
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurol. , 09 June 2021
Sec. Epilepsy
Volume 12 - 2021 | https://doi.org/10.3389/fneur.2021.666056
 Attila Rácz1*
Attila Rácz1* Albert J. Becker2Carlos M. Quesada1Valeri Borger3Hartmut Vatter3Rainer Surges1
Albert J. Becker2Carlos M. Quesada1Valeri Borger3Hartmut Vatter3Rainer Surges1 Christian E. Elger1
Christian E. Elger1Purpose: Focal cortical dysplasias (FCDs) are a frequent cause of drug-resistant focal epilepsies. These lesions are in many cases amenable to epilepsy surgery. We examined 12-month and long-term post-surgical outcomes and its predictors including positive family history of epilepsy.
Methods: Twelve-month and long-term outcomes regarding seizure control after epilepsy surgery in patients operated on with FCD type II between 2002 and 2019 in the Epilepsy Center of Bonn were evaluated based on patient records and telephone interviews.
Results: Overall, 102 patients fulfilled the inclusion criteria. Seventy-one percent of patients at 12 months of follow-up (FU) and 54% of patients at the last available FU (63 ± 5.00 months, median 46.5 months) achieved complete seizure freedom (Engel class IA), and 84 and 69% of patients, respectively, displayed Engel class I outcome. From the examined variables [histopathology: FCD IIA vs. IIB, lobar lesion location: frontal vs. non-frontal, family history for epilepsy, focal to bilateral tonic–clonic seizures (FTBTCS) in case history, completeness of resection, age at epilepsy onset, age at surgery, duration of epilepsy], outcomes at 12 months were determined by interactions of age at onset, duration of epilepsy, age at surgery, extent of resection, and lesion location. Long-term post-surgical outcome was primarily influenced by the extent of resection and history of FTBTCS. Positive family history for epilepsy had a marginal influence on long-term outcomes only.
Conclusion: Resective epilepsy surgery in patients with FCD II yields very good outcomes both at 12-month and long-term follow-ups. Complete lesion resection and the absence of FTBTCS prior to surgery are associated with a better outcome.
Focal cortical dysplasias (FCDs) are frequent causes for medically difficult-to-treat epilepsy both in childhood and adulthood (1, 2). FCDs are highly epileptogenic (3, 4), with a distinct pattern of wiring and electrophysiological properties of cellular components (5). Functional alterations of GABAergic and parvalbumin cells have also been demonstrated in surgical specimens from FCDs (6). FCDs are primarily classified according to the Palmini–Taylor system (7), and this system was adopted and extended by the International League Against Epilepsy (ILAE) in 2011 (8). Epilepsy onset with FCD is typically at a young age or childhood (2); however, the age distribution is broad and late onset is not a rare phenomenon either (9). FCDs are primarily localized to the frontal lobe (10–13). Epilepsy surgery often confers seizure freedom to these patients (10–12, 14–22). For post-surgical seizure freedom, the removal of cortical portions of the FCD is necessary and also sufficient, and the removal of subcortical pieces is not a prerequisite (10). Post-surgical outcome regarding seizure control in different FCD subtypes is reported to be different (19, 20, 23, 24). A significant proportion of patients with FCD display positive family history for epilepsy (9), a phenomenon that might be related to genetic factors underlying the formation of FCDs, especially DEPDC5 (25, 26), NPRL2 (27) and NPRL3 (28), and PI3K/AKT (29, 30).
In the Epilepsy Center of Bonn, more than 100 patients were operated on with FCDs during the last 20 years. In this study, we evaluated the case history of these patients by examining their clinical records and focused on long-term outcomes and also evaluated the influence of possible predictors, especially that of family history for epilepsy on post-surgical outcome. In addition, we investigated the possible effect of diagnostic developments on post-surgical outcomes on a longitudinal basis over almost 20 years.
We analyzed the clinical charts and records of patients operated on with FCD type II due to their pharmacoresistant epilepsy at the Epilepsy Center of University Hospital Bonn between 2002 and the beginning of 2019 and who also had in- or outpatient visit in our department at least in the context of 12 months post-surgical follow-up (FU). Before surgery, these patients underwent a comprehensive pre-surgical diagnostic workup including brain MRI (1.5 or 3 T field strength), video-EEG monitoring with recording of habitual seizures, neuropsychological evaluation and, in certain cases, MRI post-processing [MAP07 analysis (31, 32)], PET, and ictal/interictal SPECT [SISCOM analysis (33)]. All patients in the reported series had positive MRI; however, in certain cases, several MRI images were needed to delineate the lesion. Patients with dual pathologies were excluded from further analysis. In addition, cases with operation in another center before being evaluated in our department were also discarded. After these inclusion and exclusion criteria, 102 patients were enrolled in the study. In 48 patients (47.06%), further invasive diagnostics was performed, as the non-invasive diagnostics was not conclusive enough. Histopathological confirmation of FCD and further evaluation were performed at the Department of Neuropathology of the University Bonn according to the Palmini–Taylor classification (7). The analyzed patients exclusively had FCD type II, and FCD types I and III were not included. As the ILAE classification (8) also relies on the Palmini–Taylor classification for FCD type II, the ILAE classification and the Palmini–Taylor system give identical results for the current series. Outcomes were primarily extracted from patient charts and letters in our digital database. Patients without any visit in our clinic during the last 12 months preceding study evaluation were contacted in the form of phone interviews after giving written informed consent. Outcomes regarding seizure control were presented according to the Engel classification (34). Some portions and aspects of data (age at epilepsy onset, regional distribution of FCDs, outcomes in a smaller or partially overlapping subset of patients with FCDs) have been analyzed according to different aspects and published elsewhere (9–11). Outcomes at 12 months and at the longest available FU were analyzed separately. For patients operated on twice, outcomes resulting after the first operation were used for the analysis in order to be able to draw conclusions regarding completeness of resection and to avoid further heterogeneities in the patient collective. For statistical analysis, the statistical toolbox of Matlab (MathWorks, Natick) was applied. The influence of possible predictor variables on post-surgical outcome was first tested with univariate analysis, where group comparisons regarding post-surgical outcome [Engel class as the categorical variable and, in a further step, dichotomized outcomes: excellent (Engel I) vs. not excellent (Engel II–IV), favorable (Engel I–II) vs. unfavorable (Engel III–IV) outcome] were performed with Pearson's chi-square statistics and Fisher's exact test. Outcomes at 12 months and at the longest FU for the same patient groups (comparison for the complete series and for patients operated on in different time periods) were compared with the sign test. Afterwards, we applied a multivariate logistic regression analysis with a stepwise regression analysis to verify and to test the influence of a number of possible predictor variables on post-surgical outcome. p-values below 0.05 were accepted as an indicator of statistical significance. Charts were generated with the Matlab plotting toolbox and subsequently refined with Paint. The study was carried out after approval from the local ethics committee of the University Hospital Bonn (nr. 126/19). Because of its retrospective nature, informed consent was required only for the phone interviews.
The present analysis comprised 102 patients who had been operated on with histologically verified FCD II between 2002 and the beginning of 2019 in our department. Further characteristics of these patient groups are outlined in Table 1. Histopathological analysis revealed FCD IIA in 22 and FCD IIB in 80 cases. At 12 months of FU, 70.59% of patients were completely seizure free (Engel class IA), and altogether, 84.31% could be categorized as Engel class I [72 patients with IA, 14 patients (13.73%) with IB/IC/ID, 4 patients (3.92%) with Engel class II, 7 (6.86%) with Engel class III, and 5 (4.9%) with Engel class IV outcome; see Figure 1].
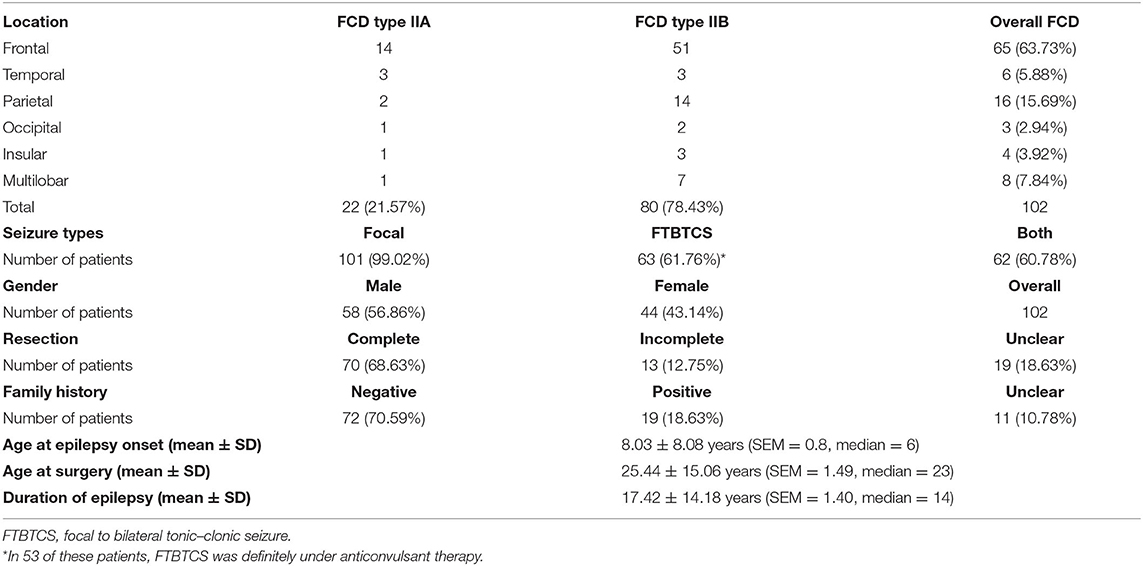
Table 1. Basic characteristics of patients operated on with medically refractory epilepsy and FCD II.
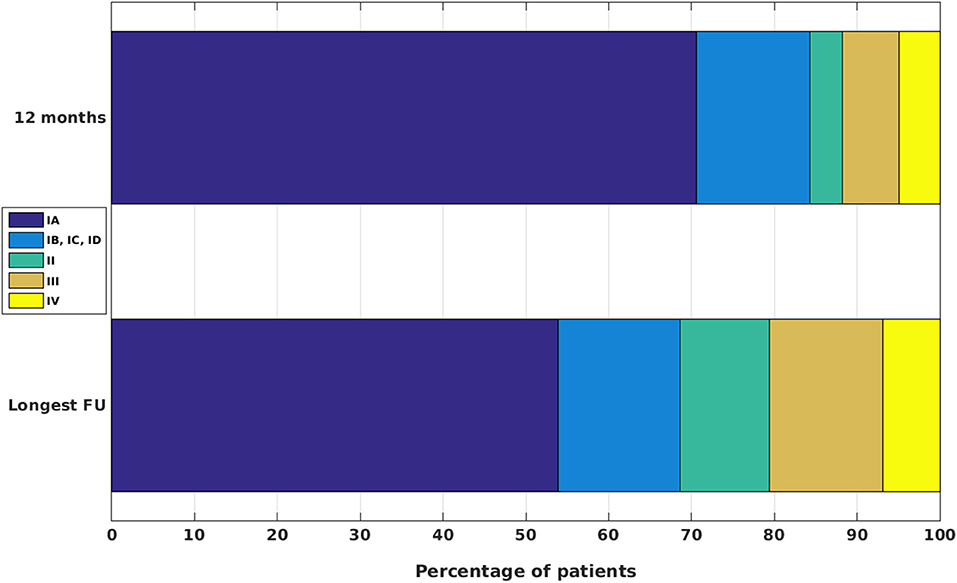
Figure 1. Post-surgical outcomes at 12 months and at the longest available FU for patients with FCD II.
We analyzed separately the longest available FU (Figure 1). After a mean long-term FU of 62.83 ± 5.06 (mean ± standard error; median 46.5) months, 55 patients (53.92%) were completely seizure free (Engel class IA), and altogether, 70 patients (68.63%) had an excellent (Engel class I) outcome [15 patients (14.71%) with Engel class IB/IC/ID, 11 (10.78%) with Engel class II, 14 (13.73%) with Engel class III, and 7 (6.86%) with Engel class IV outcome]. Compared with the outcomes at 12 months of FU for the same patients, these measures indicated a slight worsening, which reached significance (p < 0.01, sign test).
At 12 months of FU, 93 out of the 102 patients (91.18%) was on anticonvulsant pharmacotherapy (AED; four patients discontinued, in five cases we did not have reliable information on drug intake); at the longest available FU, 81 patients (79.41%) were taking AEDs, 21 (20.59%) already discontinued, and 32 patients (31.37%) converted already from anticonvulsant polytherapy to monotherapy.
Four patients (two with Engel class III and two with Engel class IV outcome at longest FU) underwent a second operation due to unfavorable outcome after the first surgery. Two of them became completely seizure free (Engel class IA): one of them attained Engel class II and the other patient had Engel class III outcome after the second surgery.
We also evaluated the possible effect of advancement in diagnostic and technical modalities on post-surgical outcomes over the last two decades. This factor can be best studied in a monocenter setting, since a number of potential confounders resulting from distinct and variable diagnostic approaches and surgical strategies over multiple epilepsy centers can be discarded. By looking at a period of 18 years, we sorted cases in three groups spanning 6 years each: early: operated between 2002 and 2007 (38 patients), middle: operated between 2008 and 2013 (48 patients), and late: surgery between 2014 and 2019 (16 patients) (Figure 2). Outcomes of patients operated on in different periods did not show a statistically significant difference either for 12 months or for the longest available FU (chi-square tests and Fisher's exact tests). Within-group comparisons of outcomes at 12 months and the longest FU revealed a significant difference only for the “early” group (p = 0.021, sign test).
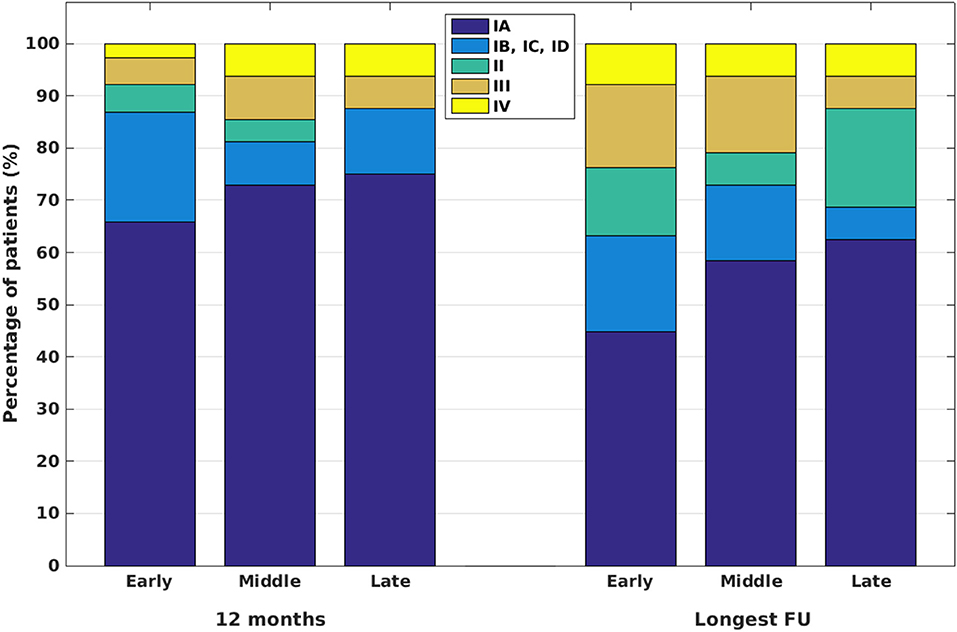
Figure 2. Post-surgical outcomes for patients operated on in the periods between 2002 and 2007 (“early”), between 2008 and 2013 (“middle”), and between 2014 and 2019 (“late”).
We further analyzed factors possibly contributing to or determining post-surgical outcome with univariate analysis. From the examined variables [exact histopathology, lobar lesion location, history of focal to bilateral tonic–clonic seizures (FTBTCS), extent of resection, and family history for epilepsy], the extent of resection (complete vs. incomplete), history of FTBTCS, and lobar lesion location (frontal vs. non-frontal, multilobar or insular) appeared to have a significant influence on post-surgical outcome in the univariate analysis at 12 months, and the extent of resection, history of FTBTCS, and family history for epilepsy or epileptic seizures have a significant influence on post-surgical outcome at the longest available FU (Table 2; Figure 3).
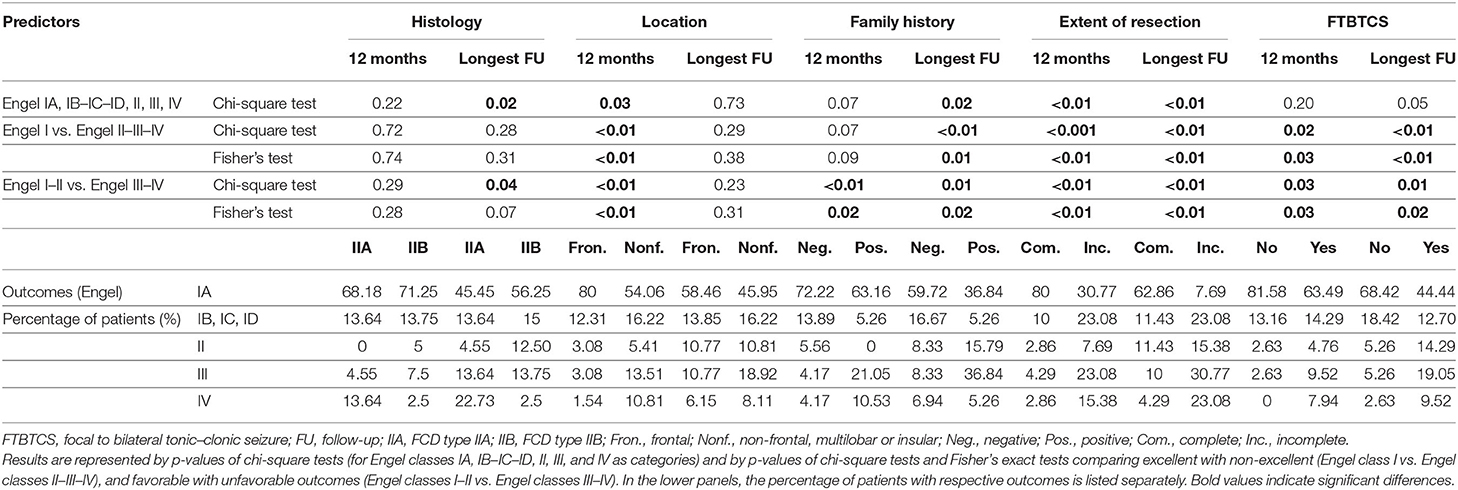
Table 2. Univariate analysis for possible predictors of post-surgical outcome.
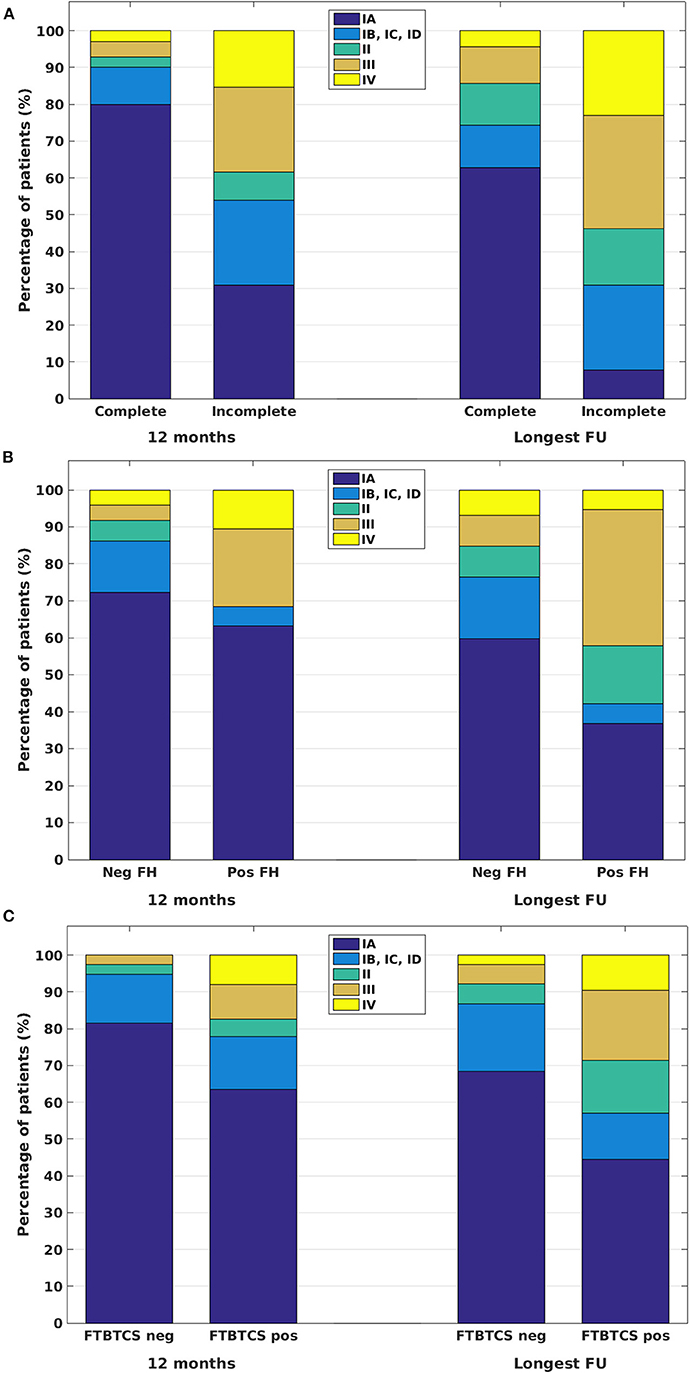
Figure 3. Post-surgical outcomes at 12 months and at the longest available FU in patients with complete and incomplete resections of FCD II (A), for patients with negative (Neg FH) and positive (Pos FH) family history for epilepsy or epileptic seizures (B), and for patients without (FTBTCS neg) and with (FTBTCS pos) focal to bilateral tonic–clonic seizures in their case history (C).
We further analyzed the above-discussed and additional factors (age at epilepsy onset, age at surgery, duration of epilepsy) with multivariate logistic regression analysis. The stepwise regression analysis verified several, partially interacting factors (age at epilepsy onset, duration of epilepsy, age at surgery, extent of resection, and lesion location) determining outcomes at 12 months, of which the extent of resection and lesion location appeared to be the most relevant (Table 3). The analysis revealed completeness of resection and history of FTBTCS as significant independent predictors for long-term outcome (Table 3). The family history for epilepsy or epileptic seizures displayed significant values only for long-term outcomes and only by contrasting Engel class I against Engel class II–IV outcomes.
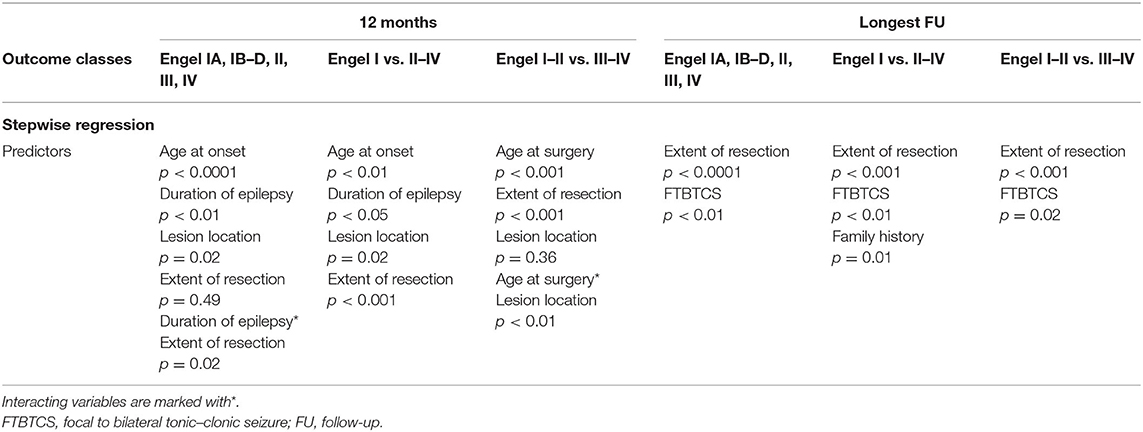
Table 3. Multivariate logistic regression analysis for possible predictors of post-surgical outcome: p-values for predictor variables.
To elucidate the potential influence of positive family history for epilepsy or epileptic seizures on post-surgical outcome, we also analyzed data in a larger set of patients operated on with glioneuronal tumors over the same period in our center. Out of 94 operated patients, 8 (8.51%) displayed positive family history for epilepsy; in 73 patients, family history was negative; and in 13 patients, we did not have reliable information on family history. Interestingly, all 8 patients were completely seizure free both at 12 months and at the longest available FU; among patients with negative family history, 70.59 and 54.79% (12 months and longest FU, respectively) were completely seizure free (Engel class IA). Outcome differences between the positive and negative family history groups with glioneuronal tumors were not found to be statistically significant (univariate analysis with chi-square tests and Fisher's exact test). When comparing patients with positive family history from the FCD group and from the glioneuronal tumor group, outcome differences were not significant at 12 months, but these were significant for the longest FU, when we contrasted excellent (Engel class I) to non-excellent (Engel classes II–IV) outcomes (p = 0.0052, chi-square test; p = 0.0082, Fisher's exact test). By contrasting favorable (Engel classes I–II) to unfavorable (Engel III–IV) outcomes, the chi-square test indicated a significant difference (p = 0.03), which was not supported by Fisher's test (p = 0.06).
Here, we report post-surgical outcomes in a series of 102 patients who underwent epilepsy surgery for medically refractory epilepsy related to FCD II. Concordant with the literature (10–12, 16–22), the majority of our patients displayed an excellent or at least favorable outcome both at 12 months and at the longest available (median 46.5 months) FU. Moreover, the extent (completeness) of resection and the absence of FTBTCS in the patient history were found to be important predictors for long-term positive post-surgical outcome, whereas age at epilepsy onset, age at surgery, duration of epilepsy, exact histopathology (FCD type IIA vs. IIB), and lesion location (frontal vs. non-frontal, multilobar or insular) did not have a consistently significant effect on long-term outcomes after epilepsy surgery. Even though positive family history for epilepsy or epileptic seizures was associated with a trend toward worse outcome at the longest available FU, this effect did not turn out to be consistently significant in the multivariate analysis. Outcomes after epilepsy surgery did not show a remarkable difference over the last 20 years in our center.
Outcome measures showed a slight but significant worsening tendency at long-term compared with 12 months of FU. Furthermore, the long-term seizure freedom rates might be underestimated when investigating patient collectives with late FU in an outpatient setting, where patients not attaining seizure freedom are probably overrepresented and patients reaching long-term seizure freedom are underrepresented for not having the need to seek further medical care. For that reason, on the other hand, we performed a detailed telephone interview with patients not having contact with our clinic during the 12 months preceding data acquisition for the study. Nevertheless, since some of these patients could not be reached any more (changing address, etc.), and some of them did not provide a written informed consent for the phone interview, we cannot completely rule out that the slight worsening tendency—though reported in several studies (35)—partially resulted from a disequilibrium of patients as described above.
The observation that the extent (i.e., completeness) of resection had a significant influence on post-surgical outcome is in concordance with previous publications (10, 12, 21, 35–37).
Even though long-term outcomes were slightly worse in patients with positive family history for epilepsy or epileptic seizures than in those with negative family history, this factor did not consistently reach significance in the multivariate regression analysis. On the other hand, we cannot rule out that the relatively low sample size of patients with positive family history (19 patients) did not allow the identification of a statistically significant effect, only a trend. Certainly, we cannot exclude that some of the patients with a positive family history for epilepsy might have had genetic variants in susceptibility genes independent of the FCD. On the other hand, our results are also reconcilable with recent observations that focal cortical malformations can be operated with excellent post-surgical outcome even in case of justified genetic alterations, especially affecting the mTOR pathway (38–41).
To further clarify the potential role of positive family history for epilepsy on post-surgical outcome, we compared data from patients operated on with glioneuronal tumors during the same period. Apparently, positive family history for epilepsy did not exert a significant influence on post-surgical outcomes among patients with glioneuronal tumors in a univariate analysis, and patients with positive family history and glioneuronal tumors displayed in certain measures a better outcome than those with FCD II. As the sample sizes were low, however, one needs to interpret the observed effects with caution. On the other hand, the observed difference between patients with FCD and glioneuronal tumors and with positive family history for epilepsy might suggest a possible FCD-specific effect in determining post-surgical outcomes.
The finding that history of FTBTCS in the patient history can be regarded as a negative predictor might hypothetically be related to a more widespread epileptogenic network reaching far beyond the histological boundaries of FCD in many patients with FTBTCS.
The effect of precise histopathology of FCD is somewhat controversial in the literature. Although several publications do not present relevant differences between distinct histopathological subtypes [(42): FCD type I vs. II; (16): FCD types I, II, and III; (12): FCD type I vs. II] or find non-significant trends [(11): FCD IIB slightly better than IIA], further studies found either better results in FCD type I (19) or in FCD type II (20, 23) and better outcomes in FCD type IIB than in type IIA (43). The effect of associated lesions in terms of a dual pathology also seems to be controversial. Patients operated on with glioneuronal tumors or hippocampal sclerosis associated with FCD type I were reported to have a significantly better post-surgical outcome (24), whereas another investigation found worse outcomes in FCD type III compared with FCD types I and II (44). In our series, we had a disproportionate distribution between FCD IIA and IIB, meaning a potential limitation in our results. This misbalance is most probably related to the better MR diagnostic features of FCD IIB compared with IIA (11) and also to the fact that patients with lesional MRI preferentially undergo epilepsy surgery in our center. In addition, we also excluded cases with dual pathologies and FCD types I and III in order to have more homogeneous histological groups for the analysis.
The precise location of FCD may also have an impact on post-surgical outcome. Among pediatric patients, frontal or temporal FCD location was associated with a significantly better outcome compared with central or posterior locations (12). A temporal lobe location in patients with FCD IIA was also found to be a predictor for positive outcome (35). In our series, we did not find a consistent and significant difference between long-term outcomes in frontal vs. non-frontal location; on the other hand, due to the paucity of temporal lobe location, we could not examine this lobar location separately.
The literature also reports conflicting results on the influence of early epilepsy surgery on post-surgical outcome. For instance, in a series of pediatric patients, age at surgery (in infancy vs. at later age) did not exert a significant influence on post-surgical outcome (12). In a series reporting on patients operated on with FCD type II before and after 20 years of age, a statistically significant difference in post-surgical outcomes was not reported either (45). However, effects can be confounded by other variables and also depend on the compared patient populations. In the pediatric series from the Freiburg Epilepsy Center, for instance, patients operated at younger ages more frequently underwent extensive operations (i.e., multilobar resections and hemispherectomies) than those operated at a later age; nevertheless, they displayed worse outcomes (42). Moreover, in the complete series from Freiburg comprising both adults and children, early surgery (before 18 years of age) proved to be a positive predictor for optimal outcome (16). In the current series, we did not find a hint on the significant effect of age at epilepsy onset, age at epilepsy surgery, and duration of epilepsy on long-term post-surgical outcomes.
The strength of our investigation relies on the big sample size and the length of FUs. Besides, the effect of family history for epilepsy or epileptic seizures on post-surgical outcome—to our best knowledge—has not been systematically analyzed in larger patient groups with FCD so far. A certain limitation may be given by a misbalance between the sample size of the reported FCD subtypes (FCD IIA and IIB), the paucity of less frequent (especially temporal and occipital) lesion locations, and the retrospective monocenter design.
Epilepsy in early childhood is frequently associated with relevant cognitive and developmental disturbances (46, 47), and epilepsy surgery early in the course of the disease can have an immense impact on the development of affected individuals (47). Concordant with published results on bigger patient collectives, epilepsy surgery still tends to be relatively late compared with epilepsy onset (48) despite diagnostic advancements during the last decades (31–33). In the analyzed group, the median duration of epilepsy till surgery was 14 years, meaning that for certain patients, it took several decades to access this therapeutic modality.
Post-surgical seizure control in patients with FCD II is slightly worse at the longest available FU with a median of 46.5 months compared with 12 months. Complete lesion resection and the absence of FTBTCS in the patients' history are found to be the most important predictors for optimal long-term post-surgical outcome, whereas exact histopathology (FCD IIA vs. FCD IIB), lobar lesion location, age at epilepsy onset, age at surgery, and epilepsy duration do not have a significant impact on long-term post-surgical outcome. Positive family history for epilepsy might have a marginal effect on post-surgical outcome. This result also supports the view that “heritable” focal cortical malformations can be excellent subjects for epilepsy surgery.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Ethik-Kommission - Medizinische Fakultät Bonn. Written informed consent from the participants' legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
AR and CE contributed to conception and design of the study. AR, AB, and CQ collected the data. AR and AB analyzed the data. AR wrote the first draft of the manuscript. AB, CQ, VB, HV, RS, and CE wrote sections of the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
AED, antiepileptic drug; FCD, focal cortical dysplasia; FTBTCS, focal to bilateral tonic–clonic seizure; FU, follow-up; GABA, gamma amino butyric acid; ILAE, International League Against Epilepsy; MRI, magnetic resonance imaging; PET, positron emission tomography; SPECT, single-photon emission computed tomography.
1. Barba C, Specchio N, Guerrini R, Tassi L, De Masi S, Cardinale F, et al. Increasing volume and complexity of pediatric epilepsy surgery with stable seizure outcome between 2008 and 2014: a nationwide multicenter study. Epilepsy Behav. (2017) 75:151–7. doi: 10.1016/j.yebeh.2017.08.010
2. Blumcke I, Spreafico R, Haaker G, Coras R, Kobow K, Bien CG, et al. Histopathological findings in brain tissue obtained during epilepsy surgery. N Engl J Med. (2017) 377:1648–56. doi: 10.1056/NEJMoa1703784
3. Aubert S, Wendling F, Regis J, McGonigal A, Figarella-Branger D, Peragut JC, et al. Local and remote epileptogenicity in focal cortical dysplasias and neurodevelopmental tumours. Brain. (2009) 132:3072–86. doi: 10.1093/brain/awp242
4. Rosenow F, Lüders HO, Dinner DS, Prayson RA, Mascha E, Wolgamuth BR, et al. Histopathological correlates of epileptogenicity as expressed by electrocorticographic spiking and seizure frequency. Epilepsia. (1998) 39:850–6. doi: 10.1111/j.1528-1157.1998.tb01179.x
5. Palmini A. Disorders of cortical development. Curr Opin Neurol. (2000) 13:183–92. doi: 10.1097/00019052-200004000-00012
6. Medici V, Rossini L, Deleo F, Tringali G, Tassi L, Cardinale F, et al. Different parvalbumin and GABA expression in human epileptogenic focal cortical dysplasia. Epilepsia. (2016) 57:1109–19. doi: 10.1111/epi.13405
7. Palmini A, Najm I, Avanzini G, Babb T, Guerrini R, Foldvary-Schaefer N, et al. Terminology and classification of the cortical dysplasias. Neurology. (2004) 62 (Suppl. 3):S2–8. doi: 10.1212/01.WNL.0000114507.30388.7E
8. Blumcke I, Thom M, Aronica E, Armstrong DD, Vinters HV, Palmini A, et al. The clinicopathologic spectrum of focal cortical dysplasias: a consensus classification proposed by an ad hoc task force of the ILAE diagnostic methods commission. Epilepsia. (2011) 52:158–74. doi: 10.1111/j.1528-1167.2010.02777.x
9. Rácz A, Müller AM, Schwerdt J, Becker A, Vatter H, Elger CE. Age at epilepsy onset in patients with focal cortical dysplasias, gangliogliomas and dysembryoplastic neuroepithelial tumours. Seizure. (2018) 58:82–9. doi: 10.1016/j.seizure.2018.04.002
10. Wagner J, Urbach H, Niehusmann P, von Lehe M, Elger CE, Wellmer J. Focal cortical dysplasia type IIb: completeness of cortical, not subcortical, resection is necessary for seizure freedom. Epilepsia. (2011) 52:1418–24. doi: 10.1111/j.1528-1167.2011.03158.x
11. Wagner J, Weber B, Urbach H, Elger CE, Huppertz HJ. Morphometric MRI analysis improves detection of focal cortical dysplasia type II. Brain. (2011) 134:2844–54. doi: 10.1093/brain/awr204
12. Kloss S, Pieper T, Pannek H, Holthausen H, Tuxhorn I. Epilepsy surgery in children with focal cortical dysplasia (FCD): results of long-term seizure outcome. Neuropediatrics. (2002) 33:21–6. doi: 10.1055/s-2002-23595
13. Hirabayashi S, Binnie CD, Janota I, Polkey CE. Surgical treatment of epilepsy due to cortical dysplasia: clinical and EEG findings. J Neurol Neurosurg Psychiatry. (1993) 56:765–70. doi: 10.1136/jnnp.56.7.765
14. Lamberink HJ, Otte WM, Blümcke I, Braun KPJ, on behalf of the European Epilepsy Brain Bank writing group study group and the European Reference Network EpiCARE. Seizure outcome and use of antiepileptic drugs after epilepsy surgery according to histopathological diagnosis: a retrospective multicentre cohort study. Lancet Neurol. (2020) 19:748–57. doi: 10.1016/S1474-4422(20)30220-9
15. Chen J, Chen X, Huang C, Zhu H, Hou Z, An N, et al. Predictors of seizure recurrence in patients with surgery for focal cortical dysplasia: pairwise and network meta-analysis and trial sequential analysis. Childs Nerv Syst. (2019) 35:753–67. doi: 10.1007/s00381-019-04124-0
16. Fauser S, Essang C, Altenmüller DM, Staack AM, Steinhoff BJ, Strobl K, et al. Long-term seizure outcome in 211 patients with focal cortical dysplasia. Epilepsia. (2015) 56:66–76. doi: 10.1111/epi.12876
17. Rowland NC, Englot DJ, Cage TA, Sughrue ME, Barbaro NM, Chang EF. A meta-analysis of predictors of seizure freedom in the surgical management of focal cortical dysplasia. J Neurosurg. (2012) 116:1035–41. doi: 10.3171/2012.1.JNS111105
18. Kral T, von Lehe M, Podlogar M, Clusmann H, Süßmann P, Kurthen M, et al. Focal cortical dysplasia: long term seizure outcome after surgical treatment. J Neurol Neurosurg Psychiatry. (2007) 78:853–6. doi: 10.1136/jnnp.2006.105361
19. Fauser S, Schulze-Bonhage A, Honegger J, Carmona H, Huppertz HJ, Pantazis G, et al. Focal cortical dysplasias: surgical outcome in 67 patients in relation to histological subtypes and dual pathology. Brain. (2004) 127:2406–18. doi: 10.1093/brain/awh277
20. Tassi L, Colombo N, Garbelli R, Francione S, Lo Russo G, Mai R, et al. Focal cortical dysplasia: neuropathological subtypes, EEG, neuroimaging and surgical outcome. Brain. (2002) 125:1719–32. doi: 10.1093/brain/awf175
21. Chassoux F, Devaux B, Landre E, Turak B, Nataf F, Varlet P, et al. Stereo-electroencephalography in focal cortical dysplasia. A 3D approach to delineating the dysplastic cortex. Brain. (2000) 123:1733–51. doi: 10.1093/brain/123.8.1733
22. Keene DL, Jimenez CC, Ventureyra E. Cortical microdysplasia and surgical outcome in refractory epilepsy of childhood. Pediatr Neurosurg. (1998) 55:131–6. doi: 10.1159/000028692
23. Kim YH, Kang HC, Kim DS, Kim SH, Shim KW, Kim HD, et al. Neuroimaging in identifying focal cortical dysplasia and prognostic factors in pediatric and adolescent epilepsy surgery. Epilepsia. (2011) 52:722–7. doi: 10.1111/j.1528-1167.2010.02950.x
24. Tassi L, Garbelli R, Colombo N, Bramerio M, Lo Russo G, Deleo F, et al. Type I focal cortical dysplasia: surgical outcome is related to histopathology. Epileptic Disord. (2010) 12:181–91. doi: 10.1684/epd.2010.0327
25. Scerri T, Riseley JR, Gillies G, Pope K, Burgess R, Mandelstam SA, et al. Familial cortical dysplasia type IIA caused by a germline mutation in DEPDC5. Ann Clin Transl Neurol. (2015) 2:575–80. doi: 10.1002/acn3.191
26. Scheffer IE, Heron SE, Regan BM, Mandelstam S, Crompton DE, Hodgson BL, et al. Mutations in mammalian target of rapamycin regulator DEPDC5 cause focal epilepsy with brain malformations. Ann Neurol. (2014) 75:782–7. doi: 10.1002/ana.24126
27. Ricos MG, Hodgson BL, Pippucci T, Saidin A, Ong YS, Heron SE, et al. Mutations in the mammalian target of rapamycin pathway regulators NPRL2 and NPRL3 cause focal epilepsy. Ann Neurol. (2016) 79:120–31. doi: 10.1002/ana.24547
28. Sim JC, Scerri T, Fanjul-Fernández M, Riseley JR, Gillies G, Pope K, et al. Familial cortical dysplasia caused by mutation in the mammalian target of rapamycin regulator NPRL3. Ann Neurol. (2016) 79:132–7. doi: 10.1002/ana.24502
29. Jansen LA, Mirzaa GM, Ishak GE, O'Roak BJ, Hiatt JB, Roden WH, et al. PI3K/AKT pathway mutations cause a spectrum of brain malformations from megalencephaly to focal cortical dysplasia. Brain. (2015) 138:1613–28. doi: 10.1093/brain/awv045
30. Schick V, Majores M, Engels G, Hartmann W, Elger CE, Schramm J, et al. Differential Pi3K-pathway activation in cortical tubers and focal cortical dysplasias with balloon cells. Brain Pathol. (2007) 17:165–73. doi: 10.1111/j.1750-3639.2007.00059.x
31. Huppertz HJ, Grimm C, Fauser S, Kassubek J, Mader I, Hochmuth A, et al. Enhanced visualization of blurred gray-white matter junctions in focal cortical dysplasia by voxel-based 3D MRI analysis. Epilepsy Res. (2005) 67:35–50. doi: 10.1016/j.eplepsyres.2005.07.009
32. Kassubek J, Huppertz HJ, Spreer J, Schulze-Bonhage A. Detection and localization of focal cortical dysplasia by voxel-based 3-D MRI analysis. Epilepsia. (2002) 43:596–602. doi: 10.1046/j.1528-1157.2002.41401.x
33. O'Brien TJ, So EL, Mullan BP, Hauser MF, Brinkmann BH, Bohnen NI, et al. Subtraction ictal SPECT co-registered to MRI improves clinical usefulness of SPECT in localizing the surgical seizure focus. Neurology. (1998) 50:445–54. doi: 10.1212/WNL.50.2.445
34. Engel J Jr, Van Ness PC, Rasmussen TB, Ojemann LM. Outcome with respect to epileptic seizures. In: Engel J Jr, editor. Surgical Treatment of the Epilepsies. New York, NY: Raven Press (1993). p. 609–21.
35. Sun Y, Wang X, Che N, Qin H, Liu S, Wu X, et al. Clinical characteristics and epilepsy outcomes following surgery caused by focal cortical dysplasia (type IIa) in 110 adult epileptic patients. Exp Therapeut Med. (2017) 13:2225–34. doi: 10.3892/etm.2017.4315
36. Oluigbo CO, Wang J, Whitehead MT, Magge S, Myseros JS, Yaun A, et al. The influence of lesion volume, perilesion resection volume, and completeness of resection on seizure outcome after resective epilepsy surgery for cortical displays in children. J Neurosurg Pediatr. (2015) 15:644–50. doi: 10.3171/2014.10.PEDS14282
37. Krsek P, Maton B, Jayakar P, Dean P, Korman B, Rey G, et al. Incomplete resection of focal cortical dysplasia is the main predictor of poor postsurgical outcome. Neurology. (2009) 72:217–23. doi: 10.1212/01.wnl.0000334365.22854.d3
38. San Antonio-Arce V. Are there surgical treatment options for genetic focal epilepsies? Z Epileptol. (2019) 32:311–8. doi: 10.1007/s10309-019-0268-4
39. Stevelink R, Sanders MW, Tuinman MP, Brilstra EH, Koeleman BP, Jansen FE, et al. Epilepsy surgery for patients with genetic refractory epilepsy: a systematic review. Epileptic Disord. (2018) 20:99–115. doi: 10.1684/epd.2018.0959
40. Weckhuysen S, Marsan E, Lambrecq V, Marchal C, Morin-Brureau M, An-Gourfinkel I, et al. Involvement of GATOR complex genes in familial focal epilepsies and focal cortical dysplasia. Epilepsia. (2016) 57:994–1003. doi: 10.1111/epi.13391
41. Zhang K, Hu WH, Zhang C, Meng FG, Chen N, Zhang JG. Predictors of seizure freedom after surgical management of tuberous sclerosis complex: a systematic review and meta-analysis. Epilepsy Res. (2013) 105:377–83. doi: 10.1016/j.eplepsyres.2013.02.016
42. Martinez-Lizana E, Fauser S, Brandt A, Schuler E, Wiegand G, Doostkam S, et al. Long-term seizure outcome in paediatric patients with focal cortical dysplasia undergoing tailored and standard surgical resections. Seizure. (2018) 62:66–73. doi: 10.1016/j.seizure.2018.09.021
43. Veersema TJ, Swampillai B, Ferrier CH, van Eijsden P, Gosselaar PH, van Rijen PC, et al. Long-term seizure outcome after epilepsy surgery in patients with mild malformation of cortical development and focal cortical dysplasia. Epilepsia Open. (2019) 4:170–5. doi: 10.1002/epi4.12289
44. Kim DW, Kim S, Park SH, Chung CK, Lee SK. Comparison of MRI features and surgical outcome among the subtypes of focal cortical dysplasia. Seizure. (2012) 21:789–94. doi: 10.1016/j.seizure.2012.09.006
45. Ramírez-Molina JL, Di Giacomo R, Mariani V, Deleo F, Cardinale F, Uscátegui-Daccarett AM, et al. Surgical outcomes in two different age groups with focal cortical dysplasia type II: any real difference? Epilepsy Behav. (2017) 70:45–9. doi: 10.1016/j.yebeh.2017.02.031
46. Choi SA, Kim KJ. The surgical and cognitive outcomes of focal cortical dysplasia. J Korean Neurosurg Soc. (2019) 62:321–7. doi: 10.3340/jkns.2019.0005
47. Veersema TJ, van Schooneveld MMJ, Ferrier CH, van Eijsden P, Gosselaar PH, van Rijen PC, et al. Cognitive functioning after epilepsy surgery in children with mild malformation of cortical development and focal cortical dysplasia. Epilepsy Behav. (2019) 94:209–15. doi: 10.1016/j.yebeh.2019.03.009
Keywords: focal cortical dysplasia, epilepsy surgery, outcome, genetics, Engel classification
Citation: Rácz A, Becker AJ, Quesada CM, Borger V, Vatter H, Surges R and Elger CE (2021) Post-Surgical Outcome and Its Determining Factors in Patients Operated on With Focal Cortical Dysplasia Type II—A Retrospective Monocenter Study. Front. Neurol. 12:666056. doi: 10.3389/fneur.2021.666056
Received: 09 February 2021; Accepted: 19 April 2021;
Published: 09 June 2021.
Edited by:
Guido Rubboli, University of Copenhagen, DenmarkReviewed by:
Laura Tassi, “Claudio Munari” Epilepsy Surgery Centre - Niguarda Hospital, ItalyCopyright © 2021 Rácz, Becker, Quesada, Borger, Vatter, Surges and Elger. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Attila Rácz, QXR0aWxhLlJhY3pAdWtib25uLmRl
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.