 Kaiming Liu
Kaiming Liu Brian Z. Wang2
Brian Z. Wang2 Mengxiong Pan
Mengxiong Pan
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Neurol., 01 December 2020
Sec. Headache and Neurogenic Pain
Volume 11 - 2020 | https://doi.org/10.3389/fneur.2020.543485
This article is part of the Research TopicStill Searching for the Origin of Migraine: From Comorbidities to ChronicizationView all 13 articles
Background: Migraine is a widespread neurological disorder. The patent foramen ovale (PFO) is a remnant of the fetal circulation. Multiple studies suggest that migraine is more prevalent in subjects with PFO and vice versa. It is unclear if there is a causal relationship or simply a co-existence of these two conditions. Furthermore, the treatment of migraine with percutaneous closure PFO remains controversial.
Methods: We reviewed studies pertaining to the relationship between PFO and migraine as well as the effects of treatments on migraine attacks.
Results: We briefly summarized potential pathophysiological mechanisms of migraine, and elaborated on migraine type, frequency, and clinical symptoms of migraine with PFO and the clinical features of PFO with migraine. We also addressed the effects of PFO closure on migraine attacks.
Conclusion: The evidence supports a “dose-response” relationship between migraine and PFO although more work needs to be done in terms of patient selection as well as the inclusion of an antiplatelet control group for PFO closure interventions to uncover possible beneficial results in clinical trials.
Migraine, one of the most common conditions of primary headache, often occurs in people aged 20-64 years old, with a high disability rate and heavy disease burden (1). According to the 2013 Global Burden of Disease survey from the World Health Organization (WHO), migraine was the 3rd most common disease and ranked 6th in causing major disability in humans, which was calculated based on the number of years of life lost to disability (2).
The foramen ovale is a channel between the left and right atria of the heart during the embryonic period. Under normal physiological conditions, the foramen ovale will close in the first year after birth. If, however, it is not closed after three years of age, it is termed as patent foramen ovale (PFO) (3). It has been reported that PFO is the most common congenital cardiac anomaly in adults (4). In fact, about 20-30% of adults have an incomplete fusion of the fossa, which is a permanent slit-like interatrial opening (5). Usually, the blood pressure of the left atrium is higher than that of the right atrium, which will not cause right-to-left shunt (RLS). RLS via the PFO may occur when the pressure in the right atrium exceeds the left to give rise to structural changes in the heart, pulmonary hypertension, coughing, sneezing, and laughing. Although atrial septal defects and pulmonary arteriovenous malformations may also cause the right-to-left blood flow, they are relatively rare in migraine patients (6).
Del (7) first proposed the relationship between migraine and PFO in 1998, he found that the incidence of PFO in migraine patients was significantly higher than that in healthy controls. Later, a number of studies found that the incidence of PFO in migraine patients was 14.6-66.5% (8) while the incidence in the general population was 9-27.3% (5, 9, 10). In turn, in the population with PFO, the incidence of migraine was 9.13-51.7%, which was also higher than the incidence of migraine in the general population (11–13). However, until now, no consensus has been reached on the relationship between PFO and migraines. Therefore, this review aims to further investigate the association between migraine and PFO.
The idea that migraine and PFO is correlated has only been around for a few decades, and much of the underlying pathophysiology is still based on hypotheses. It is thought that many vasoactive substances are usually discharged or metabolized through the pulmonary circulation. Through the PFO channel, venous blood can enter arterial blood by shunting without circulating in the lungs. Some chemicals and hormones such as serotonin can bypass the pulmonary circulation and pass directly through the blood-brain barrier to cause migraine (5). Moreover, a tiny embolus in the systemic circulation can pass through the PFO and directly into the arterial system. These “paradoxical embolisms,” which lead to tiny brain infarctions, triggering low perfusion or cortical spreading depression, may cause a migraine attack (5), and could be the most probable pathophysiological mechanism on how PFO could lead to a migraine attack. This hypothesis can also explain the use of antiplatelets or anticoagulants (14–16) and atrial fibrillation ablation (17) for relieving migraine attacks. Others have also found that a RLS is correlated with a higher frequency of multiple cortical lesions in DWI sequences, which distinguishes itself from atrial fibrillation-related ischemic stroke that is seen occurring in the cortical-subcortical territory (18). Incidentally, the posterior circulation is more likely to be involved (19). Blood flow of the posterior circulation significantly exceeds that of the anterior circulation in migraine patients with PFO when undergoing the Valsalva maneuver (20). During the aura phase, focal areas of hypoperfusion close to the ischemic threshold in occipital regions, which might be due to these cerebral microinfarcts, can cause visual symptoms (21). Meanwhile, a RLS results in decreased blood oxygen saturation and hypoxia, which increases the expression of plasminogen activator-1 and result in inhibition of fibrinolysis and thus increases the possibility of microembolization. On the other hand, a decrease in cerebral oxygen saturation will trigger cortical spreading depression as well, which can also lead to migraines (22, 23). Genetic factors may also cause these patients to develop both diseases. About 2-fold higher frequency of PFO is seen in migraineurs as compared with the general population, suggesting that a genetic influence could predispose some patients to a higher risk of developing both migraine and atrial septal abnormalities (4); hereditary associations with migraine have been found in autosomal dominant PFO (24). Taken together, the pathophysiological mechanisms are complex and migraine is possibly the result of these pathways working synergistically.
Clinical examination methods are commonly used for diagnosing PFO including transesophageal echocardiography (TEE), contrast transcranial doppler echocardiography (cTCD) and contrast transthoracic echocardiography (cTTE). Among these, TEE is considered the gold standard for PFO diagnosis (7). However, due to the invasive nature of the procedure, patients find it difficult to successfully complete the Valsalva maneuver during TEE examination. Thus, the detection rate of RLS is lower than that of cTTE (8, 9), and have been shown to normally have a 10% rate of false negatives (10). cTCD is used to predict RLS by observing the amount of air microemboli in the cranial circulation at the resting state and after Valsalva maneuver. Although cTCD is a non-traumatic procedure, about 5% of shunts detected by cTCD does not correspond with PFO (11). The sensitivity and specificity of cTCD for RLS are 68-100% and 65-100%, respectively (12). Likewise, cTTE is also noninvasive but can isolate the source of RLS with a specificity of 97-100% albeit with a slightly lower sensitivity of about 63-100% (13, 14). At present, the varying diagnostic methods contributes to the diversity in the relationship between PFO and migraine. Therefore, a comparison of these individual methods and how it affects the relationship in question may be helpful.
The incidence of migraine with aura is 4.4%, comprising about 25-30% of migraineurs (25). Studies have found a stronger association between migraine with aura and PFO (26, 27). Among migraine patients, the incidence of PFO is 46.3-88% in migraine patients with aura (22, 23, 28, 29) compared with 16.2-34.9% in migraine patients without aura (30, 31). Interestingly, the incidence of PFO in migraine patients without aura is similar to that in the general population (6, 7, 9, 31). As PFO may be associated with migraine with aura, one study investigated the incidence of PFO in migraine patients with typical or atypical aura. The authors found that the PFO prevalence in the atypical aura group was 79.2% vs. 46.3% in the typical aura group (28). Therefore, it was suggested that PFO was more closely related to patients with atypical aura migraine but the specific mechanism remains unclear. Another report investigated the incidence of PFO in non-migraine patients with visual aura; 67% of the patients had PFO and 80% of those patients had improvement in symptoms after PFO closure, indicating that the presence of PFO could be one of the underlying mechanisms associated with aura pathology (32). Therefore, we consider the PFO having a closer relationship in migraine patients with aura, especially atypical aura, although non-migraine with aura is also correlated with the presence of the PFO.
Chronic migraine occur in about 2-3% of the population (33, 34). For one to be diagnosed with chronic migraine, the ICHD-3 criteria states that the patient would have “headache occurring on ≥15 days per month for >3 months, which has the features of migraine headache on ≥8 days per month” (35). Studies have shown that the incidence of PFO in chronic migraine, with aura or without aura, is higher. Of the 131 chronic migraine patients enrolled in a study, 66% had PFO, higher than PFO incidence in both the general population and episodic migraine patients (36). Another retrospective study focused on the relationship between visual aura frequency and PFO. A hundred and forty two migraine patients were divided into (i) frequent aura group (number of visual aura >50% of frequency of headaches) and (ii) accidental aura group (number of visual aura <50% of frequency of headaches). The results showed that migraine patients with frequent visual aura suffered a higher degree of RLS, and the symptoms improved after PFO closure (37). The high prevalence of PFO in chronic migraine patients do not indicate that PFO tend to stimulate chronic headaches, but still is associated with the number of migraine attacks, especially for large, high grade shunts.
The clinical presentation of migraine seems indistinguishable in migraine patients with or without PFO. There is little statistically significant evidence in the patient's personal history, including age, sex, smoking history or migraine onset, including the symptoms of headache, and concomitant symptoms of PFO. The SAM (Shunt-Associated Migraine) study was a prospective, multicenter, observational study, intended to illustrate the difference of the clinical features of migraine with or without blood flow shunt. A total of 460 patients were included in the study. Migraine patients with RLS and without RLS accounted for 58% and 42% of the total patients, respectively. Migraine features were not significantly correlated, except that patients with RLS were relatively young and had aura sensory symptoms with slightly higher frequency (38). In chronic migraine patients, PFO and non-PFO patients have similar headache characteristics and neurological symptoms (36). PFO seems to play a role in triggering migraines but have little relation to migraine symptoms. Recently, it was found that the attack frequency, HIT-6, and MIDAS scores among migraine patients with moderate or large PFO were significantly higher than those of the mild PFO and non-PFO groups. After PFO closure, the differences in VAS, HIT-6 and MIDAS scores as well as the headache duration were statistically significant (39). At this point in time, it cannot be concluded that the scale scores changed due to the attack frequency or severity, but the result does provide more evidence supporting the relationship between PFO presence and migraine presentation. Studies are now needed to explore the correlation and the analysis of the scale needs to be refined.
Under resting conditions, no RLS exists generally because the blood pressure in the left atrium is higher than in the right. After performing the Valsalva maneuver, the pressure of the right atrium will exceed that of the left atrium to give rise to transient RLS. During PFO examination, the RLS should be detected at rest and post-Valsalva. RLS occurring under normal respiration is called permanent PFO while RLS occurring only after the Valsalva maneuver is called latent PFO (23).
Persistent shunt accounts for 67-72% and latent shunt exist 28-33% in migraine with PFO patients (22, 23, 29). One study showed that 12 of the 159 migraine patients with aura experienced a migraine attack when they were undergoing the cTCD test. Surprisingly, all these patients had permanent PFO and the majority were massive shunts (22), indicating that permanent PFO is closely associated with migraines and triggers a migraine attack.
PFO is usually divided into three types: large PFO (≥4.0 mm), medium PFO (2.0-3.9 mm) and small PFO (≤1.9 mm) (40). However, this classification standard is only accurately measured by autopsy or estimated by TEE, which is not commonly used in clinical practice. RLS from PFO is considered when microvesicles are found within 3-5 cardiac cycles during a cTTE examination (41, 42). PFO size is usually graded according to the number of microbubbles in the left atrium on a single still image. cTCD is graded according to the number of microvesicles found in the bilateral cerebral circulation. The amount of RLS detected by cTCD is positively correlated with the size of PFO measured by TEE (43).
Approximately 75% of migraine patients with PFO have a large RLS and 25% have a small shunt (23). Among all PFO subjects, the proportion of large triage is higher in migraine patients than in healthy subjects. In migraine patients with aura especially, a greater proportion of permanent PFO and large PFO were found (44). Schwartzman (6) studied 93 migraine patients with aura and 93 healthy controls. All subjects underwent cTTE and they found that the number of people having small RLS among migraineurs and healthy controls were similar but a moderate or large RLS occurred more frequently in the migraine group. Similarly, among patients with cryptogenic stroke, Anzola (45) found that migraine patients had a larger shunt vs. non-migraine patients. The difference was even more pronounced when compared with the control group. PFO is also considered a probable risk factor in cryptogenic stroke of which micro-embolism may contribute to its pathogenesis. PFO is frequently found in older patients with stroke (46) as well as several other stroke subtypes (47, 48), and the stroke attributable fraction for PFO can be defined through standardized scores (48, 49). Taken together, PFO may be associated with migraine and could increase the risk of stroke in migraine patients. The larger the PFO size indicates a larger RLS, which is more likely to cause a migraine.
Atrial septal aneurysm (ASA) is a kind of congenital atrial septal dilatation, which means that the atrial septal distention is >10 mm in one side of the atrial septal plane, and the basal width of the tumor is >15 mm, involving the fossa ovalis region (3). According to echocardiography studies and post-mortem epidemiological studies, the prevalence of ASA of the general population is about 1-2.5% (9, 50). PFO complicated with atrial septal tumor have been shown to be a risk factor for both cryptogenic (51, 52) and recurrent cryptogenic strokes, suggesting that medical treatment could be refined (53–55). Recent studies also showed that migraine has a high correlation with PFO and ASA (44, 56). In Snijder's study (44), the prevalence of PFO with ASA was significantly higher in migraine patients compared to patients without migraine. In addition, the shunt of patients with PFO combined with ASA was significantly larger than that of patients with PFO alone. Therefore, the combination of PFO and ASA may lead to increasing shunt flow and the occurrence of migraine.
The Eustachian valve (EV) and Chiari network (CN) are remnants of venous valves caused by incomplete absorption of these structures (52, 57). Embryologically, EV is a semicircular structure facing the anterior-inferior aspect of the inferior vena cava, directing blood flow from the inferior vena cava to the fossa ovale, which plays a vital role in the shunt of blood flow to the ovale (58, 59). The CN is a large multi-perforated EV with a reticular appearance found in approximately 2% of the population (60). Previous studies had reported that EV and CN were more common in patients with cryptogenic stroke (61, 62). Rigatelli (63) prospectively investigated the potential effects of EV/CN on migraine patients with PFO and found that the frequency of EV/CN was 100% and 60% in migraineurs with aura and migraineurs without aura, respectively. Meanwhile, patients with EV/CN had more “curtain pattern,” larger RLS on TCD and higher preoperative MIDAS score. After PFO closure, the MIDAS score decreased significantly. Formation of an atrial septal aneurysm and persistent EV/CN may prevent spontaneous closure of PFO afterbirth, facilitating RLS, and indirectly inducing a migraine attack.
Migraine and PFO may be in a “dose-response” relationship. For example, the large size, persistency of PFO, and anatomic variations of PFO can intensify RLS, by which increased vasoactive substances or tiny emboli can pass through the blood-brain barrier and cause a higher number of hypoperfusion events to result in a migraine. These provide further evidence for migraine treatment, not only more accurate treatment choices for different patients, but also help guide surgical treatment.
In 1992, percutaneous PFO closure was first performed (64), and the benefits of PFO closure in migraine patients were first reported in 2000 (65). Since then, there have been a series of studies about the effect of PFO closure in migraine. Among the case series studies, PFO closing resolved headaches in 14-85% of patients, among which 25-85% had migraine with aura and 14-50% were migraine without aura. 4-58% of patients had ameliorated migraine with aura and 20-68% migraine without aura. 6-43% of patients had no change in symptoms while 3-8% had worse symptoms (65–85) (see Table 1). In the case control studies, PFO closure is also associated with decreased migraine severity (32, 86–90) (see Table 2). In a study, PFO closure had statistically significant benefit with VAS, HIT-6 and MIDAS scores and the headache duration (39), especially for patients younger than 45 years (91). In addition, the closure of PFO resulted in a significant reduction in the use of abortive medications (86).
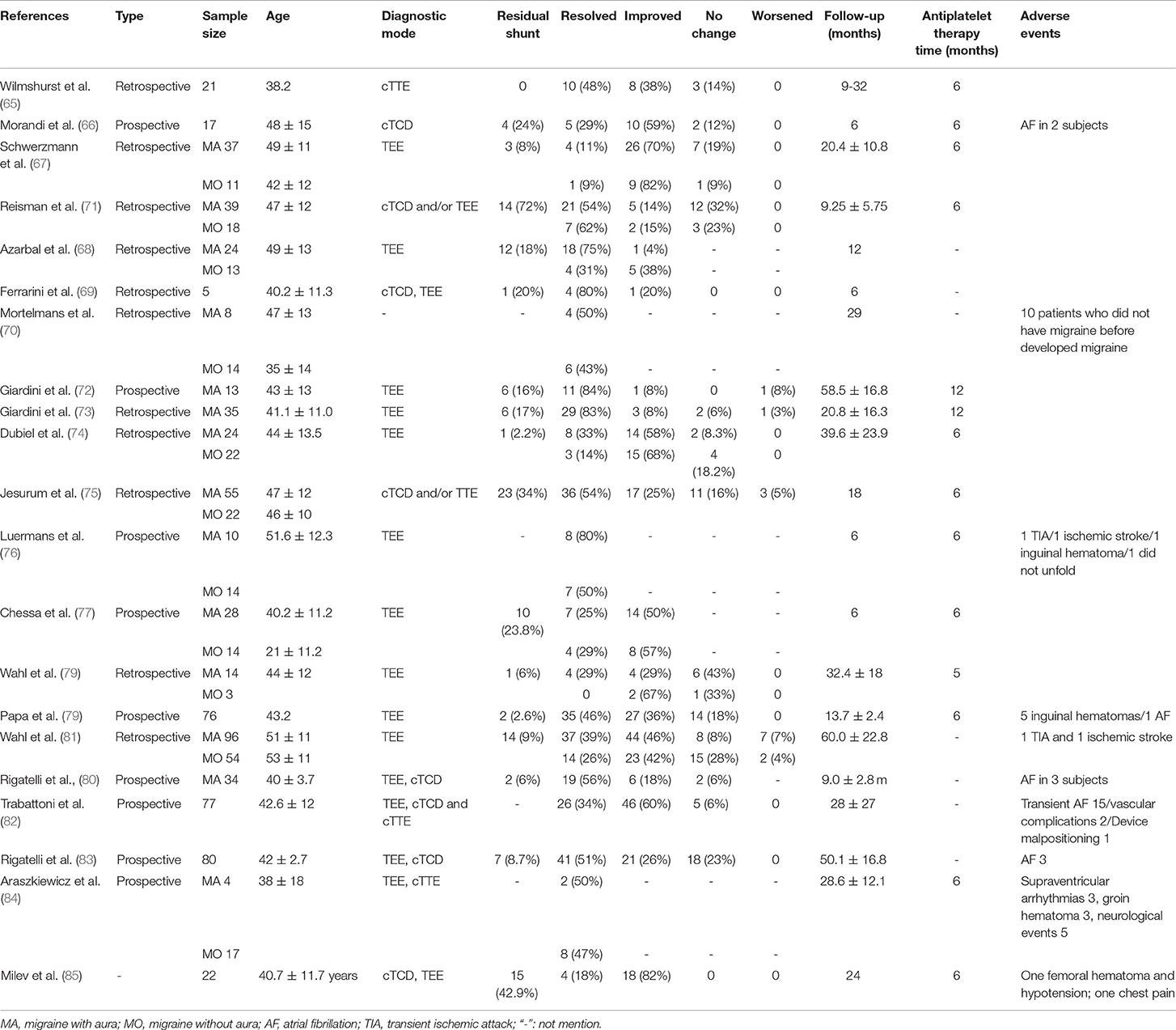
Table 1. The Effect of Patent Foramen Ovale Closure on Migraine in case series studies.
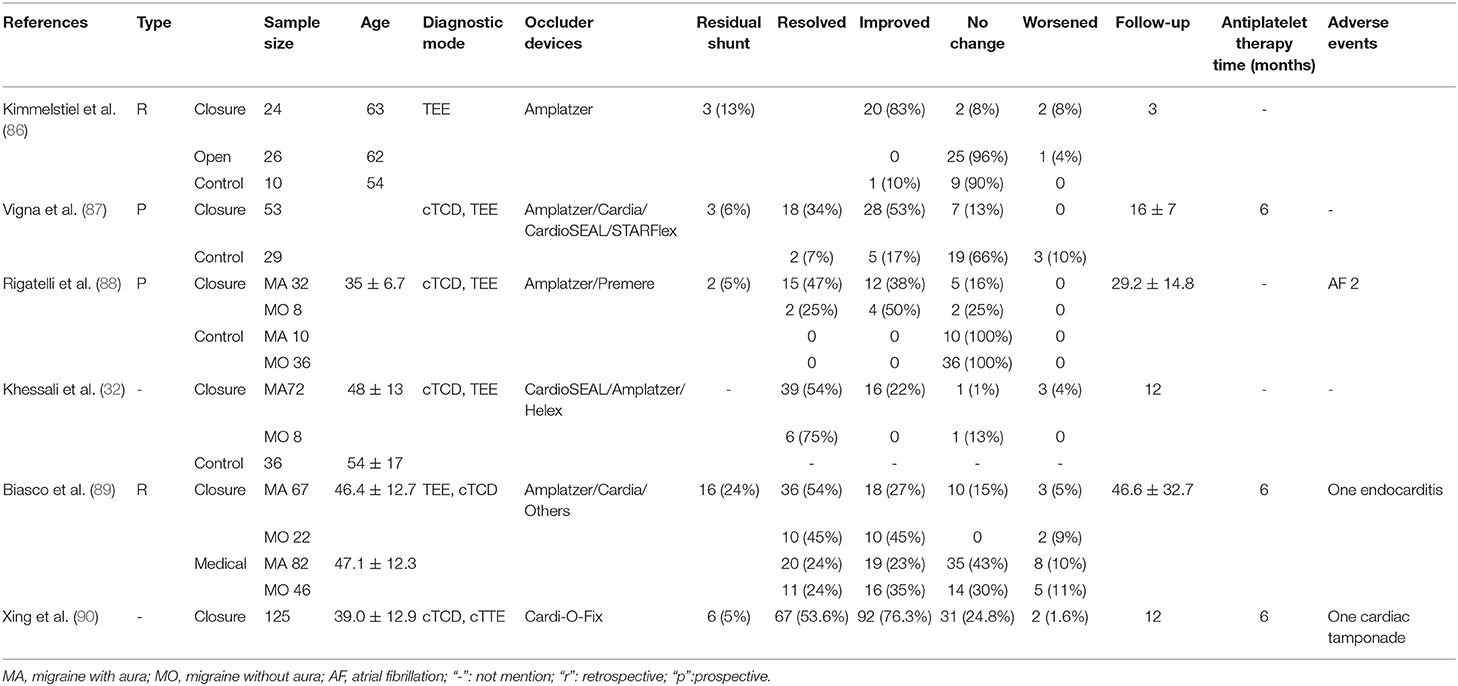
Table 2. The Effect of Patent Foramen Ovale Closure on Migraine in case-control studies.
However, in randomized controlled studies, the results were unremarkable (see Table 3). Migraine Intervention With STARFlex Technology (MIST) is the first prospective, multicenter, double-blind, controlled study to evaluate the efficacy of PFO with STARFlex implants for refractory migraine. After follow-up at 6 months, there were no significant differences (implant vs. control group) in the main therapeutic endpoints and headache cessation at 91-180 days after the closure. The same results were seen at the secondary endpoint. Upon further exploratory analysis, after excluding two outliers, the implant group saw a significant reduction in number of migraine days. With respect to the results of MIST and observational studies, it was explained that, first of all, there were physiological differences between the study group and the group of patients treated in the observational study. In addition, the RLS might not be effectively closed by the device used, which resulted in differences in experimental results (92). Subsequently, the PRIMA (Percutaneous closure of patent foramen ovale in migraine with aura) study also aimed to evaluate the efficacy of percutaneous PFO closure in patients of migraine with aura who were refractory to medical treatment. The primary and secondary efficacy endpoints, the decrease number of migraine attacked in 3 months after treatment and the average decrease number of migraine attacked separately, including the total cessation of headache, all improved in the treatment group, though with no statistical significance (93). Recently, PREMIUM (Prospective, Randomized Investigation to Evaluate Incidence of Headache Reduction in Subjects with Migraine and PFO Using the AMPLATZER PFO Occluder to Medical Management) studied patients with 6-14 days of migraine per month who had a large RLS and failed at least three preventive medications. For the primary efficacy end event endpoint, a 50% reduction in the number of headache episodes in the procedure group was seen though again, was not statistically significant. The secondary efficacy endpoint which was to reduce the number of headache days saw statistically significant differences in both groups. In the subgroup analysis, the proportion of frequent migraineurs with aura (more than 50% of migraine attacks with aura) reaching the primary efficacy end event was significantly higher than that of the control group, even 15.4% patients had headache cessation (94). These RCT results, although mostly insignificant, can still inform future clinical trials in terms of (i) patient selection e.g., patients with migraine with more frequent aura attacks and patients PFO with large RLS can be top priorities since these are affected by the “dose-response” relationship of migraine and PFO; and (ii) additional subgroup analyses e.g., excluding outliers. In fact, present ethical considerations stipulate that clinical studies can only recruit those with severe refractory migraine and not non-refractory migraine, which is an issue that needs to be addressed since a study design involving non-refractory migraine patients would be beneficial on many levels.
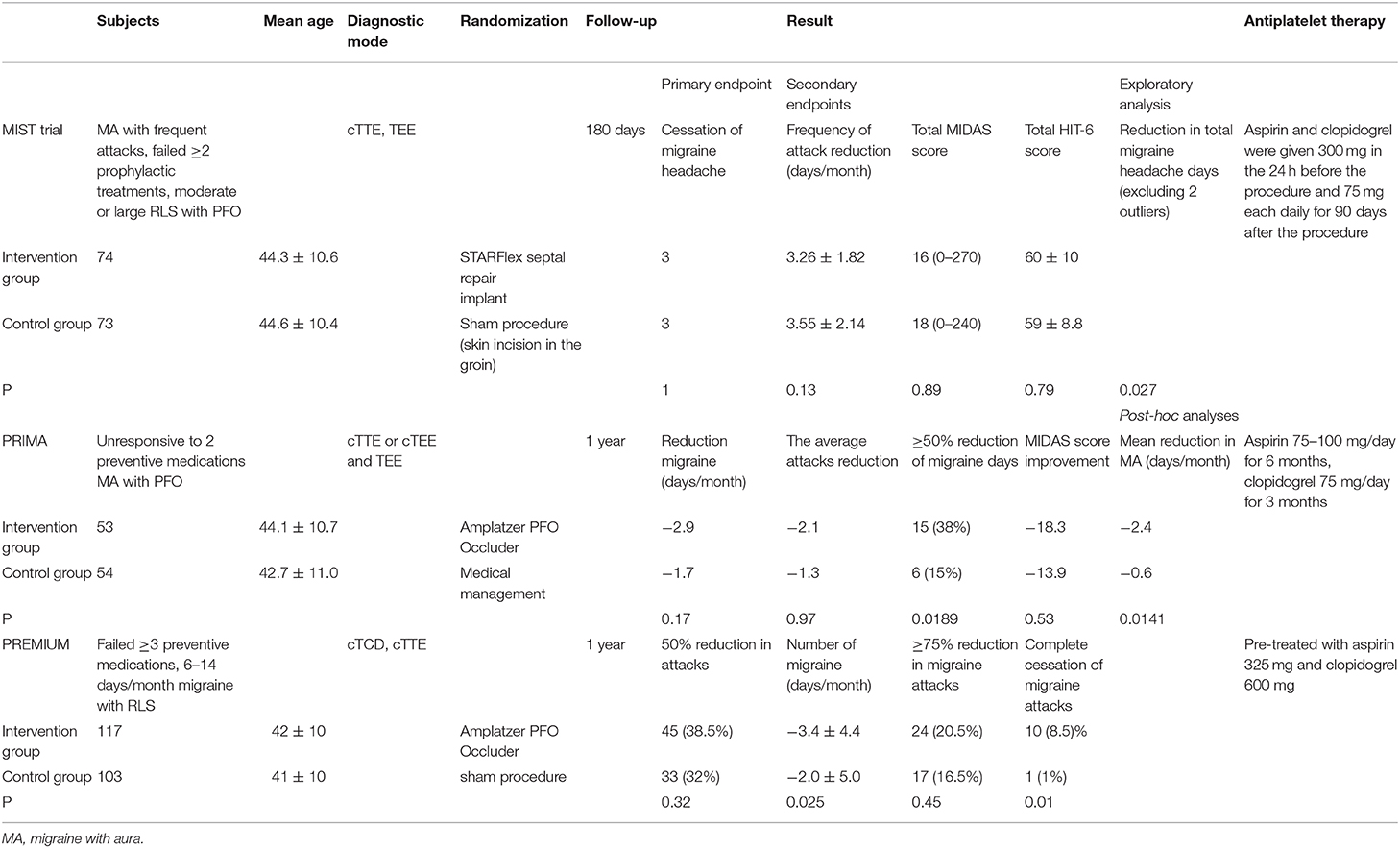
Table 3. The Effect of Patent Foramen Ovale Closure on Migraine in randomized controlled studies.
Considering the abnormal coagulation mechanism, the formation of “micro-embolisms” may also be one of the important causes of migraine. Some studies had reported the effects of antiplatelet agents on PFO associated with migraine (95, 96). A study of 136 patients with migraine and PFO who had a stroke previously, found that 90 patients (66%) had ≥50% decreased headache days per month compared to baseline after administration of clopidogrel or prasugrel. Fifty-five patients received PFO closure and discontinued antiplatelet medication 3 months after PFO surgery. Out of these, 52 patients (94%) had relief of headaches up until the follow-up of 6 years. Twenty-six patients without PFO closure who had been taking antiplatelet drugs also responded favorably up till 4 years of follow-up. However, 8 patients who did not take antiplatelet drugs or receive PFO closure, later experienced headache after 4-5 days, which was the anticipated washout period for the antiplatelet drugs. Antiplatelet medicine and PFO closure had a similar effect in migraine patients, so it was speculated that migraine pathogenesis involves venous platelet activation or aggregation, wherein tiny emboli causes the migraine (97). Subsequently, a prospective study found that the use of Tigarelor also reduced the frequency of migraine attacks in some PFO patients (98). Therefore, postoperative antiplatelet drug should be considered an important confounding factor in assessing the efficacy of PFO closure, and future research should consider setting the antiplatelet medication group as the control group for PFO closure. Of note, many studies of follow-up periods of less than 6 months possibly had their results confounded by the administration of antiplatelet drugs which they did not take into account during analyses.
In this review, we attempted to specifically address the relationship between migraine and PFO, elucidate mechanisms and improve estimation of the risks and benefits of the different therapeutic strategies available. The incidence of PFO in migraine patients is higher than that in the general population, suggesting that PFO and migraine may be risk factors for each other, but more research is needed to confirm this speculation. An increasing number of studies have found that migraines with aura are more closely associated with PFO, and the presence of RLS increased the likelihood of aura attacks, reducing the susceptibility to migraine attacks after exposure to other triggers. The frequency of headache onset, but not its clinical features, is also correlated with PFO, which seem to suggest that RLS may trigger the onset of migraine without directly affecting the migraine symptoms. In addition, the type and size of the foramen ovale are also associated with migraine. Persistent PFO, larger PFO, and complex tissue structures may cause more RLS of the blood to increase the incidence of migraine. Taken together, these support the “dose-response” relationship between RLS and migraine.
Based on the current findings, PFO occlusion was not satisfactory for the improvement of headaches in migraine patients. More accurate adequate patient recruitment may lead to greater postoperative benefit and more significant symptom improvement. Observational studies may further elaborate on the relationship between migraine and PFO type. Furthermore, randomized controlled studies should not be limited to patients with medication refractory migraineurs. Moving forward, investigation is needed to identify those migraineurs who are more likely to benefit or invalid from the closure of PFO, and in our opinion, migraines with more frequent aura attacks and PFO with larger RLS shunt should be research priorities. In addition, antiplatelet agents must be a control group for clinical trials of PFO closure. Lastly, researchers should consider that the closure of PFO may carry a small but relevant risk of serious adverse events including stroke, pericardial tamponade, atrial fibrillation and death (99).
KL conceived the idea for and edited the manuscript. BZW substantially revised the manuscript for readability and intellectual content. YH contributed to table design and manuscript revision. SS contributed expert medical advice and to manuscript revision. MP reviewed the literature and drafted and edited the manuscript. All authors read and approved the final submitted version.
This study was supported by the following funding sources: the Shandong Provincial Natural Science Foundation of China (Grant No. ZR2013HQ050), the Zhejiang Provincial Natural QA14 Science Foundation of China (Grant Nos. Y19H090025 and LQ15H090003), the National Natural Science Foundation of China (Grant 357 No. 81101157).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Stewart WF, Roy J, Lipton RB. Migraine prevalence, socioeconomic status, and social causation. Neurology. (2013) 81:948–55. doi: 10.1212/WNL.0b013e3182a43b32
2. Global Burden of Disease Study C. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. (2015) 386:743–800. doi: 10.1016/S0140-6736(15)60692-4
3. Kerut EK, Norfleet WT, Plotnick GD, Giles TD. Patent foramen ovale: a review of associated conditions and the impact of physiological size. J Am Coll Cardiol. (2001) 38:613–23. doi: 10.1016/S0735-1097(01)01427-9
4. Kumar P, Kijima Y, West BH, Tobis JM. The Connection Between Patent Foramen Ovale and Migraine. Neuroimaging Clin N Am. (2019) 29:261–70. doi: 10.1016/j.nic.2019.01.006
5. Wilmshurst P, Nightingale S. Relationship between migraine and cardiac and pulmonary right-to-left shunts. Clin Sci. (2001) 100:215–20. doi: 10.1042/cs1000215
6. Schwerzmann M, Nedeltchev K, Lagger F, Mattle HP, Windecker S, Meier B, et al. Prevalence and size of directly detected patent foramen ovale in migraine with aura. Neurology. (2005) 65:1415–8. doi: 10.1212/01.wnl.0000179800.73706.20
7. Del Sette M, Angeli S, Leandri M, Ferriero G, Bruzzone GL, Finocchi C, et al. Migraine with aura and right-to-left shunt on transcranial Doppler: a case-control study. Cerebrovasc Dis. (1998) 8:327–30. doi: 10.1159/000015875
8. Lip PZ, Lip GY. Patent foramen ovale and migraine attacks: a systematic review. Am J Med. (2014) 127:411–20. doi: 10.1016/j.amjmed.2013.12.006
9. Hagen PT, Scholz DG, Edwards WD. Incidence and size of patent foramen ovale during the first 10 decades of life: an autopsy study of 965 normal hearts. Mayo Clin Proc. (1984) 59:17–20. doi: 10.1016/S0025-6196(12)60336-X
10. Fisher DC, Fisher EA, Budd JH, Rosen SE, Goldman ME. The incidence of patent foramen ovale in 1,000 consecutive patients. A contrast transesophageal echocardiography study. Chest. (1995) 107:1504–9. doi: 10.1378/chest.107.6.1504
11. Dao CN, Tobis JM. PFO and paradoxical embolism producing events other than stroke. Catheter Cardiovasc Interv. (2011) 77:903–9. doi: 10.1002/ccd.22884
12. Faggiano P, Frattini S, Piovesana P, Lorusso R, Chiari E, Scolari F, et al. Low cerebrovascular event rate in subjects with patent foramen ovale and different clinical presentations: results from a prospective non-randomized study on a population including patients with and without patent foramen ovale closure. Int J Cardiol. (2012) 156:47–52. doi: 10.1016/j.ijcard.2010.10.032
13. Truong T, Slavin L, Kashani R, Higgins J, Puri A, Chowdhry M, et al. Prevalence of migraine headaches in patients with congenital heart disease. Am J Cardiol. (2008) 101:396–400. doi: 10.1016/j.amjcard.2007.08.047
14. Lipton RB, Goldstein J, Baggish JS, Yataco AR, Sorrentino JV, Quiring JN. Aspirin is efficacious for the treatment of acute migraine. Headache. (2005) 45:283–92. doi: 10.1111/j.1526-4610.2005.05065.x
15. Maggioni F, Bruno M, Mainardi F, Lisotto C, Zanchin G. Migraine responsive to warfarin: an update on anticoagulant possible role in migraine prophylaxis. Neurol Sci. (2012) 33:1447–9. doi: 10.1007/s10072-011-0926-4
16. Russo A, Santi S, Gueraldi D, De Paola M, Zani F, Pini LA. An unusual case report on the possible role of Warfarin in migraine prophylaxis. Springerplus. (2013) 2:48. doi: 10.1186/2193-1801-2-48
17. Mohanty S, Mohanty P, Rutledge JN, Di Biase L, Yan RX, Trivedi C, et al. Effect of catheter ablation and periprocedural anticoagulation regimen on the clinical course of migraine in atrial fibrillation patients with or without pre-existent migraine: results from a prospective study. Circ Arrhythm Electrophysiol. (2015) 8:279–87. doi: 10.1161/CIRCEP.114.002285
18. Kim BJ, Sohn H, Sun BJ, Song JK, Kang DW, Kim JS, et al. Imaging characteristics of ischemic strokes related to patent foramen ovale. Stroke. (2013) 44:3350–6. doi: 10.1161/STROKEAHA.113.002459
19. He D, Li Q, Xu G, Hu Z, Li X, Guo Y, et al. Clinical and imaging characteristics of PFO-related stroke with different amounts of right-to-left shunt. Brain Behav. (2018) 8:e01122. doi: 10.1002/brb3.1122
20. Hayashida K, Fukuchi K, Inubushi M, Fukushima K, Imakita S, Kimura K. Embolic distribution through patent foramen ovale demonstrated by (99m)Tc-MAA brain SPECT after Valsalva radionuclide venography. J Nucl Med. (2001) 42:859–63.
21. Finsterer J, Sommer O, Stiskal M, Stollberger C, Baumgartner H. Closure of a patent foramen ovale: effective therapy of migraine and occipital stroke. Int J Neurosci. (2005) 115:119–27. doi: 10.1080/00207450490512687
22. Caputi L, Usai S, Carriero MR, Grazzi L, D'Amico D, Falcone C, et al. Microembolic air load during contrast-transcranial Doppler: a trigger for migraine with aura? Headache. (2010) 50:1320–7. doi: 10.1111/j.1526-4610.2010.01621.x
23. Liboni W, Molinari F, Allais GB, Mana O, Negri E, D'Andrea G, et al. Patent foramen ovale detected by near-infrared spectroscopy in patients suffering from migraine with aura. Neurol Sci. (2008) 29(Suppl.1):S182–5. doi: 10.1007/s10072-008-0920-7
24. Wilmshurst PT, Pearson MJ, Nightingale S, Walsh KP, Morrison WL. Inheritance of persistent foramen ovale and atrial septal defects and the relation to familial migraine with aura. Heart. (2004) 90:1315–20. doi: 10.1136/hrt.2003.025700
25. Merikangas KR. Contributions of epidemiology to our understanding of migraine. Headache. (2013) 53:230–46. doi: 10.1111/head.12038
26. Anzola GP, Magoni M, Guindani M, Rozzini L, Dalla Volta G. Potential source of cerebral embolism in migraine with aura: a transcranial Doppler study. Neurology. (1999) 52:1622–5. doi: 10.1212/WNL.52.8.1622
27. Schwedt TJ, Demaerschalk BM, Dodick DW. Patent foramen ovale and migraine: a quantitative systematic review. Cephalalgia. (2008) 28:531–40. doi: 10.1111/j.1468-2982.2008.01554.x
28. Marchione P, Ghiotto N, Sances G, Guaschino E, Bosone D, Nappi G, et al. Clinical implications of patent foramen ovale in migraine with aura. Funct Neurol. (2008) 23:201–5.
29. Caputi L, D'Amico D, Usai S, Grazzi L, Parati EA, Bussone G. Prevalence and characteristics of right-to-left shunt in migraine with aura: a survey on 120 Italian patients. Neurol Sci. (2009) 30(Suppl.1):S109–11. doi: 10.1007/s10072-009-0064-4
30. Carod-Artal FJ, da Silveira Ribeiro L, Braga H, Kummer W, Mesquita HM, Vargas AP. Prevalence of patent foramen ovale in migraine patients with and without aura compared with stroke patients. A transcranial Doppler study. Cephalalgia. (2006) 26:934–9. doi: 10.1111/j.1468-2982.2006.01156.x
31. Dalla Volta G, Guindani M, Zavarise P, Griffini S, Pezzini A, Padovani A. Prevalence of patent foramen ovale in a large series of patients with migraine with aura, migraine without aura and cluster headache, and relationship with clinical phenotype. J Headache Pain. (2005) 6:328–30. doi: 10.1007/s10194-005-0223-9
32. Khessali H, Mojadidi MK, Gevorgyan R, Levinson R, Tobis J. The effect of patent foramen ovale closure on visual aura without headache or typical aura with migraine headache. JACC Cardiovasc Interv. (2012) 5:682–7. doi: 10.1016/j.jcin.2012.03.013
33. Bigal ME, Serrano D, Reed M, Lipton RB. Chronic migraine in the population: burden, diagnosis, and satisfaction with treatment. Neurology. (2008) 71:559–66. doi: 10.1212/01.wnl.0000323925.29520.e7
34. Scher AI, Stewart WF, Liberman J, Lipton RB. Prevalence of frequent headache in a population sample. Headache. (1998) 38:497–506. doi: 10.1046/j.1526-4610.1998.3807497.x
35. Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders 3rd edition. Cephalalgia. (2018) 38:1–211. doi: 10.1177/0333102417738202
36. Nahas SJ, Young WB, Terry R, Kim A, Van Dell T, Guarino AJ, et al. Right-to-left shunt is common in chronic migraine. Cephalalgia. (2010) 30:535–42. doi: 10.1111/j.1468-2982.2009.02002.x
37. Kijima Y, Miller N, Noureddin N, Gevorgyan R, Tobis J. TCT-738 The Degree of Right-to-Left Shunt is Associated with Visual Aura Due to Migraine. J Am College Cardiol. (2015) 66:B301. doi: 10.1016/j.jacc.2015.08.761
38. Anzola GP, Meneghetti G, Zanferrari C, Adami A, Dinia L, Del Sette M, et al. Is migraine associated with right-to-left shunt a separate disease? Results of the SAM study. Cephalalgia. (2008) 28:360–6. doi: 10.1111/j.1468-2982.2008.01539.x
39. He Q, Zhang Y, Wang F, Li C, Guo R, Li X, et al. Impact of right-to-left shunt and transcatheter closure on the clinical features of migraine. Int J Neurosci. (2020) 130:270–5. doi: 10.1080/00207454.2019.1672681
40. Fukuoka T, Dembo T, Nagoya H, Kato Y, Yasuko O, Deguchi I, et al. Factors related to recurrence of paradoxical cerebral embolism due to patent foramen ovale. J Neurol. (2012) 259:1051–5. doi: 10.1007/s00415-011-6297-1
41. Freeman JA, Woods TD. Use of saline contrast echo timing to distinguish intracardiac and extracardiac shunts: failure of the 3- to 5-beat rule. Echocardiography. (2008) 25:1127–30. doi: 10.1111/j.1540-8175.2008.00741.x
42. Shub C, Tajik AJ, Seward JB, Dines DE. Detecting intrapulmonary right-to-left shunt with contrast echocardiography. Observations in a patient with diffuse pulmonary arteriovenous fistulas. Mayo Clin Proc. (1976) 51:81–4.
43. Telman G, Yalonetsky S, Kouperberg E, Sprecher E, Lorber A, Yarnitsky D. Size of PFO and amount of microembolic signals in patients with ischaemic stroke or TIA. Eur J Neurol. (2008) 15:969–72. doi: 10.1111/j.1468-1331.2008.02232.x
44. Snijder RJ, Luermans JG, de Heij AH, Thijs V, Schonewille WJ, Van De Bruaene A, et al. Patent foramen ovale with atrial septal aneurysm is strongly associated with migraine with aura: a large observational study. J Am Heart Assoc. (2016) 5:3771. doi: 10.1161/JAHA.116.003771
45. Anzola GP, Morandi E, Casilli F, Onorato E. Different degrees of right-to-left shunting predict migraine and stroke: data from 420 patients. Neurology. (2006) 66:765–7. doi: 10.1212/01.wnl.0000201271.75157.5a
46. Mazzucco S, Li L, Binney L, Rothwell PM. Prevalence of patent foramen ovale in cryptogenic transient ischaemic attack and non-disabling stroke at older ages: a population-based study, systematic review, and meta-analysis. Lancet Neurol. (2018) 17:609–17. doi: 10.1016/S1474-4422(18)30167-4
47. Consoli D, Paciaroni M, Galati F, Aguggia M, Melis M, Malferrari G, et al. Prevalence of patent foramen ovale in ischaemic stroke in Italy: results of SISIFO study. Cerebrovasc Dis. (2015) 39:162–9. doi: 10.1159/000375152
48. Giannandrea D, Padiglioni C, Eusebi P, Mengoni A, Romoli M, Galati F, et al. Clinical RoPE (cRoPE) score predicts patent foramen ovale detection among stroke patients: a multicenter observational study. Neurol Sci. (2020) 41:3227–33. doi: 10.1007/s10072-020-04386-6
49. Kent DM, Ruthazer R, Weimar C, Mas JL, Serena J, Homma S, et al. An index to identify stroke-related vs incidental patent foramen ovale in cryptogenic stroke. Neurology. (2013) 81:619–25. doi: 10.1212/WNL.0b013e3182a08d59
50. Di Tullio MR, Sacco RL, Sciacca RR, Jin Z, Homma S. Patent foramen ovale and the risk of ischemic stroke in a multiethnic population. J Am Coll Cardiol. (2007) 49:797–802. doi: 10.1016/j.jacc.2006.08.063
51. Handke M, Harloff A, Olschewski M, Hetzel A, Geibel A. Patent foramen ovale and cryptogenic stroke in older patients. N Engl J Med. (2007) 357:2262–8. doi: 10.1056/NEJMoa071422
52. Overell JR, Bone I, Lees KR. Interatrial septal abnormalities and stroke: a meta-analysis of case-control studies. Neurology. (2000) 55:1172–9. doi: 10.1212/WNL.55.8.1172
53. Romoli M, Giannandrea D, Eusebi P, Cupini LM, Ricci S, Calabresi P. Aspirin or anticoagulation after cryptogenic stroke with patent foramen ovale: systematic review and meta-analysis of randomized controlled trials. Neurol Sci. (2020) 41:2819–24. doi: 10.1007/s10072-020-04388-4
54. Sagris D, Georgiopoulos G, Perlepe K, Pateras K, Korompoki E, Makaritsis K, et al. Antithrombotic treatment in cryptogenic stroke patients with patent foramen ovale: systematic review and meta-analysis. Stroke. (2019) 50:3135–40. doi: 10.1161/STROKEAHA.119.026512
55. Vidale S, Russo F, Campana C, Agostoni E. Patent foramen ovale closure versus medical therapy in cryptogenic strokes and transient ischemic attacks: a meta-analysis of randomized trials. Angiology. (2019) 70:325–31. doi: 10.1177/0003319718802635
56. Lamy C, Giannesini C, Zuber M, Arquizan C, Meder JF, Trystram D, et al. Clinical and imaging findings in cryptogenic stroke patients with and without patent foramen ovale: the PFO-ASA study. Atrial Septal Aneurysm. Stroke. (2002) 33:706–11. doi: 10.1161/hs0302.104543
57. Knirsch W, Dodge-Khatami A, Valsangiacomo-Buechel E, Weiss M, Berger F. Challenges encountered during closure of atrial septal defects. Pediatr Cardiol. (2005) 26:147–53. doi: 10.1007/s00246-004-0958-0
58. Anderson RH, Brown NA. The anatomy of the heart revisited. Anat Rec. (1996) 246:1–7. doi: 10.1002/(SICI)1097-0185(199609)246:1<1::AID-AR1>3.0.CO;2-Y
59. Kilner PJ, Yang GZ, Wilkes AJ, Mohiaddin RH, Firmin DN, Yacoub MH. Asymmetric redirection of flow through the heart. Nature. (2000) 404:759–61. doi: 10.1038/35008075
60. Loukas M, Sullivan A, Tubbs RS, Weinhaus AJ, Derderian T, Hanna M. Chiari's network: review of the literature. Surg Radiol Anat. (2010) 32:895–901. doi: 10.1007/s00276-010-0639-z
61. Schneider B, Hofmann T, Justen MH, Meinertz T. Chiari's network: normal anatomic variant or risk factor for arterial embolic events? J Am Coll Cardiol. (1995) 26:203–10. doi: 10.1016/0735-1097(95)00144-O
62. Schuchlenz HW, Saurer G, Weihs W, Rehak P. Persisting eustachian valve in adults: relation to patent foramen ovale and cerebrovascular events. J Am Soc Echocardiogr. (2004) 17:231–3. doi: 10.1016/j.echo.2003.12.003
63. Rigatelli G, Dell'avvocata F, Cardaioli P, Giordan M, Braggion G, Aggio S, et al. Migraine-patent foramen ovale connection: role of prominent eustachian valve and large Chiari network in migrainous patients. Am J Med Sci. (2008) 336:458–61. doi: 10.1097/MAJ.0b013e31816e189d
64. Bridges ND, Hellenbrand W, Latson L, Filiano J, Newburger JW, Lock JE. Transcatheter closure of patent foramen ovale after presumed paradoxical embolism. Circulation. (1992) 86:1902–8. doi: 10.1161/01.CIR.86.6.1902
65. Wilmshurst PT, Nightingale S, Walsh KP, Morrison WL. Effect on migraine of closure of cardiac right-to-left shunts to prevent recurrence of decompression illness or stroke or for haemodynamic reasons. Lancet. (2000) 356:1648–51. doi: 10.1016/S0140-6736(00)03160-3
66. Morandi E, Anzola GP, Angeli S, Melzi G, Onorato E. Transcatheter closure of patent foramen ovale: a new migraine treatment? J Interv Cardiol. (2003) 16:39–42. doi: 10.1046/j.1540-8183.2003.08001.x
67. Schwerzmann M, Wiher S, Nedeltchev K, Mattle HP, Wahl A, Seiler C, et al. Percutaneous closure of patent foramen ovale reduces the frequency of migraine attacks. Neurology. (2004) 62:1399–401. doi: 10.1212/01.WNL.0000120677.64217.A9
68. Azarbal B, Tobis J, Suh W, Chan V, Dao C, Gaster R. Association of interatrial shunts and migraine headaches: impact of transcatheter closure. J Am Coll Cardiol. (2005) 45:489–92. doi: 10.1016/j.jacc.2004.09.075
69. Ferrarini G, Malferrari G, Zucco R, Gaddi O, Norina M, Pini LA. High prevalence of patent foramen ovale in migraine with aura. J Headache Pain. (2005) 6:71–6. doi: 10.1007/s10194-005-0154-5
70. Mortelmans K, Post M, Thijs V, Herroelen L, Budts W. The influence of percutaneous atrial septal defect closure on the occurrence of migraine. Eur Heart J. (2005) 26:1533–7. doi: 10.1093/eurheartj/ehi170
71. Reisman M, Christofferson RD, Jesurum J, Olsen JV, Spencer MP, Krabill KA, et al. Migraine headache relief after transcatheter closure of patent foramen ovale. J Am Coll Cardiol. (2005) 45:493–5. doi: 10.1016/j.jacc.2004.10.055
72. Giardini A, Donti A, Formigari R, Salomone L, Palareti G, Guidetti D, et al. Long-term efficacy of transcatheter patent foramen ovale closure on migraine headache with aura and recurrent stroke. Catheter Cardiovasc Interv. (2006) 67:625–9. doi: 10.1002/ccd.20699
73. Giardini A, Donti A, Formigari R, Salomone L, Prandstraller D, Bonvicini M, et al. Transcatheter patent foramen ovale closure mitigates aura migraine headaches abolishing spontaneous right-to-left shunting. Am Heart J. (2006) 151:922 e1–5. doi: 10.1016/j.ahj.2005.09.019
74. Dubiel M, Bruch L, Schmehl I, Liebner M, Winkelmann A, Stretz A, et al. Migraine headache relief after percutaneous transcatheter closure of interatrial communications. J Interv Cardiol. (2008) 21:32–7. doi: 10.1111/j.1540-8183.2007.00316.x
75. Jesurum JT, Fuller CJ, Kim CJ, Krabill KA, Spencer MP, Olsen JV, et al. Frequency of migraine headache relief following patent foramen ovale “closure” despite residual right-to-left shunt. Am J Cardiol. (2008) 102:916–20. doi: 10.1016/j.amjcard.2008.05.035
76. Luermans JG, Post MC, Temmerman F, Thijs V, Schonewille WJ, Plokker HW, et al. Closure of a patent foramen ovale is associated with a decrease in prevalence of migraine: a prospective observational study. Acta Cardiol. (2008) 63:571–7. doi: 10.2143/AC.63.5.2033223
77. Chessa M, Colombo C, Butera G, Negura D, Piazza L, Varotto L, et al. Is it too early to recommend patent foramen ovale closure for all patients who suffer from migraine? A single-centre study. J Cardiovasc Med. (2009) 10:401–5. doi: 10.2459/JCM.0b013e328329caf5
78. Papa M, Gaspardone A, Fragasso G, Ajello S, Gioffre G, Iamele M, et al. Usefulness of transcatheter patent foramen ovale closure in migraineurs with moderate to large right-to-left shunt and instrumental evidence of cerebrovascular damage. Am J Cardiol. (2009) 104:434–9. doi: 10.1016/j.amjcard.2009.03.061
79. Wahl A, Praz F, Findling O, Nedeltchev K, Schwerzmann M, Tai T, et al. Percutaneous closure of patent foramen ovale for migraine headaches refractory to medical treatment. Catheter Cardiovasc Interv. (2009) 74:124–9. doi: 10.1002/ccd.21921
80. Rigatelli G, Cardaioli P, Dell'Avvocata F, Giordan M, Braggion G, Chinaglia M, et al. Transcatheter patent foramen ovale closure is effective in reducing migraine independently from specific interatrial septum anatomy and closure devices design. Cardiovasc Revasc Med. (2010) 11:29–33. doi: 10.1016/j.carrev.2008.04.002
81. Wahl A, Praz F, Tai T, Findling O, Walpoth N, Nedeltchev K, et al. Improvement of migraine headaches after percutaneous closure of patent foramen ovale for secondary prevention of paradoxical embolism. Heart. (2010) 96:967–73. doi: 10.1136/hrt.2009.181156
82. Trabattoni D, Fabbiocchi F, Montorsi P, Galli S, Teruzzi G, Grancini L, et al. Sustained long-term benefit of patent foramen ovale closure on migraine. Catheter Cardiovasc Interv. (2011) 77:570–4. doi: 10.1002/ccd.22826
83. Rigatelli G, Dell'avvocata F, Cardaioli P, Giordan M, Braggion G, Aggio S, et al. Improving migraine by means of primary transcatheter patent foramen ovale closure: long-term follow-up. Am J Cardiovasc Dis. (2012) 2:89–95.
84. Araszkiewicz A, Grygier M, Iwanczyk S, Trojnarska O, Lesiak M, Grajek S. Long-term follow-up after percutaneous closure of patent foramen ovale with Amplatzer PFO Occluder: a single center experience. Postepy Kardiol Interwencyjnej. (2016) 12:49–54. doi: 10.5114/pwki.2016.56949
85. Milev I, Zafirovska P, Zimbakov Z, Idrizi S, Ampova-Sokolov V, Gorgieva E, et al. Transcatheter closure of patent foramen ovale: a single center experience. Open Access Maced J Med Sci. (2016) 4:613–8. doi: 10.3889/oamjms.2016.113
86. Kimmelstiel C, Gange C, Thaler D. Is patent foramen ovale closure effective in reducing migraine symptoms? A controlled study. Catheter Cardiovasc Interv. (2007) 69:740–6. doi: 10.1002/ccd.21025
87. Vigna C, Marchese N, Inchingolo V, Giannatempo GM, Pacilli MA, Di Viesti P, et al. Improvement of migraine after patent foramen ovale percutaneous closure in patients with subclinical brain lesions: a case-control study. JACC Cardiovasc Interv. (2009) 2:107–13. doi: 10.1016/j.jcin.2008.10.011
88. Rigatelli G, Dell'Avvocata F, Ronco F, Cardaioli P, Giordan M, Braggion G, et al. Primary transcatheter patent foramen ovale closure is effective in improving migraine in patients with high-risk anatomic and functional characteristics for paradoxical embolism. JACC Cardiovasc Interv. (2010) 3:282–7. doi: 10.1016/j.jcin.2009.11.019
89. Biasco L, Infantino V, Orzan F, Vicentini S, Rovera C, Longo G, et al. Impact of transcatheter closure of patent foramen ovale in the evolution of migraine and role of residual shunt. J Cardiol. (2014) 64:390–4. doi: 10.1016/j.jjcc.2014.02.023
90. Xing YQ, Guo YZ, Gao YS, Guo ZN, Niu PP, Yang Y. Effectiveness and safety of transcatheter patent foramen ovale closure for migraine (EASTFORM) trial. Sci Rep. (2016) 6:39081. doi: 10.1038/srep39081
91. He YD, Yan XL, Qin C, Zhang P, Guo ZN, Yang Y. Transcatheter patent foramen ovale closure is effective in alleviating migraine in a 5-year follow-up. Front Neurol. (2019) 10:1224. doi: 10.3389/fneur.2019.01224
92. Dowson A, Mullen MJ, Peatfield R, Muir K, Khan AA, Wells C, et al. Migraine Intervention With STARFlex Technology (MIST) trial: a prospective, multicenter, double-blind, sham-controlled trial to evaluate the effectiveness of patent foramen ovale closure with STARFlex septal repair implant to resolve refractory migraine headache. Circulation. (2008) 117:1397–404. doi: 10.1161/CIRCULATIONAHA.107.727271
93. Mattle HP, Evers S, Hildick-Smith D, Becker WJ, Baumgartner H, Chataway J, et al. Percutaneous closure of patent foramen ovale in migraine with aura, a randomized controlled trial. Eur Heart J. (2016) 37:2029–36. doi: 10.1093/eurheartj/ehw027
94. Tobis JM, Charles A, Silberstein SD, Sorensen S, Maini B, Horwitz PA, et al. Percutaneous closure of patent foramen ovale in patients with migraine: the PREMIUM trial. J Am Coll Cardiol. (2017) 70:2766–74. doi: 10.1016/j.jacc.2017.09.1105
95. Rodes-Cabau J, Horlick E, Ibrahim R, Cheema AN, Labinaz M, Nadeem N, et al. Effect of clopidogrel and aspirin vs aspirin alone on migraine headaches after transcatheter atrial septal defect closure: the CANOA randomized clinical trial. JAMA. (2015) 314:2147–54. doi: 10.1001/jama.2015.13919
96. Spencer BT, Qureshi Y, Sommer RJ. A retrospective review of clopidogrel as primary therapy for migraineurs with right to left shunt lesions. Cephalalgia. (2014) 34:933–7. doi: 10.1177/0333102414523845
97. Sommer RJ, Nazif T, Privitera L, Robbins BT. Retrospective review of thienopyridine therapy in migraineurs with patent foramen ovale. Neurology. (2018) 91:1002–9. doi: 10.1212/WNL.0000000000006572
98. Reisman AM, Robbins BT, Chou DE, Yugrakh MS, Gross GJ, Privitera L, et al. Ticagrelor for Refractory Migraine/Patent Foramen Ovale (TRACTOR): an open-label pilot study. Neurology. (2018) 91:1010–7. doi: 10.1212/WNL.0000000000006573
99. Steiner TJ, Jensen R, Katsarava Z, Linde M, MacGregor EA, Osipova V, et al. Aids to management of headache disorders in primary care (2nd edition): on behalf of the European Headache Federation and Lifting The Burden: the Global Campaign against Headache. J Headache Pain. (2019) 20:57. doi: 10.1186/s10194-018-0899-2
Keywords: migraine, patent foramen ovale, prevalence, patent foramen ovale closure, systematic review
Citation: Liu K, Wang BZ, Hao Y, Song S and Pan M (2020) The Correlation Between Migraine and Patent Foramen Ovale. Front. Neurol. 11:543485. doi: 10.3389/fneur.2020.543485
Received: 17 March 2020; Accepted: 28 September 2020;
Published: 01 December 2020.
Edited by:
Linxin Li, University of Oxford, United KingdomReviewed by:
Michele Romoli, University of Perugia, ItalyCopyright © 2020 Liu, Wang, Hao, Song and Pan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mengxiong Pan, cGFubXg5MTgyQDE2My5jb20=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.