
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
STUDY PROTOCOL article
Front. Neurol. , 18 March 2021
Sec. Multiple Sclerosis and Neuroimmunology
Volume 12 - 2021 | https://doi.org/10.3389/fneur.2021.596791
 Jie Ding1†
Jie Ding1† Yu Cai1†Ye Deng1Xianguo Jiang1
Yu Cai1†Ye Deng1Xianguo Jiang1 Meichun Gao1Yan Lin1Nan Zhao1Ze Wang1
Meichun Gao1Yan Lin1Nan Zhao1Ze Wang1 Haojun Yu1Wenwen Lv2Ying Zhang1
Haojun Yu1Wenwen Lv2Ying Zhang1 Yong Hao1*
Yong Hao1* Yangtai Guan1*
Yangtai Guan1*Background: Neuromyelitis optica spectrum disorder (NMOSD) is an autoimmune demyelinating disease that recurrently relapses and leads to severe disability. The available choices for disease prevention are few or intolerable. Previous studies suggested that telitacicept may provide a promising therapeutic strategy for autoimmune diseases involving B cells. Therefore, this study aims to assess the effectiveness and safety of telitacicept for recurrent NMOSD.
Methods: We will perform a single-arm, single-center, open-label, specialist study with a total enrollment of eight participants. The treatment regimen includes plasma exchange three times and subcutaneous injection of telitacicept for 46 cycles, with a total period of 48 weeks. The primary endpoint is the time to first recurrence after enrollment. Secondary endpoints are Expanded Disability Status Scale (EDSS) score, Opticospinal Impairment Scale (OSIS) score, Hauser Ambulation Index, number of lesions on MRI, and changes in visual evoked potential (VEP), optical coherence tomography (OCT) and immunologic status. All adverse events after medication will be documented and investigated.
Discussion: This study will explore the safety and effectiveness of telitacicept following plasma exchange regarding the time to recurrence in neuromyelitis optica spectrum disorder (NMOSD) for the first time.
Clinical Trial Registration: Chictr.org.cn, identifier ChiCTR1800019427
Neuromyelitis optica spectrum disorder (NMOSD) is a primary B-cell mediated central nervous system autoimmune disease with an incidence of 0.5–10 per 100,000 people (1), less than the number of 60 per 100,000 people in areas with high incidence of Multiple Sclerosis(MS). However, as the diagnostic criteria of NMOSD was firstly revised in 2015 (2), there may be some missed diagnoses in current incidence of NMOSD. Current study also showed that NMOSD is more prevalent than MS in Asian population. In addition, NMOSD commonly occurs in young and middle-aged patients. It may relapse recurrently and lead to severe disability (3, 4). Therefore, it is of great importance to reduce the relapse rate to ameliorate severe neurological disability (4, 5).
Currently, infusions of high-dose intravenous methylprednisolone (IVMP) and plasma exchange (PLEX) (6) are commonly used in acute phase treatment. Drugs such as azathioprine, rituximab and mycophenolate mofetil are available immunotherapies used for patients with NMOSD to prevent relapse (5, 7, 8). However, recurrent relapse is still common in patients with NMOSD as lack of specific therapeutic target. In addition, some patients may not tolerate certain treatments because of their side effects, such as avascular necrosis of femoral head and hepatic impairment (5). Some new drugs are underway for NMOSD such as CD19 targeting antibody inebilizumab and IL-6 receptor antibody satralizumab (9). However, they are still inaccessible especially in China. Thus, it remains urgent to develop a new therapy targeting the pathogenesis of NMOSD with better effectiveness and safety, so as to remit rapidly and reduce recurrence.
NMOSD is a primary B-cell and antibody-mediated autoimmune disease (10). The release of autoantibodies from B cells indicates that there may be a specific step in B-cell receptor signaling that can be targeted to inhibit disease occurrence. B-lymphocyte stimulator (BLyS) and proliferation-inducing ligand (APRIL) both belong to the tumor necrosis factor (TNF) ligand superfamily. Accumulating evidence suggests the interplay between BLyS and APRIL plays a role in regulating B-cell maturation, function and survival (11–13). Overexpressed BLyS and APRIL are found in immune disorders such as rheumatoid arthritis (RA), systemic lupus erythematosus (SLE) and NMOSD (14–17). They are also correlated with disease activity and severity (18). Therefore, suppressing both BLyS and APRIL is also highly likely to be effective in treating NMOSD.
The regulatory role of BLyS and APRIL involves both B-cell maturation antigen (BCMA) receptors and transmembrane activator and calcium modulator and cyclophilin-ligand interactor (TACI) (19, 20). Telitacicept (previously known as TACI-Ig or Atacicept) is a recombinant fusion protein of both the ligand-binding domain of the TACI receptor and the Fc component of human IgG. Telitacicept is designed to inhibit the effects of B-cell BLyS and APRIL and may provide therapeutic potential for NMOSD (21, 22).
Studies have shown the safety and efficacy of telitacicept in B-cell-mediated diseases such as SLE and RA (23–25). Studies have also demonstrated that agents blocking BLyS and APRIL could improve clinical manifestations in a rodent model of experimental autoimmune encephalomyelitis (26). Nevertheless, telitacicept may increase clinical disease activity in patients with multiple sclerosis, a primary T-cell mediated central nervous system autoimmune disease. (27) It may also increase conversion to clinically definite multiple sclerosis in patients with unilateral symptomatic Optic neuritis as a clinically isolated syndrome (CIS) (28). However, the effectiveness and safety of telitacicept in aquaporin-4 antibody associated NMOSD patients has rarely been reported. Thus, the purpose of this study is to initially observe the effectiveness and safety of telitacicept following plasma exchange in NMOSD patients with recurrent onset.
Our study is a single-center, single-arm, open-label clinical study and abide by the SPIRIT reporting guidelines (29). The purpose of this study is to assess any reduction in the incidence of recurrence in patients with recurrent NMOSD by the administration of telitacicept after plasma exchange, and safety was also analyzed. All participating individuals will receive plasma exchange three times and then undergo subcutaneous injection of telitacicept for 46 cycles, with a total period of 48 weeks (Figure 1). The study is planned to enroll eight participants.
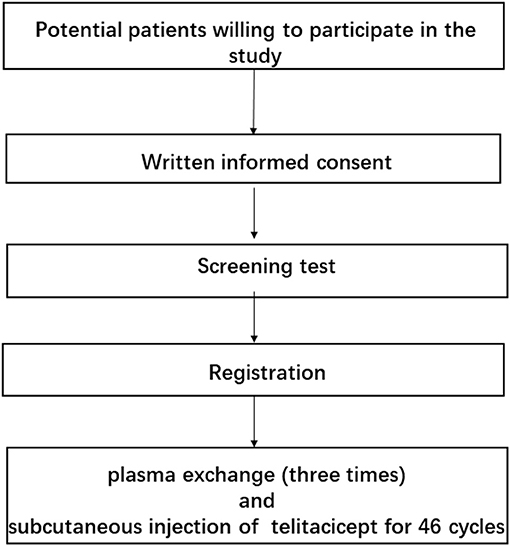
Figure 1. Summary of the study.
Considering the small and special nature of the study, the sample size will not be analyzed.
The potential participants of this study are patients with AQP4-IgG-seropositive NMOSD in the acute phase, with ≥2 recurrences occurring in the past 12 months prior to screening (including the acute phase recurrence). Written informed consent is required for all potential participants recruited prior to screening in Renji Hospital affiliated to Shanghai Jiao Tong University, School of Medicine. After rigorous screening, the patients enrolled in this study are required to meet all the inclusion criteria without satisfying any of the exclusion criteria (Box 1).
Box 1. Inclusion and exclusion criteria for patients.
Inclusion criteria
1. Meet the diagnostic criteria for NMOSD in the 2015 international consensus; AQP4-IgG-seropositive.
2. Age 18–75 years.
3. NMOSD in the acute phase; that is, new onset of neurological symptoms or aggravation of existing symptoms within 30 days before screening, lasting for at least 24 hours without accompanying fever.
4. NMOSD recurrence (including acute onset during screening): ≥2 recurrences occurring 12 months before screening.
5. Effective contraception during the study. 6. Provide written informed consent.
Exclusion criteria
1. Progressively deteriorating neurological disorders unrelated to NMOSD.
2. Active hepatitis or severe liver dysfunction (over 2 times the normal value of liver function examination); HBsAg-positive patients were excluded. Patients with only HBc-Ab positivity are needed for the HBV-DNA quantitative test and are not excluded if negative.
3. Severe renal insufficiency (including acute kidney injury and chronic kidney disease, or serum creatinine clearance <60 mL/min calculated by the Cockcroft-Gault equation).
4. Current pregnancy, breastfeeding or plans to become pregnant in the past 48 weeks.
5. Participation in any clinical trial drug within 28 days before enrollment or 5 times the half-life period of the experimental drug (for a shorter time).
6. History of splenectomy.
7. Allergic reaction: history of allergies to contrast agents or human-derived biological products for parenteral administration.
8. Severe psychiatric symptoms and the inability to cooperate.
9. Unable to undergo magnetic resonance imaging.
10. Medication history of rituximab or mitoxantrone 3 months prior to enrollment.
11. Considered unsuitable by the investigators.
Participants providing written informed consent will undergo screening tests, and the investigators will review the criteria of patient inclusion and exclusion. If participating individuals meet all the inclusion criteria without satisfying any of the exclusion criteria, they will be documented as registered in our study. After written informed consent is obtained, the study will consist of a screening period with a maximum of 2 weeks and a period of treatment for 48 weeks. The patients will be treated with plasma exchange during the first 2 weeks of the treatment period. Afterward, telitacicept will be given weekly for 46 weeks (Table 1). After registration, the participants will not receive any treatment with glucocorticoids or immunosuppressive agents until the recurrence of NMOSD.
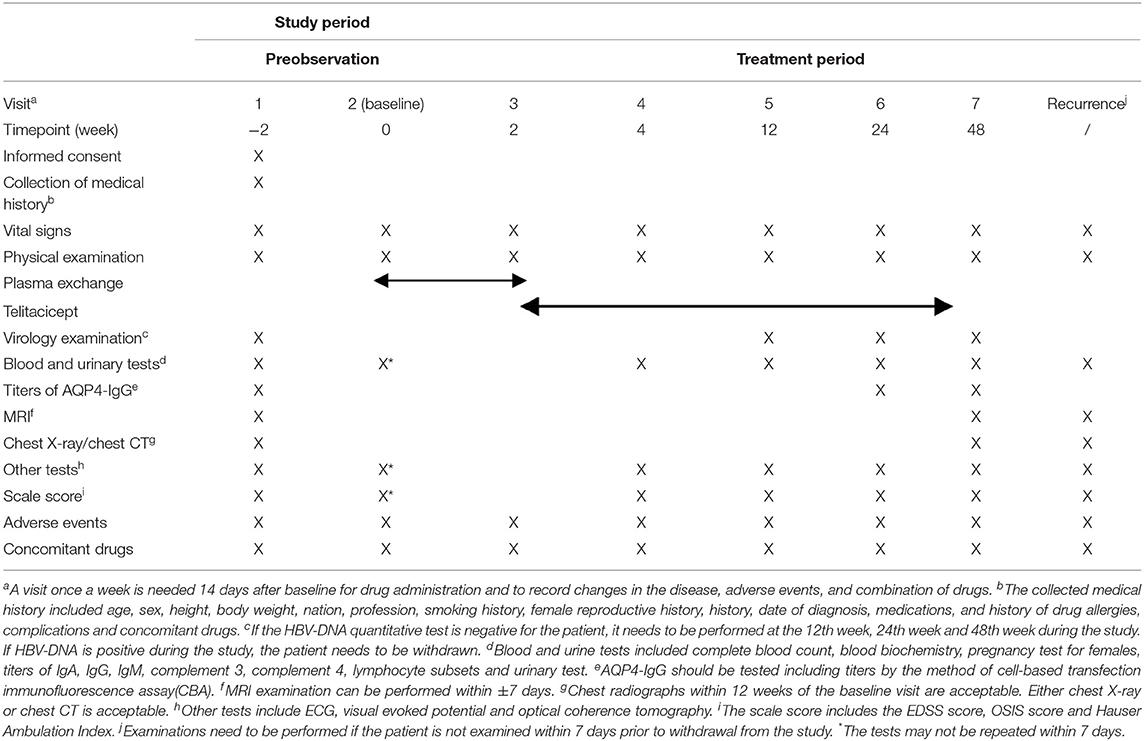
Table 1. Schedule of enrollment, interventions and assessments.
When participants are enrolled, they will be given plasma exchange three times, lasting no more than 14 days. Afterward, they will receive telitacicept treatment weekly for 46 weeks. The time lapse from onset of symptoms to first administration of telitacicept is within 17 to 58 days. The interval is at least 48 hours. A dose of 240 mg will be subcutaneously injected once. The injection site can be the thigh, abdomen or upper arm. At least one clinician needs to observe the patients for 30 min, mainly observing the patient's consciousness and vital signs.
Telitacicept is a freeze-dried powder injection. The specification is 80 mg for one piece. It needs to be stored and transported at 2°C~8°C. After rehydration, the drug should not be left at room temperature for more than 30 min. Every 80 mg of drug will be dissolved in 1 mL of injection water into an isotonic solution.
The patients will be withdrawn from the study if relapse occurs. Except for special situations, the dosage, method of administration and time interval are not allowed to be changed during the study. However, during or after the 12-week visit, the investigator will evaluate the safety of the therapy in the patient. If the investigator considers that the dose needs to be reduced to ensure safety, then the dose can be adjusted. Supposing that a dose started at 240 mg, it can be adjusted to 160 mg for the first time and adjusted again to 80 mg. The minimum dose is 80 mg.
The drug should be suspended if any of the following conditions appear: (1) cell count of leukocytes <2.0 × 109/L; (2) cell count of neutrophils <1.0 × 109/L; (3) cell count of lymphocytes <0.5 × 109/L; (4) count of platelets <75 × 109/L; (5) aspartate aminotransferase (AST) or alanine aminotransferase (ALT) > 3×upper limit of normal (ULN); or (6) hemoglobin <80 g/L. With the approval of the investigator, drug use can be continued if participants meet the following criteria: (1) cell count of leukocytes ≥2.5 × 109/L; (2) cell count of neutrophils >2.0 × 109/L or the count at baseline; (3) cell count of lymphocytes ≥ 0.75 × 109/L; (4) count of platelets ≥100 × 109/L or the count at baseline; (5) AST or ALT < 2×ULN; and (6) hemoglobin ≥100 g/L or the count at baseline. If the conditions listed above occur again after restarting the drug administration, the patient should permanently discontinue the drug. In addition, if any of the following conditions occur during the study, the patient should also withdraw from the study: (1) AST or ALT > 8×ULN; (2) AST or ALT > 5×ULN and the duration of drug suspension exceeds 2 weeks; (3) AST or ALT > 3×ULN and serum total bilirubin concentration>2×ULN; (4) AST or ALT >3×ULN along with fever, rash, nausea, vomiting, fatigue, right upper abdomen pain, or eosinophilia; (5) cell count of leukocytes <1.0×109/L; (6) cell count of neutrophils <0.5×109/L; (7) cell count of lymphocytes <0.2×109/L; or (8) hemoglobin <65 g/L.
At each visit and drug administration, compliance instructions will be provided and confirmed by the investigators.
Concomitant drugs or therapies will not be applied during either the screening or treatment period. The oral or intravenous administration of glucocorticoids is not allowed; however, intranasal, intraocular, topical or inhaled glucocorticoids will be allowed. Immunosuppressants are also not allowed, such as tripterygium glycosides, cyclosporine, methotrexate, mitoxantrone, cyclophosphamide, azathioprine, tacrolimus, leflunomide, mycophenolate mofetil and teriflunomide. The following concomitant drugs and therapies are prohibited: biological immunosuppressive agents such as rituximab, hematopoietic stem cell transplantation, lymphatic irradiation and immunoglobulin injection.
Mecobalamin and vitamin B1 are allowed to be used during the study. In the case of other diseases during the study, drugs that do not affect the efficacy of the telitacicept (such as antibiotics) can be used. However, the reasons for the use of drugs and method of application should be recorded in detail.
The primary outcome is time to first recurrence after enrollment. The definition of recurrence needs to meet the following criteria: (1) new nervous system abnormalities or worsening of existing symptoms; (2) symptoms lasting for at least 24 h; (3) over 30 days after the last relapse; and (4) no associated fever, temperature <37.5°C, or without known infection.
Secondary outcomes are listed below:
1. EDSS score
2. OSIS score
3. Hauser Ambulation Index
4. Number of lesions in MRI
5. Changes in visual evoked potential (VEP)
6. Changes in optical coherence tomography (OCT)
7. Changes in immunologic status
8. All adverse events after medication.
The EDSS score, OSIS score, Hauser Ambulation Index are evaluated by two professional physicians. Number of lesions in MRI include number of high signal lesions on T2 weighted imaging (T2WI), low signal lesions on T1 weighted imaging (T1WI) and lesions on gadolinium-enhanced T1WI, which are obtained in MRI of the optic nerve, brain and spinal cord. MRI scans are analyzed independently by radiologists at the Department of Radiology at Renji Hospital affiliated with Shanghai Jiaotong University School of Medicine. The latency and amplitude of evoked potential P100 were recorded by VEP. Optical coherence tomography (OCT) is used to measure the thickness of the retinal nerve fiber layer (RNFL), which is obtained with the “Fast RNFL Thickness” protocol. The titers of anti-AQP4 antibody are tested by the method of cell-based transfection immunofluorescence assay (CBA). Other immune tests are titers of IgA, IgG, IgM, complement 3, complement 4 in serum and lymphocyte subsets in the peripheral blood.
Adverse events will be graded using the Common Terminology Criteria for Adverse Events (CTCAE V.4.0). Common adverse events are local reactions at the injection site, including mild to moderate erythema and itchy skin rashes. Other potential adverse events include upper respiratory tract infection, bruises and itching at the injection site, soreness and redness at the injection site, urinary tract infection, herpes zoster, mumps, periodontitis, abnormality of liver function, hypothyroidism, fatigue, headache, sore throat, nasopharyngitis, diarrhea, nausea, vomiting, flu-like symptoms, cough, oral ulcer, nasal congestion, palpebral edema, right upper abdominal pain, joint pain, back pain, and perianal abscess.
Patients who are enrolled in this study and receive the test drugs at least once, with at least one post-medication evaluation, will be included in the full analysis set (FAS). The per protocol set (PPS) is described as participating individuals in the FAS who comply with the protocol, including the therapeutic regimen and the availability of the primary outcome with no major violation of the protocol. The primary outcome will be analyzed in the PPS. Participants who are administered the test drugs at least once and have recorded security evaluations will be included in the safety set (SS). Safety will be analyzed in the SS.
The quartile of time to recurrence, 95% CI and censoring rate will be calculated.
The secondary outcomes will be analyzed in the form of simple descriptive statistics, such as the mean and associated 95% CIs, SDs, median, minimum, and maximum. Paired t test will be used for statistical analyses of the difference in means before and after administration.
All adverse events will be analyzed in the SS. The Medical Dictionary for Regulatory Activities (MedDRA) will be used to code the preferred terms (PT) for adverse events and system organ class (SOC). All adverse events will be listed in detail, and the incidence of different adverse events will be calculated. All statistical analyses will be performed using JMP software (SAS V.9.3), with significance set at a two-tailed p-value.
All data for every participant will be recorded by investigators in case report forms (CRFs). CRFs will be made according to the plan at screening, at baseline, at 4 weeks, 12 weeks, and 24 weeks after baseline, at the end of treatment and if relapse occurs. The researcher will review and sign the CRF when complete. The investigator needs to re-sign the form if the data are modified.
Materials such as the research records, informed consent forms and data of all patients will be reviewed every 6 months to ensure the accuracy and integrity of the data.
Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
All information collected in our study will be stored securely in locked file cabinets at the study site. All information of every participating individual will be identified by a coded number without names or other personal identifiers to maintain participant confidentiality. A password will be applied to protect the database.
Our study will be performed according to the principles of the Declaration of Helsinki and has been approved by the ethics committee of Renji Hospital affiliated with Shanghai Jiaotong University School of Medicine. Investigators will explain the study by information sheets. Patients who are willing to participate will have enough time to ask questions. All questions will be explained in detail before obtaining written informed consent. All participants will be provided consent forms. Compensation will be given to those who suffer harm from trial participation.
The results of this study will be reported in academic conferences and peer-reviewed journals. The paper will be reviewed and approved by all authors before publication.
Recently, an increasing number of studies have focused on treatments involving biological agents in patients with NMOSD (8). Few studies have been conducted on the treatment of telitacicept in patients with NMOSD. Compared with available immunosuppressive drugs such as azathioprine and mycophenolate mofetil, telitacicept shows advantages in targeting a very specific molecule. Therefore, some off-target adverse effects may be avoided, and the treatment may be more accurate.
The results of this study may be useful for considering the safety of new biological agents in patients with NMOSD. Studies in healthy volunteers have demonstrated the safety and tolerability of telitacicept in a healthy population (30, 31). Randomized trials have also shown the safety and tolerability of telitacicept in autoimmune diseases such as SLE and RA (24, 32–34).
The study will also provide preliminary data on the efficacy of telitacicept in patients with NMOSD. Since NMOSD is a primary B cell- and antibody-mediated autoimmune disease, AQP4-IgG plays an important role in the disease (35). In our study, patients in the acute phase with AQP4-IgG seropositivity will be included. When disease occurs, plasma exchange will be first applied to filter out AQP4-IgG. Afterward, telitacicept treatment will be used to inhibit the activity of BLyS and APRIL, which may interfere with B cell function and autoantibody production. The combination of plasma exchange and telitacicept may provide better effects.
In addition, we will provide a detailed description to demonstrate the efficacy of telitacicept, including the EDSS score, OSIS score, Hauser Ambulation Index, number of lesions in MRI, and changes in OCT, VEP and immunologic status. We expect that the review of this protocol may be useful for other researchers to promote future related clinical trials.
Nevertheless, the sampling strategy is a limitation and potential source of bias in this study. We will only be able to preliminarily demonstrate the probable safety and efficacy of telitacicept, as this study is a single-center, single-arm, open-label study. Large-sample, prospective, multicenter, randomized controlled studies need to be performed in the future. In addition, the assessment of safety and tolerability will only be based on a 1-year follow-up visit. A longer follow-up period may be needed.
In this study, we expect that telitacicept may be safe and effective in patients with recurrent NMOSD; however, large sample, prospective, multicenter, randomized controlled studies are needed for further validation. Overall, as there are few studies on telitacicept treatment in patients with NMOSD, this study will be useful in presenting preliminary data for future study designs.
▸ This study will explore the safety and effectiveness of telitacicept following plasma exchange regarding the time to recurrence in neuromyelitis optica spectrum disorder (NMOSD) for the first time.
▸ This study is well-designed for the selection of NMOSD patients with a high recurrence risk.
▸ A major limitation of this study is the small sample size, which weakens the power of evidence for the effectiveness of telitacicept. As the current low incidence of NMOSD, a small and special study is firstly conducted.
▸ Because eligible NMOSD patients are relatively rare, especially those with a recurrent acute phase within 30 days and a second recurrence within 12 months, this study does not include a control group, which may produce bias.
The studies involving human participants were reviewed and approved by the ethics committee of Renji Hospital affiliated with Shanghai Jiaotong University School of Medicine (No 2018-088). The patients/participants provided their written informed consent to participate in this study.
JD wrote the initial draft of the paper. Y-TG, YH, and YC revised the paper. Y-TG, YC, and YZ designed the study. Y-TG, YC, YD, YZ, W-WL, and YL reviewed all versions of the protocol and contributed to the start of the study. Y-TG, YH, X-GJ, and JD analyzed and interpreted data. YH, X-GJ, JD, NZ, ZW, and H-JY collected the clinical data. M-CG contributed to the drug storage and electronic CRF. All authors have read and approved the final manuscript and agreed to be responsible for all aspects of the research to ensure that issues related to the accuracy or completeness of the study are properly studied and addressed.
This study was supported by grants from the National Natural Science Foundation of China (Grant No. 81771295), Innovative research team of high-level local universities in Shanghai, and Yantai Rongchang Pharmaceutical Co., Ltd. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We would like to thank Bingshun Wang and the Clinical Research Center of Medical School of Shanghai Jiaotong University for their support in establishing this research study.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2021.596791/full#supplementary-material
1. Hor JY, Asgari N, Nakashima I, Broadley SA, Leite MI, Kissani N, et al. Epidemiology of Neuromyelitis Optica Spectrum Disorder and Its Prevalence and Incidence Worldwide. Front Neurol. (2020) 11:501. doi: 10.3389/fneur.2020.00501
2. Wingerchuk DM, Banwell B, Bennett JL, Cabre P, Carroll W, Chitnis T, et al. International consensus diagnostic criteria for neuromyelitis optica spectrum disorders. Neurology. (2015) 85:177–89. doi: 10.1212/WNL.0000000000001729
3. Papadopoulos MC, Bennett JL, Verkman AS. Treatment of neuromyelitis optica: state-of-the-art and emerging therapies. Nat Rev Neurol. (2014) 10:493–506. doi: 10.1038/nrneurol.2014.141
4. Trebst C, Jarius S, Berthele A, Paul F, Schippling S, Wildemann B, et al. Update on the diagnosis and treatment of neuromyelitis optica: recommendations of the Neuromyelitis Optica Study Group (NEMOS). J Neurol. (2014) 261:1–16. doi: 10.1007/s00415-013-7169-7
5. Espiritu AI, Pasco PMD. Efficacy and tolerability of azathioprine for neuromyelitis optica spectrum disorder: a systematic review and meta-analysis. Mult Scler Relat Disord. (2019) 33:22–32. doi: 10.1016/j.msard.2019.05.011
6. Bonnan M, Valentino R, Debeugny S, Merle H, Ferge JL, Mehdaoui H, et al. Short delay to initiate plasma exchange is the strongest predictor of outcome in severe attacks of NMO spectrum disorders. J Neurol Neurosurg Psychiatry. (2018) 89:346–51. doi: 10.1136/jnnp-2017-316286
7. Poupart J, Giovannelli J, Deschamps R, Audoin B, Ciron J, Maillart E, et al. Evaluation of efficacy and tolerability of first-line therapies in NMOSD. Neurology. (2020) 94:e1645–e56. doi: 10.1212/WNL.0000000000009245
8. Zhang C, Zhang M, Qiu W, Ma H, Zhang X, Zhu Z, et al. Safety and efficacy of tocilizumab versus azathioprine in highly relapsing neuromyelitis optica spectrum disorder (TANGO): an open-label, multicentre, randomised, phase 2 trial. Lancet Neurol. (2020) 19:391–401. doi: 10.1016/S1474-4422(20)30070-3
9. Duchow A, Chien C, Paul F, Bellmann-Strobl J. Emerging drugs for the treatment of neuromyelitis optica. Expert Opin Emerg Drugs. (2020) 25:285–97. doi: 10.1080/14728214.2020.1803828
10. Melamed E, Levy M, Waters PJ, Sato DK, Bennett JL, John GR, et al. Update on biomarkers in neuromyelitis optica. Neurology(R) neuroimmunology & Neuroinflammation. (2015) 2:e134. doi: 10.1212/NXI.0000000000000134
11. Dillon SR, Gross JA, Ansell SM, Novak AJ. An APRIL to remember: novel TNF ligands as therapeutic targets. Nat Rev Drug Discov. (2006) 5:235–46. doi: 10.1038/nrd1982
12. Moore PA, Belvedere O, Orr A, Pieri K, LaFleur DW, Feng P, et al. BLyS: member of the tumor necrosis factor family and B lymphocyte stimulator. Science. (1999) 285:260–3. doi: 10.1126/science.285.5425.260
13. Schneider P, MacKay F, Steiner V, Hofmann K, Bodmer JL, Holler N, et al. BAFF, a novel ligand of the tumor necrosis factor family, stimulates B cell growth. The J Exp Med. (1999)189:1747–56. doi: 10.1084/jem.189.11.1747
14. Salazar-Camarena DC, Ortiz-Lazareno PC, Cruz A, Oregon-Romero E, Machado-Contreras JR, Munoz-Valle JF, et al. Association of BAFF, APRIL serum levels, BAFF-R, TACI and BCMA expression on peripheral B-cell subsets with clinical manifestations in systemic lupus erythematosus. Lupus. (2016) 25:582–92. doi: 10.1177/0961203315608254
15. Hegazy M, Darwish H, Darweesh H, El-Shehaby A, Emad Y. Raised serum level of APRIL in patients with systemic lupus erythematosus: correlations with disease activity indices. Clin Immunol. (2010) 135:118–24. doi: 10.1016/j.clim.2009.12.012
16. Shabgah AG, Shariati-Sarabi Z, Tavakkol-Afshari J, Mohammadi M. The role of BAFF and APRIL in rheumatoid arthritis. J Cell Physiol. (2019) 234:17050–63. doi: 10.1002/jcp.28445
17. Wang H, Wang K, Zhong X, Qiu W, Dai Y, Wu A, et al. Cerebrospinal Fluid BAFF and APRIL levels in neuromyelitis optica and multiple sclerosis patients during relapse. J Clin Immunol. (2012) 32:1007–11. doi: 10.1007/s10875-012-9709-9
18. McCarthy EM, Lee RZ, Ni Gabhann J, Smith S, Cunnane G, Doran MF, et al. Elevated B lymphocyte stimulator levels are associated with increased damage in an Irish systemic lupus erythematosus cohort. Rheumatology. (2013) 52:1279–84. doi: 10.1093/rheumatology/ket120
19. Marsters SA, Yan M, Pitti RM, Haas PE, Dixit VM, Ashkenazi A. Interaction of the TNF homologues BLyS and APRIL with the TNF receptor homologues BCMA and TACI. Curr Biol. (2000) 10:785–8. doi: 10.1016/s0960-9822(00)00566-2
20. Bossen C, Schneider P. BAFF, APRIL and their receptors: structure, function and signaling. Semin Immunol. (2006) 18:263–75.doi: 10.1016/j.smim.2006.04.006
21. Gross JA, Johnston J, Mudri S, Enselman R, Dillon SR, Madden K, et al. TACI and BCMA are receptors for a TNF homologue implicated in B-cell autoimmune disease. Nature. (2000) 404:995–9. doi: 10.1038/35010115
22. Kaegi C, Steiner UC, Wuest B, Crowley C, Boyman O. Systematic review of safety and efficacy of atacicept in treating immune-mediated disorders. Front Immunol. (2020) 11:433. doi: 10.3389/fimmu.2020.00433
23. Merrill JT, Wallace DJ, Wax S, Kao A, Fraser PA, Chang P, et al. Efficacy and safety of atacicept in patients with systemic lupus erythematosus: results of a twenty-four-week, multicenter, randomized, double-blind, placebo-controlled, parallel-arm, phase iib study. Arthritis Rheumatol. (2018) 70:266–76. doi: 10.1002/art.40360
24. Pena-Rossi C, Nasonov E, Stanislav M, Yakusevich V, Ershova O, Lomareva N, et al. An exploratory dose-escalating study investigating the safety, tolerability, pharmacokinetics and pharmacodynamics of intravenous atacicept in patients with systemic lupus erythematosus. Lupus. (2009) 18:547–55. doi: 10.1177/0961203309102803
25. van Vollenhoven RF, Kinnman N, Vincent E, Wax S, Bathon J. Atacicept in patients with rheumatoid arthritis and an inadequate response to methotrexate: results of a phase II, randomized, placebo-controlled trial. Arthritis Rheum. (2011) 63:1782–92. doi: 10.1002/art.30372
26. Huntington ND, Tomioka R, Clavarino C, Chow AM, Linares D, Mana P, et al. A BAFF antagonist suppresses experimental autoimmune encephalomyelitis by targeting cell-mediated and humoral immune responses. Int Immunol. (2006) 18:1473–85. doi: 10.1093/intimm/dxl080
27. Kappos L, Hartung H-P, Freedman MS, Boyko A, Radü EW, Mikol DD, et al. Atacicept in multiple sclerosis (ATAMS): a randomised, placebo-controlled, double-blind, phase 2 trial. Lancet Neurol. (2014) 13:353–63. doi: 10.1016/s1474-4422(14)70028-6
28. Sergott RC, Bennett JL, Rieckmann P, Montalban X, Mikol D, Freudensprung U, et al. ATON: results from a Phase II randomized trial of the B-cell-targeting agent atacicept in patients with optic neuritis. J Neurol Sci. (2015) 351:174–8. doi: 10.1016/j.jns.2015.02.019
29. Chan AW, Tetzlaff JM, Altman DG, Laupacis A, Gotzsche PC, Krleza-Jeric K, et al. SPIRIT 2013 statement: defining standard protocol items for clinical trials. Ann Intern Med. (2013) 158:200–7. doi: 10.7326/0003-4819-158-3-201302050-00583
30. Munafo A, Priestley A, Nestorov I, Visich J, Rogge M. Safety, pharmacokinetics and pharmacodynamics of atacicept in healthy volunteers. Eur J Clin Pharmacol. (2007) 63:647–56. doi: 10.1007/s00228-007-0311-7
31. Willen D, Uhl W, Wolna P, Papasouliotis O, Yalkinoglu O. Safety, tolerability, pharmacokinetics, and pharmacodynamics of atacicept in a randomized trial in healthy caucasian and Japanese subjects. Eur J Drug Metab Pharmacokinet. (2020) 45:27–40. doi: 10.1007/s13318-019-00575-7
32. Gordon C, Bassi R, Chang P, Kao A, Jayne D, Wofsy D, et al. Integrated safety profile of atacicept: an analysis of pooled data from the atacicept clinical trial programme. Rheumatol Adv Pract. (2019) 3:rkz021. doi: 10.1093/rap/rkz021
33. Tak PP, Thurlings RM, Rossier C, Nestorov I, Dimic A, Mircetic V, et al. Atacicept in patients with rheumatoid arthritis: results of a multicenter, phase Ib, double-blind, placebo-controlled, dose-escalating, single- and repeated-dose study. Arthritis Rheum. (2008) 58:61–72. doi: 10.1002/art.23178
34. Dall'Era M, Chakravarty E, Wallace D, Genovese M, Weisman M, Kavanaugh A, et al. Reduced B lymphocyte and immunoglobulin levels after atacicept treatment in patients with systemic lupus erythematosus: results of a multicenter, phase Ib, double-blind, placebo-controlled, dose-escalating trial. Arthritis Rheum. (2007) 56:4142–50. doi: 10.1002/art.23047
Keywords: neuromyelitis optica spectrum disorders, telitacicept, plasma exchange, clinical study, safety, effectiveness, study protocol
Citation: Ding J, Cai Y, Deng Y, Jiang X-G, Gao M-C, Lin Y, Zhao N, Wang Z, Yu H-J, Lv W-W, Zhang Y, Hao Y and Guan Y-T (2021) Telitacicept Following Plasma Exchange in the Treatment of Subjects With Recurrent NMOSD: Study Protocol for a Single-Center, Single-Arm, Open-Label Study. Front. Neurol. 12:596791. doi: 10.3389/fneur.2021.596791
Received: 20 August 2020; Accepted: 19 February 2021;
Published: 18 March 2021.
Edited by:
Scott S. Zamvil, University of California, San Francisco, United StatesReviewed by:
Eleonora Allocati, Istituto di Ricerche Farmacologiche Mario Negri (IRCCS), ItalyCopyright © 2021 Ding, Cai, Deng, Jiang, Gao, Lin, Zhao, Wang, Yu, Lv, Zhang, Hao and Guan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yong Hao, eWhhbzIzQDEyNi5jb20=; Yangtai Guan, eWFuZ3RhaWd1YW5Ac2luYS5jb20=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.