
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurol. , 23 November 2021
Sec. Neurorehabilitation
Volume 12 - 2021 | https://doi.org/10.3389/fneur.2021.720282
This article is part of the Research Topic Long Term Disability in Neurological Disease: A Rehabilitation Perspective View all 20 articles
 Mayra Priscila Boscolo Alvarez1†
Mayra Priscila Boscolo Alvarez1† Carlos Bandeira de Mello Monteiro1,2†
Carlos Bandeira de Mello Monteiro1,2† Talita Dias da Silva1,3,4*
Talita Dias da Silva1,3,4* Vitor E. Valenti5
Vitor E. Valenti5 Celso Ferreira-Filho3
Celso Ferreira-Filho3 Annette Sterr6
Annette Sterr6 Luiz Carlos Marques Vanderlei5Celso Ferreira3
Luiz Carlos Marques Vanderlei5Celso Ferreira3 David M. Garner7
David M. Garner7Introduction: Due to functional and autonomic difficulties faced by individuals with Duchenne Muscular Dystrophy (DMD), the use of assistive technology is critical to provide or facilitate functional abilities. The key objective was to investigate acute cardiac autonomic responses, by application of Heart Rate Variability (HRV), during computer tasks in subjects with DMD via techniques based on non-linear dynamics.
Method: HRV was attained via a Polar RS800CX. Then, was evaluated by Chaotic Global Techniques (CGT). Forty-five male subjects were included in the DMD group and age-matched with 45 in the healthy Typical Development (TD) control group. They were assessed for 20 min at rest sitting, and then 5 min whilst performing the maze task on a computer.
Results: Both TD and DMD subjects exhibited a significantly reduced HRV measured by chaotic global combinations when undertaking the computer maze paradigm tests. DMD subjects presented decreased HRV during rest and computer task than TD subjects.
Conclusion: While there is an impaired HRV in subjects with DMD, there remains an adaptation of the ANS during the computer tasks. The identification of autonomic impairment is critical, considering that the computer tasks in the DMD community may elevate their level of social inclusion, participation and independence.
Duchenne Muscular Dystrophy (DMD), is the most prevalent form of muscular dystrophy (1). It is a terminal illness characterized by progressive muscular weakness with proximal onset in the lower limbs spreading later to the rest of the body, which leads the individual to become confined to a wheelchair (2). In addition, cardiorespiratory (3), and autonomic (4) changes are observed and death in early adulthood, at around 20 years old (2).
In consideration of the progressive functional difficulties presented by people with DMD, the use of assistive technology by rehabilitation programs is important as it promotes greater functional independence and improves the social performance of these disabled persons (5). With computational advances in assistive technology, rehabilitation programs via computing situations during treatment allow the persons with DMD to practice tasks in a different environment using an informal interface and rapid responses. It is similarly capable of providing a dynamic interaction and vivacity with elements and goals, by means of logical reasoning and reaction times associated with the movement, permitting the repetition of muscle contractions and improved performance (6). In this manner, studying the acute and chronic responses of altered physiological systems in DMD individuals despite this technology is fundamental and could support a better understanding of these changes induced by DMD and, an improved guide as to it becoming a therapeutic procedure.
As described previously, an important physiological system modified by DMD is the autonomic nervous system (ANS) (7). Studies including the acute cardiac autonomic responses during computer tasks in DMD are rare. Yet, by implying the linear methods for analysis of heart rate variability (HRV) to evaluate cardiac autonomic responses in DMD subjects during computer tasks, Alvarez et al. (8) detected that DMD subjects responded with a reduced HRV. But then, those during computer tasks exhibited greater intensity of cardiac autonomic responses when compared to the Typical Developed (TD) subjects which were the control group.
Nevertheless, Sassi et al. (9) stated that non-linear techniques of HRV may provide new evidence for the understanding of cardiac control, as it provides information on the complexity of the underlying physiological mechanisms. An innovative group of procedures sensitive non-linearly for the detection of HRV fluctuations that allows us to understand the irregularity, unpredictability, extent of fractal self-similarity, and complexity of the signals are the Chaotic Global Techniques (CGT) (10). These metrics have been effectively applied to assess cardiac autonomic modulation in physiological and pathological conditions (11–15), once non-linear methods describe complex rhythm fluctuations more appropriately than linear methods (16), as “chaos theory” exhibits characteristics that are consistent with those found physiologically in the human organism.
The human organism exhibits chaotic properties, specifically, it is composed of several systems, which are dynamic, deterministic, and sensitive to initial circumstances. All these factors are capable of producing non-linear, non-proportional, or direct responses to stimuli in these systems, hence, trivial dysfunctions in one organ can engender different levels of dysfunction in the others (17, 18). Thus, the human body is better understood as a complex and non-linear system, hence assessments of HRV via non-linear techniques have gained recognition (19).
Accordingly, we proposed to study acute cardiac autonomic responses during computer tasks in individuals with DMD vs. TD people using CGT. The CGT may complement important information in the research literature on the complexity of the cardiac autonomic response during the execution of computer games. We hypothesized that during computer tasks the HRV responses via CGT demonstrated a lesser response to complexity. Subsequently, it should have a greater response in the DMD subjects.
This trial was completed using the data analyzed and published by Alvarez et al. (8), yet, for this study the data were evaluated through CGT. The present study was performed in accordance to the Declaration of Helsinki.
This study conforms to the Consolidated Standards of Reporting Trials (CONSORT) statement (20).
The study protocol was approved by the research ethics committee of the University of São Paulo, reference number 236/13 was attached. Written consent terms were obtained from participants (or guardians) over 18 years old. Acceptance terms were obtained from participants younger than 17 and also written consent terms from the legally authorized representative/parents of those participants under 17 years old.
Forty-five individuals with DMD and 45 age-matched healthy TD individuals participated in the trial. DMD diagnoses was based on molecular methods and/or muscular protein expression. Exclusion criteria comprised subjects with severely dilated myocardium, other associated diseases and individuals with inability to understand task instructions. DMD severity was classified according to the Vignos scale (21). See Table 1.
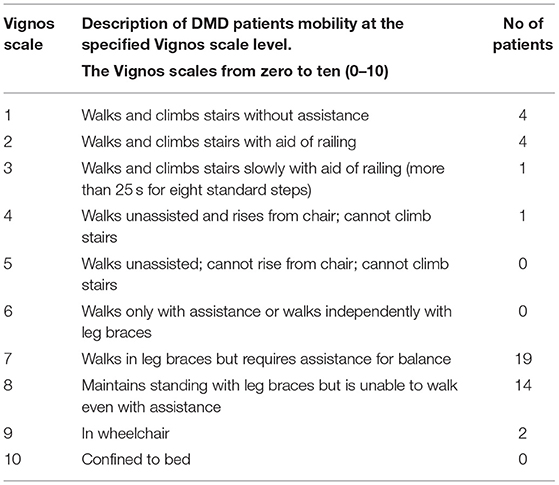
Table 1. Disease status according to Vignos scale.
The protocol was identical to that used in Alvarez et al. (8) where HR was recorded beat-to-beat (RR intervals) using the portable Polar RS800CX eletrocardiographic monitor (Polar Electro, Finland). HR was recorded prior to the onset and at the end of the 5 min of the computer maze paradigm task.
The subjects were seated in a standard chair (walkers, TD group, and DMD) or in their own wheelchair (non-walkers, DMD group), the Polar watch was situated on their wrist. The analysis of HRV was possible via the recording of RR interval in two periods: the period of 20 min at rest seated, and then during the computer task for 5 min, as demonstrated in Figure 1.
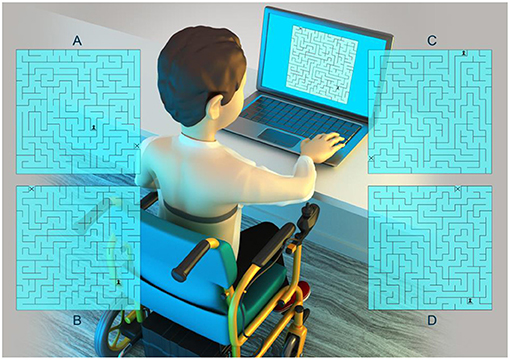
Figure 1. Visualization of experimental set up. Mazes (A–D) represent the four mazes used in this study. The range was of one to four mazes performed for the participants during 5 minutes.
The computer task used a maze paradigm with one correct pathway that could be negotiated and ultimately solved; the paradigm was adapted by Souza et al. (22). All participants were positioned comfortably with an evaluator responsible for instruction and data annotation.
Each individual was instructed to walk the correct path with the digital character pawn (pointed on the screen by the evaluator) to the exit of the maze identified by an “x” (pointed on the screen by the evaluator). It was provided for the subjects, who used the arrow buttons on the keyboard, identified by up, down, right and left, using the dominant hand, with the arrows moving through a 20 cm × 20 cm maze. Participants were told to complete the maze as quickly as possible.
HRV analysis followed the guidelines published by the Task Force of the European Society of Cardiology and North American Society of Pacing and Electrophysiology (23). The RR intervals were recorded, and then were downloaded to the Polar Precision Performance program (v.3.0). This software enabled the visualization of HR and the extraction of a cardiac period (RR intervals series; the variation of beat-to-beat interval in milliseconds) file in “.txt” format. For analysis of HRV data at rest, we evaluated 1,000 consecutive RR intervals, and for HRV analysis for the computational task, the number of consecutive RR intervals obtained was exactly 256 RR intervals. Digital filtering complemented by manual filtering was performed to eliminate artifacts and only series with >95% of sinus beats were included in the study (19). HRV analysis was undertaken through CGT.
As stated in 2016 by Wajnsztejn et al. (12) and, later by Alves et al. (24), these techniques encompass of a variety of mathematical and signal processing events. In this study, we enforced the Multi-Taper Method (MTM) power spectral technique (12, 24) to generate high spectral Entropy (hsEntropy) (24), high spectral Detrended Fluctuation Analysis (hsDFA) (25), and the Spectral Multi-Taper Method (sMTM) (10). From these three chaotic global values we computed seven non-trivial combinations which we termed the Chaotic Forward Parameters (CFP1 to CFP7) (26–29). For further information regarding the MTM techniques it is suggested to refer to Percival and Walden (30) or Thomson (31).
The dependent variables (CFP1 to CFP7), and the independent variables “group” (DMD and TD) and “task,” at (rest or computer task through maze paradigm). Parametric statistics assume the datasets are normally distributed, so the use of the mean as a measure of central tendancy. Consequently, the first assumption for the two-way analysis of variance test is normality. We applied the Anderson-Darling (26) and the Lilliefors (27) tests. The Anderson-Darling test for normality applies an empirical cumulative distribution function. The Lilliefors test is useful in studies with small sample sizes (n < 20). The results of the tests for normality were borderline. Nonetheless, as there is no non-parametric alternative to the two-way analysis of variance test we proceed aware that the accuracy could be flawed. For this reason we raise the level of significances to p < 0.01 (or <1%), rather than the usual p < 0.05 (or <5%). The second assumption was that of the equality of variances by Levene's test (32, 33). Hence, the dependent variables were submitted to a 2 (group: DMD, TD) by 2 (Task: Rest, Computer) Multiple Analysis of Variance (MANOVA) with Repeated Measures (RM) on the last factor for each CFP index. Post-hoc comparisons were undertaken by Tukey-LSD (Least Significant Difference) test. Partial eta-squared () was reported to measure the effect sizes and were interpreted as small (effect size >0.01), medium (effect size >0.06), or large (effect size >0.14) (34, 35); additionally we reported the observed power (OP). The software package operated was SPSS, version 26.0 (Chicago, Illinois, USA).
Table 2 presents the anthropometric data and Table 3 lists the medications taken by the DMD group. The TD group did not take any medications.
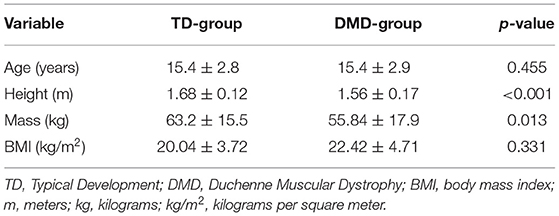
Table 2. Values (mean ± standard deviation) of age, height, mass, and body mass index (BMI) for both TD and DMD groups.
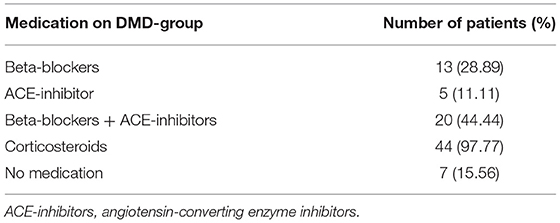
Table 3. The cardiac medications for DMD-group.
The results of the Levene's test of equality, are illustrated in Table 4. A significant p-value is set at > 0.05 (p > 0.05, >5%). This ensures that similar variances can be assumed or else the ANOVA test is invalid. This was achieved by the all of the chaotic global combinations applied with the exception of CFP7.
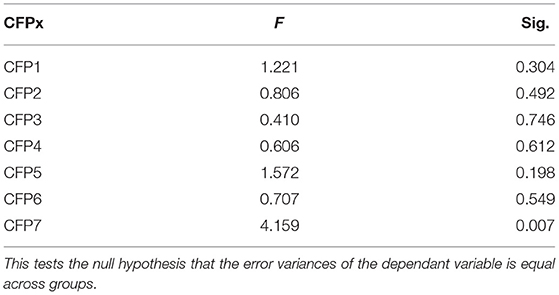
Table 4. Levene's test of equality of error variances: F-value and significances of the seven permutations of chaotic global parameters (CFP1 to CFP7).
Significant effects for Group [Wilks Lambda = 0.006; F(7, 82) = 1897.1; p < 0.001; = 0.99: OP: 1.00], Task [Wilks Lambda = 0.004; F(7, 82) = 2739.2; p < 0.001; = 0.99: OP: 1.00] and significant interaction between Group and Task [Wilks Lambda = 0.032; F(7, 82) = 352.1; p < 0.001; = 0.97: OP: 1.00]. The separate ANOVAs that established differences between Groups and Tasks in each CFP, besides their Mean, Standard Deviation, Confidence Interval, and post-hoc values are described in Table 5.
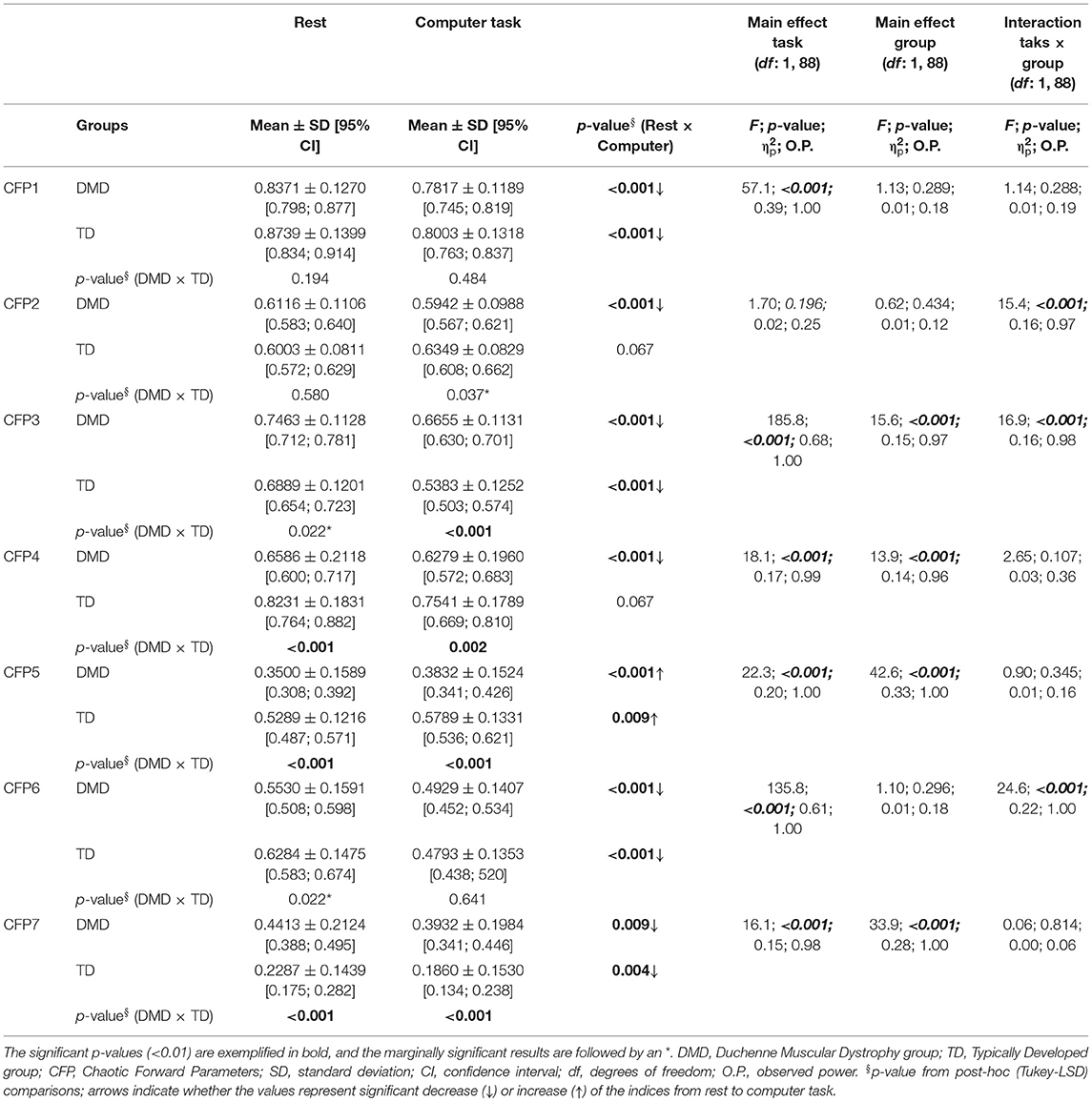
Table 5. The table below demonstrates the results of a Repeated Measures-Multiple Analysis of Variance (RM-MANOVA), between Groups, within Tasks and its interactions, in addition to mean, stardard deviation, and confidence intervals for each CFP.
Regarding Figure 2, the boxplot (left) for CFP1 to CFP7 of TD subjects RR intervals' in TD control subjects “at rest” (CCFPx: RR intervals of length 1,000) and TD control computer task subjects (TCFPx: RR intervals of length 256). Next, the boxplot (right) for CFP1 to CFP7 of DMD subjects' RR intervals in DMD control subjects “at rest” (CCFPx: RR intervals of length 1,000) and computer task subjects with DMD (TCFPx: RR intervals of length 256).
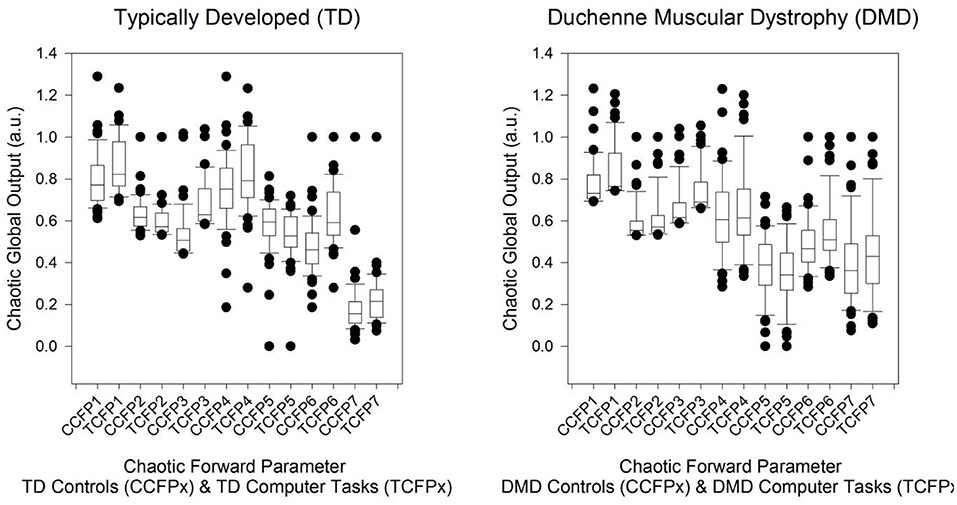
Figure 2. Boxplot (left) for CFP1 to CFP7 of TD subjects RR intervals in TD control subjects' “at rest” and TD control computer task subjects. Boxplot (right) for CFP1 to CFP7 of DMD subjects' RR intervals in DMD control subjects “at rest” and computer task subjects with DMD. The point nearest to the zero is the minimum and the point furthermost away is the maximum. The point next nearest to the zero is the 5th percentile and next furthest away is the 95th percentile. The edge of the box nearest to zero specifies the 25th percentile, and the edge of the box furthest from zero specifies the 75th percentile. The line within the box is the median. Error bars are the 10th and 90th percentiles.
The output of the RM-MANOVA can be defined as follows. Initially, deviations in the chaotic global responses in the computer task mode (Table 5). There are significant reductions from rest to computer task CFP1, CFP3, CFP4, CFP6, and CFP7, and an increase for CFP5. Next, we revealed that there are significantly lower responses in DMD group (in both rest and computer task) compared to TD group for CFP3, CFP4, CFP5, and CFP7. Finally, while the interaction term for the computer task and DMD is statistically significant for CFP2, CFP3, and CFP6, the post-hoc results are non-significant at a level of significance of p <0.01 (or <1%).
To understand which factors may influence the HRV response in DMD subjects, three regression analysis were completed between the dependent variables [(1) use of beta-blockers (yes/no), (2) use of ACE inhibitors (yes/no), and (3) use of corticoids (yes/no)] and independent variables [the differences between values of CFP1 to CFP7 on computer task and at rest, namely Δ of computer task and rest]. The analysis revealed no significant regression models for any of the three dependent variables (see Table 6).
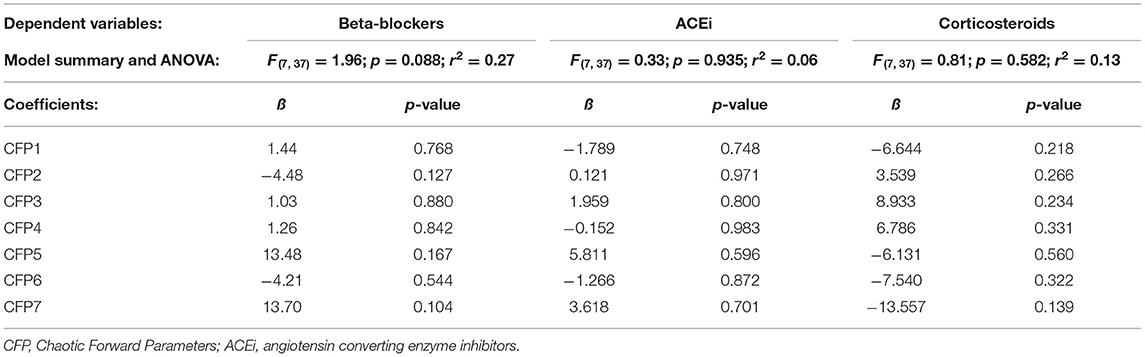
Table 6. The table illustrates the regression models and three dependent variables.
We evaluated HRV responses induced by a computer task in people with DMD and TD. As an important outcome, we established that, while the DMD group offered significantly lower autonomic responses when compared to the TD group in both rest and computer task, DMD and TD groups presented similar patterns of response from rest to computer task; explicitly, intense autonomic responses induced by the task, as established in Table 5. We can postulate that this similar pattern of responses could be due to the condition that it was a task that required more distal muscular effort, with only the need of finger movement (which is mostly maintained in adolescents with DMD), and became more of a cognitive task.
This response of both DMD and TD groups has been previously revealed in the study of Luque-Casado et al. (36), which concluded that cardiac autonomic modulation is highly sensitive to overall demands of sustained attention under the influence of cognitive processes, leading to a decrease of heart rate variability (HRV); then this is the case of the task used in our study that requires sustained attention and cognitive effort (besides the distal muscular effort) to attain the target. This process appears to be the role of the prefrontal cortex in the modulation of subcortical cardio-acceleratory circuits via an inhibitory pathway that is associated with vagal function and that can be indexed by HRV (via the baroreceptor system, namely, the negative feedback loop adjusting heart activity to the blood pressure fluctuations) (37, 38).
Considering the general lower autonomic response from DMD here, in this study; in a previous study, Silva et al. (4) through a systematic review about the HRV of subjects with DMD, confirmed that these subjects presented an impaired autonomic modulation with a decreased parasympathetic modulation and, occasionally, increased sympathetic control. Vanderlei et al. (39) revealed in obese young individuals an increase in the chaotic global response, but this is unusual since typically the pathological or disease state reduces HRV through a decreased chaotic global response.
Regarding autonomic responses during the computer task in subjects with DMD, Alvarez et al. (8) suggested the computational tasks can support the functional capacities through training and competence of the ANS, and that cardiac autonomic modulation data is useful for clinical practice. Thus, computer tasks must be performed under supervision and care taken to avoid psychological overload and exacerbation to the ANS, as previous studies have achieved reduced HRV from an early stage of disease in DMD (4, 32, 33), conceivably leading to cardiac (40, 41), or respiratory (42) failure.
Even so, Alvarez et al. (8) evaluated only linear approaches and previous studies have demonstrated that non-linear methods are clinically important for the interpretation of pathological mechanisms related to HRV, providing extra information to using linear methods alone (43). de Godoy (43) concluded, via a review study on patients with cardiovascular disease, that the non-linear analysis of HRV is valuable to characterize autonomic balance, which is a reliable marker of complications and subsequent mortality.
The HRV analysis techniques with linear methods, in the time and frequency domains are not sufficient to characterize a cardiac dynamical balance. Instead, the mechanisms involved in cardiovascular regulation interact with each other in complex and chaotic ways (43). Therefore, HRV analysis using CGT should be able to characterize the HRV in a more reliable manner and, afterwards, autonomic cardiac modulation.
In this study, we have revealed that the computer task reduces the HRV as measured by CGT in the CFP1, CFP3, CFP4, CFP5, CFP6, and CFP7 combinations. This is the case for TD and the DMD groups. It was expected that CFP1 and CFP3 would be two of the most significant parameters. CFP1 applies all three chaotic global parameters. There is evidence to enforce CFP1 as the most robust function as with the optimization study by Garner and Ling (10). Intrinsically, it is generally the most robust combination overall. Moreover, it is the most robust in the forward problems in youth and childhood obesity (44), type I diabetes mellitus (13), and COPD (11). CFP3 is frequently the most statistically significant combination, based on statistical significance alone.
This has been demonstrated for both forward (11, 13, 39) and inverse (10) problems. The critical factor regarding the significance of the results is data length. We would advise a data length of at least 900 RR intervals. This is pertinent here as in some datasets the number of RR intervals was exactly 256 hence about 5 min of time-series when undergoing the task. Despite a potential sparse data hazard the correct levels of significance were achieved (p < 0.01; <1%). There is a difference between number of RR intervals in both groups for rest and task. Task time was reduced compared to rest time owing to muscle fatigue that could be caused in the DMD group, as this is a characteristic of the disease.
Future algorithmic manipulations could involve varying the DPSS (45) settings or adjusting Thomson's non-linear combination methods (31) to maximize discrimination. Lastly, weightings of these CGT could be modified as here they are set at unity. This is particularly appropriate for the CFP1 and CFP3 combinations.
Given that DMD subjects benefit from assistive technology; social inclusion, participation, and development—the necessary physiological responses from the technology must be assessed with the possible risk of cardiac, respiratory, dynamical disease (46, 47) states, and general physiological decline. Yet, we understand that future studies should evaluate the HRV recovery from computer tasks so as to state if ANS recovers (or not) from activity, and also to measure if there are positive posterior effects on HRV, as occurs with chronic response of blood pressure after exercises. So, our results support the detection of autonomic responses in DMD during a computer task, to permit the planning of an advantageous clinical management of this group of patients.
Some limitations from this study should be highlighted:
(1) The use of pharmacotherapies could influence our results; beta-blockers and angiotensin-converting enzyme (ACE) inhibitors could interfere in autonomic functions, but these medications are often prescribed and their cessation is not medically or ethically possible, so patients included in the study continued to take these medications. Similarly, we performed a regression analysis so as to study if these medications interfered with our outcomes and did not find any significant results. Besides, we encourage additional studies to evaluate the early effects of autonomic dysfunction in DMD children during the computer tasks; especially those without medication.
(2) To obtain HRV data at different stages of the disease and to better characterize the population; various degrees of pathology (Vignos scale 1–9) were included;
(3) We did not enforce any breathing rhythm and/or emotional analysis; those data in DMD and control group provided useful information and could be important for future studies.
DMD subjects presented a lower non-linear HRV compared to TD subjects at rest and during a computer task. Both groups exhibited a similar pattern of reduced non-linear HRV during computer tasks with sustained attention demand when measured by the CGT. It demonstrates that although there is an impaired HRV in subjects with DMD, there remains an adaptation of the ANS throughout the computer task. The identification of autonomic impairment is critical when considering the patients' ANS responses, taking into consideration that the computer tasks in the DMD community may elevate their level of social inclusion, participation, and independence. Hence, assistive technologies should be organized in combination with continuous physiological monitoring to lessen serious and possibly hazardous effects.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation. The Matlab code is unavailable due to commercial reasons.
The studies involving human participants were reviewed and approved by Ethics Committee of the University of São Paulo, reference number 236/13. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
MA and TS collected data and performed conduction of experiments. MA, CM, TS, VV, CF-F, LV, CF, and DG drafted the manuscript. MA followed the journal guidelines. DG and TS performed statistical analysis. CM supervised the study. MA and CM gave final approval for the version submitted for publication. DG and AS extensively reviewed the manuscript, English Grammar, and spelling. All authors reviewed and approved the manuscript.
CM and TS received financial support from FAPESP (Fundação de Amparo à Pesquisa do Estado de São Paulo), process numbers 2012/16970-6 and 2017/24991-7 (CM) and 2016/08358-0 (TS).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Aoki Y, Yokota T, Nagata T, Nakamura A, Tanihata J, Saito T, et al. Bodywide skipping of exons 45-55 in dystrophic mdx52 mice by systemic antisense delivery. Proc Natl Acad Sci USA. (2012) 109:13763–8. doi: 10.1073/pnas.1204638109
2. Jung IY, Chae JH, Park SK, Kim JH, Kim JY, Kim SJ, et al. The correlation analysis of functional factors and age with duchenne muscular dystrophy. Ann Rehabil Med. (2012) 36:22–32. doi: 10.5535/arm.2012.36.1.22
3. Romfh A, Mcnally EM. Cardiac assessment in Duchenne and Becker muscular dystrophies. Curr Heart Fail Rep. (2010) 7:212–8. doi: 10.1007/s11897-010-0028-2
4. Silva TD, et al. Heart rate variability and cardiopulmonary dysfunction in patients with duchenne muscular dystrophy: a systematic review. Pediatr Cardiol. (2018) 39:869–83. doi: 10.1007/s00246-018-1881-0
5. Cook AM, Polgar JM, Hussey JM. Cook and Hussey's Assistive Technologies: Principles and Practice. Mosby, MO: Year book (1995).
6. Hashimoto Y, Ushiba J, Kimura A, Liu M, Tomita Y. Change in brain activity through virtual reality based brain-machine communication in a chronic tetraplegic subject with muscular dystrophy. BMC Neurosci. (2010) 11:117. doi: 10.1186/1471-2202-11-117
7. Hall JE. Guyton and Hall Textbook of Medical Physiology, Jordanian Edition E-Book. Rio de Janeiro: Elsevier (2016).
8. Alvarez MPB, Silva TDD, Favero FM, Valenti VE, Raimundo RD, Vanderlei LCM, et al. Autonomic modulation in duchenne muscular dystrophy during a computer task: a prospective control trial. PLoS ONE. (2017) 12:e0169633. doi: 10.1371/journal.pone.0169633
9. Sassi R, Cerutti S, Lombardi F, Malik M, Huikuri HV, Peng C-K, et al. Advances in heart rate variability signal analysis: joint position statement by the e-Cardiology ESC Working Group and the European Heart Rhythm Association co-endorsed by the Asia Pacific Heart Rhythm Society. Europace. (2015) 17:1341–53. doi: 10.1093/europace/euv015
10. Garner DM, Ling BWK. Measuring and locating zones of chaos and irregularity. J Syst Sci Complex. (2014) 27:494–506. doi: 10.1007/s11424-014-2197-7
11. Bernardo AF, Vanderlei LC, Garner DM. HRV analysis: a clinical and diagnostic tool in chronic obstructive pulmonary disease. Int Sch Res Notices. (2014) 2014:673232. doi: 10.1155/2014/673232
12. Wajnsztejn R, Carvalho TDD, Garner DM, Vanderlei LCM, Godoy MF, Raimundo RD, et al. Heart rate variability analysis by chaotic global techniques in children with attention deficit hyperactivity disorder. Complexity. (2015) 21:412–9. doi: 10.1002/cplx.21700
13. Souza NM, Vanderlei LCM, Garner DM. Risk evaluation of diabetes mellitus by relation of chaotic globals to HRV. Complexity. (2015) 20:84–92. doi: 10.1002/cplx.21508
14. Antonio A, Garner DM, Raimundo RD, Abreu LCD, Navega MT, Valenti VE. Chaotic analysis of heart rate dynamics after an exercise with flexible pole. Med Express. (2016) 3:1–7. doi: 10.5935/MedicalExpress.2016.05.05
15. Fontes AMG, Garner DM, Abreu LCD, Barbosa JC, Assis EVD, Souza ACAD, et al. Global chaotic parameters of heart rate variability during mental task. Complexity. (2016) 21:300–7. doi: 10.1002/cplx.21656
16. Voss A, Kurths J, Kleiner H, Witt A, Wessel N, Saparin P. The application of methods of non-linear dynamics for the improved and predictive recognition of patients threatened by sudden cardiac death. Cardiovasc Res. (1996) 31:419–33. doi: 10.1016/S0008-6363(96)00008-9
17. Godoy M, Aniño M, Torres M. Análisis multifractal de la regulación autonómica del ritmo cardiaco en episodios isquémicos. Revista Argentina de Bioingeniería. (2003) 47:3100.
18. Takakura I, Godoy M. Variabilidade da frequência cardíaca no domínio do Caos como preditora morbimortalidade em pacientes submetidos à cirurgia de Revascularização do Miocárdio. São Paulo: Faculdade de medicina de São José do Rio Preto (2007).
19. Godoy MF Takakura IT Correa PR. Relevância da análise do comportamento dinâmico não linear (Teoria do Caos) como elemento prognóstico de morbidade e mortalidade em pacientes submetidos à cirurgia de revascularização miocárdica. Arq Ciênc Saúde. (2005) 12:167–71.
20. Schulz KF, Altman DG, Moher D. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. BMJ. (2010) 340:c332. doi: 10.1136/bmj.c332
21. Vignos PJ, Archibald KC. Maintenance of ambulation in childhood muscular dystrophy. J Chron Dis. (1960) 12:273–89. doi: 10.1016/0021-9681(60)90105-3
22. Souza DE, França FR, Campos TF. Teste de labirinto: instrumento de análise na aquisição de uma habilidade motora. Braz J Phys Ther. (2006) 10:355–60. doi: 10.1590/S1413-35552006000300016
23. Heart rate variability: standards of measurement physiological interpretation and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Circulation. (1996) 93:1043–65.
24. Alves M, Garner DM, Fontes AM, Sousa LVDA, Valenti VE. Linear and complex measures of heart rate variability during exposure to traffic noise in healthy women. Complexity. (2018) 2018:2158391. doi: 10.1155/2018/2158391
25. Peng CK, Havlin S, Stanley HE, Goldberger AL. Quantification of scaling exponents and crossover phenomena in nonstationary heartbeat time series. Chaos. (1995) 5:82–7. doi: 10.1063/1.166141
26. Anderson TW, Darling DA. A test of goodness of fit. J Am Statist Assoc. (1954) 49:765–9. doi: 10.1080/01621459.1954.10501232
27. Razali NM, Wah YB. Power comparisons of Shapiro-Wilk, Kolmogorov-Smirnov, Lilliefors and Anderson-darling tests. J Statist Model Analyt. (2011) 2:21–33.
28. Gastwirth JL, Gel YR, Miao W. The impact of Levene's test of equality of variances on statistical theory and practice. Statist Sci. (2009) 24:343–60. doi: 10.1214/09-STS301
29. Carroll RJ, Schneider H. A note on Levene's tests for equality of variances. Statist Probabil Lett. (1985) 3:191–4. doi: 10.1016/0167-7152(85)90016-1
30. Percival DB, Walden AT. Spectral Analysis for Physical Applications: Multitaper and Conventional Univariate Techniques. New York, NY: Cambridge University Press (1993).
31. Thomson DJ. Spectrum estimation and harmonic analysis. Proc IEEE. (1982) 70:1055–96. doi: 10.1109/PROC.1982.12433
32. Thomas TO, Jefferies JL, Lorts A, Anderson JB, Gao Z, Benson DW, et al. Autonomic dysfunction: a driving force for myocardial fibrosis in young duchenne muscular dystrophy patients? Pediatr Cardiol. (2015) 36:561–8. doi: 10.1007/s00246-014-1050-z
33. Dittrich S, Tuerk M, Haaker G, Greim V, Buchholz A, Burkhardt B, et al. Cardiomyopathy in duchenne muscular dystrophy: current value of clinical, electrophysiological and imaging findings in children and teenagers. Klinische Pädiatrie. (2015) 227:225–31. doi: 10.1055/s-0034-1398689
34. Gomes RL, Vanderlei LCM, Garner DM, de Abreu LC, Santana MDR, Raimundo RD, et al. Novel nonlinear method of heart rate variability analysis in exercise. Int J Clin Exp Med. (2016) 9:2047–56.
35. Fritz CO, Morris PE, Richler JJ. Effect size estimates: current use, calculations, and interpretation. J Exp Psychol Gen. (2012) 141:2–18. doi: 10.1037/a0024338
36. Luque-Casado A, Perales JC, C'ardenas D, Sanabria D. Heart rate variability and cognitive processing: the autonomic response to task demands. Biol Psychol. (2016) 113:83–90. doi: 10.1016/j.biopsycho.2015.11.013
37. Thayer JF, Lane RD. A model of neurovisceral integration in emotion regulation and dysregulation. J Affect Disord. (2000) 61:201–16. doi: 10.1016/S0165-0327(00)00338-4
38. Thayer JF, Lane RD. Claude Bernard and the heart–brain connection: further elaboration of a model of neurovisceral integration. Neurosci Biobehav Rev. (2009) 33:81–8. doi: 10.1016/j.neubiorev.2008.08.004
39. Vanderlei FM, Vanderlei LCM, Garner DM. Heart rate dynamics by novel chaotic globals to HRV in obese youths. J Hum Growth Dev. (2015) 25:82–8. doi: 10.7322/jhgd.96772
40. Yotsukura M, Fujii K, Katayama A, Tomono Y, Ando H, Sakata K, et al. Nine-year follow-up study of heart rate variability in patients with Duchenne-type progressive muscular dystrophy. Am Heart J. (1998) 136:289–96. doi: 10.1053/hj.1998.v136.89737
41. Yotsukura M, Sasaki K, Kachi E, Sasaki A, Ishihara T, Ishikawa K. Circadian rhythm and variability of heart rate in Duchenne-type progressive muscular dystrophy. Am J Cardiol. (1995) 76:947–51. doi: 10.1016/S0002-9149(99)80267-7
42. Voss A, Schulz S, Schroeder R, Baumert M, Caminal P. Methods derived from nonlinear dynamics for analysing heart rate variability. Philos Trans A Math Phys Eng Sci. (2009) 367:277–96. doi: 10.1098/rsta.2008.0232
43. de Godoy MF. Nonlinear analysis of heart rate variability: a comprehensive review. J Cardiol Ther. (2016) 3:528–33. doi: 10.17554/j.issn.2309-6861.2016.03.101-4
44. Vanderlei FM, Vanderlei LCM, Garner DM. Chaotic global parameters correlation with heart rate variability in obese children. Rev Bras Crescimento Desenvolv Hum. (2014) 24:24–30. doi: 10.7322/jhgd.72041
45. Slepian S. Prolate spheroidal wave functions, Fourier analysis, and uncertainty — V: the discrete case. Bell Syst Tech J. (1978) 57:1371–430. doi: 10.1002/j.1538-7305.1978.tb02104.x
46. Mackey MC, Milton JG. Dynamical diseases. Ann N Y Acad Sci. (1987) 504:16–32. doi: 10.1111/j.1749-6632.1987.tb48723.x
Keywords: heart rate variability, Duchenne Muscular Dystrophy, autonomic nervous system, Chaotic Global Techniques, health care technology
Citation: Alvarez MPB, Monteiro CBdM, Silva TDd, Valenti VE, Ferreira-Filho C, Sterr A, Vanderlei LCM, Ferreira C and Garner DM (2021) Autonomic Modulation in Duchenne Muscular Dystrophy During a Computer Task: A Prospective Transversal Controlled Trial Assessment by Non-linear Techniques. Front. Neurol. 12:720282. doi: 10.3389/fneur.2021.720282
Received: 04 June 2021; Accepted: 20 October 2021;
Published: 23 November 2021.
Edited by:
Alessio Baricich, Università degli Studi del Piemonte Orientale, ItalyReviewed by:
Claudio Molinari, University of Eastern Piedmont, ItalyCopyright © 2021 Alvarez, Monteiro, Silva, Valenti, Ferreira-Filho, Sterr, Vanderlei, Ferreira and Garner. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Talita Dias da Silva, dGFsaXRhLmRpYXNAdW5pZmVzcC5icg==
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.