
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Neurol. , 25 August 2021
Sec. Dementia and Neurodegenerative Diseases
Volume 12 - 2021 | https://doi.org/10.3389/fneur.2021.683131
This article is part of the Research Topic Dementia in Low and Middle Income Countries View all 37 articles
 Magda Tsolaki1,2,3,4
Magda Tsolaki1,2,3,4 Marianna Tsatali1*
Marianna Tsatali1* Mara Gkioka1,2
Mara Gkioka1,2 Eleni Poptsi1
Eleni Poptsi1 Anthoula Tsolaki1,2
Anthoula Tsolaki1,2 Vasileios Papaliagkas1,5
Vasileios Papaliagkas1,5 Irene-Maria Tabakis1
Irene-Maria Tabakis1 Ioulietta Lazarou2
Ioulietta Lazarou2 Marina Makri1,2
Marina Makri1,2 Dimitrios Kazis4Sotirios Papagiannopoulos4
Dimitrios Kazis4Sotirios Papagiannopoulos4 Andreas Kiryttopoulos2Efrosyni Koutsouraki2Thomas Tegos2
Andreas Kiryttopoulos2Efrosyni Koutsouraki2Thomas Tegos2Background: This review describes the diagnostic and interventional procedures conducted in two university memory clinics (established network of G. Papanikolaou Hospital: 1988–2017 and AHEPA hospital: 2017–today) and 2 day care centers (established network of DCCs: 2005–today) in North Greece and their contribution in the scientific field of dementia. The aims of this work are (1) to provide a diagnosis and treatment protocol established in the network of memory clinics and DCCs and (2) to present further research conducted in the aforementioned network during the last 30 years of clinical practice.
Methods: The guidelines to set a protocol demand a series of actions as follows: (1) set the diagnosis criteria, neuropsychological assessment, laboratory examinations, and examination of neurophysiological, neuroimaging, cerebrospinal fluid, blood, and genetic markers; and (2) apply non-pharmacological interventions according to the needs and specialized psychosocial interventions of the patient to the caregivers of the patient.
Results: In addition to the guidelines followed in memory clinics at the 1st and 3rd Department of Neurology and two DCCs, a database of patients, educational programs, and further participation in international research programs, including clinical trials, make our contribution in the dementia field strong.
Conclusion: In the current paper, we provide useful guidelines on how major and minor neurocognitive disorders are being treated in Thessaloniki, Greece, describing successful practices which have been adapted in the last 30 years.
Dementia has been described as a clinical syndrome caused by neurodegeneration (Alzheimer's disease, Lewy body, and frontotemporal dementia being the most common pathologies) or as a secondary syndrome (vascular, metabolic, hormonal, and infectious dementia), characterized by progressive deterioration in cognitive ability, behavior, and capacity for independent living (1). Typically, it is a condition that usually affects older people (2, 3). Because of a longer life expectancy along with the lack of efficient therapeutic strategies, dementia is increasingly becoming a major public health problem. According to Alzheimer Disease International, it has been estimated that 35.6 million people were living with dementia worldwide in 2010, with the numbers expected to almost double every 20 years up to 65.7 million in 2030 (1). In Greece, there are almost 196,000 people living with dementia, while in 2050 this number is going to increase to 356,000. Moreover, family caregivers are estimated at 400,000 all over the country. Few studies have been conducted so far concerning the prevalence of dementia and mild cognitive impairment (MCI) in Greece (4–7), but the latest data revealed that the overall prevalence of dementia is 5.0%, with 75.3% of the cases attributed to Alzheimer's disease (8).
Thessaloniki, located in northern Greece, is the second biggest city of the country with high contribution in dementia research and clinical practice. The memory and dementia network in Thessaloniki, which started with the so-called Outpatient Memory and Dementia Clinic (3rd Department of Neurology), which was established in 1988 at “G. Papanikolaou” General Hospital (established network 1988–2017). Years later and specifically in 1995, Professor Magda Tsolaki, with the cooperation of dementia experts, founded the Association of Alzheimer's Disease and Related Disorders (GAADRD) which is responsible for 2 day care centers (DCCs) in Thessaloniki. Since 2005, the team of experts had the opportunity to expand the network and establish in total four DCCs in several cities across Greece (Thessaloniki, Volos, Chania, and Athens). At the end of 2017, the memory and dementia network was established to the Outpatient Memory and Dementia clinic (1st Department of Neurology) at “AHEPA” University Hospital till today. The aforementioned network between memory clinics and DCCs offer medical treatment, psychological support, and non-pharmaceutical interventions to beneficiaries who range from no cognitive impairment (NCI), subjective cognitive impairment (SCI), MCI, and dementia. Additionally, many projects and clinical trials are also being implemented with the collaboration of several dementia scientists abroad. Moreover, a large electronic database containing the information of all patients has been developed for clinical purposes. Consequently, the memory and dementia network provides high-quality diagnostic, treatment, and support services to individuals affected by major or minor neurocognitive impairment and their caregivers or family members in North Greece. Given that this initiative constitutes a significant part of global research groups, the memory and dementia network works in line with high standards provided worldwide.
The goals of this work are (1) to provide a diagnosis and treatment protocol established in memory clinics and DCCs and (2) to present further research conducted in the last 30 years of clinical practice.
The current memory clinic network includes the outpatient memory clinic of a university general hospital (AHEPA), where the initial diagnosis and follow-up assessments patients as well as education of students, including academic lectures and staff meetings, take place. The outpatient clinic operates once per week under the umbrella of the general hospital and health ministry. It consisted of a neurologist, nurses, medical students, and psychologists offering services of full screening, diagnosis, and medical treatment. Patients who visit the memory clinic, for any reason, follow the screening/diagnostic protocol, and after giving out the results and prescription of medication, they are recommended to visit a DCC for further benefits according to their needs, such as non-pharmaceutical interventions. Moreover, the research and academic team developed a new postgraduate program in 2020 (master's degree) entitled “Neuroscience and Neurodegenerative Diseases,” and therefore professionals who work on the dementia field provide new treatment horizons both in beneficiaries as well as in the research field.
GAADRD is a non-governmental organization and member of European as well as international organizations such as Alzheimer Europe and Alzheimer Disease International. It consists of neurologists, psychiatrists, general practitioner, psychologists, biologists, social workers, physical trainers, physiotherapists, and nurses who have been specially trained and educated. The DCCs under the umbrella of GAADRD are prototype and perfectly organized centers offering diagnosis and several non-pharmacological programs for the beneficiaries, namely: (a) programs of cognitive training for people with MCI and people with dementia (PwD) of first stages and (b) cognitive stimulation programs for people with mild and moderate stage of dementia. The participants attend cognitive training or stimulation programs for one or several days per week, following a protocol according to their needs, such as cognitive deficits, mood disorders, and functionality problems. The entrance to the group is determined by a psychologist who is an expert in non-pharmaceutical programs. Each program duration is almost a year. Furthermore, there are also prevention programs to minimize the conversion of SCI to MCI and dementia as well as those delivered to NCI healthy older adults who are at risk of developing dementia due to family history or other relevant health problems. Furthermore, psychotherapeutic programs are also provided to caregivers in order to support them during their caregiving role. Additionally, in the last 15 years, 1-h lectures are conducted every week, including the most recent developments in the research of neurodegenerative diseases as well as many educational projects for caregivers all over Greece. Finally, GAADRD has organized 12 national conferences, one Alzheimer Europe Conference (2003), and one Alzheimer Disease Conference (2010). GAADRD also contributed to the national observatory for dementia in Greece (2013) and one Satellite AAIC Athens Conference (2021) and has also organized DCCs all over Greece and Egypt. Since 2001, GAADRD has been a member of the European Alzheimer Disease Consortium (EADC).
The diagnostic procedure officially takes place in DCCs or in outpatient memory clinics. All patients who visit the outpatient memory clinics are screened for cognitive deficits with a neuropsychological battery (Tables 1, 2), while laboratory examinations, neurophysiological and neuroimaging examination, and genetic markers are also conducted (Table 3). The memory clinic's services are used as “a hub” of patients diagnosed with a cognitive disorder. Subsequently, some of them, if they need it, are referred to DCCs for further neuropsychological assessments (Table 2) and psychological support and to attend non-pharmaceutical programs. Vice versa, patients who visit a DCC for the first time after diagnosis may visit the memory clinic to undertake specialized examinations.
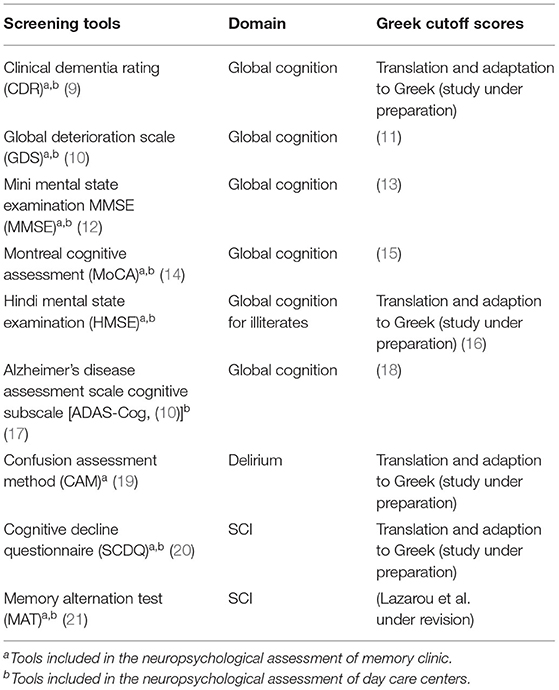
Table 1. Screening tools.
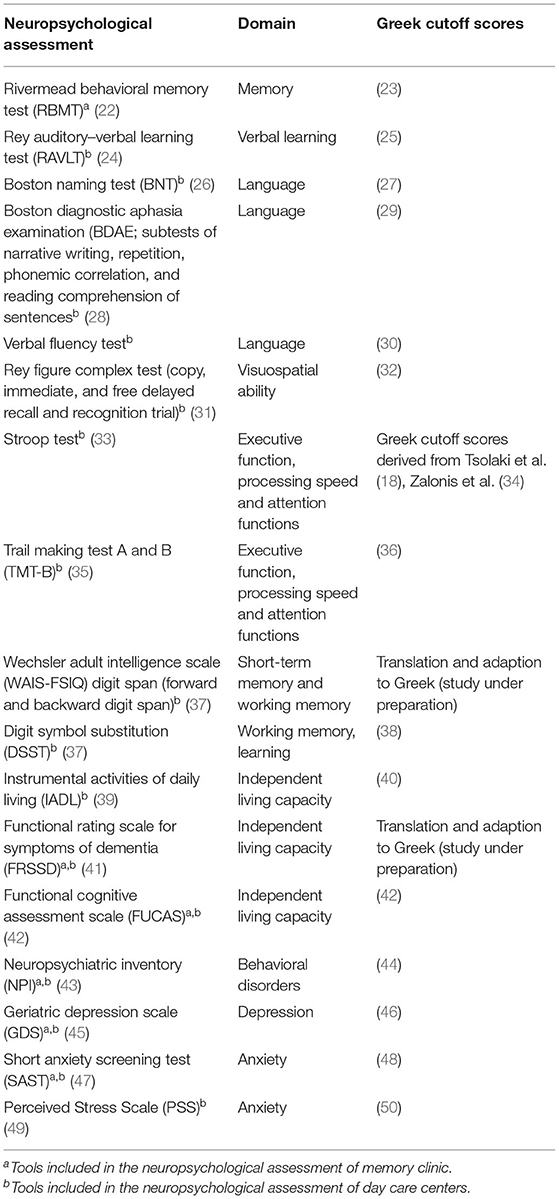
Table 2. Further neuropsychological assessment.
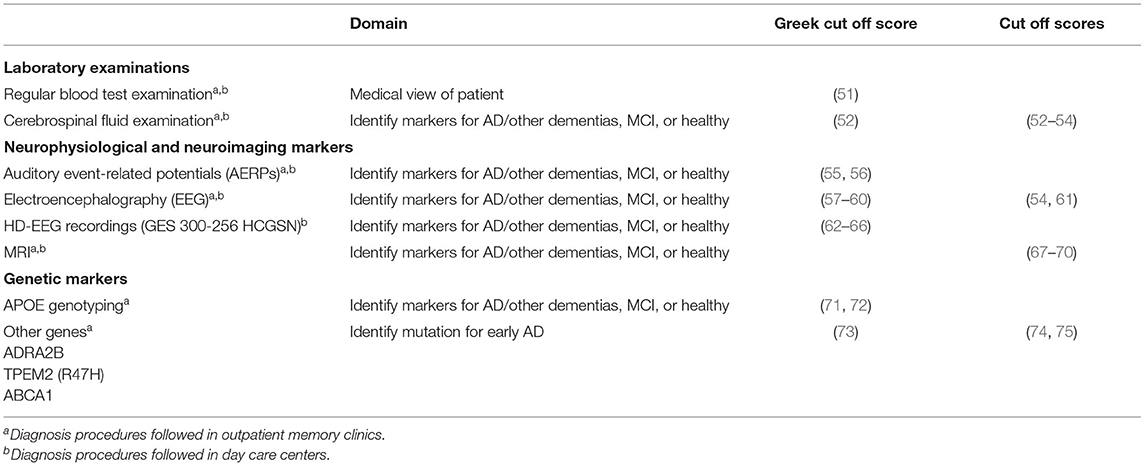
Table 3. Further examinations (neurochemical and biomarkers).
The diagnostic procedures are delivered to PwD, MCI, as well as SCI as detailed below.
The inclusion criteria for dementia are (a) diagnosis of major neurocognitive impairment of any etiology according to DSM-V criteria (76), (b) MMSE total score ≤ 23, (c) stages 4 and 5 of the disease according to the Global Deterioration Scale (GDS) (10), and (d) absence of anxiety and depression evaluated by the same scales employed for the two previous groups.
The most common types of dementia are Alzheimer's disease (AD) and vascular dementia, while frontotemporal dementia (FTD) and Lewy body dementia are less common. The neuropsychological evaluation lasts approximately 2 h, divided into two different face-to-face sessions to obtain the best performance from the participants by reducing the possibility of them getting tired. These tests are administered by a neuropsychologist consisting of screening tools, detection of memory, orientation, and language disorders, and tests of visuospatial ability, attention, executive function, and working memory ability as well as neuropsychiatric symptoms and independent living capacity (Tables 1, 2).
MCI is a transitional state between normal aging and dementia. The inclusion criteria are (a) diagnosis of MCI according to Petersen (77), excluding other pathologies not associated with dementia according to the Diagnostic and Statistical Manual of Mental Disorders, DSM-5 (76), (b) Mini Mental State Examination (MMSE) total score ≥26, (c) stage 3 of the disease according to the GDS, and (d) 1.5 standard deviation (SD) below the normal mean according to age and education in at least one cognitive domain according to the utilized neuropsychological tests.
In order to identify older adults with MCI, all the psychometric tools used for dementia detection are also administered in MCI using different cutoff scores (Tables 1, 2).
To determine SCI, we apply the Subjective Cognitive Decline Questionnaire (SCDQ) (20) and Memory Alternation Test (MAT) (21), which hold excellent reliability and sensitivity for discriminating those with SCI from NCI and MCI patients (Tables 1, 2).
Blood tests are performed in all patients. Routine blood test includes hematological (complete blood count, hematocrit, and hemoglobulin) and biochemical (glucose, cholesterol, etc.), rapid plasma reagin, as well as thyroid-stimulating hormone, and the levels of homocysteine, folic acid, vitamin D, and B12, which are correlated with cognitive impairment. Some patients who participate in clinical trials or clinical research projects, further blood tests or serum tests are performed to identify biological markers or risk genes which are possibly implicated in AD (78, 79).
Cerebrospinal fluid (CSF) samples are taken by lumbar puncture at the L3/L4 or L4/L5 interspace. The samples are stored at 80°C until further examination. CSF-Aβ42 is determined using a sandwich ELISA [INNOTEST β amyloid (1–39, 76, 77) (Lazarou et al. under revision) Innogenetics, Ghent, Belgium-−96 tests]. CSF-total tau levels are determined using the INNOTEST hTau-Antigen sandwich ELISA−96 tests (Innogenetics, Ghent, Belgium) and INNOTEST Phospho TAU protein at threonine-181hyperphosphorylated-tau–96 tests as well. The CSF Fas levels are determined with the human sAPO-1/Fas ELISA (Bender MedSystems, Vienna, Austria).
Auditory event-related potentials (AERPs) are sensitive neurophysiological biomarkers of MCI and AD using a simple discrimination task, the so-called oddball paradigm. In this task, two stimuli are presented in a random series, with one of the two less frequently, i.e., the odd ball. A series of binaural tones at 70 dB sound pressure level with 10-ms rise/fall and 100-ms plateau time is presented to all subjects. The auditory stimuli are presented in a random sequence with target tones of 2,000 Hz occurring 20% of the time and standard tones of 1,000 Hz occurring 80% of the time at a rate of 0.5 Hz. The subject is required to distinguish between the two tones by responding to the target (e.g., mentally counting) and not responding to the standard (79). The patients must pay attention in distinguishing the tones in order for the examination to be as accurate as possible.
The ERP activity is recorded at the Fz and Pz electrode sites of the 10–20 system using gold-plated electrodes affixed with electrode paste and tape, referred to as linked earlobes at the A1 A2 sites with a forehead ground and impedance at the lowest possible level. For all recordings, the electrode impedances are below 5 kΩ, and they are checked periodically during the recording session. For artifact suppression, an AC filter function was performed. For the purpose of reduced impedance, a special type of paste is used (Elefix Nihon-Kohden, EEG paste Z-401 CE). The AERPs are analyzed by means of Neuropack 4 (Nihon-Kohden, Tokyo).
Electroencephalography (EEG) activity is acquired in a resting state with a 19-channel Nihon Kohden. Neurofax J 921A EEG system at electrodes Fp1, Fp2, F7, F3, F z, F4, F8, T3, C3, Cz, C4, T4, T5, P3, P z, P4, T6, O1, and O2 of the international 10/20 system [43]. EEG data is sampled at 500 Hz, and the electrode impedance is kept lower than 5 kΩ. The signals are digitized with Neurofax EEG-1200, ver. 01–93. The patients are sitting in a comfortable armchair in a quiet room. They are instructed to remain calm, with their eyes closed, for 5 min and then open their eyes. During the pre-processing state, the EEG signal is bandpass-filtered at 0.5–50 Hz, with a notch filter at 50 Hz. These data are assessed in a qualitative way by neurologists, and quantitative analysis is performed by neurophysiologists and engineers.
Additionally, the HD- EEG EGI 300 Geodesic EEG system (GES 300), which uses a 256-channel Hydro-Cel Geodesic Sensor Net (HCGSN) (EGI Eugene, OR), is also implemented in order to investigate the ERP components and multiple network properties. Using this particular EEG system, it has been revealed that the amplitude of visual N170 ERP can differentiate SCI and MCI from the healthy older adults during a task which assessed the emotional processing of facial stimuli (62). This system is used in participants of clinical studies.
In agreement with radiology departments, brain MRI scans (mostly in 1.5 Tesla) are performed in most patients with cognitive disorders. Each MRI examination consists of the following sequences: T1W (±IV contrast), T2W, FLAIR, DWI/ADC, and 3D T2 FLAIR for volumetry. In some cases, T2*/SWI sequences are also included.
APOE alleles and different mutations are also tested if patients or family members desire to know about the genetic predisposition. The blood samples used for genotyping are collected in ethylenediaminetetraacetic acid-containing receptacles. DNA is extracted from peripheral blood using the QIAamp Blood DNA purification kit (Qiagen Inc, USA). To determine the APOE genotype, part of the APOE gene (228 bp) containing both polymorphic sites (amino acid positions 112 and 158) is amplified by PCR analysis using the following primers: forward: 5′-GGCACGGCTGTCCAAGGAGCTGCA-3′ and reverse: 5′-GCCCCGGCCTGGTACACTGCCAG-3′, according to the method described in Koutroumani et al. (73).
TREM 2 examination is performed to patients who desire to know if there is any mutation for the early onset of AD. DNA is extracted from peripheral blood. The mutation of TREM2 (c.140G>A/p.Arg47His) is amplified by PCR analysis. For the PCR, Platinum™ II Hot-Start PCR Master Mix (Thermo Fisher Scientific) was used. Primer sequencing, forward: AACACATGCTGTGCCATCC and reverse: CCCAGGATCCCTGAGAGC, was according to Sanger, using the BigDye terminator v3.1 cycle sequencing kit. Electrophoresis followed in an automated genetic analyzer SeqStudio (Applied Biosystems). The diagnosis is based on comparison with the referral sequence NM_018965.
Healthy older adults and people with SCI and MCI have the following cognitive and physical trainings. Many of the interventions are published here (80–86).
The program gives emphasis on fundamental dexterities such as stability, movement, handling, functional ability, and general fitness. Therefore, the program consists of aerobic, strength, flexibility, balance, and mobility exercises two to three times per week. It helps people maintain their good health state, improve their physical and functional abilities and their cognitive function through kinetic stimulations, and additionally sustain or decrease the development of dementia symptoms.
This program aims to improve the central executive system of working memory based on Baddeley's model. The main goal is to teach the patient three different coding strategies—double coding, hierarchical processing, and reducing speed—in order to remember a specific number of words presented at the beginning of each session.
The program aims to enhance cognitive functions such as attention, visual, and verbal memory and semantic memory and trigger the emotions and imagination of the participants through structured tasks, including famous paintings. They are specifically encouraged to answer questions about art crafts, write a story about the content, and recall significant elements of these paintings at the end of each session. It also gives them the chance to learn about masterpieces of painting and express their emotions toward art.
The program aims to improve verbal memory, attention, perception, speech production, comprehension, and learning ability, in general, by learning English as a second language. Specifically, the participants are provided with structured language tasks such as reading and writing as well as listening to simple dialogues between native speakers.
It is a cognitive training program using the history of ancient monuments. It aims to improve cognitive skills such as attention, memory, perception, creativity, speech, socialization, and orientation during the sessions. It includes audiovisual material about the history of Thessaloniki, while discussion and relevant exercises followed. Actual visits to these monuments followed as a way to improve the social life of older adults, decreasing at the same time any feelings of loneliness.
The program aims to enhance attention skills, working memory, and written speech. The participants watch an educational video for 20 min, which include various themes (health, ecology, history, arts, astronomy, philosophy, etc.). After that, the video is divided into smaller sections (to make it easier for the participants to remember), and a therapist asks them about the content. At the same time, the participants make comments about their knowledge in a specific topic while also completing some pencil-and-paper tasks.
This program aims to improve working memory, attention, language, and visuospatial functions, including several computerized memory exercises. Each participant has a touchscreen and performs the exercises in front of him/her. It does not require knowledge of computers. There are five levels of difficulty in each exercise consisting of the following categories: (1) visual–spatial exercises, (2) speech exercises, (3) numerical exercises, (4) reasonable exercises, and (5) memory exercises.
The goal of the program is to promote the learning process, as well as executive functions, and is mainly delivered to high-level participants. The learning modules are the following: (1) usability and familiarity with a PC—Microsoft Windows XP, (2) Word Processor—Microsoft Office Word 2007, (3) Internet use—Internet Explorer, and (4) using accounts—Microsoft Office Excel 2007.
The program aims to improve language skills, memory, and attention as well as enhance the quality of life, social skills, and mood. It is comprised of paper-and-pencil tasks. At first, all participants read a specific article and are encouraged to remember it, summarize it, and answer specific questions regarding the content. Thus, they are given tasks focused on language functions, including naming, comprehension, semantic memory, and verbal fluency.
This program enhances the visuospatial abilities, attention, executive function, and language skills via the execution of motion instructions. Each session consists of five visuomotor and verbal–kinetic tasks, including visual and verbal kinetic stimuli, respectively. During the tasks, the participants are encouraged to use personal strategies toward executing and completing the tasks.
The cognitive control training via the execution of dual task has as a basic aim the enhancement of cognitive abilities such as the switch of attention, inhibition, and working memory as well as other attention abilities such as divided and sustained attention. During the program, the participants divide their attention in two tasks using paper and pencil. There are also given stimuli of daily life, such as sounds, puzzles, cards, supermarket products, etc.
The attention training aims to enhance attention, executive function, and visual–verbal memory. The program includes teaching of memory strategies and adapt levels of difficulty. Each session consists of 10 cognitive tasks including visual selective attention, working memory and switched attention, shifting of visuospatial attention, and a dual task. The tasks are ecologically valid and derived from activities of daily living (ADL) scale, such as the shopping list and searching in a telephone catalog.
Language intervention aims to enhance the vocabulary, including 10 tasks of semantic expression of language (three tasks), semantic comprehension of language (three tasks), and phonemic expression of language (four tasks), whereas each set of cognitive tasks has three levels of difficulty. The tasks are ecologically valid, as they are derived from ADL scale.
The program aims to enhance the executive function components, such as working memory and verbal fluency as well as prospective memory (PM). It consists of three tasks in each session: (a) an event-based task (non-focal PM task), (b) a time-based task, and (c) a combination task (the intention should be executed after a specific period of time and if a specific cue appeared). The tasks include occupation with puzzles, watching videos, listening to music, doing handcrafts, reading newspapers, making shopping lists, etc.
The aim of the program is to improve the cognitive and functional performance of the older adult participants with MCI. At the beginning, the participants are taught a variety of internal memory strategies, which include “method of loci,” “keywords,” “visual imagery,” “association,” “categorization,” and so forth. As long as they are taught, the participants are encouraged to use internal strategies in aspects of their everyday life, such as memory for numbers, appointments, events which are going to happen in the near future, and names of individuals and places, so that the transmission of knowledge can succeed.
In this program, the participants see pictures of several places in the country. They are asked to answer specific questions in order to practice their working memory function, as well as attention abilities, and improve their verbal fluency performance. Afterwards, all participants present a favorite place among those they have previously seen, and a brief description of the place and personal experiences are followed. Finally, a discussion between all group members takes place.
The intervention aims to reduce the anxiety of the participants and help them explore their thoughts and feelings through the interpretation of symbolic mental images. The program includes three relaxation techniques: (a) progressive muscle relaxation, (b) breathing exercises, (c) autogenic relaxation and mental imagery as a cognitive rehabilitative technique. Environmental conditions, including soothing music and fragrant essence, are applied.
Patients with mild and moderate dementia have the following cognitive and physical training: physical exercise, language intervention, RHEA program, and reality orientation are administered also to PwD based on their physical and cognitive capability.
In the current program, parts of Greek movies are presented. One of the main goals of the program is mood improvement because of the pleasant content of these movies. After watching the movie, structured exercises, including memory, attention, and recall, followed. Additionally, the participants are encouraged to share the experiences they may have about the content of the movies.
The program aims to improve long-term memory, attention, and oral and written language and help them to reduce stress levels and enhance their mood. The participants listen to musical stimuli, and afterward they try to remember facts and experiences related to that song; finally, they perform written exercises about the lyrics.
The patients are encouraged to dance and play different roles in order to enhance their executive function abilities, such as planning, step sequence, accuracy, and abstract thinking. This program combines cognitive training via psychotherapy techniques, such as dance and drama, and aims to (a) enhance attention, executive function, and verbal and visual memory and (b) deal with the psychological needs of the patients, such as anxiety, depression, apathy, or irritability.
This program utilizes toys in order to enhance auditory and visual selective attention, dual-task abilities, working and episodic memory, and language and visuospatial abilities. Executive function and attention abilities are trained using toys, such as dolls, puzzles, plastic letters, plastic animals, and fruits—for example, the participants have to collect plastic fruits and categorize them according to season, color, or size. They were then asked to find words beginning with the first letter of the fruit that they had collected.
Apart from the cognitive training or cognitive stimulation programs applied in PwD and MCI, there are also provided leisure activities and psychotherapeutic sessions for the participants. These activities are as follows: (1) a choir group including PwD and MCI which aims to enhance the mood and self-esteem of a patient, (2) a painting group and an art therapy group which both aim to the expression of feelings and emotions and mental health improvement through painting or other kinds of art, and (3) Gestalt psychotherapy which is applied on patients with MCI. The aim of this psychotherapeutic procedure is the mental health improvement and the reduction of anxiety and mental deficits in general.
There is available published work for caregivers in the some studies (87–91).
The aim of the psychoeducational program is to provide information to caregivers regarding the disease and the level of functionality of the patient, in addition to the guidelines for more effective care. Education helps caregivers in making difficult decisions concerning the care and the treatment of their beloved. Caregivers also learn to be flexible in the negotiation of alternative solutions. There is also an online group which satisfies the needs of caregivers who cannot benefit from the face-to-face health support services due to health issues, transportation (due to COVID pandemic-related reasons), or time.
Family psychological support aims to help the whole family of people with dementia face and cope with the disease and reduce negative feelings and sense of burden.
Support groups aim to help the caregivers to be effective in their role and build up the necessary psychological skills to deal with difficult aspects of the disease and feelings of anger, loneliness, loss, and helplessness. During the support group, caregivers can develop new approaches of interpreting the situation they are dealing with and adapt more realistic targets and more effective pressure and anxiety management strategies.
The participants are couples, where one partner has been diagnosed with MCI or mild dementia. Based on narrative therapy principles, dyadic intervention helps the couple re-narrate and rewrite their story, including dementia in their common life. Moreover, communication techniques are presented to couples in order to improve their communication skills.
It refers to those who experience grief due to the loss of their patient. This group aims to help them accept the reality of loss, manage their emotions, and adapt the new cycle of life.
It aims to reduce the anxiety level and manage psychosomatic symptoms using relaxation techniques and mental imagery which lead to a deep relaxation of the body and mind. Relaxation intervention helps caregivers to develop their well-being and decrease stress levels.
Due to the huge amount of data of patients, the creation of a health database was crucial. Thus, an electronic health record (her) system, called Empedocles, was developed in 2016. Software developers, neurologists, psychologists, and other experts worked together to create the database which meets the needs of patients and experts, providing flexibility for different environments and clinical workflows. Empedocles is compliant with the (EU) 2016/679 General Data Protection Regulation by design. The EHR stores the following data on the patients: (1) personal information and demographic characteristics (including geospatial data), (2) medical history, triggers, and risk factors, (3) diagnosis, (4) medication, (5) neurophysiological examination, (6) dental examination, (7) neuropsychological assessment, (8) hematological and biochemical test results, (9) genetic and CSF results, (10) diagnostic neuroimaging test results, (11) perforation results, and (12) assessment of the mental health of caregivers. Currently, Empedocles EHR is hosted on a server at the Aristotle University of Thessaloniki and serves about 132 active users daily. It stores over 5,200 parameters, which can be repeatedly saved in each patient examination. Empedocles has amassed data for over 19,000 patients examined from 1988 till today (visits in memory clinics and DCCs), with more than 45,000 neuropsychological examinations. The database is continually updated and improved following both the requirements of end-users and society. During the COVID-19 pandemic, the functionalities of Empedocles were adapted so that the neuropsychological assessments could be applied from a distance (e.g., via telephone or Skype).
Memory clinic has been participated in several clinical trials to test new drugs for dementia during the last 30 years. The most indicative are provided in Table 4.
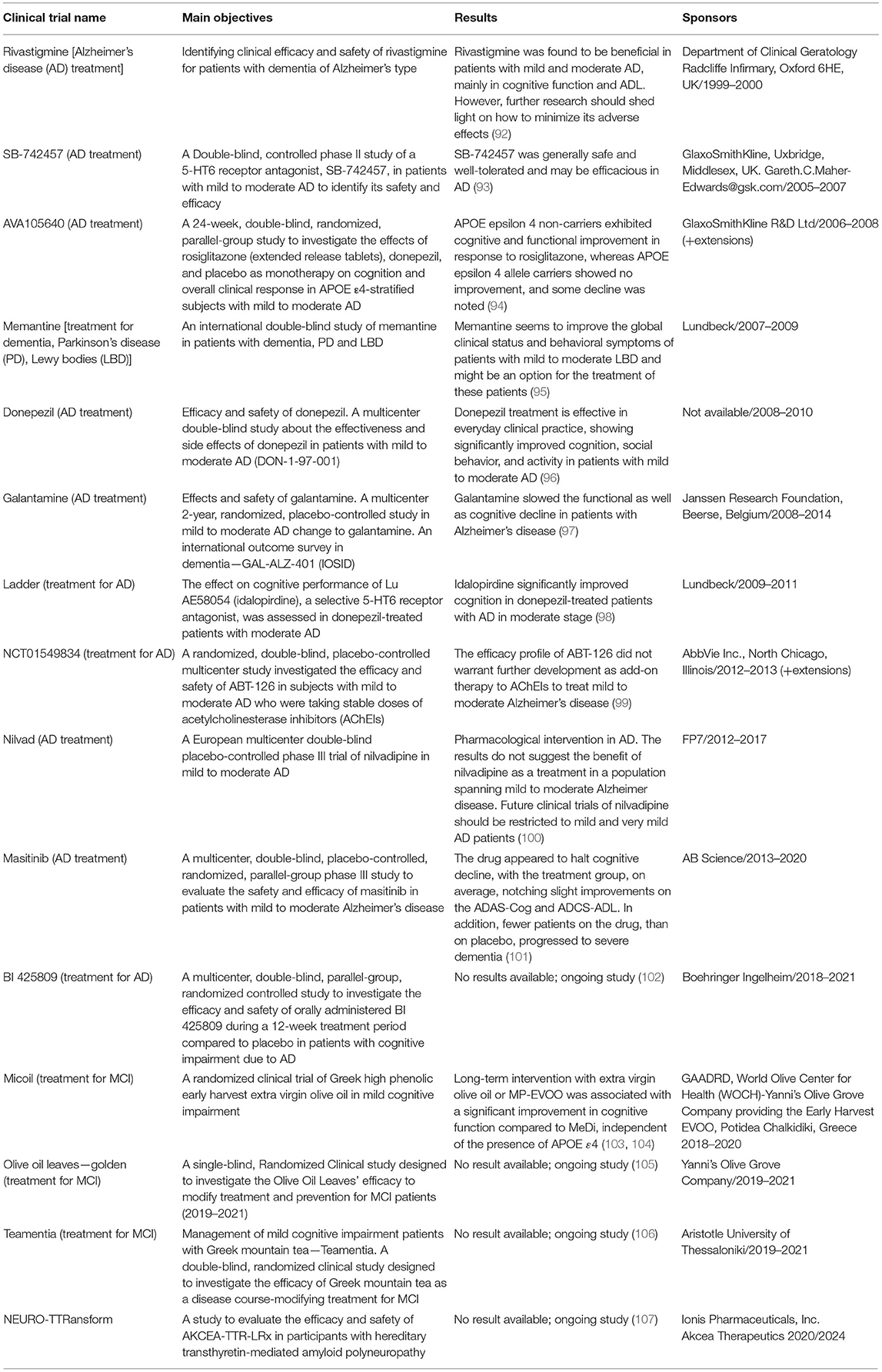
Table 4. Clinical trials.
Memory clinic and DCCs have also participated in several research studies and international projects the last 30 years. The most indicative are provided in Table 5.
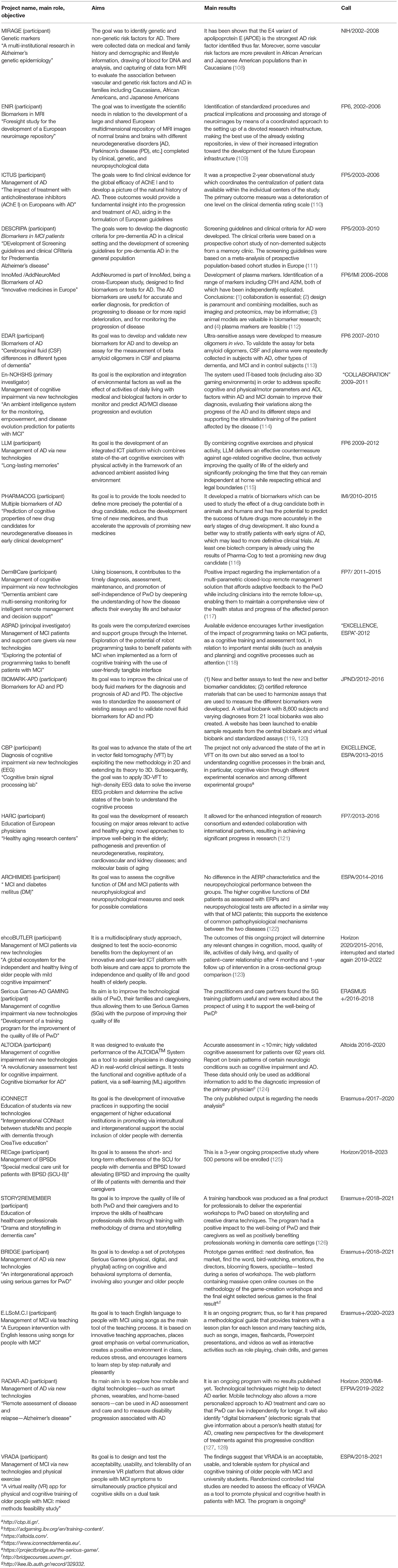
Table 5. Research studies and projects.
All the above-mentioned efforts have the following as targets:
• To provide a protocol of a holistic evaluation of cognitive status through clinical examination, an extended neuropsychological assessment, and biomarkers like blood tests, CSF, genetic tests, and MRI scans.
• To detect cognitive disorder as early as possible and carry out a differential diagnostic procedure to identify their etiologies.
• Plan the future care and provide advice to patients and their caregivers with respect to medical, psychological, legal, ethical, and social issues.
• Provide direct support to patients and caregivers by means of counseling, discussions with caregivers, and therapeutically oriented workgroups (e.g., memory training groups)
• Support families either at our day centers or at their homes
• Contribution to the dementia research and clinical field through funded projects and a plethora of studies conducted in DCC's and Outpatient Memory Clinics.
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Prince M, Bryce R, Albanese E, Wimo A, Ribeiro W, Ferri CP. The global prevalence of dementia: a systematic review and metanalysis. Alzheimers Dement. (2013) 9:63–75. doi: 10.1016/j.jalz.2012.11.007
2. Sousa RM, Ferri CP, Acosta D, Albanese E, Guerra M, Huang Y, et al. Contribution of chronic diseases to disability in elderly people in countries with low and middle incomes: a 10/66 Dementia Research Group population-based survey. Lancet. (2009) 374:1821–1830. doi: 10.1016/S0140-6736(09)61829-8
3. Prince M, Ferri CP, Acosta D, Albanese E, Arizaga R, Dewey M, et al. The protocols for the 10/66 dementia research group population-based research programme. BMC Public Health. (2007) 7:165. doi: 10.1186/1471-2458-7-165
4. Tsolaki M, Fountoulakis C, Pavlopoulos I, Chatzi E, Kazis A. Prevalence and incidence of Alzheimers disease and other dementing disorders in Pylea, Greece. Am J Alzheimers Dis Other Dement. (1999) 14:138–48. doi: 10.1177/153331759901400308
5. Tsolaki M, Kakoudaki T, Tsolaki A, Verykouki E, Pattakou V. Prevalence of mild cognitive impairment in individuals aged over 65 in a rural area in North Greece. Adv Alzheimers Dis. (2014) 3:11–9. doi: 10.4236/aad.2014.31002
6. Argyriadou S, Melissopoulou H, Krania E, Karagiannidou A, Vlachonicolis I, Lionis C. Dementia and depression: two frequent disorders of the aged in primary health care in Greece. Fam Pract. (2001) 18:87–91. doi: 10.1093/fampra/18.1.87
7. Tsolaki M, Gkioka M, Verykouki E, Galoutzi N, Kavalou E, Pattakou-Parasyri V. Prevalence of dementia, depression, and mild cognitive impairment in a rural area of the island of Crete, Greece. Am J Alzheimers Dis Other Demen. (2017) 32:252–64. doi: 10.1177/1533317517698789
8. Dardiotis E, Kosmidis MH, Yannakoulia M, Hadjigeorgiou GM, Scarmeas N. The hellenic longitudinal investigation of aging and diet (HELIAD): rationale, study design, and cohort description. Neuroepidemiology. (2014) 43:9–14. doi: 10.1159/000362723
10. Reisberg B, Ferris SH, de Leon MJ, Crook T. The global deterioration scale for assessment of primary degenerative dementia. Am J Psychiatry. (1982) 1136–9. doi: 10.1037/t48466-000
11. Mougias AA, Christidi F, Kontogianni E, Skaltsounaki E, Politis A, Politis A. Patient-and caregiver-related factors associated with caregiver assessed global deterioration scale scoring in demented patients. Curr Gerontol Geriatr Res. (2018) 2018:9396160. doi: 10.1155/2018/9396160
12. Folstein MF, Folstein SE, McHugh PR. Mini-mental state. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. (1975) 12:189–98. doi: 10.1016/0022-3956(75)90026-6
13. Fountoulakis K, Tsolaki M, Chatzi E, Kazis A. Mini mental state examination (MMSE). A validation study in demented patients from the elderly Greek population. Am J Alzheimers Dis. (2000) 15:342–7. doi: 10.1177/153331750001500604
14. Nasreddine ZS, Phillips NA, Bédirian V, Charbonneau S, Whitehead V, Collin I, et al. The montreal cognitive assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. (2005) 53:695–9. doi: 10.1111/j.1532-5415.2005.53221.x
15. Poptsi E, Moraitou D, Eleftheriou M, Kounti-Zafeiropoulou F, Papasozomenou C, Agogiatou C, et al. Normative data for the montreal cognitive assessment in Greek older adults with subjective cognitive decline, mild cognitive impairment and dementia. J Geriatr Psychiatry Neurol. (2019) 32:265–74. doi: 10.1177/0891988719853046
16. Tsolaki M, Iakovidou V, Navrozidou H, Aminta M, Pantazi T, Kazis A. Hindi mental state examination (HMSE) as a screening test for illiterate demented patients. Int J Geriatr Psychiatry. (2000) 15:662–4. doi: 10.1002/1099-1166(200007)15:7<662::AID-GPS171>3.0.CO;2-5
17. Rosen WG, Mohs RC, Davis KL. A new rating scale for Alzheimer's disease. Am J Psychiatry. (1984) 141:1356–64. doi: 10.1176/ajp.141.11.1356
18. Tsolaki M, Fountoulakis K, Nakopoulou E, Kazis A, Mohs RC. Alzheimer's Disease assessment scale: the validation of the scale in Greece in elderly demented patients and normal subjects. Dement Geriatr Cogn Disord. (1997) 8:273–80. doi: 10.1159/000106644
19. Inouye SK, van Dyck CH, Alessi CA, Balkin S, Siegal AP, Horwitz RI. Clarifying confusion: the confusion assessment method: a new method for detection of delirium. Ann Intern Med. (1990) 113:941–8. doi: 10.7326/0003-4819-113-12-941
20. Rami L, Mollica MA, García-Sanchez C, Saldaña J, Sanchez B, Sala I, et al. The subjective cognitive decline questionnaire (SCD-Q): a validation study. J Alzheimers Dis. (2014) 41:453–66. doi: 10.3233/JAD-132027
21. Rami L, Molinuevo JL, Sanchez-Valle R, Bosch B, Villar A. Screening for amnestic mild cognitive impairment and early Alzheimer's disease with M@ T (memory alteration test) in the primary care population. Int J Geriatr Psychiatry. (2007) 22:294–304. doi: 10.1002/gps.1672
22. Wilson B, Cockburn J, Baddeley A, Hiorns R. The development and validation of a test battery for detecting and monitoring everyday memory problems. J Clin Exp Neuropsychol. (1989) 11:855–70. doi: 10.1080/01688638908400940
23. Efklides A, Yiultsi E, Kangellidou T, Kounti F, Dina F, Tsolaki M. Wechsler memory scale, rivermead behavioral memory test, and everyday memory questionnaire in healthy adults and alzheimer's patients. Euro J Psychol Assess. (2002) 18:63. doi: 10.1027//1015-5759.18.1.63
24. Schmidt M. Rey Auditory Verbal Learning Test: A Handbook. Los Angeles, CA: Western Psychological Services (1996).
25. Messinis L, Tsakona I, Malefaki S, Papathanasopoulos P. Normative data and discriminant validity of rey's verbal learning test for the Greek adult population. Arch Clin Neuropsychol. (2007) 22:739–52. doi: 10.1016/j.acn.2007.06.002
26. Kaplan EF, Goodglass H, Wintraub S. The Boston Naming Test. Experimental Edition. Philadelphia, PA: Lea & Febiger (1983).
27. Patricacou A, Psallida E, Pring T, Dipper L. The Boston naming test in Greek: normative data and the effects of age and education on naming. Aphasiology. (2007) 21:1157–70. doi: 10.1080/02687030600670643
28. Goodglass H, Kaplan E. The Assessment of Aphasia and Related Disorders. Philadelphia, PA; Boston, MA: Lea & Febiger (1972).
29. Tsantali E, Tsolaki M, Efklides A, Kiosseoglou G, Pita G. Validation of the Boston diagnostic aphasia examination test in Greek elderly population. Encephalos. (2001) 38:146–66.
30. Kosmidis MH, Vlahou CH, Panagiotaki P, Kiosseoglou G. The verbal fluency task in the Greek population: normative data, and clustering and switching strategies. J Int Neuropsychol Soc. (2004) 10:164–72. doi: 10.1017/S1355617704102014
31. Rey A. L'examen psychologique dans le cas d'encephalopathie traumatique. Arch Psychol. (1941) 28:286–340.
32. Tsatali M, Emmanouel A, Gialaouzidis M, Avdikou K, Stefanatos C, Diamantidou A, et al. Rey complex figure test (RCFT): norms for the Greek older adult population. Appl Neuropsychol Adult. (2020) 1–9. doi: 10.1080/23279095.2020.1829624
33. Jensen AR, Rohwer WD. The stroop color – word test: a review. Acta Psychol. (1966) 25:36–93. doi: 10.1016/0001-6918(66)90004-7
34. Zalonis I, Christidi F, Bonakis A, Kararizou E, Triantafyllou NI, Paraskevas G, et al. The stroop effect in Greek healthy population: normative data for the stroop neuropsychological screening test. Arch Clin Neuropsychol. (2009) 24:81–8. doi: 10.1093/arclin/acp011
35. Partington JE, Leiter RG. Partington's pathway test. Psychol Serv Center Bull. (1949) 1:9–20. doi: 10.1037/t66320-000
36. Zalonis I, Kararizou E, Triantafyllou NI, Kapaki E, Papageorgiou S, Sgouropoulos P, et al. A normative study of the trail making test A and B in Greek adults. Clin Neuropsychol. (2008) 22:842–50. doi: 10.1080/13854040701629301
37. Wechsler D. Manual for the Wechsler Adult Intelligence Scale. Washington, DC: Psychological Corp (1955).
38. Tsatali M, Poptsi E, Moraitou D, Agogiatou C, Bakoglidou E, Gialaouzidis M, et al. Discriminant validity of the WAIS-R digit symbol substitution test in subjective cognitive decline, mild cognitive impairment (amnestic subtype) and Alzheimer's disease dementia (ADD) in Greece. Brain Sci. (2021) 11:881. doi: 10.3390/brainsci11070881
39. Finlayson M, Mallinson T, Barbosa VM. Activities of daily living (ADL) and instrumental activities of daily living (IADL) items were stable over time in a longitudinal study on aging. J Clin Epidemiol. (2005) 58:338–49. doi: 10.1016/j.jclinepi.2004.10.008
40. Theotoka I, Kapaki E, Vagenas V, Ilias I, Paraskevas GP, Liappas I. Preliminary report of a validation study of instrumental activities of daily living in a Greek sample. Percept Motor Skills. (2007) 104:958–60. doi: 10.2466/pms.104.3.958-960
41. Hutton JT. Alzheimer's disease. In: Rakel RE, editor. Conn's Current Therapy. Philadelphia, PA: W.B. Saunders (1990). p. 778–81.
42. Kounti F, Tsolaki M, Kiosseoglou G. Functional cognitive assessment scale (FUCAS): a new scale to assess executive cognitive function in daily life activities in patients with dementia and mild cognitive impairment. Hum Psychopharmacol. (2006) 21:305–11. doi: 10.1002/hup.772
43. Cummings JL. The neuropsychiatric inventory: assessing psychopathology in dementia patients. Neurology. (1997) 48:10–6. doi: 10.1212/WNL.48.5_Suppl_6.10S
44. Politis AM, Mayer LS, Passa M, Maillis A, Lyketsos CG. Validity and reliability of the newly translated hellenic neuropsychiatric inventory (H-NPI) applied to Greek outpatients with Alzheimer's disease: a study of disturbing behaviors among referrals to a memory clinic. Int J Geriatr Psychiatry. (2004) 19:203–8. doi: 10.1002/gps.1045
45. Yesavage JA, Brink TL, Rose TL, Lum O, Huang V, Adey M, et al. Development and validation of a geriatric depression screening scale: a preliminary report. J Psychiatric Res. (1982) 17:37–49. doi: 10.1016/0022-3956(82)90033-4
46. Fountoulakis KN, Tsolaki M, Iacovides A, Yesavage J, O'hara R, Kazis A, et al. The validation of the short form of the geriatric depression scale (GDS) in Greece. Aging Clin Exp Res. (1999) 11:367–72. doi: 10.1007/BF03339814
47. Sinoff G, Ore L, Zlotogorsky D, Tamir A. Short anxiety screening test—a brief instrument for detecting anxiety in the elderly. Int J Geriatr Psychiatry. (1999) 14:1062–71. doi: 10.1002/(SICI)1099-1166(199912)14:12<1062::AID-GPS67>3.0.CO;2-Q
48. Grammatikopoulos IA, Sinoff G, Alegakis A, Kounalakis D, Antonopoulou M, Lionis C. The short anxiety screening test in Greek: translation and validation. Ann Gen Psychiatry. (2010) 9:32. doi: 10.1186/1744-859X-9-1
49. Cohen S, Kessler RC, Gordon LU editors. Measuring Stress: A Guide for Health and Social Scientists. Oxford: Oxford University Press on Demand (1997).
50. Andreou E, Alexopoulos EC, Lionis C, Varvogli L, Gnardellis C, Chrousos GP, Darviri C. 2011 perceived stress scale: reliability and validity study in Greece. Int J Environ Res Public Health. (2011) 8:3287–98. doi: 10.3390/ijerph8083287
51. Tsolaki M. Clinical workout for the early detection of cognitive decline and dementia. Euro J Clin Nutr. (2014) 68:1186–91. doi: 10.1038/ejcn.2014.189
52. Marizzoni M, Ferrari C, Babiloni C, Albani D, Barkhof F, Cavaliere L, et al. CSF cutoffs for MCI due to AD depend on APOEε4 carrier status. Neurobiol Aging. (2020) 89:55–62. doi: 10.1016/j.neurobiolaging.2019.12.019
53. Albani D, Marizzoni M, Ferrari C, Fusco F, Boeri L, Raimondi I, PharmaCog Consortium. Plasma Aβ 42 as a biomarker of prodromal alzheimer's disease progression in patients with amnestic mild cognitive impairment: evidence from the PharmaCog/E-ADNI study. J Alzheimers Dis. (2019) 69:37–48. doi: 10.3233/JAD-180321
54. Galluzzi S, Marizzoni M, Babiloni C, Albani D, Antelmi L, Bagnoli C, et al. Clinical and biomarker profiling of prodromal Alzheimer's disease in workpackage 5 of the innovative medicines initiative PharmaCog project: a ‘European ADNI study'. J Intern Med. (2016) 279:576-591. doi: 10.1111/joim.12482
55. Papaliagkas V, Kimiskidis V, Tsolaki M, Anogianakis G. Usefulness of event-related potentials in the assessment of mild cognitive impairment. BMC Neurosci. (2008) 9:107. doi: 10.1186/1471-2202-9-107
56. Papaliagkas VT, Anogianakis G, Tsolaki MN, Koliakos G, Kimiskidis VK. Progression of mild cognitive impairment to Alzheimer's disease: improved diagnostic value of the combined use of N200 latency and β-amyloid (1–42) levels. Dement Geriatr Cogn Disord. (2009) 28:30–5. doi: 10.1159/000229023
57. Tsolaki A, Kazis D, Kompatsiaris I, Kosmidou V, Tsolaki M. Electroencephalogram and Alzheimer's disease: clinical and research approaches. Int J Alzheimers Dis. (2014) 2014:349249. doi: 10.1155/2014/349249
58. Iliadou P, Kladi A, Frantzidis CA, Gilou S, Tepelena I, Gialaouzidis M, et al. The pattern of mu rhythm modulation during emotional destination memory: comparison between mild cognitive impairment patients and healthy controls. J Alzheimers Dis. (2019) 71:1201–15. doi: 10.3233/JAD-190311
59. Dimitriadis SI, Laskaris NA, Bitzidou MP, Tarnanas I, Tsolaki MN. A novel biomarker of amnestic MCI based on dynamic cross-frequency coupling patterns during cognitive brain responses. Front Neurosci. (2015) 9:350. doi: 10.3389/fnins.2015.00350
60. Dimitriadis SI, Tarnanas I, Wiederhold M, Wiederhold B, Tsolaki M, Fleisch E. Mnemonic strategy training of the elderly at risk for dementia enhances integration of information processing via cross-frequency coupling. Alzheimers Dement Transl Res Clin Intervent. (2016) 2:241–9. doi: 10.1016/j.trci.2016.08.004
61. Jovicich J, Babiloni C, Ferrari C, Marizzoni M, Moretti DV, Del Percio C, et al. Two-year longitudinal monitoring of amnestic mild cognitive impairment patients with prodromal Alzheimer's disease using topographical biomarkers derived from functional magnetic resonance imaging and electroencephalographic activity. J Alzheimers Dis. (2019) 69:15–35. doi: 10.3233/JAD-180158
62. Lazarou I, Adam K, Georgiadis K, Tsolaki A, Nikolopoulos S, Tsolaki M. Can a novel high-density EEG approach disentangle the differences of visual event related potential (N170), elicited by negative facial stimuli, in people with subjective cognitive impairment? J Alzheimers Dis. (2018) 65:543–75. doi: 10.3233/JAD-180223
63. Lazarou I, Georgiadis K, Nikolopoulos S, Oikonomou VP, Tsolaki A, Kompatsiaris I, et al. A novel connectome-based electrophysiological study of subjective cognitive decline related to Alzheimer's disease by using resting-state high-density EEG EGI GES 300. Brain Sci. (2020) 10:392. doi: 10.3390/brainsci10060392
64. Tsolaki AC, Kosmidou V, Kompatsiaris IY, Papadaniil C, Hadjileontiadis L, Adam A, et al. Brain source localization of MMN and P300 ERPs in mild cognitive impairment and Alzheimer's disease: a high-density EEG approach. Neurobiol Aging. (2017) 55:190–201. doi: 10.1016/j.neurobiolaging.2017.03.025
65. Tsolaki A, Kosmidou V, Hadjileontiadis L, Kompatsiaris IY, Tsolaki M. Brain source localization of MMN, P300 and N400: aging and gender differences. Brain Res. (2015) 1603:32–49. doi: 10.1016/j.brainres.2014.10.004
66. Tsolaki AC, Kosmidou VE, Kompatsiaris IY, Papadaniil C, Hadjileontiadis L, Tsolaki M. Age-induced differences in brain neural activation elicited by visual emotional stimuli: a high-density EEG study. Neuroscience. (2017) 340:268–278. doi: 10.1016/j.neuroscience.2016.10.059
67. Ten Kate M, Redolfi A, Peira E, Bos I, Vos SJ, Vandenberghe R, et al. MRI predictors of amyloid pathology: results from the EMIF-AD Multimodal biomarker discovery study. Alzheimers Res Ther. (2018) 10:100. doi: 10.1186/s13195-018-0428-1
68. Marizzoni M, Ferrari C, Jovicich J, Albani D, Babiloni C, Cavaliere L, et al. Predicting and tracking short term disease progression in amnestic mild cognitive impairment patients with prodromal Alzheimer's disease: structural brain biomarkers. J Alzheimers Dis. (2019) 69:3–14. doi: 10.3233/JAD-180152
69. Khan W, Giampietro V, Banaschewski T, Barker GJ, Bokde AL, Büchel C, et al. A multi-cohort study of ApoE ε4 and Amyloid-β effects on the hippocampus in Alzheimer's disease. J Alzheimers Dis. (2017) 56:1159–74. doi: 10.3233/JAD-161097
70. Lombardi G, Crescioli G, Cavedo E, Lucenteforte E, Casazza G, et al. Structural magnetic resonance imaging for the early diagnosis of dementia due to Alzheimer's disease in people with mild cognitive impairment. Cochrane Database Syst Rev. (2020) 3:CD009628. doi: 10.1002/14651858.CD009628.pub2
71. Giannouli V, Tsolaki M. APOE ε4 allele and financial capacity performance in mild Alzheimer's disease: a pilot study. J Alzheimers Dis Rep. (2021) 5:93–7. doi: 10.3233/ADR-200254
72. Tsolaki AC, Gatzima O, Daniilidou M, Lazarou E, Bamidis PD, Verykouki E, et al. Prevalence of apolipoprotein E polymorphisms in Alzheimer's disease, mild cognitive impairment, and healthy elderly: a Northern Greece study. Neurodegenerat Dis. (2018) 18:216–24. doi: 10.1159/000491764
73. Koutroumani M, Daniilidou M, Giannakouros T, Proitsi P, Liapi D, Germanou A, et al. The deletion variant of α2b-adrenergic receptor is associated with decreased riskin Alzheimer's disease and mild cognitive impairment. J Neurol Sci. (2013) 328:19–23. doi: 10.1016/j.jns.2013.02.003
74. Wollmer MA, Sleegers K, Ingelsson M, Zekanowski C, Brouwers N, Maruszak A, et al. Association study of cholesterol-related genes in Alzheimer's disease. Neurogenetics. (2007) 8:179–88. doi: 10.1007/s10048-007-0087-z
75. Lupton MK, Proitsi P, Lin K, Hamilton G, Daniilidou M, Tsolaki M, et al. The role of ABCA1 gene sequence variants on risk of Alzheimer's disease. J Alzheimers Dis. (2014) 38:897–906. doi: 10.3233/JAD-131121
76. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®). American Psychiatric Pub (2013). doi: 10.1176/appi.books.9780890425596
77. Petersen RC. Mild cognitive impairment. Continuum. (2016) 22:404–18. doi: 10.1212/CON.0000000000000313
78. Tzekaki EE, Tsolaki M, Pantazaki AA, Geromichalos G, Lazarou E, Kozori M, et al. Administration of the extra virgin olive oil (EVOO) in Mild cognitive impairment (MCI) patients as a therapy for preventing the progress to AD. Hellen J Nucl Med. (2019) 22:181.
79. Squires K, Petuchowski S, Wickens C, Donchin E. The effects of stimulus sequence on event related potentials: a comparison of visual and auditory sequences. Percept Psychophys. (1977) 22:31–40. doi: 10.3758/BF03206077
80. Tsolaki M, Kounti F, Agogiatou C, Poptsi E, Bakoglidou E, Zafeiropoulou M, et al. Effectiveness of nonpharmacological approaches in patients with mild cognitive impairment. Neurodegenerat Dis. (2011) 8:138–145. doi: 10.1159/000320575
81. Kounti F, Bakoglidou E, Agogiatou C, Lombardo NBE, Serper LL, Tsolaki M. RHEA,* a nonpharmacological cognitive training intervention in patients with mild cognitive impairment: a pilot study. Topics Geriatr Rehabil. (2011) 27:289–300. doi: 10.1097/TGR.0b013e31821e59a9
82. Kosta-Tsolaki M, Poptsi E, Aggogiatou C, Kounti F, Zafeiropoulos S, Markou N. Computer-Based cognitive training versus paper and pencil training: which is more effective? A randomized controlled trial in people with mild cognitive impairment. JSM Alzheimers Dis Relat Dement. (2017) 4:1032.
83. Papasozomenou C, Poptsi E, Tabaki EM, Tsolaki M. The operation of the day care centre of alzheimer hellas“ saint helen” and of the memory clinic of papanikolaou general hospital from 2007 to 2017. Hellen J Nucl Med. (2017) 20:136–45.
84. Poptsi E, Lazarou I, Markou N, Vassiloglou M, Nikolaidou E, Diamantidou A, et al. A comparative single-blind randomized controlled trial with language training in people with mild cognitive impairment. Am J Alzheimers Dis Other Dement. (2019) 34:176–87. doi: 10.1177/1533317518813554
85. Mouzakidis C, Garopoulou V, Poptsi E, Antonopoulos A, Markou N, Tambaki, et al. Scientific planning of physical exercise protocols to prevent Dementia in elderly. The “fitness alzheimer mobility exercise”(FAME) project. A roadmap. J Phys Activ Nutrit Rehabil. (2019) 573–79.
86. Poptsi E, Tsatali M, Agogiatou C, Bakoglidou E, Batsila G, Dellaporta D, et al. Longitudinal cognitive and physical training effectiveness in MCI, based on the experience of the alzheimer's hellas day care centre. J Geriatr Psychiatry Neurol. (2021) 8919887211016057. doi: 10.1177/08919887211016057
87. Karagiozi K, Papaliagkas V, Giaglis G, Papastavrou E, Pattakou V, Tsolaki M. Combined intervention for caregivers of patients with dementia: a randomized controlled trial. Int J Acad Res Psychol. (2014) 1:77–95. doi: 10.46886/IJARP/v1-i1/1203
88. Karagiozi K., Margaritidou P, Makri M, Toumpalidou M, Egkiazarova M, Kosta-Tsolaki, et al. Interventions for Caregivers of people with dementia in Greece. J Family Med. (2017) 4:1125.
89. Toumpalidou M, Egkiazarova M, Iordan AR, Tsolaki M. Forgiveness as an intervention among caregivers of dementia patients: case report. J Fam Med. (2017) 4:1127. doi: 10.26420/jfammed.2017.1127
90. Karagiozi K, Margaritidou P., Tsatali M, Makri M, Apostolidis H, Dimitriou T, et al. Comparison of onsite versus online psycho education groups and reducing caregiver burden. Clin Gerontol. (2021) 1–11. doi: 10.1080/07317115.2021.1940409
91. Marki M, Sourgouni E, Tsatali M, Tsolaki M. Feelings experienced by informal caregivers of patients with dementia, from the moment of diagnosis until the beginning of psychotherapy. J Family Med. (2021) 8:1–7. doi: 10.26420/jfammed.2021.1248
92. Birks J, Grimley Evans J, Iakovidou V, Tsolaki M. Rivastigmine for Alzheimer's disease. Cochrane Database Syst Rev. (2000) CD001191. doi: 10.1002/14651858.CD001191
93. Maher-Edwards G, Zvartau-Hind M, Hunter AJ, Gold M, Hopton G, Jacobs G, et al. Double-blind, controlled phase II study of a 5-HT6 receptor antagonist, SB-742457, in Alzheimer's disease. Curr Alzheimer Res. (2010) 7:374–85. doi: 10.2174/156720510791383831
94. Risner ME, Saunders AM, Altman JFB, Ormandy GC, Craft S, Foley IM, et al. Efficacy of rosiglitazone in a genetically defined population with mild-to-moderate Alzheimer's disease. Pharmacogenom J. (2006) 6:246–54. doi: 10.1038/sj.tpj.6500369
95. Emre M, Tsolaki M, Bonuccelli U, Destée A, Tolosa E, Kutzelnigg A, et al. Memantine for patients with Parkinson's disease dementia or dementia with Lewy bodies: a randomised, double-blind, placebo-controlled trial. Lancet Neurol. (2010) 9:969–77. doi: 10.1016/S1474-4422(10)70194-0
96. Boada-Rovira M, Brodaty H, Cras P, Baloyannis S, Emre M, Zhang R, et al. Efficacy and safety of donepezil in patients with Alzheimer's disease. Drugs Aging. (2004) 21:43–53. doi: 10.2165/00002512-200421010-00004
97. Wilcock GK, Lilienfeld S, Gaens E. Efficacy and safety of galantamine in patients with mild to moderate Alzheimer's disease: multicentre randomised controlled trial. BMJ. (2000) 321:1445. doi: 10.1136/bmj.321.7274.1445
98. Wilkinson D, Windfeld K, Colding-Jørgensen E. Safety and efficacy of idalopirdine, a 5-HT6 receptor antagonist, in patients with moderate Alzheimer's disease (LADDER): a randomised, double-blind, placebo-controlled phase 2 trial. Lancet Neurol. (2014) 13:1092–9. doi: 10.1016/S1474-4422(14)70198-X
99. Florian H, Meier A, Gauthier S, Lipschitz S, Lin Y, Tang Q, et al. Efficacy and safety of ABT-126 in subjects with mild-to-moderate Alzheimer's disease on stable doses of acetylcholinesterase inhibitors: a randomized, double-blind, placebo-controlled study. J Alzheimers Dis. (2016) 51:1237–47. doi: 10.3233/JAD-150978
100. Lawlor B, Segurado R, Kennelly S, Olde Rikkert MG, Howard R, Pasquier F, et al. Nilvadipine in mild to moderate Alzheimer disease: a randomised controlled trial. PLoS Med. (2018) 15:e1002660. doi: 10.1371/journal.pmed.1002660
101. NIH. Masitinib in Patients With Mild to Moderate Alzheimer's Disease. (2020). Available online at: https://www.clinicaltrials.gov/ct2/show/NCT01872598
102. Alzforum. Positive Phase 2 Results Claimed for Masitinib in Alzheimer's. Available online at: https://www.alzforum.org/news/research-news/positive-phase-2-results-claimed-masitinib-alzheimers
103. Tsolaki M, Lazarou E, Kozori M, Petridou N, Tabakis I, Lazarou I, et al. A Randomized clinical trial of greek high phenolic early harvest extra virgin olive oil in mild cognitive impairment: the MICOIL pilot study. J Alzheimers Dis. (2020) 78:801–17. doi: 10.3233/JAD-200405
104. Tzekaki EE, Tsolaki M, Pantazaki AA, Geromichalos G, Lazarou E, Kozori M, et al. The pleiotropic beneficial intervention of olive oil intake on the Alzheimer's disease onset via fibrinolytic system. Exp Gerontol. (2021) 150:111344. doi: 10.1016/j.exger.2021.111344
105. ICH Good Clinical Practice Network. Management of Dementia With Olive Oil Leaves. Available online at: https://ichgcp.net/cs/clinical-trials-registry/NCT04440020
106. NIH. Management of Mild Cognitive Impairment Patients With Greek Mountain Tea - TEAMENTIA (TEAMENTIA). Available online at: https://clinicaltrials.gov/ct2/show/NCT04435509
107. NIH. NEURO-TTRansform: A Study to Evaluate the Efficacy and Safety of AKCEA-TTR-LRx in Participants With Hereditary Transthyretin-Mediated Amyloid Polyneuropathy. Available online at: https://clinicaltrials.gov/ct2/show/NCT04136184
108. NIH. MIRAGE: Multi-Institutional Research in Alzheimer's Genetic Epidemiology. Available online at: https://www.clinicaltrials.gov/ct2/show/NCT00239759
109. European Commission. Foresight Study for the Development of an European NeuroImage Repository. Available online at: https://cordis.europa.eu/project/id/26036/reporting
110. European Commission. The Impact of Treatment With Acetylcholinesterase Inhibitors on Europeans With Alzheimers Disease. Available online at: https://cordis.europa.eu/project/id/QLK6-CT-2002-02645
111. Descripa. DESCRIPA Study Early Diagnosis of Alzheimer's Disease. Available online at: http://www.descripa.eu/publications.html
112. Lovestone S, Francis P, Kloszewska I, Mecocci P, Simmons A, Soininen H, et al. AddNeuroMed-the European collaboration for the discovery of novel biomarkers for Alzheimer's disease. Ann N Y Acad Sci. (2009) 1180:36–46. doi: 10.1111/j.1749-6632.2009.05064.x
113. EDAR. EDAR Study Biomarkers for Alzheimer's Disease. Available online at: http://www.edarstudy.eu/
114. Votis K, Segkouli S, Drosou A, Tzovaras D, Tsolaki M. An ambient intelligence system for the monitoring, empowerment, and disease evolution prediction for patients with mild cognitive impairment. In: Bamidis PD, Tarnanas I, Hadjileontiadis L, Tsolaki M, editors. Handbook of Research on Innovations in the Diagnosis and Treatment of Dementia. IGI Global (2015). p. 225–39. doi: 10.4018/978-1-4666-8234-4.ch012
115. European Commission. Project Description. Available online at: https://cordis.europa.eu/project/id/238904
116. Alzheimer Europe. PharmaCog. Available online at: https://www.alzheimer-europe.org/Research/PharmaCog
117. Demacare. The Dem@Care Project: Dementia Ambient Care Multi-Sensing Monitoring for Intelligent Remote Management and Decision Support. Available online at: https://demcare.eu/
118. Demetriadis S, Tsiatsos T, Sapounidis T, Tsolaki M, Gerontidis A. Exploring the potential of programming tasks to benefit patients with mild cognitive impairment. In: PETRA '16: Proceedings of the 9th ACM International Conference on PErvasive Technologies Related to Assistive Environments. Thessaloniki (2016).
119. JPND Research. BIOMARKAPD. Available online at: https://www.neurodegenerationresearch.eu/initiatives/annual-calls-for-proposals/closed-calls/biomarkers-transnational-call/results-of-biomarker-call/biomarkapd/
120. Reijs BLR, Teunissen CE, Goncharenko N, Betsou F, Blennow K, Baldeiras I, et al. The central biobank and virtual biobank of BIOMARKAPD: a resource for studies on neurodegenerative diseases. Front Neurol. (2015) 6:216. doi: 10.3389/fneur.2015.00216
121. Komisja Europejska. Final Report Summary - HARC (Healthy Ageing Research Centre). Available online at: https://cordis.europa.eu/project/id/316300/reporting/pl
122. Papaliagkas V, Gkioka M, Mousiolis A, Chatzidimitriou M, Skepastianos P, Tsolaki M, et al. Neurophysiological study of alzheimer's disease and diabetes mellitus type 2 patients. Is there a common link? J Adv Med Res. (2021) 10–15. doi: 10.9734/jammr/2021/v33i1230935
123. Vanova M, Irazoki E, García-Casal JA, Martínez-Abad F, Botella C, Shiells KR, et al. The effectiveness of ICT-based neurocognitive and psychosocial rehabilitation programmes in people with mild dementia and mild cognitive impairment using GRADIOR and ehcoBUTLER: study protocol for a randomised controlled trial. Trials. (2018) 19:100. doi: 10.1186/s13063-017-2371-z
124. NIH. Evaluation of a Computerized Complex Instrumental Activities of Daily Living Marker (NMI) (AltoidaML). Available online at: https://clinicaltrials.gov/ct2/show/NCT02843529
125. Poptsi E, Tsolaki M, Bergh S, Cesana BM, Ciccone A, Fabbo A, et al. Rationale, design, and methodology of a prospective cohort study for coping with behavioral and psychological symptoms of dementia: the RECage project. J Alzheimers Dis. (2021) 80:1–15. doi: 10.3233/JAD-201215
126. Petridou N, Tsolaki M, Vasile A, Tudose C, Gadalean DA, Wyman D, et al. Story2Remember: using drama and storytelling in dementia care. In: Alzheimer's Association International Conference. Thessaloniki (2020).
127. IMI. Remote Assessment of Disease and Relapse – Alzheimer's Disease. Available online at: https://www.imi.europa.eu/projects-results/project-factsheets/radar-ad
128. Stavropoulos TG, Lazarou I, Diaz A, Gove D, Georges J, Manyakov NV, et al. Wearable devices for assessing function in Alzheimer's disease: a european public involvement activity about the features and preferences of patients and caregivers. Front Aging Neurosci. (2021) 13:43135. doi: 10.3389/fnagi.2021.643135
Keywords: memory, dementia, day care centers, educational programs, Alzheimer association, neurology departments, non-pharmacological interventions
Citation: Tsolaki M, Tsatali M, Gkioka M, Poptsi E, Tsolaki A, Papaliagkas V, Tabakis I-M, Lazarou I, Makri M, Kazis D, Papagiannopoulos S, Kiryttopoulos A, Koutsouraki E and Tegos T (2021) Memory Clinics and Day Care Centers in Thessaloniki, Northern Greece: 30 Years of Clinical Practice and Experience. Front. Neurol. 12:683131. doi: 10.3389/fneur.2021.683131
Received: 19 March 2021; Accepted: 25 June 2021;
Published: 25 August 2021.
Edited by:
Rufus Olusola Akinyemi, University of Ibadan, NigeriaReviewed by:
Georgios Ponirakis, Weill Cornell Medicine-Qatar, QatarCopyright © 2021 Tsolaki, Tsatali, Gkioka, Poptsi, Tsolaki, Papaliagkas, Tabakis, Lazarou, Makri, Kazis, Papagiannopoulos, Kiryttopoulos, Koutsouraki and Tegos. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marianna Tsatali, bXRzYXRhbGlAeWFob28uZ3I=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.