
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurol., 31 July 2019
Sec. Movement Disorders
Volume 10 - 2019 | https://doi.org/10.3389/fneur.2019.00799
 Igor Straka1
Igor Straka1 Michal Minár1
Michal Minár1 Matej Škorvánek2Milan Grofik3Katarína Danterová4Ján Benetin4Egon Kurča3Andrea Gažová5Veronika Boleková1,6
Matej Škorvánek2Milan Grofik3Katarína Danterová4Ján Benetin4Egon Kurča3Andrea Gažová5Veronika Boleková1,6 Kathryn A. Wyman-Chick7
Kathryn A. Wyman-Chick7 Ján Kyselovič8
Ján Kyselovič8 Peter Valkovič1,9*
Peter Valkovič1,9*Background: Once-daily treatment formulation is associated with better adherence in comparison to more complex medication regimens. The study aimed to detect the extent of adherence to pharmacotherapy in Parkinson disease (PD) patients who take a minimum of three daily doses of drugs, and to identify factors associated with lower levels of adherence.
Methods: The cohort was selected from non-demented PD patients. The 8-Item Morisky Medication Adherence Scale (MMAS-8), 8-Item Parkinson's Disease Questionnaire (PDQ-8), Geriatric Depression Scale (GDS), Non-Motor Symptom Assessment Scale (NMSS), 9-Item Wearing-off Questionnaire (WOQ-9), MDS-UPDRS III (motor examination), and IV (motor complications) scales were used in this study.
Results: From a total of 124 subjects, 33.9% reported a high level of adherence, 29.8% reported a medium level of adherence, and 36.3% reported a low level of adherence to their pharmacotherapy. The level of non-adherence correlated with gender, longer disease duration, higher scores of PDQ-8, NMSS, WOQ-9, and MDS-UPDRS IV. Detailed analysis of NMSS demonstrated a correlation between the level of adherence and domains sleep/fatigue, mood/cognition, perceptual problems/hallucinations, attention/memory, and urinary symptoms. Independent risk factors for non-adherence were excessive daytime sleepiness, anhedonia, and forgetfulness.
Conclusion: Non-adherence to more complicated medication regimens is frequent in PD patients and is associated with gender, longer PD duration, poorer quality of life, frequency and severity of non-motor symptoms, and more severe motor and non-motor fluctuations. Non-adherence was predicted by non-motor symptoms including fatigue, mood disturbances, and subjective cognitive complaints.
Parkinson's disease (PD) is a complex neurodegenerative disorder with various motor and non-motor symptoms. The goal of dopamine replacement therapy (L-DOPA, dopamine agonists, monoamine oxidase B inhibitors and catechol-O-methyltransferase inhibitors) is to achieve good clinical outcomes and to delay or alleviate long-term complications, particularly dyskinesias, and fluctuations in motor and non-motor symptoms. Pharmacologic treatment of non-motor symptoms (NMS) includes antidepressants, anxiolytics, antidementive agents, hypnotics, analgesics, drugs for autonomic dysfunction, and others (1). Adherence to pharmacotherapy describes the extent to which patient's behavior agrees with medical instruction of their physician (2). Non-adherence to pharmacotherapy is one of the most important medicine-related problems among patients with chronic conditions and is associated with a reduced quality of life (QoL), increased social burden, and higher health care costs. Unfortunately, physicians often underestimate the extent of non-adherence of their patients (3, 4). In PD patients, suboptimal adherence varies between 10 and 67% (5). A once-daily treatment regimen is associated with higher adherence in comparison to more complex regimens (6). With disease progression, the majority of PD patients use three or more daily doses of PD medications. We did not find consistency in the existing body of research concerning adherence to pharmacotherapy specifically among PD patients and there is a lack of research examining patients who are prescribed multiple daily doses of PD medications. The aim of this study was to (1) detect the extent of adherence to pharmacotherapy in patients with PD who take three or more daily doses of dopaminergic drugs, and (2) to identify factors associated with non-adherence.
We included 124 consecutive subjects (72 men and 52 women) with clinically established or clinically probable idiopathic PD diagnosed according to the MDS Clinical Diagnostic Criteria for PD (7). Our study was cross-sectional. Subjects were recruited from movement disorders outpatient departments of University Hospitals in Bratislava, Martin, and Košice (Slovakia). Study procedures were performed according to the declaration of Helsinki, ethical aspects were approved by local ethical committee for all centers, and all subjects signed written informed consent prior to inclusion into the study. We included patients without cognitive impairment (>26/30 points on the Mini Mental State Examination), on standard dopaminergic therapy with L-DOPA and/or dopamine agonists in minimum three daily doses (at stable doses and regimen for minimum of the last 4 weeks). Drugs for NMS were considered as PD therapy in the study context. Patients with four or more treated comorbidities (at stable doses and regimen for minimum of the last 4 weeks) were excluded from this study. Patients undergoing surgical or pump therapy for PD were also excluded.
All patients were examined using validated Slovak translations of the following screening and diagnostic instruments:
• Medication adherence was measured by the 8-Item Morisky Medication Adherence Scale (MMAS-8) (8, 9), cut-offs for levels of MMAS-8 were stratify 0 points for high level of adherence, 1–2 points for medium level of adherence, and 3–8 points for low level of adherence (8);
• QoL was measured by the 8-Item Parkinson's Disease Questionnaire (PDQ-8) (10, 11);
• Depression was measured by the Geriatric Depression Scale (GDS) (12–14);
• Frequency and severity of NMS was measured by the Non-Motor Symptom Assessment Scale for PD (NMSS) (11, 15);
• Motor impairment was measured by the MDS—Unified Parkinson's Disease Rating Scale (MDS-UPDRS)—part III: motor examination (MDS-UPDRS III),
• Motor complications were measured by the MDS-UPDRS part IV: motor complications (MDS-UPDRS IV) (16, 17),
• Wearing-off phenomenon (defined as motor and non-motor symptom fluctuations) was measured by the 9-Item Wearing-off Questionnaire (WOQ-9) (18, 19).
In all scales and questionnaires, higher scores were associated with more severe symptoms.
The MMAS-8, PDQ-8, and WOQ-9 were completed by patients or caregivers. The GDS, NMSS, and MDS-UPDRS III, IV were administered by trained investigators. Baseline characteristics (age, disease duration, previous medication history, comorbidities), and Hoehn & Yahr score (H&Y) were recorded by patients and checked by investigators.
Statistical analysis of the data was performed using IBM SPSS Statistics 24. Demographic and clinical parameters were analyzed using descriptive statistics. Data in our cohort according to Kolmogorov-Smirnov test were non-parametric. The strength of the relationship between the parameters was measured by Spearman's rank correlation coefficient (rs) and correlation ratio eta (η). Stepwise multiple regressions were performed to study the relationship between the MMAS-8 and observed parameters. The level of statistical significance was set at p ≤ 0.05.
Based on MMAS-8 scores, 42 patients (33.9%; MMAS-8 = 0 points) reported a high level of adherence, 37 patients (29.8%; MMAS-8 = 1–2 points) reported a medium level of adherence, and 45 patients (36.3%; MMAS-8 ≥ 3 points) reported a low level of adherence.
Demographic and clinical data of our cohort are presented in Table 1. The scores of non-adherence to PD medication (according to the MMAS-8) positively correlated with disease duration, QoL, depression, frequency and severity of NMS, motor and non-motor complications. We observed lower adherence in male subjects. We did not find any effect of educational attainment on the level of adherence (Table 2). Also, we did not find significant differences in LEDD and MDS-UPDRS III between the groups of high, medium, and low adherent patients in our cohort.
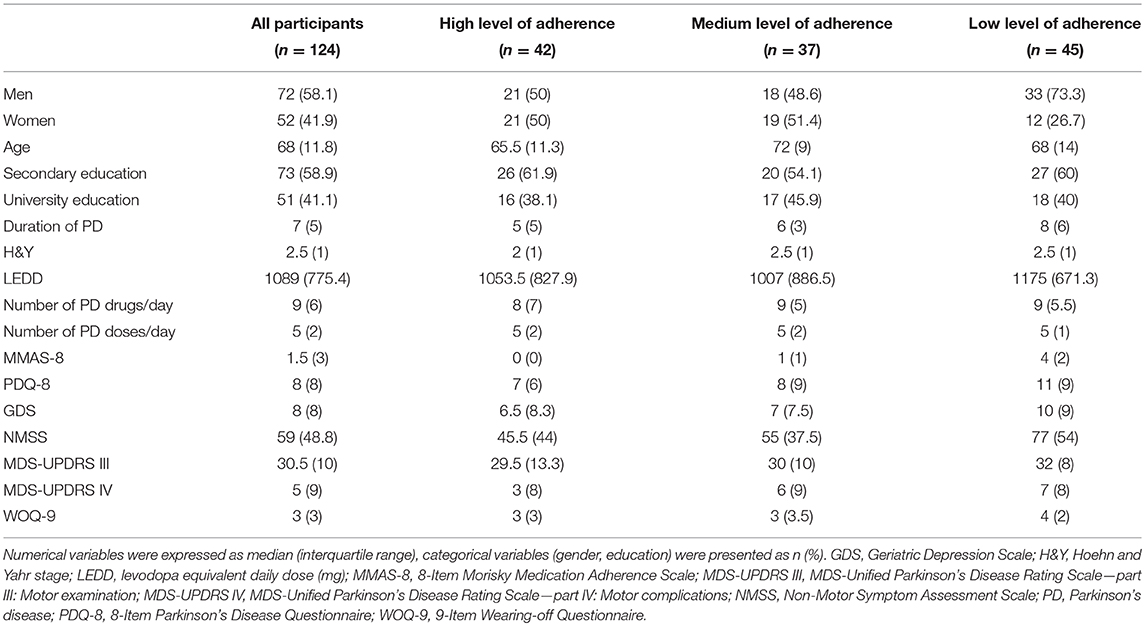
Table 1. Demographic and clinical data.
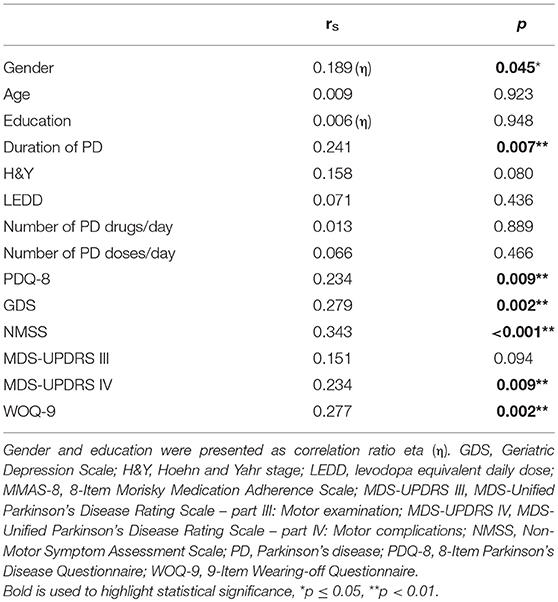
Table 2. Spearman's rank correlation coefficient (rs) of non-adherence to PD medication (MMAS-8) and other rated variables.
Only the frequency and severity of NMS predicted lower levels of adherence to pharmacotherapy (Table 3). From detailed analysis of NMS (based on NMSS scale), we found out significant correlations between the scores of non-adherences and domains sleep/fatigue, mood/cognition, perceptual problems/hallucinations, attention/memory, and urinary symptoms (Table 4). Analysis of isolated questions in NMSS scale of above-mentioned domains reported significant correlations with items 3–4, 10–14, 16–18, and 24 of the MMAS-8 (Table 5). In the stepwise multiple regressions, we confirmed that only: excessive daytime sleepiness, anhedonia, and forgetfulness (items 3, 12, and 18) predicted worse adherence to PD medication (Table 6).
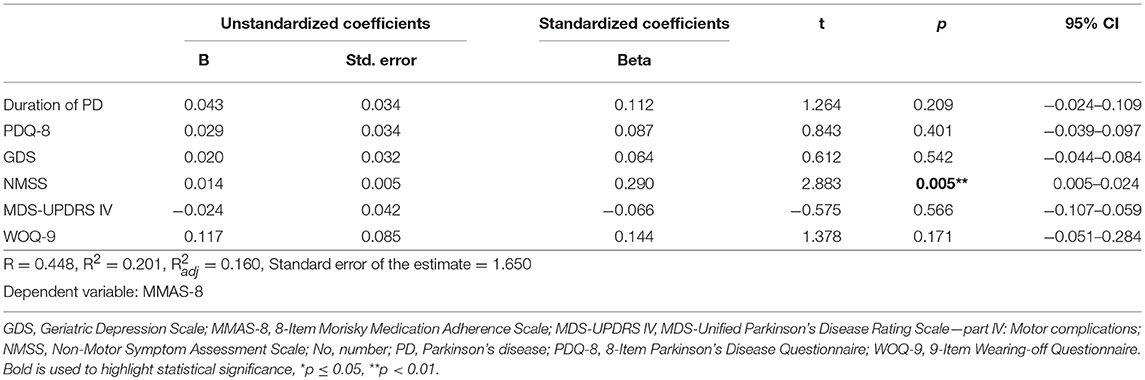
Table 3. Linear regression analysis of non-adherence to PD medication (MMAS-8) and factors associated with poorer adherence.
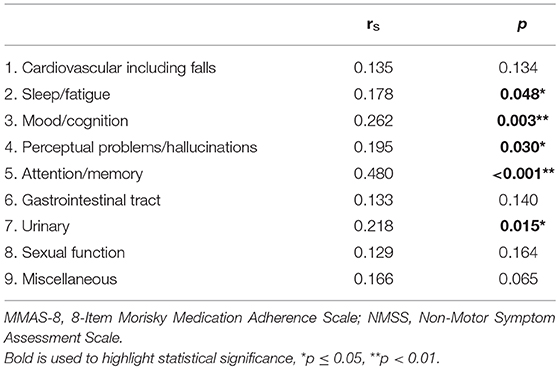
Table 4. Spearman's rank correlation coefficient (rs) of non-adherence to PD medication (MMAS-8) and domains of NMSS scale.
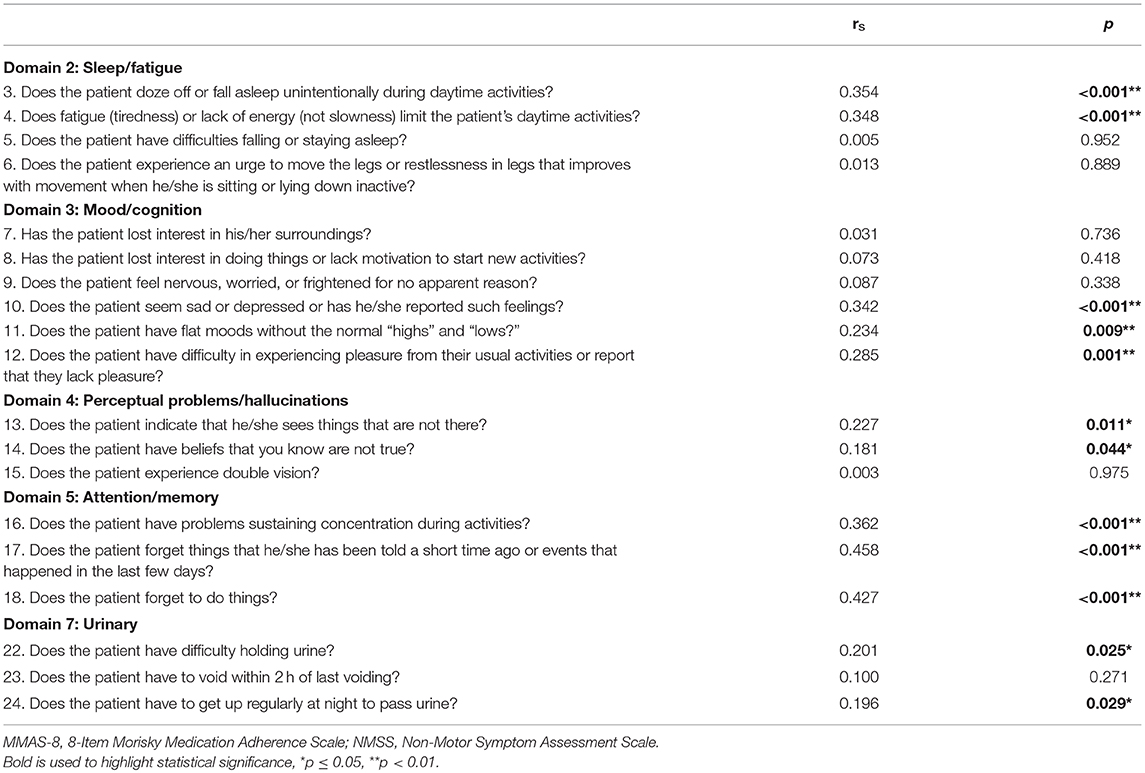
Table 5. Spearman's rank correlation coefficient (rs) of non-adherence to PD medication (MMAS-8) and questions of relevant domains of NMSS scale.
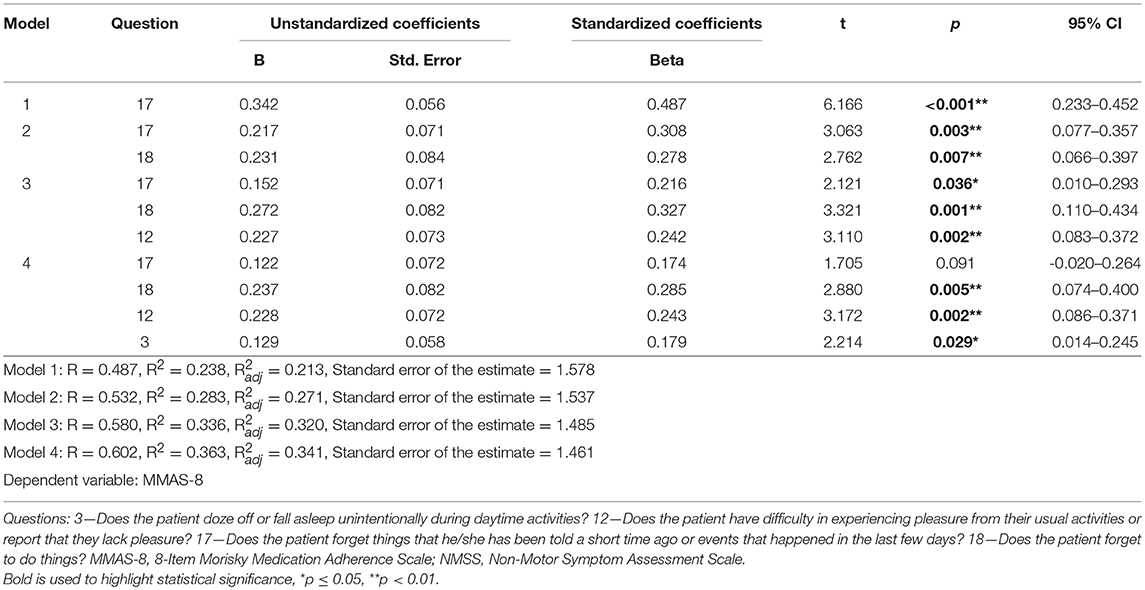
Table 6. Stepwise multiple regression analysis model of predictors of non-adherence to PD medication (MMAS-8) and relevant questions of scale NMSS.
Results of our study indicate that non-adherence to pharmacotherapy in PD patients who take at least three daily doses of medication is prevalent. These findings are consistent with previous studies of PD patients (1, 6, 20–27) but none of the existing studies specifically examined patients with more complex therapeutic regimens. The level of adherence to medications correlated with PD disease duration, which is consistent with previous research (6, 22–24); however, in our sample, longer disease duration did not predict lower adherence. This may be due to the fact that non-adherence is widespread phenomenon at all stages of PD. In our study and in a previous study by Leopold et al. (22), lower adherence was observed in male subjects, while other studies have not demonstrated a relationship between the level of adherence and gender (1, 6, 23, 24, 28). Among PD patients who take at least three daily doses of PD medication, we did not find significant correlation between the level of adherence and levodopa equivalent daily dose, number of PD drugs, or number of doses per day. Previous research has focused on differences between medication adherence of once-daily formulations of dopamine agonists vs. multiple-daily formulations of medication. For example, a Multicentre European Study showed that a once-daily medication regimen had significantly higher overall and time adherence compared to more complex regimens (6). However, a study comparing extended-release and immediate-release dopamine agonist formulation did not demonstrate significant differences between the formulations (26).
We emphasize correlations between the level of adherence and NMS. Neuropsychiatric domains of the NMS had the strongest relationship to medication adherence. Specifically, sleep/fatigue, mood/cognition, perceptual problems/hallucinations, attention/memory, and urinary problems were significantly correlated with lower levels of adherence. In our sample, sleep attacks, anhedonia, and forgetfulness predicted lower adherence to PD medication. Fatigue is one of the most common and disabling symptoms and occurs in every stage of PD, which affects everyday activities, increases disability and reduces QoL (29, 30). Based on the results of our study, excessive daytime sleepiness was an important predictor of non-adherence in PD patients. Depression is a common NMS in PD. Patients with depression have worse adherence to medication (6, 31). We found that anhedonia was independent risk factor of lower adherence. Therefore, identifying and managing depressive symptoms may improve medication adherence (32). An association between non-adherence and cognitive impairment has been described in several studies (23, 25). In our sample, we found that the presence of subjective cognitive complaints significantly predicted non-adherence. The association between non-adherence and urinary symptoms is interesting. Patients with urinary symptoms have more severe motor symptoms (especially bradykinesia and axial symptoms), more frequent falls, and worse cognition than those without urinary symptoms (33, 34). These mechanisms are currently unexplained and future research is needed.
Therapeutic goals in the early stages of PD include control of motor symptoms and prevention of motor complications. In advanced stages of PD, they include management of motor complications and non-motor symptoms (4, 23). Antiparkinsonian drugs are usually prescribed multiple times per day. As the disease progresses, the medication regimen often includes complicated dosing schedules which are required to manage worsening motor symptoms. Non-adherence is also associated with worsening of motor symptoms and motor complications. Side effects or a poor response to PD medication are also associated with poorer adherence (4–6, 21, 23, 27). Worse baseline motor scores in early treated PD do not impair adherence and, on the contrary, they are associated with better adherence (28). In our cohort, motor scores did not correlate with level of adherence. This could be explained by the fact that our study included PD patients who were relatively advanced in the disease stage and from tertiary movement disorders departments. Non-adherence to PD medication is associated with more severe motor and non-motor complications (5, 23, 27). The MMAS-8 focuses on the miss of taking or forgetting to take the daily medication. However, our study design did not allow for definite identification as to the reason or result and to establish causality. Low levels of adherence may lead to changes in therapy because the physician (and patient) may attribute worsening of Parkinsonian symptoms (or subcompensation of PD) to lack of efficacy of PD medication and it may result to changes in drug schedules, doses, or drugs. This can generate adverse effects (including motor complications as well) and may deteriorate adherence to pharmacotherapy even further (6, 23, 27). However, it is very important to emphasize that in advanced stages of the disease, omission of a dose when dyskinesia is present or an extra dose of PD medication in the presence of a sudden wearing off of medication can improve the patient's current clinical condition.
Consistent with previous research, non-adherent patients reported significantly poorer QoL (21, 23, 25, 35). Notably, the European Multicentre Study did not find poorer overall QoL in patients with suboptimal adherence and only the PDQ-39 mobility subscore was significantly associated with reduced QoL (6).
One limitation of our study was the usage of a subjective questionnaire for the detection of the level of medication adherence as opposed to objective medication monitoring methods. However, we utilized questionnaires that were specifically designed to assess medication adherence (36). Furthermore, the use of questionnaires mimics patient reports of medication adherence in clinical practice. Another limitation that may have impacted on our results was the selection of patients who take in a minimum of three daily doses of PD medication eliminating those with simpler therapeutic schemes.
In summary, non-adherence to more complicated medication regimens is frequent among PD patients. In patients who take three and more daily doses of PD drugs, further increase in the number of daily doses was not connected to increased risk of impaired adherence. Moreover, age did not have effect on level of adherence to pharmacotherapy in non-demented PD patients. On the other hand, patients with longer duration of PD and males had significantly lower adherence. Non-adherence was associated with poorer QoL, non-motor symptoms and more severe motor and non-motor complications. We discovered that motor symptoms, especially excessive daytime sleepiness, anhedonia, and forgetfulness, were independent risk factors for lower levels of adherence. Awareness of suboptimal adherence is crucial in everyday clinical practice. The MMAS-8 self-report questionnaire is an easy tool which may allow clinicians to detect non-adherence to PD medication and provide education and intervention. Strategies, such as reminders, alarms set on mobile phones or digital wrist watches, may be helpful tools for improving medication adherence.
The datasets generated for this study are available on request to the corresponding author.
The studies involving human participants were reviewed and approved by Ethics Committee of Academic Derer's University Hospital Bratislava, University Hospital Bratislava. The patients/participants provided their written informed consent to participate in this study.
PV, JB, JK, AG, and IS: project conception and organization. IS, PV, MŠ, KD, and MG: clinical examinations. VB, MM, and IS: statistical analysis. IS, MM, and KW-C: manuscript writing. PV, MŠ, JB, EK, JK, AG, KD, MG, and VB: manuscript review and critique.
This work was supported by the Scientific Grant Agency of the Ministry of Education, Science, Research and Sport of the Slovak Republic—VEGA 1/0490/16, VEGA 1/0704/17, by the Grant of the Ministry of Health of the Slovak Republic 2018/32-LFUK-6, and by the research grant from Novartis Slovakia s.r.o.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The funders had no role in study design, data collection, or preparation of the manuscript.
We wish to thank our patients for their willingness to participate.
1. Foppa AA, Chemello C, Vargas-Peláez CM, Farias MR. Medication therapy management service for patients with Parkinson's disease: a before-and-after study. Neurol Ther. (2016) 5:85–99. doi: 10.1007/s40120-016-0046-4
2. Sabaté E World Health Organization editors. Adherence to Long-Term Therapies: Evidence for Action. Geneva: World Health Organization (2003), 198 p.
3. Richy FF, Pietri G, Moran KA, Senior E, Makaroff LE. Compliance with pharmacotherapy and direct healthcare costs in patients with Parkinson's disease: a retrospective claims database analysis. Appl Health Econ Health Policy. (2013) 11:395–406. doi: 10.1007/s40258-013-0033-1
4. Straka I, Minár M, GaŽová A, Valkovič P, Kyselovič J. Clinical aspects of adherence to pharmacotherapy in Parkinson disease: a PRISMA-compliant systematic review. Medicine. (2018) 97:e10962. doi: 10.1097/MD.0000000000010962
5. Malek N, Grosset DG. Medication adherence in patients with Parkinson's disease. CNS Drugs. (2015) 29:47–53. doi: 10.1007/s40263-014-0220-0
6. Grosset D, Antonini A, Canesi M, Pezzoli G, Lees A, Shaw K, et al. Adherence to antiparkinson medication in a multicenter European study. Mov Disord. (2009) 24:826–32. doi: 10.1002/mds.22112
7. Postuma RB, Berg D, Stern M, Poewe W, Olanow CW, Oertel W, et al. MDS clinical diagnostic criteria for Parkinson's disease: MDS-PD clinical diagnostic criteria. Mov Disord. (2015) 30:1591–601. doi: 10.1002/mds.26424
8. Morisky DE, Ang A, Krousel-Wood M, Ward HJ. Predictive validity of a medication adherence measure in an outpatient setting. J Clin Hypertens. (2008) 10:348–54. doi: 10.1111/j.1751-7176.2008.07572.x
9. Cibulčík F, Hergottová A, Benetin J. Compliance of Parkinson disease in Slovakia. Ces Slov Neurol N. (2012) 75/108:S15.
10. Jenkinson C, Fitzpatrick R, Peto V, Greenhall R, Hyman N. The PDQ-8: development and validation of a short-form parkinson's disease questionnaire. Psychol Health. (1997) 12:805–14. doi: 10.1080/08870449708406741
11. Valkovic P, Harsany J, Hanakova M, Martinkova J, Benetin J. Nonmotor symptoms in early- and advanced-stage Parkinson's disease patients on dopaminergic therapy: how do they correlate with quality of life? ISRN Neurol. (2014) 2014:587302. doi: 10.1155/2014/587302
12. Ertan FS. Reliability and validity of the Geriatric Depression Scale in depression in Parkinson's disease. J Neurol Neurosurg Psychiatry. (2005) 76:1445–7. doi: 10.1136/jnnp.2004.057984
13. Németh F, Babčák M, Eliášová A. Screening and assessment tools of depression in senior population in Presov region. Geriatria. (2007) 7:150–5.
14. Yesavage JA, Brink TL, Rose TL, Lum O, Huang V, Adey M, et al. Development and validation of a geriatric depression screening scale: a preliminary report. J Psychiatr Res. (1982–1983) 17:37–49. doi: 10.1016/0022-3956(82)90033-4
15. Chaudhuri KR, Martinez-Martin P, Brown RG, Sethi K, Stocchi F, Odin P, et al. The metric properties of a novel non-motor symptoms scale for Parkinson's disease: results from an international pilot study. Mov Disord. (2007) 22:1901–11. doi: 10.1002/mds.21596
16. Goetz CG, Tilley BC, Shaftman SR, Stebbins GT, Fahn S, Martinez-Martin P, et al. Movement Disorder Society-sponsored revision of the Unified Parkinson's Disease Rating Scale (MDS-UPDRS): scale presentation and clinimetric testing results. Mov Disord. (2008) 23:2129–70. doi: 10.1002/mds.22340
17. Škorvánek M, Košutzká Z, Valkovič P, Ghorbani Saeedian R, Gdovinová Z, LaPelle N, et al. Validation of the Slovak version of the Movement Disorder Society – Unified Parkinson's Disease Rating Scale (MDS-UPDRS). Cesk Slov Neurol N. (2013) 76/109:463–8.
18. Stacy M, Hauser R, Oertel W, Schapira A, Sethi K, Stocchi F, et al. End-of-dose wearing off in parkinson disease: a 9-question survey assessment. Clin Neuropharmacol. (2006) 29:312–21. doi: 10.1097/01.WNF.0000232277.68501.08
19. Straka I, Škorvánek M, Valkovič P. Adherence to pharmacotherapy in Parkinson's Disease. Ces Slov Neurol N. (2015) 78/111:S14–5.
20. Prell T, Schaller D, Perner C, Franke GH, Witte OW, Kunze A, et al. Comparison of anonymous versus nonanonymous responses to a medication adherence questionnaire in patients with Parkinson's disease. Patient Prefer Adherence. (2019) 13:151–5. doi: 10.2147/PPA.S186732
21. Grosset KA, Bone I, Grosset DG. Suboptimal medication adherence in Parkinson's disease. Mov Disord. (2005) 20:1502–7. doi: 10.1002/mds.20602
22. Leopold NA, Polansky M, Hurka MR. Drug adherence in Parkinson's disease. Mov Disord. (2004) 19:513–7. doi: 10.1002/mds.20041
23. Valldeoriola F, Coronell C, Pont C, Buongiorno MT, Cámara A, Gaig C, et al. Socio-demographic and clinical factors influencing the adherence to treatment in Parkinson's disease: the ADHESON study: socio-demographic and clinical factors in treatment of Parkinson's disease. Eur J Neurol. (2011) 18:980–7. doi: 10.1111/j.1468-1331.2010.03320.x
24. Wei Y-J, Palumbo FB, Simoni-Wastila L, Shulman LM, Stuart B, Beardsley R, et al. Antiparkinson drug adherence and its association with health care utilization and economic outcomes in a medicare part D population. Value Health. (2014) 17:196–204. doi: 10.1016/j.jval.2013.12.003
25. Wei Y-J, Palumbo FB, Simoni-Wastila L, Shulman LM, Stuart B, Beardsley R, et al. Antiparkinson drug use and adherence in medicare Part D beneficiaries with Parkinson's disease. Clin Ther. (2013) 35:1513–1525.e1. doi: 10.1016/j.clinthera.2013.09.001
26. Bazán-Rodríguez L, Cervantes-Arriaga A, Llorens-Arenas R, Calderón-Fajardo H, Rodríguez-Violante M. No difference on adherence between immediate-release versus extended-release dopamine agonists in uninsured subjects with Parkinson's disease. Mov Disord Clin Pract. (2016) 3:68–72. doi: 10.1002/mdc3.12226
27. Kulkarni AS, Balkrishnan R, Anderson RT, Edin HM, Kirsch J, Stacy MA. Medication adherence and associated outcomes in medicare health maintenance organization-enrolled older adults with Parkinson's disease. Mov Disord. (2008) 23:359–65. doi: 10.1002/mds.21831
28. Elm JJ, Kamp C, Tilley BC, Guimaraes P, Fraser D, Deppen P, et al. Self-reported adherence versus pill count in Parkinson's disease: the NET-PD experience. Mov Disord. (2007) 22:822–7. doi: 10.1002/mds.21409
29. Skorvanek M, Gdovinova Z, Rosenberger J, Ghorbani Saeedian R, Nagyova I, Groothoff JW, et al. The associations between fatigue, apathy, and depression in Parkinson's disease. Acta Neurol Scand. (2015) 131:80–7. doi: 10.1111/ane.12282
30. Herlofson K, Kluger BM. Fatigue in Parkinson's disease. J Neurol Sci. (2017) 374:38–41. doi: 10.1016/j.jns.2016.12.061
31. Daley DJ, Myint PK, Gray RJ, Deane KHO. Systematic review on factors associated with medication non-adherence in Parkinson's disease. Parkinsonism Relat Disord. (2012) 18:1053–61. doi: 10.1016/j.parkreldis.2012.09.004
32. Shoval G, Stubbs B, Balicer RD, Feldman B, Hoshen M, Zalsman G, et al. Low adherence to antidepressants is associated with increased mortality in Parkinson disease patients. Parkinsonism Relat Disord. (2017) 43:92–6. doi: 10.1016/j.parkreldis.2017.07.032
33. Mito Y, Yabe I, Yaguchi H, Takei T, Terae S, Tajima Y. Relation of overactive bladder with motor symptoms and dopamine transporter imaging in drug-naïve Parkinson's disease. Parkinsonism Relat Disord. (2018) 50:37–41. doi: 10.1016/j.parkreldis.2018.02.017
34. Tkaczynska Z, Pilotto A, Becker S, Gräber-Sultan S, Berg D, Liepelt-Scarfone I. Association between cognitive impairment and urinary dysfunction in Parkinson's disease. J Neural Transm. (2017) 124:543–50. doi: 10.1007/s00702-017-1690-2
35. Bainbridge JL, Ruscin JM. Challenges of treatment adherence in older patients with Parkinson's disease. Drugs Aging. (2009) 26:145–55. doi: 10.2165/0002512-200926020-00006
Keywords: adherence, antiparkinson drugs, non-motor symptoms, Parkinson's disease, quality of life
Citation: Straka I, Minár M, Škorvánek M, Grofik M, Danterová K, Benetin J, Kurča E, Gažová A, Boleková V, Wyman-Chick KA, Kyselovič J and Valkovič P (2019) Adherence to Pharmacotherapy in Patients With Parkinson's Disease Taking Three and More Daily Doses of Medication. Front. Neurol. 10:799. doi: 10.3389/fneur.2019.00799
Received: 20 May 2019; Accepted: 11 July 2019;
Published: 31 July 2019.
Edited by:
Rou-Shayn Chen, Chang Gung Memorial Hospital, TaiwanReviewed by:
Roland Dominic Jamora, University of the Philippines Manila, PhilippinesCopyright © 2019 Straka, Minár, Škorvánek, Grofik, Danterová, Benetin, Kurča, Gažová, Boleková, Wyman-Chick, Kyselovič and Valkovič. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Peter Valkovič, cGV0ZXIudmFsa292aWNAZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.