and training of raters. Following such optimization, sensitivity and specificity of colon biopsy in autopsy tissue were excellent (100% accuracy for one method albeit in limited numbers of individuals) and could be useful diagnostically (13, 22, 23). However, the question of whether the colon was the best site for biopsy remained, due to an insufficient amount of submucosa obtained with current biopsy methods and invasiveness. Subsequent studies compared colon, submandibular gland, and skin biopsy. The Systemic Synuclein Sampling Study (“S4 Study”) employed consensus slide-reading by a panel of 5 specially trained neuropathologists, all blinded to diagnosis (13). The S4 Study found >90% specificity but disappointingly low sensitivity (56% in submandibular gland, 24% in skin, and very low sensitivity in colon). This may in part be attributable to the overrepresentation of early PD cases in the S4 Study: one-third of cases had a median disease duration of only 8 months, and the median disease duration for the entire PD group was 42 months (13). Sensitivity was greater in participants with more advanced PD, particularly in submandibular gland biopsies (76%). Dr. Beach concluded that improvement in the sensitivity of immunohistochemical methods was needed, or alternatively, SAAs such as RT-QuIC may soon supersede them. He hypothesized that whereas SAAs are already being done on CSF with very promising potential, peripheral tissue deposits may be a better model of brain tissue deposits and also perhaps a better measure of target engagement for monoclonal antibodies and other new therapeutic approaches.
Skin biopsy in the S4 Study consisted of two 3-mm skin punch biopsies obtained from the paravertebral posterior–inferior cervical area and mid-thigh; immunohistochemical labeling was performed with an alpha-synuclein antibody after protease pretreatment. Dr. Gibbons presented a distinct approach to skin biopsy involving three punch biopsies from the distal leg, distal thigh, and posterior cervical region in people with PD and DLB, using a double-label immunofluorescence method to detect and colocalize both alpha-synuclein and neuronal markers (PGP 9.5) in thick sections (11, 24, 25). His team found higher sensitivity than the S4 Study for a single biopsy (74%) and increased sensitivity when considering two (90%) or three (96%) biopsies (unpublished data presented at American Academy of Neurology Conference, 2020). They reported overall outstanding sensitivity and specificity for skin biopsy in this study and subsequent validation (accuracy 99.1%) as a laboratory-developed test, the “SYN-ONE” test (CND Life Sciences™), for discriminating peripheral synucleinopathies (PD, DLB, multiple system atrophy, pure autonomic failure) from controls (unpublished). In discussion, it was noted that Dr. Gibbons' unpublished data correlated with clinical scores including the Unified Parkinson's Disease Rating Scale (UPDRS), Orientation and Mobility Severity Rating Scale (OMSR), and DLB Cognitive Scale (unpublished). Biopsy acquisition was performed, using the SYN-ONE test, as part of a multicenter center study supported by the NIH Office of Rare Diseases (Autonomic Disorders Consortium). An additional multisite blinded study funded by NIH is currently underway to evaluate how this approach fares in the environment of multiple academic and private practice sites with a core reference laboratory-developed test. The skin biopsies prepared in this manner can also be quantified, and the first quantitative studies show significant autonomic and sensory nerve fiber density differences between groups, individuals with DLB having the most severe autonomic and sensory neuropathies, followed by idiopathic PD, and finally multiple system atrophy (MSA), without evidence of peripheral nerve degeneration. Dr. Gibbon's group also recently reported that cutaneous phospho-alpha-synuclein is moderately correlated (r = 0.6) with both sympathetic and total autonomic impairment in individuals with isolated REM sleep behavior disorder (iRBD) and is more common in iRBD with hyposmia (26).
The final speaker in this session, Dr. Kanthasamy, linked the SAA and tissue biopsy approaches by presenting results from skin biopsy samples that were analyzed not with immunohistochemistry but instead homogenized and processed with RT-QuIC. After establishing the method with autopsied brain tissue and submandibular gland (15, 27), his group compared skin samples from individuals with PD and controls and found that the SAAs performed on skin homogenates yielded a specificity of 96% and sensitivity of 96% (9). The maximal fluorescence metric from the seeding assay also correlated with disease severity (UPDRS p < 0.0001; Mini-Mental Status Examination (MMSE) p = 0.0035), suggesting that quantitative aspects of this assay might be useful as a marker of disease state and potentially as an outcome measure in clinical trials targeting alpha-synuclein. An advantage of seeding assays over immunohistochemistry is that they do not require extended review by specially trained neuropathologists.
Dr. Lemstra provided a summary of CSF biomarkers for AD pathology in LBD (Table 2). Studies in neuropathologically-confirmed cases have shown that mixed pathology can be detected antemortem with CSF biomarkers using similar cutoffs employed for AD. Larger in vivo cohorts including the European DLB Consortium (E-DLB), Mayo Clinic Cohort, and Amsterdam Dementia Cohort have shown that AD biomarkers, either CSF (most commonly CSF tau/Aβ42 ratio) or PET markers, are increased in DLB over PD and PDD and correlate with DLB dementia, progression, and survival. Evidence suggests that these Alzheimer markers likely reflect concomitant Alzheimer pathological process along with the Lewy body disease. Specifically, AD biomarker in DLB (DLB-AD) is defined by the presence of AD biomarkers unlike DLB-pure (DLB-p) and is a common subtype (at least 50%) of DLB characterized by more rapid clinical deterioration and mortality (33). DLB-AD is associated with increased age, female sex, increased APOE ε4 genotype, decreased memory, increased delusions and hallucinations, less REM-behavior sleep disorder and parkinsonism, worse language performance, faster progression, increased temporal thinning and tau pathology, and greater risk of institutionalization and mortality (2–4, 33–37). These findings are corroborated by postmortem clinicopathologic studies which show that AD pathologic features (neuritic plaques and also tangles) in cases clinically defined as “probable DLB” are associated with an atypical “Alzheimerized” clinical presentation (e.g., worse performed on orientation and memory testing) (57, 58). Dr. Lemstra also presented studies that show CSF AD biomarkers do not appear to influence positivity rates of DaTscan (59) or electroencephalography (60) but emphasized that more studies are needed. Different amyloid-beta species were also discussed as possible biomarkers for discriminating DLB from AD. Unlike AD, in which Aβ42 is more selectively decreased, multiple studies have shown that DLB exhibits a broader decrease of multiple amyloid-beta species (Aβ38, Aβ40, Aβ42). Furthermore, these studies show that some species of amyloid-beta (Aβ38, Aβ40) decrease independently of AD biomarkers (CSF tau/Aβ42) and APOE genotype, and some species (Aβ38) correlate with disease duration. Ratios (Aβ42/Aβ38) can discriminate clinical DLB from AD with moderate accuracy (sensitivity 78%, specificity 67%) (28, 29). Limited data suggest a negative association between symptomatic treatment with acetylcholinesterase inhibitors in DLB and longitudinal changes in AD biomarkers (61). It was proposed that DLB-AD could be considered for recruitment into clinical trials for amyloid-modifying therapy in the research setting, but future study is needed to clarify the relationship between amyloid deposition and clinical symptoms in AD and DLB-AD.
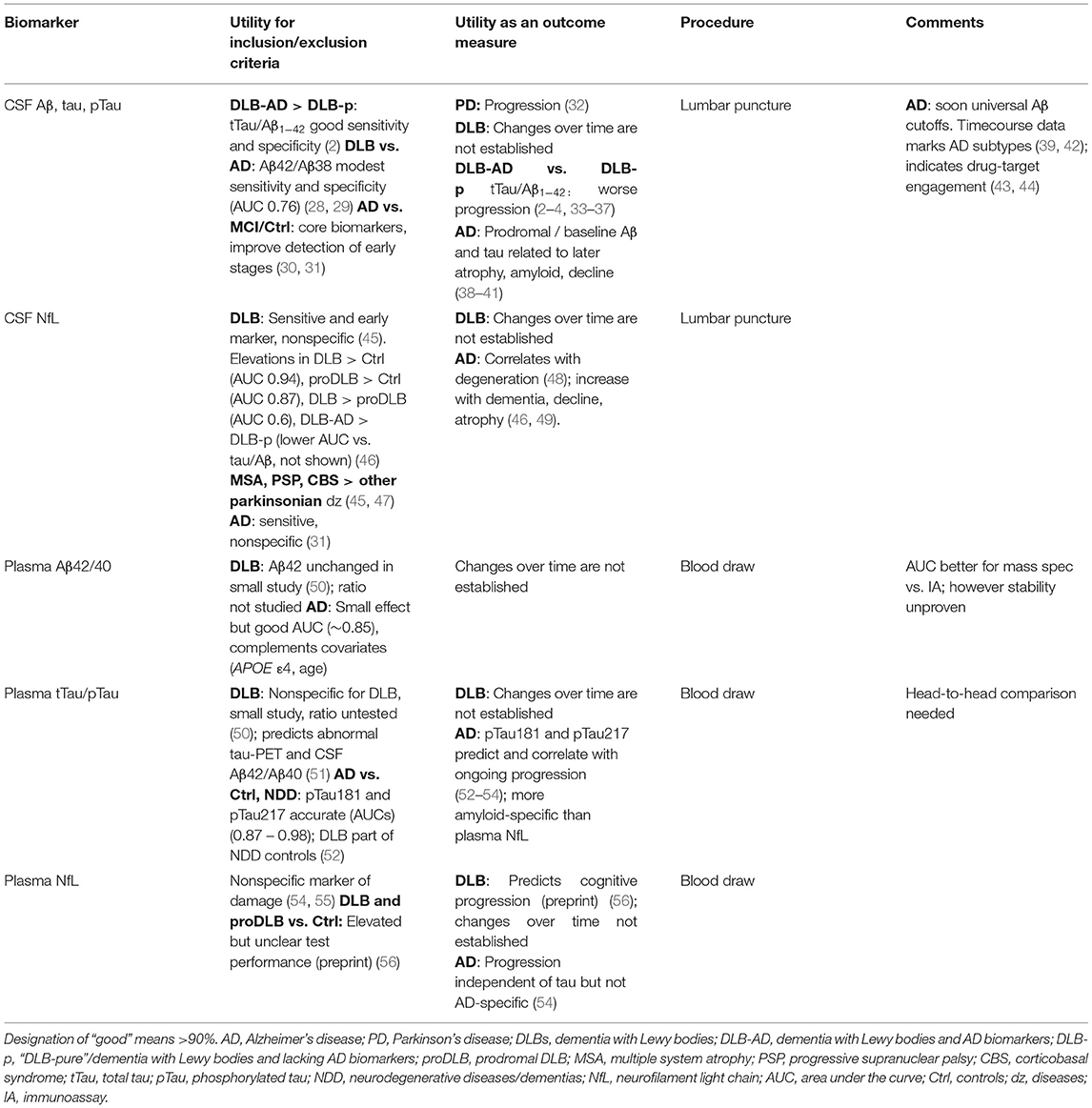
Table 2. Fluid and tissue biomarkers of AD pathology.
The final speaker, Dr. Shaw, summarized progress in blood biomarkers for AD, mainly focusing on targets whose studies are well underway (Aβ42/40, pTau181 and 217, neurofilament light chain [NfL]), with a brief mention of earlier-stage targets (alpha-synuclein, TDP-43, GFAP, NPTX2). Plasma Aβ42/40 as a biomarker shows small but reproducible absolute differences in amyloid-positive (by PET) vs. amyloid-negative patients and shows early promise as a screening test alongside covariates, APOE ε4 genotype, and age. In general, the area under the receiver operating characteristic curve (AUC) has been better in mass spectrometry studies (AUC 0.82–0.89) (62, 63) than immunoassays (AUC 0.65–0.77, up to 0.80 when Aβ42 and Aβ40 were used in a logistic regression model instead of the Aβ42/Aβ40 ratio) (64). A large head-to-head round robin study [Foundation for the National Institutes of Health Biomarkers Consortium (FNIH BC)/Alzheimer's Disease Neuroimaging Initiative (ADNI)] nearing completion will compare 3 mass spectrometry and 3 immunoassays for plasma Aβ42/40 ratio concordance with amyloid-PET. pTau181 and pTau217, tested by immunoassay or by mass spectrometry, can reliably detect tau pathology and levels correlate with amyloid PET, cerebral atrophy, and cognitive decline (53, 65). Some reports suggest that pTau217 has somewhat superior sensitivity and specificity vs. pTau181 for discriminating AD from other disorders and healthy controls (66), but more head-to-head studies are needed to definitively address this question. Preanalytical, analytical, and clinical replication studies are underway in international groups, and there are multiple companies developing diagnostic tests for these targets. Dr. Shaw also highlighted the importance of detailed preanalytical studies to test variables such as delayed centrifugation at room temperature and freeze-thaw cycles that can affect these measurements. The Alzheimer's Association Global Biomarker Standardization Consortium recently reported that these findings at the 2021 Alzheimer's Association International Conference, underscoring the need to resolve interlaboratory differences before widespread clinical applications, are implemented. NfL was also briefly mentioned as a third well-studied biomarker of nonspecific neurodegeneration that needs larger head-to-head confirmatory studies. During the discussion, other promising pTau targets were mentioned including pTau231 and diphosphorylated peptides. Low DLB enrollment in these studies was noted, and ongoing consortia were highlighted that are measuring pTau181, pTau231 and Aβ42/40, NfL, and glial fibrillary acidic protein (GFAP). Newer CSF and plasma biomarkers for AD, Lewy body, and non-AD neurodegenerative disorders are also reviewed elsewhere (67).
Two modalities for the discovery of novel CSF biomarkers were discussed: mass spectrometry and antibody array proteomics (Table 3). Mass spectrometry is an unbiased approach with longstanding precedent in laboratory testing and biomarker research (e.g., plasma AD markers discussed above), whereas newer antibody arrays, such as O-link® Proximity Extension Assay (PEA) discussed below, offer more targeted, higher throughput, and potentially more sensitive multiplexed immunoassays. Interestingly, these technologies have been shown to cover different fractions of the proteome, leading to partly complementary results (70).
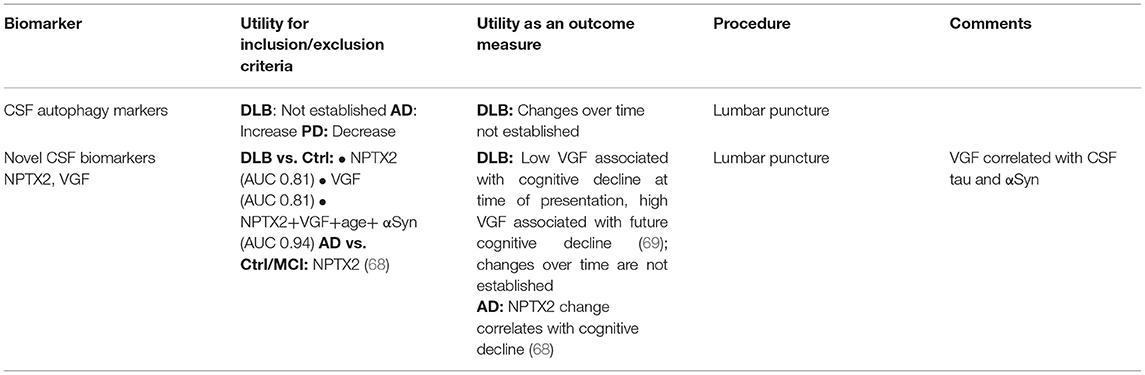
Table 3. Fluid and tissue biomarkers for other disease mechanisms.
Dr. Zetterberg presented CSF mass spectrometry data of a panel of proteins involved in endolysosomal and autophagosome processing. These fundamental intracellular sorting organelle systems have been implicated by genetic and histologic studies in DLB [reviewed in Arotcarena et al. (71)] but have rarely been studied in CSF. Dr. Zetterberg presented data from the measurement of these proteins quantitatively in AD and PD and achieved simultaneous measurement of 18 related proteins in approximately 0.2 ml of CSF. The team's results show a pattern of increase in AD vs. controls for many lysosomal markers (e.g., cathepsin B, LAMP2) and endocytosis (AP2) and ubiquitin whereas there was a decrease in PD for the same group of proteins. The causes of increased protein release in AD and decreased release in PD are unknown but results argue against nonspecific neurodegeneration since results for AD and PD are in the opposite direction. Discussants noted similar decreases across multiple proteins (synuclein, tau, Aβ) in the Parkinson's Progression Markers Initiative (PPMI) cohort and one speculated unifying explanation was retromer dysfunction (72). Studies in patients with DLB have not yet been performed using this approach.
The second speaker, Dr. Teunissen, first discussed biomarker discovery in DLB using mass spectrometry and ELISA validation. Six potential targets were identified in DLB vs. control including downregulation of neurosecretory protein VGF, neuronal pentraxin-2 (NPTX2), neuroendocrine convertase 2 (PCSK2), neuronal pentraxin receptor (NPTXR), upregulation of ubiquitin carboxyl-terminal hydrolase (USP14), and proteasome subunit beta type-7 (PSMB7) (73). The extent of downregulation of NPTX2 and VGF in DLB was greater than but overlapped with the extent of downregulation in AD and PD. It is unclear whether DLB patients with lower NPTX2 have more amyloid pathology, a potentially important distinction given that AD studies (e.g., ADNI) also find NPTX2 dysregulation (68). In the second half of his presentation, Dr. Teunissen presented early results of a broad search for distinguishing a DLB subgroup with AD CSF biomarkers (DLB-AD) using multiplexed immunoassay arrays, Olink®, discussed briefly above. Interestingly, Dr. Teunissen's early data disagree with the hypothesis that biomarkers for DLB-AD represent a simple combination of biomarkers for Lewy body disease plus AD. The team found that DLB-AD had unique features compared to DLB-p and AD, including lower CSF protein levels and specific protein differences. In contrast, few differences in proteins were observed between DLB-p and AD in these data. The identity of these proteins enriched in DLB-AD included cell adhesion, cytokine–cytokine interactions, axon guidance, and neurogenesis. Preliminary validation studies with a more quantitative immunoassay, the Ella® system, show replication of Olink® hits and further discriminatory power of candidate proteins in addition to pTau and tTau in distinguishing DLB from AD.
There was agreement by the presenters regarding the urgent need for sensitive and specific in vivo biomarkers to detect alpha-synuclein pathology, which has the potential to improve therapeutic targeting and also to inform disease pathogenesis. Panel discussants provided insights into the logistics and needs for further validation of emerging peripheral tissue biopsies and SAAs for these approaches to reach utility in therapeutic trials and eventually clinical use. Key gaps include the need for further autopsy validation, longitudinal analyses, and standardization of assay methods. Indeed, there are animal and cell-model data which suggest that alpha-synuclein pathology can spread throughout the nervous system (74, 75), but it remains unclear whether and how this occurs in humans. The Braak staging system for PD suggests that pathology begins in the peripheral autonomic nervous system or olfactory bulb and then migrates proximally to the amygdala and brainstem and in the more severe cases, to the cerebral cortex (76). This model is supported by some human studies, such as those of multiple groups finding high levels of alpha-synuclein pathology in skin biopsies in early PD and REM-sleep behavior disorder (RBD) without other clinical evidence of synucleinopathy (12, 25, 26, 77–79). However, the model is not supported by other large autopsy-based studies that find no evidence of peripheral-first synucleinopathy (e.g., stomach vs. brain) and that peripheral synucleinopathy is more common and severe in later stages (80, 81). Overall, these observations combined with the fact that limbic Lewy body pathology may occur prior to brainstem pathology in the course of DLB, indicate that the initiation and propagation of Lewy body pathology is varied among the synucleinopathies (82) and may vary by predictors such as genotype, and that future study is needed to resolve these findings.
In contrast to biomarkers of alpha-synuclein, sensitive AD biomarkers are established and provide a link between clinical and pathologic aspects of DLB with and without AD pathology. Panelists agreed with the potential importance of stratifying therapeutic trial inclusions and/or outcomes based on AD biomarker profiles in LBD due to the strong association of these biomarkers with clinical outcomes, exemplified by the prospective data in the European DLB (E-DLB) consortium. The frequency of AD pathology in DLB (DLB-AD) varies between 25 and 89% depending on biomarker cutoffs and diagnostic criteria (2–5). Distinct lines of evidence have shown that DLB-AD may represent a biological interaction of these mixed amyloid-beta, tau, and alpha-synuclein pathologies. In clinically defined DLB, unpublished data suggest that DLB-AD appears to exhibit a distinct CSF immunophenotypic pattern, raising the importance of exploratory biomarker discovery work to further refine biological subgroups in DLB. Moreover, in autopsy-defined DLB, there is lower overall tau compared to AD and higher temporal lobe enrichment of tau that is associated with both cortical thinning and cognitive impairment (37, 83). Although the longitudinal assessment of AD biomarker progression in DLB is understudied, there are conflicting results in PD (32, 84) that appear to be explained by variable disease stages and methods of measurement in individual studies, but also intrinsic biological variability between patients. Thus, future prospective longitudinal DLB-specific studies with autopsy-confirmation are needed to quantitatively compare the time course of amyloid and tau biomarkers and to consider potential DLB-specific cutoffs. By enabling the study of homogenous patient populations with similar underlying biology, these efforts will increase the capacity to assess treatment outcomes in DLB-focused clinical trials.
Overall, rapid progress has been made in the development of fluid and tissue-based biomarkers for Lewy body dementia and they show promise as useful tools. Further external validation and translational research are needed specifically in individuals with Lewy body dementia to accurately determine biomarker test characteristics and overall determine how these individuals may benefit from such a biomarker test.
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
This study is supported by the Lewy Body Dementia Association.
TB has conducted consultation for a peripheral synuclein assay and speakers honorarium from Roche Diagnostics. RL is employed full time by Amprion, serves on Amprion's Board, and is a shareholder. CT research is supported by the European Commission (Marie Curie International Training Network, grant agreement No 860197 (MIRIADE), and JPND), Health Holland, the Dutch Research Council (ZonMW), Alzheimer Drug Discovery Foundation, the Selfridges Group Foundation, Alzheimer Netherlands, Alzheimer Association. CT is the recipient of ABOARD, which is a public-private partnership receiving funding from ZonMW (#73305095007) and Health Holland, Topsector Life Sciences & Health (PPP allowance; #LSHM20106). More than 30 partners participate in ABOARD. ABOARD also receives funding from Edwin Bouw Fonds and Gieskes Strijbisfonds. IV is appointed on a research grant by Alzheimer Nederland (NL 17004). CT has a collaboration contract with ADx Neurosciences, Quanterix, and Eli Lilly, who performed contract research or received grants from AC Immune, Axon Neurosciences, Biogen, Brainstorm Therapeutics, Celgene, EIP Pharma, Eisai, PeopleBio, Roche, Toyama, Vivoryon. CT serves on editorial boards of Medidact Neurologie/Springer, Alzheimer Research and Therapy, Neurology: Neuroimmunology and Neuroinflammation, and is editor of a Neuromethods book by Springer. HZ has served at scientific advisory boards and/or as a consultant for Abbvie, Alector, Eisai, Denali, Roche Diagnostics, Wave, Samumed, Siemens Healthineers, Pinteon Therapeutics, Nervgen, AZTherapies, CogRx, and Red Abbey Labs has given lectures in symposia sponsored by Cellectricon, Fujirebio, Alzecure and Biogen, and is a co-founder of Brain Biomarker Solutions in Gothenburg AB (BBS), which is a part of the GU Ventures Incubator Program (all outside submitted work). CMo is an inventor of several US and International Georgetown University patents to use tyrosine kinase inhibitors (TKis) for the treatment of neurodegenerative diseases. CMo is a co-founder and shareholder and receives consulting fees from KeifeRx LLC. CMo receives consulting fees from Neumentum LLC, SUn Pharmaceuticals Research Industry, and SkyBIo. CMo received NIH NIA funding, Alzheimer's Association, and Sun Pharmaceuticals Research Industry Funding to study TKis in neurodegeneration, including LBD. KP has received consulting fees from Curasen and is funded by grants from the NIH, Michael J Fox Foundation for Parkinson's Research, LBDA, and Alzheimer's Drug Discovery Foundation, and has received funding from Sanofi US Services, Inc. to perform clinical trials. MS declares ownership interest (Stock or stock options): Brain Health Inc, NeuroTau, Optimal Cognitive Health Company, uMethod Health, Versanum, Athira, Cognoptix and consulting work for Alzheon, Biogen, Cortexyme, Roche Genentech, Stage 2 Innovations/Renew Research, Acadia, T3D, Eisai, KeifeRx. MS also declares royalties: HarperCollins, Humanix and speakers bureau: Health and Wellness Partners. LR receives grant funding from the NINDS, Michael J. Fox Foundation, Parkinson's Foundation, and National Ataxia Foundation. She has also served on advisory boards for Uniqure and other pharmaceutical companies through the Parkinson's Study Group. MJA receives research support from the NIA (R01AG068128, P30AG047266), the Florida Department of Health (Grant 20A08), and as the local PI of a Lewy Body Dementia Association Research Center of Excellence. MJA serves on the data safety monitoring boards (DSMBs) for ACTC/ATRI and ADCS. MJA receives royalties from the publication of the book Parkinson's Disease: Improving Patient Care. MJA serves on the level of evidence editorial board for Neurology and related publications (uncompensated). JGG declares grants/research—Acadia, Michael J. Fox Foundation, Parkinson's Foundation, Consultant—Worldwide Med, Honoraria—American Academy of Neurology, Davis Phinney Foundation, International Parkinson and Movement Disorders Society, Medscape, Parkinson's Foundation, Other: Lewy Body Dementia Association Research Center of Excellence. ZM received institutional grant support from NIH, MJFF, LBDA, Parkinson's Foundation, Eli Lilly, NeuroDerm, Cerevel Therapeutics and personal consulting honoraria from Global Kinetics Corporation, GB Sciences, ACADIA, PSG, Elsevier, Kyowa Kirin, AbbVie, and Supernus. IL's research is supported by the National Institutes of Health Grants: 2R01AG038791-06A, U01NS100610, U01NS80818, R25NS098999; U19 AG063911-1 and 1R21NS114764-01A1; the Michael J Fox Foundation, Parkinson Foundation, Lewy Body Association, CurePSP, Roche, Abbvie, Biogen, Centogene. EIP-Pharma, Biohaven Pharmaceuticals, Novartis, Brain Neurotherapy Bio, and United Biopharma SRL—UCB. IL was a member of the Scientific Advisory Board of Lundbeck and is a Scientific Advisor for Amydis and Rossy Center for the Progressive Supranuclear Palsy University of Toronto. IL receives her salary from the University of California San Diego and as Chief Editor of Frontiers in Neurology. JL receives grant funding from the NIH/NIA/NINDS (P30AG072959/P30AG062428/U01NS100610), LBDA, GE Healthcare and serves as a consultant for Eisai Pharmaceuticals. RW serves on the data safety monitoring boards for Alexion, Bukwang, and Sarepta Pharmaceuticals and the Scientific Platform Steering Committee for Adams Pharmaceuticals. RW serves as a consultant for Lundbeck, Acadia, Teva, Abbvie, Alexion, Adamas, Prime, Bukwang, Sarepta, Syneos, Techspert, Guidepoint and also for R01R01NS117547 with Principal Investigator, Virendra Mishra. AL has received research support from the Dutch Research Council (ZonMW), Alzheimer Netherlands, Dioraphte Foundation, AL has given lectures in symposia sponsored by GE. CG is a scientific consultant and has stock in CND Life Sciences. SG has served on Advisory Boards of Jannsen, Acadia, and Sanofi, has received consulting fees from EIP Pharma, and has received funding from the NIH, the DOD CDMRP, the Michael J. Fox Foundation, the FFFPRI, and the Lewy Body Dementia Association. BB has served as an investigator for clinical trials sponsored by Alector, EIP Pharma, and Biogen. He serves on the Scientific Advisory Board of the Tau Consortium. He receives institutional research support from the NIH, the Lewy Body Dementia Association Research Centers of Excellence Program, the Mayo Clinic Dorothy and Harry T. Mangurian Jr. Lewy Body Dementia Program, the Little Family Foundation, and the Ted Turner and Family Foundation. AP serves on the Scientific Advisory Board of MedRhythms, Inc. and receives research support from the Lewy Body Dementia Association (as Co-Director of the Johns Hopkins LBDA Research Center of Excellence) and NIH/NINDS/NIA (U01NS102035; K23AG059891). DG receives research support from NIA (AG062429), the State of California, and the Michael J. Fox Foundation, which is a paid consultant for Biogen, Roche, Esai, Cognition Therapeutics, Fujirebio, Amprion, Generian, and Editor of Alzheimer's Research & Therapy. DH is supported by The Michael J. Fox Foundation (MJFF-010556), NIH-NINDS 1K23NS105944-01A1, the American Parkinson's Disease Association Center for Advanced Research (Emory University), and the Lewy Body Dementia Association Research Center of Excellence (Emory University). JF is on the editorial board of the American Academy of Neurology's Brain and Life magazine (uncompensated), Lewy Body Dementia Association Scientific Affairs Committee (uncompensated), and has received honoraria from Parkinson's Foundation. JF receives grant funding from the NIH/NIA/NINDS (K23NS097615, 5P30AG064200-02), CurePSP, and Parkinson's Foundation. KD-R receives research funding from the NIH (P30 AG066509) and LBDA Research Center of Excellence; has served on a Biogen advisory board; receives speakers honoraria from MedBridge. LS receives research support from NIH/NIA U19 AG024904, ADNI3 grant; NIH/NIA P30 AG010124, UPENN ADCC grant; and the Michael J. Fox Foundation for Parkinson's Research. He is a consultant for Biogen and Roche Diagnostics and is on the speaker's bureaus for Biogen and Fujirebio. DI receives research funding from NIH (R01-NS109260, P01-AG066597, U19-AG062418, U01-NS100610), Penn Institute on Aging and is the co-PI of the Penn LBDA Research Centers of Excellence. He is a member of the scientific advisory board of Denali Therapeutics. LH is a paid consultant for Biogen, Cortexyme, Eisai, Medscape, and Prevail. LH receives grant support from NIA, NINDS, LBDA, Acumen, Alector, Avanir, Eisai, Genentech/Roche, Janssen/Johnson & Johnson, NovoNordisk, Transposon, UCB, and Vaccinex. JD receives research funding from NIH, the Department of Veterans Affairs, the Michael J. Fox Foundation and Innervace, Inc. He is also the co-PI of the Penn LBDA Research Center of Excellence. IL is the Editor in Chief of the journal but she was not involved in the process of referee selection, peer review or the acceptance decision.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We extend our appreciation to the staff of the LBDA and all centers in the LBDA Research Centers of Excellence Program and particularly to our patients and their families for whom we serve.
1. Goldman JG, Forsberg LK, Boeve BF, Armstrong MJ, Irwin DJ, Ferman TJ, et al. Challenges and opportunities for improving the landscape for Lewy body dementia clinical trials. Alzheimers Res Ther. (2020) 12:137. doi: 10.1186/s13195-020-00703-5
2. Irwin DJ, Xie SX, Coughlin D, Nevler N, Akhtar RS, McMillan CT, et al. CSF tau and β-amyloid predict cerebral synucleinopathy in autopsied Lewy body disorders. Neurology. (2018) 90:e1038–46. doi: 10.1212/WNL.0000000000005166
3. van Steenoven I, Aarsland D, Weintraub D, Londos E, Blanc F, van der Flier WM, et al. Cerebrospinal Fluid Alzheimer's Disease Biomarkers Across the Spectrum of Lewy Body Diseases: Results from a Large Multicenter Cohort. J Alzheimers Dis. (2016) 54:287–95. doi: 10.3233/JAD-160322
4. Ferreira D, Przybelski SA, Lesnick TG, Lemstra AW, Londos E, Blanc F, et al. β-Amyloid and tau biomarkers and clinical phenotype in dementia with Lewy bodies. Neurology. (2020) 95:e3257–68. doi: 10.1212/WNL.0000000000010943
5. Dugger BN, Adler CH, Shill HA, Caviness J, Jacobson S, Driver-Dunckley E, et al. Concomitant Pathologies among a Spectrum of Parkinsonian Disorders. Parkinsonism Relat Disord. (2014) 20:525–9. doi: 10.1016/j.parkreldis.2014.02.012
6. Kang UJ, Boehme AK, Fairfoul G, Shahnawaz M, Ma TC, Hutten SJ, et al. Comparative study of cerebrospinal fluid α-synuclein seeding aggregation assays for diagnosis of Parkinson's disease. Mov Disord. (2019) 34:536–44. doi: 10.1002/mds.27646
7. Rossi M, Candelise N, Baiardi S, Capellari S, Giannini G, Orrù CD, et al. Ultrasensitive RT-QuIC assay with high sensitivity and specificity for Lewy body-associated synucleinopathies. Acta Neuropathol. (2020) 140:49–62. doi: 10.1007/s00401-020-02160-8
8. Iranzo A, Fairfoul G, Ayudhaya ACN, Serradell M, Gelpi E, Vilaseca I, et al. Detection of α-synuclein in CSF by RT-QuIC in patients with isolated rapid-eye-movement sleep behaviour disorder: a longitudinal observational study. Lancet Neurol. (2021) 20:203–12. doi: 10.1016/S1474-4422(20)30449-X
9. Manne S, Kondru N, Jin H, Serrano GE, Anantharam V, Kanthasamy A, et al. Blinded RT-QuIC Analysis of α-Synuclein Biomarker in Skin Tissue From Parkinson's Disease Patients. Movement Disorders. (2020) 35:2230–9. doi: 10.1002/mds.28242
10. Wang Z, Becker K, Donadio V, Siedlak S, Yuan J, Rezaee M, et al. Skin α-synuclein aggregation seeding activity as a novel biomarker for parkinson disease. JAMA Neurol. (2020) doi: 10.1001/jamaneurol.2020.3311
11. Kim JY, Illigens BM, McCormick MP, Wang N, Gibbons CH. Alpha-Synuclein in Skin Nerve Fibers as a Biomarker for Alpha-Synucleinopathies. J Clin Neurol. (2019) 15:135–42. doi: 10.3988/jcn.2019.15.2.135
12. Donadio V, Wang Z, Incensi A, Rizzo G, Fileccia E, Vacchiano V, et al. In Vivo diagnosis of synucleinopathies: a comparative study of skin biopsy and RT-QuIC. Neurology. (2021) 96:e2513–24. doi: 10.1212/WNL.0000000000011935
13. Chahine LM, Beach TG, Brumm MC, Adler CH, Coffey CS, Mosovsky S, et al. In vivo distribution of α-synuclein in multiple tissues and biofluids in Parkinson disease. Neurology. (2020) 95:e1267–84. doi: 10.1212/WNL.0000000000010404
14. Simonsen AH, Kuiperij B, El-Agnaf OMA, Engelborghs S, Herukka S-K, Parnetti L, et al. The utility of α-synuclein as biofluid marker in neurodegenerative diseases: a systematic review of the literature. Biomark Med. (2016) 10:19–34. doi: 10.2217/BMM.14.105
15. Manne S, Kondru N, Hepker M, Jin H, Anantharam V, Lewis M, et al. Ultrasensitive Detection of Aggregated α-Synuclein in Glial Cells, Human Cerebrospinal Fluid, and Brain Tissue Using the RT-QuIC Assay: New High-Throughput Neuroimmune Biomarker Assay for Parkinsonian Disorders. J Neuroimmune Pharmacol. (2019) 14:423–35. doi: 10.1007/s11481-019-09835-4
16. Groveman BR, Orrù CD, Hughson AG, Raymond LD, Zanusso G, Ghetti B, et al. Rapid and ultra-sensitive quantitation of disease-associated α-synuclein seeds in brain and cerebrospinal fluid by αSyn RT-QuIC. Acta Neuropathol Commun. (2018) 6:7. doi: 10.1186/s40478-018-0508-2
17. Fairfoul G, McGuire LI, Pal S, Ironside JW, Neumann J, Christie S, et al. Alpha-synuclein RT-QuIC in the CSF of patients with alpha-synucleinopathies. Ann Clin Transl Neurol. (2016) 3:812–8. doi: 10.1002/acn3.338
18. Candelise N, Schmitz M, Llorens F, Villar-Piqué A, Cramm M, Thom T, et al. Seeding variability of different alpha synuclein strains in synucleinopathies. Ann Neurol. (2019) 85:691–703. doi: 10.1002/ana.25446
19. Shahnawaz M, Tokuda T, Waragai M, Mendez N, Ishii R, Trenkwalder C, et al. Development of a Biochemical Diagnosis of Parkinson Disease by Detection of α-Synuclein Misfolded Aggregates in Cerebrospinal Fluid. JAMA Neurol. (2017) 74:163–72. doi: 10.1001/jamaneurol.2016.4547
20. Bongianni M, Ladogana A, Capaldi S, Klotz S, Baiardi S, Cagnin A, et al. α-Synuclein RT-QuIC assay in cerebrospinal fluid of patients with dementia with Lewy bodies. Ann Clin Transl Neurol. (2019) 6:2120–6. doi: 10.1002/acn3.50897
21. Bargar C, Wang W, Gunzler SA, LeFevre A, Wang Z, Lerner AJ, et al. Streamlined alpha-synuclein RT-QuIC assay for various biospecimens in Parkinson's disease and dementia with Lewy bodies. Acta Neuropathol Commun. (2021) 9:1–13. doi: 10.1186/s40478-021-01175-w
22. Beach TG, Adler CH, Sue LI, Vedders L, Lue L, White Iii C, et al. Multi-organ distribution of phosphorylated alpha-synuclein histopathology in subjects with Lewy body disorders. Acta Neuropathol. (2010) 119:689–702. doi: 10.1007/s00401-010-0664-3
23. Beach TG, Corbillé A-G, Letournel F, Kordower JH, Kremer T, Munoz DG, et al. Multicenter Assessment of Immunohistochemical Methods for Pathological Alpha-Synuclein in Sigmoid Colon of Autopsied Parkinson's Disease and Control Subjects. J Parkinsons Dis. (2016) 6:761–70. doi: 10.3233/JPD-160888
24. Gibbons CH, Garcia J, Wang N, Shih LC, Freeman R. The diagnostic discrimination of cutaneous α-synuclein deposition in Parkinson disease. Neurology. (2016) 87:505–12. doi: 10.1212/WNL.0000000000002919
25. Wang N, Garcia J, Freeman R, Gibbons CH. Phosphorylated Alpha-Synuclein Within Cutaneous Autonomic Nerves of Patients With Parkinson's Disease: The Implications of Sample Thickness on Results. J Histochem Cytochem. (2020) 68:669–78. doi: 10.1369/0022155420960250
26. Miglis MG, Zitser J, Schneider L, During E, Jaradeh S, Freeman R, et al. Cutaneous Alpha-Synuclein is Correlated with Autonomic Impairment in Isolated REM Sleep Behavior Disorder. Sleep. (2021) zsab172. doi: 10.1093/sleep/zsab172
27. Manne S, Kondru N, Jin H, Anantharam V, Huang X, Kanthasamy A, et al. α-Synuclein Real-Time Quaking-Induced Conversion in the Submandibular Glands of Parkinson's Disease Patients. Movement Disorders. (2020) 35:268–78. doi: 10.1002/mds.27907
28. van Steenoven I, van der Flier WM, Scheltens P, Teunissen CE, Lemstra AW. Amyloid-β peptides in cerebrospinal fluid of patients with dementia with Lewy bodies. Alzheimers Res Ther. (2019) 11:83. doi: 10.1186/s13195-019-0537-5
29. Mulugeta E, Londos E, Ballard C, Alves G, Zetterberg H, Blennow K, et al. amyloid β38 as a novel diagnostic marker for dementia with Lewy bodies. J Neurol Neurosurg Psychiatry. (2011) 82:160–4. doi: 10.1136/jnnp.2009.199398
30. Blennow K, Hampel H, Weiner M, Zetterberg H. Cerebrospinal fluid and plasma biomarkers in Alzheimer disease. Nat Rev Neurol. (2010) 6:131–44. doi: 10.1038/nrneurol.2010.4
31. Olsson B, Lautner R, Andreasson U, Öhrfelt A, Portelius E, Bjerke M, et al. CSF and blood biomarkers for the diagnosis of Alzheimer's disease: a systematic review and meta-analysis. Lancet Neurol. (2016) 15:673–84. doi: 10.1016/S1474-4422(16)00070-3
32. Irwin DJ, Fedler J, Coffey CS, Caspell-Garcia C, Kang JH, Simuni T, et al. Evolution of Alzheimer's Disease Cerebrospinal Fluid Biomarkers in Early Parkinson's Disease. Ann Neurol. (2020) 88:574–87. doi: 10.1002/ana.25811
33. Lemstra AW, de Beer MH, Teunissen CE, Schreuder C, Scheltens P, van der Flier WM, et al. M. Concomitant AD pathology affects clinical manifestation and survival in dementia with Lewy bodies. J Neurol Neurosurg Psychiatry. (2017) 88:113–8. doi: 10.1136/jnnp-2016-313775
34. van de Beek M, Babapour Mofrad R, van Steenoven I, Vanderstichele H, Scheltens P, Teunissen CE, et al. Sex-specific associations with cerebrospinal fluid biomarkers in dementia with Lewy bodies. Alzheimers Res Ther. (2020) 12:44. doi: 10.1186/s13195-020-00610-9
35. Abdelnour C, van Steenoven I, Londos E, Blanc F, Auestad B, Kramberger MG, et al. Alzheimer's disease cerebrospinal fluid biomarkers predict cognitive decline in lewy body dementia. Mov Disord. (2016) 31:1203–8. doi: 10.1002/mds.26668
36. Howard E, Irwin DJ, Rascovsky K, Nevler N, Shellikeri S, Tropea TF, et al. Cognitive Profile and Markers of Alzheimer Disease-Type Pathology in Patients With Lewy Body Dementias. Neurology. (2021) 96:e1855–64. doi: 10.1212/WNL.0000000000011699
37. Spotorno N, Coughlin DG, Olm CA, Wolk D, Vaishnavi SN, Shaw LM, et al. Tau pathology associates with in vivo cortical thinning in Lewy body disorders. Ann Clin Transl Neurol. (2020) 7:2342–55. doi: 10.1002/acn3.51183
38. Llibre-Guerra JJ Li Y, Schindler SE, Gordon BA, Fagan AM, Morris JC, Benzinger TLS, et al. Association of Longitudinal Changes in Cerebrospinal Fluid Total Tau and Phosphorylated Tau 181 and Brain Atrophy With Disease Progression in Patients With Alzheimer Disease. JAMA Netw Open. (2019) 2:e1917126. doi: 10.1001/jamanetworkopen.2019.17126
39. Toledo JB, Xie SX, Trojanowski JQ, Shaw LM. Longitudinal change in CSF Tau and Aβ biomarkers for up to 48 months in ADNI. Acta Neuropathol. (2013) 126. doi: 10.1007/s00401-013-1151-4
40. Buchhave P, Minthon L, Zetterberg H, Wallin AK, Blennow K, Hansson O. Cerebrospinal fluid levels of β-amyloid 1-42, but not of tau, are fully changed already 5 to 10 years before the onset of Alzheimer dementia. Arch Gen Psychiatry. (2012) 69:98–106. doi: 10.1001/archgenpsychiatry.2011.155
41. Sutphen CL, Jasielec MS, Shah AR, Macy EM, Xiong C, Vlassenko AG, et al. Longitudinal Cerebrospinal Fluid Biomarker Changes in Preclinical Alzheimer Disease During Middle Age. JAMA Neurol. (2015) 72:1029–42. doi: 10.1001/jamaneurol.2015.1285
42. Villain N, Chételat G, Grassiot B, Bourgeat P, Jones G, Ellis KA, et al. Regional dynamics of amyloid-β deposition in healthy elderly, mild cognitive impairment and Alzheimer's disease: a voxelwise PiB-PET longitudinal study. Brain. (2012) 135:2126–39. doi: 10.1093/brain/aws125
43. Lewczuk P, Riederer P, O'Bryant SE, Verbeek MM, Dubois B, Visser PJ, et al. Cerebrospinal fluid and blood biomarkers for neurodegenerative dementias: An update of the Consensus of the Task Force on Biological Markers in Psychiatry of the World Federation of Societies of Biological Psychiatry. World J Biol Psychiatry. (2018) 19:244–328. doi: 10.1080/15622975.2017.1375556
44. Lleó A, Cavedo E, Parnetti L, Vanderstichele H, Herukka SK, Andreasen N, et al. Cerebrospinal fluid biomarkers in trials for Alzheimer and Parkinson diseases. Nat Rev Neurol. (2015) 11:41–55. doi: 10.1038/nrneurol.2014.232
45. Bridel C, van Wieringen WN, Zetterberg H, Tijms BM, Teunissen CE, the NFL Group, Alvarez-Cermeño JC, et al. Diagnostic value of cerebrospinal fluid neurofilament light protein in neurology: a systematic review and meta-analysis. JAMA Neurol. (2019) 76:1035–48. doi: 10.1001/jamaneurol.2019.1534
46. Delaby C, Alcolea D, Carmona-Iragui M, Illán-Gala I, Morenas-Rodríguez E, Barroeta I, et al. Differential levels of Neurofilament Light protein in cerebrospinal fluid in patients with a wide range of neurodegenerative disorders. Sci Rep. (2020) 10. doi: 10.1038/s41598-020-66090-x
47. Hu X, Yang Y, Gong D. Cerebrospinal fluid levels of neurofilament light chain in multiple system atrophy relative to Parkinson's disease: a meta-analysis. Neurol Sci. (2017) 38:407–14. doi: 10.1007/s10072-016-2783-7
48. Lleó A, Alcolea D, Martínez-Lage P, Scheltens P, Parnetti L, Poirier J, et al. Longitudinal cerebrospinal fluid biomarker trajectories along the Alzheimer's disease continuum in the BIOMARKAPD study. Alzheimer's Dementia. (2019) 15:742–53. doi: 10.1016/j.jalz.2019.01.015
49. Zetterberg H, Skillbäck T, Mattsson N, Trojanowski JQ, Portelius E, Shaw LM, et al. Alzheimer's disease neuroimaging initiative. Association of cerebrospinal fluid neurofilament light concentration with alzheimer disease progression. JAMA Neurol. (2016) 73:60–7. doi: 10.1001/jamaneurol.2015.3037
50. Lin C-H, Yang S-Y, Horng H-E, Yang C-C, Chieh J-J, Chen H-H, et al. Plasma biomarkers differentiate Parkinson's Disease from atypical parkinsonism syndromes. Front Aging Neurosci. (2018) 10. doi: 10.3389/fnagi.2018.00123
51. Hall S, Janelidze S, Londos E, Leuzy A, Stomrud E, Dage JL, et al. Plasma Phospho-Tau Identifies Alzheimer's Co-Pathology in Patients with Lewy Body Disease. Movement Disorders. (2021) 36:767–71. doi: 10.1002/mds.28370
52. Thijssen EH, Rabinovici GD. Rapid Progress Toward Reliable Blood Tests for Alzheimer Disease. JAMA Neurol. (2021) 78:143–5. doi: 10.1001/jamaneurol.2020.4200
53. Mattsson-Carlgren N, Janelidze S, Palmqvist S, Cullen N, Svenningsson AL, Strandberg O, et al. Longitudinal plasma p-tau217 is increased in early stages of Alzheimer's disease. Brain. (2020) 143:3234–41. doi: 10.1093/brain/awaa286
54. Moscoso A, Grothe MJ, Ashton NJ, Karikari TK, Lantero Rodríguez J, Snellman A, et al. Longitudinal Associations of Blood Phosphorylated Tau181 and Neurofilament Light Chain With Neurodegeneration in Alzheimer Disease. JAMA Neurol. (2021) 78:396–406. doi: 10.1001/jamaneurol.2020.4986
55. de Wolf F, Ghanbari M, Licher S, McRae-McKee K, Gras L, Weverling GJ, et al. Plasma tau, neurofilament light chain and amyloid-β levels and risk of dementia; a population-based cohort study. Brain. (2020) 143:1220–32. doi: 10.1093/brain/awaa054
56. Pilotto A, Imarisio A, Carrarini C, Russo M, Masciocchi S, Gipponi S, et al. Plasma Neurofilament Light Chain predicts cognitive progression in prodromal and clinical dementia with Lewy Bodies. medRxiv. (2021) 2021.03.19.21253993. doi: 10.1101/2021.03.19.21253993
57. McKeith IG, Boeve BF, Dickson DW, Halliday G, Taylor J-P, Weintraub D, et al. Diagnosis and management of dementia with Lewy bodies: Fourth consensus report of the DLB Consortium. Neurology. (2017) 89:88–100. doi: 10.1212/WNL.0000000000004058
58. Ferman TJ, Aoki N, Boeve BF, Aakre JA, Kantarci K, Graff-Radford J, et al. Subtypes of dementia with Lewy bodies are associated with α-synuclein and tau distribution. Neurology. (2020) 95:e155–65. doi: 10.1212/WNL.0000000000009763
59. van der Zande JJ, Joling M, Happach IG, Vriend C. Scheltens Ph, Booij J, Lemstra AW. Serotonergic deficits in dementia with Lewy bodies with concomitant Alzheimer's disease pathology: An 123I-FP-CIT SPECT study. NeuroImage: Clin. (2020) 25:102062. doi: 10.1016/j.nicl.2019.102062
60. van der Zande JJ, Gouw AA, van Steenoven I, Scheltens P, Stam CJ, Lemstra AW, et al. Characteristics of Dementia With Lewy Bodies, Alzheimer's Disease and Mixed Pathology. Front Aging Neurosci. (2018) 10:190. doi: 10.3389/fnagi.2018.00190
61. Graff-Radford J, Boeve BF, Pedraza O, Ferman TJ, Przybelski S, Lesnick TG, et al. Imaging and acetylcholinesterase inhibitor response in dementia with Lewy bodies. Brain. (2012) 135:2470–7. doi: 10.1093/brain/aws173
62. Schindler SE, Bollinger JG, Ovod V, Mawuenyega KG Li Y, Gordon BA, Holtzman DM, et al. High-precision plasma β-amyloid 42/40 predicts current and future brain amyloidosis. Neurology. (2019) 93:e1647–59. doi: 10.1212/WNL.0000000000008081
63. Nakamura A, Kaneko N, Villemagne VL, Kato T, Doecke J, Doré V, et al. High performance plasma amyloid-β biomarkers for Alzheimer's disease. Nature. (2018) 554:249–54. doi: 10.1038/nature25456
64. Palmqvist S, Janelidze S, Stomrud E, Zetterberg H, Karl J, Zink K, et al. Performance of Fully Automated Plasma Assays as Screening Tests for Alzheimer Disease-Related β-Amyloid Status. JAMA Neurol. (2019) 76:1060–9. doi: 10.1001/jamaneurol.2019.1632
65. Mattsson-Carlgren N, Janelidze S, Bateman RJ, Smith R, Stomrud E, Serrano GE, et al. Soluble P-tau217 reflects amyloid and tau pathology and mediates the association of amyloid with tau. EMBO Mol Med. (2021) e14022. doi: 10.21203/rs.3.rs-101153/v2
66. Barthélemy NR, Bateman RJ, Hirtz C, Marin P, Becher F, Sato C, et al. Cerebrospinal fluid phospho-tau T217 outperforms T181 as a biomarker for the differential diagnosis of Alzheimer's disease and PET amyloid-positive patient identification. Alz Res Therapy. (2020) 12:1–11. doi: 10.1186/s13195-020-00596-4
67. Ashton NJ, Hye A, Rajkumar AP, Leuzy A, Snowden S, Suárez-Calvet M, et al. An update on blood-based biomarkers for non-Alzheimer neurodegenerative disorders. Nat Rev Neurol. (2020) 16:265–84. doi: 10.1038/s41582-020-0348-0
68. Libiger O, Shaw LM, Watson MH, Nairn AC, Umaña KL, Biarnes MC, et al. Longitudinal CSF proteomics identifies NPTX2 as a prognostic biomarker of Alzheimer's disease. Alzheimers Dement. (2021) doi: 10.1002/alz.12353
69. van Steenoven I, Noli B, Cocco C, Ferri G-L, Oeckl P, Otto M, et al. VGF Peptides in Cerebrospinal Fluid of Patients with Dementia with Lewy Bodies. Int J Mol Sci. (2019) 20. doi: 10.3390/ijms20194674
70. Petrera A, von Toerne C, Behler J, Huth C, Thorand B, Hilgendorff A, et al. Multiplatform Approach for Plasma Proteomics: Complementarity of Olink Proximity Extension Assay Technology to Mass Spectrometry-Based Protein Profiling. J Proteome Res. (2021) 20:751–62. doi: 10.1021/acs.jproteome.0c00641
71. Arotcarena M-L, Teil M, Dehay B. Autophagy in Synucleinopathy: the overwhelmed and defective machinery. Cells. (2019) 8. doi: 10.3390/cells8060565
72. Small SA, Petsko GA. Retromer in Alzheimer disease, Parkinson disease and other neurological disorders. Nat Rev Neurosci. (2015) 16:126–32. doi: 10.1038/nrn3896
73. van Steenoven I, Koel-Simmelink MJA, Vergouw LJM, Tijms BM, Piersma SR, Pham TV, et al. Identification of novel cerebrospinal fluid biomarker candidates for dementia with Lewy bodies: a proteomic approach. Mol Neurodegener. (2020) 15:36. doi: 10.1186/s13024-020-00388-2
74. Guo JL, Covell DJ, Daniels JP, Iba M, Stieber A, Zhang B, et al. Distinct α-synuclein strains differentially promote tau inclusions in neurons. Cell. (2013) 154:103–17. doi: 10.1016/j.cell.2013.05.057
75. Kim S, Kwon S-H, Kam T-I, Panicker N, Karuppagounder SS, Lee S, Lee JH, Kim WR, Kook M, Foss CA, et al. Transneuronal propagation of pathologic α-synuclein from the gut to the brain models Parkinson's disease. Neuron. (2019) 103:627–41.e7. doi: 10.1016/j.neuron.2019.05.035
76. Braak H, Del Tredici K, Rüb U, de Vos RAI, Jansen Steur ENH, Braak E. Staging of brain pathology related to sporadic Parkinson's disease. Neurobiol Aging. (2003) 24:197–211. doi: 10.1016/S0197-4580(02)00065-9
77. Doppler K, Antelmi E, Kuzkina A, Donadio V, Incensi A, Plazzi G, et al. Consistent skin α-synuclein positivity in REM sleep behavior disorder - A two center two-to-four-year follow-up study. Parkinsonism Relat Disord. (2021) 86:108–13. doi: 10.1016/j.parkreldis.2021.04.007
78. Antelmi E, Pizza F, Donadio V, Filardi M, Sosero YL, Incensi A, et al. Biomarkers for REM sleep behavior disorder in idiopathic and narcoleptic patients. Ann Clin Transl Neurol. (2019) 6:1872–6. doi: 10.1002/acn3.50833
79. Al-Qassabi A, Tsao T-S, Racolta A, Kremer T, Cañamero M, Belousov A, et al. Immunohistochemical detection of synuclein pathology in skin in idiopathic rapid eye movement sleep behavior disorder and Parkinsonism. Mov Disord. (2020) doi: 10.1002/mds.28399
80. Beach TG, Adler CH, Sue LI, Shill HA, Driver-Dunckley E, Mehta SH, et al. Vagus nerve and stomach Synucleinopathy in Parkinson's disease, incidental lewy body disease, and normal elderly subjects: evidence against the “body-first” hypothesis. J Parkinsons Dis. (2021) doi: 10.1101/2020.09.29.20204248
81. Lionnet A, Leclair-Visonneau L, Neunlist M, Murayama S, Takao M, Adler CH, et al. Does Parkinson's disease start in the gut? Acta Neuropathol. (2018) 135:1–12. doi: 10.1007/s00401-017-1777-8
82. Beach TG, Adler CH, Lue L, Sue LI, Bachalakuri J, Henry-Watson J, et al. Unified staging system for Lewy body disorders: correlation with nigrostriatal degeneration, cognitive impairment and motor dysfunction. Acta Neuropathol. (2009) 117:613–34. doi: 10.1007/s00401-009-0538-8
83. Coughlin D, Xie SX, Liang M, Williams A, Peterson C, Weintraub D, et al. Cognitive and Pathological Influences of Tau Pathology in Lewy Body Disorders. Ann Neurol. (2019) 85:259–71. doi: 10.1002/ana.25392
Keywords: cerebrospinal fluid, alpha-synuclein, skin biopsy, seeded aggregation assays, tau, amyloid, Lewy body dementia, LBDA biomarker symposium
Citation: Scott GD, Arnold MR, Beach TG, Gibbons CH, Kanthasamy AG, Lebovitz RM, Lemstra AW, Shaw LM, Teunissen CE, Zetterberg H, Taylor AS, Graham TC, Boeve BF, Gomperts SN, Graff-Radford NR, Moussa C, Poston KL, Rosenthal LS, Sabbagh MN, Walsh RR, Weber MT, Armstrong MJ, Bang JA, Bozoki AC, Domoto-Reilly K, Duda JE, Fleisher JE, Galasko DR, Galvin JE, Goldman JG, Holden SK, Honig LS, Huddleston DE, Leverenz JB, Litvan I, Manning CA, Marder KS, Pantelyat AY, Pelak VS, Scharre DW, Sha SJ, Shill HA, Mari Z, Quinn JF and Irwin DJ (2022) Fluid and Tissue Biomarkers of Lewy Body Dementia: Report of an LBDA Symposium. Front. Neurol. 12:805135. doi: 10.3389/fneur.2021.805135
Received: 29 October 2021; Accepted: 27 December 2021;
Published: 31 January 2022.
Edited by:
Paolo Paganetti, Ente Ospedaliero Cantonale (EOC), SwitzerlandReviewed by:
Tamara Shiner, Tel Aviv Sourasky Medical Center, IsraelCopyright © 2022 Scott, Arnold, Beach, Gibbons, Kanthasamy, Lebovitz, Lemstra, Shaw, Teunissen, Zetterberg, Taylor, Graham, Boeve, Gomperts, Graff-Radford, Moussa, Poston, Rosenthal, Sabbagh, Walsh, Weber, Armstrong, Bang, Bozoki, Domoto-Reilly, Duda, Fleisher, Galasko, Galvin, Goldman, Holden, Honig, Huddleston, Leverenz, Litvan, Manning, Marder, Pantelyat, Pelak, Scharre, Sha, Shill, Mari, Quinn and Irwin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gregory D. Scott, c2NvdHRncmVAb2hzdS5lZHU=
†These authors have contributed equally to this work and share last authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.