 Anna C. Alegiani
Anna C. Alegiani Anne C. Rahn
Anne C. Rahn Anke Steckelberg4
Anke Steckelberg4 Götz Thomalla
Götz Thomalla Christoph Heesen
Christoph Heesen Sascha Köpke
Sascha Köpke
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Neurol. , 07 December 2020
Sec. Stroke
Volume 11 - 2020 | https://doi.org/10.3389/fneur.2020.526515
Background: Strokes have a huge impact on patients' quality of life. Although there are potentially effective secondary preventions and treatment options for stroke patients, adherence is mostly low. Low disease and treatment-related knowledge and, consequently, a lack of informed decision-making in stroke patients may contribute to this problem. However, stroke patient information did not seem to have relevant effects on patients' knowledge in randomized controlled trials. One contributing factor may be the lack of thoroughly developed patient information materials.
Methods: We aimed to evaluate the quality of patient information materials for stroke patients by using randomized controlled trials, applying quality criteria for evidence-based patient information (EBPI). We conducted a literature search (MEDLINE, Embase, CINAHL, PsycINFO, and CENTRAL). To be included in the review, research had to be randomized controlled trials that provided stroke patient information, were published in English, and had knowledge assessed as the primary endpoint. Authors of primary studies were contacted and asked for information materials applied.
Results: We screened 15,507 hits and identified 30 eligible studies. Information materials were available for only eight studies. Analyses revealed that all available materials had important shortcomings concerning EBPI quality criteria [concerning, for example, structural information (e.g., reporting conflicts of interest), content information (e.g., reporting sources of information), or comprehensive descriptions of treatment effects and side effects]. Frequently, treatment effects were reported only narratively without providing absolute numbers, values, or frequencies.
Conclusion: Quality of materials differed, but none sufficiently fulfilled EBPI quality criteria. Unsatisfactory trial results concerning patient knowledge and patient involvement in decision-making may at least partially be explained by limitations of the provided materials. Future patient information should consider EBPI quality criteria.
Stroke is the leading cause of disability worldwide and affects quality of life (1). Despite increasing evidence for effective stroke prevention and treatment of stroke risk factors (2), stroke incidence and prevalence remain high (3). Efforts should focus on prevention and especially on secondary prevention, i.e., the prevention of further strokes in stroke patients.
Cardiovascular risk factors are a central target for stroke prevention approaches, but knowledge on risk factors in stroke patients is insufficient (4) and has not changed in recent years (5). Additionally, patients with increased stroke risk and stroke patients are often unaware of their risk status (5, 6). As a result, stroke patients may not engage in required preventive behaviors, e.g., blood pressure control, lifestyle modification, or medication intake for secondary prevention (7, 8).
Adherence to medical advice for secondary stroke prevention is poor, with one-quarter of stroke patients discontinuing prescribed medications 3 months after hospital discharge (9). A systematic review and meta-analysis of prospective epidemiological studies revealed that among cardiovascular diseases (CVD), including stroke, a substantial proportion of patients do not adhere adequately to cardiovascular medications. Approximately nine percent of all CVD events in Europe can be attributed to poor medication adherence (10).
Patients in different countries and settings claim multiple unmet educational needs concerning knowledge about the clinical aspects of stroke prevention and treatment (11). Overall stroke knowledge, as well as knowledge concerning secondary stroke prevention in patients with cerebrovascular diseases, is low to moderate (12).
Stroke patients want to be involved in treatment decisions and prefer an informed choice model of decision making (12). The use of decision aids may lead to informed choices and positively influence health behavior, by providing information on treatment options and supporting value clarification (13). Evidence-based patient information (EBPI) is an important part of decision aids. EBPI is based on systematic synthesis of the literature and communication of treatment effects using numerical data, presented in an understandable format (14). EBPI improves knowledge and increases satisfaction with the decision processes (14, 15). EBPI quality criteria defines how information should be presented (14) to allow for shared decision-making (15).
High-quality information constitutes the basis for shared decision-making, showing substantial potential to improve care (16–19). Consequently, increased patient involvement in decision-making may lead to behavioral changes, as we have shown in neurological patients with multiple sclerosis (20, 21).
In 2012, a Cochrane review analyzed the effectiveness of stroke patient information interventions (22). In total, 21 studies were included, covering a wide range of information materials (e.g., stickers, leaflets, booklets, videos, and audiotapes) from different sources (e.g., neurologists, pharmaceutical companies, and patient support groups). The review showed evidence that interventions addressing information provision can improve stroke knowledge. Actively involving patients may accelerate this effect (22).
Based on the Cochrane review, this study aims to analyze the quality of information materials for stroke patients tested in randomized-controlled trials (RCTs) by applying EBPI quality criteria (14).
We updated the outdated search of the Cochrane review (22) that included RCTs, comparing information interventions with standard care, and used patient or carer knowledge as the primary outcome. We followed the search strategy of the Cochrane review and conducted searches in the following databases:
• Ovid MEDLINE and Epub Ahead of Print, In-Process & Other Non-Indexed Citations, Daily and Versions 1946 to July 2020
• Embase 1980 to July 2020
• CINAHL EBSCO from 1982 to July 2020
• PsycINFO 1806 to July 2020
• CENTRAL Issue 9 of 12, July 2020.
Titles and abstracts were reviewed by seven researchers and irrelevant studies were excluded. Full texts of the remaining studies were checked concerning the following inclusion criteria: randomized controlled trial, provision of stroke patient information for stroke patients, published in English, and knowledge assessed as the primary endpoint. Following the Cochrane review, we excluded trials in which information provision was only one component of a complex intervention. We initially aimed to focus on information materials addressing secondary stroke prevention only, which led to a small number of information materials. Therefore, we decided to evaluate all available materials addressing stroke patients. The software Rayyan (https://rayyan.qcri.org/) was used for study selection.
We added the results of our literature search to the studies included in the Cochrane review. We contacted authors of all studies, preferably via email, for a minimum of three times. If the first author was not available, senior authors or co-authors were approached. All authors were asked for information materials used and for consent to review these materials regarding EBPI criteria. Available information materials were analyzed using EBPI quality criteria (14) (for details see Table 1). We used a standardized data extraction sheet based on the item list (Table 1). Each quality item was rated as follows: 3 (yes/ complete/ good), 2 (in part/ incomplete/ satisfactory), or 1 (no/ unsatisfactory).
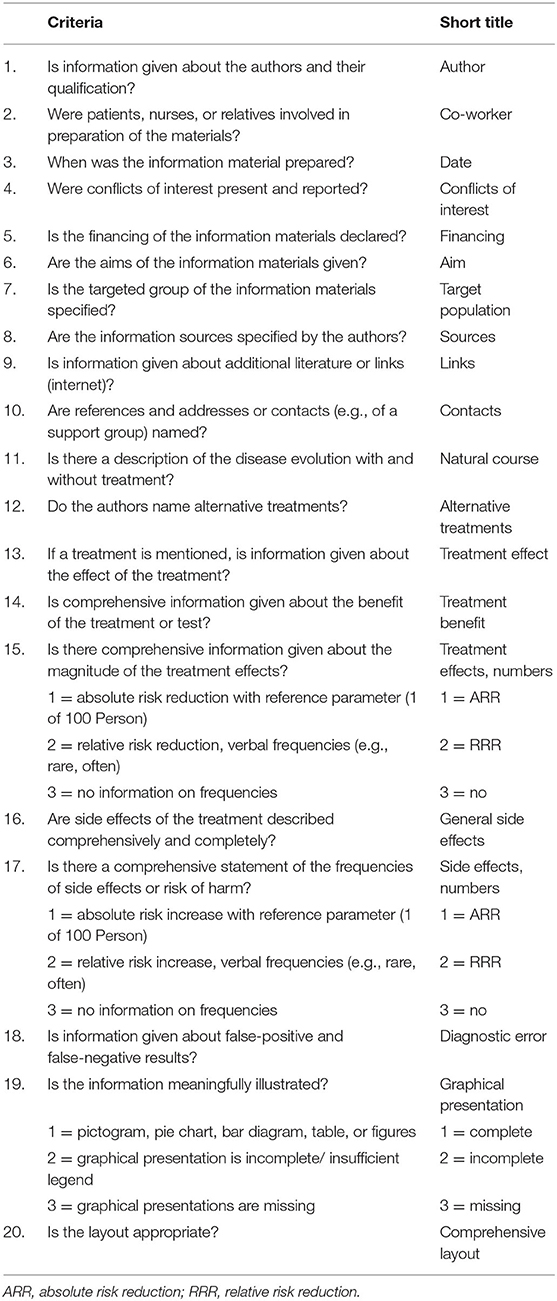
Table 1. Checklist of EBPI quality criteria (14).
The search resulted in 15,193 citations without duplicates. 15,181 citations were excluded after title and abstract screening. In total, 12 full-text articles were assessed and nine studies were included (Figure 1). Those were added to the 21 studies already included in the Cochrane review. We contacted the authors of all 30 studies and received 16 replies. For 14 studies, authors could not be contacted (24–37). Of these, one study was excluded because materials were in Chinese (38). One study consisted of a multicomponent intervention, which we noticed after receiving the materials, and was therefore excluded (39). The remaining six authors were not able to send the materials, because they were not available anymore (40–45). Finally, eight (27%) studies provided materials that could be analyzed (Table 2).
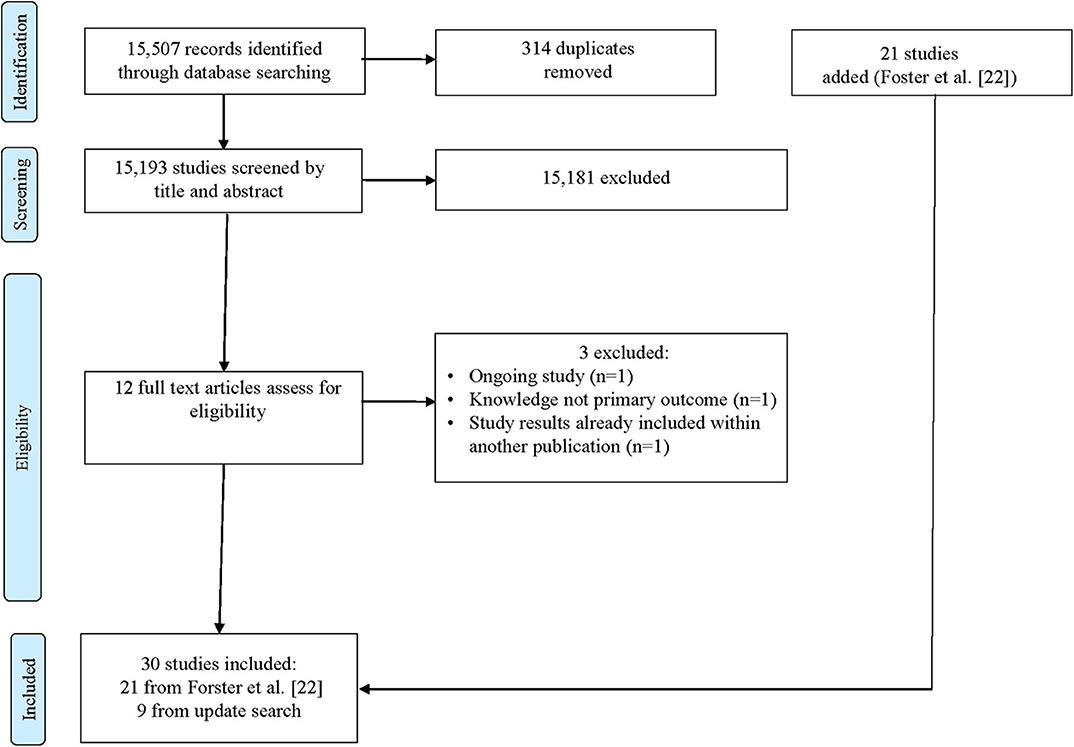
Figure 1. The flow diagram of the study selection following the PRISMA Guidelines (23). Identification shows the results of the updated systematic literature search following the Cochrane Review search strategy (22).
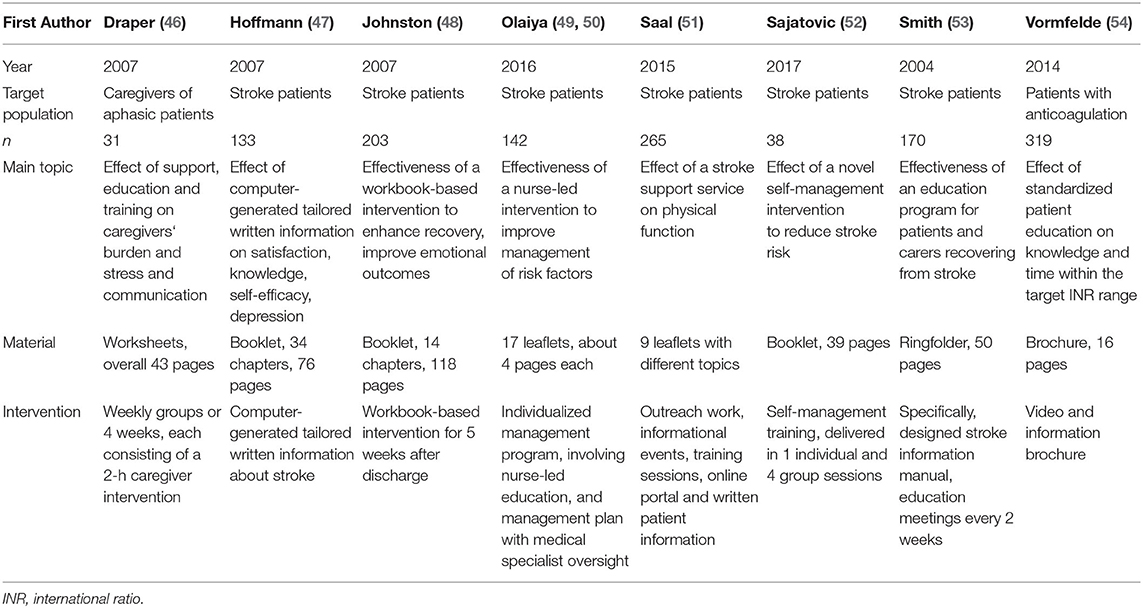
Table 2. Assessment of information materials using criteria of evidence-based patient information (15).
In the following, a short description of included studies is provided, sorted by the type of intervention.
Draper et al. (46), Vormfelde et al. (54), Saal et al. (51), and Olaiya et al. (49) studied educational programs. Draper et al. (46) conducted an RCT with a wait-list design in Australia. Participants received a weekly educational program with four subsequent sessions, showing short-term effects on stress levels. Vormfelde et al. (54) performed a cluster RCT including a 1-h patient education session on oral anticoagulation with Phenprocoumon that included a video, a questionnaire, and an information brochure in Germany. The control group received the information brochure only. The intervention was feasible and improved knowledge. Saal et al. (51) conducted a stroke support service for post-stroke outpatients in Germany. The post-discharge stroke support service included outreach work (via telephone contact and home-visit), informational events, training sessions, an online portal, and written patient information. The control group received optimized standard care by written patient information (51). The service did not improve physical function, health-related quality of life, depression, somatization, or re-infarcts, but results suggest a lower overall risk of mortality in the intervention group (51). Olaiya et al. (49) included patients of the STAND FIRM RCT (55) evaluating the effectiveness of the nurse education component of the intervention in Australia. The intervention group received an individualized management program, comprising a chronic disease management plan and two home visits by nurses to provide tailored education for secondary prevention. The control group received the usual care. The study did not find any evidence for better knowledge of secondary prevention medications in the intervention group compared to controls.
Two studies applied written information materials (47, 53). Hoffmann et al. (47) compared a computer-generated tailored written education package in Australia to generic written information. Results showed improved satisfaction with the stroke information, but the program did not affect knowledge, self-efficacy, depression, or perceived health status. Smith et al. (53) conducted an RCT in England. Patients and caregivers in the intervention group received a specifically designed stroke information manual applied in bi-weekly meetings compared to the usual practice in the control group. Results showed no statistical difference in knowledge.
Finally, Johnston et al. (48) and Sajatovic et al. (52) conducted self-management programs. Johnston et al. (48) performed an RCT in Scotland. Patients were allocated to a 5-week self-management intervention incorporating three information components and support and behavior change techniques after discharge or care as usual. The intervention group showed a better recovery compared to the control group. Sajatovic et al. (52) conducted a study assessing a self-management program to reduce secondary stroke risk in African-American men in the USA delivering a self-management training in one individual followed by group sessions over 3 months. Qualitative results suggested improved awareness of risk factors. For detailed data see Table 2.
Quality ratings regarding EBPI quality criteria (14) revealed heterogeneous and often unsatisfactory results. Structural information about financing, authors, and co-workers were frequently met, while information about conflicts of interest and sources of information were often missing. In terms of content information, information about alternative treatments, treatment effects, and the natural course of the disease were frequently met. Information on treatment effects in (absolute) numbers was given only once, while reporting of side effects in numbers was not present in any information material (Table 3). Three materials were scored as moderate quality (reached at least 60% of the quality score, i.e., ≥36 of max. 60 points) (47, 53, 54). The other five materials were scored as low quality (<36 points).
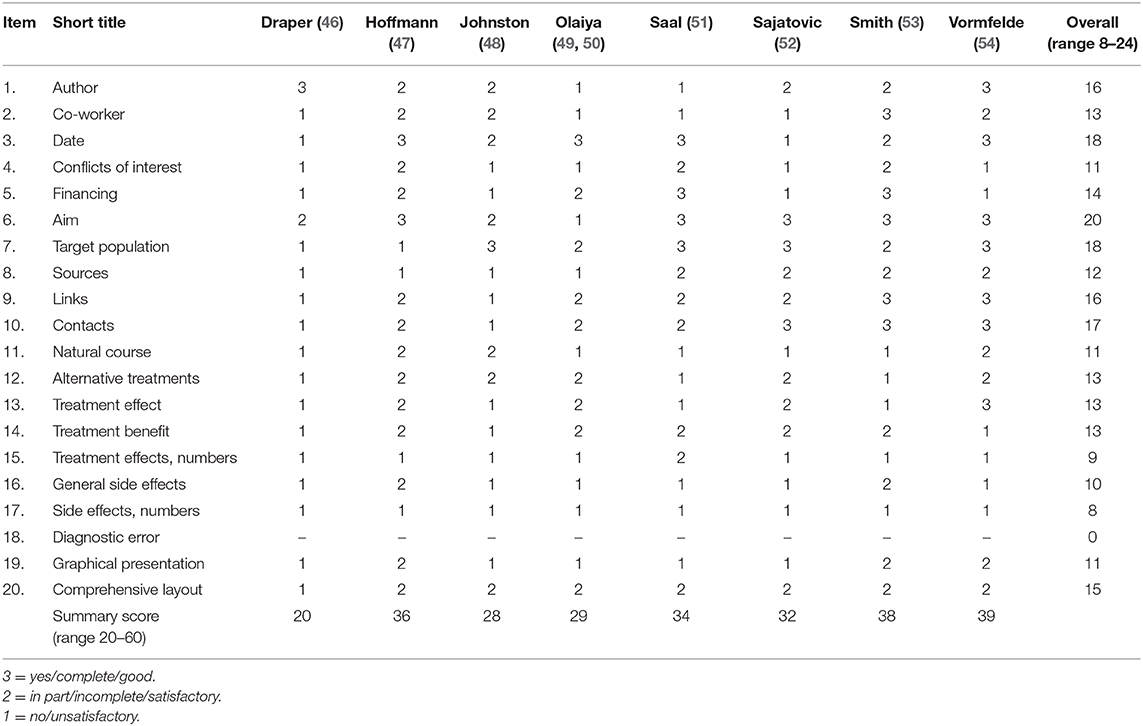
Table 3. Quality rating based on established quality criteria for evidence-based patient information (18).
This literature review aimed to evaluate the quality of information materials for stroke patients. We evaluated RCTs from a Cochrane review (22) and updated the search. Although 30 studies were identified, information materials were only available for eight studies. All studies were RCTs addressing interventions aiming to inform stroke patients, but most studies had important methodological weaknesses. Analyses of the information materials revealed a profound lack of quality when applying EBPI quality criteria (15).
Results show important shortcomings in the investigated materials, especially regarding information on the natural course of the disease, which is essential to understand the possible benefit of a treatment (15) and crucial for informed decision-making, individual risk perception, preferences and values, physician expertise, and counseling (13).
Importantly, presentation of (absolute) numbers, values, or frequencies was mostly missing e.g., concerning treatment benefits or side effects. As both patients and physicians have difficulties in understanding risk data (56), providing only verbal descriptions does not meet state of the art risk communication (57).
The Cochrane review by Forster et al. (22) concluded that the best way to provide information to stroke patients is still unclear, as results show no consistent effect on knowledge and health behavior (22), although multiple unmet needs of patients regarding information provision for stroke have been reported (11). Considering the small number of available intervention materials and the often poor quality of the analyzed materials, it is not justified to conclude that patient information for stroke patients is not effective. We found the quality of information materials to be limited in all categories applied. Although aspects of reporting were at least met in some information materials, aspects referring to transparent reporting of results of treatment effects were presented inadequately throughout. Therefore, future interventions should use materials that adhere to the quality criteria of EPBI in order to be helpful for patients in making informed choices and being involved in shared decision-making. Specific focus should be placed on issues allowing patients to make informed decisions. Therefore, reporting of treatment effects using absolute differences instead of relative risks, reporting natural disease courses, and using graphical presentations adapted to the target group are needed to enhance informed decisions. Also, interventions should be described in detail, for example by using the TIDieR criteria (58), and materials should be made available. This conclusion is not new. In 1979, Ley et al. proposed that the content and form of patient information materials significantly impact on their effectiveness (59).
It has been argued that EBPI may disturb patients by communicating scientific uncertainties using absolute risks (19). However, most patients appreciate this transparent approach (19) and the use of absolute risks is generally recommended (60). We have repeatedly shown in neurological patients with multiple sclerosis that patients can understand and handle complex and even uncertain information (20, 61). Also, recent findings demonstrate that stroke patients, without cognitive impairment and/or aphasia, want to be involved in treatment decision-making and are able to understand basic statistical data without relevant differences to healthy controls (12).
The main strengths of our review are the use of established criteria for EBPI and the systematic search for RCTs on patient information interventions based on a Cochrane review. As a limitation, we were unable to evaluate most information materials, as there was no feedback from authors or materials were not available. This means that there is a risk of an inadvertent selection bias. Authors of studies who did not reply and those that could not provide materials may have not responded due to poor quality of the materials, leading to an overestimation of the quality of information materials. Another limitation is that the included information materials had different targets and were based on different concepts and sources of evidence. Some studies focused on basic stroke knowledge, while others aimed to support psychological aspects of rehabilitation after stroke.
In conclusion, we were able to evaluate eight information materials for stroke patients already tested in randomized controlled trials. Although some materials were rated considerably better than others, overall, materials did not meet the criteria of high-quality EBPI and therefore might not meet patients' needs as they fail to provide adequate information. Unsatisfactory trial results concerning patient knowledge and patient involvement in decision-making may at least partially be explained by the limitations of the provided materials. Future patient information materials should consider EBPI quality criteria.
All datasets generated for this study are included in the article/supplementary material.
AA made substantial contributions to conception and design, acquisition of data, analysis and interpretation of data, and drafting the article. AR made substantial contributions to conception and design, acquisition of data and analysis, and critically revised the article for important intellectual content. AS made substantial contributions to conception and analysis, interpretation of data, and also revised the article critically for important intellectual content. GT made substantial contributions to analysis, interpretation of data, and revised the article critically for important intellectual content. CH made substantial contributions to conception and design, analysis and interpretation of data and also participated in drafting the article and revising the article critically for important intellectual content. SK made substantial contributions to conception and design, acquisition of data, analysis and interpretation of data and participated in drafting the article and revising the article critically for important intellectual content. All authors contributed to the article and approved the submitted version.
AA received a grant from the National Multiple Sclerosis Society, USA (Grant No. G-1508-06034).
AA received lecture fees from Bayer Vital. GT has received fees as a consultant or lecture fees from Acandis, Bayer Vital, Bristol-Myers Squibb/Pfizer, Boehringer Ingelheim, Daichii Sankyo, GlaxoSmithKline, and Stryker, and received a research grant from Bayer.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We would like to acknowledge the support of Anne Forster, Sara Joice, Ulla Hedegaard, Susanne Saal, Tammy Hoffmann, Marie Johnston, Brian Draper, Stefan Viktor Vormfelde, Janet Sit, Amanda G. Thrift, and Martha Sajatovic for providing their materials. Also, we appreciate the support of the Cochrane Stroke group, especially Joshua Cheyne (information specialist) and Peter Langhorne (coordinating editor).
1. Dennis M, O'Rourke S, Lewis S, Sharpe M, Warlow C. A quantitative study of the emotional outcome of people caring for stroke survivors. Stroke. (1998) 29:1867–72. doi: 10.1161/01.STR.29.9.1867
2. Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Borden WB, et al. Heart disease and stroke statistics 2013 update: a report from the American Heart Association. Circulation. (2013) 127:e6–245. doi: 10.1161/CIR.0b013e31828124ad
3. Feigin VL, Forouzanfar MH, Krishnamurthi R, Mensah GA, Connor M, Bennett DA, et al. Global and regional burden of stroke during 1990–2010:findings from the Global Burden of Disease Study 2010. Lancet. (2014) 383:245–54. doi: 10.1016/S0140-6736(13)61953-4
4. Müller-Nordhorn J, Nolte CH, Rossnagel K, Jungehülsing GJ, Reich A, Roll S, et al. Knowledge about risk factors for stroke: a population-based survey with 28,090 participants. Stroke. (2006) 37:946–50. doi: 10.1161/01.STR.0000209332.96513.82
5. Ellis C, Barley J, Grubaugh A. Poststroke knowledge and symptom awareness: a global issue for secondary stroke prevention. Cerebrovasc Dis. (2013) 35:572–81. doi: 10.1159/000351209
6. Samsa GP, Cohen SJ, Goldstein LB Bonito AJ, Duncan PW, Enarson C, et al. Knowledge of risk among patients at increased risk for stroke. Stroke. (1997) 28:916–21. doi: 10.1161/01.STR.28.5.916
7. Jones SP, Jenkinson AJ, Leathley MJ, Watkins CL. Stroke knowledge and awareness: an integrative review of the evidence. Age Ageing. (2010) 39:11–22. doi: 10.1093/ageing/afp196
8. Bushnell CD, Olson DM, Zhao X, Pan W, Zimmer LO, Goldstein LB, et al. Secondary preventive medication persistence and adherence 1 year after stroke. Neurology. (2011) 77:1182–90. doi: 10.1212/WNL.0b013e31822f0423
9. Bushnell CD, Zimmer LO, Pan W, Olson DM, Zhao X, Meteleva T, et al. Persistence with stroke prevention medications 3 months after hospitalization. Arch Neurol. (2010) 67:1456–63. doi: 10.1001/archneurol.2010.190
10. Chowdhury R, Khan H, Heydon E, Shroufi A, Fahimi S, Moore C, et al. Adherence to cardiovascular therapy: a meta-analysis of prevalence and clinical consequences. Eur Heart J. (2013) 34:2940–8. doi: 10.1093/eurheartj/eht295
11. Hafsteinsdóttir TB, Vergunst M, Lindeman E, Schuurmans M. Educational needs of patients with a stroke and their caregivers: a systematic review of the literature. Patient Educ Couns. (2011) 85:14–25. doi: 10.1016/j.pec.2010.07.046
12. Riechel C, Alegiani AC, Koepke S, Kaspar J, Rosenkranz M, Thomalla G, et al. Subjective and objective knowledge and decisional role preferences in cerebrovascular patients compared to controls. Patient Prefer Adherence. (2016) 10:1453–60. doi: 10.2147/PPA.S98342
13. Stacey D, Légaré F, Lewis K, Barry MJ, Bennett CL, Eden KB, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. (2017) 4:CD001431. doi: 10.1002/14651858.CD001431.pub5
14. Bunge M, Mühlhauser I, Steckelberg A. What constitutes evidence-based patient information? Overview of discussed criteria. Patient Educ Couns. (2010) 78:316–28. doi: 10.1016/j.pec.2009.10.029
15. Barratt A. Evidence based medicine and shared decision making: the challenge of getting both evidence and preferences into health care. Patient Educ Couns. (2008) 73:407–12. doi: 10.1016/j.pec.2008.07.054
16. Mulley AG, Trimble C, Elwyn E. Stop the silent misdiagnosis: patients' preferences matter. BMJ. (2012) 345:e6572. doi: 10.1136/bmj.e6572
17. Lee OE, Emanuel EJ. Shared decision making to improve care and reduce costs. N Engl J Med. (2013) 3:6–8. doi: 10.1056/NEJMp1209500
18. Patel SR, Bakken S, Ruland C. Recent advances in shared decision making for mental health. Curr Opin Psychiatry. (2008) 21:606–12. doi: 10.1097/YCO.0b013e32830eb6b4
19. Wilson SR, Strub P, Buist AS, Knowles SB, Lavori PW, Lapidus J, et al. Shared treatment decision making improves adherence and outcomes in poorly controlled asthma. Am J Respir Crit Care Med. (2010) 181:566–77. doi: 10.1164/rccm.200906-0907OC
20. Köpke S, Kasper J, Mühlhauser I, Nübling M, Heesen C. Patient education program to enhance decision autonomy in multiple sclerosis relapse management: a randomized-controlled trial. Mult Scler. (2009) 15:96–104. doi: 10.1177/1352458508095921
21. Köpke S, Solari A, Khan F, Heesen C, Giordano A. Information provision for people with multiple sclerosis. Cochrane Database Syst Rev. (2014) 4:CD008757. doi: 10.1002/14651858.CD008757.pub2
22. Forster A, Brown L, Smith J, House A, Knapp P, Wright JJ, et al. Information provision for stroke patients and their caregivers (Review). Cochrane Database Syst Rev. (2012) 11:CD001919. doi: 10.1002/14651858.CD001919.pub3
23. Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J Clin Epidemiol. (2009) 62:1006–12. doi: 10.1016/j.jclinepi.2009.06.005
24. Banet GA, Felchlia MA. The potential utility of a shared medicalrecord in a “first-time” stroke population. J Vasc Nurs. (1997) 15:29–33. doi: 10.1016/S1062-0303(97)90050-9
25. Chinchai P, Bunyamark T, Sirisatayawong P. Effects of caregivereducation in stroke rehabilitation on the quality of life of strokesurvivors. World Feder Occup Ther Bull. (2010) 61:56–63. doi: 10.1179/otb.2010.61.1.015
26. Chiu C-C, Wu S-S, Lee P-H, Huang Y-C, Tan T-Y, Chang K-C. Control of modifiable risk factors in ischemic stroke outpatients by pharmacist intervention: an equalal location stratified randomized study. J Clin Pharm Ther. (2008) 33:529–35. doi: 10.1111/j.1365-2710.2008.00940.x
27. Downes B, Rooney V, Roper-Hall A, Oyebode J, Main A, Mayer P. The effectiveness of counselling stroke survivors and their carers in the community. Age Ageing. (1993) 22:28–9. doi: 10.1093/ageing/22.suppl_3.P28-c
28. Evans RL, AL Bishop Stranahan S, Pederson C. Family intervention after stroke: does counseling or education help? Stroke. (1988) 19:1243–9. doi: 10.1161/01.STR.19.10.1243
29. Kaira L, Evans A, Perez I, Melbourn A, Patel A, Knapp M, et al. Training carers of stroke patients: randomised controlled trial. BMJ. (2004) 328:1099. doi: 10.1136/bmj.328.7448.1099
30. Frank G, Johnston M, Morrison V, Pollard B, MacWalter R. Perceived control and recovery from functional limitations: preliminary evaluation of a workbook-based intervention for discharged stroke patients. Br J Health Psychol. (2000) 5:413–20. doi: 10.1348/135910700169017
31. Lomer M, McLellan DL. Informing hospital patients and their relatives about stroke. Int J Rehabil Res. (1986) 9:103–4.
32. Lowe D, Sharma A, Leathley M. The CareFile project: a feasibility study to examine the effects of an individualised information booklet on patients after stroke. Age Ageing. (2007) 36:83–9 doi: 10.1093/ageing/afl145
33. Mant J, Carter J, Wade DT, Winner S. The impact of an information pack on patients with stroke and their carers: a randomized controlled trial. Clin Rehabil. (1998) 12:465–76. doi: 10.1191/026921598668972226
34. O'Connell B, Hawkins M, Botti M, Buchbinder R, Baker L. Providing information to stroke survivors: lessons from a failed randomised controlled trial. J Aust Rehabil Nurses Assoc. (2009) 12:4–6.
35. Pain HSB, McLellan DL. The use of individualised booklets after a stroke. Clin Rehabil. (1990) 4:265–72. doi: 10.1177/026921559000400403
36. Lakshmi R, James E, Kirthivasan R. Study on impact of clinical pharmacist's interventions in the optimal use of oral anticoagulants in stroke patients. Indian J Pharm Sci. (2013) 75:53–9. doi: 10.4103/0250-474X.113550
37. Cameron JI, Naglie G, Green TL, Gignac MA, Bayley M, Huijbregts M, et al. A feasibility and pilot randomized controlled trial of the “timing it right stroke family support program”. Clin Rehabil. (2015) 29:1129–40. doi: 10.1177/0269215514564897
38. Sit JW, Chair SY, Choi KC, Chan CW, Lee DT, Chan AW, et al. Do empowered stroke patients perform better at self-management and functional recovery after a stroke? A randomized controlled trial. Clin Interv Aging. (2016) 11:1441–50. doi: 10.2147/CIA.S109560
39. Hedegaard U, Kjeldsen LJ, Pottegård A, Bak S, Hallas J. Multifaceted intervention including motivational interviewing to support medication adherence after stroke/transient ischemic attack: a randomized trial. Cerebrovasc Dis Extra. (2014) 4:221–34. doi: 10.1159/000369380
40. Ellis G, Rodger J, McAlpine C, Langhorne P. The impact of stroke nurse specialist input on risk factor modification: a randomised controlled trial. Age Ageing. (2005) 34:389–92. doi: 10.1093/ageing/afi075
41. Johnson J, Pearson V, McDivitt L. Stroke rehabilitation: assessing stroke survivors' long-term learning needs. Rehabil Nurs. (1997) 22:243–8. doi: 10.1002/j.2048-7940.1997.tb02110.x
42. Larson J, Franzen-Dahlin A, Billing E, von Arbin M, Murray V, Wredling R. The impact of a nurse-led support and education programme for spouses of stroke patients: a randomised controlled trial. J Clin Nurs. (2005) 14:995–1003. doi: 10.1111/j.1365-2702.2005.01206.x
43. Maasland E, Koudstaal PJ, Habbema JDF, Dippel DWJ. Effects of an individualised multimedia computer programme for health education in patients with a recent minor stroke or transient ischemic attack - a randomized controlled trial. Actaneurol Scand. (2007) 115:41–8. doi: 10.1111/j.1600-0404.2006.00722.x
44. Rodgers H, Atkinson C, Bond S, Suddes M, Dobson R, Curless R. Randomized controlled trial of a comprehensive stroke education program for patients and caregivers. Stroke. (1999) 30:2585–91. doi: 10.1161/01.STR.30.12.2585
45. Sides EG, Zimmer LO, Wilson L, Pan W, Olson DM, Peterson ED, et al. Medication coaching program for patients with minor stroke or TIA: a pilot study. BMC Public Health. (2012) 12:549. doi: 10.1186/1471-2458-12-549
46. Draper B, Bowring G, Thompson C, Van Heyst J, Conroy P, Thompson J. Stress in caregivers of aphasic stroke: a randomized controlled trial. Clin Rehabil. (2007) 2:122–30. doi: 10.1177/0269215506071251
47. Hoffmann T, McKenna K, Worrall L, Read SJ. Randomised trial of a computer-generated tailored written education package for patients following stroke. Age Ageing. (2007) 36:280–6. doi: 10.1093/ageing/afm003
48. Johnston M, Bonetti D, Joice S, Pollard B, Morrison V, Francis JJ, et al. Recovery from disability after stroke as a target for a behavioural intervention: results of a randomized controlled trial. Disabil Rehabil. (2007) 30:1117–27. doi: 10.1080/03323310600950411
49. Olaiya MT, Cadilhac D, Kim J, Ung D, Nelson MR, Srikanth VK, et al. Nurse-led intervention to improve knowledge of medications in survivors of stroke or transient ischemic attack: a cluster randomized controlled trial. Front Neurol. (2016) 7:205. doi: 10.3389/fneur.2016.00205
50. Olaiya MT, Cadilhac DA, Kim J, Ung D, Nelson MR, Srikanth VK, et al. Effectiveness of an intervention to improve risk factor knowledge in patients with stroke: a randomized controlled trial. Stroke. (2017) 48:1101–3. doi: 10.1161/STROKEAHA.116.016229
51. Saal S, Becker C, Lorenz S, Schubert M, Kuss O, Stang A, et al. Effect of a stroke support service in Germany: a randomized trial. Topics Stroke Rehabil. (2015) 22:429–36. doi: 10.1179/1074935714Z.0000000047
52. Sajatovic M, Tatsuoka C, Welter E, Colon-Zimmermann K, Blixen C, Pezynski AT, et al. A targeted self-management approach for reducing stroke risk factors in african american men who have had a stroke or transient ischemic attack. Am J Health Promot. (2018) 32:282–93. doi: 10.1177/0890117117695218
53. Smith J, Forster A, Young J. A randomized trial to evaluate an education programme for patients and carers after stroke. Clin Rehabil. (2004) 18:726–36. doi: 10.1191/0269215504cr790oa
54. Vormfelde SV, Abu Abed M, Hua TD, Schneider S, Friede T, Chenot JF. Educating orally anticoagulated patients in drug safety: a cluster-randomized study in general practice. Dtsch Arztebl Int. (2014) 12:607–14. doi: 10.3238/arztebl.2014.0607
55. Thrift AG, Srikanth VK, Nelson MR, Kim J, Fitzgerald SM, Gerraty RP, et al. Risk factor management in survivors of stroke: a double-blind, cluster-randomized, controlled trial. Int J Stroke. (2014) 9:652–7. doi: 10.1111/j.1747-4949.2012.00933.x
56. Gaissmaier W, Wegwarth O, Skopec D, Müller AS, Broschinski S, Politi MC. Numbers can be worth a thousand pictures: individual differences in understanding graphical and numerical representations of health-related information. Health Psychol. (2012) 3:286–96. doi: 10.1037/a0024850
57. Trevena LJ, Zikmund-Fisher BJ, Edwards A, Gaissmaier W, Galesic M, Han PK, et al. Presenting quantitative information about decision outcomes: a risk communication primer for patient decision aid developers. BMC Med Inform Decis Mak. (2013) 13:7. doi: 10.1186/1472-6947-13-S2-S7
58. Hoffmann TC, Glasziou PP, Boutron I, Milne R, Perera R, Moher D, et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ. (2014) 348:g1687. doi: 10.1136/bmj.g1687
59. Ley P, Pike LA, Whitworth MA, Woodward R. Effects of source, context of communication and difficulty level on the success of health educational communications concerning contraception and the menopause. Health Educ J. (1979) 38:47–52. doi: 10.1177/001789697903800204
60. Spiegelhalter D. Risk and uncertainty communication. Annu Rev Stat Appl. (2017) 4:31–60. doi: 10.1146/annurev-statistics-010814-020148
Keywords: stroke, prevention, knowledge, evidence based patient information, stroke patient information
Citation: Alegiani AC, Rahn AC, Steckelberg A, Thomalla G, Heesen C and Köpke S (2020) Quality of Stroke Patient Information Applied in Randomized Controlled Trials—Literature Review. Front. Neurol. 11:526515. doi: 10.3389/fneur.2020.526515
Received: 17 January 2020; Accepted: 06 November 2020;
Published: 07 December 2020.
Edited by:
Paulette Van Vliet, The University of Newcastle, AustraliaReviewed by:
Bleydy Dimech-Betancourt, La Trobe University, AustraliaCopyright © 2020 Alegiani, Rahn, Steckelberg, Thomalla, Heesen and Köpke. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anna C. Alegiani, YS5hbGVnaWFuaUB1a2UuZGU= orcid.org/0000-0001-8216-6220
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.