
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neuroinform. , 13 May 2024
Volume 18 - 2024 | https://doi.org/10.3389/fninf.2024.1379932
This article is part of the Research Topic Innovative Methods for Sleep Staging Using Neuroinformatics View all 8 articles
 Benedikt Holm1,2*
Benedikt Holm1,2* Gabriel Jouan1,2*Emil Hardarson1,2
Gabriel Jouan1,2*Emil Hardarson1,2 Sigríður Sigurðardottir2Kenan Hoelke2,3Conor Murphy2,4
Sigríður Sigurðardottir2Kenan Hoelke2,3Conor Murphy2,4 Erna Sif Arnardóttir1,2
Erna Sif Arnardóttir1,2 María Óskarsdóttir1,2†
María Óskarsdóttir1,2† Anna Sigríður Islind1,2†
Anna Sigríður Islind1,2†Introduction: Polysomnographic recordings are essential for diagnosing many sleep disorders, yet their detailed analysis presents considerable challenges. With the rise of machine learning methodologies, researchers have created various algorithms to automatically score and extract clinically relevant features from polysomnography, but less research has been devoted to how exactly the algorithms should be incorporated into the workflow of sleep technologists. This paper presents a sophisticated data collection platform developed under the Sleep Revolution project, to harness polysomnographic data from multiple European centers.
Methods: A tripartite platform is presented: a user-friendly web platform for uploading three-night polysomnographic recordings, a dedicated splitter that segments these into individual one-night recordings, and an advanced processor that enhances the one-night polysomnography with contemporary automatic scoring algorithms. The platform is evaluated using real-life data and human scorers, whereby scoring time, accuracy, and trust are quantified. Additionally, the scorers were interviewed about their trust in the platform, along with the impact of its integration into their workflow.
Results: We found that incorporating AI into the workflow of sleep technologists both decreased the time to score by up to 65 min and increased the agreement between technologists by as much as 0.17 κ.
Discussion: We conclude that while the inclusion of AI into the workflow of sleep technologists can have a positive impact in terms of speed and agreement, there is a need for trust in the algorithms.
The emergence of explainable artificial intelligence (XAI) presents vast potential for revolutionizing various application areas, such as in healthcare (De Bock et al., 2023). However, despite the great potential, there are significant issues that need to be tackled before XAI can be fully utilized (Jermutus et al., 2022). One such issue originates from application areas within healthcare, where automation of manual tasks and data-driven decision-support has to take the central stage before XAI can become a viable option (Loh et al., 2022).
A subfield of healthcare is the collection and analysis of sleep recordings, referred to as polysomnography (PSG) (Arnardottir et al., 2021). A PSG is an overnight recording of various biomedical signals, such as an electroencephalogram (EEG), electromyogram (EMG), electrooculogram (EOG), and various respiratory signals. Upon collection, the PSG must be manually annotated by a sleep technologist which is a cumbersome and time-consuming task (Arnardottir et al., 2021). PSG scoring is a vital step in the process of identifying and diagnosing the presence of many sleep disorders, some of which are extremely prevalent (Benjafield et al., 2019). A sleep technologist will manually review the recording according to a set of rules devised by the American Academy of Sleep Medicine (AASM), labeling events such as respiratory events, and sleep stages in a process referred to as scoring. The sleep stage scoring is done by assigning a specific class to each 30-s segment (also called epochs) in the recording. The sleep stages classes are categorized into five categorical values: the Wake (W) class for wake period, the rapid eye movement category (REM) and three non-REM stages (N1, N2, and N3) that respectively describe the depth of sleep. A product of the PSG scoring is the creation of a hypnogram, a graphical representation tracing the progression of sleep stages throughout the night. This visual tool, often complemented by a hypnodensity graph, provides a detailed overview of the patient's sleep architecture, capturing transitions between sleep stages (Jang et al., 2022; Pevernagie and Arnardottir, 2024). Self-applied-PSG (henceforth referred to as simply PSG), a newly designed simplified version of traditional PSG, utilizing frontal EEG instead of the conventional International 10–20 System, refers to a type of sleep study that the participant can set up themselves and sleep with at home for up to three nights in the current work (Arnardottir et al., 2022).
One of the main drawbacks of the current scoring process is, as stated earlier, that it can be excessively time-consuming, which can cause considerable delays in providing sleep reports to healthcare providers and consequently delay diagnosis (Biedebach et al., 2024), as well as increase the cost of healthcare considerably (Wickwire, 2021). Adding to this challenge, significant inter-scorer variability exists (Nikkonen et al., 2024); disagreements can reach 19.3% for sleep stages (Nikkonen et al., 2024) and 11.6% for respiratory events (Redline et al., 2007). Delays and disagreements such as these can have negative effects on patient outcomes, as untreated sleep disorders can have a significantly negative impact on patient health (Dikeos and Georgantopoulos, 2011).
The advent of machine learning and other automatic scoring algorithms offers a potential solution by automating the process of manual scoring, which the AASM sees great potential in Goldstein et al. (2020). However, the development and application of machine learning are often prohibitively technical, requiring diverse knowledge of computer science to achieve (Giray, 2021; Brennan and Kirby, 2022). There is also a dire need for socio-technical alignment, i.e. the multi-disciplinary collaboration between the computer scientists integrating the algorithms, and the professionals working in the context in which the algorithms are being integrated (Brennan and Kirby, 2022). The integration of AI, machine learning, or advanced data-driven decision-making of any kind into the workflow may move the industry professionals from a generative role (creating the outputs themselves) to the role of auditors, where they correct the output of the algorithms, and consult with computer scientists to tweak and alter the models to handle edge cases or incorrect generations by the algorithm (Grønsund and Aanestad, 2020). Moreover, in the rare case when socio-technical alignment is reached, trust issues often surface, where the professionals working within the context that the algorithms are integrated into, may not trust the outcomes (Islind and Hult, 2022), which has posed a great limitation in healthcare (Lee and Yoon, 2021; Jermutus et al., 2022). This mistrust has received limited focus in terms of research contributions and needs to be studied further.
Machine learning models are often deemed a “black box,” owing to their lack of transparency and the extensive technical knowledge needed to understand them. Moreover, their incapacity to adapt to dynamically evolving requisites often leads to their obsolescence. This has resulted in the increasing prevalence of human-in-the-loop AI systems (Mosqueira-Rey et al., 2023). Human-in-the-loop AI systems allow one or more human experts to take an active part in the training process by continuously evaluating the model and providing new inputs that are then selectively used to re-train the model in a process called active learning (Settles, 2009).
To advance and modernize sleep research as well as to enable the collection of a large-scale European sleep recording dataset, the Sleep Revolution project, a joint venture involving 24 European partners, was initiated (Arnardottir et al., 2022). Each partner contributes ~60 sets of three-night PSGs. Sleep technologists then evaluate these on a shared workstation which is a part of the Sleep Revolution high-performance cluster. After this, healthcare professionals analyze sleep parameters, which helps them to diagnose the patient. A significant objective of the Sleep Revolution is to reduce scoring time (Arnardottir et al., 2022). One strategy to achieve that goal is to direct the focus of the sleep technologists to the areas of sleep that automatic algorithms have less “certainty” of. By displaying these areas of high uncertainty, referred to as gray areas from now on, we can specifically target the sleep technologists toward these areas, instead of unilaterally trusting or mistrusting the automatic scoring algorithms (Jouan et al., 2023).
Most of the research done on automatic sleep staging algorithms mainly focuses on the increase in model prediction accuracy or agreement. With recent datasets mobilizing an ensemble of independent sleep technologists scoring the same record, research on uncertainty quantification, such as gray area identification in the domain of sleep staging, is growing (Bakker et al., 2023; Rusanen et al., 2023; Nikkonen et al., 2024). However, the union of sleep staging algorithms, including selectively focusing the attention of sleep technologists using uncertainty or gray areas during sleep scoring, is a newborn concept that needs to be assessed.
To enable these algorithms to benefit sleep technologists in their daily work, a system is required that bridges the gap between the data collection and the manual scoring itself. To collect the data required for this work, a digital platform was designed to handle automatically collecting, segmenting, and processing the PSG. The concept of digital platforms takes into account that a digital platform is both a piece of software, while it is also an intermediary that connects needs with resources. Therefore the concept of digital platforms encompasses a larger array than the software itself as it, in a socio-technical manner, also takes the context into account. In this case, the digital platform is accessed via the users' web browser and is hereinafter referred to as the platform.
Computer-assisted automatic scoring with manual review has demonstrated the ability to reduce PSG scoring time significantly, with some studies showing improvements by factors of 1.26–2.41 (Alvarez-Estevez and Rijsman, 2022). Moreover, automatic sleep scoring algorithms can halve the scoring time (Liang et al., 2019; Choo et al., 2023).
Some research on the integration of automated scoring has been conducted in the last few years as listed in Table 1. Rayan et al. (2023) discuss the challenges and advancements in automatic sleep scoring in the context of rodent and human sleep research. They note limitations in handling atypical data and lack of flexibility but also note that automatic algorithms can make the process more efficient. A recent study evaluated a deep-learning-based automatic scoring software for its accuracy and efficiency compared to manual scoring. The results indicated a high correlation between the automatic scoring system and manual scoring, particularly in sleep staging and the apnea-hypopnea index. The automatic scoring system also demonstrated a significant reduction in manual scoring time, leading to improved workflow efficiency in sleep laboratories (Choo et al., 2023). Oxholm et al. (2021) interviewed nine healthcare professionals and five patients about their attitudes toward using data from electronic health records in an algorithm to screen for alcohol abuse in hospitals. Professionals were mixed in their views, appreciating the tool's time-saving potential but concerned about losing instinctual decision-making. While this work is only tangentially related to our work, the authors point out the requirement to include healthcare professionals in the process of integrating automatic algorithms. Gerla et al. (2018) presented a computer-assisted approach for sleep staging using EEG recordings and AASM 2012 scoring rules, focusing on real clinical data with artifacts and missing electrodes, evaluating the influence of AI in clinical settings by comparing traditional manual sleep stage classification with AI-based methods, including expert-in-the-loop strategies, for the analysis of EEG recordings in sleep studies. In a later study, Gerla et al. (2019) developed a semi-supervised method for evaluating PSG, blending expert-scored segments with automated classification. This approach, tested on both healthy individuals and chronic insomnia patients, showed enhanced efficiency and accuracy in sleep data analysis compared to conventional manual scoring methods, demonstrating the impactful role of AI in streamlining sleep study workflows.

Table 1. Comparison of contributions of this work and similar work.
As is evident from Table 1, existing research on automatic sleep scoring addresses either the impact on workflow or the opinions of medical professionals on AI in the workflow. To the best of our knowledge, no research exists that addresses the integration of automatic sleep scoring into existing work environments which is an important aspect to consider to achieve socio-technical alignment.
To fill this research gap, we designed both a platform and a process for evaluating the effectiveness of introducing gray areas into the work of sleep technologists and their trust in the process. By integrating the platform featuring machine learning algorithms into the work of sleep technologists through our empirical case within the Sleep Revolution, we extrapolate three main contributions. Firstly, we outline the architecture for a platform that has been designed and developed to enable the integration of automatic scoring. Secondly, we introduce the concept of “gray areas” as a method of selectively focusing the attention of sleep technologists on fewer areas in the PSG. Thirdly, we illustrate the decreased scoring time and increased agreement gained by integrating the automatic scoring algorithms into the workflow of sleep technologists. Throughout this research, and particularly when analyzing the results, we realized that the phenomena we encountered consistently and that was common to all of our results, was missing a clear clinical terminology that we attempt to address in this work.
PSG sharing and scoring between research centers require sophisticated architectures that rest heavily on the principles of storing and processing medical data cohesively. The proposed platform has the main purpose of connecting needs with resources, which in this case outlines the sharing and scoring of PSG between research centers.
The methodology is three-fold; (1) the design and development of the platform, (2) the validation of the platform, and (3) interviews with sleep technologists. The design section covers the architecture, components, and technologies chosen to implement the platform, the validation section covers how the platform was assessed in terms of processing duration, sleep technologist speed, and agreement improvements, and the interview section describes how sleep technologists were interviewed for their sentiment toward integrating AI tools into the workflow.
The platform needed to be conceived in agreement with the main constraints as having a simple user interface for sleep technologists to be able to authenticate and upload their PSG; providing administrative oversight on uploads from different centers; being fault-tolerant; and being scalable (Prasad, 2015). The platform is split into three distinct components:
1. Web-based front-end for user uploads, administration, and dispatching of jobs to the other components (henceforth referred to as the front end).
2. Three-night PSG splitter (henceforth referred to as the splitter).
3. Processing pipeline that augments PSGs with automatic scorings (henceforth referred to as the processor).
Figure 1 shows an overview of the platform architecture. An important feature of the platform is to allow users (e.g., sleep technologists and healthcare professionals) to upload multiple PSGs to be shared and scored at the same time without breaking the platform. To achieve this, the FastAPI Python web framework was used, which despite its simplicity handles multi-user web applications supporting asynchronous code (tiangolo, 2023). The platform is protected with a user login access in which each user is a validated member of Sleep Revolution consortium (Sle, 2021).

Figure 1. Overview of the platform showing how the front end, processor, and splitter are combined.
Additionally, the front end handles receiving signals from both the splitter and the processor via HTTP requests and issuing jobs to the splitter when a new PSG is received and to the processor when a PSG has successfully been split. Splitting is necessary when several nights' PSG are combined into one file. The job queue was achieved using a RabbitMQ queuing server, which is a program that allows disparate asynchronous programs to communicate by listening and issuing messages to a queue (RabbitMQ Contributors, 2007). By utilizing a message-queue protocol, the font end can offload more time and memory-consuming projects such as generating automatic scorings to other processes, thus reducing the probability of users experiencing downtime, or data loss.
The processor is the final component of the architecture. Its purpose is to prepare the individual night PSG by augmenting the PSG with the AI scoring, along with the gray area scoring. The output of the processor is twofold. Firstly, the processor prepares a “scoring” version of the PSG that is augmented with predicted sleep stages from an automatic scoring algorithm integrating gray areas and is made available for manual scoring, and a version meant for later computer processing and machine learning. Each component was containerized using the virtualization software Docker (Merkel, 2014) for enhanced isolation, consistency, and reproducibility during deployments, which is important in sustainable and secure development.
As introduced previously, the processor prepares the PSG to be manually scored, stored, and ready for further analysis. To reduce the manual work of the sleep technologists, a crucial step in the processor is highlighting areas in the PSG that are hard to score for the algorithm, i.e. gray areas. The gray area augmentation works first by sending each one-night PSG EDF file to the trained deep learning model aSAGA (Rusanen et al., 2023). The aSAGA architecture is based on a revisited U-time architecture for scoring and respiratory events prediction (Perslev et al., 2021; Huttunen et al., 2022). The U-time is an encoder-decoder structure consisting of blocks of consecutive convolutional, batch normalization, and pooling layers. However, in the aSAGA algorithm, a single-channel model is used, which was first trained on PSGs' EEG (C4-M1) and then fine-tuned with an EOG (E1-M2) channel using self-applied PSGs with frontal setup. This was done to have generalizability between EEG and EOG channels and to increase the compliance of the model for frontal EEG and EOG setups. The aSAGA model is parameterized to return a hypnogram of the same length as the number of epochs from the signal input. The model has an accuracy of 80% estimated over different scored sleep datasets. This accuracy is on par with manual scoring Nikkonen et al. (2024), however, the gray areas from aSAGA model prediction have been validated by comparing the match with the gray areas from predicted manual scoring uncertainty.
The second part concerns the gray areas. Using the predicted hypnodensity from the aSAGA model as input, a trained clustering algorithm tags each epoch that belongs to the gray areas (Jouan et al., 2023). The clustering algorithm is a multi-objective method based on multinomial mixture models clustering the different levels of sleep technologist agreement and summarizing the results into two sets of high-agreement and gray area clusters. The threshold is selected according to the maximization of the distance between two distributions of the sleep technologist's agreement measure. When the algorithm receives a new hypnodensity, it outputs a hypnogram called aSAGA-UA with gray area. Figure 2B illustrate such predicted hypnogram where each gray area are represented as a line discontinuity named “whitespace.”
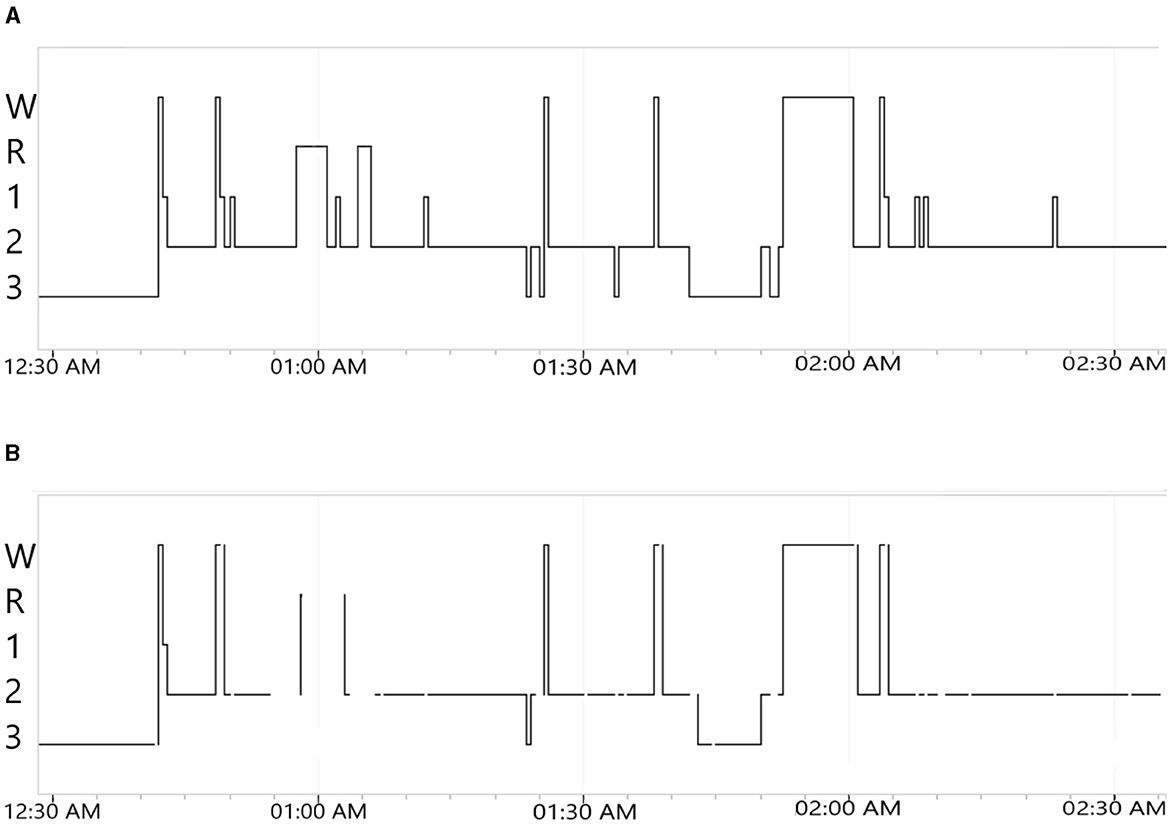
Figure 2. Example of output 2 h hypnograms for the no. 1 PSG from 50 × 10PSG, obtained using the processor and rendered in Nox Medical's Noxturnal software for manual review. (A) aSAGA predicted 2 h hypnogram. W, wake; R, rapid-eye-movement; 1, 2 and 3 are respectively for N1, N2, and N3. (B) aSAGA-UA predicted 2 h hypnogram with gray areas. Each discontinuity in the hypnogram line represent a gray area. W: Wake; R: Rapid-Eye-Movement; 1, 2 and 3 are respectively for N1, N2 and N3.
Using aSAGA-UA, it becomes easier for the sleep technologists to view epochs where the AI scoring may not be accurate, and need to be re-evaluated. In Figure 2A between 12:30 a.m. and 1:30 there are many transitions between Wake, N1, N2, and REM scored by the algorithm. For the same time period in Figure 2B, there are many line discontinuities characterized by a whitespace symbolizing gray areas. For instance, the predicted N1 and REM sleep stages in Figure 2A are not present in Figure 2B where whitespaces are clearly visible instead. Regarding the high number of sleep transitions happening in a few minutes, the associated signal might be hard to interpret by the algorithm. A manual review from the sleep technologist is needed in that part of the hypnogram. The method has been evaluated on a real case of uncertainty analysis of 50 PSGs manually scored by 10 sleep technologists. We refer to this dataset as 50 × 10PSG. This dataset comes from a cohort of 50 participants that have previously been scored by ten independent sleep technologists to create a consensus scoring (Jouan et al., 2023; Rusanen et al., 2023). After testing the clustering algorithm on predicted hypnodensities from aSAGA, the threshold separating the gray area clusters from other epochs was lowered to 0.73 according to a sleep technologist's recommendations. The new value avoids the creation of an excessive amount of white spaces in the final hypnogram.
All three components were hosted on a Linux virtual machine run on a Cisco Hyperflex high-performance compute system located at Reykjavik University. The virtual machine was equipped with 10 Intel(R) Xeon(R) Gold 6248R central processing units, and 20 gigabytes of random access memory.
The platform is validated with the help of three sleep technologists, referred to from this point as Sleep Technologist One, Sleep Technologist Two, and Sleep Technologist Three (ST1, ST2, and ST3 respectively). ST1 and ST2 are experienced sleep technologists, whereas ST3 is considered less experienced. Each sleep technologist was asked to score a randomly selected subset of from the 50 × 10PSG. The sleep technologists looked at multiple channels when scoring the data, using the NoxTurnal sleep study annotation program. The EOG channels E2 and E3 referenced against AFz were used to track eye movements, the EEG channels AF3, AF4, AF7, AF8 all referenced against the average value of the eye channels E3 and E4 were used to observe EEG activity. There were no EMG electrodes as part of the setup, however the sleep technologists used the muscle component derived from the eye electrodes to their aid in scoring. Each sleep technologist received half of the subset scored with a default proprietary industry-standard automatic scoring and the other half had the automatic scoring with gray areas (aSAGA-UA). We also refer to these to options as without and with AI, respectively. The partitioning of the subsets can be seen in Table 2.
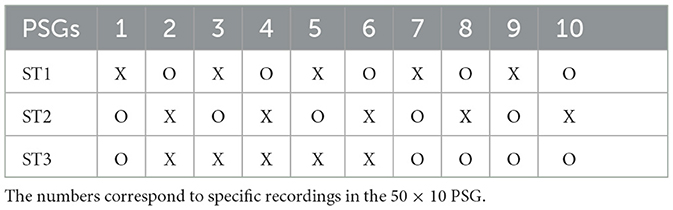
Table 2. The layout of PSGs to be scored, where X indicates default automatic scoring and O indicates aSAGA-UA, that is aSAGA with gray areas.
The sleep technologists were instructed to score sleep stages and arousals. The PSGs with the default automatic scoring were manually reviewed as sleep technologists would normally do in a clinical setting, reviewing every epoch manually. For the PSGs with aSAGA-UA, only the gray areas were manually reviewed by the sleep technologists. The standard operating proceeding follows these specific steps:
1. Start by running automatic analysis.
2. Adjust the time frame from lights out to lights on (start and stop times for the correct analysis period).
3. Score sleep stages and arousals according to AASM version v. 3.0 (Troester et al., 2023).
4. For the aSAGA-UA scoring, after reviewing all visible gray areas, look for possible missed epochs by searching for sleep stage scorings that contain the word “uncertain,” and correct them.
Each sleep technologist was asked to accurately measure the duration of the scoring process for each PSG in their subset. Subseqently, their scoring was collected andcompared it to the existing consensus scoring from the 50 × 10 PSG. The scoring accuracy of the sleep technologists using the system as support was assessed via Fleiss's multi-rater (Fleiss, 1971) κ coefficient. This coefficient κ∈[0, 1] measures the agreement of the current sleep technologist sequence to the scoring sequences given by the ten sleep technologists in the consensus scoring. In the case of samples with high agreement between sleep technologists, Fleiss's κ coefficient converges to 1 and 0 otherwise.
The perceived trust and reliability of the automated scoring system were evaluated through semi-structured interviews with the three sleep technologists, following an interview guide. These 30-min interviews aimed to explore the sleep technologists' confidence in the system's output and their comfort in integrating the system into their workflow. The sleep technologists provided feedback on the system's overall performance, as well as reflected on their trust in the system's automatic scoring algorithm and gray area identification. The interviews were transcribed verbatim and relevant segments of the interviews were and the qualitative data was analyzed with thematic analysis.
This section is divided into three main subsections. Firstly, we present the performance of the platform itself. Secondly, we present the performance gain in terms of both scoring time and agreement of the sleep technologists. Thirdly, we present the results from interviews with sleep technologists.
Table 3 lists the time taken by the two main components of the pipeline, the splitter and the processor. Since the platform must split the upload into individual nights before further processing, the initial three-night PSG takes ~458.5 s (7.6 min) to become available for scoring, including both splitting and processing time. However, for the subsequent PSGs, the sleep technologists mainly perceived the processing time, which averages 336.2 s (5.6 min) per PSG. The processing time for later PSGs is negligible, as the sleep technologist can begin scoring the first file while the others are being processed. Consequently, the processing time is optimally utilized, preventing any significant delays in the scoring workflow. When employed in the early stages of the data collection, the queue sizes of the splitter and processor did not grow to excessive lengths, with the processor queue generally not exceeding the size of three pending processing jobs.

Table 3. Samples of processing time in minutes (min) taken by each queue according to file size in mego octets (Mo).
The front end was designed to be clean, and provide a structured interface to submit both the PSG itself and information about the participant. A screen grab of the user interface is presented in Figure 3.

Figure 3. Front end user interface for uploading recordings.
This section provides insights into sleep technologists' performance when using the AI for scoring. Each sleep technologist received an identical set of PSGs to score, both with and without aSAGA-UA. Here, the analysis encompasses the sleep technologist's time efficiency and agreement metrics.
In the following section, the study results first delve into the outcomes of the sleep technologist's time to score. Figure 4 displays the scoring duration for each of the 10 PSGs and all sleep technologists with and without aSAGA-UA assistance. As seen in Figure 4A, ST1 using aSAGA-UA assistance shows an average ± standard deviation scoring duration of 20.8 ± 8 min compared to 36.8 ± 16 min for ST2. ST1 reviews faster than ST2. This efficiency translates into an average scoring duration reduction of 16 min.
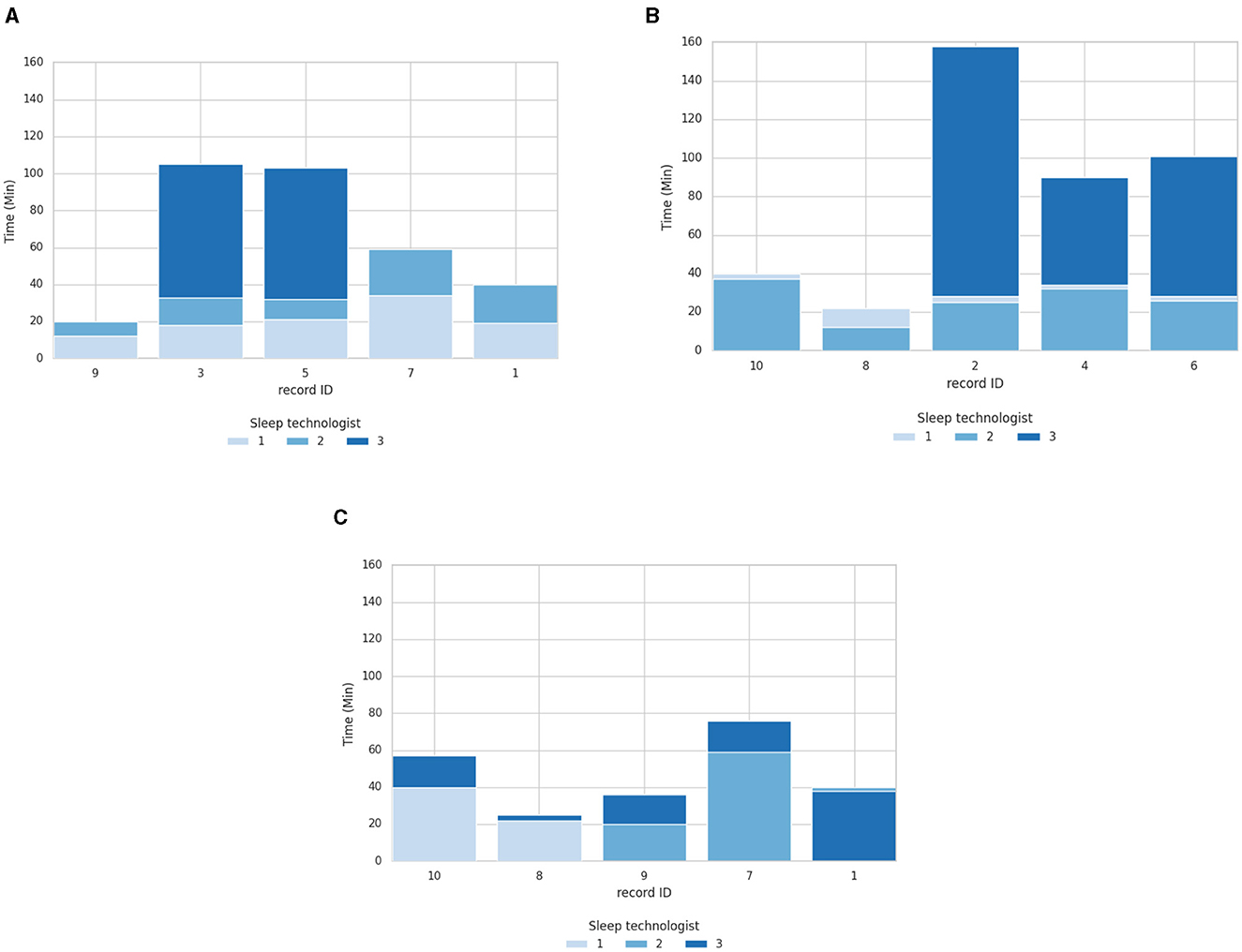
Figure 4. Overlapped bars of scoring duration comparison of PSG with one sleep technologist using aSAGA-UA and the other two using the standard procedure. (A) Scoring duration with ST1 using pipeline aSAGA-UA assistance. (B) Scoring duration with ST2 using pipeline aSAGA-UA assistance. (C) Scoring duration with ST3 using pipeline aSAGA-UA assistance.
Meanwhile, as seen in Figure 4B, when using aSAGA-UA, ST2 approximately equaled the time of ST1. ST2 displayed a scoring duration of 26 ± 9 min, and ST1 displayed 30 ± 6 min, with ST2 reducing their mean scoring duration by 4 min when using aSAGA-UA. Finally, Figures 4A, B display ST3 having a time of 111 ± 26.7 min without AI. ST3, as the least experienced in this study, was noticeably slower in scoring than the other sleep technologists. However, Figure 4C shows that ST3 depicted a significant decrease in the time to score, of 46 ± 20.2 when using aSAGA-UA, or a reduction of 65 min.
Turning to the agreement analysis, Table 4 is divided into two parts; the first half details the sleep technologist's agreement based on the analysis of the complete PSGs, while the second half assesses the agreement specifically for the gray area epochs which the sleep technologist handled with aSAGA-UA assistance.

Table 4. Fleiss's multi-rater κ mean ± standard deviation estimated on overall hypnograms and gray areas epochs only by sleep technologists manually scoring and using aSAGA-UA assistance.
When the agreement was calculated based on gray areas, the sleep technologist using aSAGA-UA assistance was the only one aware of the nature of these epochs. A steady trend in the overall agreement of sleep technologists using AI for scoring is observed in Table 4. However, the agreement rating of ST3 appears to be negatively affected by the use of aSAGA-UA assistance. This reduction is possibly attributed to a more challenging sample of associated PSGs, which generally achieved a lower agreement score, but this is not clear.
Figure 5 shows the agreement analysis of each of the three sleep technologists in this study with the 50 × 10 PSG with and without aSAGA-UA. The performance levels of ST3, represented in Figures 5A, C, consistently matched or surpassed the levels achieved by ST1 and ST2 while using the aSAGA-UA tool. However, there is a discernible decrease in scoring agreement for the three PSGs illustrated in Figure 5E when ST3 utilizes aSAGA-UA. Despite this decrease, the performance levels of ST3 generally remained comparable to and occasionally exceeded those of ST2. Moreover, across all three Figures 5A, C, E, the agreement of the sleep technologists stayed consistent, indicating that the scorings produced traditionally and using aSAGA-UA are comparable. For instance, PSGs IDs 1, 7, 8, and 10 all display complete agreement, having been scored twice by the sleep technologists using aSAGA-UA.
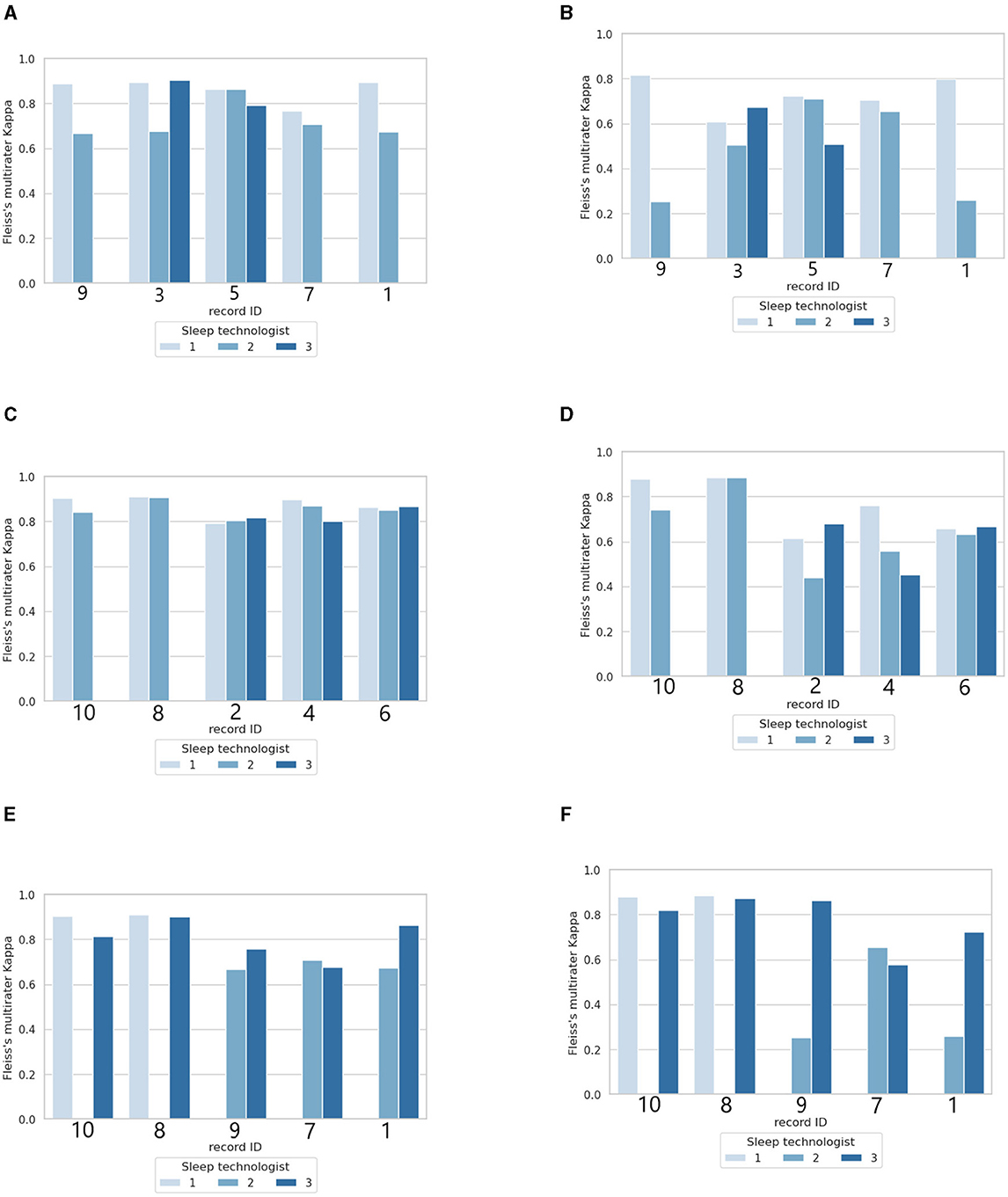
Figure 5. Agreement analysis of 10 sleep technologists compared to a sleep technologist with or without aSAGA-UA assistance. The first column (A, C, E) shows the total agreement per polysomnographs. The second column (B, D, F) shows the agreement for gray area epochs tagged by the artificial intelligence. (A) Fleiss's multiraters κ overview with ST1 using aSAGA-UA assistance. (B) Fleiss's multiraters κ of only gray area epochs with ST1 using aSAGA-UA assistance. (C) Fleiss's multiraters κ overview with ST2 using aSAGA-UA assistance. (D) Fleiss's multiraters κ of only gray area epochs with ST2 using aSAGA-UA assistance. (E) Fleiss's multiraters κ overview with ST3 using aSAGA-UA assistance. (F) Fleiss's multiraters κ of only gray area epochs with ST3 using aSAGA-UA assistance.
A second aspect depicted in Table 4 is the agreement of the sleep technologists only calculated for the gray areas on both samples (sleep technologists using aSAGA-UA assistance and without aSAGA-UA assistance). In this table, ST2 and ST3 got a marked increase in their agreement when using aSAGA-UA, with ST2 and ST3 gaining ~0.17 κ, but with ST1 a decrease of 0.03 κ for the gray areas.
Figures 5B, D, F offer the Fleiss's multiraters κ estimated on only gray areas per PSG ID. In this comparison, only the sleep technologist using aSAGA-UA knew that these epochs were labeled as gray areas. As expected, in Figures 5B, D, F, ST1 depicted the same stability observed previously. ST2 and ST3 showed an increase in κ when using aSAGA-UA. The increase, however, was less strong for ST2 who showed more agreement's dispersion among the PSGs. Otherwise, in Figure 5F, ST3's agreement showed a significant increase for PSGs 1 and 9 compared to ST2's agreement which might explain the difference in Figure 5E. This last result indicates that aSAGA-UA assistance may benefit a beginner more than an experienced sleep technologist.
In summary, all the participating sleep technologists showed a decrease in their time to score but to a different degree. Regarding their scoring agreement, the sleep technologists depicted three distinct results when using aSAGA-UA. The agreement of the experienced sleep technologist with the PSG signals was not affected by aSAGA-UA. On the other hand, the second experienced sleep technologist has shown more dispersion among the PSG with on average an increase when using aSAGA-UA. Finally, the third, less experienced sleep technologist benefited the most from aSAGA-UA assistance.
The sleep technologists were interviewed about their experience when using aSAGA-UA. The transcript of the interviews was compiled as a word cloud (Figure 6).
Figure 6. A word cloud of the interview transcripts.
Initially, the sleep technologists approached the new system with optimism. ST1 expressed initial enthusiasm: “[Before starting] I was very optimistic that it would decrease the scoring time.” All sleep technologists found it simple to integrate AI scoring with gray areas into their current workflows with ST3 commenting “I do not think it is an issue at all […] it is pretty easy to implement.”
However, as they used the new system, the sleep technologists noticed a need for a more accurate staging algorithm, with ST1 noting “What I saw is that the algorithm is not good enough.” For ST1 and ST3, improved accuracy is essential for reducing the scoring time and building trust in the new system. ST2 provided a slightly different perspective, suggesting that the system's staging accuracy might already be on par with the inter-scorer agreement of human sleep technologists.
Overall, all three sleep technologists expressed in various ways that trust in AI technology is significant for its continual adaptation into their practice. The sleep technologists articulated the psychological impact of integrating AI staging with gray areas into their workflows. ST2 expressed concern that the AI suggestion might slightly shift their bias in selecting a sleep stage. ST3 spoke along similar lines: “Maybe I had an unconscious bias to lean toward the [suggested sleep stage].”
Overall, the sleep technologists found the new system promising and were optimistic about the approach. ST3 was interested in seeing a more detailed quantification of the gray area uncertainty, asking for “the percentage of the prediction or something like that.” However, all sleep technologists agreed that improving the staging algorithm's accuracy was important, as ST1 put it: “You need to trust the algorithm.” Their sentiments reflected a cautious optimism, recognizing the potential benefits while anticipating enhancements in usability and trust as the accuracy of the underlying staging algorithm improves.
This paper introduces an advanced web platform aimed at filling the gap of sharing, processing, and storing three subsequent nights of PSG in the sleep research field. The platform has three distinct components: a front end, a PSG splitter, and a processor component with automatic scoring and storing of each PSG. The front end is connected with the two subsequent parts using a flexible message-queue protocol, preventing the front end from crashing in case of failure in the processing of PSGs. The platform was tested on a set of 60 three-night PSGs files. The average processing time of the platform ranged between 5.6 min, for an associated file size of 1,920 Mo, and 7.6 min, for a file of size 2,400 Mo.
Moreover, the automatic scoring, including the gray areas implemented in the processor component has been assessed with the help of three sleep technologists. The predicted scores by the platform showed a decidedly positive effect on the speed of scoring. This enhancement is achieved without significantly complicating the workflow of sleep technologists. The strategic incorporation of AI support into their routine not only optimizes the time efficiency of scoring but also adds a layer of precision and reliability to the process. The most experienced sleep technologists showed a high agreement on an average of 0.85 κ when using AI support. This value of agreement is in line with the observed agreement obtained for other data sets manually scored (Rosenberg and Hout, 2013). Additionally, a significant increase in both the scoring speed and agreement was observed for the less experienced sleep technologist, suggesting that the use of automatic algorithms and gray area assistance has the potential to bridge the gap between more experienced sleep technologists and the less experienced ones, and thus speeding up the training of new sleep technologists.
Utilizing a message queue protocol imparted a considerable complication in implementing the platform that would have been avoidable if we had instead opted for a separate process using e.g. HTTP requests, or implemented the splitting and processing as part of the same program as the front end. Utilizing message queues in favor of more ad-hoc solutions allowed us more flexibility and scalability than with other solutions. The need to split PSGs similarly complicated the work, since it added a component to the process. However, the benefits gained from working with separate nights later in the process outweighed this added complexity.
In the results part, the processor component has been evaluated over a study composed of three sleep technologists with different experiences scoring 10 PSGs with and without aSAGA-UA. However, the dispersion obtained in the results reflected a lack of PSG required to obtain an accurate representation of the time to score and sleep technologists' agreement distributions. A study with a greater number of PSGs would allow us to validate the result obtained in the presented paper. Moreover, using aSAGA-UA, the effectiveness of the sleep technologists in terms of scoring duration is affected differently. Their disparity may be explained by the difference in experience with the self-applied PSG frontal signals, the baseline speed of both sleep technologists, and the trust given to the AI-predicted scores in the gray areas. Furthermore, a study with a higher number of PSGs and more sleep technologists is needed to have a better estimation of the effectiveness obtained by the use of AI as a scoring support tool.
The interviews revealed the sleep technologists' agreement that the platform integrated well into their workflow, with ST3 commenting especially on the ease of implementation. The sleep technologists did raise issues with the performance of the scoring algorithm itself, with ST1 reporting that the scoring algorithm is “not good enough.” ST3 expressed some concern that the sleep stage recommendation system was influencing their decision-making. This worry reflects the need for trust and alignment between the sleep technologist and the algorithms, especially in the context of healthcare AI recommendation systems. As the final sentiment of ST3 indicates, the experts display interest in having more insight into the reason why the algorithm assigned areas as gray, aligning with the rise in demand for xAI, reflecting a broader desire for transparency and clarity in human-in-the-loop AI systems.
Traditional accuracy and agreement measures are both derived from the confusion matrix offering an overview of the performance of the classification algorithm. Accuracy variation across different datasets of < 1% is considered insignificant for that kind of algorithm (Phan et al., 2023; Rusanen et al., 2023). However, confusion matrix-derived metrics such as accuracy only assess if the algorithm prediction matches the correct output. It does not guarantee that the algorithm captures a key signal pattern related to a specific sleep stage hiding in this 1% accuracy variation. For clinical experts, such as sleep technologists, it is crucial to ensure that key signal patterns are correctly interpreted. If a scoring algorithm with high accuracy and agreement is missing these key patterns, it becomes hard for the sleep technologist to trust the algorithm's prediction. To summarize, there is a need for a metric assessing the scoring algorithm's conformity that also assures sleep technologists' trust in the algorithm. Clinical acumen is a term symbolizing the ability of healthcare professionals to make quick and accurate decisions on complex issues that a clinical AI along with a human-in-the-loop might include in the future to make a diagnosis (Krause et al., 2018). In this work, we would like to introduce a general term to define the act of accepting or agreeing to the use of AI as a decision-making tool by clinical experts: Clinical Acquiescence.
Our research is not without limitations and below we highlight the most notable ones. Although the web platform was architectured with the main purpose of being scalable and robust, this paper does not include an extensive scalability evaluation of the web platform itself. In the current study, this was not the focus, as the platform was tested and evaluated primarily on the improvement it could provide in the task of scoring PSG. Future works could be directed toward stress-testing the platform, evaluating the maximum number of PSG it can handle simultaneously, and determining whether the web platform could sustain heavy traffic loads without considerably slowing down or crashing. Since neither the splitter nor processor queue grew to prohibitively big lengths during testing, we did not see a reason to implement scaling functions, nevertheless, the implementation of the system as a whole lends itself well to dynamic scaling. The gray area threshold of 0.73 was selected with the help of a sleep technologist, and adjusted to produce the least number of gray areas without including blatantly incorrect algorithmic scorings. This study does not evaluate the effect of this threshold on scorer speed or reliability and notes that the threshold value is highly dependent on the algorithm used to produce the scoring. Detailed sensitivity analysis would need to be performed on the threshold value in order to evaluate its performance and create guidelines on how to optimally determine its value. Only global metrics such as the scoring duration and the agreement of the sleep technologists have been considered in this paper. However, this study does not go into detail about the source of the uncertainty in sleep staging between sleep technologists. For instance, it is well known that one primary uncertainty source is the transition between the sleep stages N2 and N3 (Bakker et al., 2023; Jouan et al., 2023).
In the future, a replication of this study needs to be performed, with a greater number of both sleep technologists and a larger subset of PSG to gain a broader perspective of the effects of integrating AI augmentation into the sleep technologist's workflow, along with algorithm trust assessment.
The next step would be to loop the manual review of the gray area with the automatic scoring algorithm. This process is referred to as active learning (Settles, 2009; Ren et al., 2021), and aligns with the AI-integrated human-in-the-loop workflow. A continuous loop would link the reviewed gray area with the scoring AI updating the model and sending a new set of gray areas corresponding to the actual sleep technologist.
Due to the modularity of the platform, it is easy to add more algorithms and augments to the processor, making the adoption of any additional algorithms more approachable without resulting in downtime or causing data loss. For example, the BreathFinder (Holm, 2020) respiratory isolation algorithm is planned for addition to the processor to allow future analysis of individual respiratory cycles. Additionally, adding new destinations and output formats for the PSGs is made easy, e.g. using a micro-scoring platform with integrated machine-learning capabilities, currently under development.
One possible avenue to further advance the platform is to allow researchers to upload their custom automatic scoring algorithms to be vetted and be run autonomously on test data, without ever having to gain physical or digital access to the data, allowing for a reliable method for testing disparate algorithms on the same datasets for greater consistency, reproducibility and transparency in future sleep research.
In this work, we presented a platform that enables PSG collection, integrated with automatic AI scoring algorithms. We evaluated the platform in terms of its effect on sleep technologists' time, and accuracy when scoring PSGs that incorporate AI assistance. In our results, we observed a clear gap in research addressing the integration and evaluation of automatic scoring algorithms for PSG. The proposed platform incorporates AI assistance but still prioritizes the human expert as the ultimate decision-maker. This balance of human expertise and AI presents a promising avenue for future advancements in the field of sleep study and analysis, potentially leading to more refined and accurate diagnostic practices.
All code has been made publicly available and open source via GitHub code repositories. The frontend platform can be accessed via https://github.com/Sleep-Revolution/sleepscorerapi, the splitter service can be accessed via https://github.com/Sleep-Revolution/ESADASplitterService, and finally, the processor can be accessed via https://github.com/Sleep-Revolution/EsadaFileConsumer.
The datasets presented in this article are not readily available because, it contains medical data and other confidential polysomnographic data. Requests to access the datasets should be directed at: c2xlZXBzdXBwb3J0QHJ1Lmlz.
The studies involving humans were approved by National Bioethics committee of Iceland, #21-070. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
BH: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Visualization, Writing—original draft. GJ: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Visualization, Writing—original draft. EH: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Visualization, Writing—original draft. SS: Conceptualization, Data curation, Investigation, Methodology, Resources, Writing—original draft. KH: Data curation, Writing—original draft. CM: Data curation, Writing—review & editing. EA: Conceptualization, Funding acquisition, Methodology, Resources, Supervision, Writing—review & editing. MÓ: Conceptualization, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Writing—original draft. AI: Conceptualization, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Writing—original draft.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. The authors of this paper have received funding to craft this paper from the European Union's Horizon 2020 research and innovation programme (grant agreement 965417) as well as NordForsk (NordSleep project 90458) via Business Finland (5133/31/2018), the Icelandic Research Fund (ESA & ASI). The Sleep Revolution project has received funding from the European Union's Horizon 2020 research and innovation program under grant agreement No. 965417. The sleep technologists who scored the studies—Heidur Grétarsdóttir, Marjo Sunnari, Beate Diecker, Jacob Siegert, Dina Fernandes, Cátia Lígia Rito de Oliveira, Elena Robbi, Paul Murphy, and Alexander Ryan—are especially thanked for there essential contribution to this paper, as well as Kristín Anna Ólasfdóttir, who led the team of scorers.
We express our gratitude to Nox Medical for their essential software support in our research. Their tools and expertise significantly contributed to our work. We appreciate their commitment and support, without which the work described in this paper would have been impossible.
EA reports lecture honoraria from Nox Medical, Philips, ResMed, Jazz Pharmaceuticals, Linde Healthcare, Wink Sleep, Vistor (NovoNordisk), and Apnimed, participation on the Philips Sleep Medicine and Innovation medical advisory board, and has a leadership role as Secretary of the board of the European Sleep Research Society, outside the submitted work.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Alvarez-Estevez, D., and Rijsman, R. M. (2022). Computer-assisted analysis of polysomnographic recordings improves inter-scorer associated agreement and scoring times. PLoS ONE 17:e0275530. doi: 10.1371/journal.pone.0275530
Arnardottir, E. S., Islind, A. S., and Óskarsdóttir, M. (2021). The future of sleep measurements: a review and perspective. Sleep Med. Clin. 16, 447–464. doi: 10.1016/j.jsmc.2021.05.004
Arnardottir, E. S., Islind, A. S., Óskarsdóttir, M., Ólafsdottir, K. A., August, E., Jónasdóttir, L., et al. (2022). The sleep revolution project: the concept and objectives. J. Sleep Res. 31:e13630. doi: 10.1111/jsr.13630
Bakker, J. P., Ross, M., Cerny, A., Vasko, R., Shaw, E., Kuna, S., et al. (2023). Scoring sleep with artificial intelligence enables quantification of sleep stage ambiguity: hypnodensity based on multiple expert scorers and auto-scoring. Sleep 46:zsac154. doi: 10.1093/sleep/zsac154
Benjafield, A. V., Ayas, N. T., Eastwood, P. R., Heinzer, R., Ip, M. S. M., Morrell, M. J., et al. (2019). Estimation of the global prevalence and burden of obstructive sleep apnoea: a literature-based analysis. Lancet Respir. Med. 7, 687–698. doi: 10.1016/S2213-2600(19)30198-5
Biedebach, L., Óskarsdóttir, M., Arnardóttir, E. S., Sigurdardóttir, S., Clausen, M. V., Sigurdardóttir, S. Þ., et al. (2024). Anomaly detection in sleep: detecting mouth breathing in children. Data Min. Knowl. Disc. 38, 976–1005. doi: 10.1007/s10618-023-00985-x
Brennan, H. L., and Kirby, S. D. (2022). Barriers of artificial intelligence implementation in the diagnosis of obstructive sleep apnea. J. Otolaryngol.-Head Neck Surg. 51, 1–9. doi: 10.1186/s40463-022-00566-w
Choo, B. P., Mok, Y., Oh, H. C., Patanaik, A., Kishan, K., Awasthi, A., et al. (2023). Benchmarking performance of an automatic polysomnography scoring system in a population with suspected sleep disorders. Front. Neurol. 14:1123935. doi: 10.3389/fneur.2023.1123935
De Bock, K. W., Coussement, K., De Caigny, A., Slowiński, R., Baesens, B., Boute, R. N., et al. (2023). Explainable AI for operational research: a defining framework, methods, applications, and a research agenda. Eur. J. Oper. Res. doi: 10.1016/j.ejor.2023.09.026
Dikeos, D., and Georgantopoulos, G. (2011). Medical comorbidity of sleep disorders. Curr. Opin. Psychiatry 24, 346–354. doi: 10.1097/YCO.0b013e3283473375
Fleiss, J. L. (1971). Measuring nominal scale agreement among many raters. Psychol. Bull. 76, 378–382. doi: 10.1037/h0031619
Gerla, V., Kremen, V., Macas, M., Dudysova, D., Mladek, A., Sos, P., et al. (2019). Iterative expert-in-the-loop classification of sleep PSG recordings using a hierarchical clustering. J. Neurosci. Methods 317, 61–70. doi: 10.1016/j.jneumeth.2019.01.013
Gerla, V., Kremen, V., Macas, M., Saifutdinova, E., Mladek, A., Lhotska, L., et al. (2018). “Expert-in-the-loop learning for sleep EEG data,” in 2018 IEEE International Conference on Bioinformatics and Biomedicine (BIBM) (Madrid: IEEE), 2590–2596. doi: 10.1109/BIBM.2018.8621557
Giray, G. (2021). A software engineering perspective on engineering machine learning systems: state of the art and challenges. J. Syst. Softw. 180:111031. doi: 10.1016/j.jss.2021.111031
Goldstein, C. A., Berry, R. B., Kent, D. T., Kristo, D. A., Seixas, A. A., Redline, S., et al. (2020). Artificial intelligence in sleep medicine: background and implications for clinicians. J. Clin. Sleep Med. 16, 609–618. doi: 10.5664/jcsm.8388
Grønsund, T., and Aanestad, M. (2020). Augmenting the algorithm: emerging human-in-the-loop work configurations. J. Strateg. Inf. Syst. 29:101614. doi: 10.1016/j.jsis.2020.101614
Holm, B. (2020). BreathFinder. Available online at: https://arxiv.org/pdf/2203.01828
Huttunen, R., Leppänen, T., Duce, B., Arnardottir, E. S., Nikkonen, S., Myllymaa, S., et al. (2022). A comparison of signal combinations for deep learning-based simultaneous sleep staging and respiratory event detection. IEEE Trans. Biomed. Eng. 70, 1704–1714. doi: 10.1109/TBME.2022.3225268
Islind, A. S., and Hult, H. V. (2022). “Balancing overreliance and mistrust in data-driven decision making: a critical view on the role of quantified self in diabetes management,” in 8th International Workshop on Socio-Technical Perspective in IS Development (STPIS 2022), Vol. 329. Available online at: https://ceur-ws (accessed May 3, 2024).
Jang, R. S., Ciliberti, D., Mankin, E. A., and Poe, G. R. (2022). Recurrent hippocampo-neocortical sleep-state divergence in humans. Proc. Natl. Acad. Sci. 119:e2123427119. doi: 10.1073/pnas.2123427119
Jermutus, E., Kneale, D., Thomas, J., and Michie, S. (2022). Influences on user trust in healthcare artificial intelligence: a systematic review. Wellcome Open Res. 7. doi: 10.12688/wellcomeopenres.17550.1
Jouan, G., Arnardottir, E. S., Islind, A. S., and Óskarsdóttir, M. (2023). An algorithmic approach to identification of gray areas: analysis of sleep scoring expert ensemble non agreement areas using a multinomial mixture model. Eur. J. Oper. Res. doi: 10.1016/j.ejor.2023.09.039
Krause, J., Gulshan, V., Rahimy, E., Karth, P., Widner, K., Corrado, G. S., et al. (2018). Grader variability and the importance of reference standards for evaluating machine learning models for diabetic retinopathy. Ophthalmology 125, 1264–1272. doi: 10.1016/j.ophtha.2018.01.034
Lee, D., and Yoon, S. N. (2021). Application of artificial intelligence-based technologies in the healthcare industry: opportunities and challenges. Int. J. Environ. Res. Public Health 18:271. doi: 10.3390/ijerph18010271
Liang, S.-F., Shih, Y.-H., Chen, P.-Y., and Kuo, C.-E. (2019). Development of a human-computer collaborative sleep scoring system for polysomnography recordings. PLoS ONE 14:e0218948. doi: 10.1371/journal.pone.0218948
Loh, H. W., Ooi, C. P., Seoni, S., Barua, P. D., Molinari, F., Acharya, U. R., et al. (2022). Application of explainable artificial intelligence for healthcare: a systematic review of the last decade (2011-2022). Comput. Methods Programs Biomed. 226:107161. doi: 10.1016/j.cmpb.2022.107161
Merkel, D. (2014). Docker: lightweight linux containers for consistent development and deployment. Linux J. 2014:2. doi: 10.5555/2600239.2600241
Mosqueira-Rey, E., Hernández-Pereira, E., Alonso-Ríos, D., Bobes-Bascarán, J., and Fernández-Leal, Á. (2023). Human-in-the-loop machine learning: a state of the art. Artif. Intell. Rev. 56, 3005–3054. doi: 10.1007/s10462-022-10246-w
Nikkonen, S., Somaskandhan, P., Korkalainen, H., Kainulainen, S., Terrill, P. I., Gretarsdottir, H., et al. (2024). Multicentre sleep-stage scoring agreement in the sleep revolution project. J. Sleep Res. 33:e13956. doi: 10.1111/jsr.13956
Oxholm, C., Christensen, A.-M. S., Christiansen, R., Wiil, U. K., and Nielsen, A. S. (2021). Attitudes of patients and health professionals regarding screening algorithms: qualitative study. JMIR Form Res. 5:e17971. doi: 10.2196/17971
Perslev, M., Darkner, S., Kempfner, L., Nikolic, M., Jennum, P. J., Igel, C., et al. (2021). U-sleep: resilient high-frequency sleep staging. NPJ Digit. Med. 4:72. doi: 10.1038/s41746-021-00440-5
Pevernagie, D. A., and Arnardottir, E. S. (2024). Looking for clues in the hypnogram - the human eye and the machine. Sleep. 47:zsae011.doi: 10.1093/sleep/zsae011
Phan, H., Lorenzen, K. P., Heremans, E., Chén, O. Y., Tran, M. C., Koch, P., et al. (2023). L-seqsleepnet: whole-cycle long sequence modelling for automatic sleep staging. IEEE J Biomed Health Inform. 27, 4748–4757. doi: 10.1109/JBHI.2023.3303197
Prasad, S. (2015). “Designing for scalability and trustworthiness in mhealth systems,” in Distributed Computing and Internet Technology. ICDCIT 2015. Lecture Notes in Computer Science, Vol. 8956, eds. R. Natarajan, G. Barua, and M. R. Patra (Cham: Springer), 114–133. doi: 10.1007/978-3-319-14977-6_7
RabbitMQ Contributors (2007). RabbitMQ Documentation. RabbitMQ. Version 3.9.0. Available online at: https://www.rabbitmq.com/
Rayan, A., Szabo, A. B., and Genzel, L. (2023). The pros and cons of using automated sleep scoring in sleep research: comparative analysis of automated sleep scoring in human and rodents: advantages and limitations. Sleep 47:zsad275. doi: 10.1093/sleep/zsad275
Redline, S., Budhiraja, R., Kapur, V., Marcus, C. L., Mateika, J. H., Mehra, R., et al. (2007). The scoring of respiratory events in sleep: reliability and validity. J. Clin. Sleep Med. 03, 169–200. doi: 10.5664/jcsm.26818
Ren, P., Xiao, Y., Chang, X., Huang, P.-Y., Li, Z., Gupta, B. B., et al. (2021). A survey of deep active learning. ACM Comput. Surveys 54, 1–40. doi: 10.1145/3472291
Rosenberg, R. S., and Hout, S. V. (2013). The American academy of sleep medicine inter-scorer reliability program: sleep stage scoring. J. Clin. Sleep Med. 09, 81–87. doi: 10.5664/jcsm.2350
Rusanen, M., Jouan, G., Huttunen, R., Nikkonen, S., Sigurðardóttir, S., Töyrðs, J., et al. (2023). asaga: Automatic sleep analysis with gray areas. Available online at: https://arxiv.org/abs/2310.02032
Settles, B. (2009). Active learning literature survey. Available online at: https://minds.wisconsin.edu/handle/1793/60660
Sle (2021). Revolution of sleep diagnostics and personalized health care based on digital diagnostics and therapeutics with health data integration. Technical report. Available online at: https://cordis.europa.eu/project/id/965417
tiangolo (2023). Fastapi. Available online at: https://fastapi.tiangolo.com/
Troester, M., Quan, S., and Berry, R. B. (2023). The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications, volume Version 3.0. Darien, IL: American Academy of Sleep Medicine.
Keywords: sleep research, platform, human-in-the-loop, machine learning, scoring time, agreement, explainable AI, trust
Citation: Holm B, Jouan G, Hardarson E, Sigurðardottir S, Hoelke K, Murphy C, Arnardóttir ES, Óskarsdóttir M and Islind AS (2024) An optimized framework for processing multicentric polysomnographic data incorporating expert human oversight. Front. Neuroinform. 18:1379932. doi: 10.3389/fninf.2024.1379932
Received: 31 January 2024; Accepted: 29 April 2024;
Published: 13 May 2024.
Edited by:
Michel Le Van Quyen, Institut National de la Santé et de la Recherche Médicale (INSERM), FranceReviewed by:
Vaidotas Marozas, Kaunas University of Technology, LithuaniaCopyright © 2024 Holm, Jouan, Hardarson, Sigurðardottir, Hoelke, Murphy, Arnardóttir, Óskarsdóttir and Islind. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Benedikt Holm, YmVuZWRpa3RodGhAcnUuaXM=; Gabriel Jouan, Z2FicmllbGpAcnUuaXM=
†Co-supervisors
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.