 Clément Chollat
Clément Chollat Loïc Sentilhes3
Loïc Sentilhes3 Stéphane Marret
Stéphane Marret- 1INSERM U1245, Team 4 Neovasc, School of Medicine of Rouen, Institute of Innovation and Biomedical Research, Normandie University, Rouen, France
- 2Department of Neonatal Intensive Care, Port-Royal University Hospital, APHP, Paris, France
- 3Department of Obstetrics and Gynecology, Bordeaux University Hospital, Bordeaux, France
- 4Department of Neonatal Pediatrics and Intensive Care – Neuropediatrics, Rouen University Hospital, Rouen, France
Despite improvements in perinatal care, preterm birth still occurs regularly and the associated brain injury and adverse neurological outcomes remain a persistent challenge. Antenatal magnesium sulfate administration is an intervention with demonstrated neuroprotective effects for preterm births before 32 weeks of gestation (WG). Owing to its biological properties, including its action as an N-methyl-d-aspartate receptor blocker and its anti-inflammatory effects, magnesium is a good candidate for neuroprotection. In hypoxia models, including hypoxia-ischemia, inflammation, and excitotoxicity in various species (mice, rats, pigs), magnesium sulfate preconditioning decreased the induced lesions’ sizes and inflammatory cytokine levels, prevented cell death, and improved long-term behavior. In humans, some observational studies have demonstrated reduced risks of cerebral palsy after antenatal magnesium sulfate therapy. Meta-analyses of five randomized controlled trials using magnesium sulfate as a neuroprotectant showed amelioration of cerebral palsy at 2 years. A meta-analysis of individual participant data from these trials showed an equally strong decrease in cerebral palsy and the combined risk of fetal/infant death and cerebral palsy at 2 years. The benefit remained similar regardless of gestational age, cause of prematurity, and total dose received. These data support the use of a minimal dose (e.g., 4 g loading dose ± 1 g/h maintenance dose over 12 h) to avoid potential deleterious effects. Antenatal magnesium sulfate is now recommended by the World Health Organization and many pediatric and obstetrical societies, and it is requisite to maximize its administration among women at risk of preterm delivery before 32 WG.
Introduction
Preterm brain injury remains a crucial and unresolved issue among neonatologists. The ensuing cerebral lesions (i.e., brain injury related to encephalopathy of prematurity, including white matter injury, periventricular leukomalacia, and intraventricular/intraparenchymal hemorrhage) are strongly associated with later cerebral palsy and neurobehavioral developmental disorders. The mechanisms leading to these forms of brain injury are numerous and may include inflammation or ischemic insult. Numerous risk factors may be present before, during, and after birth (e.g., intra- and extra-uterine growth restriction, systemic inflammation, or perinatal hypoxia-ischemia). Although no single neuroprotective intervention is known to prevent preterm brain injury, neuroprotective strategies should be adopted to reduce the risk of neurodevelopmental anomalies in premature newborns. One such intervention is antenatal administration of magnesium sulfate (MgSO4) in women at risk of preterm birth. This mini review discusses the benefits of antenatal MgSO4 administration for fetal neuroprotection.
Why is MgSO4 a Good Candidate for Neuroprotection?
Biological Properties
Magnesium is the fourth most prevalent ion in the body and contributes to several physiological processes including storage, metabolism, and energy utilization. In the brain, magnesium is predominantly bound to chelators such as adenosine triphosphate (ATP) and is a cofactor in more than 300 enzymatic reactions (1, 2). Magnesium ions are essential for DNA, RNA, and protein synthesis. It contributes to glycolysis and ATP production and functions as a cell membrane stabilizer. In the central nervous system, magnesium is a non-competitive blocker of the N-methyl-d-aspartate (NMDA) glutamate receptor and modulates calcium influx. Its physiological role as a calcium channel blocker (3) and modulator of sodium and potassium flux through its action on ion pumps (e.g., Na+/K+ ATPase) and other membrane receptors (e.g., nicotinic acetylcholine receptor) (4) underlies its central role in heart function, muscle contraction, vascular tone, and nerve impulse conduction.
Sixty percent of magnesium is stored in bone, 20% in muscle, and 20% in soft tissue. Magnesium exists primarily in an ionized state (60%) but may also be complexed to proteins (33%) or anions (7%). Normal adult plasma concentration of magnesium is 0.75 mmol/L (95% confidence interval [CI]: 0.45–1.05) (5). In newborns, magnesium levels increase during the first week after birth (0.91 mmol/L [95% CI: 0.55–1.26]) (6).
Potential Mechanisms of Action Underlying the Neuroprotective Effect of Magnesium
Multiple mechanisms may underlie the neuroprotective impact of magnesium. Magnesium affects several pathways potentially involved in preterm brain injury. As a non-competitive NMDA receptor antagonist, magnesium prevents excitotoxic calcium-induced injury (7). Magnesium decreases extracellular glutamate under ischemic conditions, possibly reducing excitotoxicity (8). Magnesium limits calcium influx through voltage-gated channels, which may reduce the activation of apoptosis (9).
Magnesium also has anti-inflammatory properties as it reduces oxidative stress and reduces the production of pro-inflammatory cytokines interleukin-6 and tumor necrosis factor-α (10–14). Magnesium deficiency increases endothelial nitric oxide production, which can promote endothelial dysfunction (15, 16). This could involve decreased calcium influx and activation of phagocytic cells, inhibition of neurotransmitter release, or inhibition of nuclear factor kappa B.
Neuroprotective Effects of Magnesium in Preclinical Studies
Since the 1980s, animal studies have investigated the neuroprotective role of magnesium. Early experiments involved adult animal models of hypoxia, stroke, or traumatic brain injury. In 1984, Vacanti and Ames demonstrated neuroprotective effects of MgSO4 in an adult rabbit spinal cord ischemia model (17). In 1987, MgSO4 administration to rat hippocampal slices reduced the effect of hypoxia (18). McIntosh et al. demonstrated in 1989 that post-traumatic MgSO4 injection decreased neurological disorders in a dose-dependent manner (19). In 1996, Marinov et al. showed that MgSO4 administration before a focal ischemic episode in rats could be neuroprotective by blocking NMDA receptors (20). The neurological impact of MgSO4 on the developing brain was evaluated in several lesion models. In 1990, McDonald et al. showed that cerebral lesions induced by intraspinal injection of NMDA in postnatal (P) day 7 rats were decreased after intraperitoneal administration of MgSO4 (21). Several studies have reported the importance of the timing of MgSO4 administration. Intraperitoneal administration of MgSO4 reduced the excitotoxic brain lesions in mice induced by intracerebral injection of ibotenate (a glutamate receptor agonist) on P5. However, there was no effect on brain lesions developing on the day of birth or on P10 (brain lesions induced by intracerebral injection of ibotenate in mice are comparable to those identified in preterm human infants by age, specifically P0–22 weeks of gestation (WG), P2–26 WG, P5–32 WG, P10–41 WG) (22). In this P5 model, MgSO4 prevented sensorimotor alterations in P6 and P7 and prevented motor impairment, fine motor skill alteration, and memory deficits in adolescent mice (P34–40) (23). In the seminal model of focal hypoxia-ischemia established by the Rice-Vannucci procedure (surgical ligature of the right carotid artery followed by a 1–2-h exposure to 8% oxygen) in rats, MgSO4 injection before the hypoxic episode on P7 led to reduced lesion sizes, decreased hippocampal apoptosis, and improved adult sensorimotor performances (9, 24). In that model, MgSO4 treatment preserved mitochondrial respiration and reduced inflammation, thus reducing the production of reactive oxygen species after hypoxia-ischemia (16).
Under hypoxic conditions (fraction of inspired oxygen 5–7%) in P2 piglet brains, MgSO4 prevented the changes induced by hypoxia in the function of neuronal nuclear membrane, which decreased the transcription of apoptotic proteins and kinase activity. These actions ultimately prevented programmed cell death (25, 26). The neuroprotective effect of MgSO4 was also assessed under inflammatory conditions. In pregnant rats, lipopolysaccharide (LPS)-induced inflammation affected progeny learning and memory capabilities at 3 months, which is improved by antenatal MgSO4 treatment (27). MRI abnormalities (increased T2 and diffusion coefficient levels in white and gray matter) were highlighted for pups of LPS-treated dams, consistent with diffuse cerebral injury, which may be prevented by antenatal MgSO4 treatment (28). MgSO4 protected oligodendrocyte lineage cells in vitro in a model of hypoxic-ischemic injury (29).
Effects of MgSO4 Treatment in Pregnancy
Use of MgSO4 in Obstetrics for Maternal Indication
MgSO4 has been used in obstetrics for decades as a tocolytic agent and for prevention or treatment of seizures in women with preeclampsia or eclampsia (30, 31). Despite strong evidence indicating effectiveness in preventing eclampsia, MgSO4 is ineffective in delaying preterm birth (32). Despite weak evidence, MgSO4 is still recommended by the American College of Obstetricians and Gynecologists for short-term pregnancy prolongation (up to 48 h) to allow the administration of corticosteroids (33). In a European population-based cohort study, 35% of women with severe pre-eclampsia, eclampsia, or HELLP syndrome received MgSO4 before delivery. Only 1 of 119 hospital units reported using MgSO4 as a first-line tocolytic (34).
MgSO4 Transplacental Passage
Fetuses are passively exposed to MgSO4 administered to pregnant women. In animals, fetal blood magnesium concentrations increase after maternal administration (35–37) and correlate with maternal blood levels (38, 39). The ratio of the mean fetal magnesium level to the mean maternal serum level at delivery was estimated at 0.94 ± 0.15 (40).
Observational Studies
Considering its use in obstetrics for maternal indications, its transplacental passage, and its neuroprotective action in animal studies, several observational studies have focused on the impact of MgSO4 on neurological outcomes in preterm neonates. Nelson and Grether showed that exposure to MgSO4 exposure was higher in the control group than in the group of children with cerebral palsy (odds ratio [OR], 0.14; 95% CI, 0.05–0.51) (41). In another cohort study, prenatal MgSO4 exposure was associated with a reduced risk of cerebral palsy at 3–5 years (OR, 0.11; 95% CI, 0.02–0.81) (42). Other observational studies have not shown effects of MgSO4 on infant neurological outcomes (43–52). A meta-analysis of these observational studies highlighted that antenatal MgSO4 treatment was associated with a significantly reduced risk of mortality (risk ratio [RR], 0.73; 95% CI 0.61–0.89) and cerebral palsy (OR, 0.64; 95% CI 0.47–0.89) (53). Antenatal MgSO4 treatment was also associated with a decreased incidence of apparent echodensities and echolucencies on neonatal cranial ultrasonography and cerebellar hemorrhage on MRI (54, 55).
Randomized Controlled Trials (RCTs) of Magnesium as a Neuroprotectant
A total of five RCTs were performed in the 1990s and 2000s. Notably, two RCTs are ongoing: MASP (for administration of antenatal magnesium sulfate for the prevention of cerebral palsy in preterm infants, inclusion at 24–32 WG) and MAGENTA (inclusion at 30–34 WG) (56, 57).
Magnesium and Neurological Endpoints Trial (MagNET)
A total of 1,049 women in preterm labor at 25–33 WG (165 fetuses) treated at a single US center between October 1995 and January 1997 were included in the MagNET. Cases of triplet pregnancy or chorioamnionitis were excluded. In the tocolytic arm, women in active labor with cervical dilatation of at least 4 cm were randomly allocated to receive MgSO4 (4 g bolus then 2–3 g/h maintenance dose) or another tocolytic agent. In the neuroprotection arm, women with cervical dilatation of more than 4 cm were randomly allocated to receive MgSO4 (4 g bolus only) or 0.9% saline placebo.
The study was stopped prematurely in January 1997 due to significant mortality in the MgSO4 group (58, 59) and was widely discussed (60–63). The excessive number of mortalities occurred primarily in the tocolytic arm. The mortality rate in the MgSO4 group (11%) was consistent with that in previous reports of premature infants, whereas that in the placebo group was unusually low (1.4%). Moreover, causes of death were similar to those typical among premature children and were therefore difficult to attribute solely to MgSO4 treatment. Additionally, the confounding impact of multiple births was not accounted for, as more twin neonates were assigned to the treatment group than the placebo group. Finally, this increased mortality rate conflicted with the results of observational studies.
Australasian Collaborative Trial of Magnesium Sulfate (ACTOMgSO4)
A total of 1,062 women in preterm labor before 30 WG from 16 centers were included in the Australasian Collaborative Trial of Magnesium Sulfate (ACTOMgSO4) between February 1996 and September 2000 (64). MgSO4 (4 g bolus followed by 1 g/h maintenance for 24 h or until birth) was randomly allocated to 535 women (629 live fetuses), and 527 women (626 live fetuses) received placebo. Although the primary study outcome, the rate of cerebral palsy at 2 years, was similar between the groups (5.7% in the MgSO4 group versus 6.7% in the control group; RR, 0.85; 95% CI, 0.55–1.31), the rate of motor dysfunction was significantly lower in the MgSO4 group (2.9 versus 5.4% in the control group; RR, 0.53; 95% CI, 0.30–0.92). Neonatal and pediatric mortality rates were also similar.
PREMAG Trial
The PREMAG trial included 573 women treated at 18 French centers between July 1997 and July 2003 (65), with 286 women (354 fetuses) randomly assigned to receive a 4-g bolus of MgSO4 and 278 women (341 fetuses), placebo. The trial was stopped after 6 years of enrollment. The primary outcomes (the rates of white matter injury and mortality) were similar between the groups (white matter injury, 10% versus 11.7%; OR, 0.78; 95% CI, 0.47–1.31; mortality, 9.4 versus 10.4%; OR, 0.79; 95% CI, 0.44–1.44). Combined death or gross motor dysfunction at 2 years was lower in the MgSO4 group (25.6 versus 30.8%; OR, 0.62; 95% CI, 0.41–0.93), but there was no difference in cerebral palsy (66).
Beneficial Effects of Antenatal Magnesium Sulfate (BEAM)
The BEAM trial included 2241 women in preterm labor before 32 WG at 20 centers between December 1997 and May 2004 (67). Women were randomized to receive a 6-g bolus of MgSO4 followed by a 2-g/h maintenance dose for 12 h (1,096 women, 1,188 fetuses) or placebo (1,145 women, 1,256 fetuses). Antenatal MgSO4 administration had no impact on pediatric mortality. Although the primary outcome (composite of stillbirth or death by 1 year or cerebral palsy at 2 years) was similar in the two groups, moderate or severe cerebral palsy was significantly reduced in the MgSO4 group (1.9 versus 3.5%; RR, 0.55; 95% CI, 032–0.95).
MAGnesium Sulfate for Prevention of Eclampsia (MAGPIE)
The MAGPIE trial, a large international trial to evaluate the impact of antenatal MgSO4 administration in the prevention of eclampsia, included 10,141 women with preeclampsia between July 1998 and November 2001: 1,544 women (1,593 fetuses) before 37 WG (68). The women were randomly allocated to receive either MgSO4 (4 g bolus followed by 1 g/h maintenance dose for 24 h) or placebo. A pediatric follow-up study including 4,483 children (2,254 and 2,229 in the MgSO4 and placebo groups, respectively) showed no difference in neurological outcomes (Ages and Stages questionnaire) or mortality at 18 months. Notably, only 19% of the children followed were born before 33 WG.
Meta-Analyses
These five RCTs have been the subject of four meta-analyses to date, with consistent findings and conclusions (69–73). In all meta-analyses, antenatal MgSO4 given to women at risk of preterm delivery was associated with a significantly reduced risk of cerebral palsy in children exposed in utero, with an RR ranging from 0.61 to 0.70 and no impact on mortality. The number of women needed to treat (NNT) to prevent one case of cerebral palsy ranged from 56 to 74 in infants born before 34 WG, and it was 29 in those born before 28 WG (Table 1). Minor maternal side effects (e.g., flushing, nausea or vomiting, sweating, injection site discomfort) were more frequent in the MgSO4 groups, but with no significant effect on serious maternal complications.
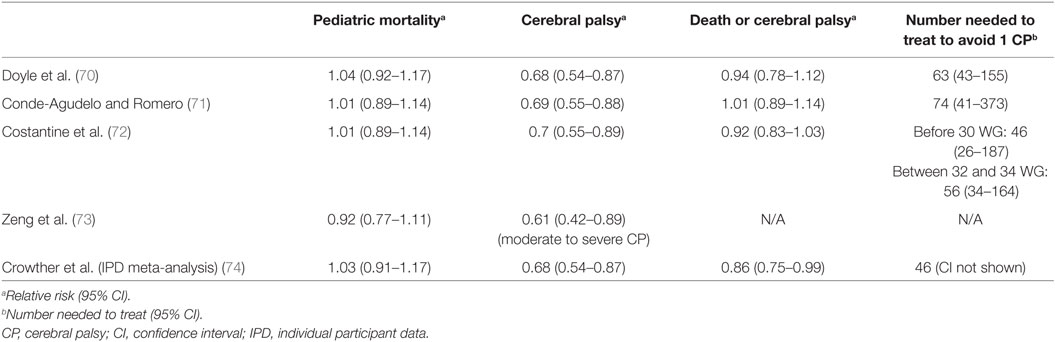
Table 1. Main outcomes of the meta-analyses.
An individual participant data meta-analysis was also undertaken by the AMICABLE group (Antenatal Magnesium sulfate Individual participant data international Collaboration: Assessing the benefits for babies using the Best Level of Evidence) to explore the interaction between treatment and participant characteristics (74), which included the 5 above-mentioned RCTs (5,493 women and 6,131 babies). The overall RR of cerebral palsy among survivors after antenatal MgSO4 was 0.68 (95% CI, 0.54–0.87), and the NNT was 46. Interestingly, MgSO4 also reduced the combined risk of fetal/infant death or cerebral palsy in the analysis of the 4 trials with fetal neuroprotective intent (RR 0.86, 95% CI, 0.75–0.99).
In all RCTs and meta-analyses to date, MgSO4 treatment had no impact on pediatric mortality or neonatal morbidity (respiratory distress syndrome, chronic lung disease, any intraventricular hemorrhage, cystic periventricular leukomalacia, necrotizing enterocolitis, patent ductus arteriosus, and retinopathy of prematurity). Similarly, MgSO4 treatment was not associated with serious maternal side effects. The benefit remained constant regardless of gestational age, cause of prematurity, total dose received, or maintenance dose administration after the loading dose. These data indicating persistent benefits of MgSO4 regardless of dose and support the use of low doses (e.g., 4 g loading dose ± 1 g/h maintenance dose for 12 h, 16 g maximum total dose) compared to high doses (e.g., 6 g loading dose + 2 g/h maintenance dose during 24 h, maximum total dose received: 54 g). Indeed, high MgSO4 dosage was implicated in the vasculopathy and high mortality observed in the MagNET trial (75). In a mouse preclinical model, MgSO4 demonstrated a dose-dependent, potentially deleterious effect on brain angiogenesis, vessel damage, and endothelial cell survival. The highest neuroprotective dose of MgSO4 induced cerebral hypoperfusion, whereas the lowest dose did not (76). These results support the use of MgSO4 in low doses.
Long-Term Follow-Up
Cohorts from the PREMAG and ACTOMgSO4 trials were followed up over their school-age years. From the PREMAG trial, 431 children were assessed at a mean age of 11 years (26.9% lost to follow-up) using a questionnaire completed by the parents (77). Although the ORs for motor, cognitive, behavioral outcomes, and school performance were favorable after magnesium treatment, the impact on neurodevelopment was not statistically significant. From the ACTOMgSO4, 669 children (21.3% lost to follow-up) were assessed at a mean age of 8 years using pediatric and psychological assessments and questionnaires completed by parents and teachers (78). Antenatal MgSO4 treatment had no impact on neurological, cognitive, behavioral, or school-related outcomes. Neither the PREMAG study nor the ACTOMgSO4 showed any effect on cerebral palsy at 2 years, likely because of limited sample sizes. Only the larger BEAM trial and meta-analyses reported reductions in cerebral palsy at 2 years. These long-term follow-up studies detected no harmful effects after antenatal MgSO4 treatment, although they were not designed for this purpose.
Implementation of Magnesium in Neuroprotective Protocols Worldwide
In France, in 2015, only 60% of tertiary maternity hospitals used MgSO4 for fetal neuroprotection, with protocols that differed by maximum gestational age, possibility of retreatment, and monitoring (79). In Europe, in 2012, only 9 of 119 tertiary maternity hospitals (7.6%) used MgSO4 for fetal neuroprotection (34). Lack of experience and an absence of a written protocol or national guidelines, decision-making processes, environmental contexts, or beliefs about possible consequences seemed to represent barriers to widespread applications of MgSO4 in women at risk of preterm delivery (79, 80). Studies assessing MgSO4 protocol implementation found that nearly 70% of eligible women received MgSO4 before preterm delivery, and approximately 90% delivered within 24 h. The main reasons for not giving treatment were omission by the medical team and urgent delivery (81, 82). In an Australasian audit, the proportion of eligible women not receiving MgSO4 decreased significantly after publication of national guidelines, from 69.7% in 2010 to 26.9% in 2011, which was maintained in 2012 and 2013 (22.5%) (83). In Canada, a knowledge translation strategy (including national practice guidelines, online e-learning modules, educational rounds, and evaluation of barriers and feasibility) was associated with an 84% increase in optimal MgSO4 use (84). To improve the rates of MgSO4 administration to eligible women, implementing educational programs could be effective.
Conclusion
Preterm birth is a major cause of death and a significant cause of long-term disability worldwide (85). MgSO4 is a safe and effective molecule that plays a key role in protecting the immature brain. It is a cost-effective, feasible, efficient, and safe intervention that contributes to the improvement of neurological outcomes. While MgSO4 has not been found to significantly improve cognition and behavior outcomes at school age, it prevents cerebral palsy at 2 years. Its use is now recommended by several pediatric and obstetrical societies, as well as the World Health Organization (strong recommendation based on moderate-quality evidence) for women at risk of imminent preterm birth before 32 WG. More work is needed to clarify the impact of MgSO4 on the cognitive outcome and efforts to improve the MgSO4 coverage of eligible women should be reinforced.
Author Contributions
CC, LS, and SM contributed equally to the writing of this review.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
3. Iseri LT, French JH. Magnesium: nature’s physiologic calcium blocker. Am Heart J (1984) 108:188–93. doi:10.1016/0002-8703(84)90572-6
4. Herroeder S, Schönherr ME, Hert SGD, Hollmann MW. Magnesium – essentials for anesthesiologists. Anesthes (2011) 114:971–93. doi:10.1097/ALN.0b013e318210483d
5. Duncanson GO, Worth HG. Determination of reference intervals for serum magnesium. Clin Chem (1990) 36:756–8.
6. Rigo J, Pieltain C, Christmann V, Bonsante F, Moltu SJ, Iacobelli S, et al. Serum magnesium levels in preterm infants are higher than adult levels: a systematic literature review and meta-analysis. Nutrients (2017) 9:E1125. doi:10.3390/nu9101125
7. Nowak L, Bregestovski P, Ascher P, Herbet A, Prochiantz A. Magnesium gates glutamate-activated channels in mouse central neurones. Nature (1984) 307:462–5. doi:10.1038/307462a0
8. Kang SW, Choi S-K, Park E, Chae S-J, Choi S, Jin Joo H, et al. Neuroprotective effects of magnesium-sulfate on ischemic injury mediated by modulating the release of glutamate and reduced of hyperreperfusion. Brain Res (2011) 1371:121–8. doi:10.1016/j.brainres.2010.11.057
9. Türkyilmaz C, Türkyilmaz Z, Atalay Y, Söylemezoglu F, Celasun B. Magnesium pre-treatment reduces neuronal apoptosis in newborn rats in hypoxia-ischemia. Brain Res (2002) 955:133–7. doi:10.1016/S0006-8993(02)03395-4
10. Mazur A, Maier JAM, Rock E, Gueux E, Nowacki W, Rayssiguier Y. Magnesium and the inflammatory response: potential physiopathological implications. Arch Biochem Biophys (2007) 458:48–56. doi:10.1016/j.abb.2006.03.031
11. Aryana P, Rajaei S, Bagheri A, Karimi F, Dabbagh A. Acute effect of intravenous administration of magnesium sulfate on serum levels of interleukin-6 and tumor necrosis factor-α in patients undergoing elective coronary bypass graft with cardiopulmonary bypass. Anesth Pain Med (2014) 4:e16316. doi:10.5812/aapm.16316
12. Rayssiguier Y, Libako P, Nowacki W, Rock E. Magnesium deficiency and metabolic syndrome: stress and inflammation may reflect calcium activation. Magnes Res (2010) 23:73–80. doi:10.1684/mrh.2010.0208
13. Burd I, Breen K, Friedman A, Chai J, Elovitz MA. Magnesium sulfate reduces inflammation-associated brain injury in fetal mice. Am J Obstet Gynecol (2010) 202:292.e1–9. doi:10.1016/j.ajog.2010.01.022
14. Cho GJ, Hong H-R, Hong S-C, Oh M-J, Kim H-J. The neuroprotective effect of magnesium sulfate in preterm fetal mice. J Perinat Med (2015) 43:537–43. doi:10.1515/jpm-2014-0176
15. Zheltova AA, Kharitonova MV, Iezhitsa IN, Spasov AA. Magnesium deficiency and oxidative stress: an update. Biomedicine (Taipei) (2016) 6:20. doi:10.7603/s40681-016-0020-6
16. Koning G, Leverin A-L, Nair S, Schwendimann L, Ek J, Carlsson Y, et al. Magnesium induces preconditioning of the neonatal brain via profound mitochondrial protection. J Cereb Blood Flow Metab (2017):271678X17746132. doi:10.1177/0271678X17746132
17. Vacanti FX, Ames A III. Mild hypothermia and Mg++ protect against irreversible damage during CNS ischemia. Stroke (1984) 15:695–8. doi:10.1161/01.STR.15.4.695
18. Clark GD, Rothman SM. Blockade of excitatory amino acid receptors protects anoxic hippocampal slices. Neuroscience (1987) 21:665–71. doi:10.1016/0306-4522(87)90027-3
19. McIntosh TK, Vink R, Yamakami I, Faden AI. Magnesium protects against neurological deficit after brain injury. Brain Res (1989) 482:252–60. doi:10.1016/0006-8993(89)91188-8
20. Marinov MB, Harbaugh KS, Hoopes PJ, Pikus HJ, Harbaugh RE. Neuroprotective effects of preischemia intraarterial magnesium sulfate in reversible focal cerebral ischemia. J Neurosurg (1996) 85:117–24. doi:10.3171/jns.1996.85.1.0117
21. McDonald JW, Silverstein FS, Johnston MV. Magnesium reduces N-methyl-d-aspartate (NMDA)-mediated brain injury in perinatal rats. Neurosci Lett (1990) 109:234–8. doi:10.1016/0304-3940(90)90569-U
22. Marret S, Gressens P, Gadisseux JF, Evrard P. Prevention by magnesium of excitotoxic neuronal death in the developing brain: an animal model for clinical intervention studies. Dev Med Child Neurol (1995) 37:473–84.
23. Daher I, Le Dieu-Lugon B, Dourmap N, Lecuyer M, Ramet L, Gomila C, et al. Magnesium sulfate prevents neurochemical and long-term behavioral consequences of neonatal excitotoxic lesions: comparison between male and female mice. J Neuropathol Exp Neurol (2017) 76:883–97. doi:10.1093/jnen/nlx073
24. Pazaiti A, Soubasi V, Spandou E, Karkavelas G, Georgiou T, Karalis P, et al. Evaluation of long-lasting sensorimotor consequences following neonatal hypoxic-ischemic brain injury in rats: the neuroprotective role of MgSO4. Neonatology (2009) 95:33–40. doi:10.1159/000151753
25. Mami AG, Ballesteros JR, Fritz KI, Kubin J, Mishra OP, Delivoria-Papadopoulos M. Effects of magnesium sulfate administration during hypoxia on CaM kinase IV and protein tyrosine kinase activities in the cerebral cortex of newborn piglets. Neurochem Res (2006) 31:57–62. doi:10.1007/s11064-005-9135-y
26. Mami AG, Ballesteros J, Mishra OP, Delivoria-Papadopoulos M. Effects of magnesium sulfate administration during hypoxia on Ca(2+) influx and IP(3) receptor modification in cerebral cortical neuronal nuclei of newborn piglets. Neurochem Res (2006) 31:63–70. doi:10.1007/s11064-005-9076-5
27. Lamhot VB, Khatib N, Ginsberg Y, Anunu R, Richter-Levin G, Weiner Z, et al. Magnesium sulfate prevents maternal inflammation-induced impairment of learning ability and memory in rat offspring. Am J Obstet Gynecol (2015) 213:851.e1–8. doi:10.1016/j.ajog.2015.07.042
28. Ginsberg Y, Khatib N, Weiss B, Arison S, Ross MG, Weiner Z, et al. Magnesium sulfate (MG) prevents maternal inflammation induced offspring cerebral injury evident on MRI but not via IL-1β. Neuroscience (2017) 353:98–105. doi:10.1016/j.neuroscience.2017.03.046
29. Itoh K, Maki T, Shindo A, Egawa N, Liang AC, Itoh N, et al. Magnesium sulfate protects oligodendrocyte lineage cells in a rat cell-culture model of hypoxic-ischemic injury. Neurosci Res (2016) 106:66–9. doi:10.1016/j.neures.2015.12.004
30. ACOG Committee on Practice Bulletins – Obstetrics. ACOG practice bulletin. Diagnosis and management of preeclampsia and eclampsia. Number 33, January 2002. Obstet Gynecol (2002) 99:159–67. doi:10.1016/S0029-7844(01)01747-1
31. Duley L, Gülmezoglu AM, Chou D. Magnesium sulphate versus lytic cocktail for eclampsia. Cochrane Database Syst Rev (2010):CD002960. doi:10.1002/14651858.CD002960.pub2
32. Crowther CA, Brown J, McKinlay CJD, Middleton P. Magnesium sulphate for preventing preterm birth in threatened preterm labour. Cochrane Database Syst Rev (2014):CD001060. doi:10.1002/14651858.CD001060.pub2
33. The American College of Obstetricians and Gynecologists Committee on Obstetric Practice Society for maternal-Fetal medicine. Committee opinion No 652: magnesium sulfate use in obstetrics. Obstet Gynecol (2016) 127:e52–3. doi:10.1097/AOG.0000000000001267
34. Wolf HT, Huusom L, Weber T, Piedvache A, Schmidt S, Norman M, et al. Use of magnesium sulfate before 32 weeks of gestation: a European population-based cohort study. BMJ Open (2017) 7:e013952. doi:10.1136/bmjopen-2016-013952
35. Hallak M, Cotton DB. Transfer of maternally administered magnesium sulfate into the fetal compartment of the rat: assessment of amniotic fluid, blood, and brain concentrations. Am J Obstet Gynecol (1993) 169:427–31. doi:10.1016/0002-9378(93)90101-N
36. Hallak M, Berry SM, Madincea F, Romero R, Evans MI, Cotton DB. Fetal serum and amniotic fluid magnesium concentrations with maternal treatment. Obstet Gynecol (1993) 81:185–8.
37. Reynolds A, Slattery S, Byrne S, Neary E, Müllers S, Kent E, et al. Timing of administration of antenatal magnesium sulfate and umbilical cord blood magnesium levels in preterm babies. J Matern Fetal Neonatal Med (2017):1–6. doi:10.1080/14767058.2017.1398724
38. Borja-Del-Rosario P, Basu SK, Haberman S, Bhutada A, Rastogi S. Neonatal serum magnesium concentrations are determined by total maternal dose of magnesium sulfate administered for neuroprotection. J Perinat Med (2014) 42:207–11. doi:10.1515/jpm-2013-0151
39. Sherwin CMT, Balch A, Campbell SC, Fredrickson J, Clark EAS, Varner M, et al. Maternal magnesium sulphate exposure predicts neonatal magnesium blood concentrations. Basic Clin Pharmacol Toxicol (2014) 114:318–22. doi:10.1111/bcpt.12166
40. Brookfield KF, Su F, Elkomy MH, Drover DR, Lyell DJ, Carvalho B. Pharmacokinetics and placental transfer of magnesium sulfate in pregnant women. Am J Obstet Gynecol (2016) 214:737.e1–9. doi:10.1016/j.ajog.2015.12.060
41. Nelson KB, Grether JK. Can magnesium sulfate reduce the risk of cerebral palsy in very low birthweight infants? Pediatrics (1995) 95:263–9.
42. Schendel DE, Berg CJ, Yeargin-Allsopp M, Boyle CA, Decoufle P. Prenatal magnesium sulfate exposure and the risk for cerebral palsy or mental retardation among very low-birth-weight children aged 3 to 5 years. JAMA (1996) 276:1805–10. doi:10.1001/jama.1996.03540220029026
43. Leviton A, Paneth N, Susser M, Reuss ML, Allred EN, Kuban K, et al. Maternal receipt of magnesium sulfate does not seem to reduce the risk of neonatal white matter damage. Pediatrics (1997) 99:E2. doi:10.1542/peds.99.4.e2
44. Paneth N, Jetton J, Pinto-Martin J, Susser M. Magnesium sulfate in labor and risk of neonatal brain lesions and cerebral palsy in low birth weight infants. The Neonatal Brain Hemorrhage Study Analysis Group. Pediatrics (1997) 99:E1. doi:10.1542/peds.99.5.e1
45. O’Shea TM, Klinepeter KL, Meis PJ, Dillard RG. Intrauterine infection and the risk of cerebral palsy in very low-birthweight infants. Paediatr Perinat Epidemiol (1998) 12:72–83. doi:10.1046/j.1365-3016.1998.00081.x
46. Canterino JC, Verma UL, Visintainer PF, Figueroa R, Klein SA, Tejani NA. Maternal magnesium sulfate and the development of neonatal periventricular leucomalacia and intraventricular hemorrhage. Obstet Gynecol (1999) 93:396–402. doi:10.1097/00006250-199903000-00017
47. Boyle CA, Yeargin-Allsopp M, Schendel DE, Holmgreen P, Oakley GP. Tocolytic magnesium sulfate exposure and risk of cerebral palsy among children with birth weights less than 1,750 grams. Am J Epidemiol (2000) 152:120–4. doi:10.1093/aje/152.2.120
48. Grether JK, Hoogstrate J, Walsh-Greene E, Nelson KB. Magnesium sulfate for tocolysis and risk of spastic cerebral palsy in premature children born to women without preeclampsia. Am J Obstet Gynecol (2000) 183:717–25. doi:10.1067/mob.2000.106581
49. Weintraub Z, Solovechick M, Reichman B, Rotschild A, Waisman D, Davkin O, et al. Effect of maternal tocolysis on the incidence of severe periventricular/intraventricular haemorrhage in very low birthweight infants. Arch Dis Child Fetal Neonatal Ed (2001) 85:F13–7. doi:10.1136/fn.85.1.F13
50. Elimian A, Verma R, Ogburn P, Wiencek V, Spitzer A, Quirk JG. Magnesium sulfate and neonatal outcomes of preterm neonates. J Matern Fetal Neonatal Med (2002) 12:118–22. doi:10.1080/jmf.12.2.118.122
51. Jazayeri A, Jazayeri MK, Sutkin G. Tocolysis does not improve neonatal outcome in patients with preterm rupture of membranes. Am J Perinatol (2003) 20:189–93. doi:10.1055/s-2003-40606
52. Kimberlin DF, Hauth JC, Goldenberg RL, Bottoms SF, Iams JD, Mercer B, et al. The effect of maternal magnesium sulfate treatment on neonatal morbidity in < or = 1000-gram infants. Am J Perinatol (1998) 15:635–41. doi:10.1055/s-2007-994082
53. Wolf HT, Hegaard HK, Greisen G, Huusom L, Hedegaard M. Treatment with magnesium sulphate in pre-term birth: a systematic review and meta-analysis of observational studies. J Obstet Gynaecol (2012) 32:135–40. doi:10.3109/01443615.2011.638999
54. Hirtz DG, Weiner SJ, Bulas D, DiPietro M, Seibert J, Rouse DJ, et al. Antenatal magnesium and cerebral palsy in preterm infants. J Pediatr (2015) 167:834–9.e3. doi:10.1016/j.jpeds.2015.06.067
55. Gano D, Ho M-L, Partridge JC, Glass HC, Xu D, Barkovich AJ, et al. Antenatal exposure to magnesium sulfate is associated with reduced cerebellar hemorrhage in preterm newborns. J Pediatr (2016) 178:68–74. doi:10.1016/j.jpeds.2016.06.053
56. Crowther CA, Middleton PF, Wilkinson D, Ashwood P, Haslam R; MAGENTA Study Group. Magnesium sulphate at 30 to 34 weeks’ gestational age: neuroprotection trial (MAGENTA) – study protocol. BMC Pregnancy Childbirth (2013) 13:91. doi:10.1186/1471-2393-13-91
57. Wolf HT, Hegaard HK, Pinborg AB, Huusom LD. Does antenatal administration of magnesium sulphate prevent cerebral palsy and mortality in preterm infants? A study protocol. AIMS Public Health (2015) 3:727–9. doi:10.3934/publichealth.2015.4.727
58. Mittendorf R, Covert R, Boman J, Khoshnood B, Lee KS, Siegler M. Is tocolytic magnesium sulphate associated with increased total paediatric mortality? Lancet (1997) 350:1517–8. doi:10.1016/S0140-6736(97)24047-X
59. Mittendorf R, Dambrosia J, Pryde PG, Lee K-S, Gianopoulos JG, Besinger RE, et al. Association between the use of antenatal magnesium sulfate in preterm labor and adverse health outcomes in infants. Am J Obstet Gynecol (2002) 186:1111–8. doi:10.1067/mob.2002.123544
60. Bénichou J, Zupan V, Fernandez H, Marpeau L, Marret S. Tocolytic magnesium sulphate and paediatric mortality. Lancet (1998) 351:290–1. doi:10.1016/S0140-6736(05)78242-8
61. Crowther C, Hiller J, Doyle L, Lumley J, Carlin J. Tocolytic magnesium sulphate and paediatric mortality. Lancet (1998) 351:291. doi:10.1016/S0140-6736(05)78241-6
62. Grether J, Hirtz D, McNellis D, Nelson K, Rouse DJ. Tocolytic magnesium sulphate and paediatric mortality. Lancet (1998) 351:292. doi:10.1016/S0140-6736(05)78239-8
63. Leveno KJ. Tocolytic magnesium sulphate and paediatric mortality. Lancet (1998) 351:291–2. doi:10.1016/S0140-6736(05)78240-4
64. Crowther CA, Hiller JE, Doyle LW, Haslam RR. Effect of magnesium sulfate given for neuroprotection before preterm birth: a randomized controlled trial. JAMA (2003) 290:2669–76. doi:10.1001/jama.290.20.2669
65. Marret S, Marpeau L, Zupan-Simunek V, Eurin D, Lévêque C, Hellot M-F, et al. Magnesium sulphate given before very-preterm birth to protect infant brain: the randomised controlled PREMAG trial*. BJOG (2007) 114:310–8. doi:10.1111/j.1471-0528.2006.01162.x
66. Marret S, Marpeau L, Bénichou J. Benefit of magnesium sulfate given before very preterm birth to protect infant brain. Pediatrics (2008) 121:225–6. doi:10.1542/peds.2007-2971
67. Rouse DJ, Hirtz DG, Thom E, Varner MW, Spong CY, Mercer BM, et al. A randomized, controlled trial of magnesium sulfate for the prevention of cerebral palsy. N Engl J Med (2008) 359:895–905. doi:10.1056/NEJMoa0801187
68. Altman D, Carroli G, Duley L, Farrell B, Moodley J, Neilson J, et al. Do women with pre-eclampsia, and their babies, benefit from magnesium sulphate? The Magpie Trial: a randomised placebo-controlled trial. Lancet (2002) 359:1877–90. doi:10.1016/S0140-6736(02)08778-0
69. Doyle LW, Crowther CA, Middleton P, Marret S. Magnesium sulphate for women at risk of preterm birth for neuroprotection of the fetus. Cochrane Database Syst Rev (2007):CD004661. doi:10.1002/14651858.CD004661.pub2
70. Doyle LW, Crowther CA, Middleton P, Marret S, Rouse D. Magnesium sulphate for women at risk of preterm birth for neuroprotection of the fetus. Cochrane Database Syst Rev (2009):CD004661. doi:10.1002/14651858.CD004661.pub3
71. Conde-Agudelo A, Romero R. Antenatal magnesium sulfate for the prevention of cerebral palsy in preterm infants less than 34 weeks’ gestation: a systematic review and metaanalysis. Am J Obstet Gynecol (2009) 200:595–609. doi:10.1016/j.ajog.2009.04.005
72. Costantine MM, Weiner SJ; Eunice Kennedy Shriver National Institute of Child Health and Human Development Maternal-Fetal Medicine Units Network. Effects of antenatal exposure to magnesium sulfate on neuroprotection and mortality in preterm infants: a meta-analysis. Obstet Gynecol (2009) 114:354–64. doi:10.1097/AOG.0b013e3181ae98c2
73. Zeng X, Xue Y, Tian Q, Sun R, An R. Effects and safety of magnesium sulfate on neuroprotection: a meta-analysis based on PRISMA guidelines. Medicine (Baltimore) (2016) 95:e2451. doi:10.1097/MD.0000000000002451
74. Crowther CA, Middleton PF, Voysey M, Askie L, Duley L, Pryde PG, et al. Assessing the neuroprotective benefits for babies of antenatal magnesium sulphate: an individual participant data meta-analysis. PLoS Med (2017) 14:e1002398. doi:10.1371/journal.pmed.1002398
75. Mittendorf R, Dammann O, Lee K-S. Brain lesions in newborns exposed to high-dose magnesium sulfate during preterm labor. J Perinatol (2006) 26:57–63. doi:10.1038/sj.jp.7211419
76. Lecuyer M, Rubio M, Chollat C, Lecointre M, Jégou S, Leroux P, et al. Experimental and clinical evidence of differential effects of magnesium sulfate on neuroprotection and angiogenesis in the fetal brain. Pharmacol Res Perspect (2017) 5:e00315. doi:10.1002/prp2.315
77. Chollat C, Enser M, Houivet E, Provost D, Bénichou J, Marpeau L, et al. School-age outcomes following a randomized controlled trial of magnesium sulfate for neuroprotection of preterm infants. J Pediatr (2014) 165(2):398–400.e3. doi:10.1016/j.jpeds.2014.04.007
78. Doyle LW, Anderson PJ, Haslam R, Lee KJ, Crowther C; Australasian Collaborative Trial of Magnesium Sulphate (ACTOMgSO4) Study Group. School-age outcomes of very preterm infants after antenatal treatment with magnesium sulfate vs placebo. JAMA (2014) 312:1105–13. doi:10.1001/jama.2014.11189
79. Chollat C, Le Doussal L, de la Villéon G, Provost D, Marret S. Antenatal magnesium sulphate administration for fetal neuroprotection: a French national survey. BMC Pregnancy Childbirth (2017) 17:304. doi:10.1186/s12884-017-1489-z
80. Bain E, Bubner T, Ashwood P, Van Ryswyk E, Simmonds L, Reid S, et al. Barriers and enablers to implementing antenatal magnesium sulphate for fetal neuroprotection guidelines: a study using the theoretical domains framework. BMC Pregnancy Childbirth (2015) 15:176. doi:10.1186/s12884-015-0618-9
81. Bouet P-E, Brun S, Madar H, Baisson A-L, Courtay V, Gascoin-Lachambre G, et al. Implementation of an antenatal magnesium sulfate protocol for fetal neuroprotection in preterm infants. Sci Rep (2015) 5:14732. doi:10.1038/srep14732
82. Ow LL, Kennedy A, McCarthy EA, Walker SP. Feasibility of implementing magnesium sulphate for neuroprotection in a tertiary obstetric unit. Aust N Z J Obstet Gynaecol (2012) 52:356–60. doi:10.1111/j.1479-828X.2012.01434.x
83. Siwicki K, Bain E, Bubner T, Ashwood P, Middleton P, Crowther CA. Nonreceipt of antenatal magnesium sulphate for fetal neuroprotection at the Women’s and Children’s Hospital, Adelaide 2010-2013. Aust N Z J Obstet Gynaecol (2015) 55:233–8. doi:10.1111/ajo.12334
84. De Silva DA, Synnes AR, von Dadelszen P, Lee T, Bone JN; MAG-CP, CPN and CNN Collaborative Groups. Magee LA. MAGnesium sulphate for fetal neuroprotection to prevent Cerebral Palsy (MAG-CP)-implementation of a national guideline in Canada. Implement Sci (2018) 13:8. doi:10.1186/s13012-017-0702-9
Keywords: magnesium sulfate, neuroprotection, preterm birth, cerebral palsy, animal studies, randomized controlled trials
Citation: Chollat C, Sentilhes L and Marret S (2018) Fetal Neuroprotection by Magnesium Sulfate: From Translational Research to Clinical Application. Front. Neurol. 9:247. doi: 10.3389/fneur.2018.00247
Received: 30 January 2018; Accepted: 28 March 2018;
Published: 16 April 2018
Edited by:
Masahiro Tsuji, National Cerebral and Cardiovascular Center, JapanReviewed by:
Tomoki Arichi, King’s College London, United KingdomSheffali Gulati, All India Institute of Medical Sciences, India
Copyright: © 2018 Chollat, Sentilhes and Marret. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Clément Chollat, Y2xlbWVudC5jaG9sbGF0QGdtYWlsLmNvbQ==