 Rodrigo Rocamora1,2,3*†
Rodrigo Rocamora1,2,3*† Beatriz Chavarría1
Beatriz Chavarría1 Eva Pérez1Carmen Pérez-Enríquez1,2Ainara Barguilla1Luisa Panadés-de Oliveira1
Eva Pérez1Carmen Pérez-Enríquez1,2Ainara Barguilla1Luisa Panadés-de Oliveira1 Alessandro Principe1,2,3
Alessandro Principe1,2,3 Riccardo Zucca1,2,3
Riccardo Zucca1,2,3- 1Epilepsy Monitoring Unit, Department of Neurology, Hospital del Mar, Barcelona, Spain
- 2Hospital del Mar Medical Research Institute, Barcelona, Spain
- 3Faculty of Health and Life Sciences, Universitat Pompeu Fabra, Barcelona, Spain
Introduction: The overall combined prevalence of anxiety and depression in patients with epilepsy has been estimated at 20.2 and 22.9%, respectively, and is considered more severe in drug-refractory epilepsy. Patients admitted to epilepsy monitoring units constitute a particular group. Also, patients with psychogenic non-epileptic seizures can reach more than 20% of all admissions. This study aims to characterize these symptoms in a large cohort of patients admitted for evaluation in a tertiary epilepsy center.
Materials and Methods: The study was conducted among 493 consecutive patients (age: 38.78 ± 12.7, 57% females) admitted for long-term video EEG from January 2013 to February 2021. Demographic, clinical, and mood disorder patients' data were collected. Anxiety and depression symptoms were assessed through the Hospital Anxiety Depression Scale (HADS-A and HADS-D), the State Trait Anxiety Inventory (STAI), and Beck Depression Inventory (BDI-II). Quality of life was determined using the QOLIE-10. Patients were divided into three groups: patients with epilepsy (n = 395), psychogenic non-epileptic seizures (PNES) (n = 56), and combined (n = 33). A univariate and multivariate regression analysis was performed for variables associated with quality of life.
Results: Of 493 patients, 45.0% had structural etiology, and considering epilepsy classification, 43.6% were of temporal lobe origin. In addition, 32.45% of patients had a previous psychiatric history, 49.9% of patients had depressive symptoms in BDI, and 30.9% according to HADS-D; 56.42 and 52.63% of patients presented pathological anxiety scores in STAI-T and STAI-S, respectively; and 44.78% according to HADS-A. PNES and combined groups revealed a higher incidence of pathologic BDI scores (64.29 and 78.79%, p < 0.001) as well as pathologic HADS-A scores (p = 0.001). Anxiety and depression pathologic results are more prevalent in females, HADS-A (females = 50.7%, males = 36.8%; p = 0.0027) and BDI > 13 (females = 56.6%, males = 41.0%; p = 0.0006). QOLIE-10 showed that 71% of the patients had their quality of life affected with significantly higher scores in the combined group than in the epilepsy and PNES groups (p = 0.0015).
Conclusions: Subjective anxiety, depression, and reduced quality of life are highly prevalent in patients with refractory epilepsy. These symptoms are more evident when PNES are associated with epilepsy and more severe among female patients. Most of the cases were not previously diagnosed. These factors should be considered in everyday clinical practice, and specific approaches might be adapted depending on the patient's profile.
Introduction
Anxiety and depression are frequent among patients with epilepsy (PWE) and constitute one of the most important comorbidities (1). Moreover, psychiatric disorders represent one of the principal modulating factors of the quality of life in PWE acting independently even of the seizure control itself (2). There is an agreement that principally depression but also anxiety are the main psychiatric comorbidities although the prevalence appears to be highly variable depending on the populations studied. However, the relevance of psychiatric comorbidities and the impact on quality of life in PWE has been consistent in different cultural contexts (3–5).
Contrary to the general concept of a higher prevalence of depression in PWE, recently it has been postulated that anxiety may be even more prevalent than depressive symptoms (6). Current analysis based on population studies in PWE described an overall prevalence of 23.1% for depression, and anxiety disorders ranged from 4.4 to 52.1% (7–9). On the other hand, when the studies carried out in patients with refractory epilepsy are analyzed, depression varies between 4.5 and 30%, and anxiety disorders are between 5 and 28% (10–13). A recent meta-analysis reports that the global pooled prevalence of anxiety disorders in PWE was 20.2%, and the overall pooled prevalence of depressive disorders was 22.9% (14).
Patients admitted for long-term video-EEG monitoring (LT-VEEGM) probably represent a different group. Drug-refractory epilepsy patients principally comprise them and less frequently differential diagnostic cases. Still, a significant percentage of patients admitted to an epilepsy monitoring unit (EMU) suffer from psychogenic non-epileptic seizures (PNES), and a non-negligible group presents an association of both pathologies. Diverse studies report that between 20 and 40% of patients admitted to an EMU suffer from PNES (15). In turn, ca. 9–11% of patients with PNES also present with epileptic seizures (16, 17).
Health personnel responsible for this group of patients are confronted not uniquely with epilepsies that are difficult to manage and also with a group of patients with psychiatric comorbidities probably differing from those reported in general population studies, which also determine their quality of life beyond epilepsy. In addition, the identification of psychiatric comorbidities is essential for defining multidimensional therapeutic strategies, preventing serious psychiatric complications and prognostic factors when making surgical decisions (6).
The objective of this study was to analyze the prevalence of anxiety and depression symptoms and to establish the impact on quality of life in a large sample of consecutive patients admitted for LT-VEEGM in our EMU.
Materials and Methods
Participants
The inclusion criteria for this study were admission to the EMU due to refractory epilepsy or differential diagnosis, aged 16 years or older, and having completed the evaluation tests. Exclusion criteria included intellectual disability (estimated IQ lower than 70), unwillingness to participate in the study, or insufficient proficiency in the Spanish language.
From January 2013 to February 2021, 836 patients were evaluated in the EMU of Hospital del Mar (Barcelona, Spain), a national reference center for refractory epilepsy and member of the European Reference Network EPI-Care. Finally, 493 consecutive (mean age: 38.78 ± 12.7 years, 57% females) patients were included in the study.
Clinical and Sociodemographic Variables
Clinical data included medical records, seizure type, age at onset, seizure duration, current antiseizure medication (ASM) history, etiology, epilepsy localization, and history of psychiatric illnesses obtained from electronic clinical files and referenced by the patient. Sociodemographic data included age, gender, marital status, occupation, and educational level. Patients were subsequently classified into three groups: PWE (n = 395), PNES (n = 56), and combined (PWE + PNES, n = 33), and nine patients were not diagnosed and excluded from the analysis. These patient groups represent the totality of patients admitted to our EMU, which allows comprehensive research and may be helpful for comparison purposes.
Epilepsy Variables
The group of PWE was analyzed to assess differences in the prevalence of psychiatric symptoms between focal vs. generalized epilepsies. Within focal epilepsies, prevalence in the temporal lobe vs. extratemporal epilepsy group was compared. The combined group was discarded from the analysis to avoid confounders.
Psychiatric Assessment
The psychiatric evaluation was carried out using validated tests designed to measure levels of depression and anxiety. At the same time, the quality of life of the patients was assessed to evaluate the impact of the above symptoms on this important measure of well-being. Anxiety and depression symptoms were assessed through the Hospital Anxiety and Depression Scale (HADS), the State Trait Anxiety Inventory (STAI), and Beck Depression Inventory II (BDI-II) (18–21). Quality of life was determined using the Quality of Life in Epilepsy-10 (QOLIE-10), validated for the Spanish population (22, 23).
The PNES diagnosis was obtained after a consensual decision between epileptologists and psychiatrists. In our EMU, PNES are first detected by the epilepsy team as they occur during VEEGM. Immediately afterward, a referral psychiatrist with experience in epilepsy evaluates the behavioral aspects of the semiology and visits the patient during admission, establishing a specific treatment plan.
The HADS is a 14-item questionnaire designed to detect states of anxiety and depression symptoms in hospitalized patients. The HADS produces two scales, one for anxiety (HADS-A) and one for depression (HADS-D), and scores ≥8 on either scale indicate a pathologic case. The STAI is a 40-item, self-report scale assessing separate dimensions of “state” and “trait” anxiety. Items are rated on a 4-point Likert scale with higher scores indicating greater levels of anxiety. The BDI-II is a 21-item measure estimating the frequency and severity of depressive symptoms. Each item consists of four self-evaluative statements scored 0 to 3 with increasing scores indicating greater depression severity. The QOLIE-10 is a 10-item, self-report measure covering general and epilepsy-specific domains (medication effects, mental health, role functioning, and seizure worry) and scored on a 10 (normal) to 50 (very high) scale. BDI-II is the most widely used scale for detecting depression. Together with the HADS, it constitutes two of the three instruments approved by the National Institute for Health and Clinical Excellence to measure the severity of initial depression and response to treatment. Cutting scores for the different scales are reported in Table 1.

Table 1. Cutoff points of the inventory scales.
Ethics Committee
The protocol, informed consent, and any related relevant documents were examined and approved by the Clinical Research Ethics Committee (CEIC-Parc de Salut Mar). All patients signed an informed consent for the use of their data in this protocol. The study met the international and national good clinical practice as required by the principles of the Declaration of Helsinki of 2008 of the World Medical Association and the current legislation on protection of personal data (Organic Law 3/2018, of December 5, on the Protection of Personal Data and the Guarantee of Digital Rights).
Data Analysis
The omnibus normality test (scipy.stats.normaltest) was carried out to examine the normality of the data. Chi-square and Fisher's exact statistics were used to compare proportions. Depending on the normality of data, t-test, Mann–Whitney, or Kruskal–Wallis tests for continuous variables were conducted to compare scores among the diagnostic groups. Multiple comparisons were corrected with Bonferroni adjustments. To determine the relationship between demographic, clinical, and mood factors and quality of life, a stepwise regression analysis on QOLIE-10 scores was conducted. The criteria for factor inclusion and exclusion were set at p = 0.01 and p = 0.05, respectively, and a list-wise deletion was used in the multivariate analysis. Statistical analyses were performed using SPSS21 (Armonk, NY, USA) and the scientific python library (scipy) with the level of significance set at p < 0.05 (two-sided) unless otherwise stated.
Results
Of the population of 493 patients (57% female), 395 (80.12%) had epilepsy, 56 (11.36%) presented with PNES, and 33 (6.69%) had concurrent epilepsy and PNES (Tables 2, 3). Nine patients (1.83%) were not diagnosed and were not included in the group's comparison analyses. Of the total group with epilepsy (428 patients), 7.7% has PNES. Likewise, of the total group with PNES (89 patients), 37% has epilepsy.
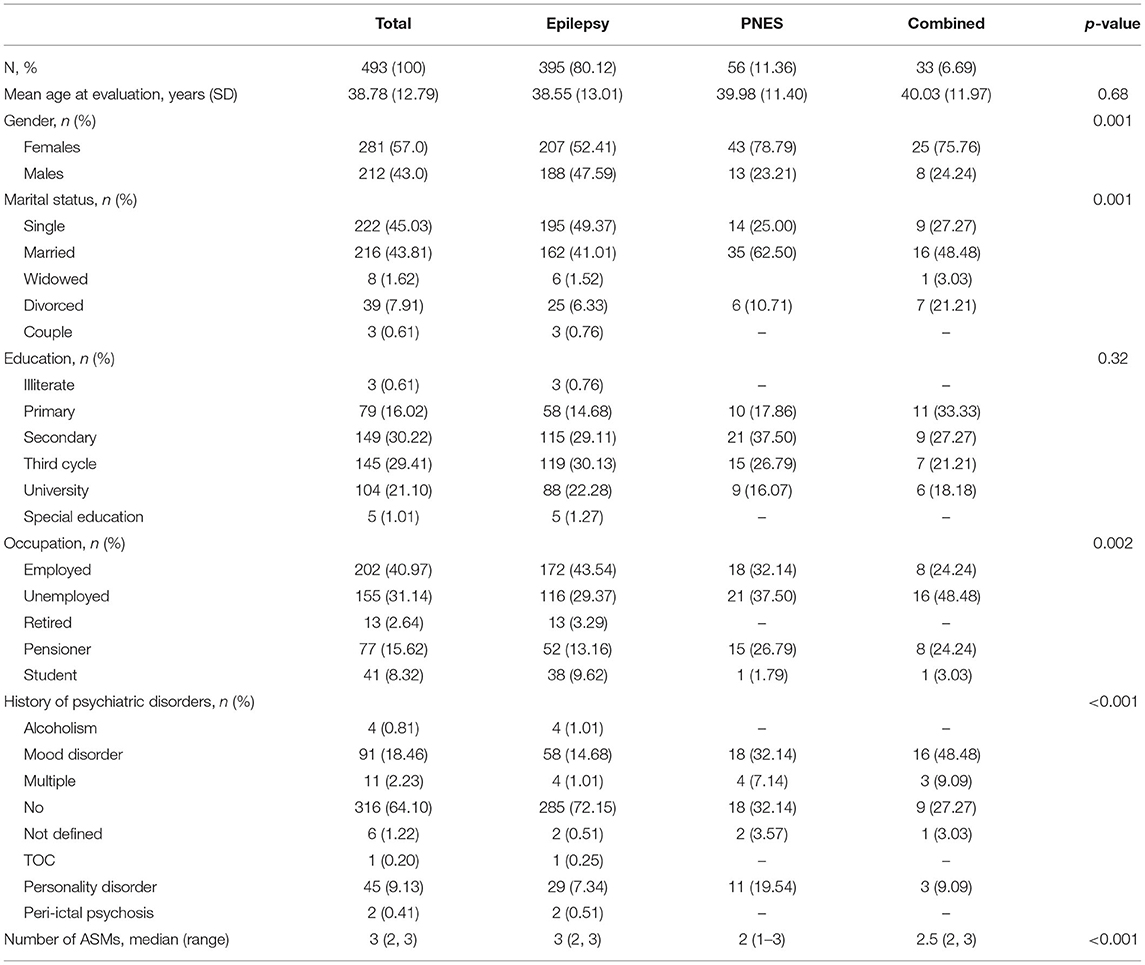
Table 2. Clinical and sociodemographic characteristics of the patients included in the analysis (N = 493).
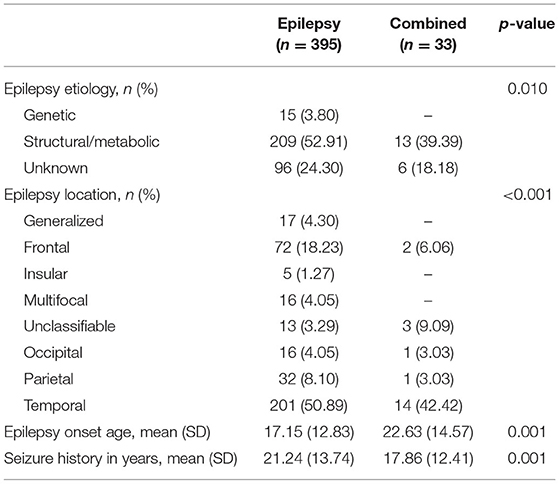
Table 3. Clinical characteristics of the patients.
Diagnostic groups were balanced for age (KW, p = 0.68) and education (chi2, p = 0.32), but not so regarding gender (chi2, p < 0.001 with females more prevalent in the PNES and the combined groups), epilepsy onset (KW, p = 0.001), epilepsy duration (KW, p = 0.001), marital status (chi2, p = 0.001), and employment (chi2, p =0.002). Patients' mean age at evaluation was 38.78 years (SD 12.79, 95% CI [37.65–39.91]), the mean age of epilepsy onset was 18.20 years (SD 13.52, 95% CI [16.98–19.43]), and the average duration of epilepsy was 20.43 years (SD 13.95, 95% CI [19.16–21.69]). Epilepsy duration was calculated as the interval (in years) from age at seizure onset to age at evaluation. A structural etiology was observed in 222 (45.0%) cases, and considering epilepsy classification, 215 (43.6%) were of temporal origin. In addition, 279 (61.18%) patients were on treatment with one or more ASMs with a median number of three [2–3] drugs. LEV was the most frequent ASM, being prescribed to 217 (44.0%) patients. Psychiatry disorders were previously diagnosed in 160 patients (32.45%) with mood disorders being the most prevalent (91 cases, 18.46%).
Prevalence of Anxiety and Depression in the Total Population
A series of D'Agostino K2 tests revealed a non-normal distribution for QOLIE-10 (K2 = 15.962, p < 0.001), BDI-II (K2 = 45.720, p < 0.001), HADS-D (K2 = 26.718, p < 0.001), HADS-A (K2 = 21.766, p < 0.001), STAI-S (K2 = 16.324, p < 0.001), STAI-T (K2 = 29.839, p < 0.001).
Depressive symptoms in the BDI-II (14 or above) were observed in 246/493 (49.90%) of the patients and 144/467 (30.84%) according to HADS-D (8 or above). The mean scores were 15.69 (SD 11.53) for BDI-II and 5.53 (SD 4.06) for the HADS-D scale (Tables 4, 5). Females had significantly higher BDI-II scores (females: 17.49, SD = 12.13; males: 13.31, SD = 10.24, p = 0.0002), whereas the difference was not significant for the HADS-D scores (females: 5.80, SD = 4.36; males: 5.19, SD = 3.59, p = 0.28) (Figure 1).
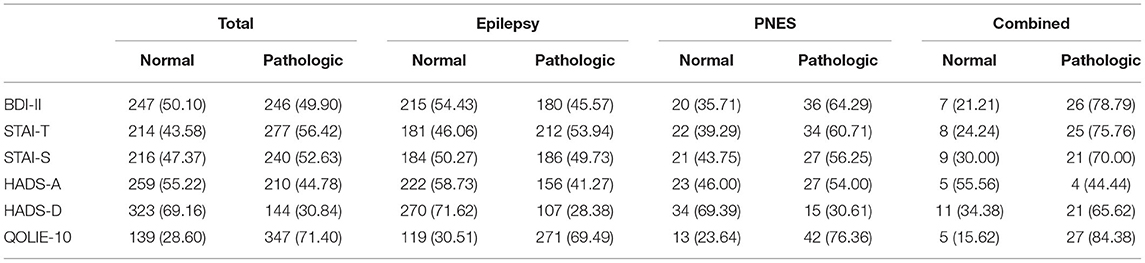
Table 4. Prevalence or frequency of depression, anxiety, and quality of life per diagnostic groups.
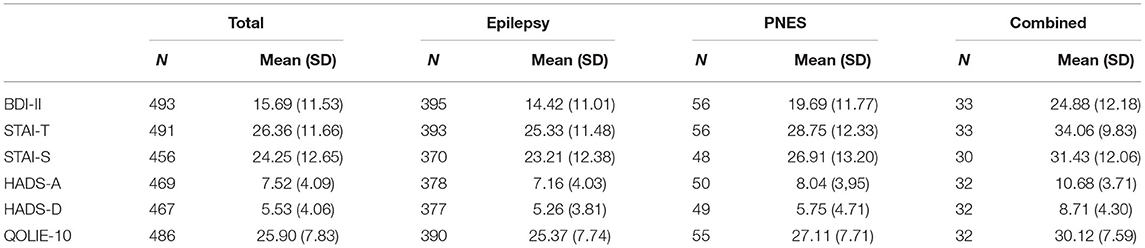
Table 5. Average scores on anxiety, depression, and quality of life inventories per diagnostic groups.
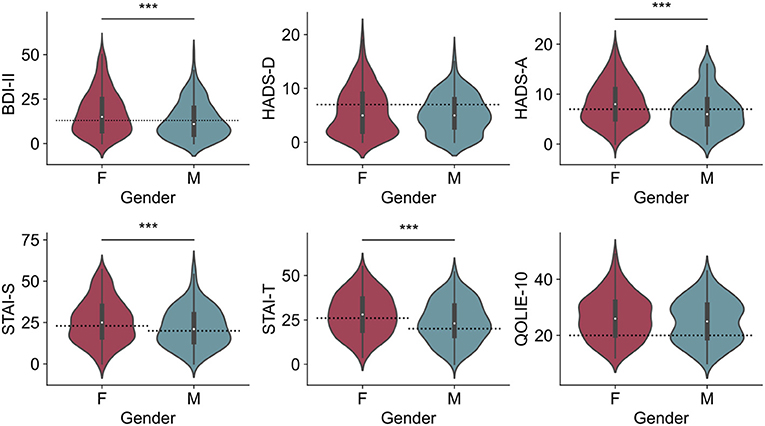
Figure 1. Median of scores on the inventory scales according to gender. BDI, HADS-A, STAI-S, and STAI-T scores were significantly higher in female patients. ***p < 0.01.
Pathologic anxiety scores in the STAI-S and the HADS-A were present in 240/456 (52.63%) and 210/469 (44.78%) patients, respectively. The mean STAI-S score was 24.25 (SD 12.65), whereas the mean HADS-A score was 7.52 (SD 4.09). Females had significantly higher anxiety scores in both the STAI-S (females: 25.86, SD = 13.11; males: 22.16, SD = 11.71, p = 0.003), and in the HADS-A inventory (females: 8.16, SD = 4.15; males: 6.66, SD = 3.87, p < 0.001) (Figure 1).
Differences in the Prevalence of Anxiety and Depression Scores per Diagnostic Group
In our series, 360 patients had focal epilepsy (73.0%), and 17 were generalized (3.44%). Within the group of focal epilepsies, 215 (59.7%) were categorized as temporal lobe epilepsy (TLE), and 128 (35.5%) were grouped within the extratemporal group (Table 3). Across TLE and extratemporal epilepsies, no difference in the prevalence of pathologic scores was found for all the scales employed (all p > 0.05).
The PNES and combined groups revealed a higher incidence of pathologic BDI-II scores (64.29 and 78.79%, p < 0.001) as well as pathologic HADS-A scores (p = 0.001). The combined group showed a higher incidence of pathologic HADS-D scores (65.62%, p < 0.001). Pathologic anxiety and depression results were more prevalent in females, HADS-A (females = 50.7%; males = 36.8%; p = 0.0027) and BDI-II>13 (females = 56.6%; males = 41.0%; p = 0.0006) (Figure 2), but no gender differences could be observed for the HADS-D and STAI scales. A significant difference in the number of ASMs was observed for the PNES group, which, on average, was on less medication (p < 0.001).
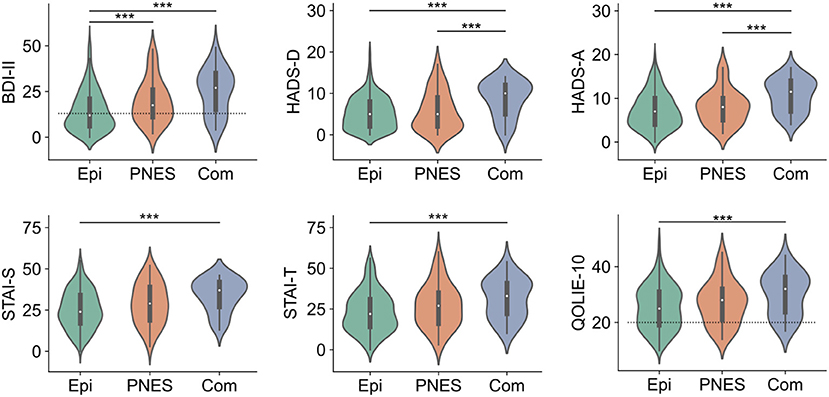
Figure 2. Inventory scores according to the diagnostic group. Epi, epilepsy group; PNES, psychogenic non-epileptic seizure group; Com, combined group. ***p < 0.01.
Quality of Life (QOLIE-10)
According to the QOLIE-10 scores (21 or above), 347/486 patients (71.40%) had their quality of life affected. The mean QOLIE-10 score was 25.90 (SD 7.83) with females showing a slightly higher incidence of pathologic QOLIE-10 scores (females = 74.73%, males = 66.99%, p = 0.06) (Figure 1). No significant difference in the prevalence of pathologic scores was found across diagnostic groups (p = 0.13) (Figure 2).
Significant bivariate relations were observed between QOLIE-10 scores and the measures of depression, including the BDI-II and the HADS-D scale (R2 = 0.399 and R2 = 0.374, respectively, both p < 0.001). Increased endorsement of mood symptoms is associated with lower quality of life (Figure 3). A significant bivariate association was also observed between QOLIE-10 scores and measures of anxiety, including the HADS-A and the STAI-S inventories (R2 = 0.302 and R2 = 0.228, respectively, both p < 0.001). Increasing anxiety is similarly associated with a reduction in quality of life (Figure 3).
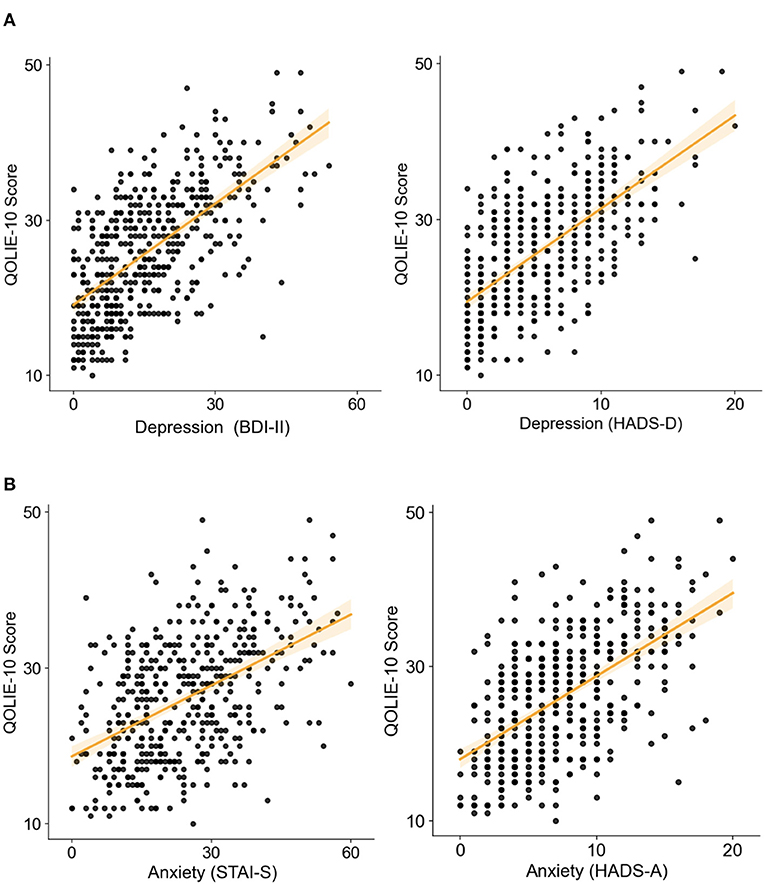
Figure 3. Inferior health-related quality of life is significantly associated with increased symptoms of depression and anxiety (higher score means lower perceived quality of life). Correlation between Quality of Life in Epilepsy Inventory-10 (QOLIE-10) overall score and scores of (A left) Beck Depression Inventory-II (BDI-II), (A right) Hospital-Anxiety and Depression-Scale (HADS) depression subscale, (B left) State-Trait-Anxiety-Inventory (STAI), and (B right) HADS anxiety subscale (all with p < 0.001).
Depression and anxiety affect QoL independently. The partial correlations between QOLIE-10 and the two depression inventories remain significant after controlling for the two anxiety scales (BDI-II controlled for HADS-A, R2 = 0.163; BDI-II controlled for STAI-S, R2 = 0.223; HADS-D controlled for HADS-A, R2 = 0.396; HADS-D controlled for STAI-S, R2 = 0.199. All p < 0.001). Similarly, the partial correlations between the anxiety scores and the QOLIE-10 remain significant after controlling for the depression factor (HADS-A controlled for BDI-II, R2 = 0.054; HADS-A controlled for HADS-D, R2 = 0.077; STAI-S controlled for BDI-II, R2 = 0.043; STAI-S controlled for HADS-D, R2 = 0.036. All ps < 0.001).
We used multivariate stepwise regression to quantify the relative explanatory power of the different demographic, clinical, and mood factors on QOLIE-10 scores. The QoL score was significantly predicted (R2 = 0.477, p < 0.001) by a regression model, including the age of the patient, the age of epilepsy begins, the number of ASMs, depression (BDI-II, HADS-D scores), and anxiety scores (STAI-T) as latent factors.
Discussion
Patients admitted to epilepsy monitoring units constitute a group of patients with unique characteristics. The presence of drug resistance and clinical features allow grouping and differentiating them even from outpatients, especially considering the diagnostic context. The admissions usually last a week in adult patients although they tend to be shorter for children. Admission times for invasive epilepsy procedures are even longer, lasting 2 or 3 weeks. During this time frame, medical efforts aim to answer epileptological questions, and subtle psychiatric disorders are usually overlooked (24). Throughout this period, patients are seen by nurses, medical technologists, neurologists, neurophysiologists, and health care teams indirectly related to epilepsy for whom the awareness of specific comorbidities is perhaps even more unknown.
Taking into consideration psychiatric comorbidities during the diagnostic process and subsequent discharge is relevant from several aspects. When the health care team is aware of psychiatric symptomatology, it can help establish a more empathetic physician–patient relationship and improve the patient's compliance to receive instructions, understand specific diagnostic procedures, and describe symptoms that psychiatric modulators can influence. In our series, 32.45% of the patients had a history of psychiatric mood disorders. The prevalence at the time of admission was higher, being between 30.84 and 49.9% for depressive symptoms, according to the scale used, and between 44.78 and 52.63% for anxiety symptoms. This finding is consistent with previous reports describing that psychiatric disorders are underdiagnosed in epilepsy (9). The determination of psychiatric comorbidity should influence a change in the choice of ASM with suitable characteristics for this comorbidity and the eventual indication of a specific psychiatric treatment under the specialist's control. Severe psychiatric symptoms, especially suicide risk, must be detected to establish adequate preventive measures (25, 26). On the other hand, the severity of the preexisting psychiatric pathology can be seriously affected after surgical procedures when this comorbidity is overlooked (27).
In our sample, we did not find a significant correlation between the number of ASMs and the prevalence of psychiatric symptoms or quality of life. However, other groups, using specific tools such as the Epitrack, a test specifically designed to evaluate cognitive side effects of medication, have found a negative correlation between them and the number of ASMs in TLE patients (28). A significant difference was only observed in the number of ASMs for the PNES group, which, on average, was on less medication. In the same line, other groups have found similar differences in this regard (24).
Several studies analyze the prevalence of psychiatric symptoms by epilepsy subtype. Some studies show a higher prevalence of mood disorders in TLE, arguing the involvement of mesial temporal structures part of the limbic system (29–31). However, many other studies find no differences during their lifetime (3, 32, 33). Methodological factors could explain these discrepancies. Various diagnostic instruments are used for psychiatric evaluation, ranging from questionnaires to more objective and reliable clinical diagnostic assessments. On the other hand, the diagnostic criteria for focal epilepsies can be inhomogeneous, depending on the setting in which the patient is evaluated. Finally, another confounding factor may be the use of diverse ASMs that can, in turn, modulate psychiatric factors in patients. The psychiatric findings of the studies are, therefore, difficult to compare (32). In our series, no differences were found between the prevalence of symptoms of depression or anxiety in TLE vs. extratemporal focal epilepsies despite the large number of patients evaluated. Nor were significant changes seen in the comparison between generalized and focal epilepsies. Only the duration of epilepsy in the PWE group was a risk factor for the appearance of symptoms. Therefore, our results support the hypothesis of a multifactorial cause in patients with refractory epilepsy (24).
Another relevant finding of this study is the gender differences found in the prevalence of psychiatric symptoms. The analysis of our series reveals that the BDI-II scores showed significant differences; that is, females had a higher incidence of pathological BDI-II scores than males (F: 56.58%, M: 41.04%). However, the comparison of HADS-D scores was not significant. Similarly, anxiety domains showed differences in pathologic HADS-A scores. Female patients revealed a higher incidence of pathologic HADS-A scores (50.75%) than male patients (36.82%) and scored higher also in STAI-S. Considering differences in quality of life by gender, a significant gap was also observed. Females (74.91%) had higher pathologic QOLIE-10 scores than males (66.5%). Recent studies also report similar results, suggesting that gender-specific approaches can be taken (34).
Besides epilepsy, a substantial number of the patients admitted to EMUs present with PNES, and a smaller group displays an association of both pathologies (35, 36). It is shown that PNES patients manifest functional, anatomical, and autonomic brain changes compared with healthy subjects and epilepsy patients without PNES (37–40). On the other hand, it is suggested that a wide range of psychopathologies may be the basis of PNES and that their treatment could improve clinical outcomes, avoiding the perpetuation of ongoing psychogenic seizures (35). In our series, 11.36% of patients presented isolated PNES, and another 6.69% had concurrent epilepsy and PNES, the total prevalence of PNES was 18.05%, which is consistent with previous reports (24, 33, 41). Of the total group with epilepsy (428 patients), 7.7% had PNES. Likewise, of the total group with PNES (89 patients), 37% had epilepsy. A recent metanalysis shows that the pooled frequency of epilepsy among those with PNES was 22% compared with 12% of PNES among those with epilepsy (42). In other words, in our case of EMU patients, the prevalence of epilepsy in PNES is approximately double among PWE, and that of PNES in PWE is around half. This could be explained by more selective screening of patients by excluding PNES before admission to UMEs compared with the general epilepsy population.
Furthermore, most studies exclude the mixed pathology group from their analyses. However, in our experience, it constitutes a clinical entity differentiated from patients with epilepsy or PNES alone. Our results suggest it is relevant to analyze this group separately.
When considering the prevalence of psychiatric symptoms in patients admitted to UMEs, a recent study of 101 patients detected that PNES patients scored significantly higher on the depression and anxiety scales than PWE. In addition, the overall QOLIE-31 score was worse for PWE than for PNES (3, 24). A different study including 200 participants shows that PNES patients have higher self-reported anxiety and depression levels but similar QoL to PWE (24).
In our comparative group analysis of depression rating scales, we observed that the PNES and combined groups have a higher incidence of pathologic BDI-II scores. BDI-II scores were significantly higher in the PNES (64.29%) and combined groups (78.79%) than the epilepsy group (45.57%). Similarly, HADS-D scores were significantly higher in the combined group (65.62%) than the epilepsy group (28.38%) and the PNES group (30.61%).
In relation to anxiety scores between the groups, a significant association of the pathological HADS-A scores is demonstrated, showing that the PNES and the combined group also have a higher incidence of pathological scores than the epilepsy group. HADS-A scores were also significantly higher in the combined group (71.88%) than in the PNES group (54%) and the epilepsy group (41.27%). On the other hand, The STAI-T score was significantly higher in the combined group (75.76%) than in the epilepsy group (53.94%) as were the STAI-S scores (70 and 50.27%, respectively).
Finally, these differences also corresponded with worsening in the quality of life of the patients. QOLIE-10 scores positively correlate with BDI-II scores and STAI-T. Partial correlations revealed significant independent relations between anxiety and depression and QoL, suggesting that the quality of life is affected similarly by both symptoms. Using multiple regression procedures, we also found that psychiatric comorbidities are relevant latent predictors of QoL associated with the patient's age, the age at which epilepsy was first diagnosed, and the number of ASMs. In the comparative analysis of groups, the QOLIE demonstrated pathological values in the group with epilepsy, PNES, and combined of 69.49, 76.36, and 84.38%, respectively. QOLIE-10 scores were also significantly higher in the combined group than in the epilepsy group.
These data confirm that patients with PNES have higher rates of depression than patients with isolated epilepsy, which has been previously reported (24). Moreover, we also found that patients suffering from both pathologies (epilepsy + PNES) present even higher ranges of depression and anxiety than patients with isolated psychogenic seizures or epilepsy. To interpret this difference, we propose a perspective within a broader framework, that is, a dual pathological model of the functional substrates of PNES and focal epilepsy. There is growing evidence from biomarker studies in PNES, suggesting that structural and functional changes observed in the brain may act as predisposing or precipitating factors for PNES. These changes could be secondary to early emotional trauma (37, 43). On the other hand, modern concepts of focal epilepsy interpret epileptogenicity based on the interaction of abnormal brain networks (44). How both etiological substrates interact is unknown, but they could theoretically explain the differences observed in the prevalence of psychiatric phenomena.
Our study has several limitations. First, it is a monocentric study with the constraints that this entails. Second, the scales used are for general psychiatric use and have not been designed explicitly for epilepsy. For this, using specifically developed scales, such as EpiTrack or the Neurological Disorders Depression Inventory for Epilepsy, could have provided more specific data. Third, we have not controlled the evolution of the patients, which could have provided important information regarding prognostic factors. Finally, our sample is based on the prospective collection of psychiatric symptoms using scales properly validated in Spanish but does not include clinical psychiatric diagnosis obtained through a specialized medical evaluation. Neuropsychiatric tests can identify people with anxiety and depression, but the results may be inconsistent with the clinical psychiatric evaluation. False negative screening tests can incorrectly assure that patients do not have a depressive or anxiety disorder, especially in patients with PNES (45). In our sample, only patients with PNES received, per protocol, a formal psychiatric evaluation at the time of VEEGM.
In conclusion, our study comprehends a large record of patients admitted to EMUs. Anxiety and depression symptoms are present in at least half of them with a direct negative effect on the quality of life of patients. Even more, anxiety symptoms seem to be more prevalent than depression. It provides valuable information comparing diagnostic groups, revealing that patients who have epilepsy associated with PNES present the highest rates of depression and anxiety. In addition, our analysis confirms that female patients show severer symptomatic and a worse QoL. Finally, it is evidenced that both depression and anxiety symptoms can independently affect the QoL of patients.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by the Clinical Research Ethics Committee (CEIC-Parc de Salut Mar). The patients/participants provided their written informed consent to participate in this study.
Author Contributions
RR was responsible for the study concept, methodology design, and medical writing. EP and AB were responsible for data collecting. BC was responsible for data collecting and statistical analysis. CP-E was responsible for data collecting, manuscript reviewing, and neuropsychological analysis. LP was responsible for data collecting and manuscript reviewing. AP contributed with data collecting and manuscript reviewing. RZ contributed with the statistical analysis, methodology, medical writing, and reviewing the article. All authors contributed to the article and approved the submitted version.
Funding
This work received support from the project Emergent Cluster of the Human Brain (CECH) and the European Regional Development Fund under the framework of the ERFD Operative Program for Catalonia.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Tellez-Zenteno JF, Patten SB, Jetté N, Williams J, Wiebe S. Psychiatric comorbidity in epilepsy: A population-based analysis. Epilepsia. (2007) 48:2336–44. doi: 10.1111/j.1528-1167.2007.01222.x
2. Johnson EK, Jones JE, Seidenberg M, Hermann BP. The relative impact of anxiety, depression, and clinical seizure features on health-related quality of life in epilepsy. Epilepsia. (2004) 45:544–50. doi: 10.1111/j.0013-9580.2004.47003.x
3. Avalos JC, Silva BA, Tevés Echazu MF, Rosso B, Besocke AG, Del M, et al. Quality of life in patients with epilepsy or psychogenic nonepileptic seizures and the contribution of psychiatric comorbidities. Epilepsy Behav. (2020) 112:107447. doi: 10.1016/j.yebeh.2020.107447
4. Scévola L, Sarudiansky M, Lanzillotti A, Oddo S, Kochen S, D'alessio L. To what extent does depression influence quality of life of people with pharmacoresistant epilepsy in Argentina? Clin Res. (2017) 69:133–8. doi: 10.1016/j.yebeh.2017.01.007
5. Myers L, Trobliger R, Bonafina M, Vazquez-Casals G, Lancman M, Lancman M. Clinical Research Depression, anxiety, and clinical history in Spanish-speaking American patients with psychogenic nonepileptic seizures (PNES) compared with Spanish-speaking American patients with epilepsy. Epilepsy Behav. (2019) 102:106694. doi: 10.1016/j.yebeh.2019.106694
6. Suda T, Tatsuzawa Y, Mogi T, Yoshino A. Interictal dysphoric disorder in patients with localization-related epilepsy: diagnostic relationships with DSM-IV psychiatric disorders and the impact of psychosocial burden. Epilepsy Behav. (2016) 54:142–7. doi: 10.1016/j.yebeh.2015.11.020
7. Fiest KM, Dykeman J, Patten SB, Wiebe S, Kaplan GG, Maxwell CJ, et al. Depression in epilepsy: a systematic review and meta-analysis. Neurology. (2013) 80:590–9. doi: 10.1212/WNL.0b013e31827b1ae0
8. Dalmagro CL, Velasco TR, Bianchin MM, Martins APP, Guarnieri R, Cescato MP, et al. Psychiatric comorbidity in refractory focal epilepsy: A study of 490 patients. Epilepsy Behav. (2012) 25:593–7. doi: 10.1016/j.yebeh.2012.09.026
9. Jones JE, Hermann BP, Barry JJ, Gilliam F, Kanner AM, Meador KJ. Clinical assessment of axis I psychiatric morbidity in chronic epilepsy: a multicenter investigation. J Neuropsychiatry Clin Neurosci. (2005) 17:172–9. doi: 10.1176/jnp.17.2.172
10. Desai S, Shukla G, Goyal V, Srivastava A, Srivastava MVP, Tripathi M, et al. Changes in psychiatric comorbidity during early postsurgical period in patients operated for medically refractory epilepsy-A MINI-based follow-up study. Epilepsy Behav. (2013) 32:29–33. doi: 10.1016/j.yebeh.2013.11.025
11. Guarnieri R, Walz R, Hallak JEC, Coimbra É, de Almeida E, Cescato MP, et al. Do psychiatric comorbidities predict postoperative seizure outcome in temporal lobe epilepsy surgery? Epilepsy Behav. (2009) 14:529–34. doi: 10.1016/j.yebeh.2009.01.002
12. Maria De Araujo Filho G, Eliza A, Furlan R, Sa AE, Ribeiro A, Helena L, et al. Psychiatric disorders as " hidden" contraindications for presurgical VEEG in patients with refractory epilepsy: A retrospective cohort study in a tertiary center. Epilepsy Behav. (2015) 45:35–8. doi: 10.1016/j.yebeh.2015.02.026
13. Cankurtaran ES, Ulug B, Saygi S, Tiryaki A, Akalan N. Psychiatric morbidity, quality of life, and disability in mesial temporal lobe epilepsy patients before and after anterior temporal lobectomy. Epilepsy Behav. (2005) 7:116–22. doi: 10.1016/j.yebeh.2005.03.019
14. Scott AJ, Sharpe L, Hunt C, Gandy M. Anxiety and depressive disorders in people with epilepsy: A meta-analysis. Epilepsia. (2017) 58:973–82. doi: 10.1111/epi.13769
15. Milán-Tomás Á, Persyko M, del Campo M, Shapiro CM, Farcnik K. An overview of psychogenic non-epileptic seizures: etiology, diagnosis and management. Canad J Neurol Sci. (2018) 45:130–6. doi: 10.1017/cjn.2017.283
16. Benbadis SR, Agrawal V, Tatum WO. How many patients with psychogenic nonepileptic seizures also have epilepsy? Neurology. (2001) 57:915–7. doi: 10.1212/wnl.57.5.915
17. Wadwekar V, Nair PP, Murgai A, Thirunavukkarasu S, Thazhath HK. Semiologic classification of psychogenic non epileptic seizures (PNES) based on video EEG analysis: Do we need new classification systems? Seizure. (2014) 23:222–6. doi: 10.1016/j.seizure.2013.12.005
18. Spielberger CD. State-Trait Anxiety Inventory: Bibliography (2nd ed.). Palo Alto, CA: Consulting Psychologists Press (1989).
19. Guillén-Riquelme A, Buela-Casal G. [Psychometric revision and differential item functioning in the State Trait Anxiety Inventory (STAI)]. Psicothema. (2011) 23:510–5.
20. Beck AT, SRA & BGK. Manual for the Beck Depression Inventory-II. San Antonio, TX: Psychological Corporation (1996).
21. Sanz J, Luis A, Carmelo P, Resumen V. CLÍNICA Y SALUD 249 ARTÍCULOS Adaptación española del Inventario para la Depresión de Beck-II (BDI-II): 2. Propiedades psicométricas en población general The spanish adaptation of Beck's Depression Inventory-II (BDI-II): 2. Psychometric properties in the general population. (2003) Available online at: https://www.redalyc.org/pdf/1806/180617972001.pdf (accessed August 17, 2021).
22. Cramer JA, Perrine K, Devinsky O, Meador K. A brief questionnaire to screen for quality of life in epilepsy: the QOLIE-10. Epilepsia. (1996) 37:577–82. doi: 10.1111/j.1528-1157.1996.tb00612.x
23. Viteri C, Codina M, Cobaleda S, Lahuerta J, Barriga J, Barrera S, et al. [Validation of the Spanish version of the QOLIE-10 quality of life in epilepsy questionnaire]. Neurologia. (2008) 23:157–67.
24. Abe C, Denney D, Doyle A, Cullum M, Adams J, Perven G, et al. Comparison of psychiatric comorbidities and impact on quality of life in patients with epilepsy or psychogenic nonepileptic spells. Epilepsy Behav. (2020) 102:106649. doi: 10.1016/j.yebeh.2019.106649
25. Blumer D, Montouris G, Davies K, Wyler A, Phillips B, Hermann B. Suicide in epilepsy: Psychopathology, pathogenesis, and prevention. Epilepsy Behav. (2002) 3:232–41. doi: 10.1016/S1525-5050(02)00006-9
26. Fazel S, Wolf A, Långström N, Newton CR, Lichtenstein P. Premature mortality in epilepsy and the role of psychiatric comorbidity: A total population study. Lancet. (2013) 382:1646–54. doi: 10.1016/S0140-6736(13)60899-5
27. Wrench J, Wilson J, Bladin F. Mood disturbance before and after seizure surgery: a comparison of temporal and extratemporal resections. Epilepsia. (2004) 45:534–43. doi: 10.1111/j.0013-9580.2004.48803.x
28. Lozano-García A, Hampel KG, Villanueva V, González-Bono E, Cano-López I. The number of anti-seizure medications mediates the relationship between cognitive performance and quality of life in temporal lobe epilepsy. Epilepsy Behav. (2021) 115:107699. doi: 10.1016/j.yebeh.2020.107699
29. Kondziella D, Alvestad S, Vaaler A, Sonnewald U. Which clinical and experimental data link temporal lobe epilepsy with depression? J Neurochemistry. (2007) 103:2136–52. doi: 10.1111/j.1471-4159.2007.04926.x
30. Yilmazer-Hanke D, O'Loughlin E, Mcdermott K. Contribution of amygdala pathology to comorbid emotional disturbances in temporal lobe epilepsy. J Neurosci Res. (2016) 94:486–503. doi: 10.1002/jnr.23689
31. Lu E, Pyatka N, Burant CJ, Sajatovic M. Systematic literature review of psychiatric comorbidities in adults with epilepsy. J Clin Neurol. (2021) 17:176–86. doi: 10.3988/jcn.2021.17.2.176
32. Swinkels WAM, van Emde Boas W, Kuyk J, van Dyck R, Spinhoven P. Interictal depression, anxiety, personality traits, and psychological dissociation in patients with temporal lobe epilepsy (TLE) and extra-TLE. Epilepsia. (2006) 47:2092–103. doi: 10.1111/j.1528-1167.2006.00808.x
33. Sanchez-Gistau V, Pintor L, Sugranyes G, Baillés E, Carreño M, Donaire A, et al. Prevalence of interictal psychiatric disorders in patients with refractory temporal and extratemporal lobe epilepsy in Spain. A comparative study. Epilepsia. (2010) 51:1309–13. doi: 10.1111/j.1528-1167.2009.02464.x
34. de Barros ACS, Furlan AER, Marques LHN, de Araújo Filho GM. Gender differences in prevalence of psychiatric disorders, levels of alexithymia, and coping strategies in patients with refractory mesial temporal epilepsy and comorbid psychogenic nonepileptic seizures. Epilepsy Behav. (2018) 82:1–5. doi: 10.1016/j.yebeh.2018.02.026
35. Diprose W, Sundram F, Menkes DB. Psychiatric comorbidity in psychogenic nonepileptic seizures compared with epilepsy. Epilepsy Behav. (2016) 56:123–30. doi: 10.1016/j.yebeh.2015.12.037
36. Bodde NMG, Brooks JL, Baker GA, Boon PAJM, Hendriksen JGM, Aldenkamp AP. Psychogenic non-epileptic seizures-diagnostic issues: a critical review. Clin Neurol Neurosurg. (2009) 111:1–9. doi: 10.1016/j.clineuro.2008.09.028
37. Mcsweeney M, Reuber M, Levita L. Neuroimaging studies in patients with psychogenic non-epileptic seizures: A systematic meta-review. NeuroImage: Clin. (2017) 16:210–21. doi: 10.1016/j.nicl.2017.07.025
38. Allendorfer JB, Nenert R, Hernando KA, DeWolfe JL, Pati S, Thomas AE, et al. FMRI response to acute psychological stress differentiates patients with psychogenic non-epileptic seizures from healthy controls – A biochemical and neuroimaging biomarker study. NeuroImage: Clin. (2019) 24:101967. doi: 10.1016/j.nicl.2019.101967
39. Ding J, An D, Liao W, Wu G, Xu Q, Zhou D, et al. Abnormal functional connectivity density in psychogenic non-epileptic seizures. Epilepsy Res. (2014) 108:1184–94. doi: 10.1016/J.EPLEPSYRES.2014.05.006
40. Romigi A, Ricciardo Rizzo G, Izzi F, Guerrisi M, Caccamo M, Testa F, et al. Heart rate variability parameters during psychogenic non-epileptic seizures: comparison between patients with pure PNES and comorbid epilepsy. Front Neurol. (2020) 11:713. doi: 10.3389/fneur.2020.00713
41. Hamed SA, Attiah FA, Fawzy M. Psychogenic nonepileptic seizures in adults with epilepsy: a tertiary hospital-based study. Int J Neurosci. (2020) 130:522–32. doi: 10.1080/00207454.2019.1698566
42. Kutlubaev MA, Xu Y, Hackett ML, Stone J. Dual diagnosis of epilepsy and psychogenic nonepileptic seizures: Systematic review and meta-analysis of frequency, correlates, and outcomes. Epilepsy Behav. (2018) 89:70–8. doi: 10.1016/j.yebeh.2018.10.010
43. Mcsweeney M, Reuber M, Hoggard N, Levita L. Cortical thickness and gyrification patterns in patients with psychogenic non-epileptic seizures. Neurosci Lett. (2018) 678:124–30. doi: 10.1016/j.neulet.2018.04.056
44. Bartolomei F, Lagarde S, Wendling F, McGonigal A, Jirsa V, Guye M, et al. Defining epileptogenic networks: contribution of SEEG and signal analysis. Epilepsia. (2017) 58:1131–47. doi: 10.1111/epi.13791
Keywords: epilepsy, anxiety, depression, quality of life, epilepsy monitoring unit
Citation: Rocamora R, Chavarría B, Pérez E, Pérez-Enríquez C, Barguilla A, Panadés-de Oliveira L, Principe A and Zucca R (2021) Mood Disturbances, Anxiety, and Impact on Quality of Life in Patients Admitted to Epilepsy Monitoring Units. Front. Neurol. 12:761239. doi: 10.3389/fneur.2021.761239
Received: 19 August 2021; Accepted: 23 September 2021;
Published: 28 October 2021.
Edited by:
Zucai Xu, Affiliated Hospital of Zunyi Medical University, ChinaReviewed by:
Silvia Kochen, Hospital EL Cruce, ArgentinaMirna Portuguez, Pontifical Catholic University of Rio Grande do Sul, Brazil
Copyright © 2021 Rocamora, Chavarría, Pérez, Pérez-Enríquez, Barguilla, Panadés-de Oliveira, Principe and Zucca. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rodrigo Rocamora, cnJvY2Ftb3JhQHBzbWFyLmNhdA==
†Member of the European Reference Network EpiCARE