 Marcio Soto-Añari1*
Marcio Soto-Añari1* Norman López2
Norman López2 Claudia Rivera-Fernández3Verónica Belón-Hercilla1
Claudia Rivera-Fernández3Verónica Belón-Hercilla1 Sara Fernández-Guinea4
Sara Fernández-Guinea4- 1Laboratorio de Neurociencia, Departamento de Psicología, Universidad Católica San Pablo, Arequipa, Peru
- 2Universidad de la Costa, Barranquilla, Colombia
- 3Universidad Nacional de San Agustín de Arequipa, Arequipa, Peru
- 4Departamento de Psicología Experimental, Facultad de Psicología, Universidad Complutense de Madrid, Madrid, Spain
Introduction: Early-life educational experiences are associated with cognitive performance in aging. Early literacy seems to improve executive control mechanisms, however, it is not clear whether early education would still be an advantage in countries like Peru, where access to and quality of education is highly variable.
Aim: Our objective was to analyze the association of literacy level with executive control factors.
Method: We evaluated 93 healthy older adults with a clinical protocol that included the Mini-Mental State Examination, the Geriatric Depression Scale and Global Dementia Staging. We also used a neuropsychological executive function battery which included the Trail-Making Test parts A and B, the Stroop Test, phonological and semantic verbal fluency tasks, Forward and Backward Digits, Numbers and Letters of the Wechsler Scale, and the Go/No-Go task. We used a principal component analysis for the dimensional reduction of the variables. To measure the level of literacy we used the word accentuation test (WAT).
Results: We observed statistically significant correlations between the principal components (PCs) of working memory, cognitive flexibility and inhibitory control with the WAT scores. Furthermore, we observed that processing speed and WAT predict the scores on PCs factors better than years of education and age.
Conclusions: Literacy level correlates more closely with better cognitive performance than years of education and thus, might improve executive control factors that could compensate and protect against brain changes in cognitive decline and dementia.
Introduction
The rapid aging of the population is one of the most serious issues worldwide in this century (1). An estimated 2.1 billion people will be elderly by 2050. Eighty percentage will live in low- and middle-income countries, such as most Latin-American countries, and a high percentage will be illiterate, have difficulty in accessing education or have received poor quality education (1). This scenario will bring an increase in diseases and health disorders such as dementia (2), for which a low educational level is one of the main risk factors (3, 4), along with a low literacy level.
Early-life educational experiences have an important effect on cognition throughout development (5). The pioneering studies of Manly et al. (6, 7), demonstrated that literacy level was a more reliable predictor of cognitive decline in ethnic minorities and immigrants than years of education. Later studies confirmed these findings (8, 9). Therefore, the literacy level achieved, including not only the ability to read and write but also the competent use of information, seems to modulate the cognitive response in older adults with different ethnicities, through basic and complex cognitive mechanisms (10).
This modulation has been associated with basic attentional mechanisms such as processing speed, which is known as an important factor influencing cognition in aging (11) and executive control (12), which includes working memory, inhibitory control and cognitive flexibility (13). These mechanisms are activated in normal (14, 15) and pathological (16) cognitive aging to better cope with physiological changes or task demands (12, 17).
These executive control mechanisms are activated during a complex or novel task, or when processing resources are reduced, as in pathological aging (18). They activate brain processing networks that compensate for changes (19, 20). Other studies have suggested that these compensatory activations are not always positive, because it seems to have a threshold above which they could be rather inefficient, thus reflecting a greater level of deterioration (21).
Literacy level has been assessed through asking subjects to read low-frequent words, classically used for the estimation of premorbid IQ (22). It is assumed that the pronunciation of these words is associated with the literacy level achieved and that this in turn is correlated with IQ (23). For this, the Word Accentuation Test (WAT) has been used for Spanish speakers (24). This has shown itself to be useful in studies with neuropsychiatric populations for the measurement of premorbid IQ (25, 26) and suitable for evaluating educational quality where education is not homogeneous (27).
Previous studies in Peru have shown that older adults with higher reading level scores performed better in executive functions and memory tasks (28). This study concludes that higher literacy levels might reflect a higher quality education received early in life.
These early-life educational experiences (exposure to quality content), also promote the implementation of mechanisms for regulating cognition, such as executive control, which are associated with cognitive reserve and brain resilience mechanisms in later-life (29). Consequently, it seems that limited years of education is not the only risk factor for neurodegenerative diseases, but also low literacy level. Thus, our objective is to analyze the association of literacy level with executive control factors in normal aging. In addition, we analyze the effect of processing speed, years of education and age on executive control. We hypothesize that higher scores in the Word Accentuation Test will predict better performance in executive control tasks, which will be independent of age, years of education, and processing speed. These results will permit us to identify the influence of educational quality on the dynamics of cognition in older adults.
Methods
Participants
The initial sample consisted of 121 older adults from public and private senior citizen clubs in the city of Arequipa, Peru. The participants were selected according to the following criteria: not having a history of neurological or psychiatric disease and not having major visual or auditory problems. Besides we excluded participants with Mini-Mental State Examination scores below 27 points if they had more than 7 years of schooling, below 23 points for those with 4–7 years of schooling and below 21 points for those with 1–3 years of schooling; following the used by Custodio & Lira (30). Finally, we excluded participants with scores above 6 points on the Yesavage Geriatric Depression Scale (31) and above 2 points on Reisberg's Global Dementia Staging (32). The final sample was made up of 93 healthy older adults (see Table 1).
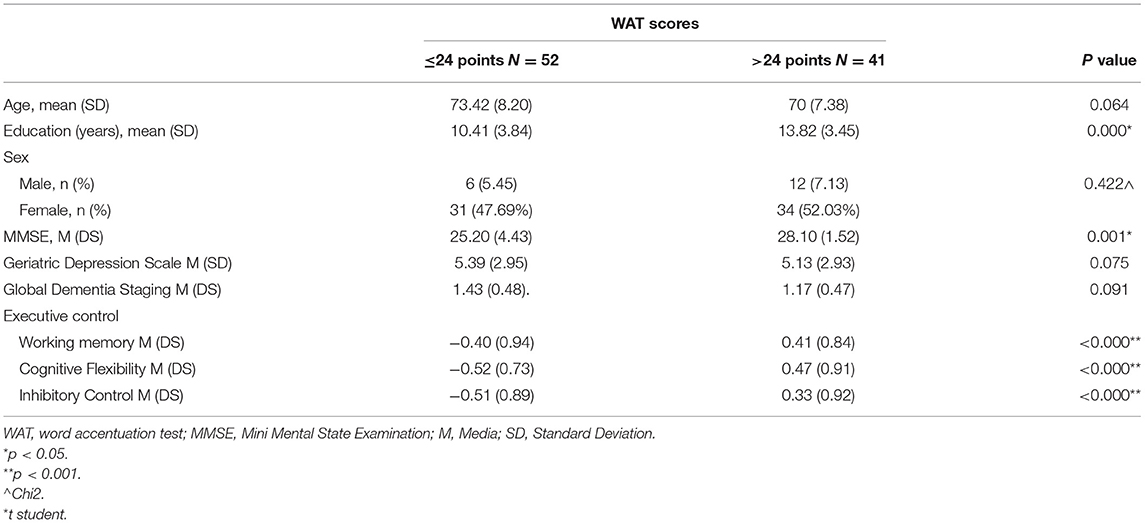
Table 1. Sociodemographic, clinical and cognitive characteristics of the final sample (N = 93), according to the WAT score.
Instruments
We used a paper and pencil neuropsychological battery to test various components of executive control. Working memory was assessed with the raw scores of Forward and Backward Digits, as well as of Numbers and Letters from the III Wechsler Scale (33). For cognitive flexibility, we used the raw scores (time) of Trail Making Test B (TMT-B) (34) and the total number of words with “P” (phonological fluency) and animals (semantic fluency) named in 60 s (35). Inhibitory control was evaluated with the Word-Color subtest and interference scores of Stroop Test (36) and the Go/No-Go subtest of the Frontal Assessment Battery (FAB) (37).
Likewise, we evaluated processing speed as a basic attention mechanism that modulates cognition in aging (11). For that purpose, we used the raw scores of Trail Making Test A (time) (TMT-A) (38) and Word and Color subtests of the Stroop Test (36), accordingly the proposal of Perea et al. (39), along with the raw scores of the Digit Symbol subtest from the Wechsler scale (WAIS IV).
Literacy level was measured through the Word Accentuation Test (WAT) (24). We used the Ecuadorian version (26), which showed good internal consistency as well as good test-retest reliability. This test requires the subject to read aloud some low-frequency words presented visually, written in capital letters without an accent mark. The subjects were asked to read the word correctly and mark the tonic accent. We used the 30-item version.
Procedure
Two sessions of approximately 50 min each were carried out over a period of 2–3 weeks. The assessments were carried out in 2 phases. In the first one, a clinical screening protocol was applied to all subjects, excluding those who did not meet the inclusion criteria. In the second phase, the subjects were administered the neuropsychological battery.
Statistical Analysis
We performed a Principal Component Analysis (PCA) to reduce the neuropsychological factors and identify executive control and processing speed components. To obtain PCA components, we transformed Direct scores of individual tests into Z scores for standardized data. The number of principal components (PCs) extracted was prespecified using the standard eigenvalues >1 criterion. Top contributors of each rotated PC were defined as those with a factor loading > 0.5.
We used the median obtained in the word accentuation test (Me = 24) to split the participants into two groups (lower score ≤ 24 and higher score > 24) according with Manly et al. (6). Afterwards, Pearson bivariate correlation tests were performed between the PCs found with the WAT score. Finally, we performed a linear regression analysis, in which the PCs were analyzed as dependent variables and the age factor, years of education, WAT scores and composite index of the processing speed factor were the independent variables. The processing was performed using the statistical software SPSS version 24.
Ethical Aspects
This study is part of a follow-up research project about the impact of literacy level on cognition in preclinical and clinical phases of dementia and was reviewed and approved by the Ethics Committee of the Research unit of San Pablo Catholic University (Acta N° 012.CEDI.UCSP.2020). All participants gave written informed consent in accordance with the declaration of Helsinki.
Results
Demographic, Clinical and PC Information on the Participants
The sociodemographic, clinical and PC data (Supplementary Material) of the sample are presented in Table 1. Participants with WAT scores below and above 24 points do not differ significantly in age and sex, but they do in years of education and MMSE (see Table 1). The PCs obtained were inhibitory control (Word-Color and Interference subtests of Stroop Test), cognitive flexibility (TMT-B, semantic [animal] and phonological [letter P] fluency task) and working memory (Forward and Backward Digits and Numbers and Letters). These components explained 72.9% of the variance. In addition, their scores differ significantly between the groups.
Associations Between Composite Factors and WAT Score
Pearson bivariate correlation tests showed significant correlations between PC scores of working memory (r = 0.527, p < 0.000); cognitive flexibility (r = 0.521, p < 0.000) and inhibitory control (r = 382, p < 0.000) with the WAT scores across participants (see Figure 1).
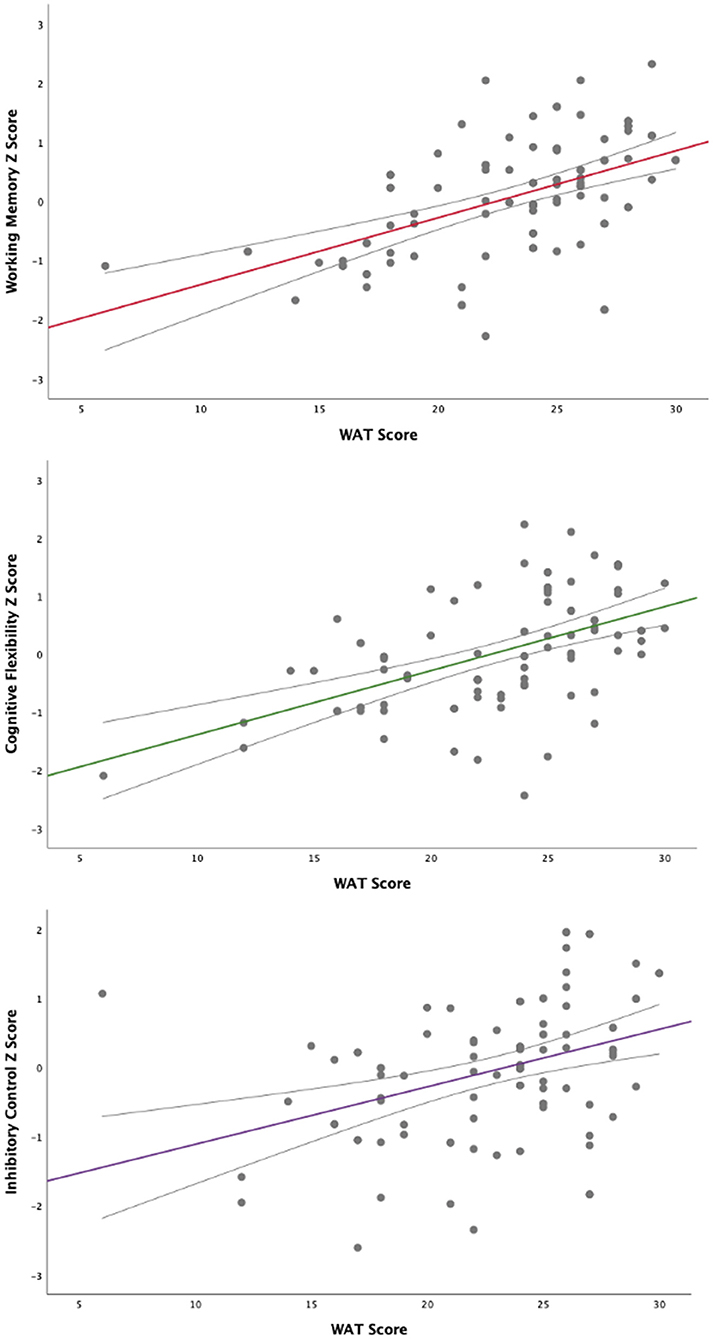
Figure 1. Correlations of executive control PCs with the WAT score.
Linear Regression for Principal Components of Executive Control
We performed the linear regression analysis using the composite factor of working memory as the dependent variable and the composite index of processing speed, years of education and age as independent variables. We observed that the WAT and processing speed scores significantly predict the working memory scores and explain 52.7% (adjusted R2) of the variability in the scores, while years of education and age did not predict working memory scores (see Table 2).
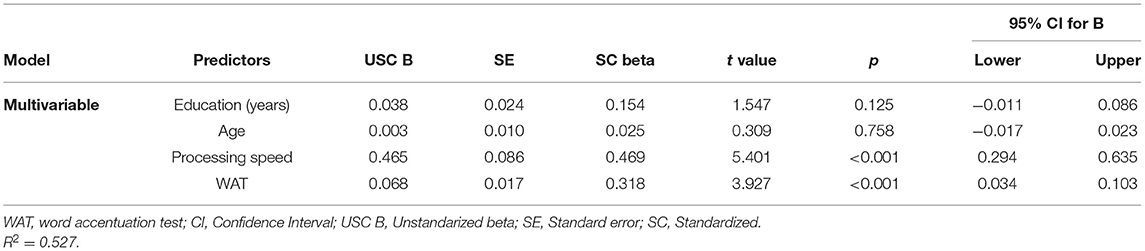
Table 2. Linear regression of years of education, age, processing speed and WAT with working memory factor as DV.
In the case of the cognitive flexibility, we observed that WAT scores, age and processing speed significantly predict the factor scores. In addition, these factors explain 62.3% (adjusted R2) of the variability (see Table 3).
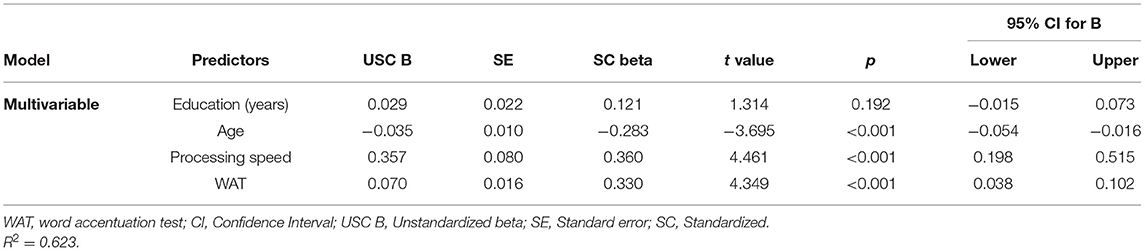
Table 3. Linear regression of years of education, age, processing speed and WAT with cognitive flexibility factor as DV.
Finally, we observed that processing speed and WAT scores predict the inhibitory control factor scores. Similarly, these factors explain 26% (adjusted R2) of the variations in the factor (see Table 4).

Table 4. Linear regression of years of education, age, processing speed and WAT with inhibitory control factor as DV.
Discussion
This study examined the association of literacy level with executive control factors in normal aging by using the word accentuation test (WAT). Our results showed better scores in working memory, cognitive flexibility and inhibitory control in subjects who performed better on the WAT. In addition, we found that scores on this measure, together with the processing speed, better predict executive control scores. These results confirm our hypothesis that literacy level is a better predictor of executive control than years of education or age.
Predictors of Scores in Executive Control
Our results show that subjects with better WAT scores exhibit a greater capacity to retain and manipulate information (working memory). These results have been confirmed in other studies (40, 41), where working memory, modulated by education, is associated with cognition during aging. This suggests that perhaps formal education strengthens the ability to select, update, and manipulate information available in the working memory, through the promotion of progressively more complex activities in classroom settings, autonomous learning and improvement curricula.
In addition, we found that WAT scores predict performance on inhibitory control measures. Thus, people with higher WAT scores and faster processing speed show a greater ability to inhibit powerful and/or automatic stimuli. Similar results have been found by de Bruin et al. (42) and Hull et al. (43). Their studies showed that inhibitory control is modulated by processing speed and the type of task used for its assessment. Some tasks are more demanding than others and therefore require more inhibitory control mechanisms to be carried out correctly.
Likewise, we found higher scores for the cognitive flexibility factor when the WAT score is higher, and performance is better predicted by this, together with age and processing speed, as has been reported in research by Gallen et al. (12). We observed that participants who are younger and those with higher literacy (higher WAT scores) have a greater capacity to change attentional and mental sets (44). This is a fundamental aspect in accomplishing complex cognitive tasks (45).
These results could help us to understand the importance of executive control mechanisms in brain and cognitive aging, showing a bigger impact in the case of low-quality education. As a result, we would observe a weakening in mechanisms associated with brain resilience, like white matter integrity and cortical thinning, which could contribute to cognitive decline in the following years (46) and cognitive reserve (47) used to compensate for cognitive changes with an alternative network or better processing strategy. Therefore, people with low literacy levels could perform worse on tasks and have a greater risk of cognitive impairment and dementia.
Literacy Level, Executive Control and Education
Literacy level allows us to explain the scores on the executive control tasks. Nonetheless, it should be noted that processing speed is a mechanism with a significant effect on adult cognitive performance (11, 48). Our data show that the measurement and analysis of literacy level (educational quality) and processing speed can more clearly explain cognitive changes in older adults than years of education. That is, exposure to quality content or being exposed to a more enriching education might make the execution of general processing tasks and those that involve executive control more efficient.
If individuals with a more efficient processing capacity faces a neurodegenerative event, they can generate brain and cognitive compensatory strategies that minimize the impact of the pathology (49–52) and reduce the risk of cognitive impairment or dementia. This could help to achieve satisfactory aging, through the implementation of cognitive reserve mechanisms (53), and thus protect against neurodegenerative pathology. This is an aspect we might not see in subjects with low literacy levels.
This first look at studying the literacy level in Peru can help us to explain the cognitive and behavioral variants observed in older adults who have different scores and performances despite having the same years of education. We consider that literacy level is a more accurate measure than years of education when assessing the effect of formal education on cognition and, consequently, as a protective factor for the development of neurodegenerative pathologies. This is particularly important in settings such as Peru where the quality of education is highly variable, educational quality statistics are below international standards (54) and where the education received depends on socioeconomic status and area of residence (55).
Limitations
Our findings are interesting, but they are not without limitations. As we do not have a group of subjects with a clinical diagnosis (mild cognitive impairment or mild Alzheimer's), we cannot establish a point of comparison with impairment at the executive and cognitive level derived from the WAT score. Furthermore, since it is a cross-sectional study, we cannot precisely establish the protective factor of literacy level. We need to carry out longitudinal studies to estimate the level of protection participants have against deterioration. Furthermore, the Socio-Economic Status (SES) and Intelligence Quotient (IQ) have not been considered in the present study and could be associated with the results obtained (56). The impact of SES on cognition could be mitigated by years of schooling, literacy level, and other environmental factors (57), so they need to be evaluated in future research. Finally, as we do not have a standardized WAT test in Peru, we used the Ecuadorian version. Despite similarities between Andean nations in many aspects (e.g., culturally, educational, etc.), it is necessary to validate the WAT in the Peruvian context.
Conclusions
We can conclude that literacy level, measured through the WAT, is significantly correlated with executive control processes in elderly people in Peru. One interpretation of this is that higher educational quality in young age (as indicated by literacy scores in older age) favor a better development of executive control over the life span.
In this context, we consider that in Peru it is not only illiterate people who have a higher risk of developing dementia, but also adults with lower scores in literacy level and quality of education measures. Consequently, there is a need to develop programs aimed at improving educational quality from the early years of education. This is in addition to the implementation of cognitive intervention programs that favor cognitive mechanisms such as attention and executive function among our adults.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by the Ethics Committee of the Research unit of San Pablo Catholic University (Acta N° 012.CEDI.UCSP.2020). Written informed consent to participate in this study was provided by the patients/participants.
Author Contributions
MS-A: designed the study, performed the statistical analysis and the preparation, and final approval of the manuscript. NL: participated in the statistical analysis and in the preparation and final revision of the manuscript. CR-F and VB-H: analyzed the data and participate in the preparation and final revision of the manuscript. SF-G: designed the study and revised and approved the manuscript. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2021.629048/full#supplementary-material
References
1. United Nations, Department of Economic and Social Affairs, Population Division. World Population Prospects. (2019)
2. Parra MA, Baez S, Allegri R, Nitrini R, Lopera F, Slachevsky A, et al. Dementia in Latin America: Assessing the present and envisioning the future. Neurology. (2018) 90:222–31. doi: 10.1212/WNL.0000000000004897
3. Arce Rentería M, Vonk J, Felix G, Avila JF, Zahodne LB, Dalchand E, et al. Illiteracy, dementia risk, and cognitive trajectories among older adults with low education. Neurology. (2019) 93:e2247–56. doi: 10.1212/WNL.0000000000008587
4. Nitrini R, Bottino C, Albala C, Santos S, Custodio N, Ketzoian C, et al. Prevalence of dementia in Latin America: a collaborative study of population-based cohorts. Int Psychogeriat. (2009) 21:622–30. doi: 10.1017/S1041610209009430
5. Mantri S, Nwadiogbu C, Fitts W, Dahodwala N. Quality of education impacts late-life cognition. Int J Geriatr Psychiatry. (2019) 34:855–62. doi: 10.1002/gps.5075
6. Manly J, Touradji P, Tang M, Stern Y. Literacy and memory decline among ethnically diverse elders. J Clini Exp Neuropsychol. (2003) 25:680–90 doi: 10.1076/jcen.25.5.680.14579
7. Manly J, Schupf N, Tang M, Stern Y. Cognitive decline and literacy among ethnically diverse elders. J Geriatr Psychiatry Neurol. (2005) 18:213–17 doi: 10.1177/0891988705281868
8. Gamaldo AA, Sardina AL, Corona RT, Willingham K, Migoyo RV, Andel RA. The association between educational parameters and a cognitive screening measure in older blacks. Int Psychogeriatr. (2018) 30:311–22. doi: 10.1017/S1041610217001107
9. Sisco S, Gross AL, Shih RA, Sachs BC, Glymour MM, Bangen KJ, et al. The role of early-life educational quality and literacy in explaining racial disparities in cognition in late life. J Gerontol B Psychol Sci Soc Sci. (2015) 70:557–67. doi: 10.1093/geronb/gbt133
10. UNESCO. Replantear la educación. ‘Hacia un buen común mundial? (2015) Available online at: http://unesdoc.unesco.org/images/0023/002326/232697s.pdf
11. Salthouse TA. Trajectories of normal cognitive aging. Psychol Aging. (2019) 34:17–24. doi: 10.1037/pag0000288
12. Gallen CL, Turner GR, Adnan A, D'Esposito M. Reconfiguration of brain network architecture to support executive control in aging. Neurobiol Aging. (2016) 44:42–52. doi: 10.1016/j.neurobiolaging.2016.04.003
13. Friedman NP, Miyake A. Unity and diversity of executive functions: Individual differences as a window on cognitive structure. Cortex. (2017) 86:186–204. doi: 10.1016/j.cortex.2016.04.023
14. Park DC, Reuter-Lorenz P. The adaptive brain: aging and neurocognitive scaffolding. Annu Rev Psychol. (2009) 60:173–96. doi: 10.1146/annurev.psych.59.103006.093656
15. Turner G, Spreng N. Executive functions and neurocognitive aging: dissociable patterns of brain activity. Neurobiol of Aging. (2012) 33:826e1–826e13. doi: 10.1016/j.neurobiolaging.2011.06.005
16. Schroeter ML, Vogt B, Frisch S, Becker G, Barthel H, Mueller K, et al. Executive deficits are related to the inferior frontal junction in early dementia. Brain. (2012) 135:201–15. doi: 10.1093/brain/awr311
17. Isingrini M, Angel L, Fay S, Taconnat L, Lemaire P, Bouazzaoui B. Age-related differences in the reliance on executive control in working memory: role of task demand. PLoS ONE. (2015) 10:e0145361. doi: 10.1371/journal.pone.0145361
18. Colangeli S, Boccia M, Verde P, Guariglia P, Bianchini F, Piccardi L. Cognitive reserve in healthy aging and Alzheimer's Disease: A meta-analysis of fMRI studies. Am J Alzheimers Dis Other Demen. (2016) 31:443–9. doi: 10.1177/1533317516653826
19. Cabeza R, Albert M, Belleville S, Craik F, Duarte A, Grady CL, et al. Maintenance, reserve and compensation: the cognitive neuroscience of healthy ageing. Nat Rev Neurosci. (2018) 19:701–10. doi: 10.1038/s41583-018-0068-2
20. Daselaar S, Iyengar V, Davis S, Eklund K, Hayes S, Cabeza R. Less wiring, more firing: low-performing older adults compensate for impaired white matter with grater neural activity. Cerebral Cortex. (2013) 25:983–90. doi: 10.1093/cercor/bht289
21. Pusil S, López ME, Cuesta P, Bruña R, Pereda E, Maestú F. Hypersynchronization in mild cognitive impairment: the 'X' model. Brain. (2019) 142:3936–50. doi: 10.1093/brain/awz320
22. Bright P, Jaldow E, Kopelman MD. The National Adult Reading Test as a measure of premorbid intelligence: a comparison with estimates derived from demographic variables. J Int Neuropsychol Soc. (2002) 8:847–54. doi: 10.1017/S1355617702860131
23. Lezak MD, Howieson DB, Bigler ED, Tranel D. Neuropsychological Assessment. 5th ed New York: Oxford University Press. (2012).
24. Gonzales Montalvo J.Creación y validación de un test de lectura para el diagnco del deterioro mental en el anciano. Tesis doctoral. Madrid: Universidad Complutense de Madrid (1991).
25. Sierra, N, Torralva, T, Roca, M, Manes, F, Burin, D. Estimación de la inteligencia premórbida en deterioro cognitivo leve y moderado y en déficit ejecutivo. Revista Neuropsicologia Latinoamericana. (2010) 2:25–32.
26. Pluc, G, Almeida-Meza P, Gonzalez-Lorza A, Muñoz-Ycaza RA, Trueba AF. Estimación de la Función Cognitiva Premórbida con el Test de Acentuación de Palabras. Rev Ecuat Neurol. (2017) 26:226–34. Available online at: http://scielo.senescyt.gob.ec/scielo.php?script=sci_arttext&pid=S2631-25812017000200226&lng=es.
27. Contador I, Bermejo-Pareja F, Del Ser T, Benito-León J. Effects of education and word reading on cognitive scores in a community-based sample of Spanish elders with diverse socioeconomic status. J Clin Exp Neuropsychol. (2015) 37:92–101. doi: 10.1080/13803395.2014.989819
28. Soto-Añari M, Flores G, Fernández-Guinea S. Nivel de lectura como medida de reserva cognitiva. Revista de neurología. (2013) 56:79–85. doi: 10.33588/rn.5602.2012402
29. Stern Y, Chételat G, Habeck C, Arenaza-Urquijo EM, Vemuri P, Estanga A, et al. Mechanisms underlying resilience in ageing. Nat Rev Neurosci. (2019) 20:246. doi: 10.1038/s41583-019-0138-0
30. Custodio, N, Lira, D. Adaptación peruana del Mini-mental State Examination (MMSE). Rev invest UNMSN. Anales de la Facultad de Medicina. (2014) 75:69. doi: 10.15381/anales.v75i1.6951
31. De la Torre Maslucan J, Shimabukuro Maeki R, Varela Pinedo L, Krüger Malpartida H, Huayanay Falconí L, Cieza Zevallos J, et al. Validación de la versión reducida de la escala de depresión geriátrica en el consultorio externo de geriatría del Hospital Nacional Cayetano Heredia. Acta méd. peruana [Internet]. (2006) 23:144–7. Available online at: http://www.scielo.org.pe/scielo.php?script=sci_arttext&pid=S1728-59172006000300003&lng=es.
32. Reisberg B, Ferris S, de León M, Crook T. The global deterioration scale for assessment of primary degenerative dementia. Am J Psychiat. (1982) 139:1136–9 doi: 10.1176/ajp.139.9.1136
34. Hobert M, Niebler R, Meyer S, Brochmann K, Becker C, Huber H, et al. Poor trail making test performance is directly associated with altered dual task prioritization in the elderly – baseline results from the TREND study. PLOS ONE. (2011) 6:e27831. doi: 10.1371/journal.pone.0027831
35. Olabarrieta-Landa L, Rivera D, Galarza-del-Angel J, Garza MT, Saracho CP, Rodríguez W, et al. Verbal Fluency Tests: Normative data for the Latin American Spanish speaking adult population. Neuro Rehabilitation. (2015) 37:515–61. doi: 10.3233/NRE-151279
36. Rivera D, Perrin PB, Stevens LF, Garza MT, Weil C, Saracho CP, et al. Stroop color-word interference test: Normative data for the Latin American Spanish speaking adult population. Neuro Rehabilitation. (2015) 37:591–624. doi: 10.3233/NRE-151281
37. Dubois B, Slachevsky A, Litvan I, Pillon B. The FAB: a frontal assesment battery at bedside. Neurology. (2000) 55:1621–26. doi: 10.1212/WNL.55.11.1621
38. Arango-Lasprilla JC, Rivera D, Aguayo A, Rodríguez W, Garza CT, Saracho CP, et al., Trail Making Test: Normative data for the Latin American Spanish speaking adult population. Neuro Rehabilitation. (2015) 37:639–61. doi: 10.3233/NRE-151284
39. Perea MV, García R, Cañas M, Ladera V. Velocidad de procesamiento de la información en la enfermedad de Alzheimer. Revista chilena de neuro-psiquiatría. (2019) 57:228–37. doi: 10.4067/S0717-92272019000300228
40. Pliatsikas C, Veríssimo J, Babcock L, Pullman MY, Glei DA, Weinstein M, et al. Working memory in older adults declines with age, but is modulated by sex and education. Q J Exp Psychol (Hove). (2019) 72:1308–27. doi: 10.1177/1747021818791994
41. Adrover-Roig D, Sesé A, Barceló F, Palmer A. Latent variable approach to executive control in healthy aging. Brain Cogn. (2012) 78:284–99. doi: 10.1016/j.bandc.2012.01.005
42. de Bruin A, Sala SD. Effects of age on inhibitory control are affected by task-specific features. Q J Exp Psychol (Hove). (2018) 71:1219–33. doi: 10.1080/17470218.2017.1311352
43. Hull R, Martin R., Beie, M, Lane D, Hamilton C. Executive function in older adults: a structural equation modelling approach Neuropsychology. (2008) 22:508–22. doi: 10.1037/0894-4105.22.4.508
44. Friedman N, Miyake A, Young S, DeFries J, Corley R. Hewitt J. Individual difrerences in executive functions are almost entirely genetic in origin J Exp Psychol Gen. (2008) 137:201–25. doi: 10.1037/0096-3445.137.2.201
45. López N, Véliz A, Soto-Añari M, Ollari J, Chesta S, Allegri R. Efectos de un programa combinado de actividad física y entrenamiento cognitivo en pacientes chilenos con Alzheimer leve. Neurología Argentina. (2015) 73:131–9. doi: 10.1016/j.neuarg.2015.04.001
46. Vemuri P, Lesnick TG, Knopman DS, Przybelski SA, Reid RI, Mielke MM, et al. Amyloid, vascular, and resilience pathways associated with cognitive aging. Ann Neurol. (2019) 86:866–77. doi: 10.1002/ana.25600
47. Bettcher BM, Gross AL, Gavett BE, Widaman KF, Fletcher E, Dowling NM, et al. Dynamic change of cognitive reserve: associations with changes in brain, cognition, and diagnosis. Neurobiol Aging. (2019) 83:95–104. doi: 10.1016/j.neurobiolaging.2019.08.016
48. Craik F, Bialystok E. Cognition through the lifespan: mechanisms of change. TRENDS in Cognitive Science. (2006) 10:131–9. doi: 10.1016/j.tics.2006.01.007
49. Skouras S, Falcon C, Tucholka A, Rami L, Sanchez-Valle R, Lladó A, et al. Mechanisms of functional compensation, delineated by eigenvector centrality mapping, across the pathophysiological continuum of Alzheimer's disease. Neuroimage Clin. (2019) 22:101777. doi: 10.1016/j.nicl.2019.101777
50. Daselaar S, Cabeza R. Age-related changes in hemispheric organization. En Cabeza, R., Nyberg, L. y Park, D. (Eds). Cognitive neurosciences of aging: linking cognitive and cerebral aging. London: Oxford University press. (2005) p. 325–35. doi: 10.1093/acprof:oso/9780195156744.003.0014
51. Davis S, Dennis N, Daselaar S, Fleck M. Cabeza, R. Que PASA The posterior anterior shift in aging. Cereb cortex. (2008) 22:1201–9. doi: 10.1093/cercor/bhm155
52. Reuter-Lorenz P, Park D. How does it STAC Up? Revisiting the Scaffolding Theory of Aging and Cognition. Neuropsychol Rev. (2014) 24:355–70. doi: 10.1007/s11065-014-9270-9
53. Stern Y, Arenaza-Urquijo EM, Bartrés-Faz D, Belleville S, Cantilon M, Chetelat G, et al. Whitepaper: Defining and investigating cognitive reserve, brain reserve, and brain maintenance. Alzheimers Dement. (2020) 16:1305–11. doi: 10.1016/j.jalz.2018.07.219
54. Ministerio de Educación. Oficina de medición de la calidad de los aprendizajes. Evaluación PISA. MINEDU. (2018). Available online at: http://umc.minedu.gob.pe/wp-content/uploads/2020/10/PPT-PISA-2018_Web_vf-15-10-20.pdf
55. Beltrán A, Seinfeld J. Hacia una educación de calidad: la importancia de los recursos pedagógicos en el rendimiento escolar. Lima: Universidad del Pacífico. (2011)
56. Hackman DA, Farah MJ, Meaney MJ. Socioeconomic status and the brain: mechanistic insights from human and animal research. Nat Rev Neurosci. (2010) 11:651–9. doi: 10.1038/nrn2897
Keywords: literacy level, executive control, aging, neuropsychology, dementia, education
Citation: Soto-Añari M, López N, Rivera-Fernández C, Belón-Hercilla V and Fernández-Guinea S (2021) Literacy Level and Executive Control in Healthy Older Peruvian Adults. Front. Neurol. 12:629048. doi: 10.3389/fneur.2021.629048
Received: 13 November 2020; Accepted: 30 July 2021;
Published: 26 August 2021.
Edited by:
Christopher Butler, University of Oxford, United KingdomReviewed by:
Maria Paula Foss, University of São Paulo, BrazilLambros Messinis, Aristotle University of Thessaloniki, Greece
Vera U. Ludwig, University of Pennsylvania, United States
Pablo Luis Martino, Universidad Nacional de Rosario, Argentina
Tanu Wadhera, Dr. B. R. Ambedkar National Institute of Technology Jalandhar, India
Copyright © 2021 Soto-Añari, López, Rivera-Fernández, Belón-Hercilla and Fernández-Guinea. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marcio Soto-Añari, bXNvdG9AdWNzcC5lZHUucGU=