 Jose Luis Salas-Pacheco1,2
Jose Luis Salas-Pacheco1,2 Jose Manuel Arreola-Guerra3
Jose Manuel Arreola-Guerra3 Ricardo Marquez-Velasco4
Ricardo Marquez-Velasco4 Israel Perez-Torres5
Israel Perez-Torres5 Sergio Casarez-Alvarado4
Sergio Casarez-Alvarado4 Giovanny Fuentevilla-Alvarez6
Giovanny Fuentevilla-Alvarez6 Verónica Guarner-Lans6Randall Cruz-Soto7María Elena Soto2,4,7,8*
Verónica Guarner-Lans6Randall Cruz-Soto7María Elena Soto2,4,7,8*- 1Cardiology Department, Centenario Hospital Miguel Hidalgo, Aguascalientes, Mexico
- 2UNAM Master’s and Doctoral Program in Medical, Dental and Health Sciences UNAM, Mexico City, Mexico
- 3Nephrology Department, Centenario Hospital Miguel Hidalgo, Aguascalientes, Mexico
- 4Immunology Department, Instituto Nacional de Cardiología Ignacio Chavez, Mexico City, Mexico
- 5Cardiovascular Biomedicine Department, Instituto Nacional de Cardiología Ignacio Chavez, Mexico City, Mexico
- 6Physiology Department, Instituto Nacional de Cardiología Ignacio Chavez, Mexico City, Mexico
- 7Research Direction, Instituto Nacional de Cardiología Ignacio Chavez, Mexico City, Mexico
- 8Cardiovascular Line Department, Centro Médico ABC Sur, Mexico City, Mexico
Background: Type 4 cardiorenal syndrome (CRS) involves cardiovascular alterations caused by chronic kidney disease (CKD). Fibroblast growth factor-23 (FGF23), carboxy-terminal propeptide of procollagen type I (PIP), and parathyroid hormone (PTH) have been proposed as biomarkers of pathological cardiac remodeling in CKD. In contrast, it has been suggested that MicroRNA 221 has a cardioprotective role. Available evidence shows that, 12 months after kidney transplantation (KT), type 4 CRS reverts in only half of the patients.
Objective: To assess long-term cardiac reverse remodeling after KT and its association with FGF23, PIP, and PTH levels.
Methods: Patients with end-stage renal disease were assessed before and 28 months after KT using FGF23, PIP, and PTH serum concentrations and transthoracic echocardiography.
Results: Fifty-three patients were followed for 28 months after KT. All the patients showed cardiac abnormalities upon inclusion. A follow-up assessment showed a reduction in left ventricle (LV) mass (121 ± 48 vs. 65 ± 14 gr/m2) and left atrial volume (46 vs. 30 ml/m2). The LV ejection fraction (53 vs. 63%), LV global longitudinal strain (-15.9 vs.-19.4%), and LV diastolic function improved. miR-221 expression increased after KT (8.73 RIQ= 3.7-25 vs. 40.16 RIQ= 24-223, p=0.001) and was correlated with the Ee´ratio (r= -0.32, p= 0.02). Multivariate analysis showed that post-KT LV mass was determined by pre-KT LV mass, serum Cr level, post-KT PIP, and hypertension (R2 = 0.65, F=12.1, p=0.001).
Conclusions: Contrary to other evidence, this study demonstrated that type 4 CRS is reversible over the long term. This is a paramount finding because KT normalizes cardiac structure and function independently of the severity of basal cardiac abnormalities.
1 Introduction
Cardiorenal syndrome (CRS) encompasses the interactions between the heart and kidneys, where acute or chronic dysfunction in one organ can induce dysfunction in the other (1, 2).
Type 4 CRS involves cardiovascular alterations caused by chronic kidney disease (CKD). The cardiac phenotype shows alterations induced by pressure and volume overload (3). The main findings are cardiac chamber dilatation, LV hypertrophy, LV diastolic dysfunction that is almost universal, and LV systolic dysfunction, with a prevalence ranging from 16 to 28% (4, 5). Hystologically, Type 4 CRS is characterized by a structural disarray of cardiomyocytes, severe myocyte hypertrophy, and increased cardiac interstitial collagen deposition (6).
The decrease in glomerular filtration rate triggers a surge in toxic substances known as uremic toxins. Fibroblast growth factor 23 (FGF23) is associated with pathological cardiac remodeling and an increased risk of adverse cardiovascular events (7–9). In vitro studies have shown that high levels of FGF23 modify the phenotype of smooth vascular muscle cells (VSMCs) from contractile to synthetic by acting on its specific receptors FGFR1 and Erk1/2. This change was mediated by the downregulation of miR-221/222, which increased the expression of MAP3K2 and PAK1. Moreover, miR-221/222 transfection recovered the contractile phenotype of VSMCs. Additionally, infusion of recombinant FGF23 in rats increased vascular wall thickness and VSMCs showed a synthetic phenotype with reduced miR-221 expression. Ex vivo studies on aortic rings from patients with CKD demonstrated that elevated FGF23 levels increased arterial wall stiffness and were associated with increased pulse wave velocity and reduced plasma levels of miR-221/222 (10).
Some studies have suggested that parathyroid hormone (PTH) can induce LV hypertrophy (11, 12) in a similar manner as FGF23; however, the evidence is contradictory.
MicroRNAs (miRs) are small non-coding RNAs measuring between 20 and 25 nucleotides in length that are involved in the regulation of gene expression. Recently, miR-221 was reported to exhibit cardioprotective and antifibrotic properties. Specifically, it promotes the survival of cardiomyocytes during stress conditions and suppresses excessive collagen production (13–16).
Histological analysis of the heart in patients with CKD shows a high amount of interstitial collagen, which deteriorates the mechanical properties of the heart and promotes the development of heart failure (17). Endomyocardial biopsy is the standard method for measuring interstitial collagen; nevertheless, its implementation in routine clinical practice is not feasible (18). However, the serum concentration of the carboxy-terminal propeptide of procollagen type I (PIP) serves as a reliable and non-invasive proxy for assessing the quantity of interstitial collagen (19–21).
Kidney transplantation (KT) has proven to be highly effective in restoring the uremic environment and relieving hemodynamic overload caused by CKD (Figure 1). However, recent studies have shown that substantial cardiac abnormalities prevail in approximately half of the patients in the short term (22–24). Therefore, this study aimed to evaluate the extent of long-term reverse cardiac remodeling following KT using echocardiography and to explore its relationship with serum levels of FGF23, PIP, PTH, and miR-221.
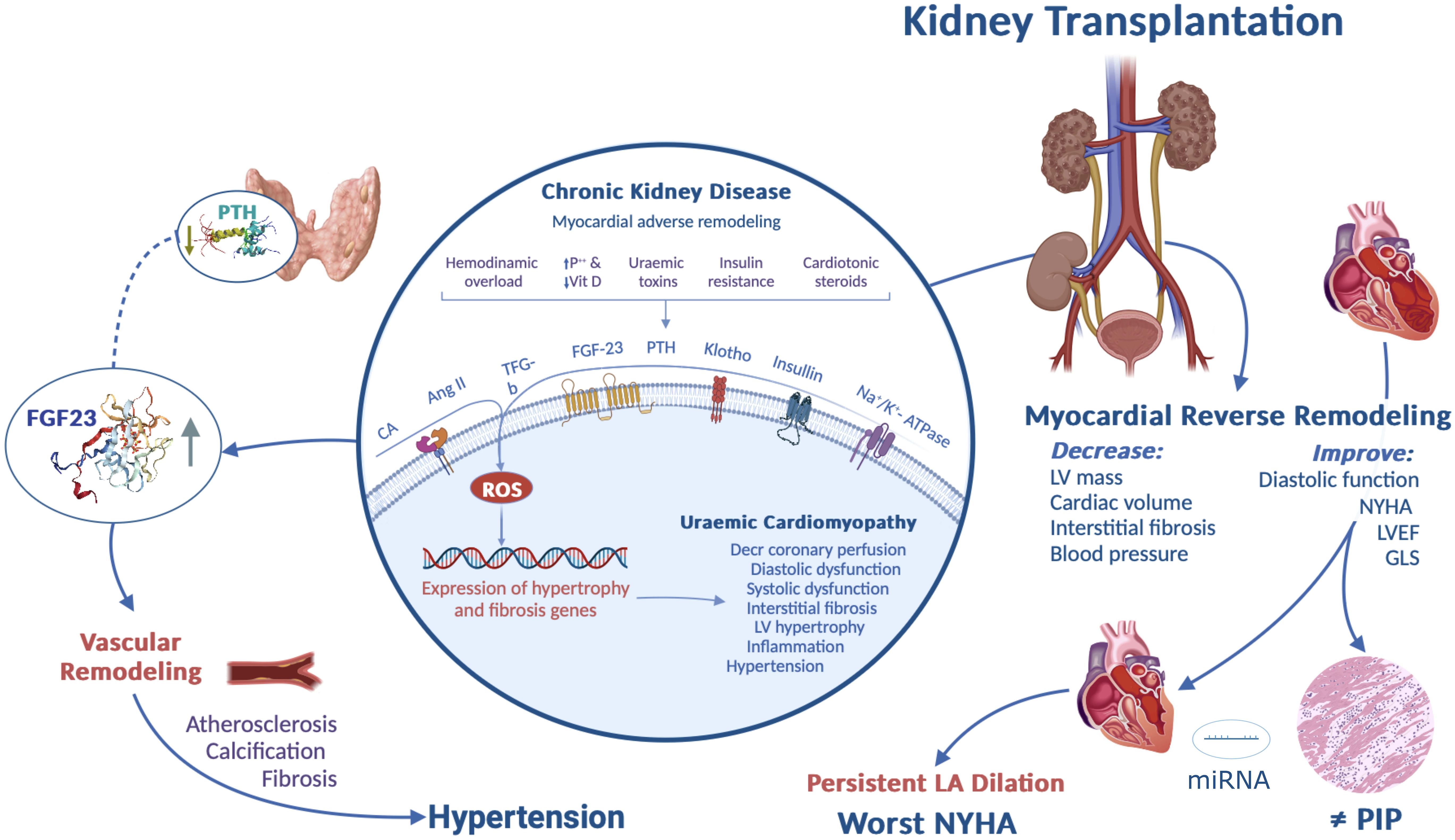
Figure 1. Graphical abstract. Cardiorenal syndrome, which encompasses the complex interplay between cardiac and renal dysfunction, has significant physiological implications in various organs and systems.
2 Materials and methods
2.1 Study population
This dynamic prospective cohort study was conducted between March 2019 and November of 2022, and included both male and female patients aged > 18 years who were diagnosed with CKD at K-DIGO stage V, irrespective of whether they were receiving renal replacement therapy, and who were approved by the institutional transplant committee to receive KT. Patients with diabetes mellitus were not eligible for inclusion. Patients who did not undergo KT after the initial evaluation, those who experienced graft loss, and those lost to follow-up were excluded. On the day preceding the surgical intervention, transthoracic echocardiography, and blood samples were collected. Subsequent to the procedure, telephone follow-up was conducted every six months. At 28 months follow-up, additional transthoracic echocardiography and blood samples were obtained. Blood pressure was measured noninvasively using an aneroid sphygmomanometer (WA7670-10, WA, Inc.), following the World Health Organization technical specifications for non-invasive blood pressure measuring devices with a cuff. Graft function was assessed using serum creatinine (Cr) levels, and creatinine clearance (CrCl) was estimated using the CKDEPI equation.
2.2 Cardiorenal syndrome operational definition
Type 4 CRS was considered present when patients had alterations in LV geometry, LV dilatation, LV hypertrophy, or abnormalities in systolic or diastolic LV function (25).
2.3 Transthoracic echocardiography
Transthoracic echocardiography was performed using a Philips Epiq 7 ultrasound and a 2–5 mHz sectorial transducer following the recommendations of the American Society of Echocardiography (ASE) (26). Left ventricle (LV) mass was calculated using the modified Devereux equation, and chamber volumes were measured using Simpson´s method. The left ventricular ejection fraction (LVEF) was determined using the biplane disc method. Diastolic function was evaluated using pulsed-wave Doppler of transmitral flow, tissue Doppler mitral annulus velocities, left atrial (LA) volume, and tricuspid regurgitation maximum gradient (27). Pulmonary artery systolic pressure (PASP) was determined by adding the right atrial pressure (estimated by the diameter and collapsibility of the inferior vena cava) to the maximum gradient of tricuspid regurgitation. The left ventricular global longitudinal strain (GLS) was obtained from an average of 16 segments using the QLab software (version 13.0) and the LV auto-strain tool (Philips, Andover MA).
2.4 Blood sample collection
Blood samples (12 ml) were collected from each patient by venipuncture. The samples were then centrifuged at 2500rpm for 15 min at 4°C without any additives. The resulting components were then placed in 1.5 ml Eppendorf tubes and stored at -80°C until biomarker quantification and analysis could be performed.
2.5 Blood sample analysis
For the FGF23, PIP, and PTH ELISA tests, the manufacturer’s recommendations were followed. Biological samples of 500 µL were used for each assay. FGF23 levels were quantified using the Human FGF23 monoclonal antibody and R&D Systems reagent (Minneapolis, MN, USA). The kit featured a lower detection limit of 3 pg/ml and detection range of 3-8000 pg/ml. For PIP assessment, a reagent sourced from MyBioSource (San Diego, CA, USA) was used, with a detection range of 25-2000 ng/ml and sensitivity of 5 ng/ml. Serum PTH levels were determined using a reagent from Abbexa (Texas, USA), with a detection range of 3.13-800 pg/ml and a sensitivity of 1.88 pg/ml.
Serum Cr concentration was quantified using standardized dry chemistry (Vitros 4600; Ortho Clinical Diagnostics). Hemoglobin levels were assessed using a hematology analyzer (DxH900 Workcell Solution; Beckman Coulter, Inc.).
2.6 Quantification of miRNA-221-5p
Total RNA was purified from plasma samples using the miRN easy Serum/Plasma Kit (Qiagen) following the manufacturer’s instructions. The pulsed reverse transcription reaction was performed in serum to obtain cDNA of miR-221-5p, using the specific primers for the mature forms, through the TaqMan miRNA RT Kit (TaqMan® Advanced miRNA cDNA, Synthesis Kit, Applied Biosystem, Foster City, CA, USA, Catalog Number A28007). miR-221-5p (hsa-mir-221-5p) was quantified using a commercial system kit (TaqMan gene expression assay) for miRNA using the CFX96 real-time PCR system (Bio-Rad). The expression levels were measured in duplicate and normalized to the endogenous gene miR-16 (hsa-mir-16). Relative quantification was performed using the following formula: 2−ΔΔCt (28).
2.7 Ethical statement
This study was approved by the Institutional Ethics Committee (protocol number CEI/52/CI/32/18) and conducted in accordance with the Declaration of Helsinki. The study protocol followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. Written informed consent was obtained from all patients.
2.8 Statistical analysis
We estimated the sample size with 95% confidence and 80% power, which gave us a sample size of 55 patients, and used the formula for the difference in means. The variable distributions were evaluated using the Kolmogorov-Smirnov test. The association between qualitative variables was assessed using the chi-square test. Differences between groups were identified using Student’s t-test or the Mann-Whitney U test. Correlations were evaluated using Pearson’s or Spearman’s correlation coefficient. Differences between the paired data before and after KT were assessed using the paired t-test or Wilcoxon signed-rank test. Differences between the LA volume categories (normal volume, mild dilation, and moderate dilation) were evaluated using the Kruskal–Wallis test. Predictors of persistent arterial hypertension after KT were assessed using a logistic regression analysis. Multiple regression analysis was used to identify the variables associated with post-KT LV mass. Both multivariable models included predictor variables with a statistical significance of < 0.1 in the bivariate analysis. Differences were considered significant when the p-value was less than 0.05 bilateral. The statistical analysis was conducted using the R software (version 4.2.3) with R Studio interface (version 2023.03.0 + 386).
3 Results
3.1 Pre-transplant
Table 1 presents the demographic characteristics. We included 53 patients, with a mean age of 34 ± 11 years. Sixty-three percent of the patients were male, and CKD etiology was idiopathic in most cases. Six patients did not receive renal replacement therapy (RRT) at admission, and the remaining patients were on hemodialysis three times per week. The median RRT lapse duration was 10 months. Hypertension was present in 75% of the patients, and all were poorly controlled despite a minimum of three antihypertensive drugs. Twenty-three patients were excluded, primarily because they were lost to follow-up.
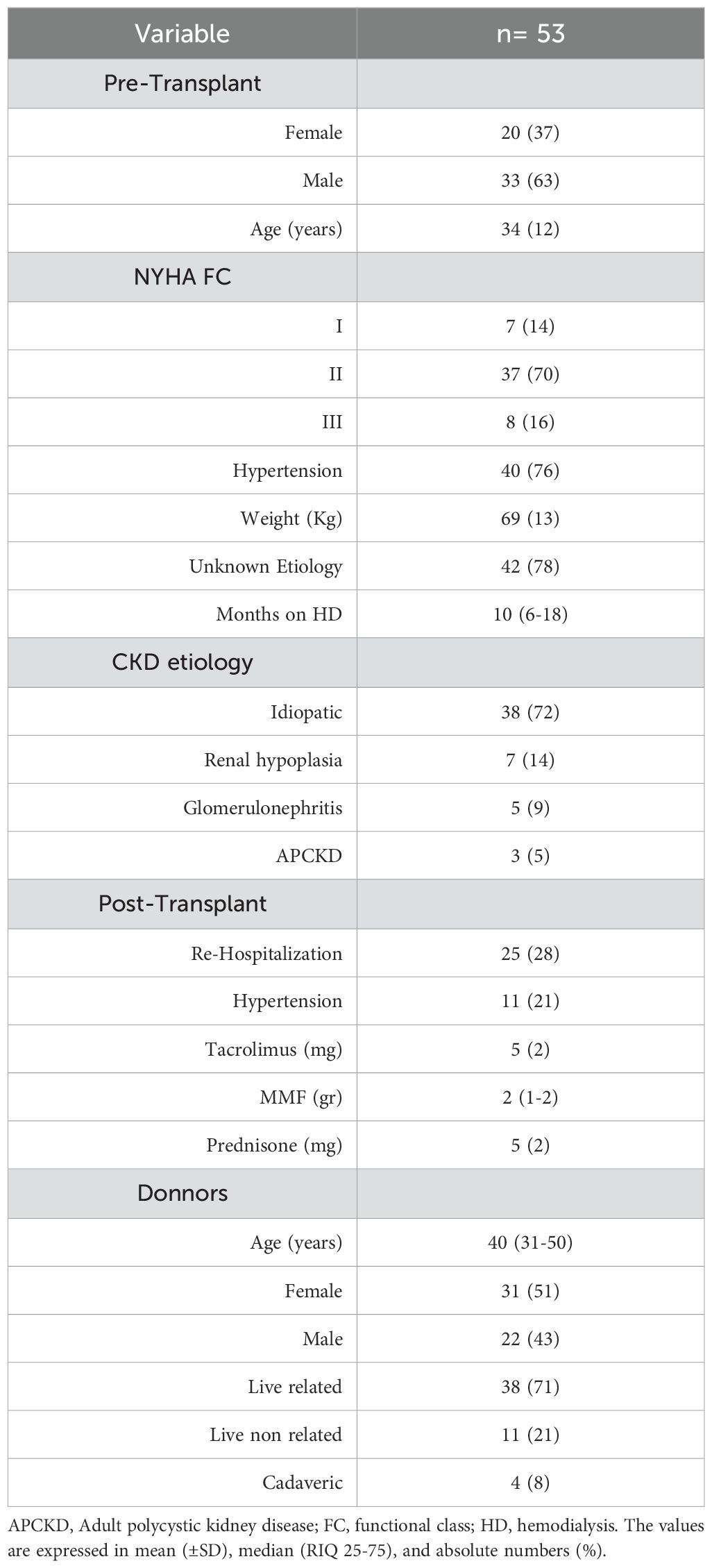
Table 1. General demograhic characteristics.
Initial echocardiographic investigation showed that concentric hypertrophy was the most common pattern of left ventricular (LV) geometry, accounting for 48% of cases. The mean LVEF was 53% ± 11; however, 36% of the patients had a value of < 50%. The majority of patients (62%) had reduced LV GLS, with a mean value of -13.5%. Abnormal LV diastolic function was observed in 81% of the patients, and 34% had evidence of increased LV filling pressure. Left atrial dilatation was present in 80% of patients, with a mean volume of 46 ± 16 mL/m2.
The RRT duration before KT affected cardiac structure and function. The findings revealed that LV mass (r2 = 0.40, p = 0.03), LV volume (r2 = 0.30, p = 0.02), LVEF (r2 = 0.27, p = 0.04), and GLS (r2 = 0.32, p = 0.01) were worse in patients undergoing hemodialysis for longer periods. This was similar to diastolic function, as indicated by the E/e’ ratio (r2 = 0.37, p = 0.006).
All patients had elevated FGF23 and PIP levels (Figure 2). Surprisingly, the PTH levels were lower than expected (42 pg/ml; RIQ: 22-78). Patients with higher FGF23 levels exhibited a higher LV mass (r= 0.4, p= 0.001) and had been receiving RRT for an extended period (r= 0.3, p= 0.04). PTH level was not associated with structural or functional cardiac abnormalities. Examination of the interactions between biomarkers revealed that individuals with normal or inhibited PTH levels had increased FGF23 concentrations (H= 5.9, p= 0.049).
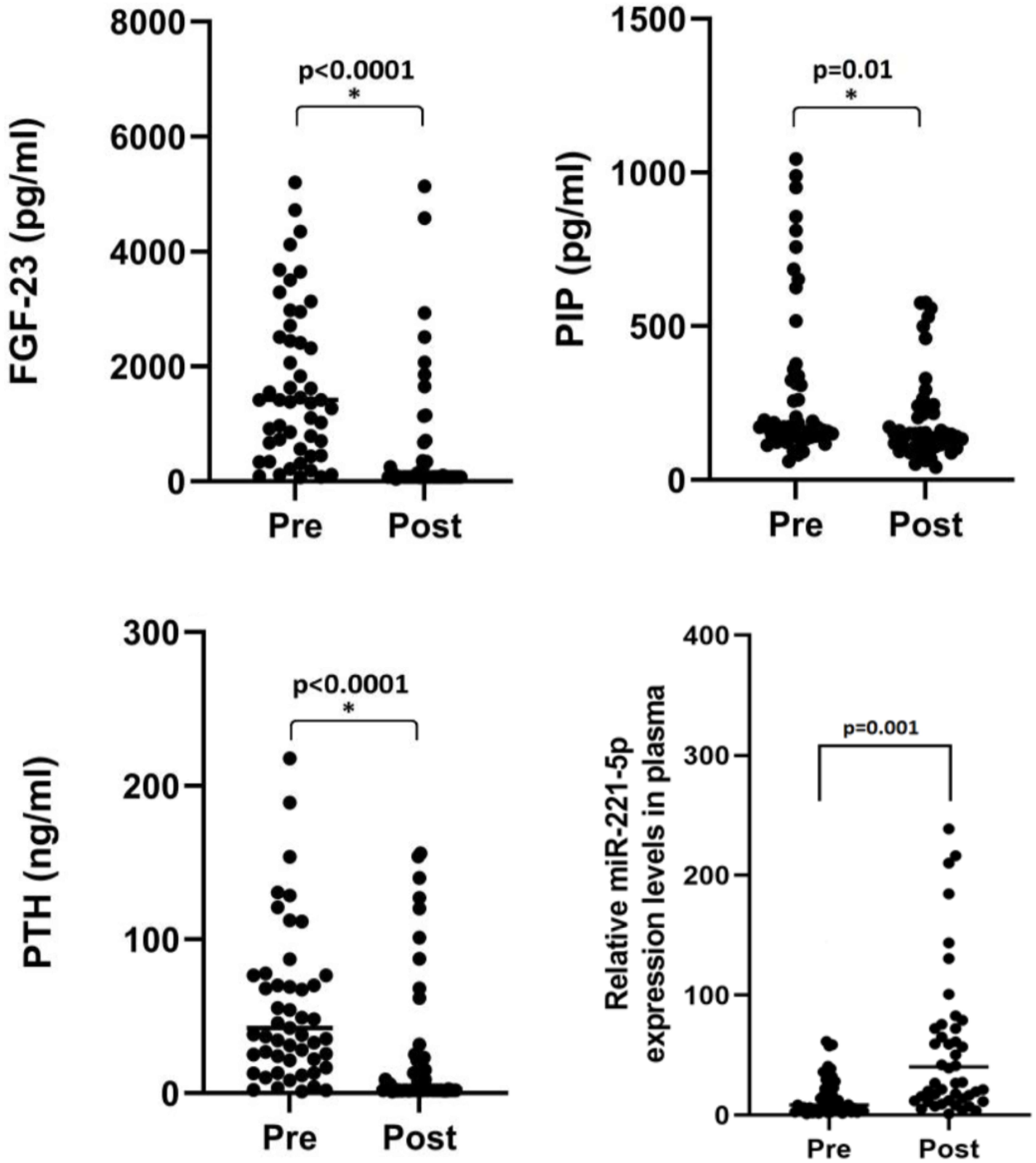
Figure 2. Changes in serum biomarker levels after kidney transplantation.
3.2 Post-transplant
After KT, patients were followed up for an average of 28 ± 6 months. The New York Heart Association (NYHA) functional class scores improved considerably (Table 2). Additionally, at six months, all patients experienced resolution of anemia. One-third (28%) of the patients were hospitalized within the first three months following KT because of urinary tract infection; however, this did not correlate with adverse long-term outcomes.

Table 2. Change in clinical and biochemical variables, and biomarkers after kidney transplantation.
The prevalence of hypertension decreased significantly, and only 20% of patients had hypertension. However, all patients achieved their blood pressure goals using a single drug (46 patients received an angiotensin receptor antagonist, six received a calcium channel blocker, and one received a beta-blocker). The only variable associated with persistent hypertension was the pre-KT FGF23 level (X2 = 12.1, R2 = 0.3, p=0.032). Surprisingly, the duration of RRT did not correlate with post-KT cardiac structure and function or with persistent hypertension.
The long-term graft function demonstrated a mean serum Cr level of 1.22 mg/dL and CrCl of 65 mL/min/1.73 m2. Notably, CrCl was below 60 mL/min/1.73 m2 in 43% of the patients, but it was not less than 30 mL/min/1.73 m2. Among the variables analyzed, only donor age was associated with lower CrCl (r= -0.29, p= 0.03).
According to echocardiographic data, all patients demonstrated a decrease in both the volume of the cardiac chambers and LV mass (Table 3). In terms of LV systolic function, LVEF and GLS increased by 10 and 3 percentage points, respectively. Notably, the LVEF was >50% in all patients. The pre- and post-transplant echocardiographic findings are presented in Table 3 and Figure 3, respectively. Despite a significant decrease in LA volume, six patients showed mild LA dilatation (LA volume index 34-38 ml/m2), and nine patients exhibited moderate LA dilatation (LA volume index 39-48 ml/m2). Individuals with a dilated LA had greater LV mass (r= 0.43, p= 0.001) and worse diastolic function (r= 0.31, p= 0.023). Similarly, Figure 4 shows that patients with NYHA class II had a significantly higher LA volume than those with NYHA class I (35 ± 7 vs. 25 ± 5 ml/m2, t= 6.1, p= 0.001). Despite multiple baseline cardiac alterations, reverse remodeling after KT significantly improved cardiac size and function. Table 4 shows the population according to basal LVEF; it is evident that even in the sickest patients, LV systolic function is normalized after KT.
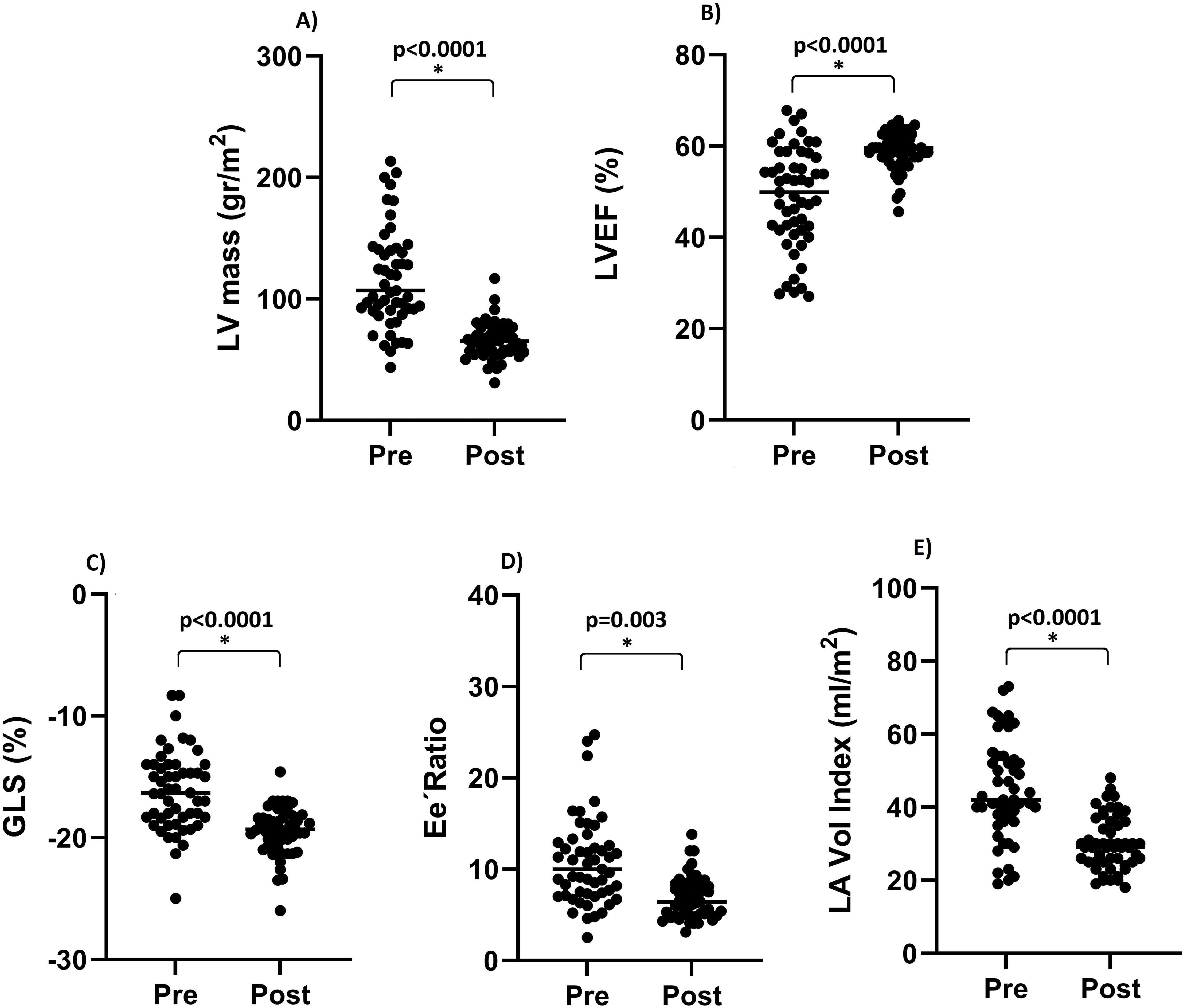
Figure 3. Changes in echocardiographic parameters after kidney transplantation. The figure shows the change in left ventricle mass (A), left ventricle ejection fraction (B), left ventricle global longitudinal strain (C), Ee´ ratio (D), and left atrial volume (E) after kidney trcasplantarion. GLS, global longitudinal strain; LA, left atrial; LV, left ventricle.
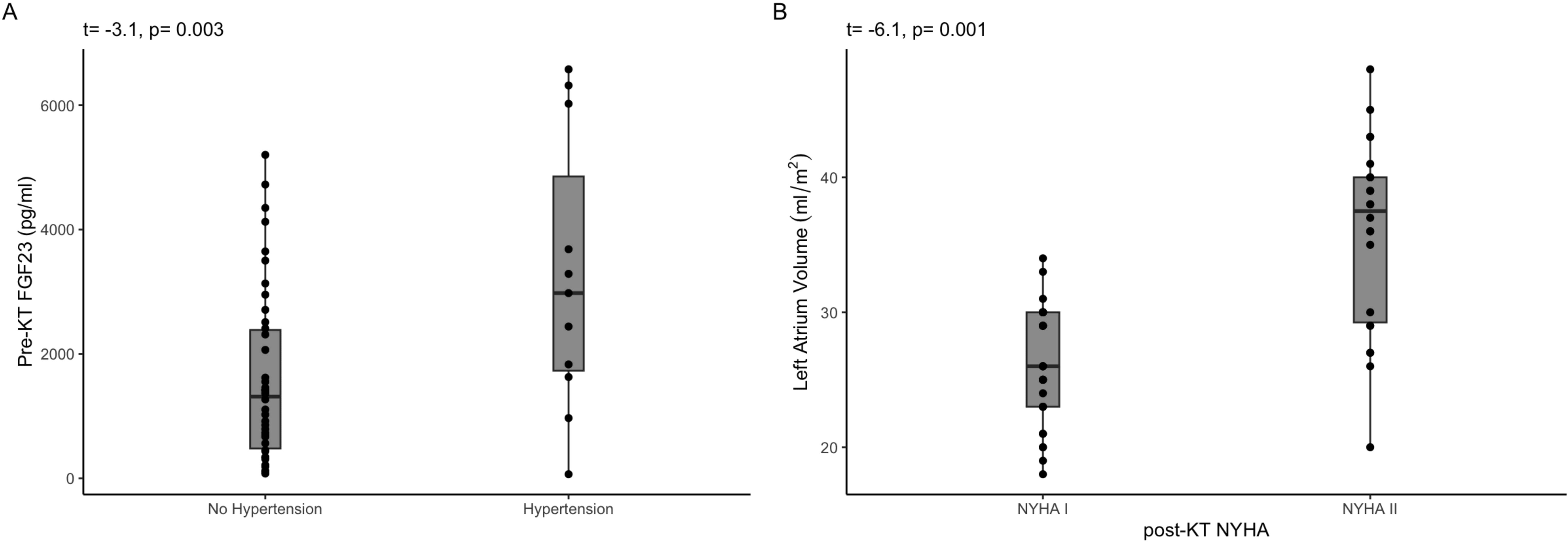
Figure 4. (A) displays the distribution of post-KT FGF23 levels based on the hypertension status. (B) shows that the patients with larger LA volumes had the worst NHYA class.
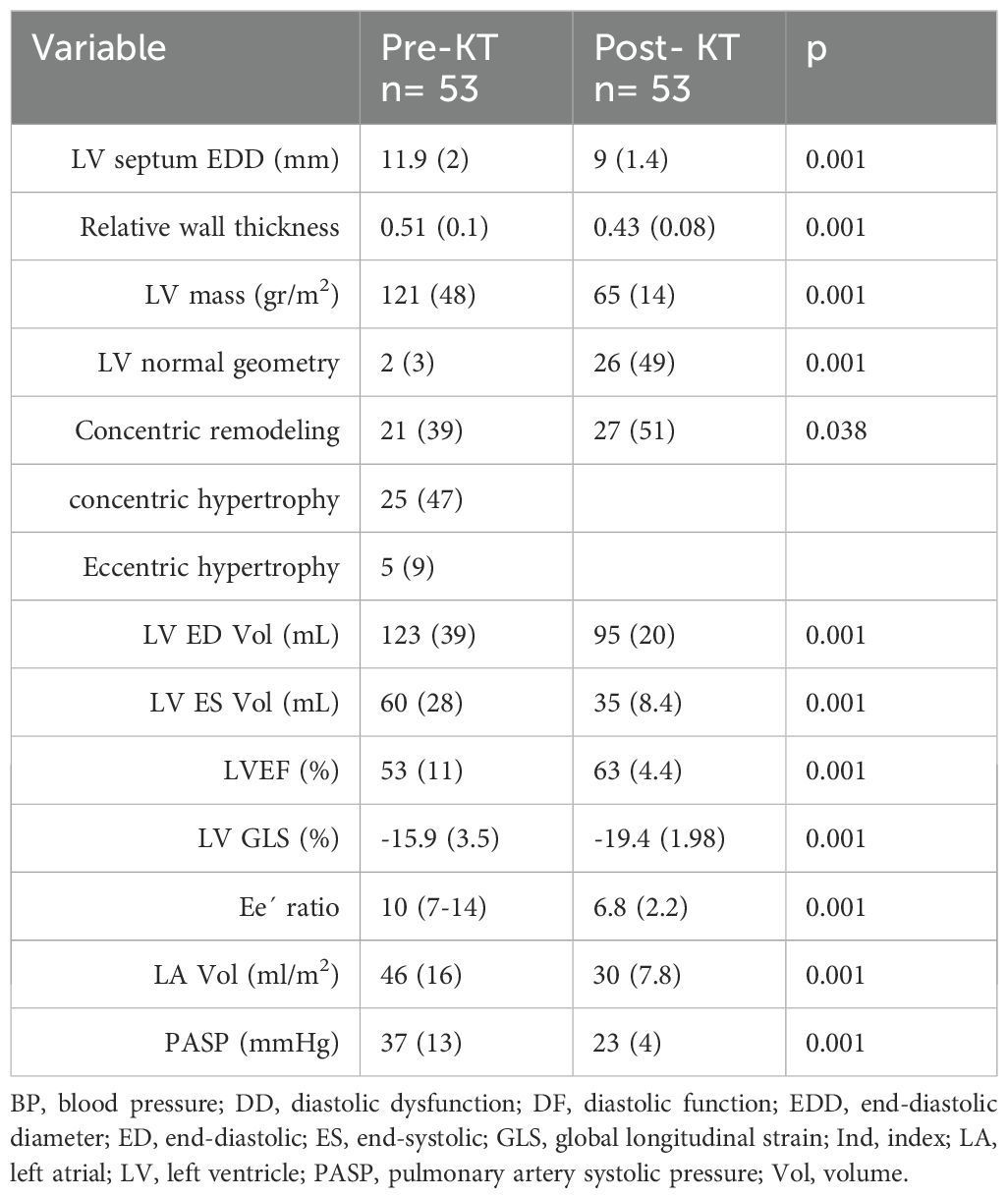
Table 3. Change in echocardiographic parameters after kidney transplantation.
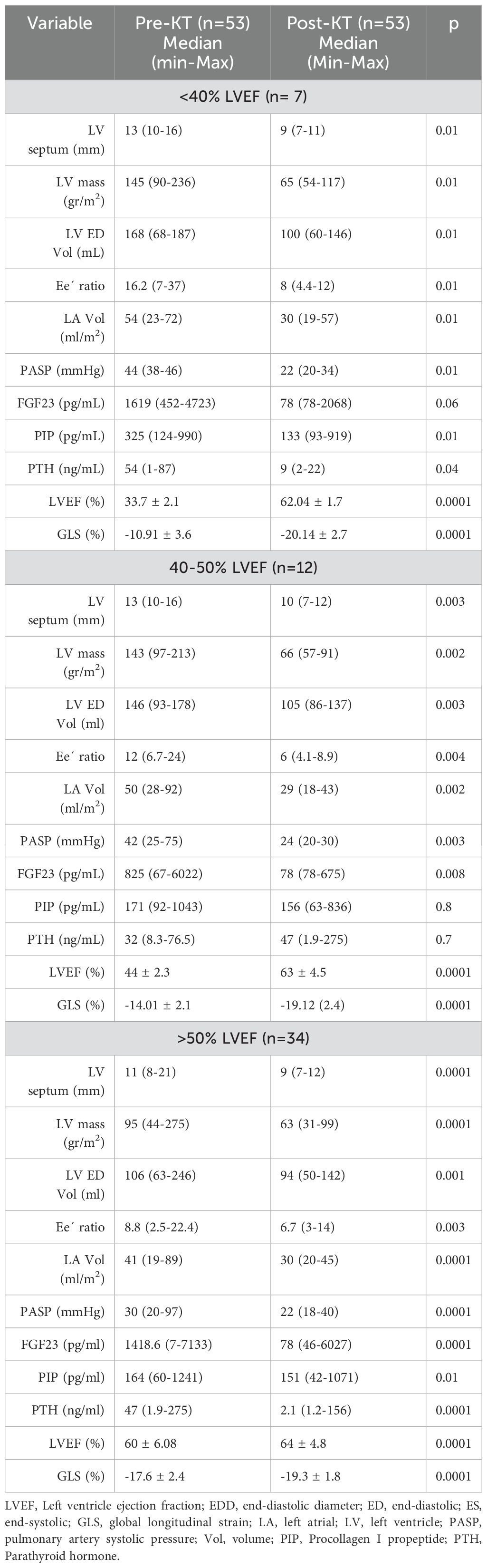
Table 4. Biochemical and echocardiographic characteristics grouped according the basal LVEF and after KT.
Regarding LV mass after KT, multivariable analysis identified pre-KT LV mass (r2 = 0.15, p=0.001), serum Cr (r2 = 16.6, p=0.001), post-KT PIP (r2 =-0.015, p=0.01), and hypertension (r2 = 8.5, p=0.01) as predictor variables. The overall regression was significant (r2 = 0.65, p=0.001).
A significant decrease in the FGF23, PIP, and PTH levels was observed at 28 months (Figure 2). Pre-KT FGF23 levels were associated with persistent hypertension (X2 = 12.1, R2 = 0.3, p=0.032). Post-KT PIP levels were weakly associated with LV mass. The expression of miR-221 was significantly increased after KT (8.73 RIQ= 3.7-25 vs. 40.16 RIQ= 24-223, p=0.001) and was negatively correlated with the Ee´ratio (r= -0.32, p= 0.02), a parameter used for diastolic function assessment.
4 Discussion
The specifics of the pathophysiology associated with type 4 CRS are not yet fully understood, although they are believed to be the result of several interrelated factors such as neurohormonal activation, inflammation, oxidative stress, and impaired endothelial function (29). Individuals with CKD exhibit a heightened risk of cardiac-related death, which is 10–20 times greater than that in matched controls. Thus, CKD patients die prematurely from cardiovascular diseases rather than from renal dysfunction (30). After renal transplantation, mortality of cardiovascular origin remains high; up to 30% of patients die of cardiovascular disease (31).
The patients included in this study were mostly young and without other chronic diseases such as diabetes mellitus. Thus, this population may reflect the behavior of cardiovascular disease after kidney transplantation, isolated from its interaction with other chronic pathologies. That is, it is a model of cardiorenal syndrome, without the post-transplant influence of the main risk factors for major cardiovascular events. According to the results of this study, renal transplantation leads to significant improvements in both structural and functional cardiac anomalies regardless of pre-existing abnormalities. Discrepancies with other studies may reflect the sustained deleterious effects of other comorbidities on the cardiovascular system.
In systemic diseases involving the heart or in primary cardiac diseases characterized by pressure overload, the myocardial interstitium experiences a specific type of cardiac fibrosis called reactive or diffuse fibrosis, which is characterized by the diffuse deposition of cross-linked collagen in interstitial and perivascular areas. In advanced stages, myocytes are surrounded by widespread fibrous tissue, resulting in elevated LV filling pressure, symptoms of heart failure, and poor response to standard treatment (32, 33). Histologically, in CKD, myocytes display structural disarray and severe hypertrophy with a lower proportion of interstitial fibrous tissue than in other cardiac diseases (34). This minor relative amount of fibrous tissue may explain the weak correlation between the PIP levels and LV mass. This observation suggests that the reduction in myocyte size, rather than a decrease in interstitial volume, primarily accounts for the diminution in LV mass. This phenomenon may be the basis for the impressive improvement in LV systolic and diastolic functions after KT.
Previous studies using echocardiography that assessed cardiac reverse remodeling 12 months after KT found that LV hypertrophy and systolic dysfunction persisted in 60% of patients (22–24). Similar results were observed in patients with hypertension and aortic stenosis despite receiving treatment (35, 36). In contrast, Franz et al. observed that in hypertensive patients, after 32 months of optimal blood pressure control, LV mass normalized in >90% of the patients (37). Similar to Franz et al., we observed a significant reduction in LV mass 28 months after KT. This demonstrates that resolution of LV hypertrophy is a long-term phenomenon. Pressure overload is not the only mechanism that triggers LV hypertrophy. The presence of multiple comorbidities, including diabetes, obesity, and obstructive sleep apnea, has been documented to play independent or synergistic roles in the development of LV hypertrophy (38). Long-term follow-up and absence of other comorbidities are critical factors that could contribute to our findings.
Studies have suggested that miR-221 plays an important role in the regulation of cell survival in cardiovascular diseases. Furthermore, decreased miR-221 expression in the myocardium is associated with severe cardiac fibrosis in HF patients. It has been proposed that miR-221 enhances cardiomyocyte survival by inhibiting apoptosis and autophagy through downregulation of total P53 protein expression (39). Preclinical studies have indicated that miR-221 reduces cardiac fibrosis in chronic kidney disease (CKD) by suppressing the expression of thrombospondin 1 and transforming growth factor B1 (40). Myocardial fibrosis is an important pathophysiological process that contributes to diastolic and eventually systolic dysfunction by increasing myocardial stiffness and reducing LV pumping capacity (41). In individuals with end-stage CKD, the levels of circulating total and specific miRNAs are generally lower than those in patients with milder forms of renal impairment or normal renal function (42). In our cohort, the observed increase in miR221 expression after renal transplantation was consistent with the findings of other studies. The Increase in miR221 levels was the only variable associated with improved LV diastolic function. These findings suggest that miR-221 is a potential therapeutic target for CKD-related cardiac fibrosis. Additionally, it may be useful as a biomarker in patients with heart failure and preserved LVEF, in which diastolic dysfunction is one of the main pathophysiological features.
Previous studies have demonstrated a relationship between FGF23 levels and hypertension (43). In this population, we observed that patients with higher pre-KT FGF23 levels were more likely to have post-transplant hypertension. However, the linking mechanisms have not been elucidated. In patients with CKD undergoing hemodialysis, FGF23 promotes peripheral vascular and aortic calcification, in addition to carotid atherosclerosis. Calcification mainly affects the medial layer, which reduces vascular elasticity (44). These vascular phenomena are closely related to hypertension and may contribute to post-KT hypertension.
Finally, it was evident that LA reverse remodeling was of lower magnitude than that observed in the LV. Additionally, patients with persistent LA dilation had worse NYHA scores. One of the main determinants of LA volume is LV diastolic function; however, LV diastolic function was similar between different degrees of LA dilatation. This finding suggests that LA abnormalities are responsible for a lower functional status. The LA plays a crucial hemodynamic role by coupling continuous blood flow from the pulmonary bed to the LV, which has pulsatile dynamics (45). Manifestations associated with LA dysfunction range from mild exercise intolerance to pulmonary hypertension, pulmonary edema, and right-sided heart failure, as observed in stiff LA syndrome (46). The minor reversibility of LA abnormalities after KT may suggest a non-return point for the structural damage induced by CRS.
5 Limitations
Although diabetes is a common etiology of CKD, in our media a small number of patients with diabetic nephropathy underwent KT. Consequently, to reduce the population heterogeneity, we excluded patients with diabetes. Therefore, these results apply only to individuals without diabetes.
6 Conclusions
This study demonstrated that in young patients without diabetes mellitus or other comorbidities, cardiovascular abnormalities due to CKD were almost completely reversed after kidney transplantation. The role played by biomarkers such as FGF23 and PIP helps us to understand the complex pathophysiology of the cardiorenal axis in more detail. The advent of new molecules, such as miR-221, provides essential information from a pathophysiological point of view, in addition to its potential as a biomarker for cardiorenal syndrome and other cardiovascular or renal diseases. The anti-fibrotic effects of miR-221 and its potential therapeutic role in LV diastolic dysfunction warrant further investigation.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Comite de Etica del Centenario Hospital Miguel Hidalgo. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. The study protocol was reviewed and approved by the institute’s ethics committee and was conducted in accordance with the Declaration of Helsinki (approval number CEI52/CI3218).
Author contributions
JS-P: Conceptualization, Data curation, Supervision, Writing – original draft, Writing – review & editing, Formal analysis, Methodology, Project administration, Visualization. JA-G: Conceptualization, Methodology, Writing – review & editing. RM-V: Data curation, Investigation, Writing – review & editing. IP-T: Investigation, Writing – review & editing. SC-A: Investigation, Writing – review & editing. GF-A: Investigation, Software, Visualization, Writing – review & editing. VG-L: Investigation, Validation, Writing – review & editing. RC-S: Investigation, Writing – review & editing. MS: Conceptualization, Formal analysis, Methodology, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
We thank the Master’s and Doctoral Program in Medical, Dental, and Health Sciences UNAM México City for the scholarship to JS-P.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Rangaswami J, Bhalla V, Blair JEA, Chang TI, Costa S, Lentine KL, et al. Cardiorenal syndrome: classification, pathophysiology, diagnosis, and treatment strategies: A scientific statement from the american heart association. Circulation. (2019) 139:e840–78. doi: 10.1161/CIR.0000000000000664
2. Ronco C, Chionh C-Y, Haapio M, Anavekar NS, House A, Bellomo R. The cardiorenal syndrome. Blood Purif. (2009) 27:114–26. doi: 10.1159/000167018
3. Alpert MA. Cardiac performance and morphology in end-stage renal disease. Am J Med Sci. (2003) 325:168–78. doi: 10.1097/00000441-200304000-00003
4. Dyadyk OI, Bagriy AE, Yarovaya NF. Disorders of left ventricular structure and function in chronic uremia: how often, why and what to do with it? Eur J Heart Fail. (1999) 1:327–36. doi: 10.1016/S1388-9842(99)00057-4
5. Fujimoto S, Kagoshima T, Hashimoto T, Nakajima T, Dohi K. Left ventricular diastolic function in patients on maintenance hemodialysis: comparison with hypertensive heart disease and hypertrophic cardiomyopathy. Clin Nephrol. (1994) 42:109–16.
6. Aoki J, Ikari Y, Nakajima H, Mori M, Sugimoto T, Hatori M, et al. Clinical and pathologic characteristics of dilated cardiomyopathy in hemodialysis patients. Kidney Int. (2005) 67:333–40. doi: 10.1111/j.1523-1755.2005.00086.x
7. Faul C, Amaral AP, Oskouei B, Hu M-C, Sloan A, Isakova T, et al. FGF23 induces left ventricular hypertrophy. J Clin Invest. (2011) 121:4393–408. doi: 10.1172/JCI46122
8. Batra J, Buttar RS, Kaur P, Kreimerman J, Melamed ML. FGF-23 and cardiovascular disease: review of literature. Curr Opin Endocrinol Diabetes Obes. (2016) 23:423–9. doi: 10.1097/MED.0000000000000294
9. Scialla JJ, Xie H, Rahman M, Anderson AH, Isakova T, Ojo A, et al. Fibroblast growth factor-23 and cardiovascular events in CKD. J Am Soc Nephrol. (2014) 25:349–60. doi: 10.1681/ASN.2013050465
10. Vergara N, de Mier MVP-R, Rodelo-Haad C, Revilla-González G, Membrives C, Díaz-Tocados JM, et al. The direct effect of fibroblast growth factor 23 on vascular smooth muscle cell phenotype and function. Nephrol Dialysis Transplant. (2023) 38:322–43. doi: 10.1093/ndt/gfac220
11. Saleh F. Parathyroid hormone and left ventricular hypertrophy. Eur Heart J. (2003) 24:2054–60. doi: 10.1016/j.ehj.2003.09.010
12. Schlüter K-D, Piper HM. Cardiovascular actions of parathyroid hormone and parathyroid hormone-related peptide. Cardiovasc Res. (1998) 37:34–41. doi: 10.1016/S0008-6363(97)00194-6
13. Metzinger-Le Meuth V, Fourdinier O, Charnaux N, Massy ZA, Metzinger L. The expanding roles of microRNAs in kidney pathophysiology. Nephrol Dialysis Transplant. (2019) 34:7–15. doi: 10.1093/ndt/gfy140
14. Hu S, Huang M, Nguyen PK, Gong Y, Li Z, Jia F, et al. Novel microRNA prosurvival cocktail for improving engraftment and function of cardiac progenitor cell transplantation. Circulation. (2011) 124. doi: 10.1161/CIRCULATIONAHA.111.017954
15. Zhou Y, Chen Q, Lew KS, Richards AM, Wang P. Discovery of potential therapeutic miRNA targets in cardiac ischemia–reperfusion injury. J Cardiovasc Pharmacol Ther. (2016) 21:296–309. doi: 10.1177/1074248415604463
16. Verjans R, Peters T, Beaumont FJ, van Leeuwen R, van Herwaarden T, Verhesen W, et al. MicroRNA-221/222 family counteracts myocardial fibrosis in pressure overload–induced heart failure. Hypertension. (2018) 71:280–8. doi: 10.1161/HYPERTENSIONAHA.117.10094
17. Schelbert EB, Butler J, Diez J. Why clinicians should care about the cardiac interstitium. JACC Cardiovasc Imaging. (2019) 12:2305–18. doi: 10.1016/j.jcmg.2019.04.025
18. Leone O, Veinot JP, Angelini A, Baandrup UT, Basso C, Berry G, et al. 2011 Consensus statement on endomyocardial biopsy from the Association for European Cardiovascular Pathology and the Society for Cardiovascular Pathology. Cardiovasc Pathol. (2012) 21:245–74. doi: 10.1016/j.carpath.2011.10.001
19. López B, González A, Ravassa S, Beaumont J, Moreno MU, San José G, et al. Circulating biomarkers of myocardial fibrosis. J Am Coll Cardiol. (2015) 65:2449–56. doi: 10.1016/j.jacc.2015.04.026
20. López B, Ravassa S, González A, Zubillaga E, Bonavila C, Bergés M, et al. Myocardial collagen cross-linking is associated with heart failure hospitalization in patients with hypertensive heart failure. J Am Coll Cardiol. (2016) 67:251–60. doi: 10.1016/j.jacc.2015.10.063
21. González A, Schelbert EB, Díez J, Butler J. Myocardial interstitial fibrosis in heart failure. J Am Coll Cardiol. (2018) 71:1696–706. doi: 10.1016/j.jacc.2018.02.021
22. Patel RK, Mark PB, Johnston N, McGregor E, Dargie HJ, Jardine AG. Renal transplantation is not associated with regression of left ventricular hypertrophy. Clin J Am Soc Nephrol. (2008) 3:1807–11. doi: 10.2215/CJN.01400308
23. Ferreira SRC, Moisés VA, Tavares A, Pacheco-Silva A. Cardiovascular effects of successful renal transplantation: a 1-year sequential study of left ventricular morphology and function, and 24-hour blood pressure profile1. Transplantation. (2002) 74:1580–7. doi: 10.1097/00007890-200212150-00016
24. Ślubowska K, Lichodziejewska B, Pruszczyk P, Szmidt J, Durlik M. Left ventricular hypertrophy in renal transplant recipients in the first year after transplantation. Transplant Proc. (2014) 46:2719–23. doi: 10.1016/j.transproceed.2014.08.019
25. Granata A, Clementi A, Virzì GM, Brocca A, de Cal M, Scarfia VR, et al. Cardiorenal syndrome type 4: From chronic kidney disease to cardiovascular impairment. Eur J Intern Med. (2016) 30:1–6. doi: 10.1016/j.ejim.2016.02.019
26. Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the american society of echocardiography and the european association of cardiovascular imaging. J Am Soc Echocardiography. (2015) 28:1–39.e14. doi: 10.1016/j.echo.2014.10.003
27. Nagueh SF, Smiseth OA, Appleton CP, Byrd BF, Dokainish H, Edvardsen T, et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography: an update from the american society of echocardiography and the european association of cardiovascular imaging. J Am Soc Echocardiography. (2016) 29:277–314. doi: 10.1016/j.echo.2016.01.011
28. Livak KJ, Schmittgen TD. Analysis of relative gene expression data using real-time quantitative PCR and the 2–ΔΔCT method. Methods. (2001) 25:402–8. doi: 10.1006/meth.2001.1262
29. Foley RN, Parfrey PS, Sarnak MJ. Epidemiology of cardiovascular disease in chronic renal disease. J Am Soc Nephrol. (1998) 9:S16–23. doi: 10.1053/ajkd.1998.v32.pm9820470
30. Sarnak MJ, Levey AS, Schoolwerth AC, Coresh J, Culleton B, Hamm LL, et al. Kidney disease as a risk factor for development of cardiovascular disease. Hypertension. (2003) 42:1050–65. doi: 10.1161/01.HYP.0000102971.85504.7c
31. Berthoux F, Mariat C. Cardiovascular death after renal transplantation remains the first cause despite significant quantitative and qualitative changes. Transplantation. (2010) 89:806. doi: 10.1097/TP.0b013e3181caeece
32. Jain P, Arava S, Seth S, Lalwani S, Ray R. Histological and morphometric analysis of dilated cardiomyopathy with special reference to collagen IV expression. Indian J Pathol Microbiol. (2017) 60:481. doi: 10.4103/IJPM.IJPM_213_16
33. Balčiūnaitė G, Besusparis J, Palionis D, Žurauskas E, Skorniakov V, Janušauskas V, et al. Exploring myocardial fibrosis in severe aortic stenosis: echo, CMR and histology data from FIB-AS study. Int J Cardiovasc Imaging. (2022) 38:1555–68. doi: 10.1007/s10554-022-02543-w
34. Yoshizawa S, Uto K, Nishikawa T, Hagiwara N, Oda H. Histological features of endomyocardial biopsies in patients undergoing hemodialysis: Comparison with dilated cardiomyopathy and hypertensive heart disease. Cardiovasc Pathol. (2020) 49:107256. doi: 10.1016/j.carpath.2020.107256
35. Devereux RB, Agabiti-Rosei E, Dahlöf B, Gosse P, Hahn RT, Okin PM, et al. Regression of left ventricular hypertrophy as a surrogate end-point for morbid events in hypertension treatment trials. J Hypertens. (1996) 14:S95–S102. doi: 10.1097/00004872-199609002-00018[39
36. Hachiro K, Kinoshita T, Asai T, Suzuki T. Left ventricular mass regression in patients without patient–prosthesis mismatch after aortic valve replacement for aortic stenosis. Gen Thorac Cardiovasc Surg. (2020) 68:227–32. doi: 10.1007/s11748-019-01188-2
37. Franz IW, Tönnesmann U, Müller JF. Time course of complete normalization of left ventricular hypertrophy during long-term antihypertensive therapy with angiotensin converting enzyme inhibitors. Am J Hypertens. (1998) 11:631–9. doi: 10.1016/S0895-7061(98)00024-7
38. Sayin BY, Oto A. Left ventricular hypertrophy: etiology-based therapeutic options. Cardiol Ther. (2022) 11:203–30. doi: 10.1007/s40119-022-00260-y
39. Zhou Y, Richards AM, Wang P. MicroRNA-221 is cardioprotective and antifibrotic in a rat model of myocardial infarction. Mol Ther Nucleic Acids. (2019) :17:185–197. doi: 10.1016/j.omtn.2019.05.018
40. Zhou Y, Ng DYE, Richards AM, Wang P. microRNA-221 inhibits latent TGF-β1 activation through targeting thrombospondin-1 to attenuate kidney failure-induced cardiac fibrosis. Mol Ther Nucleic Acids. (2020) 22:803–14. doi: 10.1016/j.omtn.2020.09.041
41. Weber KT, Brilla CG, Janicki JS. Myocardial fibrosis: functional significance and regulatory factors. Cardiovasc Res. (1993) 27:341–8. doi: 10.1093/cvr/27.3.341
42. Neal CS, . Michael MZ, . Pimlott LK, . Yong TY, Li JYZ, . Gleadle JM. Circulating microRNA expression is reduced in chronic kidney disease. Nephrol Dialysis Transplant. (2011) 26:3794–802. doi: 10.1093/ndt/gfr485
43. Drew DA, Katz R, Kritchevsky S, Ix JH, Shlipak MG, Newman AB, et al. Fibroblast growth factor 23 and blood pressure in older adults. Hypertension. (2020) 76:236–43. doi: 10.1161/HYPERTENSIONAHA.120.14703
44. Jimbo R, Kawakami-Mori F, Mu S, Hirohama D, Majtan B, Shimizu Y, et al. Fibroblast growth factor 23 accelerates phosphate-induced vascular calcification in the absence of Klotho deficiency. Kidney Int. (2014) 85:1103–11. doi: 10.1038/ki.2013.332
45. Pagel PS, Kehl F, Gare M, Hettrick DA, Kersten JR, Warltier DC. Mechanical function of the left atrium. Anesthesiology. (2003) 98:975–94. doi: 10.1097/00000542-200304000-00027
Keywords: cardiorenal syndrome, left ventricle hypertrophy, reverse cardiac remodeling, kidney transplantation, echocardiography, fibroblast growth facctor-23, microRNA
Citation: Salas-Pacheco JL, Arreola-Guerra JM, Marquez-Velasco R, Perez-Torres I, Casarez-Alvarado S, Fuentevilla-Alvarez G, Guarner-Lans V, Cruz-Soto R and Soto ME (2025) Role of kidney transplantation in long-term cardiac reverse remodeling and interconnecting mechanisms in type 4 cardiorenal syndrome. Front. Nephrol. 4:1455036. doi: 10.3389/fneph.2024.1455036
Received: 26 June 2024; Accepted: 15 November 2024;
Published: 06 March 2025.
Edited by:
Todd Pesavento, The Ohio State University, United StatesReviewed by:
Gaetano La Manna, University of Bologna, ItalyMingxing Sui, Second Military Medical University, China
Arksarapuk Jittirat, University Hospitals Cleveland Medical Center, United States
Copyright © 2025 Salas-Pacheco, Arreola-Guerra, Marquez-Velasco, Perez-Torres, Casarez-Alvarado, Fuentevilla-Alvarez, Guarner-Lans, Cruz-Soto and Soto. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: María Elena Soto, ZWxlbmEuc290b0BjYXJkaW9sb2dpYS5vcmcubXg=