
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
STUDY PROTOCOL article
Front. Neurol. , 09 August 2021
Sec. Neurogenetics
Volume 12 - 2021 | https://doi.org/10.3389/fneur.2021.710572
 Tatiana Usnich1
Tatiana Usnich1 Eva-Juliane Vollstedt1
Eva-Juliane Vollstedt1 Nathalie Schell1Volha Skrahina2
Nathalie Schell1Volha Skrahina2 Xenia Bogdanovic2Hanaa Gaber2Toni M. Förster2Andreas Heuer2Natalia Koleva-Alazeh3
Xenia Bogdanovic2Hanaa Gaber2Toni M. Förster2Andreas Heuer2Natalia Koleva-Alazeh3 Ilona Csoti3
Ilona Csoti3 Ayse Nazli Basak4Sibel Ertan5Gencer Genc6Peter Bauer2Katja Lohmann1
Ayse Nazli Basak4Sibel Ertan5Gencer Genc6Peter Bauer2Katja Lohmann1 Anne Grünewald7Emma L. Schymanski7
Anne Grünewald7Emma L. Schymanski7 Joanne Trinh1Susen Schaake1
Joanne Trinh1Susen Schaake1 Daniela Berg8
Daniela Berg8 Doreen Gruber9
Doreen Gruber9 Stuart H. Isaacson10
Stuart H. Isaacson10 Andrea A. Kühn11Brit Mollenhauer12
Andrea A. Kühn11Brit Mollenhauer12 David J. Pedrosa13
David J. Pedrosa13 Kathrin Reetz14Esther M. Sammler15
Kathrin Reetz14Esther M. Sammler15 Enza Maria Valente16Franco Valzania17
Enza Maria Valente16Franco Valzania17 Jens Volkmann18Simone Zittel19
Jens Volkmann18Simone Zittel19 Norbert Brüggemann1,20Meike Kasten1,21Arndt Rolfs2
Norbert Brüggemann1,20Meike Kasten1,21Arndt Rolfs2 Christine Klein1* and The LIPAD Study Group
Christine Klein1* and The LIPAD Study GroupBackground: Pathogenic variants in the Leucine-rich repeat kinase 2 (LRRK2) gene are the most common known monogenic cause of Parkinson's disease (PD). LRRK2-linked PD is clinically indistinguishable from idiopathic PD and inherited in an autosomal dominant fashion with reduced penetrance and variable expressivity that differ across ethnicities and geographic regions.
Objective: To systematically assess clinical signs and symptoms including non-motor features, comorbidities, medication and environmental factors in PD patients, unaffected LRRK2 pathogenic variant carriers, and controls. A further focus is to enable the investigation of modifiers of penetrance and expressivity of LRRK2 pathogenic variants using genetic and environmental data.
Methods: Eligible participants are invited for a personal or online examination which comprises completion of a detailed eCRF and collection of blood samples (to obtain DNA, RNA, serum/plasma, immune cells), urine as well as household dust. We plan to enroll 1,000 participants internationally: 300 with LRRK2-linked PD, 200 with LRRK2 pathogenic variants but without PD, 100 PD patients with pathogenic variants in the GBA or PRKN genes, 200 patients with idiopathic PD, and 200 healthy persons without pathogenic variants.
Results: The eCRF consists of an investigator-rated (1 h) and a self-rated (1.5 h) part. The first part includes the Movement Disorder Society Unified Parkinson's Disease Rating, Hoehn &Yahr, and Schwab & England Scales, the Brief Smell Identification Test, and Montreal Cognitive Assessment. The self-rating part consists of a PD risk factor, food frequency, autonomic dysfunction, and quality of life questionnaires, the Pittsburgh Sleep Quality Inventory, and the Epworth Sleepiness as well as the Hospital Anxiety and Depression Scales. The first 15 centers have been initiated and the first 150 participants enrolled (as of March 25th, 2021).
Conclusions: LIPAD is a large-scale international scientific effort focusing on deep phenotyping of LRRK2-linked PD and healthy pathogenic variant carriers, including the comparison with additional relatively frequent genetic forms of PD, with a future perspective to identify genetic and environmental modifiers of penetrance and expressivity
Clinical Trial Registration: ClinicalTrials.gov, NCT04214509.
Pathogenic variants in the Leucine-rich repeat kinase 2 (LRRK2) gene are the most common known monogenic cause of Parkinson's disease (PD). First identified in 2004, LRRK2 pathogenic variants account for up to ~40% of all PD cases in selected populations, e.g., North African Berber (1). In the PD phenotype-genotype database MDSGene (www.mdsgene.org), ~700 individual LRRK2 pathogenic variant carriers are listed, but clinical information apart from cardinal signs of PD is overall scarce (1).
The majority of the reported LRRK2 pathogenic variant-positive PD patients are of European descent (63%), whereas all other ethnicities comprise ~10% or fewer patients of described pathogenic variant carriers despite clusters in the Ashkenazi Jewish (AJ) and Arab Berber populations (1, 2). Definitely pathogenic variants identified in LRRK2 include p.G2019S, p.R1441C/G/H, p.N1437H, p.Y1699C, and, p.I2020T. Of these, the p.G2019S pathogenic variant is the most common with an estimated frequency of 1% in sporadic and 4% in hereditary PD cases worldwide (3). However, data on many populations are still missing.
LRRK2-linked PD is inherited in an autosomal dominant fashion with reduced, age-dependent penetrance and variable expressivity that differ across ethnicities and geographic regions, indicating that ancestral background or environmental factors contribute to the manifestation and expressivity of pathogenic LRRK2 variants. For example, at the age of 60 years, 60% of Tunisian p.G2019S pathogenic variant carriers manifest PD, compared with only 20% of the Norwegian carriers of the same pathogenic variant (4). Recent studies have suggested mitochondrial involvement in the penetrance of LRRK2-linked PD (5, 6). Environmental factors can also influence penetrance, as recently found in the Tunisian Arab Berber population, where tobacco and black tea use delayed age at onset in LRRK2 pathogenic variant carriers (7).
LRRK2-linked PD is clinically indistinguishable from idiopathic PD, i.e., PD of unknown cause, although the disease course appears to be milder with regard to motor and cognitive functions (8). In this comparatively small subgroup of PD patients with a known etiology, valuable clues can be garnered toward pathophysiological mechanisms and targeted treatments, which may be generalized to idiopathic PD. Currently, there are three substances in clinical trial specifically targeting LRRK2: the LRRK2 kinase inhibitors DNL151 (NCT04557800) and DNL201 (NCT04551534) from Denali and the antisense oligonucleotide BIIB094 (NCT03976349) from Biogen (2). However, no genetic testing guidelines and no clinical trial-ready cohorts exist to date.
To identify LRRK2 pathogenic variant carriers among 10,000 PD patients from 15 countries and to establish a clinical trial-ready cohort, the ROPAD study was initiated (9). The ROPAD study performs genetic testing of pathogenic variants in the LRRK2 and GBA genes and, if negative, carries out genetic screening of 68 genes linked to PD or related movement disorders. Out of the first 1,288 participants who underwent genetic testing in ROPAD, 40 (3.1%) harbored pathogenic or likely pathogenic LRRK2 variants, 109 (8.5%) harbored GBA variants, three (0.2%) had alterations in both genes (9). The ROPAD study is still ongoing and continues to identify LRRK2 pathogenic variant carriers internationally. It gathers only basic clinical data: age at examination, age at onset, cardinal PD symptoms, and 12/33 items of MDS-UPDRS Part III and, thus, does not allow a systematic in-depth characterization of LRRK2 pathogenic variant carriers.
Recently published data from the currently largest multinational prospective study that includes LRRK2 pathogenic variant carriers, i.e., the Parkinson's Progression Markers Initiative (PPMI), provide more phenotypic details on LRRK2 pathogenic variant carriers across international sites (6). However, as the focus of the PPMI study is predominantly on biomarkers, it does not cover environmental factors in-depth, and only includes participants with a PD diagnosis 2 years or less before enrolment who are untreated with PD medication. There remains a gap in combining phenotypic, genetic, and environmental data on LRRK2 pathogenic variant carriers internationally, regardless of the onset of signs and symptoms and their medication status, that LIPAD is aiming to close. The objectives of the LIPAD study are (1) to provide a systematic characterization of PD patients and unaffected carriers with pathogenic variants in the LRRK2 gene; and (2) to enable the investigation of modifiers of penetrance of LRRK2 pathogenic variants using genetic and environmental data.
Here, we describe a protocol and a feasibility study of the first 150 participants and give a brief overview of nested studies within LIPAD. Of note, the LIPAD protocol has also been adapted to take place online due to COVID19 contact restriction measures.
We aim to build the LIPAD cohort consisting of 1,000 participants internationally: 300 of them with LRRK2-PD (LRRK2+/PD+), 200 with pathogenic LRRK2 variants but without PD (LRRK2+/PD-), 100 PD patients with pathogenic variants in PD genes other than LRRK2 (genPD), 200 patients with idiopathic PD from the same populations (iPD; LRRK2-/PD+), and 200 healthy persons without pathogenic variants (HC). The majority of participants will be enrolled after genetic analysis within ROPAD (Figure 1). Extrapolating from the ROPAD findings, we expect to have a sufficient number of participants in the LRRK2+/ PD+, iPD, and genPD groups. Further, family members of pathogenic LRRK2 variant carriers will be asked to participate in the LIPAD study and will be genetically tested for the familial pathogenic LRRK2 variant. Depending on the results, they will be assigned either to LRRK2+/PD- or HC group. Healthy persons without pathogenic variants will be recruited from spouses of study participants or the general population. Within an anticipated 24-month recruitment period per site, ~25 centers in 10 countries on three continents will be established. Each center will have 24 months for recruitment after initiation. The majority of the centers will be those already participating in ROPAD, however, additional centers that do not participate in ROPAD but follow LRRK2 pathogenic variant carriers will be invited to become LIPAD sites.
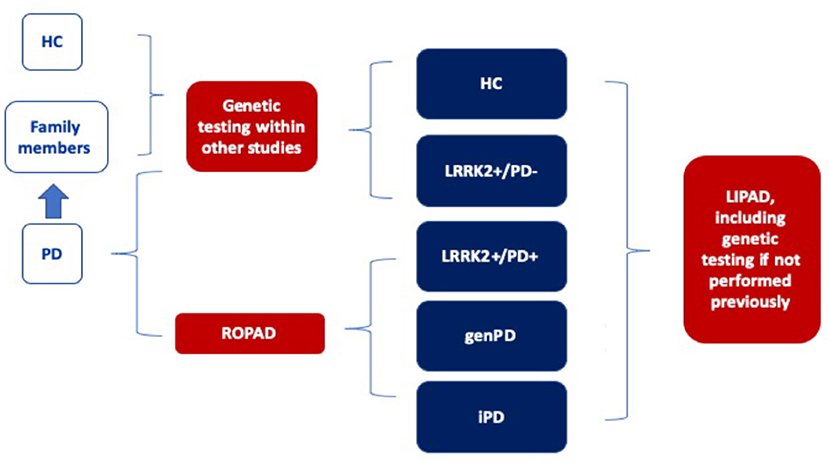
Figure 1. Paths of enrolment into the LIPAD study. LRRK2+/PD+: PD patients carrying a pathogenic LRRK2 variant, LRRK2+/PD-: unaffected carriers of pathogenic LRRK2 variants, genPD: PD patients with pathogenic variants in PD genes other than LRRK2, iPD; LRRK2-/PD+: patients with idiopathic PD from the same populations, HC: healthy persons without pathogenic variants.
Recruited participants have to meet one of the following criteria: (i) clinical diagnosis of PD according to the Movement disorder Society (MDS) diagnostic criteria, (ii) first- or second-degree relative of a participant that is positive for a pathogenetic LRRK2 variant, (iii) healthy participants with or without a family history of PD in a control group. All participants have to be above 18 years of age and have to sign an informed consent form.
Participants with the following LRRK2 variants will be included in the LRRK2+ group: p.Gly2019Ser (c.6055G>A), p.Arg1441His (c.4322G>A), p.Arg1441Cys (c.4321C>T), p.Arg1441Gly (c.4321C>G), p.Asn1437His (c.4309A>C), p.Ile2020Thr (c.6059T>C), p.Tyr1699Cys (c.5096A>G).
Upon completion of genetic screening (e.g., in ROPAD), participants are invited for a personal examination using the three-level biomaterial protocol. During a single visit, an electronic Case Report Form (eCRF) is administered and blood samples for DNA, RNA, serum/plasma, immune cell isolation, urine, and household dust for toxicological analyses are collected.
The three-level protocol was designed to accommodate available laboratory facilities at the different sites. The details of the three levels for biomaterial sampling are listed in Supporting Information Methods S2 in Supplementary Material.
In case genetic testing has not been performed before, a dried blood spot card will be sent for DNA extraction and genetic screening, as specified in ROPAD.
There are no serious safety concerns associated with the study. Participants may experience temporary discomfort during venous blood sampling and while answering the questions. However, they are instructed that they are free to omit questions they would rather not answer. There are no health risks associated with the collection of urine and house dust.
Data analysis will be performed at the Institute of Neurogenetics (University of Luebeck, Germany). To cover the first objective, which is the systematic characterization of PD patients and unaffected carriers with pathogenic variants in the LRRK2 gene, we will describe the frequency of all clinical signs and symptoms including non-motor signs and the most important influencing factors such as sex, disease duration, and medication. This will result in raw and corrected frequencies with 95% confidence intervals. We will use t-tests for numerical and continuous variables and chi-square tests for categorical variables at a significance level of 0.05 for the comparisons of the clinical signs and symptoms across the groups.
For aim 2, which is to investigate the modifiers of penetrance of pathogenic LRRK2 variants using genetic and environmental data, we will examine penetrance in logistic regression models to quantify the influence of different factors impacting penetrance.
All LIPAD centers can suggest nested projects, which will be coordinated by a Scientific Advisory Board. These projects can apply for external funding, will have individual ethics approvals, and can use the ROPAD/LIPAD network. The following nested studies are planned or have started at the Institute of Neurogenetics (University of Luebeck):
Penetrance of LRRK2-linked PD depends on the age of a given individual subject. Asymptomatic carriers may, however, already demonstrate neurodegenerative changes including hyposmia, abnormal midbrain hyperechogenicity upon transcranial sonography, pathologic dopaminergic neurotransmission, structural changes of the gray and white matter, and functional reorganization of neural networks. Although first morphological and functional brain changes in pathogenic LRRK2 variant carriers have already been identified, the overall picture is still elusive due to the relatively low number of included subjects in most studies, ascertainment biases, and variable imaging protocols. Multimodal high-quality MRI, however, is a promising secondary endpoint for clinical trials given its wide availability, cost-effectiveness, and lack of radiation.
To reveal an MRI-based biomarker for LRRK2+/PD+ and prodromal LRRK2+/PD+, we aim to acquire the following MRI modalities:
1. Multiparameter mapping (R1, PD*, MT, and R2*) to reveal physical tissue properties.
2. Diffusion-weighted imaging for multicompartment diffusion models to reveal neuroinflammation and microstructural alterations.
3. Neuromelanin imaging to reveal substantia nigra and locus coeruleus degeneration.
4. Blood-oxygen-level-dependent functional MRI to identify changes in functional connectivity.
5. Magnetic resonance spectroscopy to depict the mechanisms of neurodegeneration, such as involvement of energy metabolism due to mitochondrial dysfunction, which may be subject to faster change than other aspects of MR-based imaging (e.g., changes in gray matter).
To investigate whether metabolic changes in LRRK2 carriers already exist before the motor manifestation or are secondary to it, we conduct the following studies:
1. Energy consumption at rest using indirect calorimetry, where energy consumption is determined by measuring the air the subject breathes.
2. Measurement of body composition, i.e., the proportion of body fat mass and lean mass, employing air displacement plethysmography. In addition, body circumference (e.g., waist and hips) and body skin folds (e.g., on the arm and waist) are measured.
3. Measurement of physical activity and sleep behavior under everyday conditions using accelerometry. The study participants are asked to wear the accelerometer in the form of a wristwatch continuously for 7 days.
We will perform a genome-wide association study analysis in manifesting vs. non-manifesting carriers aimed at discovering genetic modifiers of penetrance of LRRK2 pathogenic variants.
A broad non-target liquid chromatography high-resolution mass spectrometry (LC-HR-MS) screening will be performed on household dust samples collected by participants in vacuum bags [see (10)], with identification of potential toxicants of interest via the in silico fragmenter MetFrag (11) coupled with open chemical databases such as PubChem (12) and CompTox (13), plus specific neurotoxicity-related candidate lists and end-point information (14).
A comprehensive eCRF has been developed, consisting of an investigator-rated (1 h) and a self-rated (1.5-h) part. The questionnaires are listed in Table 1. We used validated versions of questionnaires and scales in the local languages.
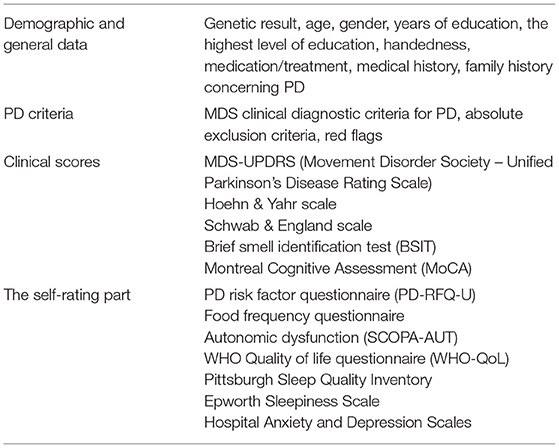
Table 1. Content of the LIPAD electronic case report form.
The first 10 centers across Germany and five international sites have been initiated with further centers currently undergoing ethical review (Figure 2). The first 150 participants have been enrolled (as of March 25th, 2021); Table 2.
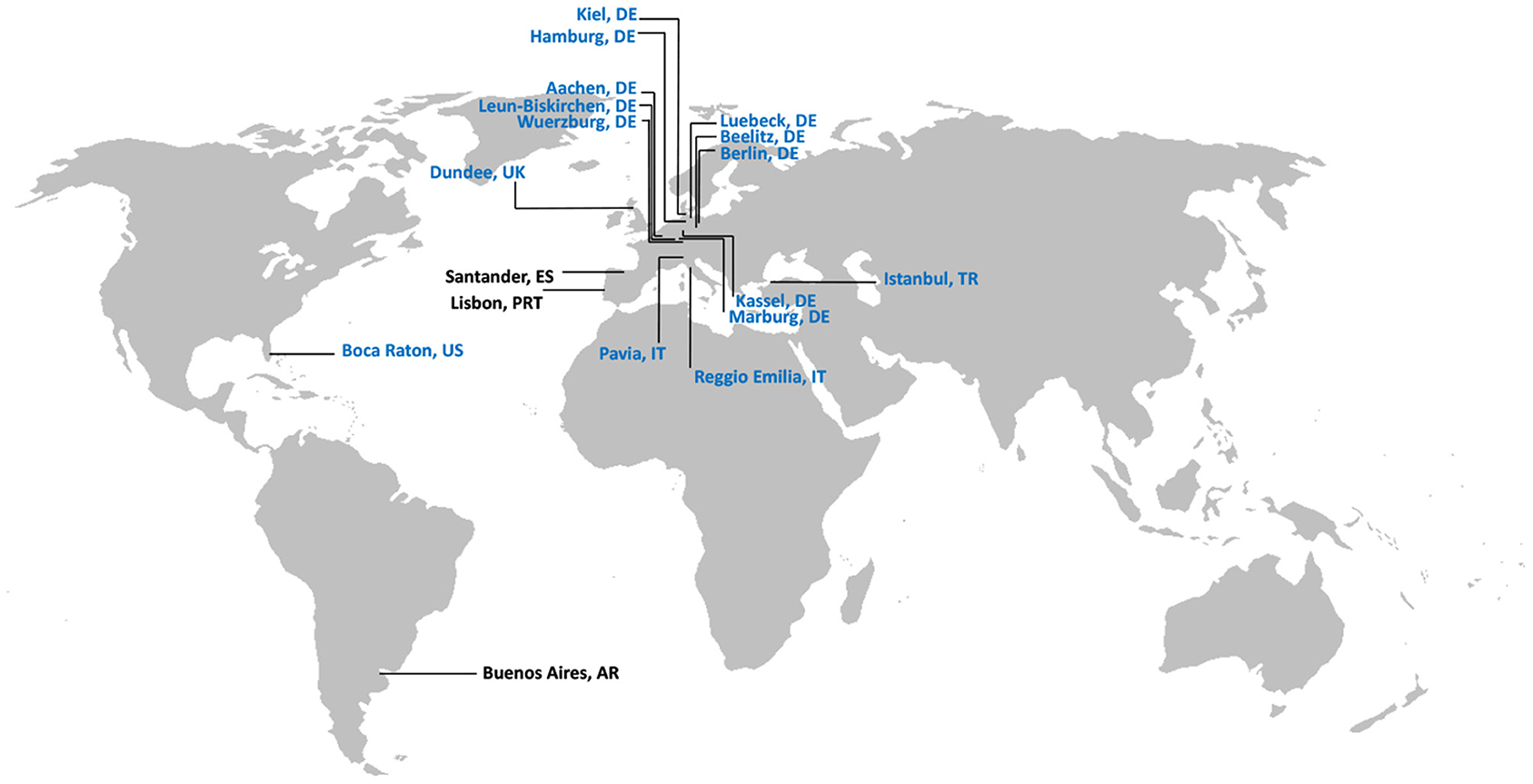
Figure 2. International centers participating in LIPAD. In blue: centers with ethics approval; in black: centers in the process of receiving ethics approval.
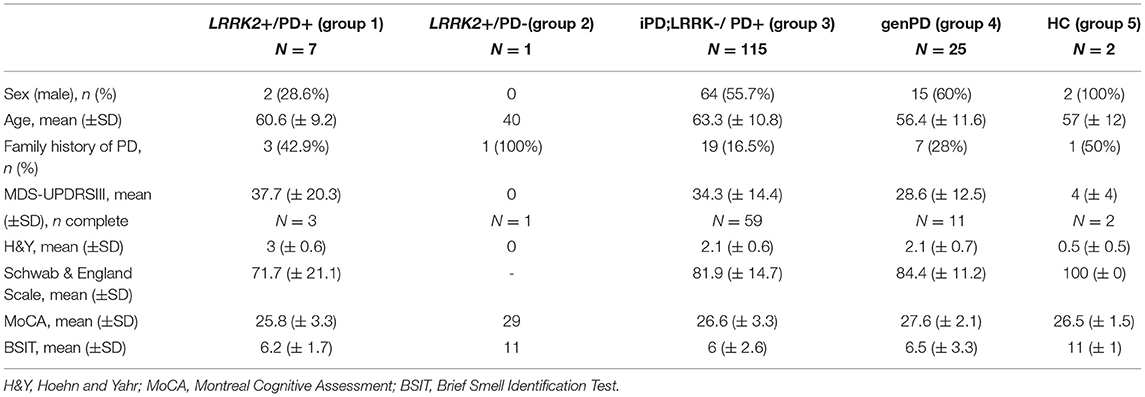
Table 2. Exemplary demographic and clinical characteristics of the first 150 enrolled LIPAD participants.
LIPAD is a large-scale international scientific effort focusing on deep phenotyping of LRRK2-linked PD and healthy pathogenic variant carriers, including a comparison with additional relatively frequent genetic forms of PD, and with a future perspective to identify genetic and environmental modifiers of penetrance and expressivity.
The clinical assessment in LIPAD is close to the one used in the currently largest multinational cohort of genetic PD (PPMI), except for lack of collection of cerebrospinal fluid, but with the addition of an extensive questionnaire on environmental factors (15). Further, there are no restrictions on the age at diagnosis or medication for inclusion in the LIPAD study. Several other multinational prospective studies focusing on pathogenic LRRK2 variants included only a small number of populations (4, 16, 17), revealing an important knowledge gap in multinational, standardized, genetic prospective studies, which LIPAD is aiming to close.
A comprehensive investigation of modifiers of penetrance and expressivity requires assessment of a considerable number of pathogenic variant carriers. Due to the direct enrolment of family members at an international scale, the LIPAD study will enable the analysis of modifiers of penetrance in different populations in one setting. Our recruitment strategy, mainly through the international multicenter ROPAD study, will ensure participation of a large number of LRRK2+/PD+ patients.
With the nested studies, which will be conducted on a subset of participants, we are aiming to provide a more in-depth phenotypic characterization especially of non-affected carriers of LRRK2 pathogenic variants.
Currently, a complication affecting many patient studies across the world are measures imposed on personal visits to contain SARS-CoV-2 in many countries, limiting the possibility for the collection of data and biomaterials. To allow the study to proceed under these circumstances, we adjusted the protocol and procedures to collect the necessary data online. After making an online appointment, patients receive a package with patient information, informed consent forms, and a smell test by post. Then an online appointment with the study team takes place, during which the study is explained, the data is collected and the examination is performed. Study participants send signed informed consent forms and a household dust sample back to the study center by post. Biomaterials will be taken at a general practitioner's office or the study center at a later time point when study visits become possible again. The study will revert to the on-site recruitment as soon as possible after the pandemic restrictions are lifted.
LIPAD aims for a longitudinal follow-up of its study participants over a 10–15-year time period. The exact protocol is currently being developed and potential funding opportunities are being explored.
The studies involving human participants were reviewed and approved by Ethics Committee (EC) of the University of Lübeck (19-065); EC LÄK Hessen (2019-1364-zvBO); EC LÄK Hamburg (MC-002/20); EC LÄK Brandenburg [AS 35(bB)/2020]; EC Würzburg (161/19_z-sc); EC Kiel (B 292/19); EC Marburg (111/20); EC UK IRAS (project ID: 275553, REC reference: 20/NE/011); EC USA IRB tracking number: 20193494; Pavia, Italy (20200048346); Reggio Emilia, Italy (1268/2020/OSS/AUSLRE); Istanbul, Turkey (2020.362.IRB1.144). The patients/participants provided their written informed consent to participate in this study.
Daniela Berg, University Hospital Schleswig-Holstein, Kiel, Germany; Leonor Correia Guedes, Hospital de Santa Maria, Lisbon, Portugal; Ilona Csoti, Natalia Koleva-Alazeh, Gertrudis-Kliniken im Parkinson-Zentrum, Leun-Biskirchen, Germany; Georg Ebersbach, Doreen Gruber, Neurologisches Fachkrankenhaus für Bewegungsstörungen/Parkinson, Beelitz-Heilstätten, Germany; Sibel Ertan, Özgür Öztop Çakmak, Department of Neurology, Koç University School of Medicine, Istanbul, Turkey; Jon Infante, University Hospital Marqués de Valdecilla, Santander, Spain; Stuart Isaacson, Parkinson's Disease and Movement Disorder Center of Boca Raton, Boca Raton, U.S.A.; Christine Klein, Universität zu Lübeck, Lübeck, Germany; Andrea A. Kühn, Friederike Borngräber, Charité University Medicine Berlin, Berlin, Germany; Marcello Merello, Malco Rossi, FLENI Foundation, Buenos Aires, Argentina; Brit Mollenhauer, Paracelsus-Elena-Klinik, Kassel, Germany; David J. Pedrosa, University Hospital Marburg, Marburg, Germany; Kathrin Reetz, University Hospital RWTH Aachen, Aachen, Germany; Esther Sammler, University of Dundee, Dundee, Scotland, UK; Enza Maria Valente, Department of Molecular Medicine, University of Pavia and IRCCS Mondino Foundation, Pavia, Italy; Micol Avenali, IRCCS Mondino Foundation, Neurorehabilitation Unit, Department of Brain and Behavioral Sciences, University of Pavia, Pavia, Italy; Franco Valzania, Giulia Toschi, Francesco Cavallieri, Azienda USL – IRCCS, Reggio Emilia, Italy; Jens Volkmann, University Hospital Würzburg, Würzburg, Germany; Simone Zittel, Lisa Prilop, University Medical Center Hamburg-Eppendorf, Hamburg, Germany.
TU: organization and execution of the research project, design and execution of statistical analysis, and writing the first draft of the manuscript. E-JV and AR: conception and organization of the research project, review and critique of statistical analysis, and review and critique of the manuscript. NS and SS: organization and execution of the research project, review and critique of statistical analysis, and review and critique of the manuscript. VS, XB, HG, TF, AH, NK-A, IC, DG, ESa, EV, FV, SZ, AB, SE, and GG: organization of the research project, review and critique of statistical analysis, and review and critique of the manuscript. PB, AG, ESc, JT, DB, SI, AK, BM, DP, and JV: review and critique of statistical analysis and review and critique of the manuscript. KL: organization of the research project and review and critique of the manuscript. NB, MK, and CK: conception and organization of the research project, design and review and critique of statistical analysis, and review and critique of the manuscript. All authors contributed to the article and approved the submitted version.
The LIPAD study has been supported by institutional funds (Institute of Neurogenetics, University of Lübeck), and partly supported by Centogene GmbH. AB (NDAL) was funded by Suna and Inan Kirac Foundation, grant no 2018-2020. ESc was supported by the Luxembourg National Research Fund (FNR) for project A18/BM/12341006.
VS, XB, HG, TF, AH, PB, and AR were employed by company CENTOGENE GmbH. The authors declare that this study received funding from Centogene GmbH. The funder was involved in the study design, organization of the research project and review and critique of the manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
AB is grateful to Suna and Inan Kirac Foundation for their sustained support and both to the Foundation and Koç University-KUTTAM for the excellent research environment created. ESc acknowledges the efforts of Begoña Talavera.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2021.710572/full#supplementary-material
1. Trinh J, Zeldenrust FMJ, Huang J, Kasten M, Schaake S, Petkovic S, et al. Genotype-phenotype relations for the Parkinson's disease genes SNCA, LRRK2, VPS35: MDSGene systematic review. Mov Disord. (2018) 33:1857–70. doi: 10.1002/mds.27527
2. Tolosa E, Vila M, Klein C, Rascol O. LRRK2 in Parkinson disease: challenges of clinical trials. Nat Rev Neurol. (2020) 16:97–107. doi: 10.1038/s41582-019-0301-2
3. Healy DG, Falchi M, O'Sullivan SS, Bonifati V, Durr A, Bressman S, et al. Phenotype, genotype, and worldwide genetic penetrance of LRRK2-associated Parkinson's disease: a case-control study. Lancet Neurol. (2008) 7:583–90. doi: 10.1016/S1474-4422(08)70117-0
4. Hentati F, Thompson C, Nosova E, Farrer MJ, Aasly JO. LRRK2 parkinsonism in Tunisia and Norway: a comparative analysis of disease penetrance. Neurology. (2014) 83:568–9. doi: 10.1212/WNL.0000000000000675
5. Ouzren N, Delcambre S, Ghelfi J, Seibler P, Farrer MJ, König IR, et al. Mitochondrial DNA deletions discriminate affected from unaffected LRRK2 mutation carriers. Ann Neurol. (2019) 86:324–6. doi: 10.1002/ana.25510
6. Delcambre S, Ghelfi J, Ouzren N, Grandmougin L, Delbrouck C, Seibler P, et al. Mitochondrial mechanisms of LRRK2 G2019S penetrance. Front Neurol. (2020) 11:881. doi: 10.3389/fneur.2020.00881
7. Lüth T, König IR, Grünewald A, Kasten M, Klein C, Hentati F, et al. Age at onset of LRRK2 p.Gly2019Ser is related to environmental and lifestyle factors. Mov Disord. (2020) 35:1854–8. doi: 10.1002/mds.28238
8. Saunders-Pullman R, Mirelman A, Alcalay RN, Wang C, Ortega RA, Raymond D, et al. Progression in the LRRK2-asssociated Parkinson disease population. JAMA Neurol. (2018) 75:312–9. doi: 10.1001/jamaneurol.2017.4019
9. Skrahina V, Gaber H, Usnich T, Curado F, Bogdanovic X, Zülbahar S. The rostock international Parkinson's disease (ROPAD) study : protocol and initial findings. Mov Disord. (2020) 36:1005–10. doi: 10.1002/mds.28416
10. Rostkowski P, Haglund P, Aalizadeh R, Alygizakis N, Thomaidis N, Arandes JB, et al. The strength in numbers: comprehensive characterization of house dust using complementary mass spectrometric techniques. Anal Bioanal Chem. (2019) 411:1957–77. doi: 10.1007/s00216-019-01615-6
11. Ruttkies C, Schymanski EL, Wolf S, Hollender J, Neumann S. MetFrag relaunched: incorporating strategies beyond in silico fragmentation. J Cheminform. (2016) 8:1–16. doi: 10.1186/s13321-016-0115-9
12. Kim S, Chen J, Cheng T, Gindulyte A, He J, He S, et al. PubChem in 2021: new data content and improved web interfaces. Nucleic Acids Res. (2021) 49:D1388–95. doi: 10.1093/nar/gkaa971
13. Williams AJ, Grulke CM, Edwards J, McEachran AD, Mansouri K, Baker NC, et al. The compTox chemistry dashboard: a community data resource for environmental chemistry. J Cheminform. (2017) 9:1–27. doi: 10.1186/s13321-017-0247-6
14. Schymanski EL, Baker NC, Williams AJ, Singh RR, Trezzi JP, Wilmes P, et al. Connecting environmental exposure and neurodegeneration using cheminformatics and high resolution mass spectrometry: potential and challenges. Environ Sci Process Impacts. (2019) 21:1426–45. doi: 10.1039/C9EM00068B
15. Simuni T, Brumm MC, Uribe L, Caspell-Garcia C, Coffey CS, Siderowf A, et al. Clinical and dopamine transporter imaging characteristics of leucine rich repeat kinase 2 (LRRK2) and glucosylceramidase beta (GBA) Parkinson's disease participants in the parkinson's progression markers initiative: a cross-sectional study. Mov Disord. (2020) 35:833–44. doi: 10.1002/mds.27989
16. Marder K, Wang Y, Alcalay RN, Mejia-Santana H, Tang MX, Lee A, et al. Age-specific penetrance of LRRK2 G2019S in the Michael J. Fox Ashkenazi Jewish LRRK2 consortium. Neurology. (2015) 85:89–95. doi: 10.1212/WNL.0000000000001708
Keywords: Parkinson's disease, LRRK2, GBA, clinical study, genetic cohort
Citation: Usnich T, Vollstedt E-J, Schell N, Skrahina V, Bogdanovic X, Gaber H, Förster TM, Heuer A, Koleva-Alazeh N, Csoti I, Basak AN, Ertan S, Genc G, Bauer P, Lohmann K, Grünewald A, Schymanski EL, Trinh J, Schaake S, Berg D, Gruber D, Isaacson SH, Kühn AA, Mollenhauer B, Pedrosa DJ, Reetz K, Sammler EM, Valente EM, Valzania F, Volkmann J, Zittel S, Brüggemann N, Kasten M, Rolfs A, Klein C and The LIPAD Study Group (2021) LIPAD (LRRK2/Luebeck International Parkinson's Disease) Study Protocol: Deep Phenotyping of an International Genetic Cohort. Front. Neurol. 12:710572. doi: 10.3389/fneur.2021.710572
Received: 16 May 2021; Accepted: 13 July 2021;
Published: 09 August 2021.
Edited by:
Ignacio Mata, Cleveland Clinic, United StatesReviewed by:
Vitor Tumas, University of Ribeirão Preto, BrazilCopyright © 2021 Usnich, Vollstedt, Schell, Skrahina, Bogdanovic, Gaber, Förster, Heuer, Koleva-Alazeh, Csoti, Basak, Ertan, Genc, Bauer, Lohmann, Grünewald, Schymanski, Trinh, Schaake, Berg, Gruber, Isaacson, Kühn, Mollenhauer, Pedrosa, Reetz, Sammler, Valente, Valzania, Volkmann, Zittel, Brüggemann, Kasten, Rolfs, Klein and The LIPAD Study Group. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Christine Klein, Y2hyaXN0aW5lLmtsZWluQG5ldXJvLnVuaS1sdWViZWNrLmRl
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.