 Hira Ishaq1†
Hira Ishaq1† Nemat Khan
Nemat Khan Pamela McCombe
Pamela McCombe Mian Ayaz Ul Haq
Mian Ayaz Ul Haq
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Neurol., 07 June 2021
Sec. Multiple Sclerosis and Neuroimmunology
Volume 12 - 2021 | https://doi.org/10.3389/fneur.2021.672524
This article is part of the Research TopicMultiple Sclerosis and Neuroimmunology – Case Report Collection, Volume IView all 28 articles
Background: Coronavirus disease-2019 (COVID-19), caused by the severe acute respiratory distress syndrome–coronavirus-2 (SARS-CoV-2), is primarily a respiratory infection but has been recently associated with a variety of neurological symptoms. We present herewith a COVID-19 case manifesting as opsoclonus-myoclonus syndrome (OMS), a rare neurological disorder.
Case Presentation: A 63-year-old male diagnosed with COVID-19 infection developed behavioral changes, confusion, and insomnia followed by reduced mobility and abnormal eye movements within 48 h of recovery from respiratory symptoms associated with COVID-19. On examination, he had rapid, chaotic, involuntary saccadic, multidirectional eye movements (opsoclonus), and limb myoclonus together with truncal ataxia. CSF analysis, MRI of the brain, and screening for anti-neuronal and encephalitis related antibodies were negative. Extensive testing revealed no underlying malignancy. The patient was successfully treated with intravenous immunoglobulin (IVIG) with complete resolution of symptoms within 4 weeks of treatment.
Conclusion: COVID-19 infection can be associated with the manifestation of opsoclonus myoclonus syndrome, a rare neurological disorder that can be treated with IVIG if not responsive to corticosteroids.
- Following the recovery of respiratory symptoms, SARS-CoV-2 can manifest OMS, a rare neurological disorder.
- OMS manifested by SARS-CoV-2 can have a good response to IVIG in steroid-resistant cases.
Coronavirus disease-2019 (COVID-19), caused by the severe acute respiratory distress syndrome–coronavirus-2 (SARS-CoV-2), is primarily a respiratory infection but has been recently associated with a variety of neurological symptoms (1). Here, we present a case of post-COVID opsoclonus-myoclonus syndrome (OMS), a rare neurological syndrome characterized by a subacute onset of opsoclonus, a disorder of involuntary saccadic eye movements, ataxia, and involuntary multifocal myoclonus mainly affecting the trunk, limbs, or craniocervical region (2, 3).
A 63-year-old male patient, with a history of hypertension and ischemic heart disease, presented with fever, diarrhea, cough, malaise, and sore throat, with high clinical suspicion of COVID-19. The PCR for SARS-CoV-2 was positive, and the patient was managed with conservative clinical care with quarantine. The patient's COVID symptoms recovered in 3 weeks that was correlated with negative a PCR result and positive serum antibody test (IgG) for COVID-19.
Following 48 h of recovery (day 23 after the onset of COVID), the patient developed mental confusion, behavioral changes, and insomnia with a gradual reduction in mobility and abnormality in eye movements. On examination, he had rapid, involuntary saccadic multidirectional eye movements (opsoclonus) (Supplementary Video 1). Marked truncal ataxia and limb myoclonus were also present at this point (Supplementary Video 2). His baseline investigations including complete blood count, urine routine examination, thyroid profile and cerebrospinal fluid (CSF) analysis were within normal limits. Hepatitis B, C, and HIV serology were negative. Chest X-ray, ultrasound of abdomen and pelvis, and MRI of the brain were normal (Table 1). At that point, a presumed diagnosis of OMS was made. OMS is a rare disorder that is thought to be immune mediated, with primarily para-neoplastic or para-infectious etiologies. Our investigations failed to discover any malignancy or para-neoplastic condition in the patient. Additionally, the anti-neuronal antibodies profile and auto-immune encephalitis screen were also negative. Taken together, OMS manifested by the patient appeared to be associated with COVID-19 infection.
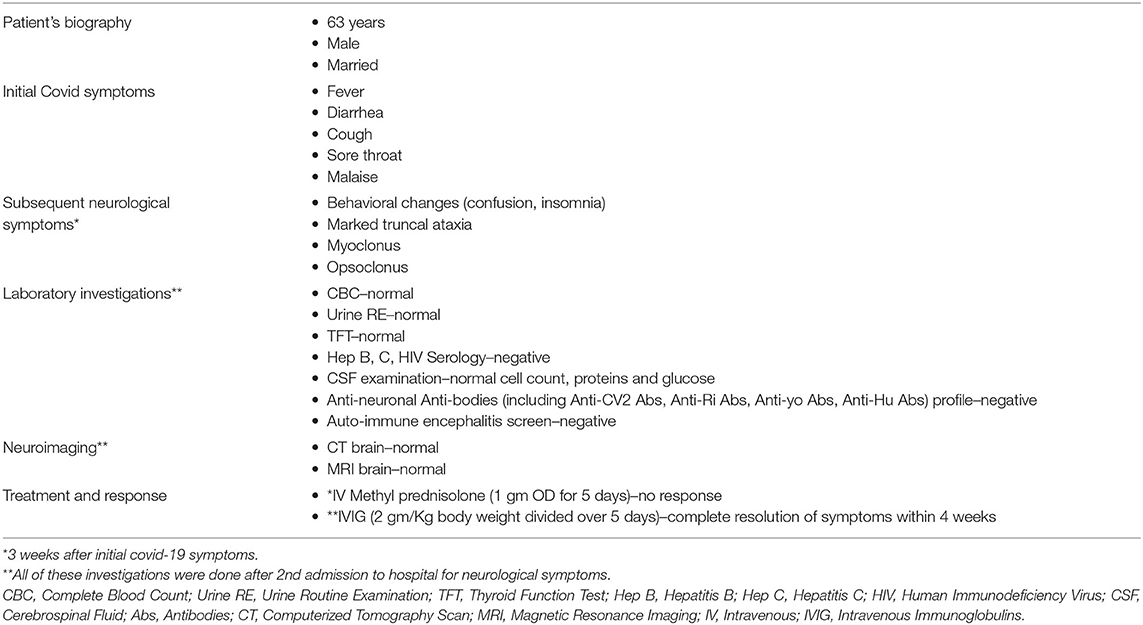
Table 1. Summary of patient features.
Before admission at our neurology ward, the patient was administered with IV methylprednisolone 1 gm OD for 5 days with no response. The patient was given IVIG treatment (2 gm/kg body weight in five divided doses) following 5 days of his last dose of methylprednisolone. Interestingly, we observed gradual but substantial improvement in OMS following IVIG treatment. The patient exhibited complete recovery over the next 4 weeks following immunotherapy (Supplementary Video 3). Subsequent follow-up of the patient to date did not show any recurrence of signs and symptoms of OMS.
Herein we report another case of OMS following COVID-19 infection in an adult. OMS is a rare neuroinflammatory disease of paraneoplastic, parainfectious, toxic/metabolic or idiopathic origin, characterized by opsoclonus, myoclonus, ataxia, and behavioral and sleep disorders (4). The important aspect in clinical features is that opsoclonus might not be present during the time of presentation, which can lead to delay in diagnosis or misdiagnosis as cerebellar ataxia (5).
OMS has been often reported with paraneoplastic etiology such as neuroblastoma (6, 7); however, it can manifest with parainfectious etiology, that is, following viral infections (e.g., enterovirus, Epstein–Barr virus, poliovirus, Coxsackie virus, mumps, West-Nile virus, HIV) or bacterial pathogens (e.g., Salmonella species, parasitic infections like Plasmodium falciparum and Mycobacterium tuberculosis) (4). Additionally, it is important to rule out any toxic-metabolic states caused by cocaine intoxication, phenytoin overdose, or hyperosmolar non-ketotic coma that may lead to OMS symptoms (4, 8). The prognosis of OMS is worse with paraneoplastic etiology, which might show resistance to immunotherapy and can lead to severe encephalopathy or death (9). In contrast, parainfectious or idiopathic OMS responds well to immunotherapy (mainly intravenous immunoglobulins or corticosteroids) (10, 11). A critical aspect in the management of OMS is to rule out underlying malignancy. In our case, there was no evidence of underlying malignancy, so suspicion of a post-infectious etiology is reasonable (4).
The emergence of neurological disorders, particularly OMS following COVID-19 infection, has been recently reported in several studies (2, 3, 12–14). Interestingly, the majority of these COVID patients developing OMS were affected by mild-to-moderate respiratory symptoms as observed in our case (2). Emamikhah et al. reported seven COVID patients affected by OMS who showed normal brain MRI scans and CSF findings as in our case (2). However, none of the patients in this case series had features of encephalopathy (2). By contrast, our patient showed behavioral changes and confusion, which has been typically reported previously with paraneoplastic OMS (4).
Our patient showed complete remission of OMS following immunotherapy within 4 weeks. Previous studies also support that OMS patients showed dramatic recovery with immunotherapy (2, 15). In agreement to our case, another study showed that a patient with generalized myoclonus and ataxia (without opsoclonus) exhibited better response to IVIG compared to high-dose methylprednisolone pulse therapy (16). However, there are reports showing recovery of OMS or myoclonus patients devoid of opsoclonus symptoms patients with IV methylprednisolone (1 g/d) (3).
The exact pathophysiology of OMS is poorly understood. It is hypothesized to have autoimmune etiology because of its response to immunosuppressive therapy, but the specific autoantibodies leading to the disorder have not yet been identified. However, it is proposed that the pathogenesis involves antibodies that react against cerebellar Purkinjie cells (17) since mild cell loss has been described in Purkinjie cell layer, inferior olives, and brainstem along with mild inflammatory changes. Hence, the diagnosis of OMS is based on clinical presentation. Furthermore, there is no specific standard or guideline for treatment, but glucocorticoids with IVIG are commonly used as first-line therapy (10).
Our case provides further evidence that COVID-19 can trigger OMS irrespective of the severity of respiratory symptoms in such patients (2, 3, 12–14). Hence, further research is needed to dissect the underlying pathophysiological mechanisms associated with COVID-19-induced neurological disorders including OMS.
SARS-CoV-2 infection can lead to the manifestation of various neurological events, including a rare autoimmune OMS. This parainfectious OMS presumably caused by COVID-19 showed a dramatic response to IVIG treatment compared to corticosteroids.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
HI, TD, ZU, and MU identified the patient and wrote the first draft of the paper. NK and PM contributed to revising the paper. All authors revised and commented on the final draft.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2021.672524/full#supplementary-material
1. Nordvig AS, Rimmer KT, Willey JZ, Thakur KT, Boehme AK, Vargas WS, et al. Potential neurological manifestations of COVID-19. Neurol Clin Practice. (2020) 11:1–11. doi: 10.1212/CPJ.0000000000000897
2. Emamikhah M, Babadi M, Mehrabani M, Jalili M, Pouranian M, Daraie P, et al. Opsoclonus-myoclonus syndrome, a post-infectious neurologic complication of COVID-19: case series and review of literature. J Neurovirol. (2021) 27:26–34. doi: 10.1007/s13365-020-00941-1
3. Shah PB, Desai DS. Opsoclonus myoclonus ataxia syndrome in the setting of COVID-19 infection. Neurology. (2021) 96:33. doi: 10.1212/WNL.0000000000010978
4. Bataller L, Graus F, Saiz A, Vilchez JJ. Clinical outcome in adult onset idiopathic or paraneoplastic opsoclonus-myoclonus. Brain. (2001) 124:437–43. doi: 10.1093/brain/124.2.437
5. Singer HS, Mink JW, Gilbert DL, Jankovic J. Myoclonus. In: Singer HS, Mink JW, Gilbert DL, Jankovic J, editors. Movement Disorders in Childhood. Philadelphia, PA: Saunders WB (2010) doi: 10.1016/B978-0-7506-9852-8.00011-4
6. De Grandis E, Parodi S, Conte M, Angelini P, Battaglia F, Gandolfo C, et al. Long-term follow-up of neuroblastoma-associated opsoclonus-myoclonus-ataxia syndrome. Neuropediatrics. (2009) 40:103–11. doi: 10.1055/s-0029-1237723
7. Matthay KK, Blaes F, Hero B, Plantaz D, De Alarcon P, Mitchell WG, et al. Opsoclonus myoclonus syndrome in neuroblastoma a report from a workshop on the dancing eyes syndrome at the advances in neuroblastoma meeting in Genoa, Italy, 2004. Cancer Lett. (2005) 228:275–82. doi: 10.1016/j.canlet.2005.01.051
8. Armangué T, Sabater L, Torres-Vega E, Martínez-Hernández E, Ariño H, Petit-Pedrol M, et al. Clinical and immunological features of opsoclonus-myoclonus syndrome in the era of neuronal cell surface antibodies. JAMA Neurol. (2016) 73:417–24. doi: 10.1001/jamaneurol.2015.4607
9. Hammer MS, Larsen MB, Stack VC. Outcome of children with opsoclonus-myoclonus regardless of etiology. Pediatr Neurol. (1995) 13:21–4. doi: 10.1016/0887-8994(95)00083-R
10. Groiss SJ, Siebler M, Schnitzler A. Full recovery of adult onset opsoclonus myoclonus syndrome after early immunotherapy: a case report. Mov Disord. (2011) 26:1805–7. doi: 10.1002/mds.23854
11. Glatz K, Meinck H-M, Wildemann B. Parainfectious opsoclonus-myoclonus syndrome: high dose intravenous immunoglobulins are effective. J Neurol. (2003) 74:279–80. doi: 10.1136/jnnp.74.2.279
12. Urrea-Mendoza E, Okafor K, Ravindran S, Absher J, Chaubal V, Revilla JF. Opsoclonus-Myoclonus-Ataxia Syndrome (OMAS) associated with SARS-CoV-2 Infection: post-infectious neurological complication with benign prognosis. Tremor Other Hyperkinet Mov. (2021) 11:7. doi: 10.5334/tohm.580
13. Sanguinetti SY, Ramdhani AR. Opsoclonus-myoclonus-ataxia syndrome related to the novel coronavirus (COVID-19). J Neuroophthalmol. (2021). doi: 10.1097/WNO.0000000000001129
14. Foucard C, San-Galli A, Tarrano C, Chaumont H, Lannuzel A, Roze E. Acute cerebellar ataxia and myoclonus with or without opsoclonus: a parainfectious syndrome associated with COVID-19. Eur J Neurol. (2021). doi: 10.1111/ene.14726
15. Wiegand SE, Mitchell WG, Santoro DJ. Immunotherapy responsive SARS-CoV-2 infection exacerbating opsoclonus myoclonus syndrome. Multiple Sclerosis Related Disord. (2021) 50:102855. doi: 10.1016/j.msard.2021.102855
16. Dijkstra F, Van den Bossche T, Willekens B, Cras P, Crosiers D. Myoclonus and cerebellar ataxia following coronavirus disease 2019 (COVID-19). Mov Disord Clin Pract. (2020) 7:974–6. doi: 10.1002/mdc3.13049
Keywords: ataxia, COVID-19, movement disorder, neurological disorder, opsoclonus myoclonus syndrome, autoimmue disease
Citation: Ishaq H, Durrani T, Umar Z, Khan N, McCombe P and Ul Haq MA (2021) Post-COVID Opsoclonus Myoclonus Syndrome: A Case Report From Pakistan. Front. Neurol. 12:672524. doi: 10.3389/fneur.2021.672524
Received: 25 February 2021; Accepted: 26 April 2021;
Published: 07 June 2021.
Edited by:
Jorge Matias-Guiu, Complutense University of Madrid, SpainReviewed by:
Enrique Urrea-Mendoza, Prisma Health Neuroscience Associates, United StatesCopyright © 2021 Ishaq, Durrani, Umar, Khan, McCombe and Ul Haq. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pamela McCombe, cGFtZWxhLm1jY29tYmVAdXEuZWR1LmF1; Nemat Khan, bi5raGFuMkB1cS5lZHUuYXU=
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.