
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurol. , 23 January 2020
Sec. Epilepsy
Volume 10 - 2019 | https://doi.org/10.3389/fneur.2019.01256
 Rosane Brondani1,2,3Andrea Garcia de Almeida1,2,3Pedro Abrahim Cherubini2,3,4
Rosane Brondani1,2,3Andrea Garcia de Almeida1,2,3Pedro Abrahim Cherubini2,3,4 Thaís Leite Secchi1,2,3,4Marina Amaral de Oliveira2Sheila Cristina Ouriques Martins1,3
Thaís Leite Secchi1,2,3,4Marina Amaral de Oliveira2Sheila Cristina Ouriques Martins1,3 Marino Muxfeldt Bianchin1,2,3,4*
Marino Muxfeldt Bianchin1,2,3,4*The effects of thrombolysis in seizure and epilepsy after acute ischemic stroke have been poorly explored. In this study, we examine risk factors and consequences of intravenous rt-PA for treatment of acute ischemic stroke. In a retrospective cohort study we evaluate risk factors for seizure and epilepsy after stroke thrombolysis, as well as the impact of seizures and epilepsy in outcome of stroke patients. In our cohort, mean age of patients was 67.2 years old (SD = 13.1) and 79 of them (51.6%) were male and. Initial NIHSS mean score were 10.95 (SD = 6.25). Three months NIHSS mean score was 2.09 (SD = 3.55). Eighty seven (56.9%) patients were mRS of 0–1 after thrombolysis. Hemorrhagic transformation was observed in 22 (14.4%) patients. Twenty-one (13.7%) patients had seizures and 15 (9.8%) patients developed epilepsy after thrombolysis. Seizures were independently associated with hemorrhagic transformation (OR = 3.26; 95% CI = 1.08–9.78; p = 0.035) and with mRS ≥ 2 at 3 months after stroke (OR = 3.51; 95% CI = 1.20–10.32; p = 0.022). Hemorrhagic transformation (OR = 3.55; 95% CI = 1.11–11.34; p = 0.033) and mRS ≥ 2 at 3 months (OR = 5.82; 95% CI = 1.45–23.42; p = 0.013) were variables independently associated with post-stroke epilepsy. In our study, independent risks factors for poor outcome in stroke thrombolysis were age (OR = 1.03; 95% CI = 1.01–1.06; p = 0.011), higher NIHSS (OR = 1.08; 95% CI = 1.03–1.14; p = 0.001), hemorrhagic transformation (OR = 2.33; 95% CI = 1.11–4.76; p = 0.024), seizures (OR = 3.07; 95% CI = 1.22–7.75; p = 0.018) and large cortical area (ASPECTS ≤ 7) (OR = 2.04; 95% CI = 1.04–3.84; p = 0.036). Concluding, in this retrospective cohort study, the neurological impairment after thrombolysis (but not before) and hemorrhagic transformation remained independent risk factors for seizures or post-stroke epilepsy after thrombolysis. Moreover, we observed that seizures emerged as an independent risk factor for poor outcome after thrombolysis therapy in stroke patients (OR = 3.07; 95% CI = 1.22–7.75; p = 0.018).
Stroke is a prevalent disorder, responsible for 9.5% of total deaths each year and is the leading cause of disability in the world (1, 2). After stroke, new onset epilepsy might affect a significant proportion of patients and due to large stroke prevalence, post-stroke epilepsy is one of the leading causes of new diagnoses of epilepsy in patients older than 65 years old (3–6). Seizures or post-stroke epilepsy adds additional burden to stroke patients (7). Both seizures and post-stroke epilepsy might increase stroke morbidity and mortality (8–14). Drugs used for epilepsy control might decrease rehabilitation and impair patient cognition, perhaps having impact in the quality of life of these patients (15–17).
Since the 1995 NINDS study, recombinant tissue plasminogen activator (rt-PA) has been indicated to treat acute ischemic stroke (AIS) (18). Thrombolysis treatment is associated with reduction of disability as measured by the modified Rankin Scale (mRS) (19). The ECASS (20–22), ATLANTIS (23, 24), and EPITHET (25) trials, alone or grouped in a systematic review with meta-analysis (26), confirmed benefits of stroke thrombolysis. Thrombolytic therapy, associated with development of stroke units (27) and specialization in stroke treatment (28, 29) improved stroke outcome. Thrombolysis therapy had impact not only in stroke disability as evaluated by mRS, but it improved overall quality of life in patients. In spite of being largely studied, some effects of reperfusion therapy have not been properly investigated. This is the case of acute seizure after stroke or post-stroke epilepsy, its incidence and its characteristics. In early times, relatively few works have investigated the development of seizure or epilepsy in patients submitted to thrombolysis (30–35). Even fewer studies have evaluated risk factors for acute seizures or post-stroke epilepsy and its characteristics after thrombolysis. While some authors have observed that rt-PA per se might have a protective impact on cerebral tissue (36) and acute seizures might be a marker of successful reperfusion (30, 37), others point out that rt-PA might be neurotoxic or might be a risk factor for post-stroke seizures (38). Moreover, Tan et al. designed one study that combined experimental and clinical evidence specifically projected to address the effect of thrombolysis in post-stroke seizures (34). By using transgenic mice and studying clinical thrombolysis, the authors concluded that overexpression of endogenous t-PA lowers seizure threshold, but does not influence epileptogenesis or the development of acquired post-stroke epilepsy. However, considering all these evidences, the impact of thrombolysis therapy in acute seizures or post-stroke epilepsy remains not fully understood and because of its importance, needs to be further studied.
Here we report results of a retrospective cohort-study of 153 patients submitted to thrombolysis therapy for ischemic stroke, having evaluated risk factors for seizures or epilepsy after AIS thrombolysis. We hope this study helps clarify the incidence rates and characteristics of acute seizures or post-stroke epilepsy in patients receiving thrombolysis therapy for treatment of stroke, also aiding in planning new strategies for reperfusion therapies for acute ischemic stroke.
Protocol of study was approved by the Ethics Committee of Hospital de Clínicas de Porto Alegre and it was conducted according to the principles expressed in the Declaration of Helsinki. All patients or legal representatives gave written informed consent to participate in this study.
After approval by the Ethics Committee of Hospital de Clinicas de Porto Alegre, we retrospectively evaluated 153 consecutive patients submitted to stroke thrombolysis from 2005 to 2011. After stroke patients were followed for at least 2 years. Among variables studied were age, sex, ethnicity, hypertension, diabetes mellitus, hypercholesterolemia, smoking, drinking alcohol, atrial fibrillation, and variables associated with stroke like National Institute of Health and Stroke Scale (NIHSS), stroke etiology, stroke vascular territories, stroke severity, hemorrhagic transformation, and thrombolysis outcome.
Patients were classified in three groups, according to the presence or absence of early-onset seizures (i.e., if seizures developed during the first 7 days after stroke), late onset-seizures (i.e., if seizures started after the first week), and post-stroke epilepsy. Post-stroke epilepsy was independent of the time of seizures onset, encompassing both types of patients; those patients with earlier seizures that continued to have seizures after the acute phase, as well as those patients that presented seizures after the first week after stroke. Thus, post-stroke epilepsy was considered if patients had recurrent seizures, showed seizures after attempts to withdraw antiepileptic drugs, or if patients were maintained in treatment with anti-epileptic drugs because of a great chance of seizure recurrence as evaluated by EEGs, neuroimaging findings, and physician evaluation. As a consequence, post-stroke epilepsy was defined according to the recommendations of the International League Against Epilepsy (39). Moreover, all patients were submitted to at least two EEG monitoring for at least 30 min. All patients had seizures of focal onset and thus seizures were classified as focal seizures. As video-EEG was not performed, further characteristics of the seizures (e.g., semiology) could not be precisely established. Patients with no seizures were compared to those who presented early seizure, late seizures or post stroke epilepsy in order to determine risk factors for development of seizures or post-stroke epilepsy and for studying other plausible associations.
Thrombolytic treatment was administered following the American guideline to thrombolysis in stroke (19). Briefly, patients received an rt-PA dose of 0.9 mg/kg within to 3 or 4.5 h from the onset of symptoms. Thrombolytic drug was administered over a period of 1 h to patients older than 18 years of age with a clinical diagnosis of AIS, screened by computed tomography (19). Stroke severity was evaluated using the NIHSS, a scale of 0–42 points, where minimal or no symptoms are scored as 0 and points are added according to increasing stroke severity. NIHSS scale was validated for the Brazilian population and applied by a neurologist (40). NIHSS results were recorded before treatment and 3 months later. After thrombolysis, patients were admitted at the stroke unit or the intensive care unit. Response to treatment was evaluated according to the Rankin scale (41) and NIHSS scale 3 months after stroke. For analysis, a good outcome was considered if patients showed mRS scores of 0 or 1 and a bad outcome was defined as mRS of 2 or above. Bleeding was defined as any central nervous system bleeding, defined according to radiological criteria (42).
Categorical data were compared using Fisher's exact test, and results are expressed in odds ratio with 95% confidence interval. Numerical variables were compared by Student's independent t-test. This allowed identification of potential prognostic indicators. Variables with a significance level of p < 0.20 or lower on initial univariate analysis were included in a multivariate Cox proportional hazards regression model. This method allows testing the correlation of specific variables with outcome while taking into account any interactions and associations among those variables, and their variation with time. All results were considered significant if p < 0.05. The software SPSS version 20.0 was used for statistical analysis.
The characteristics of 153 patients included in the study are presented in Table 1. Seventy-four patients 74 (48.4%) were female and mean age of patients was 67.2 years-old (SD = 13.1). Frequency of vascular risk factors for stroke, among them hypertension, diabetes mellitus, hypercholesterolemia, smoking, drinking alcohol, and atrial fibrillation are also present in Table 1. NIHSS mean score was, 10.95 (SD = 6.25) and 2.09 (SD = 3.55) after 3 months. Hemorrhagic transformation occurred in 22 (14.4%) patients. A good outcome, defined by mRS of 0–1, was observed in 87 (56.9%) patients.
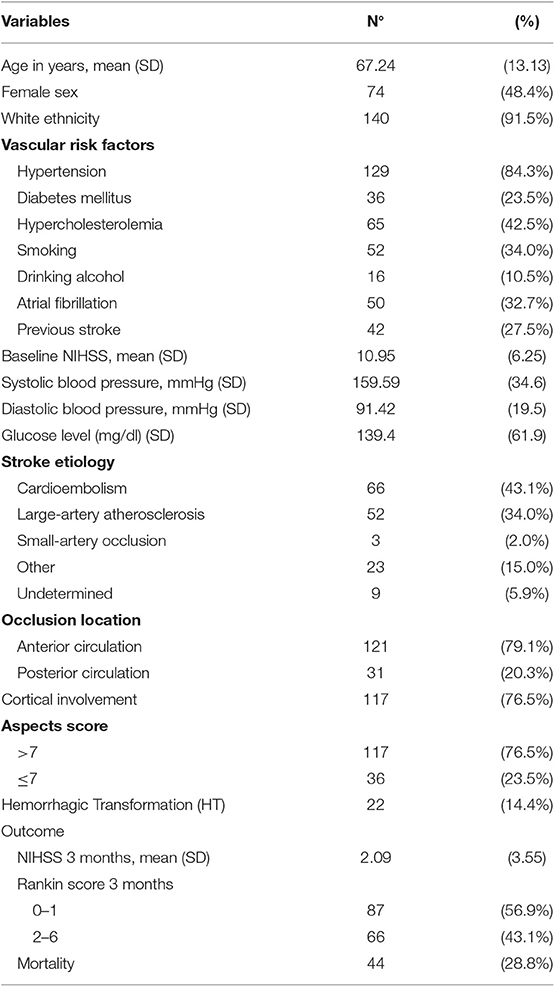
Table 1. Characteristics of 153 patients treated with rt-PA.
Of 153 patients, 21 (13.7%) presented seizures. Seizures were classified as focal with aware and motor onset with clonic facial and arm movements in two patients. Eleven patients had focal seizures, with impaired awareness and motor onset with clonic facial and limb movements with posterior evolution to bilateral tonic-clonic seizures. Additionally, five patients had focal seizures with impaired awareness with no motor onset that evolved to bilateral tonic-clonic seizures. In three patients, the seizure onset was unknown and patients evolved possibly to bilateral tonic-clonic seizures, if one is considering that the onset was probably focal. Table 2 presents distribution of seizures according to variables studied. Seizures were more prone to occur in patients with diabetes, in those with higher NIH stroke scores at first evaluation, and also after 3 months. AIS that involved cortical areas or those with hemorrhagic transformation were also more frequently associated with seizures. No significant differences were observed in the other parameters investigated. Moreover, seizures could not be attributed to renal dysfunction or blood sodium abnormalities. In patients that had seizures, the mean blood creatine 24 h before seizures was 1.03 mg/dl (minimum = 0.4 mg/dl and maximum = 1.9 mg/dl; SD = 0.32), the mean blood urea was 40.76 mg/dl (minimum = 24 mg/dl and maximum = 60 mg/dl; SD = 11.09), and the mean blood sodium was 140.38 mEq/L (minimum = 135.00 mEq/L and maximum = 145.00 mEq/L; SD = 2.49). These values were not different from those of patients that had no seizures. As stroke thrombolysis outcome 3 months later was measured using NIHSS and also mRS, only mRS, dichotomized in favorable or unfavorable outcome, was included in the regression model.
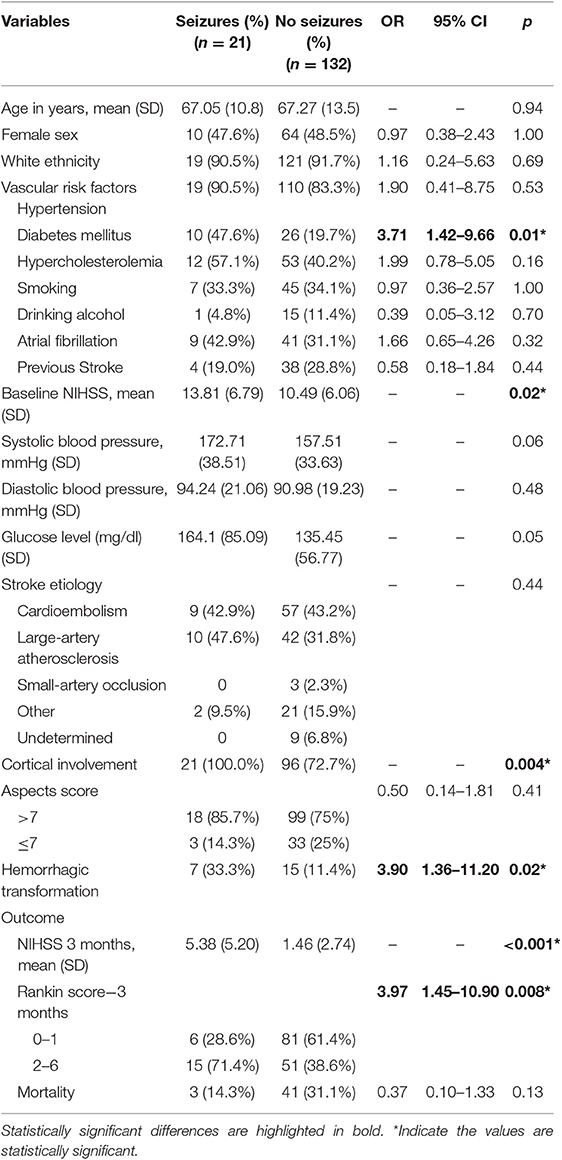
Table 2. Variables according with seizures.
Table 3 presents distribution of patients according with presence of early or late seizures. Four patients showed seizures during first 7 days after stroke (early seizures) while 17 patients showed seizures after 7 days of the stroke (late seizures). Interestingly, those patients who presented early seizures showed a trend to better thrombolysis outcome. In spite of this, no significant differences were observed in the parameters investigated (Table 3).

Table 3. Variables according with early or late seizures.
Of 153 patients, 15 presented epilepsy. Table 4 presents post-stroke epilepsy according to clinical and acute stroke variables studied. Factors associated with post-stroke epilepsy after thrombolysis in AIS were hemorrhagic transformation, involvement of cortical areas, higher NIHSS at stroke onset and after 3 months, and mRS of 2 or higher 3 months after stroke. No significant differences were observed in the other parameters investigated. After Cox regression (Table 5), stroke severity, as defined by mRS 2 or higher 3 months after stroke and hemorrhagic transformation were the only two variables independently associated with seizures. As expected, only patients with cortical involvement presented seizures after stroke. As no one patient with noncortical involvement presented seizures, an odds ratio could not be adequately estimated. Also, including cortical involvement in logistic regression models resulted in multicollinearity and an absurdly high 95% confidence interval. For this reason, we did not include cortical involvement in the Cox regressions analysis. After Cox regression, mRS of 2 or higher 3 months after stroke and hemorrhagic transformation were the only two independent predictors of post-stroke epilepsy (Table 6). The effect of stroke cortical involvement was not included in the model, for reasons explained above, but it is presented as a variable associated with post-stroke epilepsy.
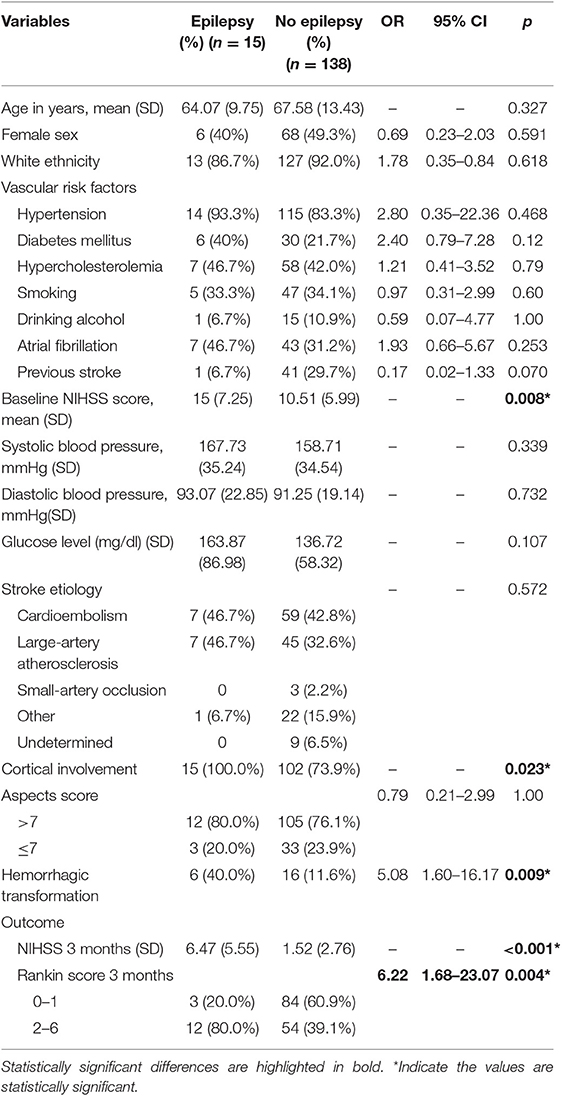
Table 4. Variables according epilepsy.
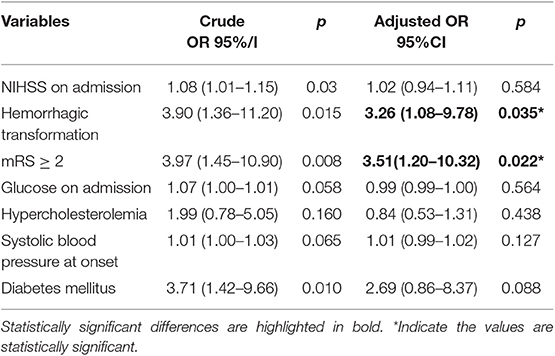
Table 5. Independent risk factors for seizures.
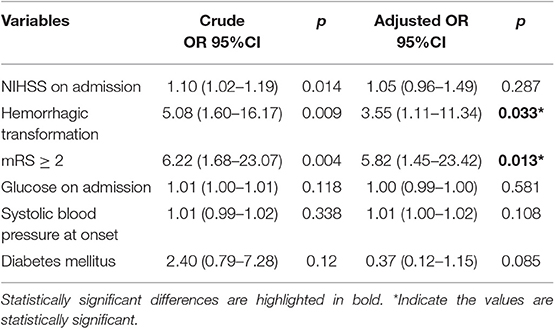
Table 6. Independent risk factors for epilepsy.
At this point, it was not established if seizures would be an independent risk factor for unfavorable outcome in stroke thrombolysis or, if alternatively, those patients who had larger strokes or those who had poor reperfusion after thrombolysis would be at risk for seizures. To solve this problem, we analyzed if seizures were an independent predictor for unfavorable thrombolysis outcome. After corrections for multiple comparisons, we concluded that seizure is effectively an isolated risk factor for unfavorable outcome after thrombolysis. In this analysis, NIHSS, hemorrhagic transformation, and size of stroke as evaluated by ASPECTS also emerged as independent risk factors for unfavorable outcome in stroke thrombolysis (Table 7).
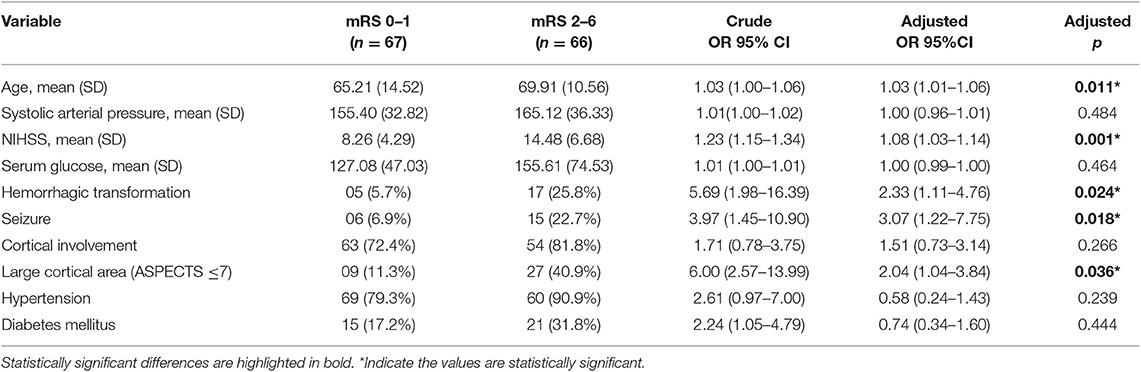
Table 7. Independent risk factor for unfavorable outcome in thrombolysis: the independent effect of seizures.
In our cohort, 21 (13.7%) patients had seizures and 15 (9.8%) patients developed epilepsy after thrombolysis for AIS treatment. Seizures were independently associated with hemorrhagic transformation and with mRS ≥ 2 at 3 months after stroke. Early seizures showed a trend to occur more often in patients who showed favorable outcome. Hemorrhagic transformation and unfavorable outcome, as measured by mRS ≥ 2 at 3 months, were variables independently associated with post-stroke epilepsy. An additional analysis confirmed that seizures were an independent factor for poor outcome in stroke thrombolysis.
Post-stroke seizure is a well-studied complication of stroke, but many questions remain to be solved, the main question being what defines early seizures, late seizures, or post-stroke epilepsy. These have been defined in heterogeneous ways in the literature, making it difficult to compare results and variables among studies. Here, we attempt to separate early or late seizures and also to evaluate post-stroke epilepsy. In studies from the last two decades, the frequency of seizures in non-thrombolyzed stroke patients range from 2 to 20% (7, 9, 43–70). In pre-thrombolysis years and after, reported risk factors for post-stroke seizures or epilepsy were multilobar involvement (43), embolic etiology (44), cortical involvement (7, 9, 43, 45, 46), headache and loss of consciousness during stroke (47), either female or male sex (45, 47, 48), hemorrhagic transformation (49), and severity of stroke (7, 11, 50–53). In spite of different variables, some of the parameters studied may reflect similar aspects of the same variable, for example severity of the event, extension of cortical involvement, and hemorrhagic transformation. The lack of modern statistical tools in earlier analysis make difficult for the identification of isolated risk factors for post-stroke seizures or post-stroke epilepsy. In a recent systematic review and meta-analysis, Zhang et al. described as risk factors for early post-stroke seizures hemorrhagic transformation, stroke severity, and alcoholism (54). In this same meta-analysis, risk factors for late seizures were cortical involvement and stroke severity (54). In our study, all patients with seizures or epilepsy had cortical involvement and the inclusion of cortical involvement in logistic regression models resulted in multicollinearity. Cortical involvement in stroke is perhaps better seen as a sine qua non condition for seizure or epilepsy to occur rather than as a risk factor such as others. In fact, it is reasonable to expect that virtually all patients with seizure or epilepsy would have some degree of cortical involvement. Although subcortical epilepsy does exist, it is extremely rare and should not affect post-stroke seizures or epilepsy rates. Thus, it is necessary, in the future, to evaluate specific sub-types of cortical regions and the extension of its involvement as risk factors for post-stroke seizures rather than the cortical involvement per se.
As large-scale reperfusion therapy is relatively recent, much less is known about seizures or epilepsy after AIS thrombolysis. First reports observed that seizures during or right after thrombolysis could be a marker of successful reperfusion (30, 37). If this would be common, it would be expected that reperfusion therapy would lead to seizure or post-stroke epilepsy increase. After these first observations, some recent studies reported on frequency of seizures or post-stroke epilepsy in AIS thrombolysis era (10, 31–35, 38, 71–78). The frequency of seizures after thrombolysis ranged from 4–15%, and it is in the range of pre-thrombolytic decades. The frequency of early seizures, defined as seizures which occurred during the first 7 days after stroke and thrombolysis, ranged from 2.5 to 5%. The frequency of late seizures, again described as seizures occurring after the first 7 days from stroke, ranged from 1.5 to 11.3% of patients. These studies also evaluated risk factors for seizure development in the thrombolysis scenario. In a case-control study of 28 patients submitted to thrombolysis and 100 controls, Alvarez et al. identified thrombolysis itself and cortical involvement as risk factors for seizures after reperfusion therapy (38). Other risk factors for seizures after stroke thrombolysis were atrial fibrillation (32), younger age, and higher NIHSS at arrival (33). Keller et al. (35) identified as independent risk factors for post-stroke epilepsy low Barthel Index at discharge, hemianopia, infection acquired during the hospital stay, and involvement of the temporal lobe or perirolandic cortex. In this study rt-PA was not an independent risk factor for post-stroke epilepsy. Tan et al. evaluated the role of rt-PA in development of post-stroke epilepsy in a controlled way (34). They study seizures after stroke in mice deficient in t-PA and in animals that overexpress t-PA. These authors also evaluated thrombolysis in a clinical scenario comparing post-stroke epilepsy in patients with or without thrombolysis (34). They concluded that therapeutic administration of t-PA does not influence the development of acquired post-stroke epilepsy. However, other authors have reported an increase in seizures incidence during the acute period of stroke after rt-PA (31, 38). Moreover, Naylor et al. reported that the risk of seizures after rt-PA extends further than the acute stage of stroke, and might occur over a 24-months period (71). Among the mechanisms involved in the effect of rt-PA in post-stroke increasing seizure risk are sudden change in cerebral perfusion which might be associated with a cascade of inflammatory responses, the development of the reperfusion syndrome and subsequent seizures and post-stroke epilepsy. In spite that rt-PA might show some toxicity, the similar rates of occurrence of post-stroke seizures between patients treated only with IA with those treated with IA plus rt-PA suggest that reperfusion, per se, might be the responsible for the increase of seizure frequency after rt-PA therapy (71).
In spite of earlier evidences that seizures might be a sign of successful reperfusion (30, 37), some authors suggest that patients who showed seizures after thrombolysis might present worst thrombolysis outcome when compared to patients without seizures (10, 32). In this venue, our results are in line with ENCHANTED trial that showed that seizures after stroke are associated with poor outcome (73). Since studies in post-stroke epilepsy after thrombolysis are few, recent, retrospective in design, and evaluate a relatively small number of patients, their findings need further confirmation. Unfortunately, large randomized controlled multicenter trials for stroke thrombolysis which confirmed the intravenous safety and efficacy of rt-PA for stroke did not report on seizure occurrence or post-stroke epilepsy. The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group (18), ECASS (20–22), ATLANTIS (23, 24) EPITHET trials (25), SITS-MOST (79), and SITS-ISTR (80).
Thus, the magnitude of seizure occurrence or post-stroke epilepsy and its impact on patient quality of life remains not fully studied, and prospective studies designed to assess the burden of post-stroke epilepsy in thrombolysis are still necessary. Eventually, these studies would be important for planning and developing new strategies for preventing seizures or epilepsy in AIS reperfusion scenario as well.
Taking all the data together, the clinical risk factors for seizures or post-stroke epilepsy seems to be related to the degree of cortical involvement, the size of the brain region involved and the efficacy of reperfusion. The sine qua non condition for post-stroke seizures seems to be related to the cortical involvement itself, for obvious reasons. In our study, neuroimaging of all patients with seizure or epilepsy showed cortical involvement. Secondly, seizures or epilepsy risk might be related to the extension of the cortical involvement. In the DECIMAL trial (DEcompressive Craniectomy In MALignant MCA Stroke), authors observed greater risk of seizures in patients with malignant middle cerebral artery stroke, independently of decompressive craniectomy, being 6 of 15 survivors (40%) with craniectomy and 2 of 4 survivors (50%) without decompressive hemicraniectomy (81). We have previously observed similar rates after decompressive craniectomy (82). Our data showed that initial NIHSS scores correlate with seizures or epilepsy development. However, Cox regression analysis showed that only residual deficits that remained after thrombolysis, as evaluated by mRS unfavorable outcome, were independently associated with seizures or post-stroke epilepsy. This suggests that when reperfusion therapy saves neural tissue, the chance of post-stroke epilepsy decreases. On the other hand, thrombolytic therapy is associated with an increased chance of hemorrhagic transformation in ischemic stroke. Bleeding, on its turn, is associated with increased chance of seizures or post-stroke epilepsy as observed in our study and in line with literature. This is further supported by higher rates of seizures or post-stroke epilepsy after hemorrhagic stroke when compared with ischemic stroke. Thus, patients who experience hemorrhagic transformation after thrombolysis might have an increased risk for seizures or post-stroke epilepsy. Considering hemorrhagic transformation after rt-PA, one might expect increased rates of seizures or post-stroke epilepsy. However, this might not be the case because of the neural tissue saving effects of thrombolysis that might well counterbalance its hemorrhagic effects. These possibilities are interesting matters for future research. Nevertheless, we observed an increased unfavorable outcome in patients who develop clinical seizures. This is an interesting finding, in line with the literature, and should also motivate future research.
We recognize that our work has limitations. This is a retrospective study with a relative small sample size, which resulted in lower precision and confidence interval very long. Moreover, negative associations need to be interpreted with caution because of lack of statistical power. Also, due to the small number of patients included in this study, we could not evaluate if seizures, as well as post-stroke epilepsy were both independent risk factors for poor outcome in ischemic stroke. However, we could observe interesting aspects of seizures or post-epilepsy in the thrombolysis scenario. Some of our findings corroborate the literature, and others are new and need confirmation.
In summary, in our study seizures or post-stroke epilepsy rates after thrombolysis are high, perhaps higher than in patients not submitted to thrombolysis. In our study, hemorrhagic transformation and degree of neurological compromise after thrombolysis, but not before, were the only two variables independently associated with seizures or post-stroke epilepsy. Importantly, we also observed that seizures were an independent risk factor associated with a less favorable outcome after thrombolysis therapy.
Protocol of study was approved by the Ethics Committee of Hospital de Clínicas de Porto Alegre and it was conducted according to the principles expressed in the Declaration of Helsinki. All patients or legal representatives gave written informed consent to participate in this study.
RB, AA, PC, TS, MO, SM, and MB: conception and design of the work, acquisition, analysis and interpretation of data for the work, and final approval of the version to be published. RB, TS, and MB: drafting the work and revising the manuscript.
Partial results of this study were presented at during World Congress of Neurology (WCN 2017) and were published in the Abstracts of the congress. This study was fully supported by the Brazilian Government research grant agencies CNPq, and FAPERGS. MB was further supported by CNPq (#485423/2012-0, #307084/2014-0, #438548/2018-3, #312683/2018-9) and PRONEM-FAPERGS/CNPq (#11/2043.0). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - BRAZIL (CAPES). Finance Code 01.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Feigin VL, Forouzanfar MH, Krishnamurthi R, Mensah GA, Connor M, Bennett DA, et al. Global and regional burden of stroke during 1990–2010: findings from the Global Burden of Disease Study 2010. Lancet. (2014) 383:245–54. doi: 10.1016/S0140-6736(13)61953-4
2. Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Blaha MJ, et al. Executive summary: heart disease and stroke statistics−2014 update: a report from the American Heart Association. Circulation. (2014) 129:399–410. doi: 10.1161/01.cir.0000442015.53336.12
3. Forsgren L, Bucht G, Eriksson S, Bergmark L. Incidence and clinical characterization of unprovoked seizures in adults: a prospective population-based study. Epilepsia. (1996) 37:224–9. doi: 10.1111/j.1528-1157.1996.tb00017.x
4. Ramsay RE, Rowan AJ, Pryor FM. Special considerations in treating the elderly patient with epilepsy. Neurology. (2004) 62:S24–9. doi: 10.1212/WNL.62.5_suppl_2.S24
5. Stefan H. Epilepsy in the elderly: facts and challenges. Acta Neurol Scand. (2011) 124:223–37. doi: 10.1111/j.1600-0404.2010.01464.x
6. Zou S, Wu X, Zhu B, Yu J, Yang B, Shi J. The pooled incidence of post-stroke seizure in 102 008 patients. Top Stroke Rehabil. (2015) 22:466–73. doi: 10.1179/1074935715Z.00000000062
7. Bladin CF, Alexandrov AV, Bellavance A, Bornstein N, Chambers B, Cote R, et al. Seizures after stroke: a prospective multicenter study. Arch Neurol. (2000) 57:1617–22. doi: 10.1001/archneur.57.11.1617
8. Arboix A, Garcia-Eroles L, Massons JB, Oliveres M, Comes E. Predictive factors of early seizures after acute cerebrovascular disease. Stroke. (1997) 28:1590–4. doi: 10.1161/01.STR.28.8.1590
9. Labovitz DL, Hauser WA, Sacco RL. Prevalence and predictors of early seizure and status epilepticus after first stroke. Neurology. (2001) 57:200–6. doi: 10.1212/WNL.57.2.200
10. Gensicke H, Seiffge DJ, Polasek AE, Peters N, Bonati LH, Lyrer PA, et al. Long-term outcome in stroke patients treated with IV thrombolysis. Neurology. (2013) 80:919–25. doi: 10.1212/WNL.0b013e3182840c35
11. Huang CW, Saposnik G, Fang J, Steven DA, Burneo JG. Influence of seizures on stroke outcomes: a large multicenter study. Neurology. (2014) 82:768–76. doi: 10.1212/WNL.0000000000000166
12. Arntz RM, Rutten-Jacobs LC, Maaijwee NA, Schoonderwaldt HC, Dorresteijn LD, van Dijk EJ, et al. Poststroke epilepsy is associated with a high mortality after a stroke at young age: follow-up of transient ischemic attack and stroke patients and unelucidated risk factor evaluation study. Stroke. (2015) 46:2309–11. doi: 10.1161/STROKEAHA.115.010115
13. Leung T, Leung H, Soo YO, Mok VC, Wong KS. The prognosis of acute symptomatic seizures after ischaemic stroke. J Neurol Neurosurg Psychiatry. (2017) 88:86–94. doi: 10.1136/jnnp-2015-311849
14. Bryndziar T, Sedova P, Kramer NM, Mandrekar J, Mikulik R, Brown RD Jr, et al. Seizures following ischemic stroke: frequency of occurrence and impact on outcome in a long-term population-based study. J Stroke Cerebrovasc Dis. (2016) 25:150–6. doi: 10.1016/j.jstrokecerebrovasdis.2015.09.008
15. Ryvlin P, Montavont A, Nighoghossian N. Optimizing therapy of seizures in stroke patients. Neurology. (2006) 67:S3–9. doi: 10.1212/WNL.67.12_suppl_4.S3
16. Gilad R. Management of seizures following a stroke: what are the options? Drugs Aging. (2012) 29:533–8. doi: 10.2165/11631540–000000000-00000
17. Nadeau SE, Lu X, Dobkin B, Wu SS, Dai YE, Duncan PW, et al. A prospective test of the late effects of potentially antineuroplastic drugs in a stroke rehabilitation study. Int J Stroke. (2012) 9:449–56. doi: 10.1111/j.1747-4949.2012.00920.x
18. The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. N Engl J Med. (1995) 333:1581–7. doi: 10.1056/NEJM199512143332401
19. Jauch EC, Saver JL, Adams HP Jr, Bruno A, Connors JJ, Demaerschalk BM, et al. Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. (2013) 44:870–47. doi: 10.1161/STR.0b013e318284056a
20. Hacke W, Kaste M, Fieschi C, Toni D, Lesaffre E, von Kummer R, et al. Intravenous thrombolysis with recombinant tissue plasminogen activator for acute hemispheric stroke. The European Cooperative Acute Stroke Study (ECASS). JAMA. (1995) 274:1017–25. doi: 10.1001/jama.1995.03530130023023
21. Hacke W, Kaste M, Fieschi C, von Kummer R, Davalos A, Meier D, et al. Randomised double-blind placebo-controlled trial of thrombolytic therapy with intravenous alteplase in acute ischaemic stroke (ECASS II). Second European-Australasian Acute Stroke Study Investigators. Lancet. (1998) 352:1245–51. doi: 10.1016/S0140-6736(98)08020-9
22. Hacke W, Kaste M, Bluhmki E, Brozman M, Davalos A, Guidetti D, et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med. (2008) 359:1317–29. doi: 10.1056/NEJMoa0804656
23. Clark WM, Wissman S, Albers GW, Jhamandas JH, Madden KP, Hamilton S. Recombinant tissue-type plasminogen activator (Alteplase) for ischemic stroke 3 to 5 hours after symptom onset. The ATLANTIS Study: a randomized controlled trial. Alteplase Thrombolysis for Acute Noninterventional Therapy in Ischemic Stroke. JAMA. (1999) 282:2019–26. doi: 10.1001/jama.282.21.2019
24. Clark WM, Albers GW, Madden KP, Hamilton S. The rtPA (alteplase) 0- to 6-hour acute stroke trial, part A (A0276g): results of a double-blind, placebo-controlled, multicenter study. Thromblytic therapy in acute ischemic stroke study investigators. Stroke. (2000) 31: 811–6. doi: 10.1161/01.STR.31.4.811
25. Davis SM, Donnan GA, Parsons MW, Levi C, Butcher KS, Peeters A, et al. Effects of alteplase beyond 3 h after stroke in the Echoplanar Imaging Thrombolytic Evaluation Trial (EPITHET): a placebo-controlled randomised trial. Lancet Neurol. (2008) 7:299–309. doi: 10.1016/S1474-4422(08)70044-9
26. Lees KR, Bluhmki E, von Kummer R, Brott TG, Toni D, Grotta JC, et al. Time to treatment with intravenous alteplase and outcome in stroke: an updated pooled analysis of ECASS, ATLANTIS, NINDS, and EPITHET trials. Lancet. (2010) 375:1695–703. doi: 10.1016/S0140-6736(10)60491-6
27. Langhorne P, Williams BO, Gilchrist W, Howie K. Do stroke units save lives? Lancet. (1993) 342:395–8. doi: 10.1016/0140-6736(93)92813-9
28. Bianchin MM, Spanis CW. Patients with acute stroke should see a specialist. Lancet. (1998) 351:681. doi: 10.1016/S0140-6736(05)78473-7
29. Bianchin MM, Spanis CW. Stroke thrombolysis and the stroke specialist. Mayo Clin Proc. (1998) 73:705–6. doi: 10.1016/S0025-6196(11)64901-X
30. Rodan LH, Aviv RI, Sahlas DJ, Murray BJ, Gladstone JP, Gladstone DJ. Seizures during stroke thrombolysis heralding dramatic neurologic recovery. Neurology. (2006) 67:2048–9. doi: 10.1212/01.wnl.0000247231.25231.2e
31. De Reuck J, Van Maele G. Acute ischemic stroke treatment and the occurrence of seizures. Clin Neurol Neurosurg. (2010) 112:328–31. doi: 10.1016/j.clineuro.2010.01.004
32. Couillard P, Almekhlafi MA, Irvine A, Jette N, Pow J, St. Germaine-Smith C, et al. Subacute seizure incidence in thrombolysis-treated ischemic stroke patients. Neurocrit Care. (2012) 16:241–5. doi: 10.1007/s12028-011-9657-x
33. Jung S, Schindler K, Findling O, Mono ML, Fischer U, Gralla J, et al. Adverse effect of early epileptic seizures in patients receiving endovascular therapy for acute stroke. Stroke. (2012) 43:1584–90. doi: 10.1161/STROKEAHA.111.645358
34. Tan ML, Ng A, Pandher PS, Sashindranath M, Hamilton JA, Davis SM, et al. Tissue plasminogen activator does not alter development of acquired epilepsy. Epilepsia. (2012) 53:1998–2004. doi: 10.1111/j.1528-1167.2012.03635.x
35. Keller L, Hobohm C, Zeynalova S, Classen J, Baum P. Does treatment with t-PA increase the risk of developing epilepsy after stroke? J Neurol. (2015) 262:2364–72. doi: 10.1007/s00415-015-7850-0
36. Kim YH, Park JH, Hong SH, Koh JY. Nonproteolytic neuroprotection by human recombinant tissue plasminogen activator. Science. (1999) 284:647–50. doi: 10.1126/science.284.5414.647
37. Hafeez F, Razzaq MA, Levine RL, Ramirez MA. Reperfusion seizures: a manifestation of cerebral reperfusion injury after administration of recombinant tissue plasminogen activator for acute ischemic stroke. J Stroke Cerebrovasc Dis. (2007) 16:273–7. doi: 10.1016/j.jstrokecerebrovasdis.2007.07.007
38. Alvarez V, Rossetti AO, Papavasileiou V, Michel P. Acute seizures in acute ischemic stroke: does thrombolysis have a role to play? J Neurol. (2013) 260:55–61. doi: 10.1007/s00415-012-6583-6
39. Fisher RS, Acevedo C, Arzimanoglou A, Bogacz A, Cross JH, Elger CE, et al. ILAE official report: a practical clinical definition of epilepsy. Epilepsia. (2014) 55:475–82. doi: 10.1111/epi.12550
40. de Caneda MA, Fernandes JG, de Almeida AG, Mugnol FE. Reliability of neurological assessment scales in patients with stroke. Arq Neuropsiquiatr. (2006) 64:690–7. doi: 10.1590/S0004-282X2006000400034
41. Wilson WJ, Penn C, Saffer D, Aghdasi F. Improving the prediction of outcome in severe acute closed head injury by using discriminant function analysis of normal auditory brainstem response latencies and amplitudes. J Neurosurg. (2002) 97:1062–9. doi: 10.3171/jns.2002.97.5.1062
42. Fiorelli M, Bastianello S, von Kummer R, del Zoppo GJ, Larrue V, Lesaffre E, et al. Hemorrhagic transformation within 36 hours of a cerebral infarct: relationships with early clinical deterioration and 3-month outcome in the European Cooperative Acute Stroke Study I (ECASS I) cohort. Stroke. (1999) 30:2280–4. doi: 10.1161/01.STR.30.11.2280
43. Lancman ME, Golimstok A, Norscini J, Granillo R. Risk factors for developing seizures after a stroke. Epilepsia. (1999) 34:141–3. doi: 10.1111/j.1528-1157.1993.tb02386.x
44. So EL, Annegers JF, Hauser WA, O'Brien PC, Whisnant JP. Population-based study of seizure disorders after cerebral infarction. Neurology. (1996) 46:350–5. doi: 10.1212/WNL.46.2.350
45. Cheung CM, Tsoi TH, Au-Yeung M, Tang AS. Epileptic seizure after stroke in Chinese patients. J Neurol. (2003) 250:839–43. doi: 10.1007/s00415-003-1091-3
46. Kilpatrick CJ, Davis SM, Tress BM, Rossiter SC, Hopper JL, Vandendriesen ML. Epileptic seizures in acute stroke. Arch Neurol. (1990) 47:157–60. doi: 10.1001/archneur.1990.00530020053014
47. Giroud M, Gras P, Fayolle H, Andre N, Soichot P, Dumas R. Early seizures after acute stroke: a study of 1,640 cases. Epilepsia. (1994) 35:959–64. doi: 10.1111/j.1528-1157.1994.tb02540.x
48. Kotila M, Waltimo O. Epilepsy after stroke. Epilepsia. (1992) 33:495–8. doi: 10.1111/j.1528-1157.1992.tb01698.x
49. Alberti A, Paciaroni M, Caso V, Venti M, Palmerini F, Agnelli G. Early seizures in patients with acute stroke: frequency, predictive factors, and effect on clinical outcome. Vasc Health Risk Manag. (2008) 4:715–20. doi: 10.2147/VHRM.S244
50. Burn J, Dennis M, Bamford J, Sandercock P, Wade D, Warlow C. Epileptic seizures after a first stroke: the Oxfordshire Community Stroke Project. BMJ. (1997) 315:1582–7. doi: 10.1136/bmj.315.7122.1582
51. Conrad J, Pawlowski M, Dogan M, Kovac S, Ritter MA, Evers S. Seizures after cerebrovascular events: risk factors and clinical features. Seizure. (2013) 22:275–82. doi: 10.1016/j.seizure.2013.01.014
52. Lossius MI, Ronning OM, Slapo GD, Mowinckel P, Gjerstad L. Poststroke epilepsy: occurrence and predictors–a long-term prospective controlled study (Akershus Stroke Study). Epilepsia. (2005) 46:1246–51. doi: 10.1111/j.1528-1167.2005.57904.x
53. Reith J, Jorgensen HS, Nakayama H, Raaschou HO, Olsen TS. Seizures in acute stroke: predictors and prognostic significance. The Copenhagen Stroke Study. Stroke. (1997) 28:1585–9. doi: 10.1161/01.STR.28.8.1585
54. Zhang C, Wang X, Wang Y, Zhang JG, Hu W, Ge M, et al. Risk factors for post-stroke seizures: a systematic review and meta-analysis. Epilepsy Res. (2014) 108:1806–16. doi: 10.1016/j.eplepsyres.2014.09.030
55. Feyissa AM, Hasan TF, Meschia JF. Stroke-related epilepsy. Eur J Neurol. (2019) 26:18–e3. doi: 10.1111/ene.13813
56. Yang H, Rajah G, Guo A, Wang Y, Wang Q. Pathogenesis of epileptic seizures and epilepsy after stroke. Neurol Res. (2018) 40:426–32. doi: 10.1080/01616412.2018.1455014
57. Galovic M, Döhler N, Erdélyi-Canavese B, Felbecker A, Siebel P, Conrad J, et al. Prediction of late seizures after ischaemic stroke with a novel prognostic model (the SeLECT score): a multivariable prediction model development and validation study. Lancet Neurol. (2018) 17:143–52. doi: 10.1016/S1474-4422(17)30404-0
58. Tomari S, Tanaka T, Ihara M, Matsuki T, Fukuma K, Matsubara S, et al. Risk factors for post-stroke seizure recurrence after the first episode. Seizure. (2017) 52:22–6. doi: 10.1016/j.seizure.2017.09.007
59. Bentes C, Martins H, Peralta AR, Casimiro C, Morgado C, Franco AC, et al. Post-stroke seizures are clinically underestimated. J Neurol. (2017) 264:1978–85. doi: 10.1007/s00415-017-8586-9
60. Zhao Y, Li X, Zhang K, Tong T, Cui R. The Progress of Epilepsy after Stroke. Curr Neuropharmacol. (2018) 16:71–8. doi: 10.2174/1570159X15666170613083253
61. Stefanidou M, Das RR, Beiser AS, Sundar B, Kelly-Hayes M, Kase CS, et al. Incidence of seizures following initial ischemic stroke in a community-based cohort: The Framingham Heart Study. Seizure. (2017) 47:105–10. doi: 10.1016/j.seizure.2017.03.009
62. Chen Z, Churilov L, Koome M, Chen Z, Naylor J, Kwan P, et al. Post-stroke seizures is associated with low Alberta Stroke Program Early CT Score. Cerebrovasc Dis. (2017) 43:259–65. doi: 10.1159/000458449
63. Tanaka T, Ihara M. Post-stroke epilepsy. Neurochem Int. (2017) 107:219–28. doi: 10.1016/j.neuint.2017.02.002
64. Breitweg I, Stülpnagel CV, Pieper T, Lidzba K, Holthausen H, Staudt M, et al. Early seizures predict the development of epilepsy in children and adolescents with stroke. Eur J Paediatr Neurol. (2017) 21:465–7. doi: 10.1016/j.ejpn.2016.12.007
65. Alme KN, Engelsen BA, Naik M, Naess H. Identifying patients at risk of acute symptomatic seizure after ischemic stroke. Acta Neurol Scand. (2017) 136:265–71. doi: 10.1111/ane.12721
66. Kim HJ, Park KD, Choi KG, Lee HW. Clinical predictors of seizure recurrence after the first post-ischemic stroke seizure. BMC Neurol. (2016) 16:212. doi: 10.1186/s12883-016-0729-6
67. Ferlazzo E, Gasparini S, Beghi E, Sueri C, Russo E, Leo A, et al. Epilepsy in cerebrovascular diseases: Review of experimental and clinical data with meta-analysis of risk factors. Epilepsia. (2016) 57:1205–14. doi: 10.1111/epi.13448
68. Pitkänen A, Roivainen R, Lukasiuk K. Development of epilepsy after ischaemic stroke. Lancet Neurol. (2016) 15:185–97. doi: 10.1016/S1474-4422(15)00248-3
69. Serafini A, Gigli GL, Gregoraci G, Janes F, Cancelli I, Novello S, et al. Are early seizures predictive of epilepsy after a stroke? Results of a population-based study. Neuroepidemiology. (2015) 45:50–8. doi: 10.1159/000382078
70. Tanaka T, Yamagami H, Ihara M, Motoyama R, Fukuma K, Miyagi T, et al. Seizure outcomes and predictors of recurrent post-stroke seizure: a retrospective observational cohort study. PLoS ONE. (2015) 10:e0136200. doi: 10.1371/journal.pone.0136200
71. Naylor J, Thevathasan A, Churilov L, Guo R, Xiong Y, Koome M, et al. Association between different acute stroke therapies and development of post stroke seizures. BMC Neurol. (2018) 18:61. doi: 10.1186/s12883-018-1064-x
72. Chen Z, Churilov L, Chen Z, Naylor J, Koome M, Yan B, et al. Association between implementation of a code stroke system and poststroke epilepsy. Neurology. (2018) 90:e1126–33. doi: 10.1212/WNL.0000000000005212
73. Xu Y, Hackett ML, Chalmers J, Lindley RI, Wang X, Li Q, et al. Frequency, determinants, and effects of early seizures after thrombolysis for acute ischemic stroke: the ENCHANTED trial. Neurol Clin Pract. (2017) 7:324–32. doi: 10.1212/CPJ.0000000000000384
74. Ducci RD, Lange MC, Germiniani FMB, Zétola VHF. Predictors of dependence after MCA ischemic stroke submitted to thrombolysis. Neurol Res. (2018) 40:97–101. doi: 10.1080/01616412.2017.1402534
75. Nesselroth D, Gilad R, Namneh M, Avishay S, Eilam A. Estimation of seizures prevalence in ischemic strokes after thrombolytic therapy. Seizure. (2018) 62:91–4. doi: 10.1016/j.seizure.2018.09.001
76. Castro-Apolo R, Huang JF, Vinan-Vega M, Tatum WO. Outcome and predictive factors in post-stroke seizures: a retrospective case-control study. Seizure. (2018) 62:11–6. doi: 10.1016/j.seizure.2018.09.007
77. Pande SD, Lwin MT, Kyaw KM, Khine AA, Thant AA, Win MM, et al. Post-stroke seizure - Do the locations, types and managements of stroke matter? Epilepsia Open. (2018) 3:392–8. doi: 10.1002/epi4.12249
78. Lekoubou A, Awoumou JJ, Kengne AP. Incidence of seizure in stroke patients treated with recombinant tissue plasminogen activator: a systematic review and meta-analysis. Int J Stroke. (2017) 12:923–31. doi: 10.1177/1747493017729239
79. Wahlgren N, Ahmed N, Davalos A, Ford GA, Grond M, Hacke W, et al. Thrombolysis with alteplase for acute ischaemic stroke in the Safe Implementation of Thrombolysis in Stroke-Monitoring Study (SITS-MOST): an observational study. Lancet. (2007) 369:275–8. doi: 10.1016/S0140-6736(07)60149-4
80. Ahmed N, Wahlgren N, Grond M, Hennerici M, Lees KR, Mikulik R, et al. Implementation and outcome of thrombolysis with alteplase 3–4.5 h after an acute stroke: an updated analysis from SITS-ISTR. Lancet Neurol. (2010) 9:866–74. doi: 10.1016/S1474-4422(10)70165-4
81. Vahedi K, Vicaut E, Mateo J, Kurtz A, Orabi M, Guichard JP, et al. Sequential-design, multicenter, randomized, controlled trial of early decompressive craniectomy in malignant middle cerebral artery infarction (DECIMAL Trial). Stroke. (2007) 38:2506–17. doi: 10.1161/STROKEAHA.107.485235
Keywords: reperfusion therapy, post-stroke epilepsy, acute seizures, stroke outcome, rt-PA
Citation: Brondani R, de Almeida AG, Cherubini PA, Secchi TL, de Oliveira MA, Martins SCO and Bianchin MM (2020) Risk Factors for Epilepsy After Thrombolysis for Ischemic Stroke: A Cohort Study. Front. Neurol. 10:1256. doi: 10.3389/fneur.2019.01256
Received: 08 February 2019; Accepted: 12 November 2019;
Published: 23 January 2020.
Edited by:
Luiz Eduardo Betting, São Paulo State University, BrazilReviewed by:
Lécio Figueira Pinto, University of São Paulo, BrazilCopyright © 2020 Brondani, de Almeida, Cherubini, Secchi, de Oliveira, Martins and Bianchin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marino Muxfeldt Bianchin, bWJpYW5jaGluQGhjcGEuZWR1LmJy
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.