
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Neurol., 07 July 2020
Sec. Multiple Sclerosis and Neuroimmunology
Volume 11 - 2020 | https://doi.org/10.3389/fneur.2020.00566
This article is part of the Research TopicCorticospinal Excitability in Patients with Multiple SclerosisView all 10 articles
 Mario Stampanoni Bassi1
Mario Stampanoni Bassi1 Fabio Buttari1
Fabio Buttari1 Luana Gilio1
Luana Gilio1 Nicla De Paolis1Diego Fresegna2
Nicla De Paolis1Diego Fresegna2 Diego Centonze1,3*
Diego Centonze1,3* Ennio Iezzi1
Ennio Iezzi1Transcranial magnetic stimulation (TMS) has been employed in multiple sclerosis (MS) to assess the integrity of the corticospinal tract and the corpus callosum and to explore some physiological properties of the motor cortex. Specific alterations of TMS measures have been strongly associated to different pathophysiological mechanisms, particularly to demyelination and neuronal loss. Moreover, TMS has contributed to investigate the neurophysiological basis of MS symptoms, particularly those not completely explained by conventional structural damage, such as fatigue. However, variability existing between studies suggests that alternative mechanisms should be involved. Knowledge of MS pathophysiology has been enriched by experimental studies in animal models (i.e., experimental autoimmune encephalomyelitis) demonstrating that inflammation alters synaptic transmission, promoting hyperexcitability and neuronal damage. Accordingly, TMS studies have demonstrated an imbalance between cortical excitation and inhibition in MS. In particular, cerebrospinal fluid concentrations of different proinflammatory and anti-inflammatory molecules have been associated to corticospinal hyperexcitability, highlighting that inflammatory synaptopathy may represent a key pathophysiological mechanism in MS. In this perspective article, we discuss whether corticospinal excitability alterations assessed with TMS in MS patients could be useful to explain the pathophysiological correlates and their relationships with specific MS clinical characteristics and symptoms. Furthermore, we discuss evidence indicating that, in MS patients, inflammatory synaptopathy could be present since the early phases, could specifically characterize relapses, and could progressively increase during the disease course.
Multiple sclerosis (MS) is an inflammatory immune-mediated disease of the central nervous system (CNS) with white matter demyelinating lesions and chronic diffuse neuronal degeneration, causing variable and unpredictable clinical manifestations and disease course.
Transcranial magnetic stimulation (TMS) is a neurophysiological technique that exploits the principles of electromagnetic induction. A coil of wire, connected to an electric pulse generator and placed over the scalp, produces a strong magnetic pulse of very short duration able to penetrate through the intact skull, inducing an electric current in the underlying neural tissue noninvasively and almost painlessly (1). The induced electric current mainly flows tangentially to the brain surface, preferentially activating cortical fibers oriented in parallel to the electric field (2). When applied over the primary motor cortex (M1), TMS excites the corticospinal system, eliciting multiple descending volleys, which reflect both the direct activation of cortical motor axons (D-waves) and the indirect, trans-synaptic activation of motor cortical neurons (I-waves) (3, 4). The recruitment of different combinations of D- and I-waves depends on the stimulus intensity, pulse configuration, coil shape, and orientation (5–9). In particular, with a posterior-to-anterior induced current flow, TMS at lower intensities evokes I-waves, whereas at higher intensities also D-waves occur (10). These descending activities can be recorded in contralateral target muscles as motor-evoked potentials (MEPs).
TMS is used in the clinical context of MS together with multimodal evoked potentials (i.e., visual and somatosensory) as a useful tool to detect subclinical involvement of the corresponding functional system with the aim to help early diagnosis (11). TMS alterations have also been correlated to demyelinating damage and neuronal degeneration in different MS phenotypes. For example, slowed central motor conduction time (CMTC) and reduced MEP amplitude can indicate axonal depletion or even extreme asynchrony of the multiple descending volleys to spinal motoneurons due to conduction blocks in the myelinated fibers along the corticospinal tracts (12, 13).
Experimental evidence from studies in animal models and in patients with MS suggests that inflammation critically affects synaptic functioning (14). Accordingly, neurophysiological alterations have been detected even in the absence of macroscopic damage, suggesting a role of additional pathological mechanisms (15). In particular, different proinflammatory and anti-inflammatory molecules can influence cortical excitability in MS (16) representing an additional cause of impaired synaptic functioning.
In this perspective article, we provide an overview of the main TMS studies exploring corticospinal excitability and connectivity alterations in MS, their pathophysiological correlates, and their relationship to clinical characteristics and symptoms. In addition, evidence from preclinical data and TMS studies, which highlight the role of inflammatory synaptopathy as a relevant pathophysiological mechanism that acts since the early phases of MS, is discussed.
TMS can be used to assess the functionality of the corticospinal tract and the corpus callosum (CC) and to explore some physiological properties of M1. Various TMS paradigms have been designed to investigate corticospinal excitability to test excitatory and inhibitory interactions in M1 and to probe M1 connectivity (Table 1). Single-pulse TMS can be used to assess simple cortical excitability measures, such as motor thresholds, to study MEP characteristics, to estimate CMCT, and to test cortical inhibition. With paired-pulse TMS, it is possible to explore specific inhibitory and excitatory circuits in M1. During paired-pulse TMS, two stimulators are connected to the same coil that delivers two consecutive pulses at variable interstimulus intervals (ISIs). In addition, TMS has been used to investigate interhemispheric effective connectivity of M1 by exploring transcallosal connections with either single or double-coil (d-c) approaches. In d-c TMS, two stimulation units, each connected to a corresponding coil, are used to target different motor cortical regions at various ISIs.
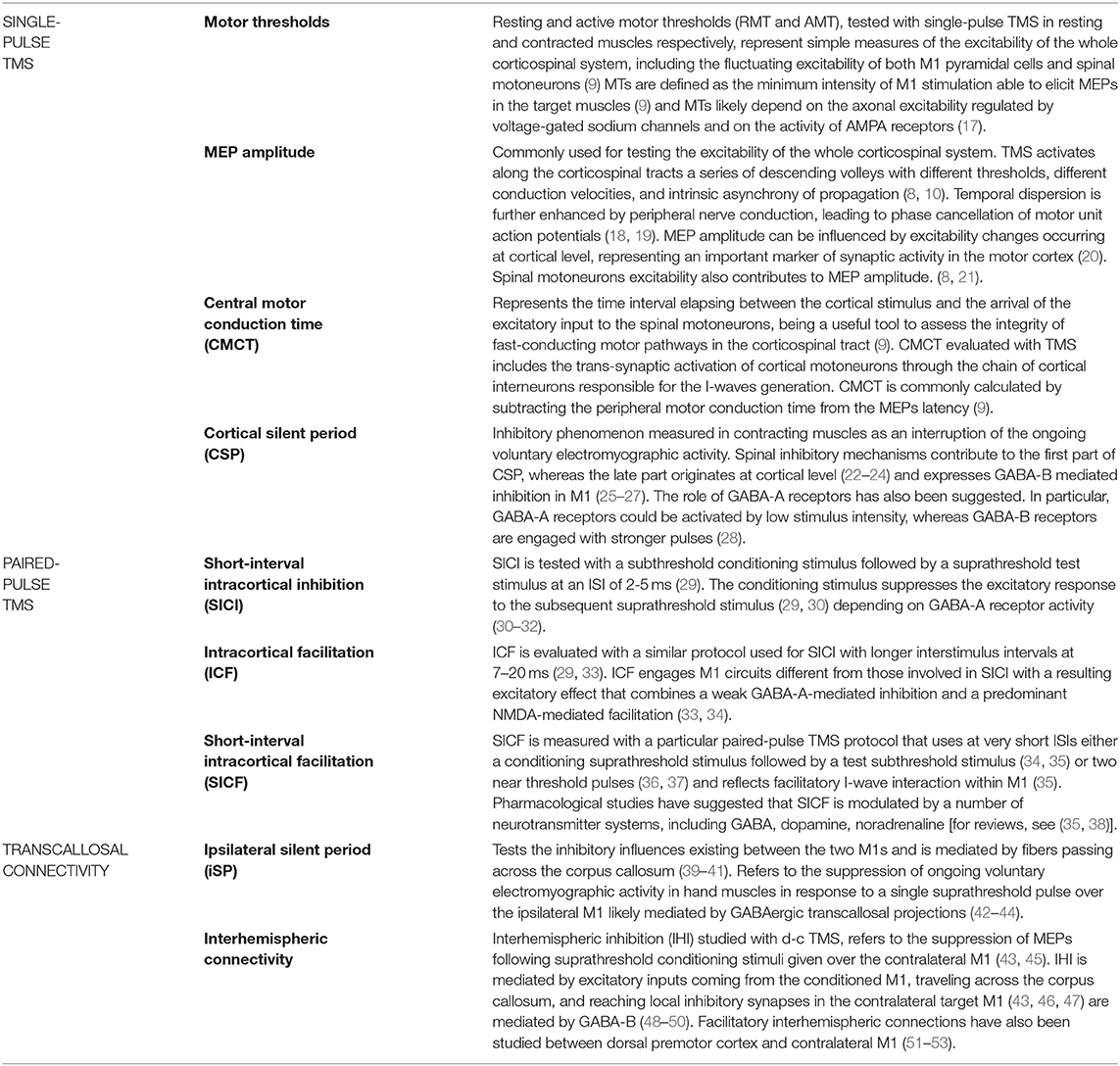
Table 1. Main TMS protocols used to explore motor cortex pathophysiology in MS patients.
Considering the clinical impact of corticospinal system lesions, different TMS studies have shown several alterations of M1 excitability and corticospinal tract conduction in MS patients. In particular, reduced MEP amplitude (54–56), increased MEP latency (57), and duration (58) have been reported in MS patients compared with control subjects. In addition, increased RMT (55, 59) and prolonged CMCT (54, 59–62) have been frequently evidenced in patients with MS. Overall, these findings have been interpreted in the light of demyelinating conduction block and axonal damage. In fact, demyelination and conduction blocks could lead to a greater temporal dispersion of the corticospinal volleys, resulting in reduced amplitude and increased MEP duration, prolonged MEP latency, and increased CMCT. Conversely, axonal loss could be more relevant in progressive MS, being associated with higher RMT, reduced MEP amplitude, and longer CMCT (55).
Cortical inhibition tested with single-pulse TMS has documented prolonged CSP duration in RR-MS patients (57, 63). One study has shown that, in remitting patients, CSP prolongation was correlated with white matter lesion volume but not with cortical thickness (57). In progressive MS patients, reduced CSP duration correlated with lower whole-brain cortical magnetization transfer ratio (MTR), suggesting a role of cortical damage (56). Altered GABA transmission could explain the CSP alteration although alternative mechanisms have been suggested, including changes in spinal motoneuron excitability (23, 24), attentional processes (64, 65), and altered voluntary motor drive (66). In addition, reduced CSP duration after a fatiguing motor task has been reported in MS patients compared to controls (67), suggesting that additional mechanisms could also be involved.
Various studies have explored SICI in MS patients (55, 56, 68). Although some authors reported comparable SICI between RR-MS and controls (55, 57, 69), in one study it has been found that lower SICI in patients with RR-MS was correlated with reduced MTR in the hand motor cortex (56). In addition, reduced SICI and increased ICF have been reported in SP-MS patients compared with RR-MS and controls (55, 69). It has been proposed that the clinical course of progressive MS phenotypes could be characterized by a deterioration of SICI over time (70). These alterations may reflect hyperexcitability due to enhanced glutamatergic transmission and reduced inhibition, which could be particularly noticeable in progressive patients, being associated with higher disability and cortical atrophy (55).
As the CC involvement represents a hallmark of MS, TMS has been specifically used to test interhemispheric connectivity in these patients. Increased iSP latency and duration have been reported in MS patients compared to controls (60–62, 71). In particular, iSP alterations found in MS have been associated to CC volume (62). One study in MS patients, combining TMS and fMRI, has demonstrated that increased ipsilateral M1 activation during the execution of a motor task was correlated with reduced iSP duration and with ultrastructural damage of the CC (61). However, prolonged iSP duration has also been associated with CMCT prolongation without significant correlations with CC abnormalities, suggesting that transcallosal inhibition could be affected by demyelination of the contralateral corticospinal tract (72). Notably, reduced IHI has also been observed in early RR-MS patients in the absence of macroscopic damage of the CC or CMCT alterations (73). Finally, one TMS study has shown that excitatory interhemispheric connectivity between premotor cortex and contralateral M1 could be reduced, irrespective of CC lesion load and in the absence of disability (53). Although the pathophysiological mechanisms underlying altered interhemispheric connectivity in MS are not fully understood, it is likely that, alternatively to CC structural damage, other mechanisms could be involved, including reduced excitatory projections from the conditioning cortex or defective GABAergic signaling in target M1 inhibitory interneurons (48, 74).
Alterations of various TMS measures have been related to MS clinical characteristics. Expanded disability status scale (EDSS) score has been associated with increased RMT, altered MEPs, and prolonged CMCT and iSP duration (55, 58, 60). A positive correlation between these TMS measures and clinical scores could reflect the prevalent role of white matter lesions in the pathogenesis of these alterations, particularly of the corticospinal tract and the CC. The role of white matter disconnection has been specifically involved in cerebellar symptoms. Cerebellar tremor in MS has been associated with lacking cerebellar-M1 inhibitory connectivity tested with d-c TMS (75). In addition, cerebellar dysfunction in MS has also been associated with increased CSP duration, likely resulting from impaired cerebellar projections to M1 (63).
Altered balance between cortical excitation and inhibition in MS has been correlated with clinical severity. One study showed that prolonged CSP duration was correlated with clinical disability and predicted greater motor impairment, suggesting that increased inhibition could lessen clinical compensation, possibly interfering with plasticity (57). Moreover, one study has demonstrated that defective SICF was correlated with increased EDSS in MS patients (76). Alterations involving both inhibitory and excitatory circuits would suggest a specific role of synaptic dysfunction in addition to demyelination of white matter tracts. The finding that steroid administration in relapsing RR-MS led to motor improvement, along with reduced SICI and enhanced ICF (77), supports this hypothesis, suggesting a restored synaptic functioning within M1. Finally, it has been proposed that corticospinal excitability asymmetry between the two hemispheres could represent a marker of clinical disability, whose mechanisms are not completely elucidated and possibly involving neurodegenerative and inflammatory processes (78).
Fatigue represents a frequent and severely disabling symptom in MS patients (79). Different mechanisms have been postulated, including white matter and cortical lesions, endocrine alterations, and the influence of neuroinflammation on brain functioning (80, 81). Enhanced GABAergic activity tested with SICI and CSP has been specifically implicated in MS fatigue (82, 83). In line with the hypothesis of increased M1 inhibition in fatigued MS patients, one study has demonstrated that a fatiguing motor task was associated with increased CSP duration. Notably, unlike healthy controls, CSP alteration also involved untrained adjacent muscles, suggesting that mechanisms of cortical spreading could intervene in generating fatigue in MS (67).
Cognitive dysfunction represents an important symptom frequently underestimated in MS patients, which involves various domains, including executive functions, processing speed, and working memory. In addition to demyelination and gray matter atrophy, different pathophysiological mechanisms, including the presence of cortical lesions, impaired brain network organization, and altered synaptic functioning, have been proposed (84). Short-latency afferent inhibition (SAI), a TMS protocol exploring the efficiency of cortical cholinergic inhibitory activity mediated by peripheral somatosensory afferent inputs to M1 (85), has been used to investigate cognitive dysfunction in MS. In particular, verbal memory impairment was associated with reduced SAI that could be partly reversed by rivastigmine administration (86). Notably, these results are in line with studies demonstrating altered SAI in patients with Alzheimer's disease (87). Although mood disturbances are frequently observed in MS, correlations with TMS alterations have been scarcely investigated. One study showed that anxiety in MS patients was associated with altered inhibitory interhemispheric connectivity, highlighting the role of increased transcallosal transfer (88).
In MS, auto-reactive T lymphocyte infiltration into the CNS and activation of resident immune cells lead to demyelinating lesions and axonal damage. Inflammatory cytokines released by immune cells play a crucial role in inducing and maintaining the inflammatory response in MS. Proinflammatory molecules promote T-helper 1 (Th1) and Th17 differentiation and lymphocyte activation and migration across the blood brain barrier (89). Accordingly, enhanced expression of various cytokines, including interleukin (IL)-1β, tumor necrosis factor (TNF), IL-6, IL-17, and interferon (IFN)-γ has been reported in animal models (i.e., experimental autoimmune encephalomyelitis, EAE) and in the perivascular infiltrates and cerebrospinal fluid (CSF) of MS patients (90–94).
In addition to their immunomodulatory activity, cytokines modulate the function of oligodendrocytes, astrocytes, and neurons (95, 96). Experimental studies have shown that inflammatory molecules specifically influence synaptic functioning, suggesting that chemokines and cytokines may represent an important communicating system in the CNS. In turn, astrocytes, endothelial cells, and neurons participate in cytokine production (97, 98), generating a neuro-immune crosstalk with crucial roles in physiological and pathological conditions (99, 100).
Experimental studies have contributed to demonstrate that inflammation alters synaptic functioning (14, 101). In the striatum of EAE mice, electrophysiological recordings revealed enhanced glutamatergic transmission and excitotoxic neurodegeneration occurring since the early phases, before the onset of symptoms, and independently of demyelinating damage (14). These excitotoxic alterations were mainly caused by increased activity and expression of the a-amino-3-hydroxy-5-methyl-4-isoxazolepropionicacid (AMPA) receptor; accordingly, the administration of inhibitors of glutamate AMPA receptors ameliorated the course of EAE and reduced loss of dendritic spines (14). In the same study, TNF released by activated microglial cells was identified as mainly responsible for these alterations as incubation of this molecule reproduced in vitro both altered AMPA activity and neuronal damage. Other inflammatory cytokines have been associated with synaptic hyperexcitability in EAE. The proinflammatory cytokine IL-1β induced pathologically enhanced glutamatergic transmission in the cerebellum of EAE mice, reducing glutamate reuptake by altering the expression of the glutamate-aspartate transporter/excitatory amino acid transporter 1 (GLAST/EAAT1) (102). Notably, the administration of the GLAST/EAAT1 inhibitor reproduced the synaptic modifications observed in symptomatic EAE mice (103). In addition, administration of the IL-1 receptor antagonist, a physiological inhibitor of IL-1β (104), ameliorated the course of EAE by reducing astroglia activation and restoring GLAST/EAAT1 expression (102, 105). Proinflammatory cytokines have also been consistently associated with altered inhibitory transmission in EAE mice. It has been evidenced that incubating IL-1β and TNF in mice brain slices impaired GABAergic transmission and promoted excitotoxic neuronal damage (106, 107). Accordingly, enhancing GABA signaling significantly improved the clinical symptoms of EAE, likely as a result of a direct neuroprotective effect and inhibition of inflammatory response (108).
Translational experiments confirmed that a similar subset of proinflammatory molecules mediates synaptic alterations in human MS. One study has demonstrated that the CSF collected from patients with active MRI lesions pathologically enhanced excitatory postsynaptic currents when incubated on mice brain slices, inducing glutamate-mediated neuronal damage (109). IL-1β has been identified as mainly responsible for these alterations by increasing AMPA receptor activity. Inflammation-induced synaptic alterations in MS have also been investigated using a heterologous chimeric model. T-lymphocytes isolated from the peripheral blood of RR-MS patients exacerbated the glutamatergic transmission when incubated on mice brain slices (110). In particular, only lymphocytes from patients with acute inflammation, as evidenced by the presence of gadolinium-enhancing lesions at MRI, were able to induce synaptic alterations. Notably, co-incubation with etanercept, a TNF antagonist, prevented these alterations, confirming that TNF was mainly responsible for these findings (110).
The role of inflammation on synaptic dysfunction in MS has been specifically addressed by some TMS studies. In relapsing MS patients, it has been shown to both reduce CSP duration and impair SICI compared to remitting patients (111). These results demonstrate that the relapsing phases could be characterized by cortical hyperexcitability, suggesting reduced GABAergic transmission similarly to as evidenced in animal models (106, 107). To explore the role of CSF inflammation on cortical excitability, different TMS measures have been correlated with the levels of specific proinflammatory molecules. In relapsing MS patients, elevated IL-1β signaling has been associated with increased ICF without effect on SICI (109). This finding has confirmed the main role of this molecule in altering synaptic functioning also in human MS by enhancing glutamatergic transmission (109). The involvement of this molecule in the excitotoxic degeneration has also been suggested by clinical studies, showing that CSF IL-1β detectability during remissions predicted greater prospective disability and neurodegeneration (112). Other inflammatory mediators have also been associated to altered synaptic transmission in relapsing MS patients. Regulated upon activation, normal T-cell expressed and secreted (RANTES) is a proinflammatory molecule regulating the leukocyte chemotaxis (113). Increased RANTES concentrations have been found in the CSF of MS patients with acute inflammation and correlated with both reduced SICI and increased ICF (114). Finally, incubating this molecule on mice hippocampal slices promoted hyperexcitability and excitotoxicity (114), confirming the role of RANTES as a central regulator of glutamatergic transmission (113).
Overall, these results indicate that exacerbated CSF inflammation negatively influences the disease course of MS, promoting synaptic hyperexcitability and neuronal damage. It has been proposed that neurodegeneration in progressive MS phenotypes could also result from inflammation-driven synaptic alterations. In fact, reduced SICI and enhanced ICF have been reported in SP-MS patients and have been related to enhanced disability (55). These findings suggest that glutamatergic excitotoxic damage could characterize the progressive MS phenotypes as demonstrated by in vitro studies showing hyperexcitability and enhanced neuronal damage induced by CSF collected from progressive MS patients, mediated by TNF (115). Conversely, anti-inflammatory cytokines, including IL-10 and IL-13, and neurotrophic factors may exert protective effects, reducing neurodegeneration and promoting a better disease course in EAE and MS (116–119). TMS studies have confirmed that anti-inflammatory molecules could reduce the synaptic alterations in MS. Accordingly, in RR-MS patients, the CSF levels of the anti-inflammatory molecule IL-13 have been associated with increased SICI, possibly contributing to restored inhibitory synaptic activity and limiting the impact of excitotoxicity. Notably, IL-13 CSF levels were also associated with reduced measures of neuronal and axonal damage and with increased amyloid-beta CSF concentrations, suggesting a protective role of this cytokine in MS (120).
Various TMS protocols have been used to characterize the neurophysiological correlates of specific pathophysiological mechanisms, such as demyelination and neuronal loss, in different disease phases and phenotypes. These studies have contributed to better defining the neurophysiological basis of specific MS symptoms, particularly those not completely explained by conventional structural damage measures, such as fatigue and cognitive deficits. Alterations of corticospinal excitability and corticospinal tract conduction have been clearly linked to both demyelinating blocks and axonal damage. MEP latency and amplitude are the most frequently altered TMS measures in MS and have been consistently associated with disability, representing useful tools in clinical settings. Although TMS studies investigating intracortical excitability and effective connectivity have shown some association with specific pathophysiological mechanisms or disease phenotypes, some discrepancies suggest that alternative mechanisms should be involved.
Evidence from experimental studies suggests that inflammatory synaptopathy could represent an independent cause of synaptic dysfunction with important implications on disease course and prognosis. Inflammation, altering corticospinal excitability and connectivity in MS patients, could contribute to better explain the variability of TMS findings. Experimental models have clearly shown that inflammation exacerbates synaptic hyperexcitability, and TMS studies have confirmed an imbalance between excitatory and inhibitory transmission in MS patients. Hence, inflammation-driven synaptic hyperexcitability could be present since the early phases, could specifically characterize MS relapses, and could progressively increase during the disease course.
Having in mind that TMS measures represent the resulting effect of different anatomic and physiological factors, it is difficult to identify the contribution of specific mechanisms to TMS alterations seen in MS patients. Therefore, when cortical excitability measures are used to investigate MS pathophysiology, the role of specific confounding factors, including disease activity and phenotypes, ongoing therapies, and symptoms, such as fatigue, should be carefully considered. Further studies conducted in specific populations, such as patients with clinically isolated syndrome or with progressive MS, or combining TMS with structural and/or functional imaging data, could help to shed light on the specific role of demyelination, atrophy, and inflammation.
MS, EI, and DC contributed conception and design of the study, MS and EI wrote the first draft of the manuscript, FB, LG, ND, and DF wrote sections of the manuscript. All authors contributed to manuscript revision, read and approved the submitted version.
This research was supported by FISM-Fondazione Italiana Sclerosi Multipla-cod. 2019/S/1 to DC; by the Italian Ministry of Health (Ricerca corrente-IRCCS Neuromed to DC; Ricerca Finalizzata 2018, RF-2018-12366144 to DC; Ricerca Finalizzata 2018, GR-2018-12366154 to FB) and by 5 × 1000 grant to IRCCS Neuromed. The funders had no role in the design of the study, in the collection, analyses, or interpretation of data, in the writing of the manuscript, or in the decision to publish the results.
The authors declare the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: FB acted as Advisory Board members of Teva and Roche and received honoraria for speaking or consultation fees from Merck Serono, Teva, Biogen Idec, Sanofi, and Novartis and non-financial support from Merck Serono, Teva, Biogen Idec, and Sanofi. DC is an Advisory Board member of Almirall, Bayer Schering, Biogen, GW Pharmaceuticals, Merck Serono, Novartis, Roche, Sanofi-Genzyme, and Teva and received honoraria for speaking or consultation fees from Almirall, Bayer Schering, Biogen, GW Pharmaceuticals, Merck Serono, Novartis, Roche, Sanofi-Genzyme, and Teva. He is also the principal investigator in clinical trials for Bayer Schering, Biogen, Merck Serono, Mitsubishi, Novartis, Roche, Sanofi-Genzyme, and Teva. His preclinical and clinical research was supported by grants from Bayer Schering, Biogen Idec, Celgene, Merck Serono, Novartis, Roche, Sanofi-Genzyme and Teva. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Barker AT, Jalinous R, Freeston IL. Non-invasive magnetic stimulation of human motor cortex. Lancet. (1985) 1:1106–07.
2. Hallett M. Transcranial magnetic stimulation and the human brain. Nature. (2000) 406:147–50. doi: 10.1038/35018000
3. Amassian VE, Stewart M, Quirk GJ, Rosenthal JL. Physiological basis of motor effects of a transient stimulus to cerebral cortex. Neurosurgery. (1987) 20:74-93.
4. Shimazu H, Maier MA, Cerri G, Kirkwood PA, Lemon RN. Macaque ventral premotor cortex exerts powerful facilitation of motor cortex outputs to upper limb motoneurons. J Neurosci. (2004) 24:1200–11. doi: 10.1523/JNEUROSCI.4731-03.2004
5. Nakamura H, Kitagawa H, Kawaguchi Y, Tsuji H. Direct and indirect activation of human corticospinal neurons by transcranial magnetic and electrical stimulation. Neurosci Lett. (1996) 210:45–8. doi: 10.1016/0304-3940(96)12659-8
6. Di Lazzaro V, Oliviero A, Mazzone P, Insola A, Pilato F, Saturno E, et al. Comparison of descending volleys evoked by monophasic and biphasic magnetic stimulation of the motor cortex in conscious humans. Exp Brain Res. (2001) 141:121–7. doi: 10.1007/s002210100863
7. Kammer T, Beck S, Thielscher A, Laubis-Herrmann U, Topka H. Motor thresholds in humans: a transcranial magnetic stimulation study comparing different pulse waveforms, current directions and stimulator types. Clin Neurophysiol. (2001) 112:250-58. doi: 10.1016/s1388-2457(00)00513-7
8. Groppa S, Oliviero A, Eisen A, Quartarone A, Cohen LG, Mall V, et al. A practical guide to diagnostic transcranial magnetic stimulation: report of an IFCN committee. Clin Neurophysiol. (2012) 123:858-882. doi: 10.1016/j.clinph.2012.01.010
9. Rossini PM, Burke D, Chen R, Cohen LG, Daskalakis Z, Di Iorio R, et al. Non-invasive electrical and magnetic stimulation of the brain, spinal cord, roots and peripheral nerves: basic principles and procedures for routine clinical and research application. An updated report from an I.F.C.N. Committee. Clin Neurophysiol. (2015) 126:1071–107. doi: 10.1016/j.clinph.2015.02.001
10. Di Lazzaro V, Oliviero A, Pilato F, Saturno E, Dileone M, Mazzone P, et al. The physiological basis of transcranial motor cortex stimulation in conscious humans. Clin Neurophysiol. (2004) 115:255-66. doi: 10.1016/j.clinph.2003.10.009
11. Ziemann U, Wahl M, Hattingen E, Tumani H. Development of biomarkers for multiple sclerosis as a neurodegenerative disorder. Prog Neurobiol. (2011) 95:670–85. doi: 10.1016/j.pneurobio.2011.04.007
12. Hess CW, Mills KR, Murray NM. Measurement of central motor conduction in multiple sclerosis by magnetic brain stimulation. Lancet. (1986) 2:355–8. doi: 10.1016/S0140-6736(86)90050-4
13. Hess CW, Mills KR, Murray NM, Schriefer TN. Magnetic brain stimulation: central motor conduction studies in multiple sclerosis. Ann Neurol. (1987) 22:744–52. doi: 10.1002/ana.410220611
14. Centonze D, Muzio L, Rossi S, Cavasinni F, De Chiara V, Bergami A, et al. Inflammation triggers synaptic alteration and degeneration in experimental autoimmune encephalomyelitis. J Neurosci. (2009) 29:3442-52. doi: 10.1523/JNEUROSCI.5804-08.2009
15. Zeis T, Graumann U, Reynolds R, Schaeren-Wiemers N. Normal-appearing white matter in multiple sclerosis is in a subtle balance between inflammation and neuroprotection. Brain. (2008) 131:288-303. doi: 10.1093/brain/awm291
16. Stampanoni Bassi M, Mori F, Buttari F, Marfia GA, Sancesario A, Centonze D, et al. Neurophysiology of synaptic functioning in multiple sclerosis. Clin Neurophysiol. (2017) 128:1148-57. Review. doi: 10.1016/j.clinph.2017.04.006
17. Ziemann U, Reis J, Schwenkreis P, Rosanova M, Strafella A, Badawy R, et al. TMS and drugs revisited 2014. Clin Neurophysiol. (2015) 126:1847-68. doi: 10.1016/j.clinph.2014.08.028
18. Rossini PM, Marciani MG, Caramia M, Roma V, Zarola F. Nervous propagation along ‘central' motor pathways in intact man: characteristics of motor responses to ‘bifocal' and ‘unifocal' spine and scalp non-invasive stimulation. Electroencephalogr Clin Neurophysiol. (1985) 61:272–86. doi: 10.1016/0013-4694(85)91094-6
19. Magistris MR, Rosler KM, Truffert A, Myers JP. Transcranial stimulation excites virtually all motor neurons supplying the target muscle. A demonstration and a method improving the study of motor evoked potentials. Brain. (1998) 121:437–50. doi: 10.1093/brain/121.3.437
20. Ferreri F, Vecchio F, Ponzo D, Pasqualetti P, Rossini PM. Time-varying coupling of EEG oscillations predicts excitability fluctuations in the primary motor cortex as reflected by motor evoked potentials amplitude: an EEG–TMS study. Hum Brain Mapp. (2014) 35:1969–80. doi: 10.1002/hbm.22306
21. Taylor JL. Stimulation at the cervicomedullary junction in human subjects. J Electromyogr Kinesiol. (2006) 16:215-23. doi: 10.1016/j.jelekin.2005.07.001
22. Fuhr P, Agostino R, Hallett M. Spinal motor neuron excitability during the silent period after cortical stimulation. Electroencephalogr Clin Neurophysiol. (1991) 81:257–62. doi: 10.1016/0168-5597(91)90011-l
23. Inghilleri M, Berardelli A, Cruccu G, Manfredi M. Silent period evoked by transcranial stimulation of the human cortex and cervicomedullary junction. J Physiol. (1993) 466:521-34.
24. Ziemann U, Netz J, Szelenyi A, Hömberg V. Spinal and supraspinal mechanisms contribute to the silent period in the contracting soleus muscle after transcranial magnetic stimulation of human motor cortex. Neurosci Lett. (1993) 156:167–71. doi: 10.1016/0304-3940(93)90464-v
25. Werhahn KJ, Kunesch E, Noachtar S, Benecke R, Classen J. Differential effects on motorcortical inhibition induced by blockade of GABA uptake in humans. J Physiol. (1999) 517(Pt 2):591-7. doi: 10.1111/j.1469-7793.1999.0591t.x
26. Pierantozzi M, Marciani MG, Palmieri MG, Brusa L, Galati S, Caramia MD, et al. Effect of Vigabatrin on motor responses to transcranial magnetic stimulation: an effective tool to investigate in vivo GABAergic cortical inhibition in humans. Brain Res. (2004) 1028:1–8. doi: 10.1016/j.brainres.2004.06.009
27. Siebner HR, Dressnandt J, Auer C, Conrad B. Continuous intrathecal baclofen infusions induced a marked increase of the transcranially evoked silent period in a patient with generalized dystonia. Muscle Nerve. (1998) 21:1209–12. doi: 10.1002/(sici)1097-4598(199809)21:9<1209::aid-mus15>3.0.co;2-m
28. Kimiskidis VK, Papagiannopoulos S, Kazis DA, Sotirakoglou K, Vasiliadis G, Zara F, et al. Lorazepam-induced effects on silent period and corticomotor excitability. Exp Brain Res. (2006) 173:603-11. doi: 10.1007/s00221-006-0402-1
29. Kujirai T, Caramia MD, Rothwell JC, Day BL, Thompson PD, Ferbert A, et al. Corticocortical inhibition in human motor cortex. J Physiol. (1993) 471:501–19. doi: 10.1113/jphysiol.1993.sp019912
30. Ilic TV, Meintzschel F, Cleff U, Ruge D, Kessler KR, Ziemann U. Short-interval paired-pulse inhibition and facilitation of human motor cortex: the dimension of stimulus intensity. J Physiol. (2002) 545:153–67. doi: 10.1113/jphysiol.2002.030122
31. Di Lazzaro V, Oliviero A, Meglio M, Cioni B, Tamburrini G, Tonali P, et al. Direct demonstration of the effect of lorazepam on the excitability of the motor cortex. Clin Neurophysiol. (2000). 111:794–99. doi: 10.1016/s1388-2457(99)00314-4
32. Ziemann U, Lönnecker S, Steinhoff BJ, Paulus W. The effect of lorazepam on the motor cortical excitability in man. Exp Brain Res. (1996) 109:127-35. doi: 10.1007/bf00228633
33. Ziemann U, Rothwell JC, Ridding MC. Interaction between intracortical inhibition and facilitation in human motor cortex. J Physiol. (1996) 496:873–81. doi: 10.1113/jphysiol.1996.sp021734
34. Hanajima R, Ugawa Y, Terao Y, Sakai K, Furubayashi T, Machii K, et al. Paired-pulse magnetic stimulation of the human motor cortex: differences among I waves. J Physiol. (1998) 509:607-18. doi: 10.1111/j.1469-7793.1998.607bn.x
35. Ziemann U, Tergau F, Wassermann EM, Wischer S, Hildebrandt J, Paulus W. Demonstration of facilitatory I-wave interaction in the human motor cortex by paired transcranial magnetic stimulation. J Physiol. (1998) 511:181–90. doi: 10.1111/j.1469-7793.1998.181bi.x
36. Tokimura H, Ridding MC, Tokimura Y, Amassian VE, Rothwell JC. Short latency facilitation between pairs of threshold magnetic stimuli applied to human motor cortex. Electroencephalogr Clin Neurophysiol. (1996) 101:263-72.
37. Di Lazzaro V, Rothwell JC, Oliviero A, Profice P, Insola A, Mazzone P, et al. Intracortical origin of the short latency facilitation produced by pairs of threshold magnetic stimuli applied to human motor cortex. Exp Brain Res. (1999) 129:494-499. doi: 10.1007/s002210050919
38. Di Lazzaro and Ziemann U. The contribution of transcranial magnetic stimulation in the functional evaluation of microcircuits in human motor cortex. Front Neural Circuits. (2013) 7:18. doi: 10.3389/fncir.2013.00018
39. Boroojerdi B, Diefenbach K, Ferbert A. Transcallosal inhibition in cortical and subcortical cerebral vascular lesions. J Neurol Sci. (1996) 144:160-70. doi: 10.1016/s0022-510x(96)00222-5
40. Meyer BU, Röricht S, Woiciechowsky C. Topography of fibers in the human corpus callosum mediating interhemispheric inhibition between the motor cortices. Ann Neurol. (1998) 43:360-9. doi: 10.1002/ana.410430314
41. Heinen F, Glocker FX, Fietzek U, Meyer BU, Lücking CH, Korinthenberg R. Absence of transcallosal inhibition following focal magnetic stimulation in preschool children. Ann Neurol. (1998) 43:608-12. doi: 10.1002/ana.410430508
42. Wassermann EM, Fuhr P, Cohen LG, Hallett M. Effects of transcranial magnetic stimulation on ipsilateral muscles. Neurology. (1991) 41:1795-9. doi: 10.1212/wnl.41.11.1795
43. Ferbert A, Priori A, Rothwell JC, Day BL, Colebatch JG, Marsden CD. Interhemispheric inhibition of the human motor cortex. J Physiol. (1992) 453:525-46. https://doi.org/10.1113/jphysiol.1992.sp019243
44. Meyer BU, Röricht S, Gräfin von Einsiedel H, Kruggel F, Weindl A. Inhibitory and excitatory interhemispheric transfers between motor cortical areas in normal humans and patients with abnormalities of the corpus callosum. Brain. (1995) 118:429-40. doi: 10.1093/brain/118.2.429
45. Uehara K, Morishita T, Kubota S, Hirano M, Funase K. Functional difference in short- and long-latency interhemispheric inhibitions from active to resting hemisphere during a unilateral muscle contraction. J Neurophysiol. (2014) 111:17-25. doi: 10.1152/jn.00494.2013
46. Wahl M, Lauterbach-Soon B, Hattingen E, Jung P, Singer O, Volz S, et al. Human motor corpus callosum: topography, somatotopy, and link between microstructure and function. J Neurosci. (2007) 27:12132-38. doi: 10.1523/JNEUROSCI.2320-07.2007
47. Ni Z, Gunraj C, Nelson AJ, Yeh IJ, Castillo G, Hoque T, et al. Two phases of interhemispheric inhibition between motor related cortical areas and the primary motor cortex in human. Cereb Cortex. (2009) 19:1654-65. doi: 10.1093/cercor/bhn201
48. Kukaswadia S, Wagle-Shukla A, Morgante F, Gunraj C, Chen R. Interactions between long latency afferent inhibition and interhemispheric inhibitions in the human motor cortex. J Physiol. (2005) 563:915-24. doi: 10.1113/jphysiol.2004.080010
49. Radhu N, Ravindran LN, Levinson AJ, Daskalakis ZJ. Inhibition of the cortex using transcranial magnetic stimulation in psychiatric populations: current and future directions. J Psychiatry Neurosci. (2012) 37:369-78. Review. doi: 10.1503/jpn.120003
50. Irlbacher K, Brocke J, Mechow JV, Brandt SA. Effects of GABA(A) and GABA(B) agonists on interhemispheric inhibition in man. Clin Neurophysiol. (2007) 118:308-16. doi: 10.1016/j.clinph.2006.09.023
51. Bäumer T, Bock F, Koch G, Lange R, Rothwell JC, Siebner HR, Münchau A. Magnetic stimulation of human premotor or motor cortex produces interhemispheric facilitation through distinct pathways. J Physiol. (2006) 572:857-68.
52. Mochizuki H, Huang YZ, Rothwell JC. Interhemispheric interaction between human dorsal premotor and contralateral primary motor cortex. J Physiol. (2004) 561:331–8. doi: 10.1113/jphysiol.2004.072843
53. Codecà C, Mori F, Kusayanagi H, Monteleone F, Boffa L, Paolillo A, et al. Differential patterns of interhemispheric functional disconnection in mild and advanced multiple sclerosis. Mult Scler. (2010) 16:1308-16. doi: 10.1177/1352458510376957
54. Kale N, Agaoglu J, Tanik O. Electrophysiological and clinical correlates of corpus callosum atrophy in patients with multiple sclerosis. Neurol Res. (2010) 32:886-90. doi: 10.1179/016164109X12445616596526
55. Vucic S, Burke T, Lenton K, Ramanathan S, Gomes L, Yannikas C, et al. Cortical dysfunction underlies disability in multiple sclerosis. Mult Scler. (2012) 18:425-32. doi: 10.1177/1352458511424308
56. Nantes JC, Zhong J, Holmes SA, Narayanan S, Lapierre Y, Koski L. Cortical Damage and Disability in Multiple Sclerosis: Relation to Intracortical Inhibition and Facilitation. Brain Stimul. (2016) 9:566-73. doi: 10.1016/j.brs.2016.01.003
57. Nantes JC, Zhong J, Holmes SA, Whatley B, Narayanan S, Lapierre Y, et al. Intracortical inhibition abnormality during the remission phase of multiple sclerosis is related to upper limb dexterity and lesions. Clin Neurophysiol. (2016) 127:1503-11. doi: 10.1016/j.clinph.2015.08.011
58. Neva JL, Lakhani B, Brown KE, Wadden KP, Mang CS, Ledwell NH, et al. Multiple measures of corticospinal excitability are associated with clinical features of multiple sclerosis. Behav Brain Res. (2016) 297:187-95. doi: 10.1016/j.bbr.2015.10.015
59. Ho KH, Lee M, Nithi K, Palace J, Mills K. Changes in motor evoked potentials to short-interval paired transcranial magnetic stimuli in multiple sclerosis. Clin Neurophysiol. (1999) 110:712-9. doi: 10.1016/s1388-2457(98)00048-0
60. Schmierer K, Irlbacher K, Grosse P, Röricht S, Meyer BU. Correlates of disability in multiple sclerosis detected by transcranial magnetic stimulation. Neurology. (2002) 59:1218-24. doi: 10.1212/wnl.59.8.1218
61. Lenzi D, Conte A, Mainero C, Frasca V, Fubelli F, Totaro P, et al. Effect of corpus callosum damage on ipsilateral motor activation in patients with multiple sclerosis: a functional and anatomical study. Hum Brain Mapp. (2007) 28:636-44. doi: 10.1002/hbm.20305
62. Llufriu S, Blanco Y, Martinez-Heras E, Casanova-Molla J, Gabilondo I, Sepulveda M, et al. Influence of corpus callosum damage on cognition and physical disability in multiple sclerosis: a multimodal study. PLoS One. (2012) 7:e37167. doi: 10.1371/journal.pone.0037167
63. Tataroglu C, Genc A, Idiman E, Cakmur R, Idiman F. Cortical silent period and motor evoked potentials in patients with multiple sclerosis. Clin Neurol Neurosurg. (2003) 105:105-10. doi: 10.1016/s0303-8467(02)00127-0
64. Hoshiyama M, Kakigi R. Changes of somatosensory evoked potentials during writing with the dominant and non-dominant hands. Brain Res. (1999) 833:10-9.
65. Ziemann U. Pharmaco-transcranial magnetic stimulation studies of motor excitability. Handb Clin Neurol. (2013) 116:387-97. Review. doi: 10.1016/B978-0-444-53497-2.00032-2
66. Tergau F, Wanschura V, Canelo M, Wischer S, Wassermann EM, Ziemann U, et al. Complete suppression of voluntary motor drive during the silent period after transcranial magnetic stimulation. Exp Brain Res. (1999) 124:447–54. doi: 10.1007/s002210050640
67. Santarnecchi E, Rossi S, Bartalini S, Cincotta M, Giovannelli F, Tatti E, et al. Neurophysiological Correlates of Central Fatigue in Healthy Subjects and Multiple Sclerosis Patients before and after Treatment with Amantadine. Neural Plast. (2015) 2015:616242. doi: 10.1155/2015/616242
68. Liepert J, Mingers D, Heesen C, Bäumer T, Weiller C. Motor cortex excitability and fatigue in multiple sclerosis: a transcranial magnetic stimulation study. Mult Scler. (2005) 11:316-21. doi: 10.1191/1352458505ms1163oa
69. Conte A, Lenzi D, Frasca V, Gilio F, Giacomelli E, Gabriele M, et al. Intracortical excitability in patients with relapsing-remitting and secondary progressive multiple sclerosis. J Neurol. (2009) 256:933-8. doi: 10.1007/s00415-009-5047-0
70. Ayache SS, Créange A, Farhat WH, Zouari HG, Lesage C, Palm U, Abdellaoui M, Lefaucheur JP. Cortical excitability changes over time in progressive multiple sclerosis. Funct Neurol. (2015) 30:257-63. doi: 10.11138/fneur/2015.30.4.257
71. Schmierer K, Niehaus L, Röricht S, Meyer BU. Conduction deficits of callosal fibres in early multiple sclerosis. J Neurol Neurosurg Psychiatry. (2000) 68:633-8. doi: 10.1136/jnnp.68.5.633
72. Jung P, Beyerle A, Humpich M, Neumann-Haefelin T, Lanfermann H, Ziemann U. Ipsilateral silent period: a marker of callosal conduction abnormality in early relapsing-remitting multiple sclerosis? J Neurol Sci. (2006) 250:133-9. doi: 10.1016/j.jns.2006.08.008
73. Wahl M, Hübers A, Lauterbach-Soon B, Hattingen E, Jung P, Cohen LG, et al. Motor callosal disconnection in early relapsing-remitting multiple sclerosis. Hum Brain Mapp. (2011) 32:846-55. doi: 10.1002/hbm.21071
74. Daskalakis ZJ, Christensen BK, Fitzgerald PB, Roshan L, Chen R. The mechanisms of interhemispheric inhibition in the human motor cortex. J Physiol. (2002) 543(Pt 1):317-26.
75. Ayache SS, Chalah MA, Al-Ani T, Farhat WH, Zouari HG, Créange A, et al. Tremor in multiple sclerosis: The intriguing role of the cerebellum. J Neurol Sci. (2015) 358:351-6. doi: 10.1016/j.jns.2015.09.360
76. Mori F, Kusayanagi H, Monteleone F, Moscatelli A, Nicoletti CG, Bernardi G, et al. Short interval intracortical facilitation correlates with the degree of disability in multiple sclerosis. Brain Stimul. (2013) 6:67-71. doi: 10.1016/j.brs.2012.02.001
77. Ayache SS, Créange A, Farhat WH, Zouari HG, Mylius V, Ahdab R, et al. Relapses in multiple sclerosis: effects of high-dose steroids on cortical excitability. Eur J Neurol. (2014) 21:630-6. doi: 10.1111/ene.12356
78. Chaves AR, Wallack EM, Kelly LP, Pretty RW, Wiseman HD, Chen A, et al. Asymmetry of Brain Excitability: A New Biomarker that Predicts Objective and Subjective Symptoms in Multiple Sclerosis. Behav Brain Res. (2019) 359:281-91. doi: 10.1016/j.bbr.2018.11.005
79. Induruwa I, Constantinescu CS, Gran B. Fatigue in multiple sclerosis - a brief review. J Neurol Sci. (2012). 323:9-15. doi: 10.1016/j.jns.2012.08.007
80. Kos D, Kerckhofs E, Nagels G, D'hooghe MB, Ilsbroukx S. Origin of Fatigue in Multiple Sclerosis: Review of the Literature. Neurorehabil Neural Repair. (2008). 22, 91-100. doi: 10.1177/1545968306298934
81. Vucic S, Burke D, Kiernan MC. Fatigue in multiple sclerosis: mechanisms and management. Clin Neurophysiol. (2010) 121:809-17. doi: 10.1016/j.clinph.2009.12.013
82. Chalah MA, Kauv P, Créange A, Hodel J, Lefaucheur JP, Ayache SS. Neurophysiological, radiological and neuropsychological evaluation of fatigue in multiple sclerosis. Mult Scler Relat Disord. (2019) 28:145-52. doi: 10.1016/j.msard.2018.12.029
83. Chaves AR, Kelly LP, Moore CS, Stefanelli M, Ploughman M. Prolonged cortical silent period is related to poor fitness and fatigue, but not tumor necrosis factor, in Multiple Sclerosis. Clin Neurophysiol. (2019) 130:474-83. doi: 10.1016/j.clinph.2018.12.015
84. Di Filippo M, Portaccio E, Mancini A, Calabresi P. Multiple sclerosis and cognition: synaptic failure and network dysfunction. Nat Rev Neurosci. (2018) 19:599-609. doi: 10.1038/s41583-018-0053-9
85. Tokimura H, Di Lazzaro V, Tokimura Y, Oliviero A, Profice P, Insola A, Mazzone P, Tonali P, Rothwell JC. Short latency inhibition of human hand motor cortex by somatosensory input from the hand. J Physiol. 523:503-13.
86. Cucurachi L, Immovilli P, Granella F, Pavesi G, Cattaneo L. Short-latency afferent inhibition predicts verbal memory performance in patients with multiple sclerosis. J Neurol. (2008) 255:1949-56. doi: 10.1007/s00415-008-0041-5
87. Di Lazzaro V, Pilato F, Dileone M, Saturno E, Oliviero A, Marra C, Daniele A, Ranieri F, Gainotti G, Tonali PA. In vivo cholinergic circuit evaluation in frontotemporal and Alzheimer dementias. Neurology. (2006) 66:1111-3. doi: 10.1212/01.wnl.0000204183.26231.23
88. Chalah MA, Palm U, Lefaucheur JP, Créange A, Ayache SS. Interhermispheric inhibition predicts anxiety levels in multiple sclerosis: A corticospinal excitability study. Brain Res. (2018) 1699:186-194. doi: 10.1016/j.brainres.2018.08.029
89. Szczucinski A, Losy J. Chemokines and chemokine receptors in multiple sclerosis. Potential targets for new therapies. Acta Neurol Scand. (2007) 115:137-46. https://doi.org/10.1111/j.1600-0404.2006.00749.x
90. Dihb-Jalbut S, Arnold DL, Cleveland DW, Fisher M, Friedlander RM, Mouradianet MM, et al. Neurodegeneration and neuroprotection in multiple sclerosis and other neurodegenerative diseases. J Neuroimmunol. (2006) 176:198–215. https://doi.org/10.1016/j.jneuroim.2006.03.027.
91. Maimone D, Gregory S, Arnason BG, Reder AT. Cytokine levels in the cerebrospinal fluid and serum of patients with multiple sclerosis. J Neuroimmunol. (1991) 32:67–74. https://doi.org/10.1016/0165-5728(91)90073-G
92. Matejčíková Z, Mareš J, Sládková V, Svrčinová T, VyslouŽilová J, Zapletalová J, et al. Cerebrospinal fluid and serum levels of interleukin-8 in patients with multiple sclerosis and its correlation with Q-albumin. Mult Scler Relat Disord. (2017) 14:12–5. doi: 10.1016/j.msard.2017.03.007
93. Kothur K, Wienholt L, Brilot F, Dale RC. CSF cytokines/chemokines as biomarkers in neuroinflammatory CNS disorders: a systematic review. Cytokine. (2016) 7:227–237. doi: 10.1016/j.cyto.2015.10.001
94. Göbel K, Ruck T, Meuth SG. Cytokine signaling in multiple sclerosis: Lost in translation. Mult Scler J. (2018) 24:432–439. https://doi.org/10.1177/1352458518763094
95. Cannella B, Raine CS. Multiple sclerosis: cytokine receptors on oligodendrocytes predict innate regulation. Ann Neurol. (2004) J55:46-57. doi: 10.1002/ana.10764
96. Werneburg S, Feinberg PA, Johnson KM, Schafer DP. A microglia-cytokine axis to modulate synaptic connectivity and function. Curr Opin Neurobiol. (2017) 47:138-45. doi: 10.1016/j.conb.2017.10.002
97. Vezzani A, Balosso S, Ravizza T. The role of cytokines in the pathophysiology of epilepsy. Brain Behav Immun. (2008) 22:797-803. doi: 10.1016/j.bbi.2008.03.009
98. Vezzani A, Viviani B. Neuromodulatory properties of inflammatory cytokines and their impact on neuronal excitability. Neuropharmacology. (2015) 96:70-82. doi: 10.1016/j.neuropharm.2014.10.027
99. Wu Y, Dissing-Olesen L, MacVicar BA, Stevens B. Microglia: Dynamic Mediators of Synapse Development and Plasticity. Trends Immunol. (2015) 36:605-613. doi: 10.1016/j.it.2015.08.008
100. Tian L, Ma L, Kaarela T, Li Z. Neuroimmune crosstalk in the central nervous system and its significance for neurological diseases. J Neuroinflammation. (2012) 9:155. doi: 10.1186/1742-2094-9-155
101. Rizzo FR, Musella A, De Vito F, Fresegna D, Bullitta S, Vanni V, et al. Tumor Necrosis Factor and Interleukin-1β Modulate Synaptic Plasticity during Neuroinflammation. Neural Plast. (2018) 2018:8430123. doi: 10.1155/2018/8430123
102. Mandolesi G, Musella A, Gentile A, Grasselli G, Haji N, Sepman H, et al. Interleukin-1β alters glutamate transmission at purkinje cell synapses in a mouse model of multiple sclerosis. J Neurosci. (2013) 33:12105-21. doi: 10.1523/JNEUROSCI.5369-12.2013
103. Takayasu Y, Iino M, Ozawa S. Roles of glutamate transporters in shaping excitatory synaptic currents in cerebellar Purkinje cells. Eur J Neurosci. (2004) 19:1285–95. doi: 10.1111/j.1460-9568.2004.03224.x
104. Seckinger P, Lowenthal JW, Williamson K, Dayer JM, MacDonald HR. A urine inhibitor of interleukin 1 activity that blocks ligand binding. J Immunol. (1987) 139:1546–9.
105. Furlan R, Bergami A, Brambilla E, Butti E, De Simoni MG, Campagnoli M, et al. HSV-1-mediated IL-1 receptor antagonist gene therapy ameliorates MOG(35–55)-induced experimental autoimmune encephalomyelitis in C57BL/6 mice. Gene Ther (2007) 14:93–8. doi: 10.1038/sj.gt.3302805
106. Rossi S, Muzio L, De Chiara V, Grasselli G, Musella A, Musumeci G, et al. Impaired striatal GABA transmission in experimental autoimmune encephalomyelitis. Brain Behav Immun. (2011) 25:947-56. doi: 10.1016/j.bbi.2010.10.004
107. Mandolesi G, Grasselli G, Musella A, Gentile A, Musumeci G, Sepman H, et al. GABAergic signaling and connectivity on Purkinje cells are impaired in experimental autoimmune encephalomyelitis. Neurobiol Dis. (2012) 46:414-24. doi: 10.1016/j.nbd.2012.02.005
108. Bhat R, Axtell R, Mitra A, Miranda M, Lock C, Tsien RW, et al. Inhibitory role for GABA in autoimmune inflammation. Proc Natl Acad Sci USA. (2010) 107:2580–5. doi: 10.1073/pnas.0915139107
109. Rossi S, Furlan R, De Chiara V, Motta C, Studer V, Mori F, et al. Interleukin-1β causes synaptic hyperexcitability in multiple sclerosis. Ann Neurol. (2012) 71:76-83. doi: 10.1002/ana.22512
110. Gentile A, De Vito F, Fresegna D, Rizzo FR, Bullitta S, Guadalupi L, et al. Peripheral T cells from multiple sclerosis patients trigger synaptotoxic alterations in central neurons. Neuropathol Appl Neurobiol. (2019) [Epub ahead of print] doi: 10.1111/nan.12569
111. Caramia MD, Palmieri MG, Desiato MT, Boffa L, Galizia P, Rossini PM, et al. Brain excitability changes in the relapsing and remitting phases of multiple sclerosis: a study with transcranial magnetic stimulation. Clin Neurophysiol. (2004) 115:956-65. doi: 10.1016/j.clinph.2003.11.024
112. Rossi S, Studer V, Motta C, Germani G, Macchiarulo G, Buttari F, et al. Cerebrospinal fluid detection of interleukin-1β in phase of remission predicts disease progression in multiple sclerosis. J Neuroinflammation. (2014) 11:32. doi: 10.1186/1742-2094-11-32
113. Pittaluga A. CCL5-Glutamate Cross-Talk in Astrocyte-Neuron Communication in Multiple Sclerosis. Front Immunol. (2017) 8:1079. doi: 10.3389/fimmu.2017.01079
114. Mori F, Nisticò R, Nicoletti CG, Zagaglia S, Mandolesi G, Piccinin S, et al. RANTES correlates with inflammatory activity and synaptic excitability in multiple sclerosis. Mult Scler. (2016) 22:1405-12. doi: 10.1177/1352458515621796
115. Rossi S, Motta C, Studer V, Barbieri F, Buttari F, Bergami A, Sancesario G, Bernardini S, De Angelis G, Martino G, Furlan R, Centonze D. Tumor necrosis factor is elevated in progressive multiple sclerosis and causes excitotoxic neurodegeneration. Mult Scler. (2014) 20:304-12. doi: 10.1177/1352458513498128
116. Zhou Z, Peng X, Insolera R, Fink DJ, Mata M. IL-10 promotes neuronal survival following spinal cord injury. Exp Neurol. (2009) 220:183-90. doi: 10.1016/j.expneurol.2009.08.018
117. Lobo-Silva D, Carriche GM, Castro AG, Roque S, Saraiva M. Balancing the immune response in the brain: IL-10 and its regulation. J Neuroinflammation. (2016) 13:297. doi: 10.1186/s12974-016-0763-8
118. Tseng HC, Dichter MA. Platelet-derived growth factor-BB pretreatment attenuates excitotoxic death in cultured hippocampal neurons. Neurobiol Dis. (2005) 19:77–83. doi: 10.1016/j.nbd.2004.11.007
119. Cheng B, Mattson MP. PDGFs protect hippocampal neurons against energy deprivation and oxidative injury: evidence for induction of antioxidant pathways. J Neurosci. (1995) 15:7095-104.
Keywords: Transcranial magnetic stimulation (TMS), multiple sclerosis (MS), inflammation, synaptic transmission, cytokines
Citation: Stampanoni Bassi M, Buttari F, Gilio L, De Paolis N, Fresegna D, Centonze D and Iezzi E (2020) Inflammation and Corticospinal Functioning in Multiple Sclerosis: A TMS Perspective. Front. Neurol. 11:566. doi: 10.3389/fneur.2020.00566
Received: 31 January 2020; Accepted: 19 May 2020;
Published: 07 July 2020.
Edited by:
Ulrich Palm, Medical Park Chiemseeblick, GermanyCopyright © 2020 Stampanoni Bassi, Buttari, Gilio, De Paolis, Fresegna, Centonze and Iezzi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Diego Centonze, Y2VudG9uemVAdW5pcm9tYTIuaXQ=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.