 Márcio Schneider Medeiros1*
Márcio Schneider Medeiros1* Artur Francisco Schumacher-Schuh1,2Vivian Altmann3
Artur Francisco Schumacher-Schuh1,2Vivian Altmann3 Carlos Roberto de Mello Rieder3
Carlos Roberto de Mello Rieder3- 1Serviço de Neurologia, Hospital de Clínicas de Porto Alegre, Porto Alegre, Brazil
- 2Departamento de Farmacologia, Universidade Federal do Rio Grande do Sul, Porto Alegre, Brazil
- 3Departamento de Neurologia, Universidade Federal de Ciências da Saúde de Porto Alegre, Porto Alegre, Brazil
Introduction: Coffee has been inversely associated with Parkinson's disease (PD) in many studies, and caffeine is the leading candidate to mediate this effect. Mate (Ilex paraguariensis, IP), a caffeinated beverage rich in antioxidants consumed in South America, was also inversely associated with PD in one study from Argentina. Other varieties of IP infusion, such as chimarrão, were never studied in PD. Chimarrão is a common caffeinated beverage consumed in Brazil made with the leaves and stems of IP.
Methods: A case–control study was conducted to evaluate the relationship between chimarrão ingestion and PD in southern Brazil. All subjects answered a questionnaire about the frequency of chimarrão and coffee intake. A multiple regression analysis adjusted for age and sex was performed to assess the association between PD and chimarrão consumption.
Results: We included 200 PD patients and 200 healthy controls. High consumption of chimarrão was inversely associated with PD (OR = 0.44, 95% CI = 0.24–0.81, P = 0.008). High consumption of coffee was also inversely associated with PD, as expected. Chimarrão remained associated when adjusted for coffee consumption, smoking history, and age (OR 0.46, 95% CI = 0.25–0.86, P = 0.014). These two exposures showed an additive effect.
Conclusion: Chimarrão consumption was inversely associated with PD, even after adjusting for coffee intake, suggesting a possible protective role. IP's effect can be mediated by caffeine and through its antioxidant components. Chimarrão has a lower concentration of caffeine compared with coffee and has numerous substances with antioxidative effects that may be important to PD protection. Further studies are needed to test this hypothesis.
Introduction
The etiology of Parkinson's disease (PD) is not fully understood, and different environmental factors have been associated with PD. These factors are thought to either enhance the risk of developing the disease or provide a protective effect. Coffee is inversely associated with PD, and this effect seems to be mediated by caffeine (1). Several studies have found this association, supporting the evidence of the protective effect of caffeine in PD (1, 2), with a more evident outcome in men (2). Other caffeinated beverages have also been studied, especially tea (3), corroborating the protective role hypothesis of caffeine on PD. Caffeine acts on adenosine A2 receptors on dopaminergic D2 neurons in the substantia nigra, a mechanism potentially implicated with a neuroprotective effect (4). By antagonizing these receptors, caffeine alters dopamine transmission, protects against glutamatergic excitotoxicity, and frees radicals such as nitric oxide (5).
Chimarrão, a hot infusion of Ilex paraguariensis (IP), is a common caffeinated beverage consumed in Brazil. IP is a native plant from South America, and chimarrão was first consumed by its indigenous people. In the Seventeenth century, it was adopted by Spanish and Portuguese colonizers, and nowadays, it is consumed daily by ~30% of the population in southern Brazil (6). It is also popular in Uruguay, Argentina, and Paraguay, where it is called mate. However, chimarrão contains both leaves and stems, different from the mate consumed in Argentina, which is usually free of stems. Mate was previously associated with lower PD risk in Argentina, and caffeine was considered the probable mediator of this effect (7). Previous studies have demonstrated a high content of antioxidants and substances with iron chelation properties in IP, which could elicit a potential protective effect on PD (8, 9). In a recent study by Bernardi et al. (10), they demonstrated that IP may have a strong neuroprotective activity on dopaminergic neurons, preventing their death with a dose-dependent effect (10).
The hypothesis of a neuroprotective effect of IP infusions on PD is understudied. Whether this effect is due to caffeine alone or in combination with antioxidants is yet to be demonstrated. We conducted a case–control study to further investigate the effect of IP on PD.
Methods
This is an observational analytic (case–control study) based on a single cohort of 233 Parkinson's disease subjects from the Movement Disorders Clinic at a University hospital in Porto Alegre, Brazil. All patients were selected between 2006 and 2012 and evaluated by neurologists with training in movement disorders (AFSS and MSM), and the diagnosis of PD was defined according to the UK Parkinson's Disease Society Brain Bank Research criteria (11) and followed until 2019. This cohort has been described elsewhere (12). A subset of 200 patients answered surveys with information about coffee and chimarrão intake, smoking history, and disease characteristics, such as age at onset and disease duration in the years 2016–2017. Inclusion criteria were patients with a diagnosis of PD and no evidence of cognitive decline defined by the Mini Mental State Examination. We excluded patients younger than 45 years of age and individuals diagnosed with vascular or atypical parkinsonism. From a study group at the same hospital, 200 healthy individuals without any neurological conditions, including cognitive decline, were selected as the control group in the same period, between 2016 and 2017. Control subjects were excluded if there was any suspicion of a neurodegenerative disorder and the possibility of drug-induced parkinsonism. Patient and control groups were matched for sex and age. Sample size was calculated using the following parameters: a matched case–control study, an expected odds ratio of 0.64, the prevalence of chimarrão consumption in southern Brazil of 30%, an alpha level of 0.05, a power of 0.90, and a moderate correlation between case and control exposures for matched pairs (0.2). The estimated sample size was 116 cases and 116 controls.
Study subjects from both case and control groups answered an environmental exposure questionnaire where the frequency and quantity of chimarrão and coffee consumption were estimated. The number of specific cups used for chimarrão (cuias) and coffee was recorded in the following categories: never, < 2 cups/cuias per week, 2–6 cups/cuias per week, 1–2 cups/cuias per day, 3–5 cups/cuias per day, and 6 or more cups/cuias per day. Data on years of consumption for both beverages were also collected to estimate lifelong intake. Smoking history was categorized as ever vs. never, and a history of smoking at least 100 cigarettes during a lifetime was required to be considered as a positive smoking history.
Chimarrão has a lower concentration of caffeine (8–27 mg/150 ml) compared with coffee (58–109 mg/150 ml) (13), and to control for this difference, two variables representing low and high levels of consumption of each caffeinated beverage were created. In these variables, high consumption of chimarrão (daily consumption of at least 6 cuias) and high consumption of coffee (daily consumption of at least 3 cups) were defined.
Two final variables of total caffeine intake were created. First, a variable was created to identify the difference between individuals who never consumed caffeinated beverages and individuals who consumed both beverages. The second variable evaluated the amount of caffeine when both beverages were consumed: no caffeinated beverages, low consumption of both chimarrão and coffee, and high consumption of both chimarrão and coffee.
This study was approved by the local ethics committee and all subjects provided written informed consent.
Statistical Analyses
All statistics were performed with R 3.5.2. Data on age and years of ingestion of chimarrão and coffee were compared between the two groups with Student t-test. Differences in sex and individuals with positive smoking history were analyzed using χ2 test. Logistic regression analysis was performed to assess the effect of chimarrão and coffee intake on PD (using the variables for consumption defined above), adjusting for possible confounding variables.
Results
We included 200 PD patients and 200 controls. There was no statistical difference concerning sex and age. Both groups had ~50% male individuals. The mean age for cases and controls were 65.69 (SD = 10.52) and 67.35 (SD = 9.23), respectively. The mean disease duration for PD patients was 8.78 (SD = 6.05) years. There was no difference in years of chimarrão and coffee consumption between the groups. Smoking history was significantly higher in the control group (P < 0.001). Sociodemographic characteristics of the population and consumption of chimarrão and coffee are shown in Table 1.
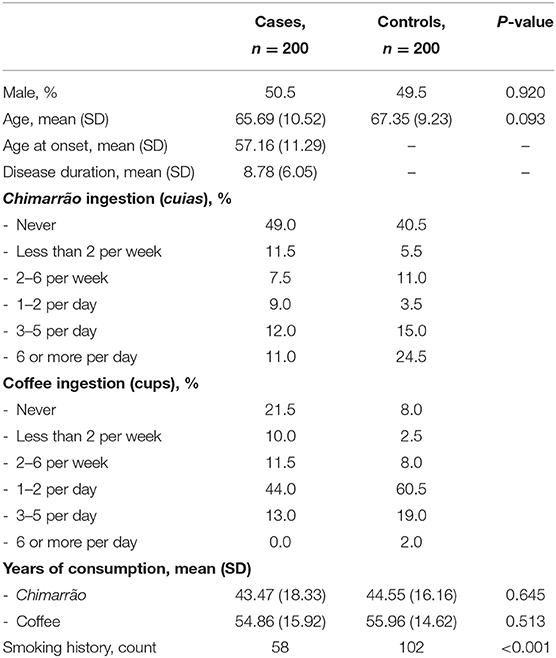
Table 1. Demographic data of cases and control subjects.
Univariate analysis showed a significant association of high consumption of chimarrão with PD (OR 0.37, 95% CI = 0.21–0.66, P = 0.001) but no association of low consumption (P = 0.798). As for coffee, low and high ingestions were associated with PD (OR 0.31, 95% CI = 0.19–0.50, P < 0.001 and OR 0.27, 95% CI = 0.14–0.50, P < 0.001, respectively). Smoking history was also inversely associated with PD (OR 0.39, 95% CI = 0.26–0.59, P < 0.001). There was no association of the duration of chimarrão and coffee consumption and PD diagnosis. Age was not significantly associated as well (Table 2).
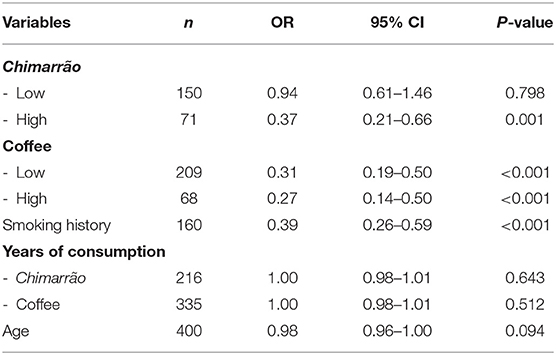
Table 2. Univariate analysis of chimarrão and coffee consumption, smoking history, years of consumption, and age (chimarrão low consumption <6 cuias/day; chimarrão high consumption ≥6 cuias/day; coffee low consumption <3 cups/day; coffee high consumption ≥3 cups/day).
In the logistic regression analysis, after adjusting for smoking history and age, the high consumption of chimarrão remained associated with PD (OR 0.44, 95% CI = 0.24–0.81, P = 0.008). Low and high consumption of coffee also remained associated with PD (Table 3).
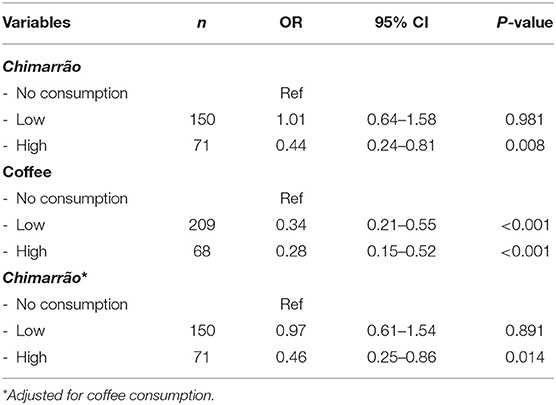
Table 3. Model of chimarrão and coffee consumption adjusted for smoking history and age (chimarrão low consumption <6 cuias/day; chimarrão high consumption ≥6 cuias/day; coffee low consumption <3 cups/day; coffee high consumption ≥3 cups/day).
The chimarrão model was adjusted for coffee consumption and the high consumption category remained inversely associated with PD independent of smoking history and age (OR 0.46, 95% CI = 0.25–0.86, P = 0.014).
Finally, a total caffeine effect was assessed by the variables including the intake of both chimarrão and coffee. The first analysis identified a lower OR when both beverages are consumed compared with either beverage alone (OR 0.23, 95% CI = 0.10–0.55, P = 0.001). The second variable (divided in three categories based on the quantity of caffeine consumed—no consumption, low consumption of both chimarrão and coffee, and high consumption of both chimarrão and coffee) indicated a strong association of low and high total caffeine consumption and PD, again with lower ORs compared to the either beverage alone (OR 0.28, 95% CI = 0.12–0.66, P = 0.003 and OR 0.20, 95% CI = 0.09–0.48, P < 0.001, respectively) (Table 4).
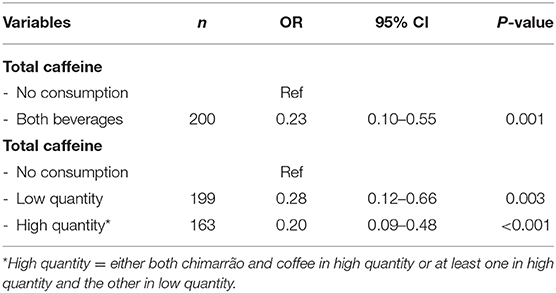
Table 4. Evaluation of total caffeine as no consumption and consumption of both beverages and total caffeine as both beverages in low vs. high consumption—multivariate analysis adjusted for smoking history and age.
Discussion
The present study shows a lower consumption of chimarrão among PD patients compared with matched controls, suggesting that it can be a protective factor for the disease. In Argentina, mate was associated with lower rates of PD in one previous study (7), and other caffeinated teas were also inversely associated with PD in different countries (14, 15). Studies with Japanese and Chinese populations showed protective effects of black tea independent of coffee intake (3).
With regard to the consumption of chimarrão, individuals in the control group showed a higher intake compared with PD patients. In Argentina, mate consumption was also inversely associated with PD in that population (7). Interestingly, Gatto et al. described a dose-dependent effect of mate with ORs ranging from 0.50 to 0.23 for intakes of 0.5–1 L/day and more than 1 L/day, respectively (7). The fact that in our study only high chimarrão consumption showed an inverse association with PD could be explained by the lower concentration of leaves in chimarrão compared with the Argentinian mate. This could lead to different concentrations of caffeine in the two kinds of IP infusion. Therefore, if both coffee and chimarrão have protective effects due to their caffeine content and its effect on adenosine A2 receptors, lower concentrations of caffeine in chimarrão [about one third compared with a cup of coffee (13)] may explain why only the high consumption group was associated with lower PD.
Chimarrão is widely consumed in southern Brazil. Although it is similar to the mate prepared in other South American countries, the Brazilian infusion usually contains more stems than the Argentinian mate, made only with the leaves. The leaves are where the studied compounds of the plant are found, including not only caffeine, but also other substances with antioxidative activity. The Brazilian blend contains more powder than other blends, has a vibrant and intense green color, and is readily packed after the harvest, unlike the Argentinian type which is left to age.
Among the substances found in IP, several can mediate a possible neuroprotective effect. One of its important compounds, chlorogenic acid (CGA), attenuated lipid and protein oxidation in a model of chronic immobilization stress (CIS) in rats (8). It also prevented the decrease in superoxide dismutase (Sod) and catalase (Cat) activities after induced seizures in the brains of Wistar rats (9). In another study with oxidative stress by De Lima et al. CGA was unable to prevent all the alterations induced by CIS, suggesting that the protective properties of IP are the result of the combined effects of all its antioxidant compounds, which includes caffeine (16). Bixby et al. in 2005 found a potent, dose-dependent protective effect against oxidative stress and the highest inhibition of protein nitration in IP compared with wine and green tea (17). The fact that the total caffeine variables were highly associated with lower PD individuals and had lower OR compared with the separate consumption of the two drinks indicates that both beverages have additive effects. Although no definite conclusions can be taken from that, this could suggest that IP and coffee may not have the same mechanisms of action—IP may act through caffeine and antioxidants.
More recently, Bernardi et al. (10) showed that IP has protective effects on dopaminergic neurons, preventing neuronal death in cell culture (10). Our study did not evaluate IP composition and the concentration of caffeine and antioxidants, but both mechanisms should be considered. Chimarrão may be less concentrated than other IP infusions, but it is possible that even more concentrated versions, as the mate consumed in Argentina, may not reach the concentration of antioxidants tested in animal and cellular studies.
In our sample, coffee consumption was lower among PD patients, and it corroborates the idea that coffee confers protection for PD, being inversely associated with PD in several studies (1, 2, 18). Caffeine also presents a possible symptomatic effect as well as an interference in disease progression. It has been associated with reduced accrual of motor and non-motor symptoms in a 4-year follow-up study in Italy and corroborated by a recent meta-analysis (19, 20). In addition, it has also been inversely associated with the development of dyskinesias (21).
Smoking is usually related to PD as a protective factor, frequently associated with coffee intake (22, 23). In our study, the results of the caffeinated drinks remained inversely associated after adjusting for smoking history.
Study Limitations and Strengths
The self-reported data, the estimation of ingestion, and caffeine concentration used in this study are limitations to be considered because of a memory bias. Patients had to remember how many cups they generally drank per week and for how many years. This bias is due to our study design, but it should be considered that the estimation was used in both case and control groups, limiting a possible negative effect of this bias. Also, we should consider as limitations the fact that we were unable to define the size of cups and cuias used by each individual, and it was not possible to evaluate the concentration of caffeine in the coffee and chimarrão consumed.
Finally, we should highlight that our study included patients from a movement disorder clinic increasing diagnostic accuracy, controls were matched for age and sex, and smoking history was included in the analysis.
Conclusion
Chimarrão was inversely associated with PD in the category of high consumption individuals. This is the first time chimarrão is studied in the context of Parkinson's disease, bringing new information concerning IP and neurodegeneration. Coffee also showed a possible protective effect on the disease as different studies have previously shown. These two exposures exhibited an additive effect, and it is not possible to conclude that chimarrão acts only through its caffeine content. New evidence of neuroprotection points to possible effects of other antioxidant substances in I. paraguariensis, although our results cannot support this hypothesis. Designing studies with a more accurate ingestion record, measuring the levels of caffeine/antioxidants consumed, and controlling dietetic sources of caffeine pose methodological challenges, but an effort in this direction would be warranted to confirm these findings.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Comitê de Ética do Hospital de Clínicas de Porto Alegre. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
MM contributed with data collection, analysis, and manuscript elaboration. VA participated in data collection and manuscript elaboration. AS-S and CR helped with the study concept and were important to interpret the results and to revise the final manuscript. All authors contributed to the article and approved the submitted version.
Funding
This project received funding from the Fundo de Incentivo à Pesquisa (FIPE-HCPA) and CNPq. It was part of MM's doctoral thesis.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Hernán MA, Takkouche B, Caamaño-Isorna F, Gestal-Otero JJ. A meta-analysis of coffee drinking, cigarette smoking, and the risk of Parkinson's disease. Ann Neurol. (2002) 52:276–84. doi: 10.1002/ana.10277
2. Costa J, Lunet N, Santos C, Santos J, Vaz-Carneiro A. Caffeine exposure and the risk of Parkinson's disease: a systematic review and meta-analysis of observational studies. J Alzheimer's Dis. (2010) 20(Suppl. 1):S221–38. doi: 10.3233/JAD-2010-091525
3. Tanaka K, Miyake Y, Fukushima W, Sasaki S, Kiyohara C, Tsuboi Y, et al. Intake of Japanese and Chinese teas reduces risk of Parkinson's disease. Park Relat Disord. (2011) 17:446–50. doi: 10.1016/j.parkreldis.2011.02.016
4. Rivera-Oliver M, Díaz-Ríos M. Using caffeine and other adenosine receptor antagonists and agonists as therapeutic tools against neurodegenerative diseases: a review. Life Sci. (2014) 101:1–9. doi: 10.1016/j.lfs.2014.01.083
5. Yadav S, Prakash S. Role of secondary mediators in caffeine-mediated neuroprotection in maneb- and paraquat-induced Parkinson' s disease phenotype in the mouse. (2012) 37:875–84. doi: 10.1007/s11064-011-0682-0
6. Antioxidant Activity of Ilex Paraguariensis And Related Species, Rosana Filip MS, Silvina B, Lotito MS. l Pharmacognosy, and l Physical Chemistry-PRALIB. School Pharmacy Biochem Universit. (2000)20:1437–46. doi: 10.1016/S0271-5317(00)80024-X
7. Gatto EM, Melcon C, Parisi VL, Bartoloni L, Gonzalez CD. Inverse association between yerba mate consumption and idiopathic Parkinson's disease. A case-control study. J Neurol Sci. (2015) 356:163–7. doi: 10.1016/j.jns.2015.06.043
8. Colpo AC, de Lima ME, Maya-López M, Rosa H, Márquez-Curiel C, Galván-Arzate S, et al. Compounds from Ilex paraguariensis extracts have antioxidant effects in the brains of rats subjected to chronic immobilization stress. Appl Physiol Nutr Metab. (2017) 42:1172–8. doi: 10.1139/apnm-2017-0267
9. Branco CDS, Scola G, Rodrigues AD, Cesio V, Laprovitera M, Heinzen H, et al. Anticonvulsant, neuroprotective and behavioral effects of organic and conventional yerba mate (Ilex paraguariensis St. Hil.) on pentylenetetrazol-induced seizures in Wistar rats. Brain Res Bull. (2013) 92:60–8. doi: 10.1016/j.brainresbull.2012.11.008
10. Bernardi A, Ballestero P, Schenk M, Ferrario M, Rivero R, Avale E, et al. Yerba mate (Ilex paraguariensis) favors survival and growth of dopaminergic neurons in culture. Mov Disord. (2019) 34:920–2. doi: 10.1002/mds.27667
11. Hughes A. UK Parkinson's disease society brain bank clinical diagnostic criteria. J Neurol Neurosurg Psychiatry. (1992) 55:181–4.
12. Rieck M, Schuh AFS, Altmann V, Francisconi CL, Fagundes PT, Monte TL, et al. DRD2 haplotype is associated with dyskinesia induced by levodopa therapy in Parkinson' s disease patients. Pharmacogenomics. (2012) 1701–10. doi: 10.2217/pgs.12.149
13. Amelia S, Tfouni V, Camara MM, Kamikata K, Moralez F, Gomes L, et al. Caffeine in teas: levels, transference to infusion and estimated intake. Food Sci Technol. (2018) 38:661–6. doi: 10.1590/1678-457x.12217
14. Hu G, Bidel S, Jousilahti P, Antikainen R, Tuomilehto J. Coffee and tea consumption and the risk of Parkinson's disease. Mov Disord. (2007) 22:2242–8. doi: 10.1002/mds.21706
15. Tan LC, Koh W, Yuan J, Wang R, Au W, June H, et al. Differential effects of black versus green tea on risk of Parkinson's disease in the Singapore Chinese health study. Am J Epidemiol. (2009) 167:553–60. doi: 10.1093/aje/kwm338
16. De Lima ME, Colpo AZC, Maya-lópez M, Rangel-lópez E, Folmer V, Santamaría A. Comparing the effects of chlorogenic acid and Ilex paraguariensis extracts on different markers of brain alterations in rats subjected to chronic restraint stress. Neurotox Res. (2019) 35:373–86. doi: 10.1007/s12640-018-9963-6
17. Bixby M, Spieler L, Menini T, Gugliucci A. Ilex paraguariensis extracts are potent inhibitors of nitrosative stress: a comparative study with green tea and wines using a protein nitration model and mammalian cell cytotoxicity. Life Sci. (2005) 77:345–58. doi: 10.1016/j.lfs.2004.11.030
18. Palacios N, Gao X, McCullough ML, Schwarzschild MA, Shah R, Gapstur S, et al. Caffeine and risk of Parkinson's disease in a large cohort of men and women. Mov Disord. (2012) 27:1276–82. doi: 10.1002/mds.25076
19. Moccia M, Erro R, Picillo M, Vitale C, Longo K, Amboni M, et al. Caffeine consumption and the 4-year progression of de novo Parkinson's disease. Park Relat Disord. (2016) 32:116–9. doi: 10.1016/j.parkreldis.2016.08.005
20. Hong CT, Chan L, Bai C. The effect of caffeine on the risk and progression of Parkinson's disease: a meta-analysis. Nutrients. (2020) 12:1860. doi: 10.3390/nu12061860
21. Nicoletti A, Pugliese P, Nicoletti G, Arabia G, Annesi G, Mari M, et al. Voluptuary habits and clinical subtypes of Parkinson's disease: the FRAGAMP case-control study. Mov Disord. (2010) 25:2387–94. doi: 10.1002/mds.23297
22. Ascherio A, Schwarzschild MA. The epidemiology of Parkinson's disease: risk factors and prevention. Lancet Neurol. (2016) 15:1257–72. doi: 10.1016/S1474-4422(16)30230-7
Keywords: Ilex paraguariensis, Parkinson's disease, coffee, caffeine, risk factor
Citation: Medeiros MS, Schumacher-Schuh AF, Altmann V and Rieder CRdM (2021) A Case–Control Study of the Effects of Chimarrão (Ilex paraguariensis) and Coffee on Parkinson's Disease. Front. Neurol. 12:619535. doi: 10.3389/fneur.2021.619535
Received: 20 October 2020; Accepted: 25 January 2021;
Published: 10 March 2021.
Edited by:
Emilia Mabel Gatto, Sanatorio de la Trinidad Mitre, ArgentinaReviewed by:
Irene Taravini, University of Buenos Aires, ArgentinaMelcon Carlos Mario, Fundación para la Investigación en Neuroepidemiologia (FINEP), Argentina
Copyright © 2021 Medeiros, Schumacher-Schuh, Altmann and Rieder. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Márcio Schneider Medeiros, bWFyY2lvLnMubWVkZWlyb3MmI3gwMDA0MDtnbWFpbC5jb20=