
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Neurol., 25 January 2021
Sec. Movement Disorders
Volume 11 - 2020 | https://doi.org/10.3389/fneur.2020.603582
This article is part of the Research TopicMeasurement Tools for Clinical Assessment, Characterization and Neurorehabilitation of Parkinson's DiseaseView all 21 articles
 Teresa Maycas-Cepeda1,2*
Teresa Maycas-Cepeda1,2* Pedro López-Ruiz1,2Cici Feliz-Feliz3Lidia Gómez-Vicente1,2Rocío García-Cobos1,2
Pedro López-Ruiz1,2Cici Feliz-Feliz3Lidia Gómez-Vicente1,2Rocío García-Cobos1,2 Rafael Arroyo1,2
Rafael Arroyo1,2 Pedro J. García-Ruiz3,4
Pedro J. García-Ruiz3,4Introduction: Amimia is one of the most typical features of Parkinson's disease (PD). However, its significance and correlation with motor and nonmotor symptoms is unknown. The aim of this study is to evaluate the association between amimia and motor and nonmotor symptoms, including cognitive status, depression, and quality of life in PD patients. We also tested the blink rate as a potential tool for objectively measuring upper facial bradykinesia.
Methods: We prospectively studied amimia in PD patients. Clinical evaluation was performed using the Unified Parkinson's Disease Rating Scale (UPDRS) and timed tests. Cognitive status, depression, and quality of life were assessed using the Parkinson's Disease Cognitive Rating Scale (PD-CRS), the 16-Item Quick Inventory of Depressive Symptomatology (QIDS-SR16), and the PDQ-39, respectively. Amimia was clinically evaluated according to item 19 of UPDRS III. Finally, we studied upper facial amimia by measuring resting blink frequency and blink rate during spontaneous conversation.
Results: We included 75 patients. Amimia (item 19 UPDRS III) correlated with motor and total UPDRS (r: 0.529 and 0.551 Spearman), and its rigidity, distal bradykinesia, and motor axial subscores (r: 0.472; r: 0.252, and r: 0.508, respectively); Hoehn and Yahr scale (r: 0.392), timed tests, gait freezing, cognitive status (r: 0.29), and quality of life (r: 0.268) correlated with amimia. Blinking frequency correlated with amimia (measured with item 19 UPDRS), motor and total UPDRS.
Conclusion: Amimia correlates with motor (especially axial symptoms) and cognitive situations in PD. Amimia could be a useful global marker of overall disease severity, including cognitive decline.
Hypomimia, amimia, facial bradykinesia, or reduced facial expression (amimia for short) is present in several conditions, including dementia and depression (1–4). Amimia is one of the most classical features of Parkinson's disease (PD) (1, 2, 4–8). It has been well recognized since classic texts (9, 10). In 1860, Charcot described the characteristics of “masked face” in PD (11), and some years later, Wilson gave a vivid description of the parkinsonian facial expression: “The parkinsonian face is a mask,” “the patient has a reptilian stare,” and “little or no play of expression animates his/her countenance.” Wilson used the term amimia to include this typical facial signature of PD (10).
Cattaneo et al. summarized some interesting aspects of human facial expression (12). Facial movements differ from limb movements in critical characteristics, including the lack of joints, visual feedback, the conventional proprioceptive feedback system (13), and the absence of the characteristic triphasic EMG pattern seen in limb movements (14, 15). In addition, there is a dissociation between voluntary and emotional facial movements, critically influenced by the amygdala and the limbic system (12).
More recently, Bologna and Marsili summarized the main characteristics and distinctive physiological features of facial bradykinesia in PD (7, 8). Amimia is a peculiar parkinsonian sign: in contrast to limb bradykinesia, amimia is rarely asymmetric (16–18), and it may be present in very early stages of the disease, being evident often years before the clinical diagnosis of PD (19, 20).
Nevertheless, despite being a well-known clinical sign of PD, the relationship between amimia and other motor and nonmotor symptoms of PD is largely unknown.
The main objective of this study is to evaluate the association between amimia and motor and nonmotor symptoms, including cognitive status, depression, and quality of life in PD patients. We also study whether amimia correlates with motor complications, such as freezing of gait and dyskinesias. In addition, we tested the blink rate as a potential tool for objectively measuring upper facial bradykinesia.
Patients were recruited between December 2016 and June 2018 from the outpatient Movement Disorders Units of Hospital Universitario Quironsalud Madrid and Hospital Fundación Jiménez Díaz (Madrid).
The diagnosis of PD was made according to the UK Brain Bank criteria definition (21). Patients with features consistent with atypical parkinsonism were excluded from the study (such as early and severe loss of postural reflexes, supranuclear gaze abnormalities, dementia during the first 2 years, or significant autonomic symptoms). Patients were also excluded if they suffered from any clinical condition that could potentially affect gait, mobility, or facial movements (including facial paralysis or hemifacial spasm, among others). The clinical evaluation of amimia was based on item 19 of UPDRS III. We also studied upper facial bradykinesia by measuring blinking frequency (the blinking rate was defined as the number of blinks per minute) both resting and during spontaneous conversation. Facial evaluations were recorded on video in order to calculate the blinking rate.
The PD clinical assessment was performed using the Schwab and England Activities of Daily Living Scale, the Hoehn and Yahr Scale, the Unified Parkinson's Disease Rating Scale (UPDRS) (22), and the four timed tests of the CAPIT protocol (23, 24) [including pronation–supination (PS), finger dexterity (FD), movement between 2 points (MTP), and the walking test (WT)]. Tremor score was calculated as the sum of items 20 (tremor at rest) and 21 (action or postural tremor) of UPDRS III; rigidity score was the sum of item 22 of UPDRS III (rigidity of neck and upper and lower extremities); distal bradykinesia score was the sum of items 23 (finger tapping), 24 (hand movements), 25 (rapid alternating movements), and 26 (leg agility); and axial motor score was calculated as the sum of items 18 (speech), 27 (arising from chair), 28 (posture), 29 (gait), and 30 (postural stability) of UPDRS III (25).
Patients were classified according to their main symptom into akinetic-rigid PD, tremor-dominant PD, or mixed PD.
Cognitive and psychiatric aspects of PD were assessed using the Disease-Cognitive Rating Scale (PD-CRS), the 16-Item Quick Inventory of Depressive Symptomatology (QIDS-SR16), and the Parkinson's Disease Questionnaire (PDQ-39).
All patients were evaluated in the mid-morning, after taking their regular medication, in a stable ON condition in order to assess the clinical condition of our patients as similarly as possible to everyday clinical practice.
The present study was performed in accordance with the ethical standards of the WMA Declaration of Helsinki and was approved by the Local Ethics Committee. Written informed consent was obtained from all participants.
Qualitative variables were expressed as absolute (n) and relative (%) frequencies. The Shapiro-Wilk test was used to evaluate the normality of the quantitative variables. Mean values ± standard deviation (SD) are given for normal distributions; for non-normal distributions, the data are reported as medians with interquartile range (IQR).
The correlation between amimia (item 19 UPDRS III) and the continuous variables was performed using the Spearman correlation. For quantitative variables, Student's t or Mann-Whitney U tests (depending on the normality distribution) were applied to analyze differences between dementia and nondementia group values; chi-square or Fisher's exact test were used for qualitative variables. Finally, univariable linear regression analyses were performed between amimia and age, disease duration, UPDRS and its subscores, rigidity, distal bradykinesia, motor axial, freezing, PD-CRS, PDQ39, and blink rate. Multivariable analyses were performed with the variables that resulted in significant association.
Data analysis was performed with the IBM-SPSS statistical software program, version 21.0 (IBM Inc., Chicago, IL, USA). The significance level was set as p < 0.05.
We included 75 PD patients. Demographic and descriptive results are shown in Table 1.
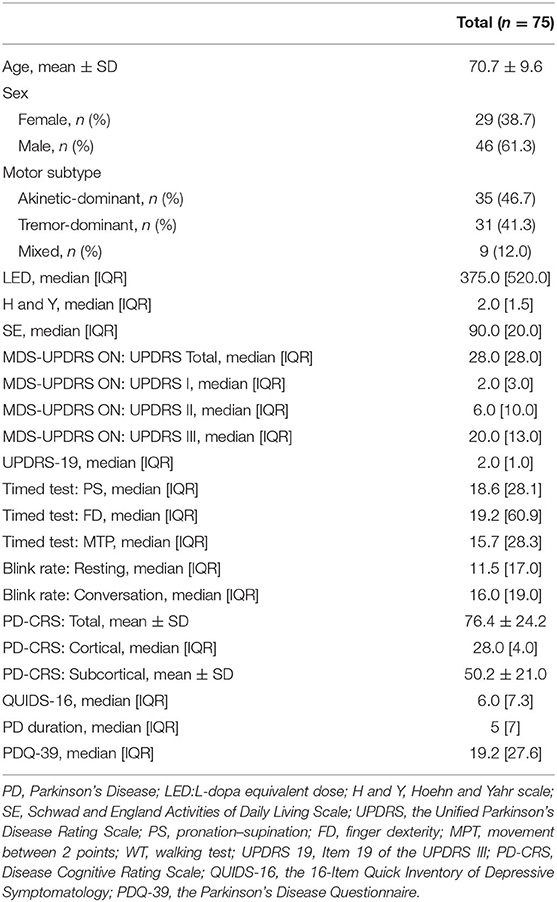
Table 1. Demographic and descriptive results.
1) Amimia (measured by item 19 UPDRS III) correlated with clinical scales including total (p < 0.01, r: 0.551) and motor UPDRS (p < 0.01, r: 0.529) (Figures 1A,B). Amimia correlated with rigidity score (p < 0.001, r: 0.472), distal bradykinesia score (p: 0.029, r: 0.252), and axial motor score (p < 0.001, r: 0.508). In contrast, amimia did not correlate with tremor score.
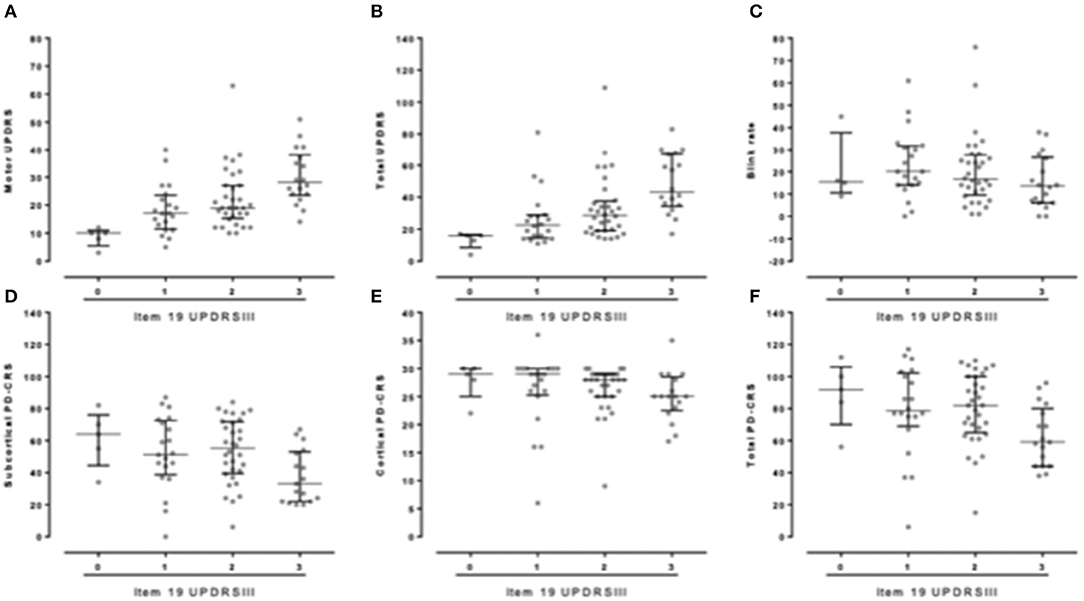
Figure 1. (A,B) Correlation between facial bradykinesia (item 19UPDRS III) and UPDRS (A. motor-UPDRS; B. Total UPDRS). (C) Correlation between facial bradykinesia (item 19UPDRS III) and blink rate at rest. (D–F) Correlation between facial bradykinesia (item 19UDPRS III) and cognitive test. (D) PD-CRS subcortical score; (E) PD-CRS cortical score; (F) Total PD-CRS.
2) Amimia scores also correlated with bradykinesia measured by timed tests: PS (p < 0.05, r: 0.257), FD (p < 0.01, r: 0.395), and MTP (p < 0.01, r: 0.437) (Table 2).
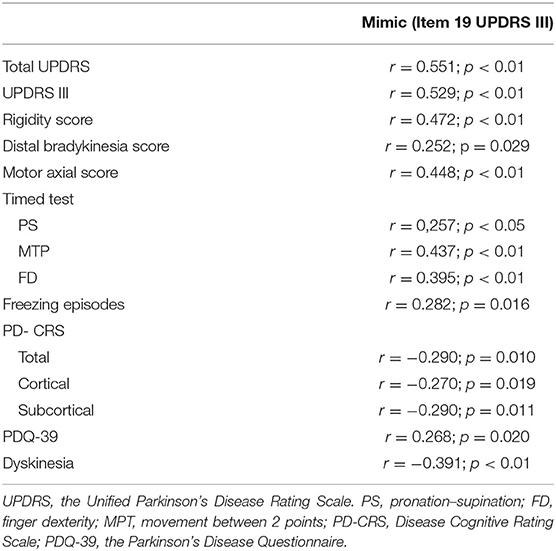
Table 2. Main correlation results using Spearman test.
3) Concerning nonmotor symptoms, amimia correlated with cognitive performance, including PD-CRS total, cortical, and subcortical (p = 0.010, r:−0.29; p = 0.019, r:−0.27; and p = 0.011, r:−0.29) (Figures 1D–F). Cognitive decline (defined as PD-CRS ≤ 64) (26) also correlated with amimia (p < 0.05; r = −0.282). The distribution score for amimia was clearly different between those patients with dementia compared with those without dementia (p < 0.05) (Table 3). In contrast, no correlation was found between amimia and depression scores.
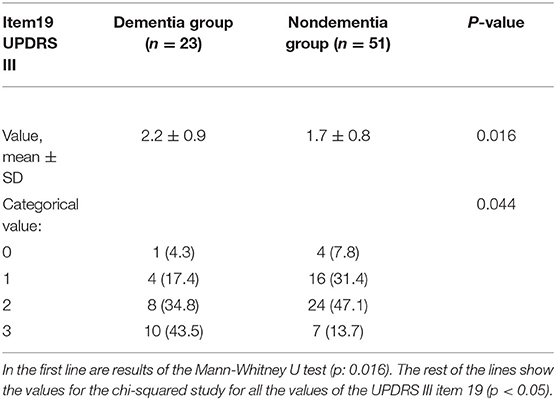
Table 3. Comparison between patients with and without dementia.
4) Regarding motor complications, amimia correlated with the frequency of gait freezing episodes (p < 0.05, r: 0.282) and with the presence of dyskinesias (p < 0.01, r:−0.391) (Table 2).
5) We also found correlation between amimia and PDQ-39 scores (p < 0.05, r: 0.268) and disease duration (p < 0.01, r: 0.378) (Table 2).
6) Upper facial bradykinesia measured by resting blink frequency correlated with total UPDRS (p < 0.01, r:−0.30), motor UPDRS (p < 0.05, r:−0.246), and cortical PD-CRS (p < 0.05; r:−0.262) but not with the rest of the studied variables. Amimia measured by item 19 UPDRS III correlated with resting blink rate (p < 0.01; r:−0.36) (Figure 1C), but not with blink frequency while participating in spontaneous conversation (p > 0.05, r: −0.198).
7) Finally, we carried out a multivariable regression analyses taking into account age, UPDRS III, rigidity, axial and distal bradykinesia subscores, freezing of gait, and cognition. Amimia was the dependent variable. Only distal bradykinesia (ß−0.500; 95% CI−0.178-0.08, p < 0.05) and UPDRS III scores (ß 1.155; 95% CI−0.019-0.155, p < 0.05) were significant.
The current study was designed to explore the relationship between amimia and other motor and nonmotor symptoms of PD and to evaluate the clinical impression that patients with higher amimia scores have a more severe illness, not only regarding motor symptoms, but also in terms of cognitive status.
Although loss of facial expression is a recognized parkinsonian sign that is well described by classic authors (9–11), its significance and correlation with other PD symptoms is poorly understood. Amimia is one of the most distinctive clinical features in PD and may be one of the earliest symptoms (19). However, in many cases, early amimia might be misinterpreted as lack of interest or depression by attending physicians and families (27). Bologna et al. summarizes several distinctive characteristics of facial expression in PD (7). It is worth recalling that rigidity and tremors scarcely affect the face in PD (15), amimia is rarely asymmetric (7, 16–18), and its response to levodopa and DBS is highly variable (14). For all these reasons, amimia is a peculiar PD symptom, much more laborious to assess than the rest of the PD signs. Furthermore, at this moment, the lack of objective tools to measure amimia makes its evaluation even more difficult.
Our sample shows the usual characteristics of a typical PD population sample (28). In our series, amimia correlated with most motor and nonmotor symptoms. It correlated with motor and total UPDRS scores, and in addition, amimia correlated with timed tests, an objective measure of bradykinesia. Globally, amimia is an indicator of motor impairment as a whole, including axial symptoms and freezing of gait. These results are in line with those from a very recent article published by Ricciardi et al. in which patients with hypomimia had a more severe burden of motor symptoms and higher axial scores (29).
A remarkable result of our study is the possible relationship between amimia and other axial symptoms, such as gait freezing. The results of Riccardi et al. support our findings, describing that patients with amimia have more severe axial symptoms (29). Previous reports also show that patients with freezing of gait often present a nontremor phenotype and have a worse cognitive status (30–32), but to the best of our knowledge, this is the first time that the relationship between amimia and gait freezing has been directly studied.
In our study, amimia also correlated with cognitive status measured by standard scales. Indeed, patients with dementia had greater amimia scores compared with the nondementia PD group. Previous studies report contradictory results about the relationship between amimia and dementia. Recently, Ricciardi et al. find that facial expression is not related to cognitive impairment (29) although Gasca-Salas suggests that de novo PD patients with mild cognitive impairment have more severe hypomimia than patients with normal performance in cognition tests (33). The cohort of Riccardi is younger than ours, which could explain, at least in part, the discrepancies in our results (70.7 ± 9.6 in our series vs. 60.3 ± 6.75) (29). According to our findings, the relationship between amimia and cognitive impairment is supported by previous reports in which patients with Lewy Body Disease exhibited more facial bradykinesia compared with PD patients (2, 34–36).
Amimia can be misdiagnosed as depression, a nonmotor symptom of PD (4); however, the relationship between amimia and depression is unclear. Although some studies associate amimia with poor facial emotion recognition and impaired simulated facial expressions (7, 36–38), we find no correlation between depression and facial bradykinesia as previously described (4, 29).
Finally, we aimed to develop an objective method for assessing amimia. In contrast to limb bradykinesia, facial bradykinesia is difficult to estimate based on clinical assessment (14). In order to find a complementary and more objective score than item 19 of UPDRS III, we studied upper facial bradykinesia by measuring both spontaneous resting blink rate and that during conversation. Unfortunately, blink rate correlated poorly with other symptoms of PD. However, resting blink frequency correlated with some motor scores (UPDRS III) as reported by Agostini and Korosec (39, 40), but it had a poor correlation with nonmotor symptoms. Additionally, spontaneous speaking blink frequency was a poor predictor of facial bradykinesia. Although most patients with PD hypomimia have a decrease in blinking frequency, it is suggested that some patients with advanced PD may have an increased spontaneous blink frequency as a form of dystonia (41). Our results suggest that the assessment of amimia should evaluate facial motility as a whole and not upper face motility alone.
Limitations of the present study include the difficulty in making an objective evaluation of amimia as item 19 UPDRS is the only clinically validated tool. At the same time, we did not evaluate the effect of dopa therapy because we assessed patients in the ON situation in order to have a sample as representative as possible of everyday patients. In addition, patients with different levels of severity were included, and for some of them, it would have been difficult to come to our outpatient clinic in an OFF condition.
On the other hand, this study was conducted prospectively on a wide spectrum of idiopathic PD patients with different cognitive and functional situations. We used a comprehensive clinical and cognitive study, including objective timed-test assessment of bradykinesia.
In conclusion, our results suggest that amimia is a potential predictor of global PD severity, including axial symptoms and cognitive decline. Nevertheless, an objective measurement of amimia that is more accurate than UPDRD19 is needed.
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found at (42).
The studies involving human participants were reviewed and approved by Comite De Ética De La Investigacion De La Fundacion Jimenez Diaz. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
TM-C and PG-R were involved in the study concept and design, the acquisition, analysis, and interpretation of study data, and in the critical revision of the manuscript for important intellectual content. PL-R collaborated in the acquisition of study data and in the critical revision of the manuscript for important intellectual content. CF-F, LG-V, and RG-C worked in the acquisition of data. RA participated in the study design and in the critical revision of the manuscript for important intellectual content. All authors have approved the final version for submission.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors thank Donna Leick for the English revision and Israel John Thuissard Vasallo for the statistical analyses.
1. Ellis RJ, Caligiuri M, Galasko D, Thal LJ. Extrapyramidal motor signs in clinically diagnosed Alzheimer disease. Alzheimer Dis Assoc Disord. (1996) 10:103–14. doi: 10.1097/00002093-199601020-00008
2. Aarsland D, Ballard C, McKeith I, Perry RH, Larsen JP. Comparison of extrapyramidal signs in dementia with lewy bodies and Parkinson's disease. J Neuropsychiatry Clin Neurosci. (2001) 13:374–9. doi: 10.1176/jnp.13.3.374
3. Mergl R, Mavrogiorgou P, Hegerl U, Juckel G. Kinematical analysis of emotionally induced facial expressions: a novel tool to investigate hypomimia in patients suffering from depression. J Neurol Neurosurg Psychiatry. (2005) 76:138–40. doi: 10.1136/jnnp.2004.037127
4. Katsikitis M, Pilowsky I. A controlled quantitative study of facial expression in Parkinson's disease and depression. J Nerv Ment Dis. (1991) 179:683–8. doi: 10.1097/00005053-199111000-00006
5. Hunker CJ, Abbs JH, Barlow SM. The relationship between parkinsonian rigidity and hypokinesia in the orofacial system: a quantitative analysis. Neurology. (1982) 32:749–54. doi: 10.1212/wnl.32.7.749
6. Katsikitis M, Pilowsky I. A study of facial expression in Parkinson's disease using a novel microcomputer-based method. J Neurol Neurosurg Psychiatry. (1988) 51:362–6. doi: 10.1136/jnnp.51.3.362
7. Bologna M, Fabbrini G, Marsili L, Defazio G, Thompson PD, Berardelli A. Facial bradykinesia. J Neurol Neurosurg Psychiatry. (2013) 84:681–5. doi: 10.1136/jnnp-2012-303993
8. Marsili L, Agostino R, Bologna M, Belvisi D, Palma A, Fabbrini G, et al. Bradykinesia of posed smiling and voluntary movement of the lower face in Parkinson's disease. Parkinsonism Relat Disord. (2014) 20:370–5. doi: 10.1016/j.parkreldis.2014.01.013
10. Neurology (volumes I&II) by Kinnier Wilson, S.A. [Samuel alexander] (edited by a. Ninian Bruce]: Very good Original Grey Cloth Hardback. Third Impression. Edinburgh Books. (1944). Available online at: https://www.abebooks.com/first-edition/Neurology-volumes-III-Kinnier-Wilson-S.A/22828917676/bd [Accessed November 7, 2020]
11. Goetz CG. The history of Parkinson's disease: early clinical descriptions and neurological therapies. Cold Spring Harb Perspect Med. (2011) 1:8862. doi: 10.1101/cshperspect.a008862
12. Cattaneo L, Pavesi G. The facial motor system. Neurosci Biobehav Rev. (2014) 38:135–59. doi: 10.1016/j.neubiorev.2013.11.002
13. Lako IM, Wigman JTW, Klaassen RMC, Slooff CJ, Taxis K, Bartels-Velthuis AA. Psychometric properties of the self-report version of the quick inventory of depressive symptoms (QIDS-SR16) questionnaire in patients with schizophrenia. BMC Psychiatry. (2014) 14:247. doi: 10.1186/s12888-014-0247-2
14. Berardelli A, Rothwell JC, Thompson PD, Hallett M. Pathophysiology of bradykinesia in Parkinson's disease. Brain J Neurol. (2001) 124:2131–46. doi: 10.1093/brain/124.11.2131
15. Bologna M, Fasano A, Modugno N, Fabbrini G, Berardelli A. Effects of subthalamic nucleus deep brain stimulation and l-DOPA on blinking in Parkinson's disease. Exp Neurol. (2012) 235:265–72. doi: 10.1016/j.expneurol.2012.02.004
16. Zingler VC, Strupp M, Jahn K, Brandt T. Hemihypomimia in Parkinson's disease. Eur Neurol. (2005) 53:92–3. doi: 10.1159/000085505
17. Crosiers D, Maréchal E, van Ael Y, Cras P. Left-sided hemihypomimia in Parkinson's disease. Acta Neurol Belg. (2011) 111:225–7.
18. Ozekmekçi S, Benbir G, Ozdogan FY, Ertan S, Kiziltan ME. Hemihypomimia, a rare persistent sign in Parkinson's disease: follow up of 11 patients. J Neurol. (2007) 254:347–50. doi: 10.1007/s00415-006-0372-z
19. Postuma RB, Lang AE, Gagnon JF, Pelletier A, Montplaisir JY. How does parkinsonism start? Prodromal parkinsonism motor changes in idiopathic REM sleep behaviour disorder. Brain J Neurol. (2012) 135:1860–70. doi: 10.1093/brain/aws093
20. Fereshtehnejad S-M, Yao C, Pelletier A, Montplaisir JY, Gagnon J-F, Postuma RB. Evolution of prodromal Parkinson's disease and dementia with lewy bodies: a prospective study. Brain J Neurol. (2019) 142:2051–67. doi: 10.1093/brain/awz111
21. Hughes AJ, Daniel SE, Kilford L, Lees AJ. Accuracy of clinical diagnosis of idiopathic Parkinson's disease: a clinico-pathological study of 100 cases. J Neurol Neurosurg Psychiatry. (1992) 55:181–4. doi: 10.1136/jnnp.55.3.181
22. Munsat TL. Assessment of Parkinson's disease. Quantification of Neurological Deficit. Edición: 1. Boston: Butterworth-Heinemann (1989).
23. Langston JW, Widner H, Goetz CG, Brooks D, Fahn S, Freeman T, et al. Core assessment program for intracerebral transplantations (CAPIT). Mov Disord Off J Mov Disord Soc. (1992) 7:2–13. doi: 10.1002/mds.870070103
24. Garcia Ruiz PJ, Muñiz de Igneson J, Ayerbe J, Frech F, Sánchez Bernardos V, Lopez Ferro O, et al. Evaluation of timed tests in advanced Parkinsonian patients who were candidates for subthalamic stimulation. Clin Neuropharmacol. (2005) 28:15–7. doi: 10.1097/01.wnf.0000150869.44630.71
25. Lau B, Meier N, Serra G, Czernecki V, Schuepbach M, Navarro S, et al. Axial symptoms predict mortality in patients with Parkinson disease and subthalamic stimulation. Neurology. (2019) 92:e2559–e70. doi: 10.1212/WNL.0000000000007562
26. Pagonabarraga J, Kulisevsky J, Llebaria G, García-Sánchez C, Pascual-Sedano B, Gironell A. Parkinson's disease-cognitive rating scale: a new cognitive scale specific for Parkinson's disease. Mov Disord Off J Mov Disord Soc. (2008) 23:998–1005. doi: 10.1002/mds.22007
27. Scott NJ, Kramer RSS, Jones AL, Ward R. Facial cues to depressive symptoms and their associated personality attributions. Psychiatry Res. (2013) 208:47–53. doi: 10.1016/j.psychres.2013.02.027
28. García-Ruiz PJ, Del Val J, Fernández IM, Herranz A. What factors influence motor complications in Parkinson disease?: a 10-year prospective study. Clin Neuropharmacol. (2012) 35:1–5. doi: 10.1097/WNF.0b013e31823dec73
29. Ricciardi L, De Angelis A, Marsili L, Faiman I, Pradhan P, Pereira EA, et al. Hypomimia in Parkinson's disease: an axial sign responsive to levodopa. Eur J Neurol. (2020) 27:2422–29. doi: 10.1111/ene.14452
30. Giladi N, McDermott MP, Fahn S, Przedborski S, Jankovic J, Stern M, et al. Freezing of gait in PD: prospective assessment in the DATATOP cohort. Neurology. (2001) 56:1712–21. doi: 10.1212/WNL.56.12.1712
31. Zhang H, Yin X, Ouyang Z, Chen J, Zhou S, Zhang C, et al. A prospective study of freezing of gait with early Parkinson disease in Chinese patients. Medicine. (2016) 95:e4056. doi: 10.1097/MD.0000000000004056
32. Ehgoetz Martens KA, Lukasik EL, Georgiades MJ, Gilat M, Hall JM, Walton CC, et al. Predicting the onset of freezing of gait: a longitudinal study: anxiety is a predictor of fog onset. Mov Disord. (2018) 33:128–35. doi: 10.1002/mds.27208
33. Gasca-Salas C, Urso D. Association between hypomimia and mild cognitive impairment in de novo Parkinson's disease patients. Can J Neurol Sci J Can Sci Neurol. (2020) 2020:1–3. doi: 10.1017/cjn.2020.93
34. Stern Y, Marder K, Tang MX, Mayeux R. Antecedent clinical features associated with dementia in Parkinson's disease. Neurology. (1993) 43:1690–2. doi: 10.1212/wnl.43.9.1690
35. Elgh E, Domellöf M, Linder J, Edström M, Stenlund H, Forsgren L. Cognitive function in early Parkinson's disease: a population-based study: cognition in Parkinson. Eur J Neurol. (2009) 16:1278–84. doi: 10.1111/j.1468-1331.2009.02707.x
36. Herrera E, Cuetos F, Rodríguez-Ferreiro J. Emotion recognition impairment in Parkinson's disease patients without dementia. J Neurol Sci. (2011) 310:237–40. doi: 10.1016/j.jns.2011.06.034
37. Argaud S, Vérin M, Sauleau P, Grandjean D. Facial emotion recognition in Parkinson's disease: a review and new hypotheses. Mov Disord. (2018) 33:554–67. doi: 10.1002/mds.27305
38. Ricciardi L, Visco-Comandini F, Erro R, Morgante F, Bologna M, Fasano A, et al. Facial emotion recognition and expression in Parkinson's disease: an emotional mirror mechanism? PLoS ONE. (2017) 12:e169110. doi: 10.1371/journal.pone.0169110
39. Korošec M, Zidar I, Reits D, Evinger C, VanderWerf F. Eyelid movements during blinking in patients with Parkinson's disease. Mov Disord. (2006) 21:1248–51. doi: 10.1002/mds.20930
40. Agostino R, Bologna M, Dinapoli L, Gregori B, Fabbrini G, Accornero N, et al. Voluntary, spontaneous, and reflex blinking in Parkinson's disease. Mov Disord Off J Mov Disord Soc. (2008) 23:669–75. doi: 10.1002/mds.21887
41. Kimber TE, Thompson PD. Increased blink rate in advanced Parkinson's disease: a form of 'off'-period dystonia? Mov Disord Off J Mov Disord Soc. (2000) 15:982–5. doi: 10.1002/1531-8257(200009)15:5<982::aid-mds1033>3.0.co
42. Maycas T. Parkinson's Disease and Facial Bradykinesia. Mendeley Data. (2020). Available online at: https://data.mendeley.com/datasets/4tjd8jrhp8/1
Keywords: facial bradykinesia, Parkinson's disease (PD), hypomimia, amimia, motor symptom, non-motor symptom
Citation: Maycas-Cepeda T, López-Ruiz P, Feliz-Feliz C, Gómez-Vicente L, García-Cobos R, Arroyo R and García-Ruiz PJ (2021) Hypomimia in Parkinson's Disease: What Is It Telling Us? Front. Neurol. 11:603582. doi: 10.3389/fneur.2020.603582
Received: 07 September 2020; Accepted: 01 December 2020;
Published: 25 January 2021.
Edited by:
Mayela Rodríguez-Violante, Manuel Velasco Suárez Instituto Nacional de Neurología y Neurocirugía, MexicoReviewed by:
James Mac Shine, The University of Sydney, AustraliaCopyright © 2021 Maycas-Cepeda, López-Ruiz, Feliz-Feliz, Gómez-Vicente, García-Cobos, Arroyo and García-Ruiz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Teresa Maycas-Cepeda, dG1heWNhc0BnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.