 Maxime Maheu
Maxime Maheu Marie-Soleil Houde
Marie-Soleil Houde Simon P. Landry
Simon P. Landry François Champoux
François Champoux
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Neurol. , 22 September 2015
Sec. Neuro-Otology
Volume 6 - 2015 | https://doi.org/10.3389/fneur.2015.00205
This article is part of the Research Topic Age-related vestibular loss: current understanding and future research directions View all 13 articles
Balance disorders are common issues for aging populations due to the effects of normal aging on peripheral vestibular structures. These changes affect the results of vestibular function evaluations and make the interpretation of these results more difficult. The objective of this article is to review the current state of knowledge of clinically relevant vestibular measures. We will first focus on otolith function assessment methods cervical-VEMP (cVEMP) and ocular-VEMP (oVEMP), then the caloric and video-head impulse test (vHIT) methods for semicircular canals assessment. cVEMP and oVEMP are useful methods, though research on the effects of age for some parameters are still inconclusive. vHIT results are largely independent of age as compared to caloric stimulation and should therefore be preferred for the evaluation of the semicircular canals function.
With the accelerating aging of the global population, age-related health issues are becoming a growing concern (1). Increased risks of falls from loss of balance are among these health concerns (2) and are considered by the WHO as an important burden on both the health care system and health of the population (3). Vestibular information, which provides information related to static and dynamic position in space, is known to play a major role in balance (4). Better understanding of the effects of aging on the vestibular system can thus be beneficial in addressing risks of fall in an aging population.
The vestibular system is located in the inner ear and is composed of three semicircular canals (lateral, anterior, and posterior) that detect angular acceleration and two otolith organs (saccule and utricule) that detect gravity (5). Information from the saccule and the posterior semicircular canal projects to central vestibular pathways mostly through the inferior vestibular nerve. Information from the utricule, the lateral, and the anterior semicircular canals mostly projects through the superior vestibular nerve (5) and primarily reaches the vestibular nuclei (5).
The integrity of these vestibular structures is essential for normal balance. Investigations on the vestibular system and aging have revealed reductions in many vestibular structures, including otoconia in both otolith organs (6, 7), vestibular hair cells in the horizontal crista ampullaris (8), scarpa ganglion neurons (9–11), and vestibular nuclei neurons (12, 13).
The objective of this article is to review the current state of knowledge of clinically relevant vestibular measures part of a comprehensive assessment protocol. Indeed, with the aging population and the increasing data from scientific research, it is becoming crucial to take a critical look at the effects of aging on clinical test results to gain insight on best practices for clinical vestibular evaluation in an elderly population.
Healthcare professionals such as audiologists frequently perform vestibular testing. These evaluations are done to detect vestibular deficits in order to improve vestibular compensation and to reduce both dizziness and unsteadiness. A comprehensive clinical test battery should include appropriate techniques to assess the otolith organs and the semicircular canals.
The vestibular-evoked myogenic potential (VEMP) is an electrophysiological technique used to assess otolith function and can be evoked using different stimuli, such as sounds, vibrations, and electrical stimulations (14–17). Two responses can be evoked using VEMP: ocular-VEMP (oVEMP) and cervical-VEMP (cVEMP).
The cVEMP is an inhibitory response measured from the ipsilateral sternocleidomastoïd muscle and originates from the saccule (16, 18). The inhibition response is measured from the first positive peak occurring around 13 ms (p13 or P1) followed by a negative peak around 23 ms (n23 or N1).
The oVEMP is an excitatory response of the inferior oblique eye muscle contralateral to the stimulated ear and is thought to originate from the utricle (18, 19). The oVEMP response is composed of a negative peak occurring at around 11–12 ms (N1) and positive peak occurring at around 18 ms (P1) (20). These responses have been found to be robust indicators of vestibular system integrity and are independent from hearing abilities (21, 22).
Caloric stimulation is a commonly used clinical vestibular evaluation method that induces a movement of the endolymph within the horizontal semicircular canal by applying either warm or cold water or air to the external ear canal (23). Despite its wide clinical use, the mechanisms underlying caloric stimulation are contested [for more details see Ref. (24)].
The video-head impulse test (vHIT) is a more recent technique for the functional assessment of all six semicircular canals (25). This latest vestibular clinical assessment tool uses an infrared camera designed to track pupillary movement and a patient-worn gyroscope mounted on goggles (26). Gain, the vHIT’s output, is calculated by comparing eye and head velocity during fast head movements in each of the six semicircular canals’ planes (25, 26). vHIT can provide useful information in the assessment of semicircular canal function through the vestibulo-ocular reflex (VOR) (25, 27). Measurement of the vertical canal function is based on the 2D modified HIT technique (28). This method yields higher gains for the vertical canals than the 3D HIT coil technique. vHIT is highly sensitive to calibration error. This can lead to erroneous calculation of gain magnitude and make comparison between studies difficult.
The effects of normal aging on VEMP responses have been analyzed for different parameters, such as peak-to-peak amplitude [the difference between both components (microvolt)], latency [time of occurrence of both components (millisecond)], thresholds [lowest intensity of a stimuli to trigger a response], response rate [prevalence of a VEMP response (%)], and asymmetry ratio [difference in amplitude between individual ears].
One of the most widely observed effects of aging with cVEMP is a decrease in recorded amplitude (15, 19, 29–35). Indeed, this decrease has been reported to happen at a rate of 0.14 μV per decade (31) and is independent of the stimulus used (35). On the other hand, cVEMP thresholds have been observed to remain steady up to 50 years of age (15) and then progressively increase (15, 19, 34). This increase has been reported for click and tone burst stimulations (12). Though the majority of studies report no significant effect of age on cVEMP latencies (19, 31, 33, 35), few authors have observed age-related increased latency on the p13 (15, 34) and n23 (9), while other have reported age-related decreases to n23 (24). cVEMP response rates are widely reported to decrease with age. However, the age at which this happens is still contested. Some report a response rate of 100% for participants <65 years old followed by a rapid decline (32), while others have observed a progressive decline starting at 50 years old (15).
Numerous studies have reported a decrease in oVEMP amplitude related to age (19, 29, 31, 33, 35–37). More specifically, oVEMP amplitude has been reported to decrease by 2.9 μV per decade, independent of the stimulus used (19, 29, 31, 33, 36, 37). Normal aging has been reported to increase oVEMP thresholds (12). Most studies report significant increases in oVEMP latency with age (19, 31, 33, 36, 37). This increase has been reported to be significant after 60 years of age (36) and at a rate of 0.12 ms per decade (31). Interestingly, it has been suggested that this increase is only significant in men (33). To the best of our knowledge, only one study did not report any significant difference in oVEMP latencies between age groups (35). oVEMP response rate has been shown to decrease with normal aging (36, 37) but can be dependent on the method of stimulus presentation used (36). A significant reduction in response rate for participants over 60 years of age can be measured when stimuli are presented by bone conduction though no significant differences in response rate were found for galvanic stimulation.
Caloric stimulation output is based on the slow-phase movement of the eyes during caloric evoked nystagmus. Few recent researches have looked at the effects of aging on caloric stimulation. Investigations on the effects of normal aging on caloric response found a significant increase in response for middle-aged groups followed by a slow decline with increasing age (32, 38, 39). However, this difference was only noted for the warm irrigation (32, 39). Despite these results suggesting an effect of aging on caloric responses, some investigations have failed to uncover any age-related differences (40, 41).
Recent advances in eye-tracking technology have led to the development of the vHIT. Numerous methods exist to calculate vHIT gain. The studies described in this review divided the area under the eye velocity curve by the area under the head velocity curve (42). In healthy adults, gain is typically between 0.8 and 1.2 (26). Investigations on the effects of aging on vHIT gain have only suggested a minor effect (26, 42–44). However, a higher head rotation velocity can elicit significant differences after 70 years old (45, 46). The decline in gain per decade has been suggested to be 0.012 (45) and significant gain differences have only been found beginning at 90 years of age (45). Till now, research on the effects of aging on vHIT has primarily investigated the effect of aging on the horizontal semicircular canals. To the best of our knowledge, only one study assessed the effect of age on vertical canals (42). The authors found that age did not influence vHIT response for anterior canals and gain only slightly decreased with age for the posterior canals.
Current clinical vestibular evaluation methods provide information on the integrity of the peripheral vestibular system. Understanding results from these evaluations in the context of normal aging is crucial to properly diagnosing vestibular disorders. Despite the well-known effects of aging on the peripheral vestibular system (6, 8), the effects of normal aging on vestibular evaluations, as highlighted by this review, is of yet a largely contested field (see Table 1). Understanding these effects has important clinical implications to help delineate various vestibular pathologies in an aging population.
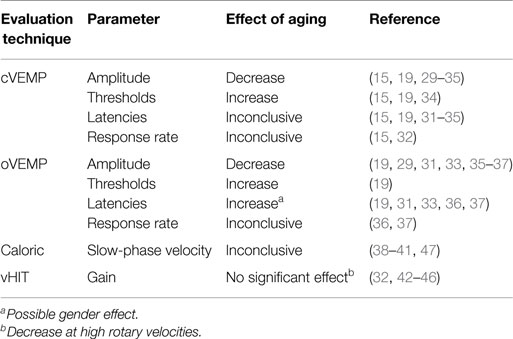
Table 1. Effects of aging on clinical vestibular evaluation techniques.
From the existing research, it is possible to propose guidelines for the use of clinical vestibular evaluations in an aging population. For instance, cVEMP is a useful tool to evaluate saccule function and the inferior vestibular nerve for the elderly when used with precaution. Reduced amplitude is reported with aging but these parameters should still be considered valuable, especially as amplitude asymmetry ratios are shown to remain stable with age (31, 35). Despite their inconsistencies in research, latencies can also be valuable complementary parameters. In fact, as most studies report no significant change in cVEMP latencies parameters, a change in latency should not be attributed to aging and should draw the attention of the clinician (19, 31, 33, 35). Taken together, these last two parameters can allow clinicians to identify vestibular pathologies using cVEMP without significant age-related interference.
Ocular-VEMP can be a useful evaluation method for utricule function and superior vestibular nerve integrity if it is used attentively. Similarly to cVEMP, amplitude remains a valid parameter for oVEMP evaluation as there is no significant asymmetry despite a strong decrease (31). Latencies must be considered with caution as multiple investigations have reported significant age-related increases (19, 31, 33, 36, 37). It has also been suggested that this increase in latency is exclusive to men (33). We therefore propose the use of clinician-established evaluation norms taking age and gender into account.
On the other hand, caloric testing should be used with precaution for an aging population. Till now, there is debate surrounding the mechanisms underlying caloric responses (47). Therefore, non-vestibular factors beyond normal aging could influence the results (40). The lack of unanimity for caloric responses in relation to age, combined with the debate surrounding the mechanisms underlying this method (47), are indicators that caloric testing still requires investigation before conclusive opinions on the effects of aging can be drawn.
We propose that vHIT is the preferable method to evaluate the vestibular canals in an aging population, although some precaution is needed regarding neck stiffness to avoid neck injuries. Results from vHIT appear to be largely independent of normal aging (45, 46) as only the posterior semicircular canal demonstrates a slight decrease in gain with increasing age (42). Therefore, semicircular canal function of older patients should be evaluated using vHIT. However, further studies are needed to measure the effect of aging for vHIT on the vertical semicircular canals.
This review provided an overlook for the existing literature for the effects of aging on clinical vestibular evaluations. Of the most popular evaluation methods, vHIT is largely independent of age and should be preferred over caloric to evaluate semicircular function. This recommendation is due to a lack of understanding of the underlying mechanisms of caloric stimulation and the inconstant reported effects of aging. cVEMP and oVEMP are also useful methods, though it should be kept in mind that research on the effects of aging are still inconclusive for some parameters.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
This work was supported by grants from the Fonds de Recherche du Québec – Santé (FRQS).
1. Lutz W, Sanderson W, Scherbov S. The coming acceleration of global population ageing. Nature (2008) 451:716–9. doi: 10.1038/nature06516
2. Iwasaki S, Yamasoba T. Dizziness and imbalance in the elderly: age-related decline in the vestibular system. Aging Dis (2014) 6:38–47. doi:10.14336/AD.2014.0128
3. World Health Organization. WHO Global Report on Falls Prevention in Older Age. France: WHO Press (2007). 47 p.
4. Cullen KE. The vestibular system: multimodal intergration and encoding of self-motion for motor control. Trends Neurosci (2012) 35:185–96. doi:10.1016/j.tins.2011.12.001
5. Baloh R, Honrubia V, Kerber KA. Clinical Neurophysiology of the Vestibular System. 4th ed. New York, NY: Oxford University Press (2011). 455 p.
6. Walther LE, Westhofen M. Presbyvertigo-aging of otoconia and vestibular sensory cells. J Vestib Res (2007) 17:89–92.
7. Igarashi M, Saito R, Mizukoshi K, Alford BR. Otoconia in young and elderly persons: a temporal bone study. Acta Otolaryngol Suppl (1993) 504:26–9. doi:10.3109/00016489309128117
8. Lopez I, Ishiyama G, Tang Y, Tokita J, Baloh RW, Ishiyama A. Regional estimates of hair cells and supporting cells in the human crista ampullaris. J Neurosci Res (2005) 82:421–31. doi:10.1002/jnr.20652
9. Velázquez-Villaseñor L, Merchant SN, Tsuji K, Glynn RJ, Wall C III, Rauch SD. Temporal bone studies of the human peripheral vestibular system. Normative Scarpa’s ganglion cell data. Ann Otol Rhinol Laryngol Suppl (2000) 181:14–9.
10. Park JJ, Tang Y, Lopez I, Ishiyama A. Age-related change in the number of neurons in the human vestibular ganglion. J Comp Neurol (2001) 431:437–43. doi:10.1002/1096-9861(20010319)431:4<437::AID-CNE1081>3.0.CO;2-P
11. Richter E. Quantitative study of human Scarpa’s ganglion and vestibular sensory epithelia. Acta Otolaryngol (1980) 90:199–208. doi:10.3109/00016488009131716
12. Alvarez JC, Díaz C, Suárez C, Fernández JA, González del Rey C, Navarro A, et al. Aging and the human vestibular nuclei: morphometric analysis. Mech Ageing Dev (2000) 114:149–72. doi:10.1016/S0047-6374(00)00098-1
13. Lopez I, Honrubia V, Baloh RW. Aging and the human vestibular nucleus. J Vestib Res (1997) 7:77–85. doi:10.1016/S0957-4271(96)00137-1
14. Zhou G, Kenna MA, Stevens K, Licameli G. Assessment of saccular function in children with sensorineural hearing loss. Arch Otolaryngol Head Neck Surg (2009) 135:40–4. doi:10.1001/archoto.2008.508
15. Singh NK, Kashyap RS, Supreetha L, Sahana V. Characterization of age-related changes in sacculocolic response parameters assessed by cervical vestibular evoked myogenic potentials. Eur Arch Otorhinolaryngol (2014) 7:1869–77. doi:10.1007/s00405-013-2672-0
16. Rosengren SM, Welgampola MS, Colebatch JG. Vestibular evoked myogenic potentials: past, present and future. Clin Neurophysiol (2010) 121:636–51. doi:10.1016/j.clinph.2009.10.016
17. Papathanasiou ES, Murofushi T, Akin FW, Colebatch JG. International guidelines for the clinical application of cervical vestibular evoked myogenic potentials: an expert consensus report. Clin Neurophysiol (2014) 125:658–66. doi:10.1016/j.clinph.2013.11.042
18. Curthoys IS. A critical review of the neurophysiological evidence underlying clinical vestibular testing using sound, vibration and galvanic stimuli. Clin Neurophysiol (2010) 121:132–44. doi:10.1016/j.clinph.2009.09.027
19. Rosengren SM, Govender S, Colebatch JG. Ocular and cervical vestibular evoked myogenic potentials produced by air- and bone-conducted stimuli: comparative properties and effects of age. Clin Neurophysiol (2011) 122:2282–9. doi:10.1016/j.clinph.2011.04.001
20. Welgampola MS, Colebatch JG. Characteristics and clinical applications of vestibular-evoked myogenic potentials. Neurology (2005) 24:1682–8. doi:10.1212/01.WNL.0000161876.20552.AA
21. Colebatch JG, Halmagyi GM. Vestibular evoked potentials in human neck muscles before and after unilateral vestibular deafferentation. Neurology (1992) 42:1635–6. doi:10.1212/WNL.42.8.1635
22. Colebatch JG, Halmagyi GM, Skuse NF. Myogenic potentials generated by a click-evoked vestibulocollic reflex. J Neurol Neurosurg Psychiatry (1994) 57:190–7. doi:10.1136/jnnp.57.2.190
23. Gonçalves DU, Felipe L, Lima TM. Interpretation and use of caloric testing. Braz J Otorhinolaryngol (2008) 74:440–6. doi:10.1590/S0034-72992008000300020
24. Stahle J. Controversies on the caloric response. From Bárány’s theory to studies in microgravity. Acta Otolaryngol (1990) 109:162–7. doi:10.3109/00016489009107430
25. Macdougall HG, McGarvie LA, Halmagyi GM, Curthoys IS, Weber KP. The video head impulse test (vHIT) detects vertical semicircular canal dysfunction. PLoS One (2013) 8:e61488. doi:10.1371/journal.pone.0061488
26. Patterson JN, Bassett AM, Mollak CM, Honaker JA. Effects of hand placement technique on the video head impulse test (vHIT) in younger and older adults. Otol Neurotol (2015) 36:1061–8. doi:10.1097/MAO.0000000000000749
27. Weber KP, MacDougall HG, Halmagyi GM, Curthoys IS. Impulsive testing of semicircular-canal function using video-oculography. Ann N Y Acad Sci (2009) 1164:486–91. doi:10.1111/j.1749-6632.2008.03730.x
28. Migliaccio AA, Cremer PD. The 2D modified head impulse test: a 2D technique for measuring function in all six semi-circular canals. J Vestib Res (2011) 21:227–34. doi:10.3233/VES-2011-0421
29. Agrawal Y, Zuniga MG, Davalos-Bichara M, Schubert MC, Walston JD, Hughes J, et al. Decline in semicircular canal and otolith function with age. Otol Neurotol (2012) 33:832–9. doi:10.1097/MAO.0b013e3182545061
30. Akin FW, Murnane OD, Tampas JW, Clinard CG. The effect of age on the vestibular evoked myogenic potential and sternocleidomastoid muscle tonic electromyogram level. Ear Hear (2011) 32:617–22. doi:10.1097/AUD.0b013e318213488e
31. Li C, Layman AJ, Carey JP, Agrawal Y. Epidemiology of vestibular evoked myogenic potentials: data from the Baltimore Longitudinal Study of Aging. Clin Neurophysiol (2015). doi:10.1016/j.clinph.2015.01.008
32. Maes L, Dhooge I, D’Haenens W, Bockstael A, Keppler H, Philips B, et al. The effect of age on the sinusoidal harmonic acceleration test, pseudorandom rotation test, velocity step test, caloric test, and vestibular-evoked myogenic potential test. Ear Hear (2010) 31:84–94. doi:10.1097/AUD.0b013e3181b9640e
33. Layman AJ, Li C, Simonsick E, Ferrucci L, Carey JP, Agrawal Y. Association between saccular function and gait speed: data from the Baltimore Longitudinal Study of Aging. Otol Neurotol (2015) 36:260–6. doi:10.1097/MAO.0000000000000544
34. Maleki M, Jafari Z, Zarrinkoob H, Akbarzadeh Baghban A. Effect of aging on saccular function. Med J Islam Repub Iran (2014) 28:117.
35. Nguyen KD, Welgampola MS, Carey JP. Test-retest reliability and age-related characteristics of the ocular and cervical vestibular evoked myogenic potential tests. Otol Neurotol (2010) 31:793–802. doi:10.1097/MAO.0b013e3181e3d60e
36. Chang CM, Young YH, Cheng PW. Age-related changes in ocular vestibular-evoked myogenic potentials via galvanic vestibular stimulation and bone-conducted vibration modes. Acta Otolaryngol (2012) 132:1295–300. doi:10.3109/00016489.2012.708437
37. Tseng CL, Chou CH, Young YH. Aging effect on the ocular vestibular-evoked myogenic potentials. Otol Neurotol (2010) 31:959–63. doi:10.1097/MAO.0b013e3181e8fb1a
39. Bruner A, Norris TW. Age-related changes in caloric nystagmus. Acta Otolaryngol Suppl (1971) 282:1–24.
40. Mallinson AI, Longridge NS. Caloric response does not decline with age. J Vestib Res (2004) 14:393–6.
41. Zapala DA, Olsholt KF, Lundy LB. A comparison of water and air caloric responses and their ability to distinguish between patients with normal and impaired ears. Ear Hear (2008) 29:585–600. doi:10.1097/AUD.0b013e3181734ed0
42. McGarvie LA, MacDougall HG, Halmagyi GM, Burgess AM, Weber KP, Curthoys IS. The video head impulse test (vHIT) of semicircular canal function – age-dependent normative values of VOR gain in healthy subjects. Front Neurol (2015) 6:154. doi:10.3389/fneur.2015.00154
43. MacDougall HG, Weber KP, McGarvie LA, Halmagyi GM, Curthoys IS. The video head impulse test: diagnostic accuracy in peripheral vestibulopathy. Neurology (2009) 73:1134–41. doi:10.1212/WNL.0b013e3181bacf85
44. Batuecas-Caletrio A, Klumpp M, Santacruz-Ruiz S, Gonzalez FB, Sánchez EG, Arriaga M. Vestibular function in cochlear implantation: correlating objectiveness and subjectiveness. Laryngoscope (2015). doi:10.1002/lary.25299
45. Matino-Soler E, Esteller-More E, Martin-Sanchez JC, Martinez-Sanchez JM, Perez-Fernandez N. Normative data on angular vestibulo-ocular responses in the yaw axis measured using the video head impulse test. Otol Neurotol (2015) 36:466–71. doi:10.1097/MAO.0000000000000661
46. Mossman B, Mossman S, Purdie G, Schneider E. Age dependent normal horizontal VOR gain of head impulse test as measured with video-oculography. J Otolaryngol Head Neck Surg (2015) 44:29. doi:10.1186/s40463-015-0081-7
Keywords: VEMP, vHIT, caloric vestibular stimulation, vestibular function tests, aging
Citation: Maheu M, Houde M-S, Landry SP and Champoux F (2015) The effects of aging on clinical vestibular evaluations. Front. Neurol. 6:205. doi: 10.3389/fneur.2015.00205
Received: 03 August 2015; Accepted: 07 September 2015;
Published: 22 September 2015
Edited by:
Yuri Agrawal, Johns Hopkins University, USAReviewed by:
Americo Migliaccio, Neuroscience Research Australia, AustraliaCopyright: © 2015 Maheu, Houde, Landry and Champoux. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: François Champoux, École d’Orthophonie et d’Audiologie, Faculté de Médecine, Université de Montréal, C.P. 6128, Succursale Centre-Ville, Montréal, QC H3C 3J7, Canada,ZnJhbmNvaXMuY2hhbXBvdXhAdW1vbnRyZWFsLmNh
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.