
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurol. , 30 August 2021
Sec. Dementia and Neurodegenerative Diseases
Volume 12 - 2021 | https://doi.org/10.3389/fneur.2021.681595
This article is part of the Research Topic Frontotemporal Dementia and its Spectrum in Latin America and the Caribbean: a Multidisciplinary Perspective View all 21 articles
 Andrea López-Cáceres1,2*
Andrea López-Cáceres1,2* María Velasco-Rueda1
María Velasco-Rueda1 Elkin Garcia-Cifuentes3
Elkin Garcia-Cifuentes3 Ignacio Zarante1
Ignacio Zarante1 Diana Matallana2,4,5
Diana Matallana2,4,5Frontotemporal dementia (FTD) is a highly heritable condition. Up to 40% of FTD is familial and an estimated 15% to 40% is due to single-gene mutations. It has been estimated that the G4C2 hexanucleotide repeat expansions in the C9ORF72 gene can explain up to 37.5% of the familial cases of FTD, especially in populations of Caucasian origin. The purpose of this paper is to evaluate hereditary risk across the clinical phenotypes of FTD and the frequency of the G4C2 expansion in a Colombian cohort diagnosed with FTD.
Methods: A total of 132 FTD patients were diagnosed according to established criteria in the behavioral variant FTD, logopenic variant PPA, non-fluent agrammatic PPA, and semantic variant PPA. Hereditary risk across the clinical phenotypes was established in four categories that indicate the pathogenic relationship of the mutation: high, medium, low, and apparently sporadic, based on those proposed by Wood and collaborators. All subjects were also examined for C9ORF72 hexanucleotide expansion (defined as >30 repetitions).
Results: There were no significant differences in the demographic characteristics of the patients between the clinical phenotypes of FTD. The higher rate phenotype was bvFTD (62.12%). In accordance with the risk classification, we found that 72 (54.4%) complied with the criteria for the sporadic cases; for the familial cases, 23 (17.4%) fulfilled the high-risk criteria, 23 (17.4%) fulfilled the low risk criteria, and 14 (10.6%) fulfilled the criteria to be classified as subject to medium risk. C9ORF72 expansion frequency was 0.76% (1/132).
Conclusion: The FTD heritability presented in this research was very similar to the results reported in the literature. The C9ORF72 expansion frequency was low. Colombia is a triethnic country, with a high frequency of genetic Amerindian markers; this shows consistency with the present results of a low repetition frequency. This study provides an initial report of the frequency for the hexanucleotide repeat expansions in C9ORF72 in patients with FTD in a Colombian population and paves the way for further study of the possible genetic causes of FTD in Colombia.
Frontotemporal dementia (FTD), a heterogeneous neurodegenerative disorder, is a highly heritable condition with reports of a positive family history in as many as 60% of cases (1, 2). In order to estimate the heritability of the family history, some criteria have been standardized—following the Goldman score and the one proposed by Wood and collaborators—according to the number of first- and second-degree relatives affected by FTD (3, 4). These efforts suggest a disease mechanism regarding the likelihood of an identifiable genetic cause and variability across clinical phenotypes (4, 5). A strong family history and higher frequency has been found in the behavioral variant of FTD (bvFTD), but less so in the semantic variant PPA (svPPA), the logopenic variant PPA (lvPPA), and the non-fluent agrammatic PPA (nfaPPA) (5–9). The heritability of FTD with motor neuron disease (FTD-MND), and atypical parkinsonian disorders are less clear, possibly due to the number of studies reported until today (5, 10). However, the G4C2 (GGGGCC) hexanucleotide repeat expansions in the C9ORF72 gene is the most common genetic cause of ALS and FTD (11, 12), and although the expansion mechanism is uncertain, it is suggested that the cause of disease in FTD includes “gain-of-toxicity” or reduction in function of the C9ORF72 protein (13).
It has been estimated that G4C2 can explain up to 37.5% of the familial cases of FTD, in particular, in populations of Caucasian origin (14). G4C2 has also been reported as a major cause of the disease in northern Europe, mainly Finland, and in North American FTD and ALS cohorts (11, 15). C9ORF72 also accounts for a significant proportion of Australian and Spanish FTD cases (16). By contrast, the C9ORF72 repeat expansion was not present or extremely rare in patients of Native American, Pacific Islander (11), Asian (17, 18), and Middle Eastern countries (19), and China (20, 21). Very few studies on the frequency of C9ORF2 have been carried out in Latin America. The first report was in an Argentinian population, where the expansion frequency in a FTD group was similar to that reported for patients in Europe and North America (14). In a Brazilian population (22, 23), the frequencies of the mutation in pure ALS and pure FTD cases were much lower than those observed in Finnish patients (11, 24), but similar to what was found for Germany (11) and Flanders-Belgium (25). There are no data as yet on the frequency and heritability of this expansion in an FTD population in Colombia (26). As such, in this study, we expect to estimate the frequency and heritability of C9ORF72 hexanucleotide repeat expansion in a group of patients with FTD diagnosis in Colombia.
A total of 132 patients were diagnosed with FTD according to consensus criteria for bvFTD, PPA: lvPPA, nfaPPA, and svPPA (27–29), at the Memory and Aging Clinic at the Hospital Universitario San Ignacio and Pontificia Universidad Javeriana in Bogotá, Colombia. The ethnicity of our sample could not be directly verified, but all patients are Colombian, and reported to be of Hispanic origin. This study was approved by the Ethics Committee at the same institution, and written consent was obtained from all participants and their legal representatives.
Family trees of the patients with FTD diagnosis were drawn up using information provided by the patients' families and caregivers. Pedigree information was obtained using the Proband application, where at least three generations of each of the subjects were described. The heritability of the disorder was classified by a geneticist with experience in the field of neurodegenerative diseases. The classification criteria were based on those proposed by Wood and collaborators. This classification method has four categories that indicate the pathogenic relationship of the mutation: high, medium, low, and apparently sporadic. These criteria are based on the number of first- and second-degree relatives affected with the spectrum of FTD disorders or other neurodegenerative diseases (4).
Genomic: All evaluated patients had a 3-cc blood sample taken in EDTA (ethylenediaminetetraacetic acid) tubes from which the genomic DNA was extracted using the Salting Out protocol. The DNA was then quantified using a NanoDrop® ND-1000 spectrophotometer. C9ORF72 hexanucleotide expansion (defined as >30 repetitions) was analyzed and tested with repeat-primed PCR and capillary electrophoresis as previously described (30). The sizes of the PCR fragments were analyzed using GeneMapper software (Applied Biosystems, Foster City, CA).
A frequency distribution was performed taking into account the risk classification of the pedigrees together with phenotypic (sex, age, and diagnosis) and genotypic (presence of the C9ORF72 expansion) characteristics. For the statistical analysis, absolute and relative measures were obtained for quantitative data. Central tendency and dispersion measures were evaluated for quantitative data.
Of the 132 patients, 51.52% were males and 48.48% were females. The latter presented a lower prevalence in the low-risk group than the male group. The main age of onset was of 59 years (12 IQR) (Table 1). The higher rate phenotype was bvFTD (62.12%), followed by non-specific PPA (18.18%), svPPA (15.90%), lvPPA (3.03%), and nfaPPA (0.75%). In categorizing by genetic risk based on the Wood pedigree classification, we found that 72 (54.4%) complied with the criteria for the sporadic cases; for the familial cases, 23 (17.4%) fulfilled the criteria for being high risk; 23 (17.4%) fulfilled the criteria for low risk; and 14 (10.6%) fulfilled the criteria for medium risk. Females and males were similarly distributed in three of the risk classification groups: apparent sporadic (40/32), medium risk (8/6), and high risk (12/11). The low-risk classification included more men than women (4/19).
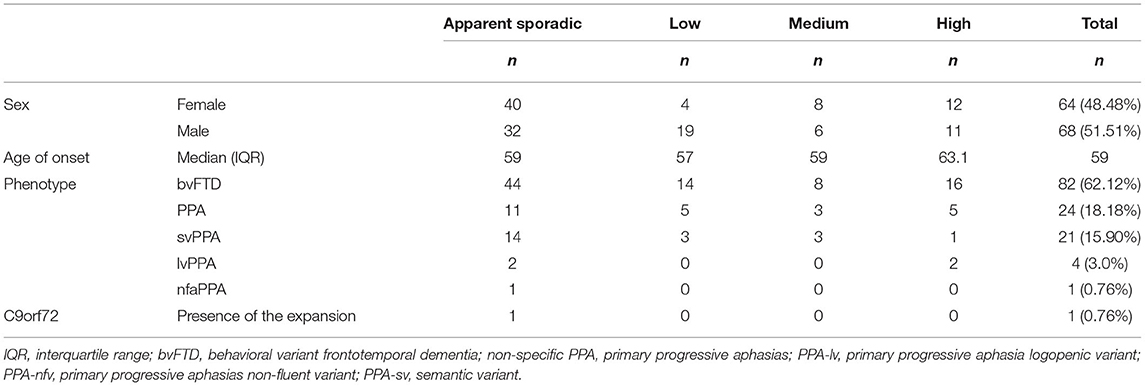
Table 1. FTD spectrum disorder pedigree categorization according to sex, age of onset, phenotype, and C9orf72 genotype.
C9ORF72 expansion was observed in 0.76% (1/132) of the sample. The positive case is a female patient diagnosed with bvFTD. The family pedigree was classified as a high-risk familial case (Figure 1), and the simple brain MRI with contrast revealed moderate supratentorial cortical atrophy predominantly in frontal and temporal regions.
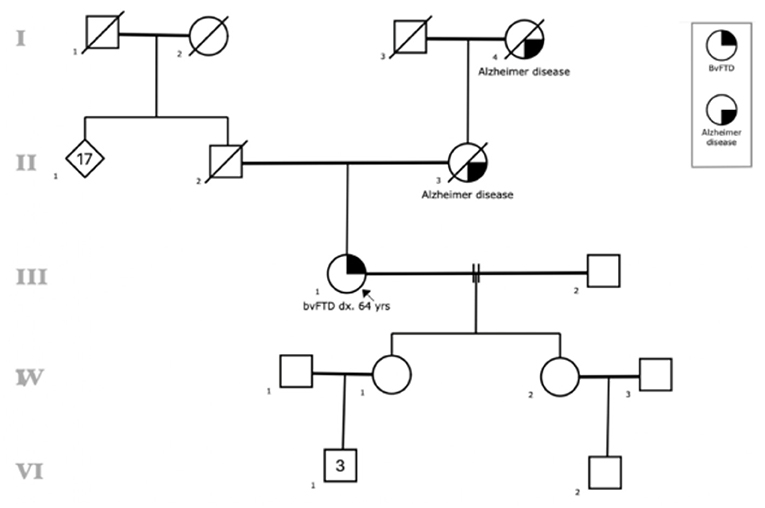
Figure 1. Family Pedigree of the patient with C90RF72 expansion. Circles: female, square: males. Black symbols reflect individuals affected with Alzheimer disease or bvFTD, lines represent those who are deceased. The arrow identifies the proband.
The present results show that the Colombian FTD sample data are similar to what is described in the literature regarding heritability, age of onset, and time of evolution of the disorder (31). Most of our patients exhibited the bvFTD followed by language variants (11, 32). One previous study demonstrated that bvFTD and the non-fluent/agrammatic variant of primary progressive aphasia (nfv-PPA) appeared to be more heritable than the semantic variant of primary progressive aphasia (sv-PPA) (33).
We observed no differences in the overall percentage of men and women in the study population, as has been reported in studies of populations in Argentina, southern Italy, and Brazil where the percentage of female patients has been higher (14, 23, 34). However, we note that our only case with the G4C2 expansion was presented by a woman and that our percentage of women classified as being of low heritable risk was much lower than that presented in other risk groups, which could support the hypothesis that female G4C2 repeat mutation carriers are more likely to develop cognitive or behavioral impairment (35). Given previous reports where C9ORF72 expansions have been found in non-familial cases (11), we found only one patient with the bvFTD that presented the C9ORF72 expansion from the high-risk cases, with a total frequency of 0.76% (1/132). The repeat expansions in the C9ORF72 gene is responsible for one of the FTD cases but not all FTD diagnoses in a Colombian cohort, revealing that there may be causes other than C9ORF72 to account for FTD cases in Colombia.
Wood and collaborators found C9ORF72 expansion in 25/306 (8.2%) of FTD patients, with the mutation-detection rate being highest in the low category and apparent sporadic cases (12, 24). This finding is consistent with prior reports of C9ORF72 expansion in sporadic families, and it coincides with findings from other studies (11, 36). Although we found C9ORF72 expansion in the high-risk group, we found no other patients that fulfilled the high-risk criteria and presented the expansion, supporting the importance of performing molecular analysis of this expansion in the idiopathic forms (11, 37–39).
The low frequency of the G4C2 expansion in the patient group with FTD 0.76% (1/132) is similar to what has been reported for Asian and Amerindian populations (17–21). There are even studies where no cases with this expansion 0/52 were identified (40). In Europe and North America, much higher frequencies have been established for the G4C2 expansion, with Finland and Sweden with overall frequencies of 29.33 and 20.73%, respectively, and Spain with 25.49%. Lower frequencies have been observed in Germany with 4.82% (41). In North America, C9ORF72 expansion accounted for almost 25% of familial FTD cases and 6% of sporadic cases (11). So far, only two studies have been conducted for the Latin American population, one in Argentina (14) where a frequency of expansion of 18.2% (6/33 cases) of patients with FTD was observed (14), and the other in Brazil, where a frequency of 7.1% (n = 67) for patients with pure familial FTD was found (23).
As it was shown before, the high frequency of the C9ORF72 expansion is associated with populations of European origin (11, 14). According to the human settlement hypothesis, Asian populations arriving through the Bering strait settled in North and South America, making the Amerindian populations very similar to the original ones and homogeneous with each other. This would support the absence of the C9ORF72 repetition in populations of Amerindian origin and this coincides with the results found for Amerindian groups in North America (11).
The populations of European ancestry with high frequencies present similar frequencies. An example of this is the Argentine population among which frequencies similar to those of European countries have been found, corroborating the Caucasian origin of this repetition (14, 42, 43). Colombia is a triethnic country, made up of a population of Native American, African, and European origin. Bogotá, the capital of Colombia, has a typical multiple ancestry population, showing a high proportion of people of European ancestry, followed by Native American and African (42). The higher frequency of Amerindian genetic markers presents a coherent result with a low frequency of repetition. This study provides an initial report of the frequency of expansions of hexanucleotide repeats in C9ORF72 in patients with FTD in the Colombian population and paves the way for further study of the possible genetic causes of FTD in Colombia.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
The studies involving human participants were reviewed and approved by Pontificia Universidad Javeriana, Facultad de Medicina. The patients/participants provided their written informed consent to participate in this study.
AL-C and MV-R: study concept development and study design. AL-C, MV-R, and DM: testing and data collection. AL-C, MV-R, EG-C, and IZ: data analysis and interpretation. AL-C, MV-R, and IZ: manuscript drafting and provision of critical reviews. All authors have participated in the work and approve the final version of the manuscript for submission.
This study was partly supported by US-South American Initiative for Genetic-Neural-Behavioral Interactions in Human Neurodegenerative Research, National Institutes of Health, National Institutes of Aging, Grant/Award Number:R01AG057234-01A1, MINCIENCIAS, 371-2011, 697-2014 and 370-201 grants, as well as the clinicians in the Memory and Cognitive Center (Intellectus) of the Hospital Universitario San Ignacio, Pontificia Universidad Javeriana, Bogotá, Colombia.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors would like to thank the US–South American Initiative for Genetic–Neural–Behavioral Interactions in Human Neurodegenerative Research (R01AG057234-01A1). The authors would also like to thank the patients, neuropsychologists, and psychiatrists who participated in the project, along with Intellectus and the APS project.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2021.681595/full#supplementary-material
1. Ratnavalli E, Brayne C, Dawson K, Hodges JR. The prevalence of frontotemporal dementia. Neurology. (2002) 58:1615–21 doi: 10.1212/WNL.58.11.1615
2. Mackenzie IRA, Frick P, Neumann M. The neuropathology associated with repeat expansions in the C9ORF72 gene. Acta Neuropathol. (2014) 127:347–57. doi: 10.1007/s00401-013-1232-4
3. Goldman JS, Farmer JM, Van Deerlin VM, Wilhelmsen KC, Miller BL, Grossman M. Frontotemporal dementia: Genetics and genetic counseling dilemmas. Neurologist. (2004) 10:227–34. doi: 10.1097/01.nrl.0000138735.48533.26
4. Wood EM, Falcone D, Suh ER, Irwin DJ, Chen-Plotkin AS, Lee EB, et al. Development and validation of pedigree classification criteria for frontotemporal lobar degeneration. JAMA Neurol. (2013) 70:1411–7. doi: 10.1001/jamaneurol.2013.3956
5. Greaves CV, Rohrer JD. An update on genetic frontotemporal dementia. J Neurol. (2019) 266:2075–86. doi: 10.1007/s00415-019-09363-4
6. Ghosh S, Lippa CF. Clinical subtypes of frontotemporal dementia. Am J Alzheimers Dis Other Demen. (2015) 30:653–61. doi: 10.1177/1533317513494442
7. Mok K, Traynor BJ, Schymick J, Tienari PJ, Laaksovirta H, Peuralinna T, et al. The chromosome 9 ALS and FTD locus is probably derived from a single founder. Neurobiol Aging. (2012) 33:209. e3–8. doi: 10.1016/j.neurobiolaging.2011.08.005
8. Boeve BF, Boylan KB, Graff-Radford NR, Dejesus-Hernandez M, Knopman DS, Pedraza O, et al. Characterization of frontotemporal dementia and/or amyotrophic lateral sclerosis associated with the GGGGCC repeat expansion in C9ORF72. Brain. (2012) 135:765–83. doi: 10.1093/brain/aws004
9. Murray ME, Dejesus-Hernandez M, Rutherford NJ, Baker M, Duara R, Graff-Radford NR, et al. Clinical and neuropathologic heterogeneity of c9FTD/ALS associated with hexanucleotide repeat expansion in C9ORF72. Acta Neuropathol. (2011) 122:673–690. doi: 10.1007/s00401-011-0907-y
10. Ferrari R, Hernandez DG, Nalls MA, Rohrer JD, Ramasamy A, Kwok JBJ, et al. Frontotemporal dementia and its subtypes: a genome-wide association study. Lancet Neurol. (2014) 13:686–99. doi: 10.1016/S1474-4422(14)70065-1
11. Majounie E, Renton AE, Mok K, Dopper EGP, Waite A, Rollinson S, et al. Frequency of the C9orf72 hexanucleotide repeat expansion in patients with amyotrophic lateral sclerosis and frontotemporal dementia: a cross-sectional study. Lancet Neurol. (2012) 11:323–30. doi: 10.1016/j.yneu.2012.05.040
12. DeJesus-Hernandez M, Mackenzie IR, Boeve BF, Boxer AL, Baker M, Rutherford NJ, et al. Expanded GGGGCC hexanucleotide repeat in noncoding region of C9ORF72 causes chromosome 9p-linked FTD and ALS. Neuron. (2011) 72:245–56. doi: 10.1016/j.neuron.2011.09.011
13. Zhu Q, Jiang J, Gendron TF, McAlonis-Downes M, Jiang L, Taylor A, et al. Reduced C9ORF72 function exacerbates gain of toxicity from ALS/FTD-causing repeat expansion in C9orf72. Nat Neurosci. (2020) 23:615–24. doi: 10.1038/s41593-020-0619-5
14. Itzcovich T, Xi Z, Martinetto H, Chrem-Méndez P, Russo MJ, de Ambrosi B, et al. Analysis of C9orf72 in patients with frontotemporal dementia and amyotrophic lateral sclerosis from Argentina. Neurobiol Aging. (2016) 40:192. e13–192.e15. doi: 10.1016/j.neurobiolaging.2016.02.001
15. Burrell JR, Kiernan MC, Vucic S, Hodges JR. Motor Neuron dysfunction in frontotemporal dementia. Brain. (2011) 134:2582–94. doi: 10.1093/brain/awr195
16. Dobson-Stone C, Hallupp M, Loy CT, Thompson EM, Haan E, Sue CM, et al. C9ORF72 Repeat expansion in australian and spanish frontotemporal dementia patients. PLoS ONE. (2013) 8:e56899. doi: 10.1371/journal.pone.0056899
17. Jang JH, Kwon MJ, Choi WJ, Oh KW, Koh SH, Ki CS, et al. Analysis of the C9orf72 hexanucleotide repeat expansion in Korean patients with familial and sporadic amyotrophic lateral sclerosis. Neurobiol Aging. (2013) 34:1311.e7–9. doi: 10.1016/j.neurobiolaging.2012.09.004
18. Ogaki K, Li Y, Atsuta N, Tomiyama H, Funayama M, Watanabe H, et al. Analysis of C9orf72 repeat expansion in 563 Japanese patients with amyotrophic lateral sclerosis. Neurobiol Aging. (2012) 33:2527.e11–16. doi: 10.1016/j.neurobiolaging.2012.05.011
19. Alavi A, Nafissi S, Rohani M, Shahidi G, Zamani B, Shamshiri H, et al. Repeat expansion in C9ORF72 is not a major cause of amyotrophic lateral sclerosis among iranian patients. Neurobiol Aging. (2014) 11:232–40. doi: 10.1016/j.neurobiolaging.2013.07.016
20. Zou ZY, Li XG, Liu MS, Cui LY. Screening for C9orf72 repeat expansions in Chinese amyotrophic lateral sclerosis patients. Neurobiol Aging. (2013) 34:1710. e5–6. doi: 10.1016/j.neurobiolaging.2012.11.018
21. Luo Y, Jiao B, Wang J, Du J, Yan X, Xia K, et al. C9orf72 hexanucleotide repeat expansion analysis in Chinese spastic paraplegia patients. J Neurol Sci. (2014) 347:104–6. doi: 10.1016/j.jns.2014.09.028
22. Takada LT, Pimentel MLV, DeJesus-Hernandez M, Fong JC, Yokoyama JS, Karydas A, et al. Frontotemporal dementia in a Brazilian kindred with the C9orf72 mutation. Arch Neurol. (2012) 69:1149–53. doi: 10.1001/archneurol.2012.650
23. Cintra VP, Bonadia LC, Andrade HMT, de Albuquerque M, Eusébio MF, de Oliveira DS, et al. The frequency of the C9orf72 expansion in a Brazilian population. Neurobiol Aging. (2018) 66:179.e1–179.e4. doi: 10.1016/j.neurobiolaging.2018.01.007
24. Renton AE, Majounie E, Waite A, Simón-Sánchez J, Rollinson S, Gibbs JR, et al. A hexanucleotide repeat expansion in C9ORF72 is the cause of chromosome 9p21-linked ALS-FTD. Neuron. (2011) 72:257–68.
25. Gijselinck I, Van Langenhove T, van der Zee J, Sleegers K, Philtjens S, Kleinberger G, et al. A C9orf72 promoter repeat expansion in a Flanders-Belgian cohort with disorders of the frontotemporal lobar degeneration-amyotrophic lateral sclerosis spectrum: a gene identification study. Lancet Neurol. (2012) 11:54–65. doi: 10.1016/S1474-4422(11)70261-7
26. Ramos C, Aguillon D, Cordano C, Lopera F. Genetics of dementia insights from Latin America. Dementia e Neuropsychol. (2020) 14:223–36. doi: 10.1590/1980-57642020dn14-030004
27. Gorno-Tempini ML, Hillis AE, Weintraub S, Kertesz A, Mendez M, Cappa SF, et al. Classification of primary progressive aphasia and its variants. Neurology. (2011) 76:1006–14. doi: 10.1212/WNL.0b013e31821103e6
28. Rascovsky K, Hodges JR, Kipps CM, Johnson JK, Seeley WW, Mendez MF, et al. Diagnostic criteria for the behavioral variant of frontotemporal dementia (bvFTD): current limitations and future directions. Alzheimer Dis AssocDisord. (2007) 21:S14–8. doi: 10.1097/WAD.0b013e31815c3445
29. Tippett DC. Classification of primary progressive aphasia: challenges and complexities. F1000Research. (2020) 9:64. doi: 10.12688/f1000research.21184.1
30. Suh ER, Lee EB, Neal D, Wood EM, Toledo JB, Rennert L, et al. Semi-automated quantification of C9orf72 expansion size reveals inverse correlation between hexanucleotide repeat number and disease duration in frontotemporal degeneration. Acta Neuropathol. (2015) 130:363–72. doi: 10.1007/s00401-015-1445-9
31. Benussi L, Rossi G, Glionna M, Tonoli E, Piccoli E, Fostinelli S, et al. C9ORF72 hexanucleotide repeat number in frontotemporal lobar degeneration: a genotype-phenotype correlation study. J Alzheimer Dis. (2014) 38:799–808. doi: 10.3233/JAD-131028
32. Van Langenhove T, Van Der Zee J, Gijselinck I, Engelborghs S, Vandenberghe R, Vandenbulcke M, et al. Distinct clinical characteristics of C9Orf72 expansion carriers compared with grn, mapt, and nonmutation carriers in a flanders-belgian ftld cohort. JAMA Neurol. (2013) 70:365–73. doi: 10.1001/2013.jamaneurol.181
33. Rohrer JD, Guerreiro R, Vandrovcova J, Uphill J, Reiman D, Beck J, et al. The heritability and genetics of frontotemporal lobar degeneration. Neurology. (2009) 73:1451–6. doi: 10.1212/WNL.0b013e3181bf997a
34. Onyike CU, Diehl-Schmid J. The epidemiology of frontotemporal dementia. Int Rev Psychiatry. (2013) 25:130–7. doi: 10.3109/09540261.2013.776523
35. Curtis AF, Masellis M, Hsiung GYR, Moineddin R, Zhang K, Au B, et al. Sex differences in the prevalence of genetic mutations in FTD and ALS. Neurology. (2017) 89:1633–42. doi: 10.1212/WNL.0000000000004494
36. Liu Y, Yu JT, Sun FR, Ou JR, Qu S, Ben, Tan L. The clinical and pathological phenotypes of frontotemporal dementia with C9ORF72 mutations. J Neurol Sci. (2013) 335:26–35. doi: 10.1016/j.jns.2013.09.013
37. Byrne S, Elamin M, Bede P, Shatunov A, Walsh C, Corr B, et al. Cognitive and clinical characteristics of patients with amyotrophic lateral sclerosis carrying a C9orf72 repeat expansion: a population-based cohort study. Lancet Neurol. (2012) 11:232–40. doi: 10.1016/S1474-4422(12)70014-5
38. Cooper-Knock J, Higginbottom A, Connor-Robson N, Bayatti N, Bury JJ, Kirby J, et al. Clinical/Scientific Notes C9ORF72 transcription in a frontotemporal dementia case with two expanded alleles. Neurology. (2013) 81:1719–21. doi: 10.1212/01.wnl.0000435295.41974.2e
39. Sabatelli M, Conforti FL, Zollino M, Mora G, Monsurrò MR, Volanti P, et al. C9ORF72 hexanucleotide repeat expansions in the Italian sporadic ALS population. Neurobiol Aging. (2012) 33:209. e3–8. doi: 10.1016/j.neurobiolaging.2012.02.011
40. Mok KY, Koutsis G, Schottlaender LV, Polke J, Panas M, Houlden H. High frequency of the expanded C9ORF72 hexanucleotide repeat in familial and sporadic Greek ALS patients. Neurobiol Aging. (2012) 33:851. e1–5. doi: 10.1016/j.neurobiolaging.2012.02.021
41. van der Zee J, Gijselinck I, Dillen L, Van Langenhove T, Theuns J, Engelborghs S, et al. A pan-european study of the C9orf72 repeat associated with FTLD: geographic prevalence, genomic instability, and intermediate repeats. Hum Mutat. (2013) 34:363–73.
42. Mogollón Olivares F, Moncada Madero J, Casas-Vargas A, Zea Montoya S, Suárez Medellín D, Gusmão L, et al. Contrasting the ancestry patterns of three distinct population groups from the northernmost region of South America. Am J Phys Anthropol. (2020) 173:437–47. doi: 10.1002/ajpa.24130
Keywords: C9ORF72, frontotemporal dementia, Colombia, family inheritance, heritability
Citation: López-Cáceres A, Velasco-Rueda M, Garcia-Cifuentes E, Zarante I and Matallana D (2021) Analysis of Heritability Across the Clinical Phenotypes of Frontotemporal Dementia and the Frequency of the C9ORF72 in a Colombian Population. Front. Neurol. 12:681595. doi: 10.3389/fneur.2021.681595
Received: 16 March 2021; Accepted: 30 June 2021;
Published: 30 August 2021.
Edited by:
Bruce Miller, University of California, San Francisco, United StatesReviewed by:
Peter S. Pressman, University of Colorado Denver, United StatesCopyright © 2021 López-Cáceres, Velasco-Rueda, Garcia-Cifuentes, Zarante and Matallana. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Andrea López-Cáceres, YW5kcmVhLWxvcGV6QGZzZmIub3JnLmNv
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.