
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurol. , 06 February 2018
Sec. Neuropharmacology
Volume 9 - 2018 | https://doi.org/10.3389/fneur.2018.00038
This article is part of the Research Topic Burden of Illness in People with Epilepsy: From Population-Based Studies to Precision Medicine View all 14 articles
 Felix Zahnert
Felix Zahnert Kristina Krause
Kristina Krause Ilka ImmischLena Habermehl
Ilka ImmischLena Habermehl Iris GornyIzabella ChmielewskaLeona MöllerAnna M. Weyand
Iris GornyIzabella ChmielewskaLeona MöllerAnna M. Weyand Peter M. MrossJan Wagner
Peter M. MrossJan Wagner Katja Menzler†
Katja Menzler† Susanne Knake*†
Susanne Knake*†
Objectives: To assess first clinical experiences with brivaracetam (BRV) in the treatment of epilepsies.
Methods: Data on patients treated with BRV from February to December 2016 and with at least one clinical follow-up were collected from electronic patient records. Data on safety and efficacy were evaluated retrospectively.
Results: In total, 93 patients were analyzed; 12 (12.9%) received BRV in monotherapy. The mean duration to follow-up was 4.85 months (MD = 4 months; SD = 3.63). Fifty-seven patients had more than one seizure per month at baseline and had a follow-up of more than 4 weeks; the rate of ≥50% responders was 35.1% (n = 20) in this group, of which five (8.8%) patients were newly seizure-free. In 50.5% (47/93), patients were switched from levetiracetam (LEV) to BRV, of which 43 (46.2%) were switched immediately. Adverse events (AE) occurred in 39.8%, with 22.6% experiencing behavioral and 25.8% experiencing non-behavioral AE. LEV-related AE (LEV-AE) were significantly reduced by switching to BRV. The discontinuation of BRV was reported in 26/93 patients (28%); 10 of those were switched back to LEV with an observed reduction of AE in 70%. For clinical reasons, 12 patients received BRV in monotherapy, 75% were seizure–free, and previous LEV-AE improved in 6/9 patients. BRV-related AE occurred in 5/12 cases, and five patients discontinued BRV.
Conclusion: BRV seems to be a safe, easy, and effective option in the treatment of patients with epilepsy, especially in the treatment of patients who have psychiatric comorbidities and might not be good candidates for LEV treatment. BRV broadens the therapeutic spectrum and facilitates personalized treatment.
More than 30% of patients with epilepsy are refractory to medication with antiepileptic drugs (AEDs) (1, 2), although pharmaceutical treatment options have expanded steadily over the last 20 years. While many AEDs have similar potency with regard to seizure control, they often vary with regard to tolerability and side effects, which have the most important impact on treatment compliance and thus on seizure control (3, 4). Brivaracetam (BRV) is the latest AED, which was approved in Germany in February 2016 as an adjunctive treatment of partial-onset seizures with and without secondary generalization in patients aged 16 years or older (5). Similar to levetiracetam (LEV), it mainly targets synaptic vesicle protein 2A, but more selectively and with a 15- to 30-fold increased affinity (6, 7). Clinical trials have demonstrated a significant reduction of seizure frequency after the initiation of BRV, with ≥50% responder rates ranging from 30.3 to 55.8% (8–15). At a dose of 100 mg/day, the amount of seizure-free patients was sevenfold compared to placebo (16). During those trials, the overall efficacy of BRV was greater in LEV-naïve patients. In previous clinical studies, treatment-emergent adverse events (AE) of BRV occurred in 54.2% of the patients. The most common AE were irritability, fatigue, asthenia, somnolence, headache, paresthesia, and dizziness (13, 16–18). Compared to LEV, the occurrence of AE and seizure control was similar, with a significantly higher incidence of dizziness in BRV (18). However, behavioral adverse events (BAE) are common in LEV (19) and they accounted in one study for 40.4% of discontinuations of LEV therapy (3). In the therapeutic range of 50–200 mg BRV per day, BAE such as anxiety, aggression, depression, or others occurred in 5.0–12.3% (5). In a small, open-label prospective exploratory study, a direct switch from LEV to BRV led to a reduction of BAE in 27/29 patients, making BRV a promising treatment option in patients with LEV-associated BAE (20).
So far, long-term post-marketing observations can provide further important insight into the efficacy and tolerability under real-life conditions. Here, we report post-marketing experience with BRV.
Data were retrospectively collected from in- and outpatients of the Epilepsy Center Hessen, Germany, who received BRV treatment after its approval and introduction to the German market between February 2016 and December 2016. All patients who had at least one clinical follow-up were included. Based on a decision of the local IRB, patients do not have to be consented for retrospective data analysis.
The effect of BRV on seizure frequency and tolerability was assessed. Data were collected at baseline (BL) (i.e., initiation on BRV) and at each of the follow-up visits, usually after 3 and 6 months. Data on concurrent anticonvulsant medication, seizure frequency, initiation, and termination of treatment as well as AE were identified from electronic patient records.
Responder rates were assessed at the most recent follow-up in patients on BRV who had seizure frequencies of ≥1 per month at BL and a follow-up of at least 4 weeks. Patients were classified as seizure-free when no seizures occurred during the entire observation period.
Analyses of AE were separated into two different subgroups: behavioral AE, including psychiatric AE such as depression and anxiety, and non-behavioral AE, including AE such as dizziness, cognitive decline, and others.
To compare the tolerability of LEV and BRV, we analyzed the reoccurrence and persistence of LEV-associated AE, which either had emerged on LEV in medical history, leading to the discontinuation of LEV, or were present on LEV at BL. The number of LEV-related AE (LEV-AE) was compared with the number of the same LEV-AE reoccurring under BRV in each respective patient using repeated measures t-tests.
A total of 93 patients who received BRV during the observation period and who had at least one follow-up visit were identified and included in the analysis.
For demographic characteristics of the study population, see Table 1. In the subpopulation eligible for the analysis of seizure frequencies, the mean length of the observation period was 5.3 months (MD = 5.5 months, SD = 4.1 months). A direct switch from LEV monotherapy to BRV monotherapy was performed in 12 patients (12.9%). Patients had received 6.3 AEDs on average since their first diagnosis of epilepsy (MD = 5 AEDs, SD = 3.7). Four (4.3%) patients were initiated on a further AED other than BRV within the observation period.
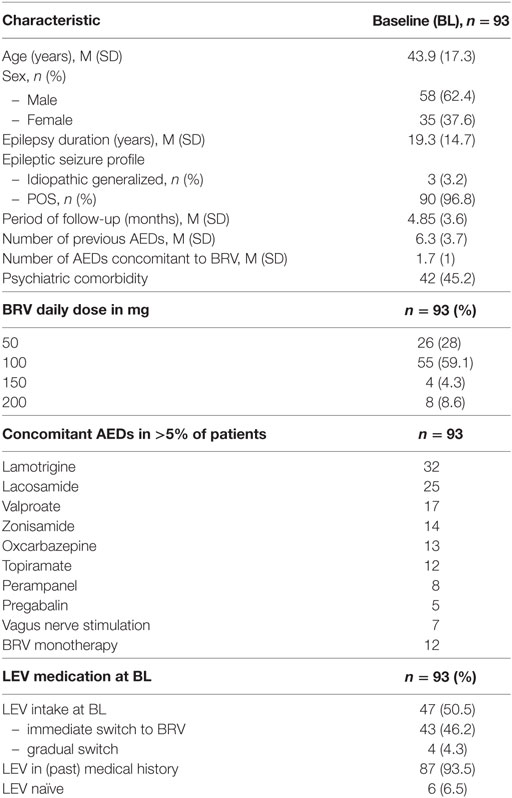
Table 1. Patients’ characteristics.
Responder rates at the most recent follow-up (average 5.3 months after first BRV prescription) were determined in 57/93 patients (Figure 1). The rate of ≥50% responders was 35.1% (n = 20), of which five (8.8%) patients became seizure-free. The rate of <50% responders was 8.8% (n = 5), while seizure frequency remained unchanged in 29.8% (n = 17). An aggravation of seizure frequency occurred in 26.3% (n = 15) of patients. Overall seizure freedom was achieved in 27/93 patients (29%). Status epilepticus was observed in four (4.3%) patients under BRV treatment.
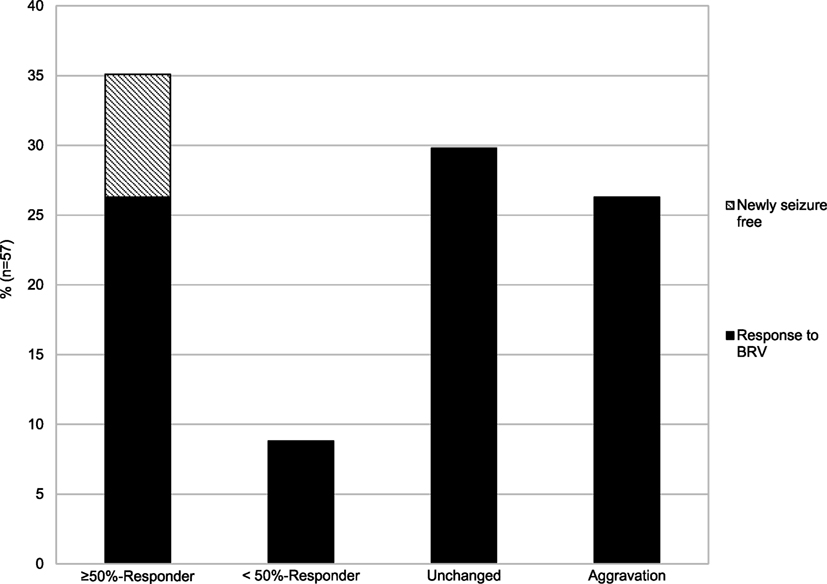
Figure 1. Change in seizure frequency after initiation of BRV treatment.
Due to sample size, we did not investigate seizure frequencies and responder rates in LEV-naïve patients (n = 6) separately.
Overall, AE during BRV intake occurred in 37 (39.8%) patients. BAE and NBAE were observed in 21 (22.6%) and 24 (25.8%) patients, respectively.
Adverse events reported in >5% of patients were irritability, depression, fatigue (n = 7, 7.5%), aggression (n = 6, 6.5%), and cognitive decline (n = 5, 5.4%). For other AE, see Table 2.
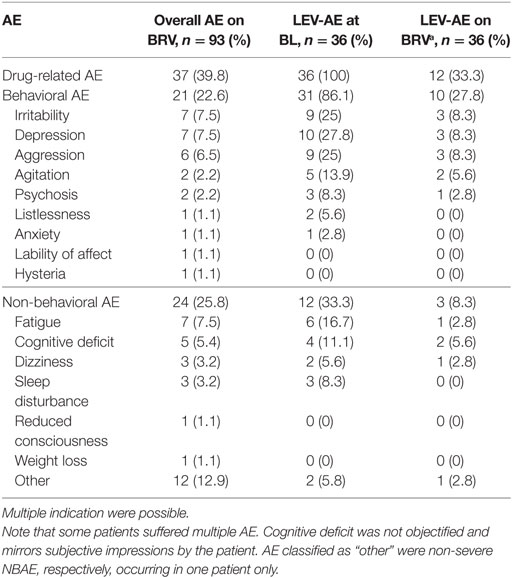
Table 2. The number of total AE during BRV therapy (overall AE under BRV) and the number of AE that were associated with previous LEV treatment at BL (LEV-AE at BL) and under treatment with BRV (aLEV-AE on BRV at the most recent follow-up).
The discontinuation of BRV was reported in 26/93 patients (28%). Reasons for the discontinuation of BRV are listed in Table 3. Two patients (2.2%) requested to discontinue AED therapy entirely. The mean duration from BRV initiation to discontinuation was 3.19 months (MD = 3 months, SD = 2.6). The most frequent AE leading to discontinuation was aggression (n = 4, 4.3%).
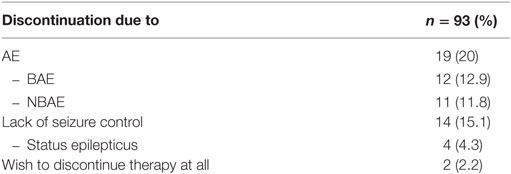
Table 3. Reason for discontinuation of BRV therapy.
In 12/15 patients (80%) who had a follow-up after BRV discontinuation, a clinically meaningful reduction of AE was observed.
An immediate switchback to LEV was performed in 10/26 patients who discontinued BRV. Of these patients, eight were followed up: seven (87.5%) of those showed clinical improvement.
More than half of the patients (57/93) had AEs under LEV treatment before, either in their prior medical history (n = 21), or at actual BL (n = 36). In this population, 44/57 (77.2%) patients reported either a clinically meaningful reduction or no reemergence of previous LEV-AE under BRV at all.
Out of 36 patients suffering from LEV-AE at BL, 24 (66.67%) experienced a clinically meaningful reduction in AE by switching to BRV. Comparison of the mean number of LEV-AE at BL and the most recent follow-up on BRV for each respective patient revealed a significant reduction of an average of 1.08 AE (p < 0.001, M1 = 1.56, SD1 = 0.91; M2 = 0.47, SD2 = 0.81) (Figure 2).
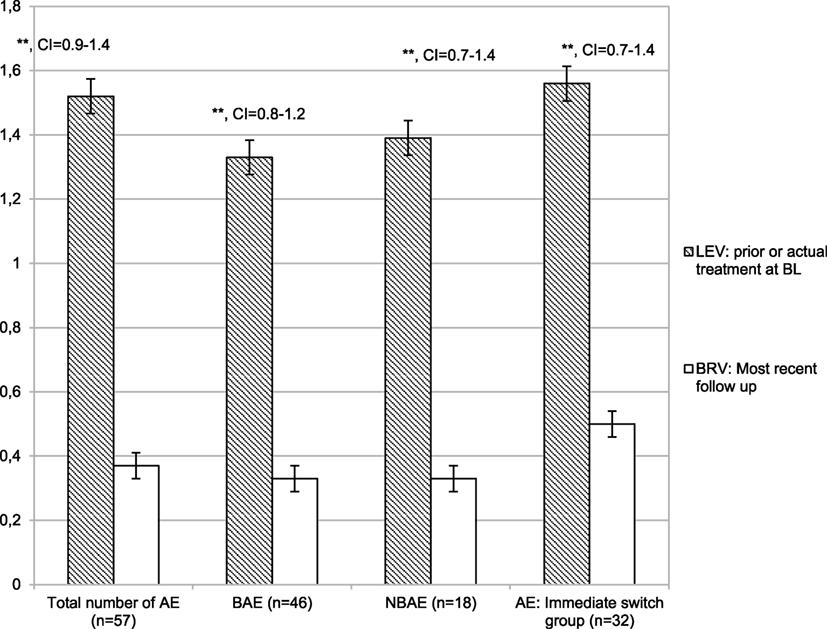
Figure 2. Number of adverse events: [total number and number of behavioral and non-behavioral adverse events (AE)] under Levetiracetam (LEV) treatment and under brivaracetam (BRV) treatment in the subpopulation of patients who ever (actual or in prior treatment) had AE under LEV medication. Thirty-two patients had been switched immediately from LEV to BRV. **p < 0.001, and error bars indicate the mean error.
The mean number of LEV-AE was reduced significantly in patients who were immediately switched from BL on LEV to BRV (n = 32) (p < 0.001, M1 = 1.56, SD1 = 0.95; M2 = 0.5, SD2 = 0.84).
Significant reductions in LEV-BAE were observed between BL on LEV and the most recent follow-up on BRV (n = 31; p < 0.001, M1 = 1.26, SD1 = 0.63; M2 = 0.39, SD2 = 0.67), and a similar reduction was observed in patients experiencing LEV-NBAE at BL (n = 12; p = 0.001, M1 = 1.4, SD1 = 0.67; M2 = 0.42, SD2 = 0.9). The aggravation of LEV-AE occurred in four patients (4.3%).
Patients who were not currently on LEV treatment, but who had discontinued LEV in the past due to AE (n = 21), reported a significantly smaller amount of those LEV-associated AEs after being treated with BRV (n = 21; p < 0.001, M1 = 1.4, SD1 = 0.75; M2 = 0.19, SD2 = 0.51). Here, similar results emerged regarding BAE (n = 15; p < 0.001, M1 = 1.47, SD1 = 0.74; M2 = 0.2, SD2 = 0.56) and NBAE (n = 6; p = 0.013, M1 = 1.33, SD1 = 0.52; M2 = 0.17, SD2 = 0.41). Only 2/21 (9.5%) patients experienced a reoccurrence of LEV-associated AE.
Within our study population, 12/93 patients received BRV in monotherapy, based on individual therapeutic decisions and on individual medical reasons. Here, the mean observation period was 4.6 months (SE = 0.8, SD = 2.7; median = 4 months) and the mean number of AEDs prescribed in prior anamnesis was 2.1 (SE = 0.3, SD = 1.2, median = 2).
In this subpopulation, freedom from seizures was achieved in 9/12 (75%) patients.
In 6/9 (66.67%) patients, LEV-AE from BL were reduced to a clinically and statistically significant extent (n = 9; p = 0.011, M1 = 2.3, SD1 = 1; M2 = 1, SD2 = 1.3). Overall, AE occurred in 5/12 patients (41.7%), the most common (in >10%) being irritability and agitation (n = 2, 16.7%).
Five of these 12 patients (41.7%) discontinued therapy with BRV, with a mean duration of therapy until discontinuation of 3.65 months (SE = 1.5, SD = 3.3, median = 3.5 months). Two patients (16.7%) discontinued due to BAE, and two stated that they wished to discontinue therapy entirely. Non-behavioral AE accounted for three discontinuations. Again, multiple, simultaneously occurring AE leading to discontinuation were common.
Our primary objective was to assess seizure control and tolerability in patients under BRV treatment.
We found that treatment with BRV can effectively reduce seizure frequency in patients with epilepsies with a ≥50% responder rate of 35.1 and 8.8% of patients being newly seizure-free.
Data are consistent with results from earlier trials (27.8–55.8%), and our rate of patients newly free of seizures (8.8%) was within the range of previously described rates (3–14.9%) (8–14, 21, 22). An exacerbation of seizure frequency occurred in 26.3%. This rate may not be surprising, considering the highly selective group of patients with a long history of treatment-resistant epilepsy resulting in a comparatively high number of previously prescribed AEDs. Responder rates on BRV were comparable to post-marketing experiences with other recently introduced AEDs such as Perampanel (PER; ≥50% responder rate in the largest three trials: 27–50%) or Lacosamide (LCM; ≥50% responder rate: 18–69%). The same did also apply to rates of seizure-free patients (PER: 14–17% in the largest three trials; LCM: 3–33%), as in the present study, 29% were seizure-free with 8.8% being newly seizure-free (23, 24).
Within our study population, AE on BRV were common and occurred in 39.8% of patients, which is consistent with the findings of a retrospective clinical study (37%) and slightly lower than indicated by the findings of a pooled analysis of phase IIb and phase III trials (54.2%) (13, 21).
In a meta-analysis of previous clinical trials, AE significantly associated with BRV compared to placebo were somnolence, dizziness, fatigue, and irritability, with an incidence of 12.4, 9.6, 7.7, and 2.8%, respectively (16). In another pooled analysis, the most common AE overall were headache (20.9%), dizziness (17.5%), somnolence (15.2%), nasopharyngitis (13.2%), fatigue (11.3%), and convulsion (10.6%) (13). In this study, the safety profile of BRV differed from the above data. While in previous studies, the most common BAE (irritability, insomnia, depression, and anxiety) occurred in only 2–3% of patients (16), BAE emerged more frequently under BRV (22.6%) in our study population. In our analysis, depression, irritability and fatigue (7.5% each), and aggression (6.5%) were the most frequently reported AEs. Dizziness, one of the most common AEs from previous studies, only occurred in 3.2%, and somnolence was observed in only one patient (1.1%). One major reason for the higher rate of BAE in our data might be that BRV was initiated in patients who mostly had psychiatric comorbidities (45.2%) or who were prone to behavioral side effects and had already discontinued LEV due to BAE. Unlike some other AEDs, BRV did not cause metabolic syndrome or weight gain (25).
As previous studies suggested, the effects on seizure frequency seemed strongest in patients who were LEV-naïve (16). Hence, the safety and efficacy of BRV administered in monotherapy is of great interest. The administration of BRV as the first anticonvulsive treatment in patients is yet to be examined. In our data, monotherapy with BRV appeared safe and was well tolerated with a reduction of LEV-associated AE in the majority of patients, supporting previously described experiences (22). Patients on monotherapy had less severe epilepsy and were previously on another monotherapy. Switching to BRV was mainly performed due to behavioral side effects or psychiatric comorbidities and not due to a lack of seizure control. This explains the greater proportion of seizure-free patients than in the overall study population.
In patients who were switched from LEV to BRV, a reduction of AE was observed. AEs, which had led to LEV discontinuation in the past, rarely reemerged under therapy with BRV.
Our findings indicate that BRV has a safety profile that is distinct from LEV, making it a useful alternative to enhance adherence to therapy with AEDs. Especially for patients who are not eligible for LEV use, BRV might be a therapeutic option, opening a chance to achieve sufficient seizure control.
These results are consistent with the findings from previous studies where a reduction of LEV-associated BAE was described (20, 22).
An immediate switch from LEV to BRV was safe and reduced LEV-associated AE in the majority of patients. Switching back from BRV to a prior anticonvulsive medication, especially LEV, was safe, and AEs as well as increases in seizure frequency emerging under BRV seem at least partially reversible this way. Due to the sample size, further studies investigating the pharmacokinetics and the clinical impact of a fast and direct switch of anticonvulsive medication are of interest.
The use of retrospective data obtained by a review of the patient charts and from a standard patient anamnesis in daily clinical practice might potentially introduce individual bias. This might stem from the neurologists’ individual evaluations and interpretations, as well as the variable comprehensiveness of patient self-reports. However, these results mirror conditions in clinical practice, where the clinician mostly relies on patient self-report, and standardized data are not always available.
Results in analyses for subgroups such as patients on monotherapy or immediate switchback to LEV might consolidate with reanalysis once more data become available. Larger, prospective, and multicenter trials of these subgroups would be desirable.
Therapy with BRV seemed safe and well tolerated. An immediate switch from LEV to BRV was easy and safe and reduced LEV-associated AE. However, behavioral and non-behavioral AEs occurred under BRV treatment. In case of newly occurred AE on BRV, a direct switchback to LEV was safe. Single patients were treated for individual reasons with BRV monotherapy, which seemed safe and achieved seizure freedom in 9/12 patients.
In summary, we demonstrated that BRV might be a promising option for the treatment of epilepsies, especially for those patients who suffer from side effects of LEV therapy. BRV seems to offer the chance to improve therapeutic effectiveness and broadens the therapeutic spectrum to facilitate personalized treatment.
For the local IRB, the ethics committee of the Department of Medicine, Philipps University Marburg, extra ethical approval is not needed, if data are collected retrospectively; any patients in our University Hospital agree upon admission that data might later be used anonymously for research purposes.
FZ contributed to conception, acquisition of data, analysis and interpretation of data, and manuscript drafting. KK participated in data analysis, manuscript drafting, and revision. II, IC, JW, LH, AS, IG, AW, PM, and LM contributed to data collection and manuscript revision. KM contributed to study conception, data analysis, and draft writing. SK contributed to study conception, data analysis, and draft writing.
FZ, KK, LH, IG, IC, LM, AW, and JW—none; II served as a study investigator for UCB, SAGE Therapeutics, Boehringer Ingelheim, Marinus Pharmaceuticals Inc., Upsher-Smith Laboratories Inc., GlaxoSmithKline, Eisai Limited. She received speaker’s honoraria for UCB. KM worked as a Consultant for UCB and Eisai. SK served on advisory boards for UCB and held lectures for UCB, Desitin and Eisai. She is study investigator for Sage, UCB and Boehringer Ingelheim, Marinus Pharmaceuticals Inc., Upsher-Smith Laboratories Inc., GlaxoSmithKline and Eisai Limited.
1. Cockerell OC, Sander J, Hart YM, Shorvon SD, Johnson AL. Remission of epilepsy: results from the National General Practice Study of Epilepsy. Lancet (1995) 346(8968):140–4. doi:10.1016/S0140-6736(95)92933-9
2. Kwan P, Brodie MJ. Early identification of refractory epilepsy. N Engl J Med (2000) 342(5):314–9. doi:10.1056/NEJM200002033420503
3. Chung S, Wang N, Hank N. Comparative retention rates and long-term tolerability of new antiepileptic drugs. Seizure (2007) 16(4):296–304. doi:10.1016/j.seizure.2007.01.004
4. Wilby J, Kainth A, Hawkins N, Epstein D, McIntosh H, McDaid C, et al. Clinical effectiveness, tolerability and cost-effectiveness of newer drugs for epilepsy in adults: a systematic review and economic evaluation. Health Technol Assess (2005) 9(15):1–157.
5. Strzelczyk A, Klein KM, Willems LM, Rosenow F, Bauer S. Brivaracetam in the treatment of focal and idiopathic generalized epilepsies and of status epilepticus. Expert Rev Clin Pharmacol (2016) 9(5):637–45. doi:10.1586/17512433.2016.1156529
6. Gillard M, Fuks B, Leclercq K, Matagne A. Binding characteristics of Brivaracetam, a selective, high affinity SV2A ligand in rat, mouse and human brain: relationship to anti-convulsant properties. Eur J Pharmacol (2011) 664(1–3):36–44. doi:10.1016/j.ejphar.2011.04.064
7. Lynch BA, Lambeng N, Nocka K, Kensel-Hammes P, Bajjalieh SM, Matagne A, et al. The synaptic vesicle protein SV2A is the binding site for the antiepileptic drug Levetiracetam. Proc Natl Acad Sci U S A (2004) 101(26):9861–6. doi:10.1073/pnas.0308208101
8. Biton V, Berkovic SF, Abou-Khalil B, Sperling MR, Johnson ME, Lu S. Brivaracetam as adjunctive treatment for uncontrolled partial epilepsy in adults: a phase III randomized, double-blind, placebo-controlled trial. Epilepsia (2014) 55(1):57–66. doi:10.1111/epi.12433
9. French JA, Costantini C, Brodsky A, von Rosenstiel P, N01193 Study Group. Adjunctive Brivaracetam for refractory partial-onset seizures: a randomized, controlled trial. Neurology (2010) 75(6):519–25. doi:10.1212/WNL.0b013e3181ec7f7f
10. Klein P, Schiemann J, Sperling MR, Whitesides J, Liang W, Stalvey T, et al. A randomized, double-blind, placebo-controlled, multicenter, parallel-group study to evaluate the efficacy and safety of adjunctive Brivaracetam in adult patients with uncontrolled partial-onset seizures. Epilepsia (2015) 56(12):1890–8. doi:10.1111/epi.13212
11. Kwan P, Trinka E, van Paesschen W, Rektor I, Johnson ME, Lu S. Adjunctive Brivaracetam for uncontrolled focal and generalized epilepsies: results of a phase III, double-blind, randomized, placebo-controlled, flexible-dose trial. Epilepsia (2014) 55(1):38–46. doi:10.1111/epi.12391
12. Ryvlin P, Werhahn KJ, Blaszczyk B, Johnson ME, Lu S. Adjunctive Brivaracetam in adults with uncontrolled focal epilepsy: results from a double-blind, randomized, placebo-controlled trial. Epilepsia (2014) 55(1):47–56. doi:10.1111/epi.12432
13. Toledo M, Whitesides J, Schiemann J, Johnson ME, Eckhardt K, McDonough B, et al. Safety, tolerability, and seizure control during long-term treatment with adjunctive Brivaracetam for partial-onset seizures. Epilepsia (2016) 57(7):1139–51. doi:10.1111/epi.13416
14. van Paesschen W, Hirsch E, Johnson M, Falter U, von Rosenstiel P. Efficacy and tolerability of adjunctive Brivaracetam in adults with uncontrolled partial-onset seizures: a phase IIb, randomized, controlled trial. Epilepsia (2013) 54(1):89–97. doi:10.1111/j.1528-1167.2012.03598.x
15. Strzelczyk A, Steinig I, Klein KM, Willems LM, Knake S, Rosenow F, et al. [Brivaracetam for add-on treatment in focal epilepsy]. Nervenarzt (2016) 87(10):1086–93. doi:10.1007/s00115-016-0163-4
16. Lattanzi S, Cagnetti C, Foschi N, Provinciali L, Silvestrini M. Brivaracetam add-on for refractory focal epilepsy: a systematic review and meta-analysis. Neurology (2016) 86(14):1344–52. doi:10.1212/WNL.0000000000002545
17. Brodie MJ, Whitesides J, Schiemann J, D’Souza J, Johnson ME. Tolerability, safety, and efficacy of adjunctive Brivaracetam for focal seizures in older patients: a pooled analysis from three phase III studies. Epilepsy Res (2016) 127:114–8. doi:10.1016/j.eplepsyres.2016.08.018
18. Zhang L, Li S, Li H, Zou X. Levetiracetam vs. Brivaracetam for adults with refractory focal seizures: a meta-analysis and indirect comparison. Seizure (2016) 39:28–33. doi:10.1016/j.seizure.2016.05.004
19. French J, Edrich P, Cramer JA. A systematic review of the safety profile of Levetiracetam: a new antiepileptic drug. Epilepsy Res (2001) 47(1–2):77–90. doi:10.1016/S0920-1211(01)00296-0
20. Yates SL, Fakhoury T, Liang W, Eckhardt K, Borghs S, D’Souza J. An open-label, prospective, exploratory study of patients with epilepsy switching from Levetiracetam to Brivaracetam. Epilepsy Behav (2015) E&B 52(Pt A):165–8. doi:10.1016/j.yebeh.2015.09.005
21. Steinhoff BJ, Bacher M, Bucurenciu I, Hillenbrand B, Intravooth T, Kornmeier R, et al. Real-life experience with Brivaracetam in 101 patients with difficult-to-treat epilepsy-A monocenter survey. Seizure (2017) 48:11–4. doi:10.1016/j.seizure.2017.03.010
22. Steinig I, von Podewils F, Möddel G, Bauer S, Klein KM, Paule E, et al. Postmarketing experience with Brivaracetam in the treatment of epilepsies: a multicenter cohort study from Germany. Epilepsia (2017) 58(7):1208–16. doi:10.1111/epi.13768
23. Paquette V, Culley C, Greanya ED, Ensom MH. Lacosamide as adjunctive therapy in refractory epilepsy in adults: a systematic review. Seizure (2015) 25:1–17. doi:10.1016/j.seizure.2014.11.007
24. Trinka E, Steinhoff BJ, Nikanorova M, Brodie MJ. Perampanel for focal epilepsy: insights from early clinical experience. Acta Neurol Scand (2016) 133(3):160–72. doi:10.1111/ane.12529
Keywords: brivaracetam, levetiracetam, epilepsy, treatment, side effects
Citation: Zahnert F, Krause K, Immisch I, Habermehl L, Gorny I, Chmielewska I, Möller L, Weyand AM, Mross PM, Wagner J, Menzler K and Knake S (2018) Brivaracetam in the Treatment of Patients with Epilepsy—First Clinical Experiences. Front. Neurol. 9:38. doi: 10.3389/fneur.2018.00038
Received: 17 October 2017; Accepted: 16 January 2018;
Published: 06 February 2018
Edited by:
Adam Strzelczyk, Universitätsklinikum Frankfurt, GermanyReviewed by:
Sulev Kõks, University of Tartu, EstoniaCopyright: © 2018 Zahnert, Krause, Immisch, Habermehl, Gorny, Chmielewska, Möller, Weyand, Mross, Wagner, Menzler and Knake. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Susanne Knake, a25ha2VAbWVkLnVuaS1tYXJidXJnLmRl
†These authors have contributed equally to this work.
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.