 Nikka Khorsandi
Nikka Khorsandi Hwarang Stephen Han
Hwarang Stephen Han Raja Rajalingam
Raja Rajalingam Jun Shoji
Jun Shoji Anatoly Urisman
Anatoly Urisman- 1Department of Pathology, University of California, San Francisco, San Francisco, CA, United States
- 2Department of Medicine, Nephrology Division, University of California, San Francisco, San Francisco, CA, United States
- 3Department of Internal Medicine, Dell Medical School, University of Texas at Austin, Austin, TX, United States
- 4Immunogenetics and Transplantation Laboratory, Department of Surgery, University of California, San Francisco, San Francisco, CA, United States
- 5Department of Medicine, Transplant Nephrology, Cedars-Sinai Medical Center, Los Angeles, CA, United States
Background: Membranous nephropathy (MN) can develop post-kidney transplant and is classified as a recurrent disease in patients with a history of MN in the native kidneys or as de novo disease in patients without such history. The mechanism of recurrent MN is thought to be like that of primary MN, but the mechanism of de novo MN is not well delineated. An association between de novo MN and antibody-mediated rejection (AMR) has been suggested.
Methods: A search of the pathology database from our medical center identified 11 cases of recurrent and 15 cases of de novo MN, in which clinical and histologic findings were compared. No significant differences were identified in the demographic characteristics, serum creatinine and proteinuria trends, or rates of allograft failure between the recurrent and de novo MN groups.
Results: Rates of concurrent AMR were high in both groups (36% and 40%, respectively) but not statistically different from each other. PLA2R immunofluorescence (IF) positivity was seen in 64% of recurrent MN cases compared to 33% of de novo MN cases, suggesting a higher incidence of PLA2R-positive de novo MN than previously reported. No significant histologic differences were identified in the initial biopsies from the two groups, except mean IgG intensity by IF was higher in the recurrent group, suggesting a higher load of immune complex deposits at diagnosis in this group.
Conclusion: The findings do not provide support for a specific association between AMR and de novo MN, but whether there is a possible link between both forms of post-transplant MN and AMR remains an unanswered question.
Highlights
● No significant clinical or histologic differences were identified among 26 recurrent and de novo membranous nephropathy (MN) patients.
● PLA2R positivity was identified in both cases of de novo MN (33%) and recurrent MN (64%).
● Similar rates of concurrent antibody mediated rejection (AMR) were seen in recurrent (36%) and de novo (40%) MN, suggesting a link between AMR and MN.
1 Introduction
Membranous nephropathy (MN) is an immune complex-mediated glomerular disease caused by the deposition of immune complexes along the epithelial surface of glomerular basement membranes (GBM) with associated podocyte injury and progressive GBM thickening and remodeling (1). The resulting damage leads to proteinuria and often progresses to renal failure (2). Immunofluorescence examination of the kidney biopsy tissue shows IgG and C3 granular staining along glomerular capillary walls, while electron microscopy demonstrates corresponding subepithelial electron-dense immune complex deposits, GBM remodeling, and effacement of the podocyte foot processes (Figure 1) (1, 3). MN is classified as either primary or secondary depending on the etiology of the glomerular injury. Primary MN was previously considered an idiopathic disease, but discoveries over the last decade point to an autoimmune response directed at specific podocyte antigens as the underlying mechanism. Autoantibodies directed against phospholipase A2 receptor (PLA2R) are found in 70-80% of primary MN cases (3, 4), and the list of less common target antigens is growing (5). Unlike primary MN, where no disease triggers are known, secondary MN represents approximately 20% of MN cases that develop in the setting of a well-defined association such as infection, drug exposure, malignancy, or systemic autoimmune diseases (e.g. systemic lupus erythematous) (6, 7). Autoantibody target discovery studies have shown that many antigens of primary MN are shared with those of secondary MN, consistent with a hypothesis that both primary and secondary MN have similar underlying autoimmune mechanisms (8, 9).
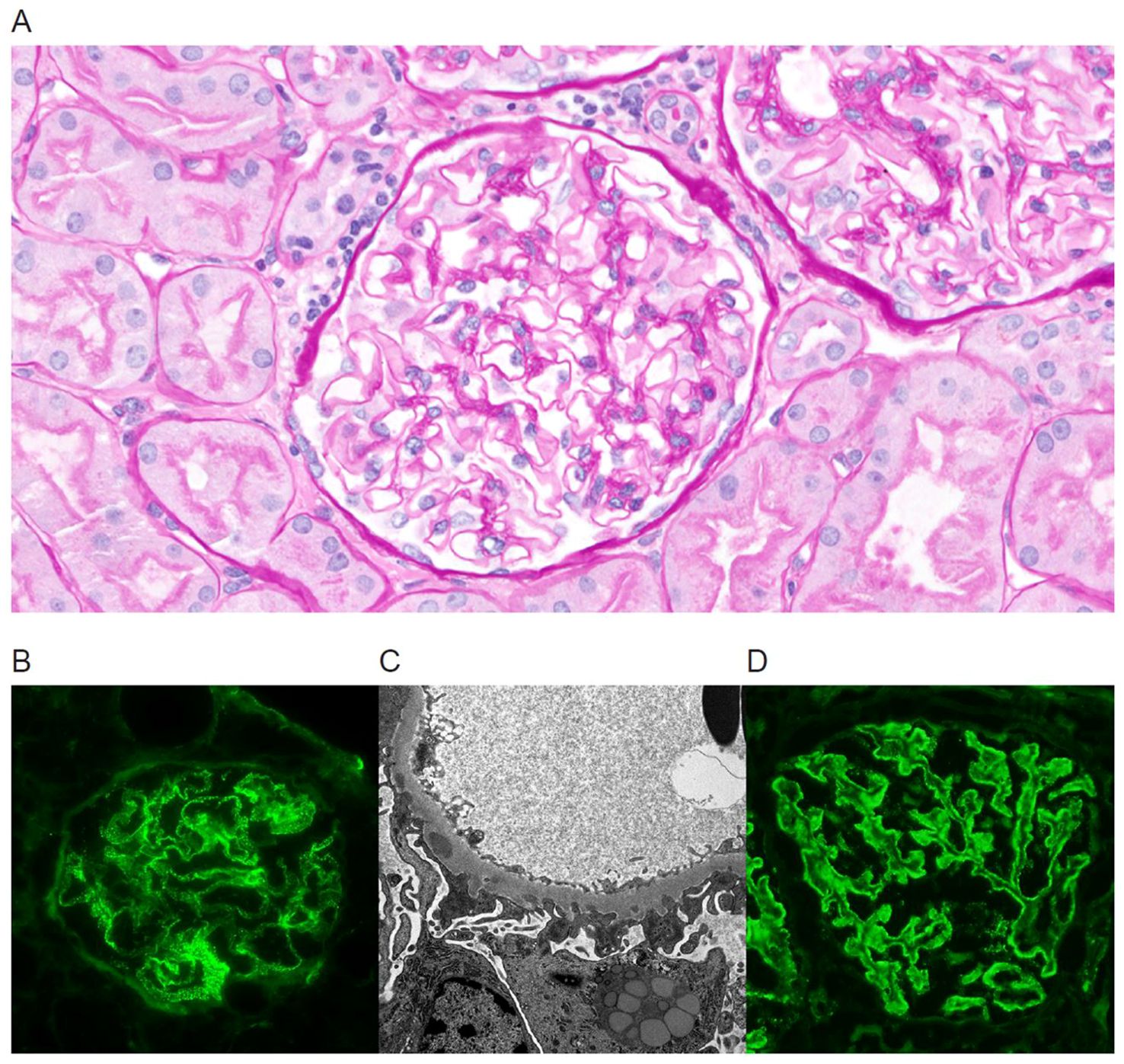
Figure 1. Kidney biopsy findings in a case of PLA2R-positive de novo MN in a 59-year-old patient with a history of ESRD from autosomal dominant polycystic kidney disease and no history of MN in the native kidney, who underwent a biopsy for proteinuria at 12 days post-transplant (A–C). The initial and 6-month follow-up biopsies revealed no PLA2R staining in the glomeruli, but in a 12-month follow-up biopsy PLA2R stain was positive (D). (A) Light microscopy at 12 months shows well-preserved renal parenchyma. The glomeruli have open capillary lumens with subtle thickening of the capillary loop walls. Proximal tubules contain increased cytoplasmic protein reabsorption droplets suggestive of proteinuria. (B) Immunofluorescence stain for IgG demonstrates granular staining along glomerular basement membranes. (C) Electron microscopy reveals scattered subepithelial electron-dense immune complex deposits with associated basement membrane remodeling and prominent podocyte foot process effacement. (D) Immunofluorescence PLA2R stain is positive at 12 months post-transplant.
MN can develop in the allograft kidney after kidney transplant, and it is classified as “de novo” if it occurs in patients without a history of MN in their native kidneys, and “recurrent” if it occurs in patients with a history of MN (10). Recurrent MN has a reported incidence as high as 48% and is associated with increased allograft loss (11–13). In contrast, de novo MN is much rarer, with an incidence of around 2% (14). Recurrent MN is believed to result from the same underlying pathophysiology as primary MN, mediated by the continued presence of circulating autoantibodies after transplant. However, the exact mechanisms by which de novo MN develops are not fully understood, although several risk factors have been proposed, including hepatitis B or C infection and antibody-mediated rejection (7). PLA2R positivity in allograft biopsies of post-transplant MN is strongly associated with recurrent disease, with a reported rate of 83% in recurrent MN compared to only 8% in de novo MN (15).
It has been proposed that the target antigens in de novo MN may be different from those of recurrent MN (16). Specifically, a possible association between de novo MN and antibody-mediated rejection (AMR) has been suggested in several case reports, in which de novo MN biopsy findings coincided with histologic features of AMR and the detection of circulating donor-specific HLA antibodies (16, 17). To better understand the clinical and pathologic differences between de novo and recurrent MN, we retrospectively analyzed cases of biopsy-proven post-transplant MN at a single large renal transplant center.
2 Methods
The study protocol was approved by the University of California San Francisco Institutional Review Board (approval #20-31731). The institution’s clinical pathology database was searched for all renal allograft biopsies diagnosed with post-transplant MN between the years 2014 and 2020. Pathology reports were reviewed to confirm the diagnosis and to extract relevant histologic data including immunofluorescence staining intensity and pathologic features of antibody-mediated rejection.
Electronic medical records of each identified patient were then searched to extract the demographic and clinical data including the etiology of end-stage renal disease (ESRD) in native kidneys, serum creatinine, urine spot protein-to-creatinine ratio, HLA types of recipient and current donor, hepatitis B and C status, CMV status and long-term allograft outcomes. Data on serum anti-PLA2R antibody measurements was only available in three of the de novo cases and two of the recurrent cases and therefore was not included in the analysis.
Patients with post-transplant MN who had a history of MN in the native kidneys were categorized as having “recurrent” disease. Patients with no history of MN and a clear history of ESRD due to a non-MN disease in the native kidneys were categorized as having “de novo” disease. Patients with an unknown cause of ESRD in the native kidneys and patients with systemic lupus erythematosus were excluded from the study. Allograft failure was defined as the return to hemodialysis or re-transplant. One patient died from a cause unrelated to renal function and was censored from outcome analysis, more specifically analysis of allograft failure. In patients with multiple allograft biopsies, the patient’s MN was categorized as PLA2R positive if at least one biopsy demonstrated PLA2R IF positivity. Similarly, a patient was considered to have AMR if at least one biopsy met Banff diagnostic criteria for AMR. In all biopsies, histologic features of rejection and chronicity were recorded prospectively using the established Banff classification system (18, 19).
In patients with multiple biopsies, the first biopsy that established the diagnosis of MN was used as the representative, “diagnostic” biopsy when comparing the pathologic features in biopsies from different patients. The intensity of C4d, C3, and IgG immunofluorescence (IF) stains was recorded using a rating scale of 0-3. Kappa and Lambda IF intensity was classified as either being present or absent with presence defined as a score of at least 1 on the 0-3 scale. IgG subsets measured by IF were available only in two of the de novo cases and three of the recurrent cases and therefore were not included in the analysis.
HLA antibodies were measured in dithiothreitol-treated serum samples using the Luminex-based single antigen bead assay (One Lambda Inc., Canoga Park, CA) (20). Antibody specificity is determined based on known cross-reactivity patterns. The median fluorescence intensity (MFI) is used as an arbitrary unit of antibody quantity. If multiple beads have allelic variants of the same antigen (e.g., HLA-A*02:01, *02:03, *02:06—variants of HLA-A2 antigen), then the average MFI of all positive beads is used to quantify HLA-A2 antibody strength. LABXpress Pipettor (One Lambda), a high throughput liquid handling system to aspirate and dispense precise volumes into test wells of a 96-well reaction plate is used to minimize interassay variations. The donor-specific antibodies (DSA) were assessed by comparing them against the current donor’s HLA types. The DSAs and their MFI values were assessed in all sera samples collected at the time of any available pre-transplant points to either the point of allograft failure or to the most recent follow-up date available. Only DSA against the patient’s current transplant were included in the analysis. The DSA were classified as preformed (those detected prior to transplant) and de novo (those detected after the current transplant). De novo DSA (dnDSA) were further divided into those that were first detected prior to MN diagnosis or concurrent with the diagnosis. The MFI of each dnDSA was charted over time relative to the patient’s MN diagnosis. Concurrent urine spot protein to creatinine ratios (UPCR) were reviewed and co-plotted along MFI to evaluate for possible correlation between dnDSA levels and proteinuria levels.
Statistical analyses were conducted with R Statistical Software (v4.1.2; R Core Team 2021). Evaluation of differences between the de novo and recurrent groups was performed using Pearson’s chi-square tests or student’s unpaired t-test, when relevant. Prior to each t-test, a test to evaluate variance was performed and appropriately applied. Significance was defined as a probability of less than 0.05.
3 Results
Fifty-two biopsies with post-transplant MN were initially identified from 31 patients. After reviewing the electronic medical records, the etiology of ESRD was unclear in 5 patients, who were excluded from further analysis. Among the remaining 26 patients, 11 were classified as having recurrent MN and 15 as having de novo MN. The diagnosis of post-transplant MN was confirmed by electron microscopy in the representative biopsy for 19 patients, including 10 of 15 cases of de novo MN and 9 of 11 cases of recurrent MN. In the recurrent MN group, 3 biopsies were performed for an elevated creatinine level, 5 for proteinuria, 1 for both an elevated creatinine level and proteinuria, and 2 for routine surveillance. In the de novo MN group, 5 biopsies were performed for an elevated creatinine level, 4 for proteinuria, and 6 for routine surveillance.
We first compared the demographic and clinical variables of patients with recurrent and de novo MN and identified no significant differences between the two groups (Table 1). The average age of the patients in the recurrent MN group at the time of diagnostic biopsy was 51.7 years compared to 44.0 years in the de novo MN group. On average, a diagnosis of MN was made in the recurrent MN group 50.0 months after transplant as compared to 32.8 months in the de novo MN group. Four of eleven patients (36%) in the recurrent MN group were female, while seven of the fifteen patients (47%) in the de novo MN group were female. The most common race/ethnicity in both the recurrent and de novo MN cohorts were white, non-Hispanic or Latino patients. None of the patients in the recurrent MN group had a history of Hepatitis B or C positivity, whereas two of the fifteen patients in the de novo MN group had a history of Hepatitis B or C. The rates of concurrent AMR were similar between the recurrent group (36%) and the de novo group (40%). The average urine protein to creatinine ratio in the recurrent MN cohort was 2.43 g/g as compared to 1.48 g/g in the de novo MN cohort, but this difference was not statistically significant. Serum creatinine levels at the time of MN diagnosis were comparable between the groups, with an average of 1.88 mg/dL in the recurrent MN group and 1.40 mg/dL in the de novo MN group. Likewise, the rates of allograft failure were also similar, with a failure rate of 55% in the recurrent MN group and 53% in the de novo MN group.
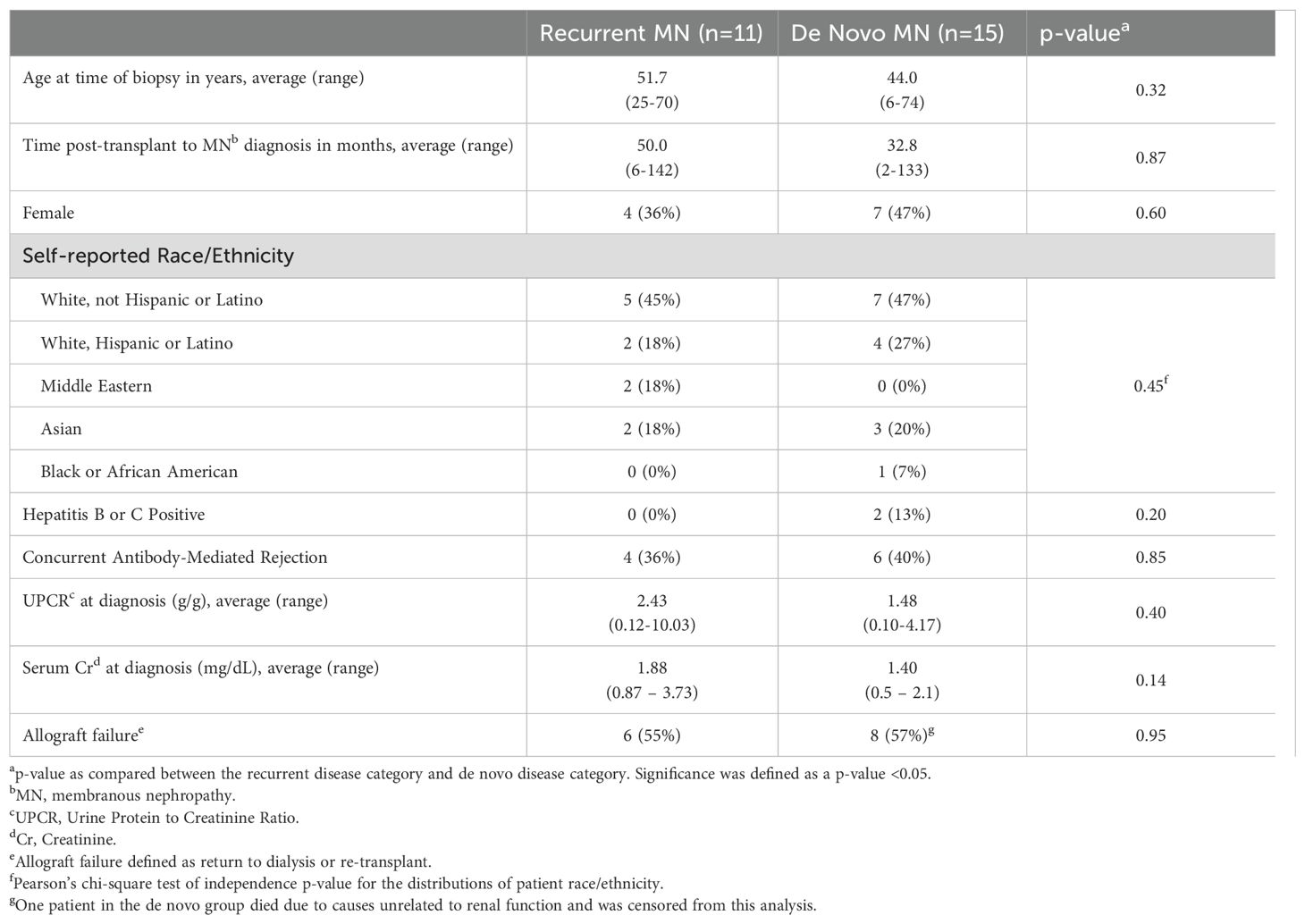
Table 1. Patient demographics and clinical features.
Next, we compared the biopsy findings in the recurrent and de novo MN groups (Table 2). Positive PLA2R staining by IF was seen more frequently in recurrent MN (64%) compared to de novo MN (33%), but this difference was not statistically significant. Somewhat unexpectedly, the mean IgG intensity observed by IF in glomerular capillary loop immune complex deposits was significantly higher in the recurrent group (2.7+ on average) compared to the de novo group (1.7+ on average; p-value of 0.002; Table 2). No significant differences were observed in IF intensities of C4d or C3 stains. Kappa and lambda IF stain results were available in 5 of 11 cases of recurrent MN and 8 of 15 cases of de novo MN, and none of the cases revealed convincing evidence of light chain restriction. Markers of chronicity, including the number of globally sclerotic glomeruli, and the extent of interstitial fibrosis (Banff ci score) and tubular atrophy (ct), were not significantly different between the two groups (Table 2). Similarly, we found no significant differences in Banff histologic markers of rejection, including glomerulitis (g), tubulitis (t), peritubular capillaritis (ptc), or intimal arteritis (v) in the recurrent MN and the de novo MN cohorts.
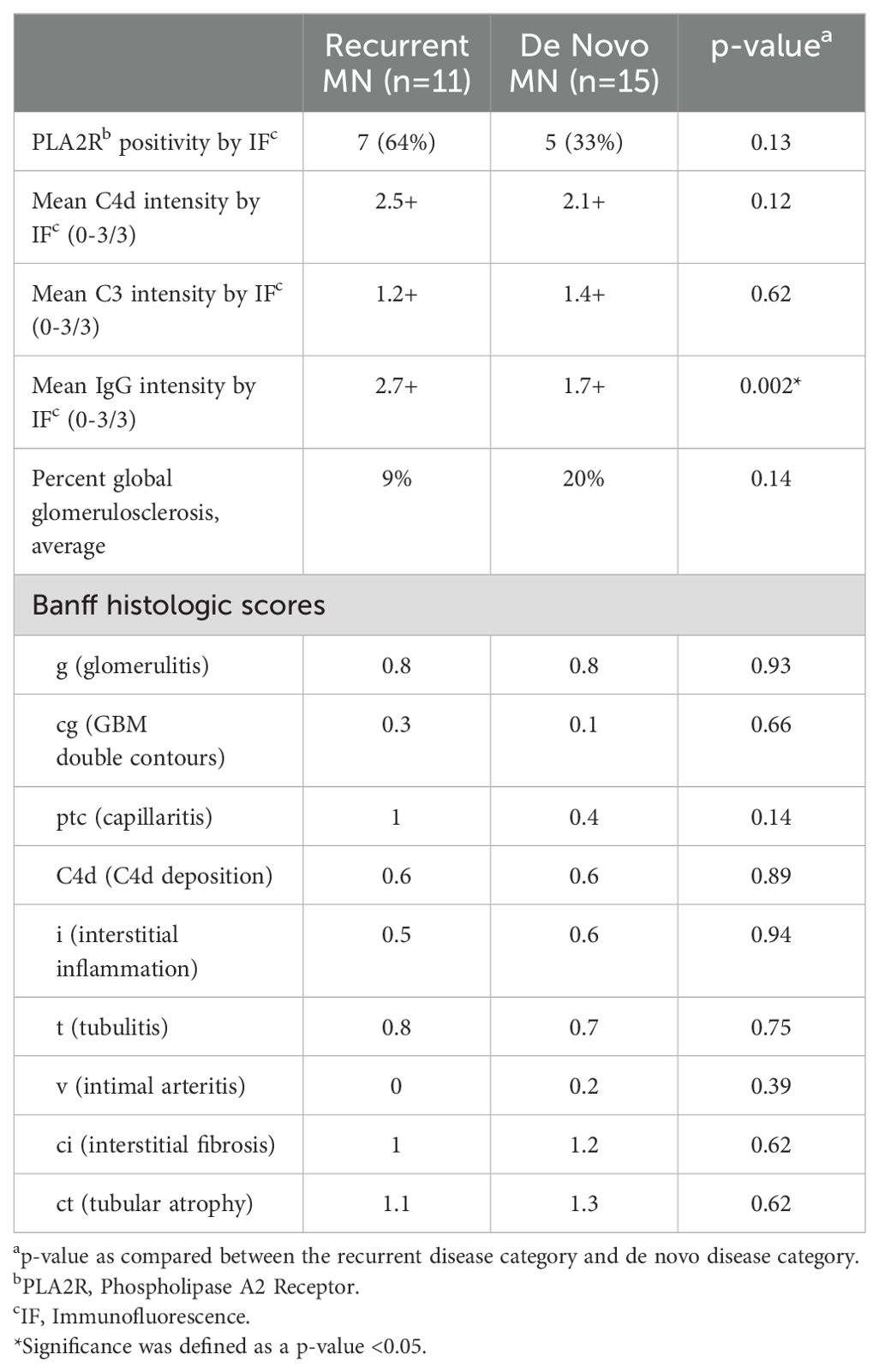
Table 2. Biopsy features.
We further focused on the 10 identified patients with post-transplant MN who also had AMR (Table 3), including 6 patients with recurrent and 4 patients with de novo MN. While the number of patients in the two groups was too small for robust statistical comparisons, we did not observe obvious differences between recurrent and de novo cases with AMR. Similar to the entire cohort of post-transplant MN (Table 1), the subset with AMR showed a similar average time to MN diagnosis in the recurrent and de novo groups. None of the patients displayed preformed DSA (those detected prior to transplant). In both groups, at least half of the patients developed dnDSA concurrent with MN diagnosis (75% in recurrent MN vs 50% in de novo MN), while the rest showed the emergence of dnDSA that preceded MN diagnosis (by 4 to 11 months in three de novo MN patients and by 15 months in a single recurrent MN patient). Furthermore, no statistically significant differences were observed in the frequency of single vs multiple DSA seropositivity, PLA2R stain positivity, or rates of allograft failure between recurrent and de novo MN subgroups with AMR (Table 3). Similarly, a time series analysis of DSA titers and proteinuria levels relative to the time at which MN was diagnosed did not show a uniform correlation between the two or convincing differences between the recurrent and de novo MN subgroups (Figures 2, 3).
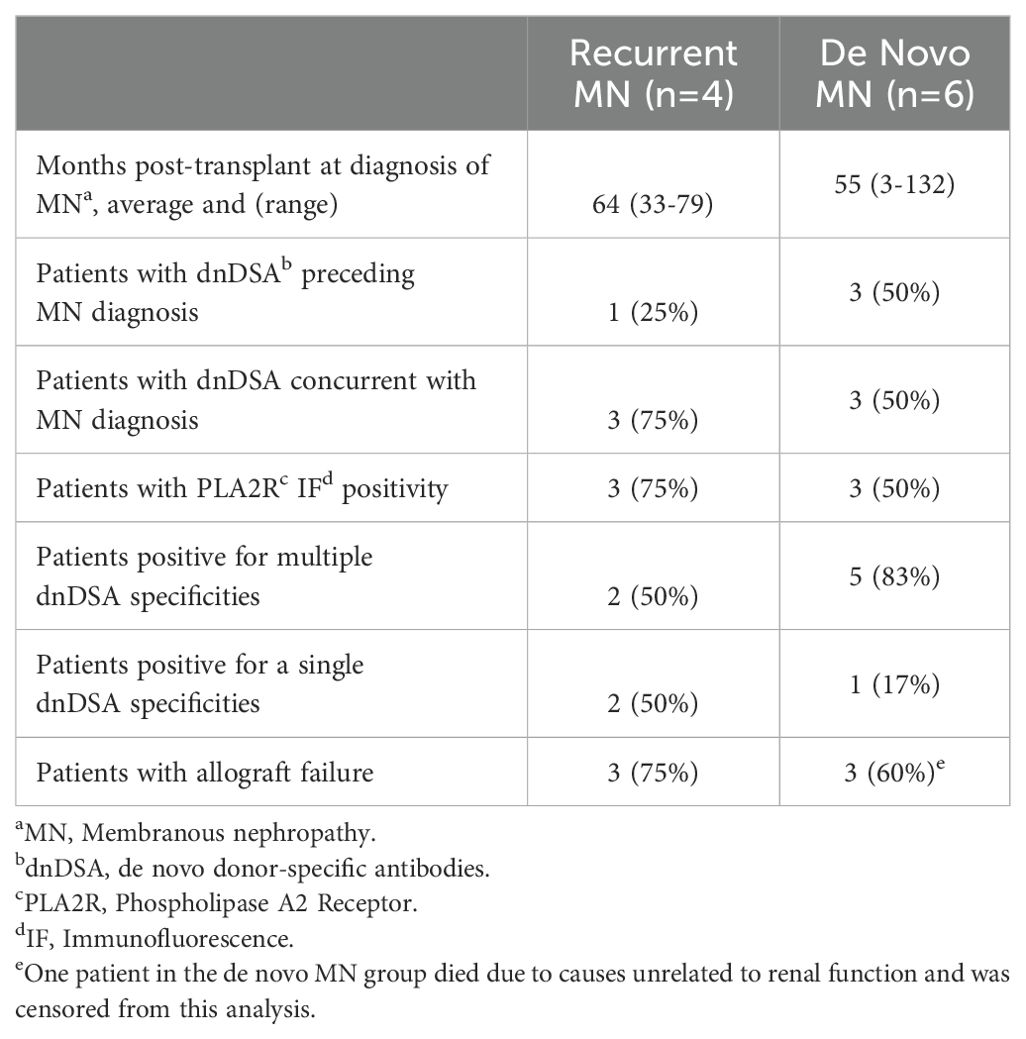
Table 3. Patients with post-transplant MN and AMR.

Figure 2. dnDSA titers and proteinuria levels in cases of recurrent MN with concurrent antibody mediated rejection. Four patients with recurrent MN and concurrent AMR were identified. The mean fluorescence index (MFI) of each dnDSA is recorded over time in months relative to MN diagnosis (time point 0). MFI trends of all detected HLA class I and II antibody specificities are shown (left y-axis); the most persistent dnDSA are presented as red lines, the second most persistent dnDSA are presented as orange lines (when present), and any other dnDSA are presented with lines of other colors (when present). Concurrent spot urine protein-to-creatinine ratios (UPCR) trends are shown as blue lines (right y-axis).
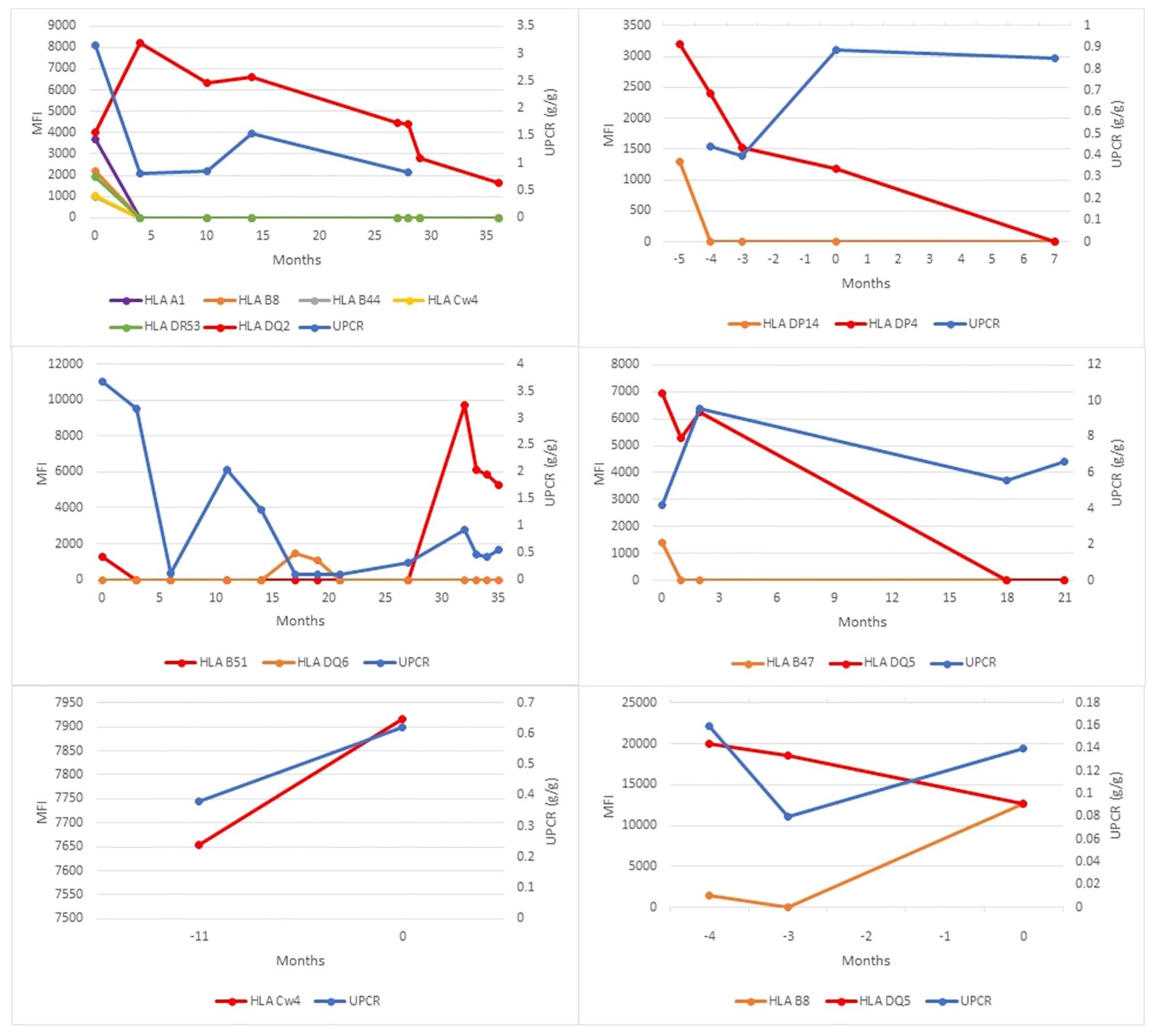
Figure 3. dnDSA titers and proteinuria levels in cases of de novo membranous nephropathy with concurrent antibody mediated rejection. Six patients with de novo MN and concurrent AMR were identified. The mean fluorescence index (MFI) of each dnDSA is recorded over time in months relative to MN diagnosis (time point 0). MFI trends of all detected HLA class I and II antibody specificities are shown (left y-axis); the most persistent dnDSA are presented as red lines, the second most persistent dnDSA are presented as orange lines (when present), and any other dnDSA are presented with lines of other colors (when present). Concurrent spot urine protein-to-creatinine ratios (UPCR) trends are shown as blue lines (right y-axis).
4 Discussion
This case series of post-transplant MN from a single institution is among the largest reported to date (15, 17, 21). Comparison of clinical and biopsy findings in 11 cases of recurrent MN and 15 cases of de novo MN did not reveal significant differences in demographic characteristics, time interval after transplant to the diagnosis of MN, laboratory values of renal function and proteinuria, frequency of concurrent AMR, or rates of allograft failure. Aside from a higher average IgG intensity of immune complex deposits observed by IF in recurrent MN compared to de novo MN (2.7+ vs 1.7+, p=0.002), no other significant histologic differences were identified in the biopsies at the time of MN diagnosis. The observed apparent difference in IgG intensity is unlikely to be a useful marker at the level of individual biopsies, but the apparent difference overall may indicate a trend for larger and/or more frequent immune complex deposits in recurrent MN as compared to de novo MN at the time of diagnosis. Of note, no apparent corresponding difference was observed in C3 intensity, which has been proposed as a possible marker of disease activity in lupus MN (22).
Similar to prior reports, we observed a higher proportion of PLA2R-positive cases in recurrent MN (64%) compared to de novo MN (33%), but the difference between the two groups was not statistically significant. Our results suggest a higher incidence of PLA2R-positivity in de novo MN than previously reported (6-8%) (15, 21) and question a prior proposals that PLA2R staining is highly specific for recurrent disease (15). In our cohort, the estimated sensitivity and specificity of PLA2R stain for recurrent MN are 64% and 71%, respectively. These findings are further supported by other reports highlighting PLA2R-positive cases in de novo MN (16, 23). We note that this apparent discrepancy may be explained, at least in part, by the less stringent definition of PLA2R positivity used in this study. We did not require a PLA2R-positive stain during the initial biopsy diagnostic of MN and accepted a positive stain in any subsequent follow-up biopsy when available (Figure 1).
We further focused on the question of a possible link between de novo MN and AMR. In addition to the similar rates of concurrent AMR seen in the recurrent MN (36%) and de novo MN (40%), the subset of cases with AMR did not reveal significant differences in rates of PLA2R positivity, Banff histologic markers of AMR (g, ptc, C4d), the timing of dnDSA emergence relative to MN diagnosis, positivity for single or multiple dnDSA specificities, or rates of allograft failure. Furthermore, no consistent correlation was seen between proteinuria levels and dnDSA titers in either recurrent or de novo MN cases. These results do not provide support for an association between AMR and de novo MN. However, the observed rates of AMR in both recurrent and de novo MN subgroups observed in this study (36-40%) are higher than that seen in allograft biopsies in general (1-21%) as previously reported (24). Therefore, the possibility that there may be a mechanistic link between MN and AMR, independent of PLA2R status or whether MN is recurrent or de novo, remains an open question. This possibility is particularly intriguing in light of the emerging view that MN is an autoimmune disease driven by autoantibodies to various cellular antigens (3–5), which has a compelling mechanistic overlap with the pathophysiology of AMR mediated by DSA that target HLA and non-HLA antigens.
In our series, allograft failure rates were similarly high in recurrent MN (55%) and de novo MN (57%). However, we did not find evidence of worse allograft survival in de novo MN compared to recurrent MN reported in a prior large multicenter study of post-transplant MN (21). Importantly, MN cases with concurrent AMR had even higher rates of allograft failure (75% in recurrent MN and 60% in de novo MN). However, none of the differences were statistically significant due to the limited number of cases in each subgroup. Despite this limitation, our findings highlight the importance of DSA monitoring in cases of post-transplant MN for possible early detection of concurrent AMR.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by University of California San Francisco Institutional Review Board. The studies were conducted in accordance with the local legislation and institutional requirements. The human samples used in this study were acquired from a byproduct of routine care or industry. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
NK: Writing – original draft, Writing – review & editing. HH: Writing – original draft, Writing – review & editing. RR: Writing – review & editing, Writing – original draft. JS: Writing – original draft, Writing – review & editing. AU: Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
MN, membranous nephropathy; AMR, antibody-mediated rejection; IF, immunofluorescence; GBM, glomerular basement membranes; PLA2R, phospholipase A2 receptor; ESRD, end-stage renal disease; MFI, median fluorescence intensity; DSA, donor-specific antibodies; dnDSA, de novo DSA; UPCR, urine spot protein to creatinine ratios; ci, interstitial fibrosis; ct, tubular atrophy; g, glomerulitis; t, tubulitis; ptc, peritubular capillaritis; v, intimal arteritis; Cr, creatinine; cg, GBM double contours; C4d, C4d deposition; i, interstitial inflammation.
References
1. Ronco P, Beck L, Debiec H, Fervenza FC, Hou FF, Jha V, et al. Membranous nephropathy. Nat Rev Dis Prim. (2021) 7:69. doi: 10.1038/s41572-021-00303-z
2. Howman A, Chapman TL, Langdon MM, Ferguson C, Adu D, Feehally J, et al. Immunosuppression for progressive membranous nephropathy: a UK randomised controlled trial. Lancet. (2013) 381:744–51. doi: 10.1016/S0140-6736(12)61566-9
3. Tesar V, Hruskova Z. Autoantibodies in the diagnosis, monitoring, and treatment of membranous nephropathy. Front Immunol. (2021) 12:593288. doi: 10.3389/fimmu.2021.593288
4. Couser WG. Primary membranous nephropathy. Clin J Am Soc Nephrol. (2017) 12:983–97. doi: 10.2215/CJN.11761116
5. Miller P, Caza T. The expanding spectrum and utility of antigens in membranous nephropathy. Curr Opin Nephrol Hypertens. (2023) 32:232–40. doi: 10.1097/MNH.0000000000000876
6. Moroni G, Ponticelli C. Secondary membranous nephropathy. A narrative review. Front Med. (2020) 7:611317. doi: 10.3389/fmed.2020.611317
7. Leon J, Pérez-Sáez MJ, Batal I, Beck LH Jr, Rennke HG, Canaud G, et al. Membranous nephropathy posttransplantation: an update of the pathophysiology and management. Transplantation. (2019) 103:1990–2002. doi: 10.1097/TP.0000000000002758
8. Bobart SA, Tehranian S, Sethi S, Alexander MP, Nasr SH, Marta CM, et al. A target antigen-based approach to the classification of membranous nephropathy. Mayo Clin Proc. (2021) 96:577–91. doi: 10.1016/j.mayocp.2020.11.028
9. Avasare R, Andeen N, Beck L. Novel antigens and clinical updates in membranous nephropathy. Annu Rev Med. (2024) 75:219–332. doi: 10.1146/annurev-med-050522-034537
10. Debiec H, Martin L, Jouanneau C, Dautin G, Mesnard L, Rondeau E, et al. Autoantibodies specific for the phospholipase A2 receptor in recurrent and de novo membranous nephropathy. Am J Transplant. (2011) 11:2144–52. doi: 10.1111/j.1600-6143.2011.03643.x
11. Pippias M, Stel VS, Aresté-Fosalba N, Couchoud C, Fernandez-Fresnedo G, Finne P, et al. Long-term kidney transplant outcomes in primary glomerulonephritis. Transplantation. (2016) 100:1955–62. doi: 10.1097/TP.0000000000000962
12. Briganti EM, Russ GR, McNeil JJ, Atkins RC, Chadban SJ. Risk of renal allograft loss from recurrent glomerulonephritis. N Engl J Med. (2002) 347:103–9. doi: 10.1056/NEJMoa013036
13. Grupper A, Cornell LD, Fervenza FC, Beck LH, Lorenz E, Cosio FG. Recurrent membranous nephropathy after kidney transplantation. Transplantation. (2016) 100:2710–6. doi: 10.1097/TP.0000000000001056
14. Schwarz A, Krause PH, Offermann G, Keller F. Impact of de novo membranous glomerulonephritis on the clinical course after kidney transplantation. Transplantation. (1994) 58:650–4. doi: 10.1097/00007890-199409270-00002
15. Larsen CP, Walker PD. Phospholipase A2 receptor (PLA2R) staining is useful in the determination of de novo versus recurrent membranous glomerulopathy. Transplantation. (2013) 95:1259–62. doi: 10.1097/TP.0b013e31828a947b
16. de Sousa MV, Fernandes LGR, de Freitas LLL, Zollner R de L, Mazzali M. De novo membranous nephropathy associated with antibody-mediated rejection in kidney transplant recipients. Transplant Proc. (2022) 54:1270–7. doi: 10.1016/j.transproceed.2021.11.041
17. Honda K, Horita S, Toki D, Taneda S, Nitta K, Hattori M, et al. De novo membranous nephropathy and antibody-mediated rejection in transplanted kidney. Clin Transplant. (2011) 25:191–200. doi: 10.1111/j.1399-0012.2010.01213.x
18. Haas M, Loupy A, Lefaucheur C, Roufosse C, Glotz D, Seron D, et al. The Banff 2017 Kidney Meeting Report: Revised diagnostic criteria for chronic active T cell-mediated rejection, antibody-mediated rejection, and prospects for integrative endpoints for next-generation clinical trials. Am J Transplant. (2018) 18:293–307. doi: 10.1111/ajt.14625
19. Loupy A, Haas M, Roufosse C, Naesens M, Adam B, Afrouzian M, et al. The Banff 2019 Kidney Meeting Report (I): Updates on and clarification of criteria for T cell- and antibody-mediated rejection. Am J Transplant. (2020) 20:2318–31. doi: 10.1111/ajt.15898
20. Roll GR, Webber AB, Gae DH, Laszik Z, Tavakol M, Mayen L, et al. A virtual crossmatch-based strategy facilitates sharing of deceased donor kidneys for highly sensitized recipients. Transplantation. (2020) 104:1239–45. doi: 10.1097/TP.0000000000002924
21. Batal I, Vasilescu E-R, Dadhania DM, Adel AA, Husain SA, Avasare R, et al. Association of HLA typing and alloimmunity with posttransplantation membranous nephropathy: A multicenter case series. Am J Kidney Dis. (2020) 76:374–83. doi: 10.1053/j.ajkd.2020.01.009
22. Ye J, Croom N, Troxell ML, Kambham N, Zuckerman JE, Andeen N, et al. Non-full house membranous lupus nephritis represents a clinically distinct subset. Kidney360. (2023) 4:935–42. doi: 10.34067/KID.0000000000000161
23. Paxton L, McMahon L, Wong L. De novo PLA2R positive membranous nephropathy following BNT162b2 mRNA COVID-19 vaccine. Intern Med J. (2022) 52:2191–2. doi: 10.1111/imj.15915
Keywords: membranous nephropathy (MN), transplant kidney, transplant kidney pathology, antibody mediated allograft rejection, de novo membranous nephropathy, recurrent membranous nephropathy
Citation: Khorsandi N, Han HS, Rajalingam R, Shoji J and Urisman A (2024) De novo and recurrent post-transplant membranous nephropathy cases show similar rates of concurrent antibody-mediated rejection. Front. Nephrol. 4:1438065. doi: 10.3389/fneph.2024.1438065
Received: 24 May 2024; Accepted: 29 July 2024;
Published: 03 September 2024.
Edited by:
Phuong Chi Pham, Olive View-UCLA Medical Center, United StatesReviewed by:
Bassam G. Abu Jawdeh, Mayo Clinic Arizona, United StatesArksarapuk Jittirat, University Hospitals Cleveland Medical Center, United States
Copyright © 2024 Khorsandi, Han, Rajalingam, Shoji and Urisman. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anatoly Urisman, YW5hdG9seS51cmlzbWFuQHVjc2YuZWR1