 Shakoor Ba-Ali
Shakoor Ba-Ali Birgit Sander
Birgit Sander Adam Elias Brøndsted
Adam Elias Brøndsted Henrik Lund-Andersen1,2
Henrik Lund-Andersen1,2
- 1Research Laboratory, Department of Ophthalmology, Glostrup Hospital, Glostrup, Denmark
- 2Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark
Purpose: The late post-illumination pupillary response (PIPR10–30s ) to blue light is reduced in glaucoma, suggesting that pupillometry can be used in clinical glaucoma evaluation. Since animal studies have indicated that common anti-glaucomatous agents affect the iris muscle, we investigated the short-term effect of the anti-glaucoma drugs on the pupillary light reflex and in particular on the PIPR10–30s.
Methods: In this randomized, double-masked, crossover trial, pupillometry was performed before and after topical administration of latanoprost, dorzolamide, and timolol in 20 healthy subjects. Stimulus was blue (463 nm) and red light (633 nm) of 2 log (lux). Main outcome was the PIPR10–30s to blue light. Additionally, pupil size, maximal contraction, and the early post-illumination pupillary response (PIPR0–10s ) to blue and red light were investigated. Pupil response variations between 8 a.m. and 2 p.m. were also assessed. Intraocular pressure (IOP) was measured before and 3.5 h after drug instillation.
Results: We found no drug effect on the blue light PIPR10–30s or any other blue light pupil parameters. During the control day, the only significant variation over time was observed for the red light PIPR0–10s (p = 0.02). Pupillary size decreased slightly with timolol (0.1 mm, p = 0.03) and dorzolamide (0.2 mm, p < 0.001), but not with latanoprost. Timolol also reduced the maximal contraction amplitude significantly during red light (p = 0.02). Intraocular pressure was significantly reduced by all three drugs after 3.5 h (p < 0.01), while it remained unchanged during the control day (p = 0.3).
Conclusion: Anti-glaucoma medications did not interfere with the blue light elicited PIPR. Dorzolamide reduced pupil size, while timolol reduced both pupil size and maximal contraction to red light, but the effect was minute and not of clinical importance.
Introduction
Chromatic pupillometry is a relatively novel research tool for the evaluation of outer and inner retina function. The outer retina photoreceptors (rod and cones) exhibit fast temporal kinetics and cause a brisk pupillary constriction in response to light, while the inner retinal melanopsin containing intrinsic photosensitive retinal ganglion cells (ipRGCs) exhibit slower temporal kinetics and elicit a sustained pupillary constriction to light stimuli, persisting after light cessation (1). The melanopsin elicited sustained pupillary response after light offset is termed post-illumination pupillary response (PIPR) (2). Three studies, using chromatic pupillometry, have shown decreased pupillary response and in particular reduced PIPR in glaucoma patients, indicating functional impairment of the ipRGCs (3–5). Thus, pupillometry may be applied as a quick, non-invasive, and objective method to evaluate glaucoma progression. However, the pupillary light response is affected by various physiological and environmental factors – importantly, topical anti-glaucoma drugs may alter this response.
Animal studies have shown that latanoprost and other ocular hypotensive prostaglandin analogs such as travoprost, prostaglandin F2α, and bimatoprost have different affinities to FP-, E2-, and D2-prostaglandin receptor subtypes (6–10). These prostaglandin receptors cause contraction in cat and bovine iris sphincter muscle (6, 9, 10). Dinslage et al. found that latanoprost decreases constriction latency and pupil size in glaucomatous human eyes (11). Pindolol, a non-selective beta-blocker used as an anti-glaucoma agent, reduced resting pupil size and contraction amplitude of pupillary light reflex in healthy adults (12). Dorzolamide, a carbonic anhydrase inhibitor used in glaucoma, did not affect the pupillary light reflex (13, 14).
The main purpose of this study was to investigate the short-term effect of anti-glaucoma medications on the blue light elicited PIPR in healthy individuals.
Materials and Methods
In this randomized, double-masked, crossover trial, the short-term effect of the three most frequently used anti-glaucoma eye drops (latanoprost 0.005%, timolol 0.5%, and dorzolamide 2%) on the pupillary light reflex were investigated by measuring the pupil response before and after administration of the eye drops.
Subjects
Twenty-six healthy non-smokers aged 18–40 years with best-corrected visual acuity ≥1.0 were screened during April–July 2014. Exclusion criteria were ocular disease, systemic disease, refractive error >6 diopters, history of ocular surgery, use of medications, caffeine consumption during day of testing, pregnancy, psychiatric disease, lack of cooperation, smoking, and ocular abnormalities. Ophthalmologic examinations were performed to ensure normal conditions: Snellen visual acuity, Ishihara color vision, swinging flash light test, slit lamp examination, and intraocular pressure (IOP) measurement by Goldmann and Icare tonometer (Icare TA01i, Icare Finland Oy, Helsinki, Finland). In addition, visual field test (Octopus 900, 30°, HAAG-STREIT AG, Koeniz, Switzerland), non-mydratic fundus photography (Mark II Retinal Camera TRC-NW7SF, Topcon Corporation, Tokyo, Japan), and optical coherence tomography (OCT) scanning of the macula and optic nerve head (Spectralis OCT, Heidelberg Engineering GmbH, Heidelberg, Germany) were conducted. Arterial blood pressure, pulse, iris color, height, and weight were recorded. Six individuals did not meet the inclusion criteria. Young participants were included to create a homogenous study population and to counter any age-related bias, thus purifying the effect of drugs.
The trial was approved by Danish National Committee on Health Research Ethics (project ID: H-2-2014-029). Informed consent was obtained according to WMA Declaration of Helsinki’s ethical guidelines.
Apparatus and Experimental Design
Pupillary response was recorded using a binocular multi-chromatic pupillometer (DP-2000 Human Laboratory Pupillometer, NeurOptics, Inc., CA, USA). This pupillometer consists of two separate integrated stimulation and recording units allowing for unilateral or bilateral eye stimulation while recording both the direct and the consensual pupillary response simultaneously. An adaptive eye cup prevents light scattering. The device is connected to a computer laptop with control software program.
The participants were assigned randomly to a sequence of latanoprost, timolol, and dorzolamide using a computer-generated randomization list including a fourth control test date without medication. Drugs were administered in a double masked fashion and washout period was minimum 1 week. In each experiment, pupil measurements were performed before (baseline), 30 and 180 min after drug application. Intraocular pressure was measured before and 3.5 h after medication. Measurements during the control visit were performed at equivalent hours. All experiments were conducted between 8 a.m. and 2 p,m. in April and September 2014 to avoid possible circadian and seasonal variations, respectively. The study eye for all participants was right eye.
Prior to pupillometry, subjects were adapted to dark for 5 min. For each measurement, the pupil size was recorded for 10 s prior to light onset, 20 s during the light stimulation, and 60 s after the stimulus offset (Figure 1). First, participants were exposed to red light (633 nm, 2 log (lux), measured as 300 CD/m2) and 5 min later to blue light (463 nm, 2 log (lux), measured as 332 CD/m2). The binocular camera tracks and measures both pupils continuously with a frequency of 30 Hz. For both eyes, pupil diameters (millimeters), recording time (seconds), and luminance (lux) were recorded.
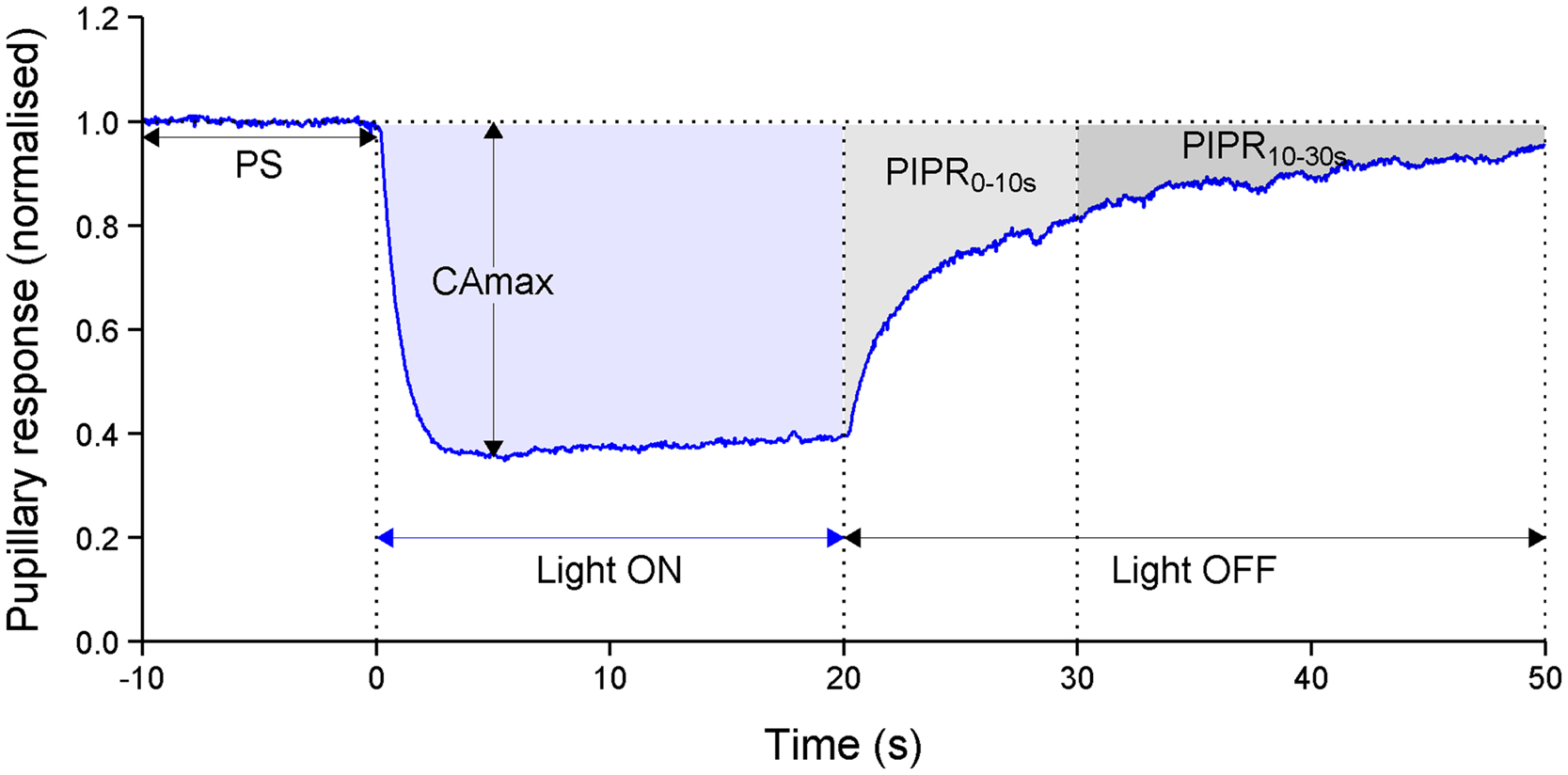
Figure 1. An example of the pupillary light reflex to blue light (463 nm, 100 lux) and outcomes of this study. The pupillary response is expressed as normalized. Time is in seconds (s). PS = mean of absolute pupillary diameter during the initial 10 s prior to light onset, CAmax = maximal contraction amplitude during 4–6 s of illumination time, PIPR0–10s = mean of early post-illumination pupillary response 0–10 s after light offset and PIPR10–30s = mean of late post-illumination pupillary response over a period of 10–30 s after light termination.
Data Processing and Outcomes
Raw data were imported into the R-statistical package (version 3.1.0). An algorithm was used to detect and correct artifacts generated by eyelid blinks. If it was not possible to remove blinks by the algorithm, correction was performed manually.
The pupil diameter was normalized, i.e., expressed as the ratio relative to the baseline pupil size, and a total of three parameters were calculated to describe the pupillary response (15):
(1) The late post-illumination pupil response (PIPR10–30s), indicative of melanopsin photo pigment activation, was defined as the mean pupil constriction from 10 to 30 s after light termination (16).
(2) The early PIPR0–10s, a measure of mixed cone and melanopsin response, was defined as the mean pupil response from 0 to 10 seconds after light termination (16).
(3) Maximal contraction amplitude (CAmax), a measure of cone response, was the maximum pupil constriction during 4 and 6 s of stimulation period (16).
Primary outcome was the PIPR10–30s to blue light. Secondary outcomes, likewise for blue light, were the dark-adapted pupil size before light onset (PS), maximal contraction amplitude (CAmax), and PIPR0–10s (see Figure 1). For all the outcomes, the pupillary response to red light was also measured.
Statistical Analysis
SAS 9.3 and R-statistical package (3.1.0) were used to perform statistical analysis and graphics. Data were summarized as mean and SD for continuous variables, assuming normally distributed. The pupillary response was analyzed in relation to timing (before vs. after medication) and drug type with separate one-way analysis and the paired observations were accounted by a random statement (random coefficient model) of the mixed model procedure. The overall comparisons between drugs and control were performed with the procedure described above, followed by post hoc tests for pairwise comparison of the drugs and control; a Tukey statement was used to adjust for multiple comparisons.
Results
Subject
Final study population consisted of 20 subjects, 8 female and 12 male with mean age 25 ± 5.39 years. All subjects had normal visual field, color vision, and IOP (13 ± 2.24 mmHg). Mean body mass index was 24 ± 3.59 kg/m2 and iris color distribution was as the following: brown (55%), blue (35%), and green (10%).
Outcome
In the following, for each outcome, baseline examination refers to pupillary measurements before medication at the start of each examination day, effect of drug over time is the comparison of pupillary response at baseline vs. after medication (30 and 180 min), and comparison between drugs and control is the testing of the results for drugs against control measurements at 30 and 180 min (Tables 1–4).
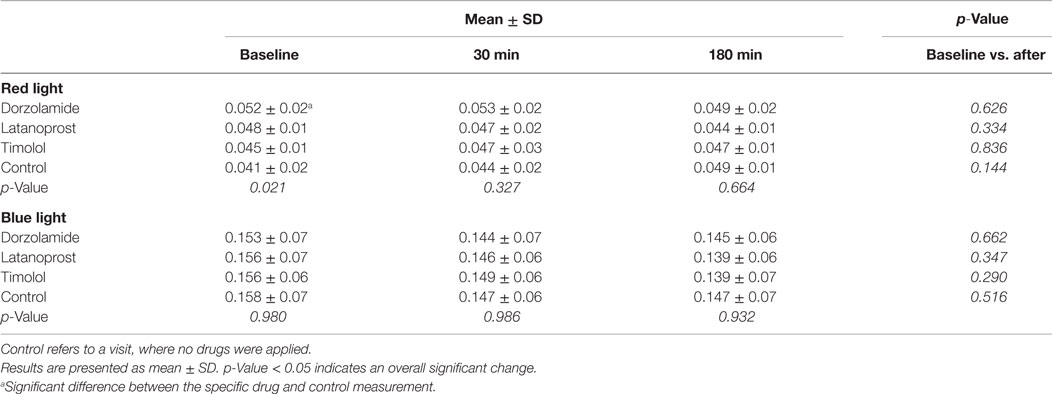
Table 1. Late post-illumination pupillary response (PIPR10–30s) to red and blue light measured at baseline and after (30 and 180 min) topical anti-glaucoma administration.
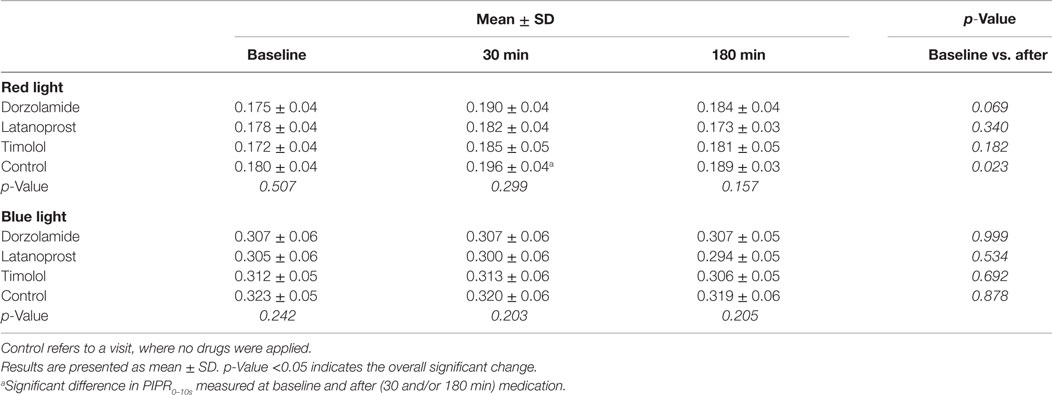
Table 2. Early post-illumination pupillary response (PIPR0–10s) to red and blue light measured at baseline and after (30 and 180 min) topical anti-glaucoma administrations.
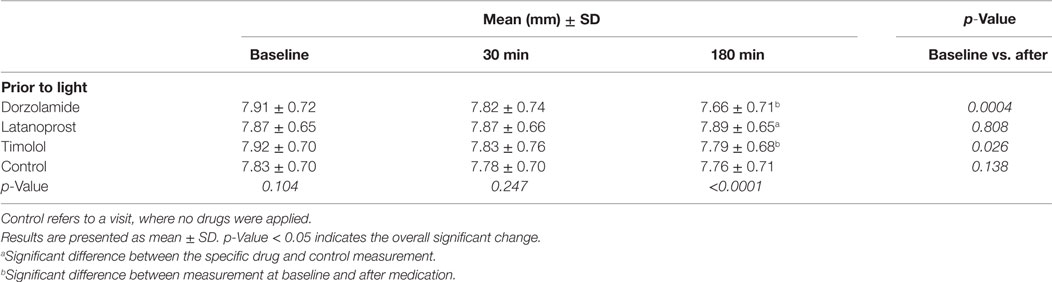
Table 3. Pupil size (PS) in millimeter at baseline and after (30 and 180 min) application with dorzolamide, latanoprost, and timolol.
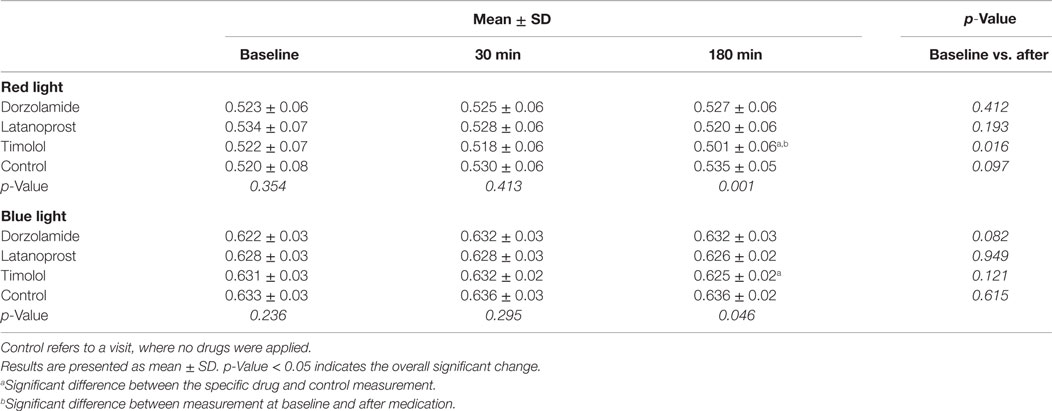
Table 4. Maximal contraction amplitude (CAmax) to red and blue light measured before (baseline) and after (30 and 180 min) topical anti-glaucoma administration.
Late PIPR
Baseline examination
The late PIPR10–30 s to blue light was similar during the days of examination (p = 0.980, Table 1; Figure 2). For red light, the response was significantly different (p = 0.021, Table 1). Post hoc analysis showed that the difference only applied to the day of dorzolamide application (p = 0.003).
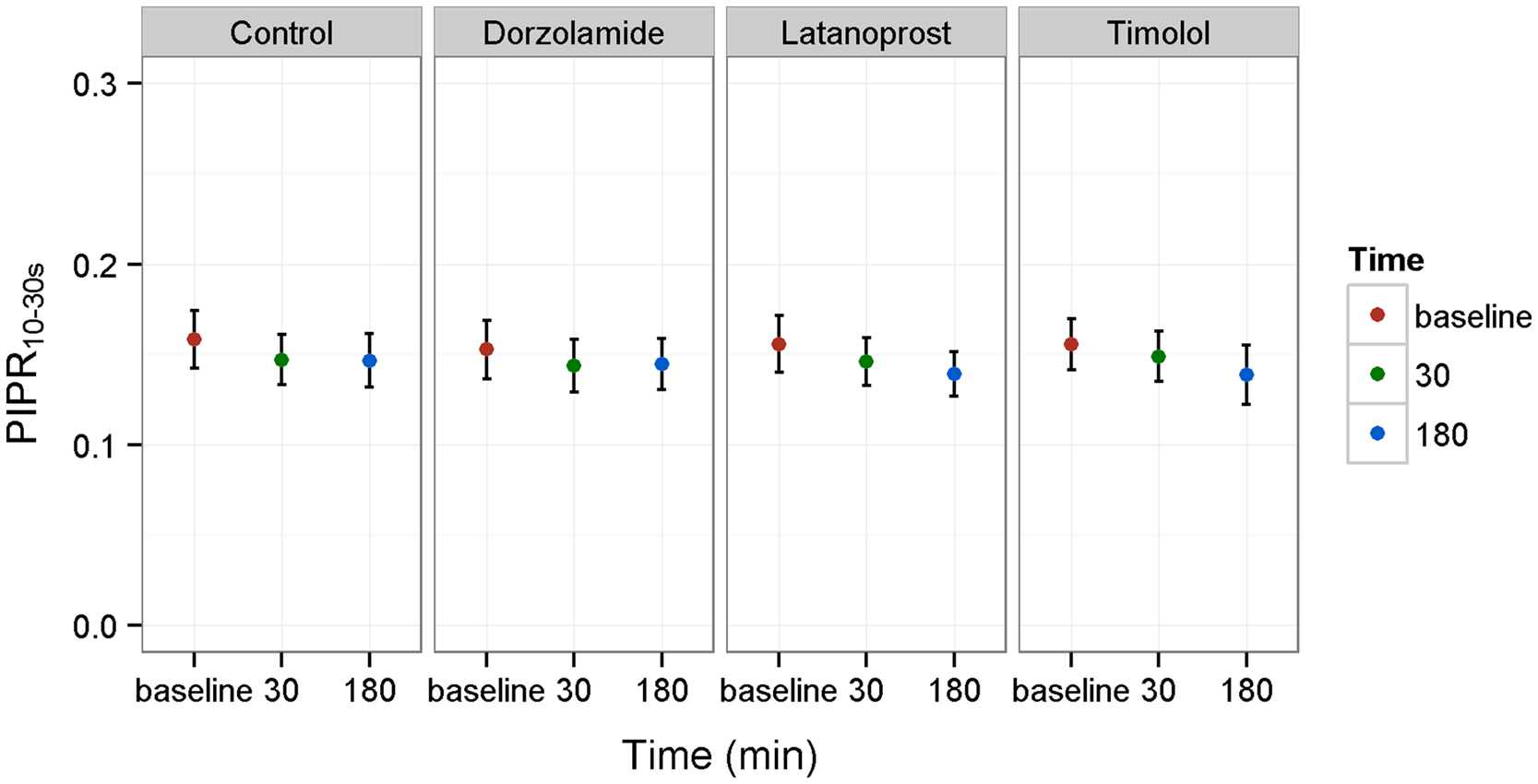
Figure 2. Late post-illumination pupillary response (PIPR10–30s) to blue light and the effect of timolol, dorzolamide, and latanoprost. Control refers to measurements without medication. PIPR10–30s is presented as mean values ± SD. Time is given as baseline (base.) and after (30 and 180 min) drug application.
Effect of Drug over Time
comparing baseline PIPR10–30s to measurements after medication, none of the drugs changed PIPR10–30s to blue or red light significantly (p > 0.1 for all data, Table 1).
Comparison Between Drugs and Control
No significant differences were found when comparing PIPR10–30s measured during the days the participants received drugs and the control day (p > 0.1, Table 1).
Early PIPR
Baseline Examination
The post-illumination pupillary constriction 0–10 s after light offset (PIPR0–10s) was similar in all examination days, both for red and blue light stimulation (red p = 0.507, blue p = 0.242, Table 2).
Effect of Drug over Time
The early PIPR0–10s to both red and blue light was not significantly different between baseline and after topical instillation with timolol, dorzolamide, or latanoprost (p > 0.1 for all data, Table 2). We did see a significant increase in PIPR0–10s during the control day after red light stimulation (p = 0.023), but not after blue light (p = 0.878). Post hoc analysis showed that the difference after red light was significant between baseline and 30 min, but not at 180 min (Table 2).
Comparison Between Drugs and Control
No significant differences were seen for either blue or red light comparing the PIPR0–10s after drug applications against control measurements (Table 2).
Pupil Size
Baseline Examination
Pupil size (PS), measured prior to light onset, did not vary significantly at the start of each examination day, i.e., before drug administration (p = 0.104, Table 3).
Effect of Drug over Time
Dorzolamide and timolol reduced PS significantly (dorzolamide, p = 0.0004 and timolol, p = 0.026, Table 3). Latanoprost did not change the PS significantly (p = 0.808).
Comparison Between Drugs and Control
The overall comparison showed that PS was significantly different at 180 min (p < 0.0001), but not at 30 min. Post hoc analyses identified that pupil size was largest for latanoprost compared to control (0.12 mm, p = 0.026); dorzolamide and timolol had not significantly different effect compared to control values (Table 3).
To examine any carryover effect from red to blue light, additional analyses were performed to compare the PS prior to red light stimulation to that before blue light, as measured 5 min later. For the initial baseline examination, we found a statistically significant difference (p = 0.0232), however the difference was clinically negligible (0.05 mm, less than 1%). For the measurements at 30 and 180 min, the PS was unchanged between before red light illumination and prior to blue light (p > 0.05).
Maximal Contraction Amplitude
Baseline Examination
CAmax to both red and blue light at the start of each examination days did not differ significantly (Table 4).
Effect of Drug over Time
CAmax to blue light did not change significantly before and after glaucoma medications, except for red light, where a significant decrease was found at 180 min after instillation with timolol (p = 0.016).
Comparison Between Drugs and Control
Both red and blue light were significantly different at 180 min (red light p = 0.001, blue light p = 0.046). Post hoc analysis showed that the decreased contraction amplitude was due to timolol (Table 4).
Effect of Covariates on PIPR and CAmax
For all parameters mentioned above including effect of drugs over time and comparisons between drugs and control, the outcomes were analyzed after adjustment for baseline PS, age, gender, and iris color. For CAmax to blue light, the p-value did not reach statistical significance after adjustment for the baseline PS in the model thereby the p-value of 0.046 (Table 4) was reduced to 0.086. No other conclusions were changed. In addition, we did not find changes of the results due to the different randomization schemes of the drugs.
Intraocular Pressure
Intraocular pressure before and after drug application and for control measurements are summarized in Table 5. All three drugs reduced IOP significantly (p < 0.01) after 3.5 h, while the IOP during control day increased slightly, although not significantly (p = 0.3).
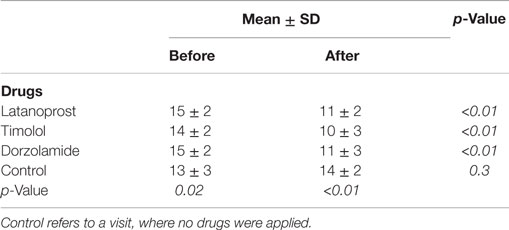
Table 5. Intraocular pressure (IOP) measured before and 3.5 h after topical anti-glaucoma administration.
Discussion
Previous studies have shown that anti-glaucoma drugs affect the iris. The dilator and sphincter muscles of the iris regulate the pupillary size. The main objective of this study was to investigate whether the topical anti-glaucoma drugs can alter the PIPR to blue light in healthy individuals. This issue is important as pupillometry is gaining more ground in the evaluation of glaucoma. The approach was to compare the pupillary light response in healthy subjects before and after topical administration of timolol, dorzolamide, and latanoprost. As an additional control and to assess the variations of pupillary responses over a short time period (8 a.m. to 2 p.m.), we performed pupillometry during a control day, where no medication was applied (control).
Our results demonstrate that PIPR to blue light was unaffected by dorzolamide, latanoprost, or timolol (Tables 1 and 2) and no significant difference in hour-to-hour measurements through the control day was observed. The comparisons between drugs and control measurements during baseline examinations and after medications neither showed significant differences (Tables 1 and 2).
PIPR to red light was likewise unaffected by anti-glaucoma eye drops. There was a significant variation in the PIPR10–30 before administration of dorzolamide in comparison to control measurement (Table 1). In addition, the PIPR0–10s to red light increased through the control day without any medication (Table 2). These two statistically significant findings in relation to red light may have the following possible explanations. As reported earlier by Herbst et al., both the PIPR0–10s and PIPR10–30s to red light show low reproducibility (15). Previous studies have shown that PIPR to continuous light of both red and blue colors exhibits significant variations over 24 h (17, 18). Our measurements were performed from 8 a.m. to 2 p.m., and PIPR0–10s to red light for both drugs and control increased during the three subsequent measurements throughout the daytime. Subjective sleepiness during the first measurement at the early morning could be an explanation for this increment, such that the test persons become more alert later on the day; Münch et al. showed a correlation between increased subject sleepiness and smaller PIPR (18), matching our findings, despite not recording the subjects” alertness during the day. Future experiments could begin with a trial stimulation to “awaken the subject” or could stimulate the pupil later in the day, e.g., commence at 10 a.m.
Since PIPR to blue light depends on the initial pupil size before light onset (19), we investigated the effect of anti-glaucoma eye drops on the PS. Dorzolamide reduced PS by 2.4% after 3 h (0.0004). Plummer et al. did not show any significant change in PS after application with dorzolamide in glaucomatous dogs (14). The inconsistency between our and Plummer’s findings could be explained by possible species differences in the effects of dorzolamide on the iris contractile muscle, in the same way as it was observed by Kaddour-Djebbar et al. for prostaglandin receptor agonist on the iris muscle (10).
Latanoprost did not change PS at 0.5 or 3 h (Table 3). Previous reports were contradictory, e.g., Dinslage et al. showed that latanoprost reduced PS in glaucomatous human eyes, while Marchini et al. did not report any significant change in glaucoma patients (11, 20).
Timolol reduced PS significantly 3 hours after medication (Table 3). This miotic effect was very small (1.64%), consistent with previous human studies, which also demonstrated a slightly non-significant decrease or no change of note in PS (21, 22).
The reducing effect of dorzolamide on the PS was also reported by Pfeiffer et al., although their results were statistically not significant (23).
The miotic effect of dorzolamide and timolol is an interesting finding since in case of substantial alteration in the PS, PIPR to blue light changed significantly as shown by Nissen et al. (19). For the results reported here, all conclusions remained unchanged after adjusting for the PS. Thus, dorzolamide and timolol have a slight, but clinical unimportant miotic effect.
The baseline examinations of the PS did not change significantly between examination days, indicating that no carryover effect was found from the drugs. We also evaluated if the pause of 5 min between red and blue light stimuli in our protocol was sufficient for the pupils to return to baseline; for the morning examination (i.e., baseline), a significant decrease in PS prior to blue light compared to PS before red light stimulation was observed. However, the difference was only 0.05 mm (<1%) and no differences were found for the examination at 30 and 180 min. Thus, 5 min is a sufficient time interval between light stimulations.
The PS did not change significantly during control measurements at 8 a.m. to 2 p.m. (Table 3), which is consistent with earlier reports investigating the PS variation over a short time period (17, 18).
Blue light CAmax during control day was consistent, revealing no variations from 8 a.m. to 2 p.m. in contrast to previous findings, Table 4 (17, 18). However, in our study, we did all the measurements between 8 a.m. and 2 p.m. to avoid the diurnal effect.
The difference observed between timolol and control in blue light CAmax at 180 min could be explained by modulations of CAmax over weeks since the time lag between control measurements and the examination day, we applied timolol, was minimum 1 week. In addition, the difference was not found when the model was adjusted for baseline PS.
Timolol reduced red light elicited CAmax by 3.85% after 180 min and moreover, there was a significant difference when comparing the drug against control (Table 4). Previous study reported similar effect of the non-selective beta-blocker pindolol on the contraction amplitude (12).
Study Limitations
One limitation of the present study was that we investigated the short-term effect of topical glaucoma medications. Latanoprost induces iris hyperpigmentation after continual use for approximately 7 months (24). However, while excessive doses of latanoprost may cause iritis, long-term trials do not indicate any adverse effects on the iris dynamics (25, 26). Dorzolamide has a very long terminal plasma elimination half-life (> 120 days), so for this drug, there could be a possible risk of drug effect several weeks following its instillation. To shed light on this issue, we investigated the carryover effect for the different drugs and found no significant change compared to baseline values. The long-term (1-year) adverse effects of timolol were studied very carefully by Sherwood et al. in a prospective trial – pupillary side effects were not reported (27).
Another limitation of the study is the role of preservatives in the three drugs. Since benzalkonium chloride (BAC) is added as preservative in all the three drugs, any possible effect of this preservative on the pupillary light reflex would not be identified in this short-term study. Benzalkonium chloride is shown to be a cytotoxic substance and cause apoptosis in conjunctival, corneal, and trabecular meshwork tissues (28–30). Although the penetration of BAC into the rabbit iris after topical instillation has been shown, its cytotoxic damage on the iris tissue has not been reported yet (31). To our knowledge, the adverse effect of the BAC on the iris has neither been investigated in pupillometry yet.
The age difference of our study population was 18–40 years, thus not representative of the common elderly glaucoma patients. Certain changes, possibly affecting the pupillary light response, occur with age: age-related miosis, photoreceptor degeneration, and decreased light transmission of especially blue light to the retina (32–34). However, currently three studies have investigated the effect of the age on the blue light elicited PIPR and neither of them showed any significant correlation between age and PIPR (2, 19, 35). In particular, Herbst et al. did not show correlation between age-related decrease in lens transmission and blue light elicited PIPR10–30s (35). Moreover, in our younger study population, the effect of the drugs on the pupillary response was not biased by other possible age-related factors, which are not yet known. We do not expect any effect of glaucoma drugs on PIPR10–30s in elderly individuals, such as glaucoma patients. However, our findings in a small number of young adults will need to be reproduced in a larger group of patients of older age, more typical of glaucoma patients, before the study can be applied directly to glaucoma patients.
Conclusion
Our results demonstrate that PIPR (both PIPR10–30s and PIPR0–10s) to blue light was not affected by anti-glaucoma medications. Red light elicited PIPR was not affected by topical glaucoma drugs either, however since the early PIPR0–10s to red light increased significantly over a time period of 8 a.m. to 2 p.m. without medication, we suggest that this parameter is inconsistent and the results should be interpreted with caution. Dorzolamide decreased the dark-adapted PS, while timolol reduced both PS and CAmax for red light, but neither of these effects was of clinical importance.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors thank the Synoptic Foundation and Velux Foundation for their grant support.
References
1. Kardon R, Anderson SC, Damarjian TG, Grace EM, Stone E, Kawasaki A. Chromatic pupil responses: preferential activation of the melanopsin-mediated versus outer photoreceptor-mediated pupil light reflex. Ophthalmology (2009) 116(8):1564–73. doi: 10.1016/j.ophtha.2009.02.007
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
2. Kankipati L, Girkin CA, Gamlin PD. Post-illumination pupil response in subjects without ocular disease. Invest Ophthalmol Vis Sci (2010) 51(5):2764–9. doi:10.1167/iovs.09-4717
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
3. Kankipati L, Girkin CA, Gamlin PD. The post-illumination pupil response is reduced in glaucoma patients. Invest Ophthalmol Vis Sci (2011) 52(5):2287–92. doi:10.1167/iovs.10-6023
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
4. Feigl B, Mattes D, Thomas R, Zele AJ. Intrinsically photosensitive (melanopsin) retinal ganglion cell function in glaucoma. Invest Ophthalmol Vis Sci (2011) 52(7):4362–7. doi:10.1167/iovs.10-7069
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
5. Nissen CSB, Milea D, Kolko M, Herbst K, Hamard P, Lund-Andersen H. Monochromatic pupillometry in unilateral glaucoma discloses no adaptive changes subserved by the ipRGCs. Front Neurol (2014) 5:15. doi:10.3389/fneur.2014.00015
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
6. Sharif NA, Kaddour-Djebbar I, Abdel-Latif AA. Cat iris sphincter smooth-muscle contraction: comparison of FP-class prostaglandin analog agonist activities. J Ocul Pharmacol Ther (2008) 24(2):152–63. doi:10.1089/jop.2007.0076
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
7. Sharif NA, Kelly CR, Crider JY, Williams GW, Xu SX. Ocular hypotensive FP prostaglandin (PG) analogs: PG receptor subtype binding affinities and selectivities, and agonist potencies at FP and other PG receptors in cultured cells. J Ocul Pharmacol Ther (2003) 19(6):501–15. doi:10.1089/108076803322660422
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
8. Ansari HR, Kaddour-Djebbar I, Abdel-Latif AA. Effects of prostaglandin F2alpha, latanoprost and carbachol on phosphoinositide turnover, MAP kinases, myosin light chain phosphorylation and contraction and functional existence and expression of FP receptors in bovine iris sphincter. Exp Eye Res (2004) 78(2):285–96. doi:10.1016/j.exer.2003.10.015
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
9. Ansari HR, Davis AM, Kaddour-Djebbar I, Abdel-Latif AA. Effects of prostaglandin F2alpha and latanoprost on phosphoinositide turnover, myosin light chain phosphorylation and contraction in cat iris sphincter. J Ocul Pharmacol Ther (2003) 19(3):217–31. doi:10.1089/108076803321908347
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
10. Kaddour-Djebbar I, Ansari HR, Akhtar RA, Abdel-Latif AA. Species differences in the effects of prostanoids on MAP kinase phosphorylation, myosin light chain phosphorylation and contraction in bovine and cat iris sphincter smooth muscle. Prostaglandins Leukot Essent Fatty Acids (2005) 72(1):49–57. doi:10.1016/j.plefa.2004.10.001
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
11. Dinslage S, Diestelhorst M, Kuhner H, Krieglstein GK. [The effect of latanoprost 0.005% on pupillary reaction of the human eye]. Ophthalmologe (2000) 97(6):396–401. doi:10.1007/s003470070087
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
12. Smith SE, Smith SA, Reynolds F, Whitmarsh VB. Ocular and cardiovascular effects of local and systemic pindolol. Br J Ophthalmol (1979) 63(1):63–6. doi:10.1136/bjo.63.1.63
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
13. Pek H, Wilhelm H. [Effect of dorzolamide on accommodation and pupillary reaction?]. Ophthalmologe (2000) 97(11):769–73. doi:10.1007/s003470070026
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
14. Plummer CE, MacKay EO, Gelatt KN. Comparison of the effects of topical administration of a fixed combination of dorzolamide-timolol to monotherapy with timolol or dorzolamide on IOP, pupil size, and heart rate in glaucomatous dogs. Vet Ophthalmol (2006) 9(4):245–9. doi:10.1111/j.1463-5224.2006.00469.x
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
15. Herbst K, Sander B, Milea D, Lund-Andersen H, Kawasaki A. Test-retest repeatability of the pupil light response to blue and red light stimuli in normal human eyes using a novel pupillometer. Front Neurol (2011) 2:10. doi:10.3389/fneur.2011.00010
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
16. Gamlin PD, McDougal DH, Pokorny J, Smith VC, Yau KW, Dacey DM. Human and macaque pupil responses driven by melanopsin-containing retinal ganglion cells. Vision Res (2007) 47(7):946–54. doi:10.1016/j.visres.2006.12.015
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
17. Munch M, Leon L, Crippa SV, Kawasaki A. Circadian and wake-dependent effects on the pupil light reflex in response to narrow-bandwidth light pulses. Invest Ophthalmol Vis Sci (2012) 53(8):4546–55. doi:10.1167/iovs.12-9494
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
18. Zele AJ, Feigl B, Smith SS, Markwell EL. The circadian response of intrinsically photosensitive retinal ganglion cells. PLoS One (2011) 6(3):e17860. doi:10.1371/journal.pone.0017860
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
19. Nissen C, Sander B, Lund-Andersen H. The effect of pupil size on stimulation of the melanopsin containing retinal ganglion cells, as evaluated by monochromatic pupillometry. Front Neurol (2011) 2:92. doi:10.3389/fneur.2011.00092
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
20. Marchini G, Ghilotti G, Bonadimani M, Babighian S. Effects of 0.005% latanoprost on ocular anterior structures and ciliary body thickness. J Glaucoma (2003) 12(4):295–300. doi:10.1097/00061198-200308000-00002
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
21. Gilmartin B, Hogan RE, Thompson SM. The effect of timolol maleate on tonic accommodation, tonic vergence, and pupil diameter. Invest Ophthalmol Vis Sci (1984) 25(6):763–70.
22. Nordmann JP, Mertz B, Yannoulis NC, Schwenninger C, Kapik B, Shams N. A double-masked randomized comparison of the efficacy and safety of unoprostone with timolol and betaxolol in patients with primary open-angle glaucoma including pseudoexfoliation glaucoma or ocular hypertension. 6 month data. Am J Ophthalmol (2002) 133(1):1–10. doi:10.1016/S0002-9394(01)01337-X
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
23. Pfeiffer N, Gerling J, Lippa EA, Brunner-Ferber FL, Panebianco D, Grehn F. Comparative tolerability of topical carbonic anhydrase inhibitor MK-927 and its S-enantiomer MK-417. Graefes Arch Clin Exp Ophthalmol (1991) 229(2):111–4. doi:10.1007/BF00170540
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
24. Chou SY, Chou CK, Kuang TM, Hsu WM. Incidence and severity of iris pigmentation on latanoprost-treated glaucoma eyes. Eye (2005) 19(7):784–7. doi:10.1038/sj.eye.6701663
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
25. Alm A. Latanoprost in the treatment of glaucoma. Clin Ophthalmol (2014) 8:1967–85. doi:10.2147/OPTH.S59162
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
26. Linden C, Alm A. The effect on intraocular pressure of latanoprost once or four times daily. Br J Ophthalmol (2001) 85(10):1163–6. doi:10.1136/bjo.85.10.1163
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
27. Sherwood MB, Craven ER, Chou C, DuBiner HB, Batoosingh AL, Schiffman RM, et al.Twice-daily 0.2% brimonidine-0.5% timolol fixed-combination therapy vs monotherapy with timolol or brimonidine in patients with glaucoma or ocular hypertension: a 12-month randomized trial. Arch Ophthalmol (2006) 124(9):1230–8. doi:10.1001/archopht.124.9.1230
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
28. De Saint Jean M, Debbasch C, Brignole F, Rat P, Warnet JM, Baudouin C. Toxicity of preserved and unpreserved antiglaucoma topical drugs in an in vitro model of conjunctival cells. Curr Eye Res (2000) 20(2):85–94. doi:10.1076/0271-3683(200002)2021-DFT085
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
29. Ayaki M, Yaguchi S, Iwasawa A, Koide R. Cytotoxicity of ophthalmic solutions with and without preservatives to human corneal endothelial cells, epithelial cells and conjunctival epithelial cells. Clin Experiment Ophthalmol (2008) 36(6):553–9. doi:10.1111/j.1442-9071.2008.01803.x
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
30. Baudouin C, Denoyer A, Desbenoit N, Hamm G, Grise A. In vitro and in vivo experimental studies on trabecular meshwork degeneration induced by benzalkonium chloride (an American Ophthalmological Society thesis). Trans Am Ophthalmol Soc (2012) 110:40–63.
31. Desbenoit N, Schmitz-Afonso I, Baudouin C, Laprevote O, Touboul D, Brignole-Baudouin F, et al.Localisation and quantification of benzalkonium chloride in eye tissue by TOF-SIMS imaging and liquid chromatography mass spectrometry. Anal Bioanal Chem (2013) 405(12):4039–49. doi:10.1007/s00216-013-6811-7
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
32. Daneault V, Vandewalle G, Hebert M, Teikari P, Mure LS, Doyon J, et al.Does pupil constriction under blue and green monochromatic light exposure change with age? J Biol Rhythms (2012) 27(3):257–64. doi:10.1177/0748730412441172
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
33. Freund PR, Watson J, Gilmour GS, Gaillard F, Sauve Y. Differential changes in retina function with normal aging in humans. Doc Ophthalmol (2011) 122(3):177–90. doi:10.1007/s10633-011-9273-2
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
34. Kessel L, Lundeman JH, Herbst K, Andersen TV, Larsen M. Age-related changes in the transmission properties of the human lens and their relevance to circadian entrainment. J Cataract Refract Surg (2010) 36(2):308–12. doi:10.1016/j.jcrs.2009.08.035
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
35. Herbst K, Sander B, Lund-Andersen H, Broendsted AE, Kessel L, Hansen MS, et al.Intrinsically photosensitive retinal ganglion cell function in relation to age: a pupillometric study in humans with special reference to the age-related optic properties of the lens. BMC Ophthalmol (2012) 12:4. doi:10.1186/1471-2415-12-4
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Keywords: melanopsin, glaucoma, pupillometry, pupillary light reflex, latanoprost, timolol, dorzolamide, iris
Citation: Ba-Ali S, Sander B, Brøndsted AE and Lund-Andersen H (2015) Effect of topical anti-glaucoma medications on late pupillary light reflex, as evaluated by pupillometry. Front. Neurol. 6:93. doi: 10.3389/fneur.2015.00093
Received: 02 March 2015; Accepted: 16 April 2015;
Published: 29 April 2015
Edited by:
Gabriella Szatmáry, Hattiesburg Clinic PA, USAReviewed by:
Heather Mack, Eye Surgery Associates, AustraliaLaszlo Marsovszky, SE Semmelweis University, Hungary
Copyright: © 2015 Ba-Ali, Sander, Brøndsted and Lund-Andersen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution and reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shakoor Ba-Ali, Department of Ophthalmology, Glostrup Hospital, Nordre Ringvej 57, Glostrup DK-2600, Denmark,c2JhYTAwMDVAcmVnaW9uaC5kayw=c2hha29vckBzaGFrb29yLmRr