
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
POLICY AND PRACTICE REVIEWS article
Front. Neurol. , 21 October 2021
Sec. Multiple Sclerosis and Neuroimmunology
Volume 12 - 2021 | https://doi.org/10.3389/fneur.2021.667398
This article is part of the Research Topic Disease Modifying Therapies in Multiple Sclerosis View all 25 articles
 César Caparó-Zamalloa1,2,3
César Caparó-Zamalloa1,2,3 Victor Velásquez-Rimachi3,4,5
Victor Velásquez-Rimachi3,4,5 Nicanor Mori3,6
Nicanor Mori3,6 Wenzel Ivan Dueñas-Pacheco7
Wenzel Ivan Dueñas-Pacheco7 Andrely Huerta-Rosario4,5,8
Andrely Huerta-Rosario4,5,8 Chandel Farroñay-García4,9
Chandel Farroñay-García4,9 Roberto A. Molina4,5,7
Roberto A. Molina4,5,7 Carlos Alva-Díaz5*
Carlos Alva-Díaz5*Background: Relapsing–remitting multiple sclerosis (RRMS) is a subtype of degenerative inflammatory demyelinating disease of multifactorial origin that affects the central nervous system and leads to multifocal neurological impairment.
Objectives: To develop a clinical pathway (CP) for the management of Peruvian patients with RRMS.
Methods: First, we performed a literature review using Medline, Embase, Cochrane, ProQuest, and Science direct. Then, we structured the information as an ordered and logical series of five topics in a defined timeline: (1) How should MS be diagnosed? (2) How should a relapse be treated? (3) How should a DMT be initiated? (4) How should each DMT be used? and (5) How should the patients be followed?
Results: The personnel involved in the care of patients with RRMS can use a series of flowcharts and diagrams that summarize the topics in paper or electronic format.
Conclusions: We propose the first CP for RRMS in Peru that shows the essential steps for diagnosing, treating, and monitoring RRMS patients based on an evidence-based medicine method and local expert opinions. This CP will allow directing relevant clinical actions to strengthen the multidisciplinary management of RRMS in Peru.
Multiple sclerosis (MS) is a degenerative inflammatory demyelinating disease of multifactorial origin that affects the central nervous system (CNS) and leads to multifocal neurological impairment. It occurs more frequently in young adults aged between 15 and 35, being more frequent in women (1). It is currently considered a complex disease influenced by genetic, epigenetic, and environmental factors (2).
The overall prevalence has been estimated at 30 per 100,000 inhabitants (3). The regions with the highest prevalence of MS are North America with 191.2 cases per 100,000 inhabitants, and Europe, with 96 to 200 cases per 100,000 inhabitants. On the other hand, Asia and sub-Saharan Africa have a lower prevalence with <0.22 per 100,000 inhabitants. In South America, a prevalence of 5.24 cases per 100,000 inhabitants was recorded, particularly in Panama and Argentina (Patagonia), with an estimated prevalence and incidence of 17.2/100,000 and 1.4/100,000, respectively (4, 5). In Peru, the prevalence calculated for Lima was 7.69 per 100,000 inhabitants (6). The current perception is that there is an increase in the prevalence and incidence of this disease that could be explained by increased disease awareness, better access to diagnostic tools, longer survival, and more sensitive diagnostic criteria resulting in better case detection (7, 8).
MS has a varied clinical presentation in which two recognized clinical phenotypes have been described and are characterized by their activity and progression: (1) relapsing MS and (2) progressive MS. However, a clinically isolated syndrome (CIS) and a radiologically isolated syndrome (RIS) have also been described and should be taken into account (9).
Clinical pathways (CP) are a helpful tool for continuous quality improvement in healthcare and facilitate the integration of clinical practice guidelines, protocols, and local algorithms. The advantages of CP are based on optimizing integrated mechanisms that include the appropriate activities necessary to manage specific medical problems (10, 11). Therefore, they allow standardizing diagnosis and treatment while always prioritizing common sense and clinical experience, positively influencing the best professional training, and facilitating teamwork (12, 13).
In 2019, the Peruvian Society of Neurology published a clinical guideline for managing patients with MS to provide neurologists with a valid, updated tool to treat these patients in a comprehensive manner (14). However, a more practical and user-friendly tool was needed to achieve greater acceptance among Peruvian neurologists, thus standardizing the management of Peruvian patients based on quality external information adapted to our context by a group of thematic experts.
Therefore, we developed a CP to diagnose and manage patients with relapsing–remitting MS (RRMS) with summary versions of the recommendations through evidence-based algorithms.
We developed a CP route with the following methodological design criteria aimed at (1) developing a structured multidisciplinary care plan; (2) channeling the translation of guides or tests to local structures; (3) describing the steps of the therapeutic course using a route, an algorithm, a guide, a protocol, or another “inventory of actions”; and (4) standardizing care for a specific clinical problem, procedure, or episode of care in a specific population (15).
To achieve this, we recruited a group of Peruvian neurologists working at public hospitals with over 5 years of experience managing MS and a methodological team with experience in synthesizing evidence. Then, we conducted a review of the literature using different sources (Medline, Embase, Cochrane, ProQuest, and Science direct) with “Multiple Sclerosis, Relapsing–Remitting” as the MeSH term. We identified relevant evidence that covers issues related to the care of patients with RRMS, and during six meetings, we planned and designed five key topics developed in this CP: (1) diagnosis, (2) relapse treatment, (3) initiation of disease-modifying treatment (DMT), (4) use of each DMT, and (5) follow-up.
We organized the present CP as an ordered and logical series of resolved topics in a consecutively defined timeline (Figure 1). In addition, we accompanied this CP with a series of flow diagrams that neurologists can use. This CP for the care of patients with MS could be used in paper or electronic format and consists of the following questions:
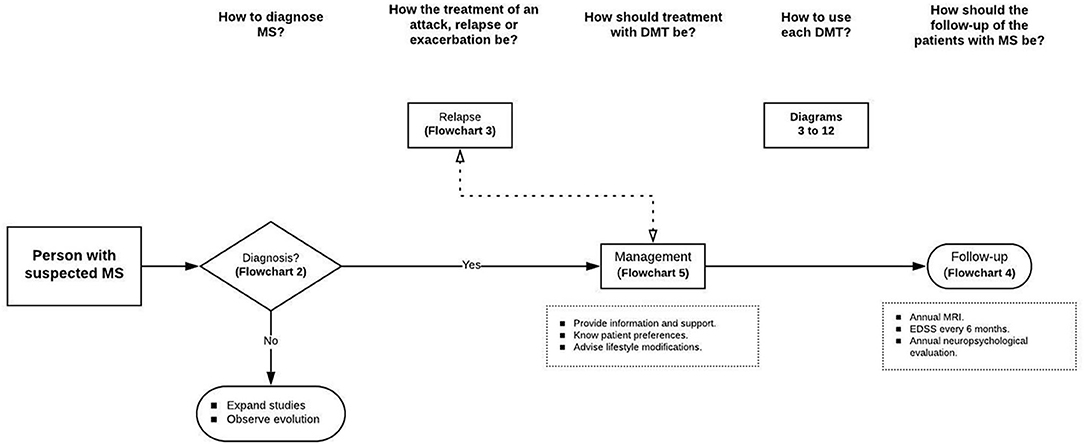
Figure 1. Clinical pathway for diagnosis and treatment of RRMS. Source: Authors.
The initial evaluation must define whether the patient presents with a typical CIS (9) (Additional File 1). Patients with ≥2 lesions on magnetic resonance imaging (MRI) have a high probability of developing MS (16, 17). The McDonald 2017 criteria must be applied to confirm the diagnosis of MS. There are no specific considerations for the Peruvian population except ruling out tuberculosis (18) (Additional File 2). Finally, the prognosis should be assessed according to the following unfavorable outcome factors: age >40 years, male sex, African American or Latin American ethnicity, polyfocal presentation, involvement of the afferent system, and partial or no recovery, all of which can increase the risk of developing aggressive forms of MS (19).
In patients presenting moderate to severe relapse (20–22) (Additional File 3), the first option is intravenous high-dose methylprednisolone pulse therapy (6, 23, 24) (Figure 2). Alternatively, oral methylprednisolone could be used since evidence of a similar effect exists (25–28), but tablets >8 mg are not available in Peru. Another alternative could be oral prednisone 1,250 mg daily; however, 25 tablets per day of prednisone 50 mg make this alternative not suitable. If the patient does not respond favorably or cannot comply with methylprednisolone therapeutic protocol, treatment with therapeutic plasma exchange should be considered (23, 29) (Figure 3).
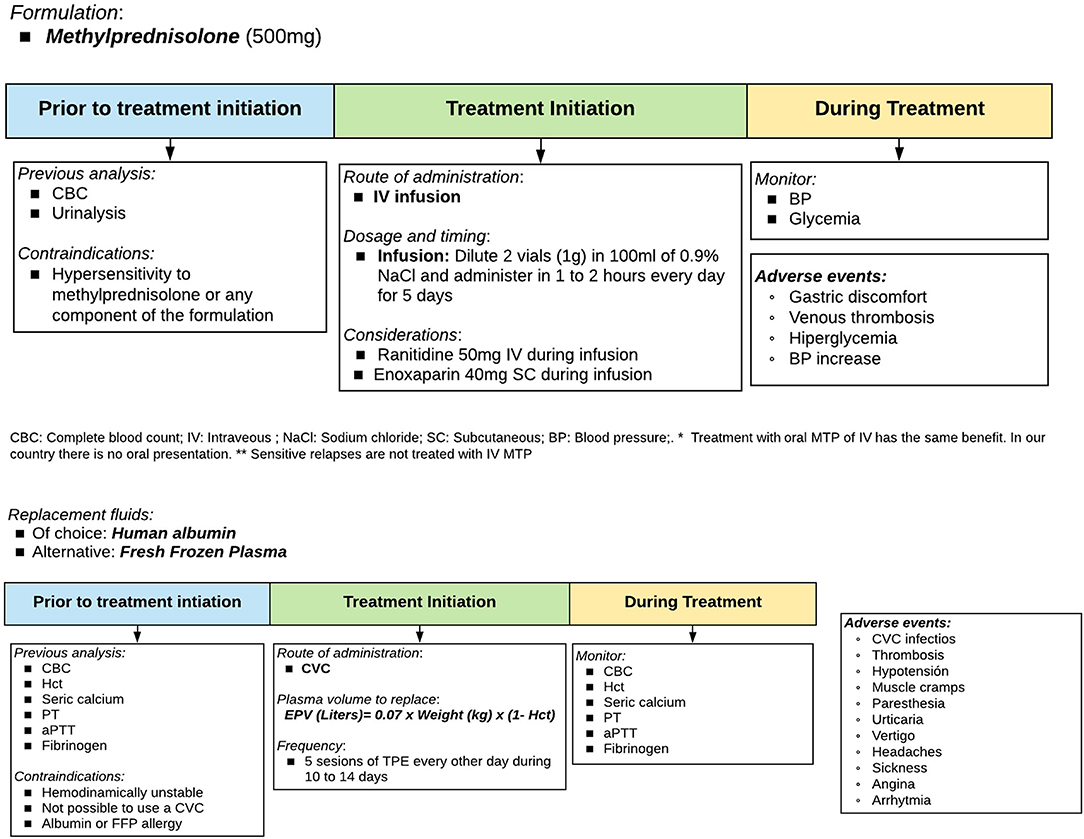
Figure 2. Therapeutic protocol for relapses: Methylprednisolone and therapeutic plasma exchange. Source: Authors.
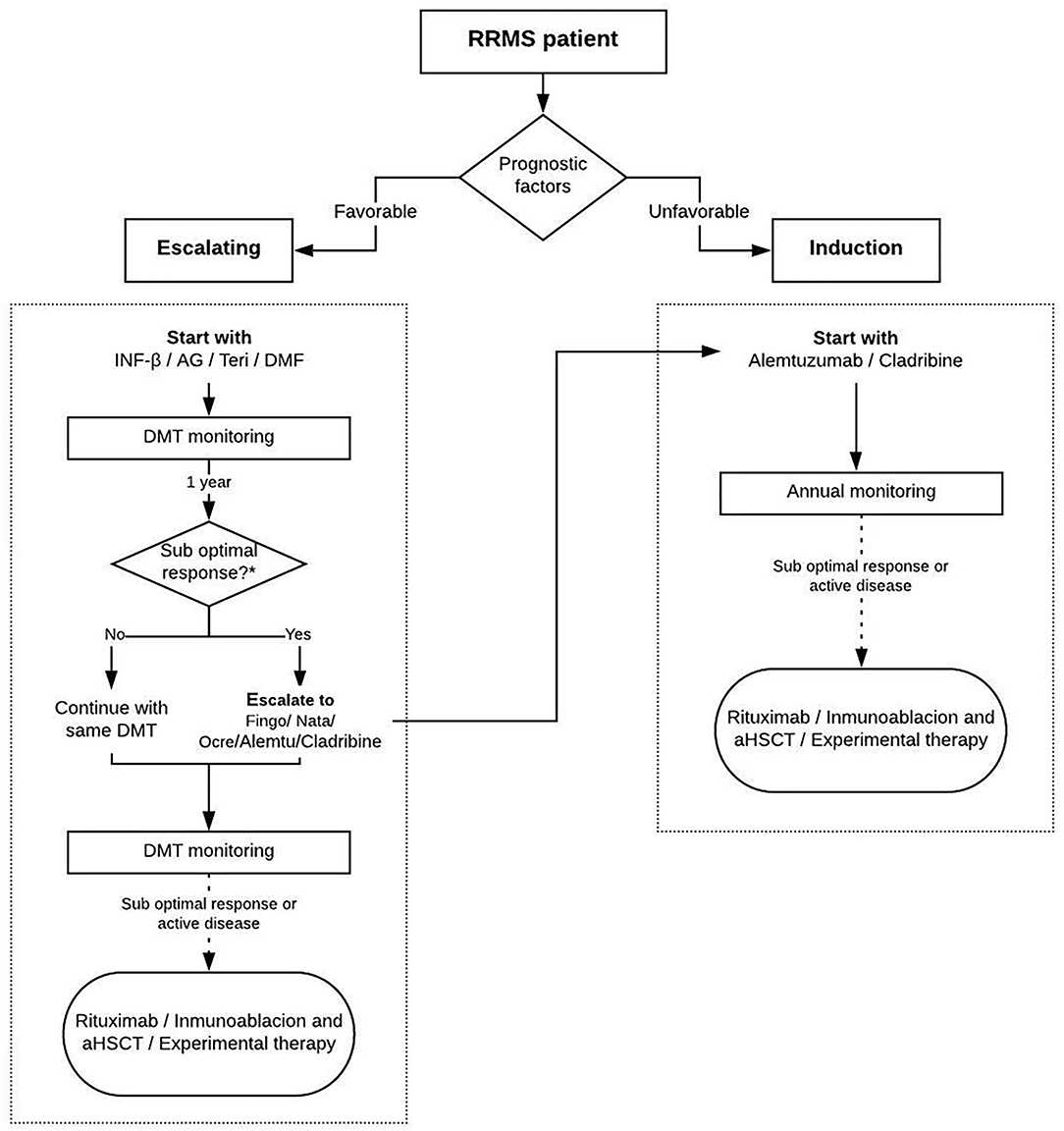
The choice of a DMT should be made according to the patients' characteristics, the evaluation of prognostic factors, the risk–benefit balance of the treatment options, and the experience of the treating neurologist (30–32) (Figure 4). It should be noted that this algorithm is only a reference since high efficacy can also be achieved with first-line therapies depending on the clinical factors. The Modified Rio score should be used to evaluate the treatment response with IFN, teriflunomide, and glatiramer acetate at 12 months later (33–35). For the remaining DMTs, clinical and imaging assessments should be performed every year (Additional File 4).
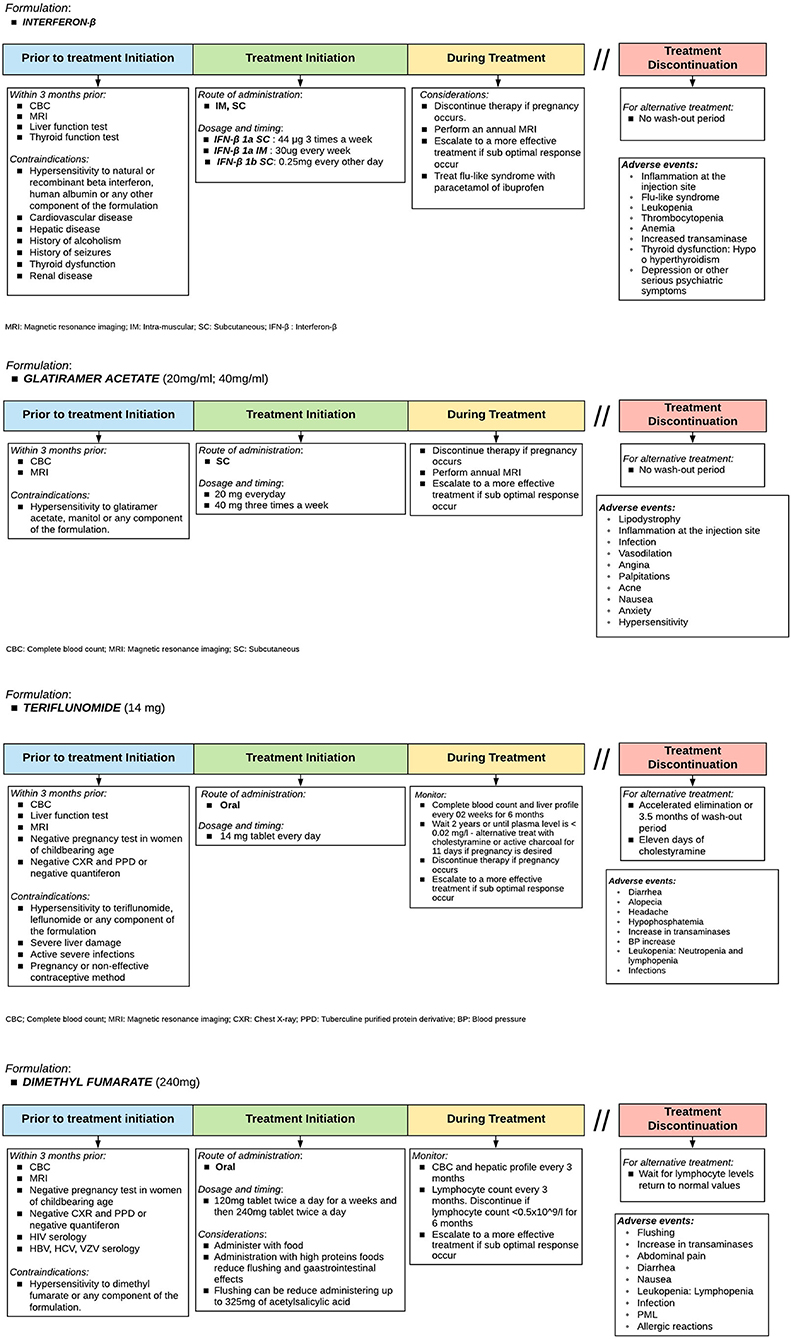
Figure 4. Therapeutic protocol for induction: Interferon-β, glatiramer acetate, teriflunomide, and dimethyl fumarate. Adapted from Sorensen et al. (33).
There are several DMT for RRMS treatment (14, 36, 37). However, specific tests are needed before initiating treatment. It is also important to know patient preferences and provide advice on individual general recommendations (38). Figures 5, 6 show diagrams describing the use of each DMT (1, 38–50).
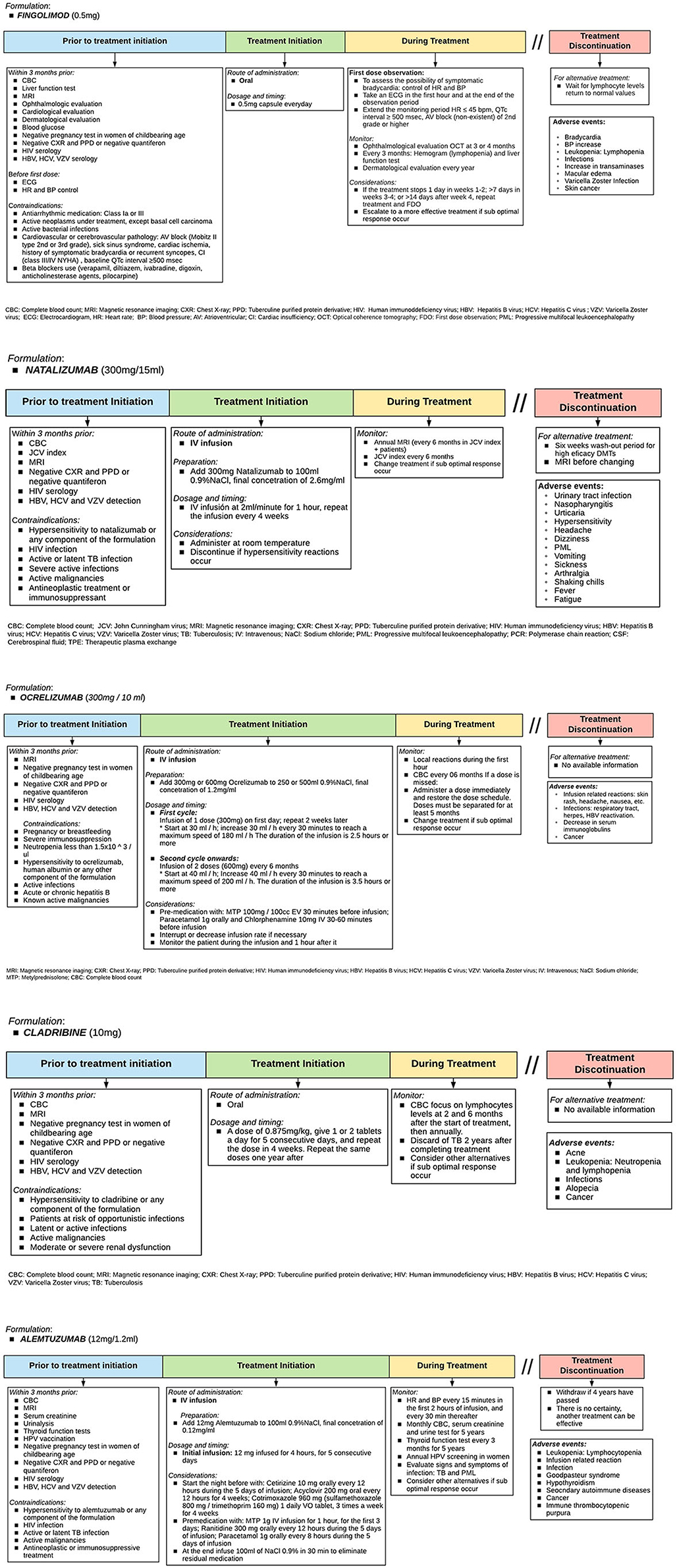
Figure 5. Therapeutic protocol for escalating: Fingolimod, natalizumab, ocrelizumab, cladribine, and alemtuzumab. Adapted from Sorensen et al. (33).
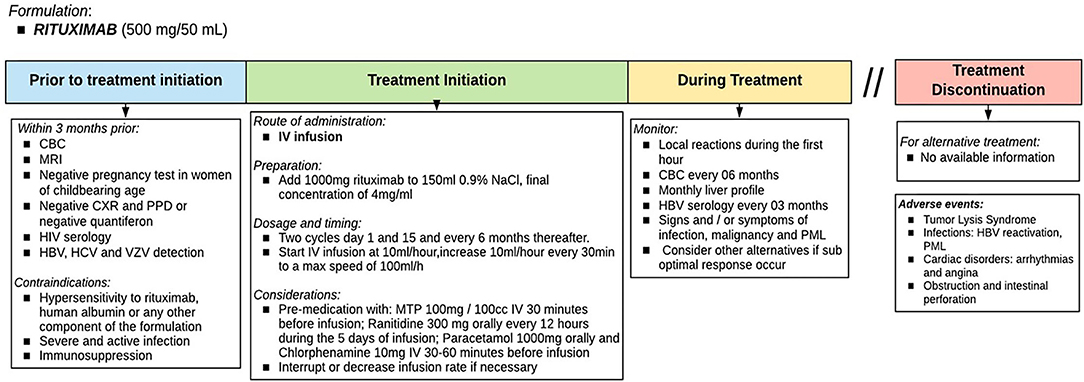
Figure 6. Therapeutic protocol for failure: Rituximab. The indication of rituximab as a DMT in RRMS has not yet been approved in Peru and is used as an off-label indication. Source: Authors.
After treatment initiation, a brain MRI must be obtained annually, and a spinal MRI should be requested only if spinal cord symptoms occurred (51). In addition, experts suggest a comprehensive clinical assessment including biannually Expanded Disability Status Scale (EDSS) and annually neuropsychological evaluations (Expert consensus) (33, 34).
No evidence of disease activity (NEDA) considering no relapses, no increase of disability (as measured with EDSS), and no new or active MRI lesions can also be used as a treatment objective (52, 53).
Patients with RRMS are young and present a chronic and disabling evolution, making it necessary to perform a multidisciplinary approach. This disease is characterized by an often-unpredictable course making diagnosis difficult and the choice of the adequate DMT for each patient challenging (1, 14, 54).
The clinical variability of RRMS requires a multidisciplinary intervention by healthcare professionals, making adequate resource management a necessity to reduce morbidity and disability, and thereby improve the quality of life of individuals with this disease. The use of the proposed CP will allow patients to receive relevant, timely clinical interventions and significantly reduce the use of hospital resources, without negatively affecting the length of stay and hospital costs (54–56).
Our CP indicates the steps to be followed in the initial phase of diagnosis, then in the treatment and monitoring phase, and finally during patient follow-up. We propose a current and adapted list of diagrams to guide DMT use in the Peruvian population based on the previous proposal by Sorensen et al. (38), which explains the tests to be made before, during, and after initiating treatment in chronological order as well as possible treatment schemes that neurologists can choose and how to perform monitoring.
There are limitations for MS diagnosis in Peru due to the difficult access to specialists access and MRI (16); therefore, there is a delay between the first clinical outbreak and the confirmatory diagnosis of up to 3.2 years (57). In addition, there are difficulties in accessing timely treatment because public institutions only have interferon and glatiramer acetate as the DMT scale. Moreover, to access induction DMT, it is necessary to evaluate a case for at least 12 months, classify it as a therapeutic failure and make a request for the new treatment that takes an average of 4–6 months, delaying the start of treatment with more significant disability and lower quality of life (16).
We organized several meetings with methodologists and neurologists to adapt the selected external information on the management of RRMS to the national context to resolve this. Our CP is innovative and is the first approach to integrating processes oriented at the diagnostic and therapeutic resources available for RRMS in Peru.
We have proposed the first CP for RRMS in Peru with a chronological description of the steps to follow for the diagnosis, treatment, and follow-up of RRMS patients. This will be a helpful tool for Peruvian neurologists in order to carry out a systematic process for the care of persons with MS.
We hope that the use of this CP will have a real impact on continuous improvement in the care and quality of health provided by neurologists, which will be reflected by the satisfaction perceived by Peruvian RRMS patients. Finally, we believe that this CP for diagnosing and managing patients with RRMS will be an essential tool for encouraging correct and methodical approaches to the disease based on quality scientific-technical evidence, generating standard use of treatments and rational use of health resources.
CA-D, VV-R, NM, CC-Z, and WD-P participated in meetings to plan, design, and elaborate on the clinical pathway. VV-R, AH-R, RM, and CF-G identified relevant studies to support the clinical pathway. VV-R, AH-R, and CA-D participated in the writing of the manuscript. All authors designed the study and approved the final version of the manuscript.
Hoffmann–La Roche Pharmaceutical provided financing for the execution and publication of the clinical pathway.
The authors declare that this study received funding from Hoffmann-La Roche Pharmaceutical. The funder had the following involvement in the study: provided financing for the execution and publication of the clinical pathway.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors wish to thank Ana M. Solís Quispe, MD, for her support and suggestions during the writing of the manuscript. The authors also acknowledge Soelberg Sorensen, MD, for permitting us to adapt some management diagrams from its review proposal.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2021.667398/full#supplementary-material
Additional File 1. MS diagnostic approach. Source: Huamani et al. (16) and Kuhler et al. (17).
Additional File 2. Diagnostic protocol: Mc Donald criteria 2017. Source: Thompson et al. (18).
Additional File 3. Relapse treatment of patients with MS. Source: Berkovich et al. (23, 26) and Correale et al. (21).
Additional File 4. Assessment of treatment response modified Rio score. Source: Sormani et al. (33, 34).
1. Filippi M, Bar-Or A, Piehl F, Preziosa P, Solari A, Vukusic S. Multiple sclerosis. Nat Rev Dis Prim. (2018) 4:43. doi: 10.1038/s41572-018-0041-4
2. Cook SD. Handbook of Multiple Sclerosis. Boca Raton, FL: Taylor & Francis (2006). p. 511. doi: 10.3109/9781420018714
3. Kurtzke JF. Multiple sclerosis in time and space–geographic clues to cause. J Neuroviral. (2000) 6(Suppl. 2):S134–40.
4. Browne P, Chandraratna D, Angood C, Tremlett H, Baker C, Taylor BV, et al. Atlas of multiple sclerosis 2013: a growing global problem with widespread inequity. Neurology. (2014) 83:1022–4. doi: 10.1212/WNL.0000000000000768
5. Smets I, Van Deun L, Bohyn C, van Pesch V, Vanopdenbosch L, Dive D, et al. Corticosteroids in the management of acute multiple sclerosis exacerbations. Acta Neurol Belgica. (2017) 117:623–33. doi: 10.1007/s13760-017-0772-0
6. Vizcarra Escobar D, Kawano Castillo J, Castañeda Barba C, Chereque Gutierrez A, Tipismana Barbarán M, Bernabé Ortiz A, et al. Prevalencia de Esclerosis Múltiple en Lima – Perú. Rev Med Herediana. (2012) 20:146. doi: 10.20453/rmh.v20i3.1014
7. Barkhof F, Filippi M, Miller DH, Scheltens P, Campi A, Polman CH, et al. Comparison of MRI criteria at first presentation to predict conversion to clinically definite multiple sclerosis. Brain. (1997) 120 (Pt 11):2059–69. doi: 10.1093/brain/120.11.2059
8. Polman CH, Reingold SC, Banwell B, Clanet M, Cohen JA, Filippi M, et al. Diagnostic criteria for multiple sclerosis: 2010 Revisions to the McDonald criteria. Ann Neurol. (2011) 69:292–302. doi: 10.1002/ana.22366
9. Lublin FD, Reingold SC, Cohen JA, Cutter GR, Sorensen PS, Thompson AJ, et al. Defining the clinical course of multiple sclerosis: the 2013 revisions. Neurology. (2014) 83:278–86. doi: 10.1212/WNL.0000000000000560
10. Campbell H, Hotchkiss R, Bradshaw N, Porteous M. Integrated care pathways. BMJ. (1998) 316:133–7. doi: 10.1136/bmj.316.7125.133
11. Isla-Guerrero A, Álvarez-Ruiz F, Aranda-Armengod B, Sarmiento-Martínez M, Pérez-Álvarez M, Chamorro-Ramos L, et al. Diseño, implantación y resultados de la vía clínica para la cirugía de la hernia de disco lumbar. Neurocirugía. (2001) 12:409–18. doi: 10.1016/S1130-1473(01)70679-3
12. Hunter B, Segrott J. Re-mapping client journeys and professional identities: a review of the literature on clinical pathways. Int J Nurs Stud. (2008) 45:608–25. doi: 10.1016/j.ijnurstu.2007.04.001
13. Vanhaecht K, De Witte K, Panella M, Sermeus W. Do pathways lead to better organized care processes? J Eval Clin Pract. (2009) 15:782–8. doi: 10.1111/j.1365-2753.2008.01068.x
14. Vizcarra Darwin R, Cruz Ana G, Rojas Edgar, Mori Nicanor, Caparó César, Castañeda Carlos C, et al. Guía de práctica clínica para el diagnóstico y tratamiento de Esclerosis Múltiple en Adultos. Rev Neurop. (2019) 82:242–57. doi: 10.20453/rnp.v82i4.3646
15. Lawal AK, Rotter T, Kinsman L, Machotta A, Ronellenfitsch U, Scott SD, et al. What is a clinical pathway? Refinement of an operational definition to identify clinical pathway studies for a Cochrane systematic review. BMC Med. (2016) 14:35. doi: 10.1186/s12916-016-0580-z
16. Huamaní C, Rojas E, Inca JJAMP. Esclerosis múltiple de alta actividad:¿ se puede iniciar precozmente el tratamiento con drogas de alta eficacia? Acta Méd Peruana. (2017) 34:301–8. doi: 10.35663/amp.2017.344.463
17. Kuhle J, Disanto G, Dobson R, Adiutori R, Bianchi L, Topping J, et al. Conversion from clinically isolated syndrome to multiple sclerosis: a large multicentre study. Mult Scler. (2015) 21:1013–24. doi: 10.1177/1352458514568827
18. Thompson AJ, Banwell BL, Barkhof F, Carroll WM, Coetzee T, Comi G, et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. (2018) 17:162–73. doi: 10.1016/S1474-4422(17)30470-2
19. Freedman MS, Rush CA. Severe, highly active, or aggressive multiple sclerosis. Continuum. (2016) 22:761–84. doi: 10.1212/CON.0000000000000331
20. Berkovich RR. Acute multiple sclerosis relapse. Continuum. (2016) 22:799–814. doi: 10.1212/CON.0000000000000330
21. Correale J, Abad P, Alvarenga R, Alves-Leon S, Armas E, Barahona J, et al. Management of relapsing–remitting multiple sclerosis in Latin America: practical recommendations for treatment optimization. J Neurol Sci. (2014) 339:196–206. doi: 10.1016/j.jns.2014.02.017
22. Freedman MS, Devonshire V, Duquette P, Giacomini PS, Giuliani F, Levin MC, et al. Treatment optimization in multiple sclerosis: Canadian MS Working Group Recommendations. Can J Neurol Sci. (2020) 47:437–55. doi: 10.1017/cjn.2020.66
23. Berkovich R. Treatment of acute relapses in multiple sclerosis. In: Translational Neuroimmunology in Multiple Sclerosis. Los Angeles, CA: Elsevier (2016). p. 307–26. doi: 10.1016/B978-0-12-801914-6.00024-6
24. Scott TF, Frohman EM, De Seze J, Gronseth GS, Weinshenker BG, Therapeutics, et al. Evidence-based guideline: clinical evaluation and treatment of transverse myelitis: report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology. (2011) 77:2128–34. doi: 10.1212/WNL.0b013e31823dc535
25. Ramo-Tello C, Grau-López L, Tintoré M, Rovira A, Ramió i Torrenta L, Brieva L, et al. A randomized clinical trial of oral versus intravenous methylprednisolone for relapse of MS. Mult Scler. (2014) 20:717–25. doi: 10.1177/1352458513508835
26. Morrow SA, Stoian CA, Dmitrovic J, Chan SC, Metz LM. The bioavailability of IV methylprednisolone and oral prednisone in multiple sclerosis. Neurology. (2004) 63:1079–80. doi: 10.1212/01.WNL.0000138572.82125.F5
27. Le Page E, Veillard D, Laplaud DA, Hamonic S, Wardi R, Lebrun C, et al. Oral versus intravenous high-dose methylprednisolone for treatment of relapses in patients with multiple sclerosis (COPOUSEP): a randomised, controlled, double-blind, non-inferiority trial. Lancet. (2015) 386:974–81. doi: 10.1016/S0140-6736(15)61137-0
28. Barnes D, Hughes RA, Morris RW, Wade-Jones O, Brown P, Britton T, et al. Randomised trial of oral and intravenous methylprednisolone in acute relapses of multiple sclerosis. Lancet. (1997) 349:902–6. doi: 10.1016/S0140-6736(96)06453-7
29. Schwartz J, Padmanabhan A, Aqui N, Balogun RA, Connelly-Smith L, Delaney M, et al. Guidelines on the use of therapeutic apheresis in clinical practice-evidence-based approach from the Writing Committee of the American Society for Apheresis: the Seventh Special Issue. J Clin Apheresis. (2016) 31:149–338. doi: 10.1002/jca.21470
30. Freedman MS, Selchen D, Prat A, Giacomini PS. Managing Multiple Sclerosis: treatment Initiation, Modification, and Sequencing. Can J Neurol Sci. (2018) 45:489–503. doi: 10.1017/cjn.2018.17
31. Giovannoni G. Disease-modifying treatments for early and advanced multiple sclerosis: a new treatment paradigm. Curr Opin Neurol. (2018) 31:233–43. doi: 10.1097/WCO.0000000000000561
32. Tintore M, Vidal-Jordana A, Sastre-Garriga J. Treatment of multiple sclerosis - success from bench to bedside. Nat Rev Neurol. (2019) 15:53–8. doi: 10.1038/s41582-018-0082-z
33. Sormani MP, De Stefano N. Defining and scoring response to IFN-beta in multiple sclerosis. Nat Rev Neurol. (2013) 9:504–12. doi: 10.1038/nrneurol.2013.146
34. Sormani MP, Rio J, Tintore M, Signori A, Li D, Cornelisse P, et al. Scoring treatment response in patients with relapsing multiple sclerosis. Mult Scler. (2013) 19:605–12. doi: 10.1177/1352458512460605
35. Vermersch P, De Sèze J, Clavelou P, Durand-Dubief F, Maillart E, Mekies C, et al. Expert opinion: criteria for second-line treatment failure in patients with multiple sclerosis. Mult Scler Relat Disord. (2019) 36:101406. doi: 10.1016/j.msard.2019.101406
36. Lucchetta RC, Tonin FS, Borba HHL, Leonart LP, Ferreira VL, Bonetti AF, et al. Disease-modifying therapies for relapsing-remitting multiple sclerosis: a network meta-analysis. CNS Drugs. (2018) 32:813–26. doi: 10.1007/s40263-018-0541-5
37. Scolding N, Barnes D, Cader S, Chataway J, Chaudhuri A, Coles A, et al. Association of British Neurologists: revised (2015) guidelines for prescribing disease-modifying treatments in multiple sclerosis. Pract Neurol. (2015) 15:273–9. doi: 10.1136/practneurol-2015-001139
38. Soelberg Sorensen P. Safety concerns and risk management of multiple sclerosis therapies. Acta Neurol Scand. (2017) 136:168–86. doi: 10.1111/ane.12712
39. Dumitrescu L, Constantinescu CS, Tanasescu R. Siponimod for the treatment of secondary progressive multiple sclerosis. Expert Opin Pharmacother. (2019) 20:143–50. doi: 10.1080/14656566.2018.1551363
40. Gelfand JM, Cree BAC, Hauser SL. Ocrelizumab and other CD20(+) B-cell-depleting therapies in multiple sclerosis. Neurotherapeutics. (2017) 14:835–41. doi: 10.1007/s13311-017-0557-4
41. Giovannoni G, Comi G, Cook S, Rammohan K, Rieckmann P, Soelberg Sorensen P, et al. A placebo-controlled trial of oral cladribine for relapsing multiple sclerosis. The New England journal of medicine. (2010) 362:416–26. doi: 10.1056/NEJMoa0902533
42. Jakimovski D, Weinstock-Guttman B, Ramanathan M, Kolb C, Hojnacki D, Minagar A, et al. Ocrelizumab: a B-cell depleting therapy for multiple sclerosis. Expert Opin Biol Ther. (2017) 17:1163–72. doi: 10.1080/14712598.2017.1347632
43. Juanatey A, Blanco-Garcia L, Tellez N. Ocrelizumab: its efficacy and safety in multiple sclerosis. Rev Neurol. (2018) 66:423–33. doi: 10.33588/rn.6612.2018132
44. Kappos L, Bar-Or A, Cree BAC, Fox RJ, Giovannoni G, Gold R. Siponimod versus placebo in secondary progressive multiple sclerosis (EXPAND): a double-blind, randomised, phase 3 study. Lancet. (2018) 391:1263–73. doi: 10.1016/S0140-6736(18)30475-6
45. Leist TP, Comi G, Cree BA, Coyle PK, Freedman MS, Hartung HP, et al. Effect of oral cladribine on time to conversion to clinically definite multiple sclerosis in patients with a first demyelinating event (ORACLE MS): a phase 3 randomised trial. Lancet Neurol. (2014) 13:257–67. doi: 10.1016/S1474-4422(14)70005-5
46. Naegelin Y, Naegelin P, von Felten S, Lorscheider J, Sonder J, Uitdehaag BMJ, et al. Association of rituximab treatment with disability progression among patients with secondary progressive multiple sclerosis. JAMA Neurol. (2019) 76:274–81. doi: 10.1001/jamaneurol.2018.4239
47. Thomas K, Ziemssen T. Management of fingolimod in clinical practice. Clin Neurol Neurosurg. (2013) 115(Suppl. 1):S60–4. doi: 10.1016/j.clineuro.2013.09.023
48. Whittam DH, Tallantyre EC, Jolles S, Huda S, Moots RJ, Kim HJ, et al. Rituximab in neurological disease: principles, evidence and practice. Pract Neurol. (2019) 19:5–20. doi: 10.1136/practneurol-2018-001899
49. Salzer J, Svenningsson R, Alping P, Novakova L, Björck A, Fink K, et al. Rituximab in multiple sclerosis: a retrospective observational study on safety and efficacy. Neurology. (2016) 87:2074–81. doi: 10.1212/WNL.0000000000003331
50. Hauser SL, Waubant E, Arnold DL, Vollmer T, Antel J, Fox RJ, et al. B-cell depletion with rituximab in relapsing-remitting multiple sclerosis. N Engl J Med. (2008) 358:676–88. doi: 10.1056/NEJMoa0706383
51. Montalban X, Gold R, Thompson AJ, Otero-Romero S, Amato MP, Chandraratna D, et al. ECTRIMS/EAN Guideline on the pharmacological treatment of people with multiple sclerosis. Mult Scler. (2018) 24:96–120. doi: 10.1177/1352458517751049
52. Hegen H, Bsteh G, Berger T. ‘No evidence of disease activity' - is it an appropriate surrogate in multiple sclerosis? Eur J Neurol. (2018) 25:1107-e101. doi: 10.1111/ene.13669
53. Sloane JA, Mainero C, Kinkel RP. No evidence of disease activity in multiple sclerosis. JAMA Neurol. (2015) 72:835–6. doi: 10.1001/jamaneurol.2015.0587
54. Oreja-Guevara C, Miralles A, Garcia-Caballero J, Noval S, Gabaldon L, Esteban-Vasallo MD, et al. [Clinical pathways for the care of multiple sclerosis patients]. Neurologia. (2010) 25:156–62. doi: 10.1016/S2173-5808(10)70031-6
55. Allen D, Rixson L. How has the impact of 'care pathway technologies' on service integration in stroke care been measured and what is the strength of the evidence to support their effectiveness in this respect? Int J Evid Based Healthc. (2008) 6:78–110. doi: 10.1097/01258363-200803000-00005
56. Rotter T, Kinsman L, James E, Machotta A, Gothe H, Willis J, et al. Clinical pathways: effects on professional practice, patient outcomes, length of stay and hospital costs. Cochrane Database Syst Rev. (2010) Cd006632. doi: 10.1002/14651858.CD006632.pub2
Keywords: multiple sclerosis, relapsing-remitting, patient care management, critical pathways, Peru
Citation: Caparó-Zamalloa C, Velásquez-Rimachi V, Mori N, Dueñas-Pacheco WI, Huerta-Rosario A, Farroñay-García C, Molina RA and Alva-Díaz C (2021) Clinical Pathway for the Diagnosis and Management of Patients With Relapsing–Remitting Multiple Sclerosis: A First Proposal for the Peruvian Population. Front. Neurol. 12:667398. doi: 10.3389/fneur.2021.667398
Received: 12 February 2021; Accepted: 09 September 2021;
Published: 21 October 2021.
Edited by:
Mahsa Ghajarzadeh, Universal Scientific Education and Research Network, IranReviewed by:
Fritz Leutmezer, Medical University of Vienna, AustriaCopyright © 2021 Caparó-Zamalloa, Velásquez-Rimachi, Mori, Dueñas-Pacheco, Huerta-Rosario, Farroñay-García, Molina and Alva-Díaz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Carlos Alva-Díaz, Y2FsdmFkQGNpZW50aWZpY2EuZWR1LnBl
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.