 Isabela Pereira Lucca1
Isabela Pereira Lucca1 Rachel Armani1,2Aluizio B. Carvalho1,2Silvia R. Manfredi1,2Monique V. Rocha E. Silva1,2Thamires B. Gratão1,2Lidia Silva1,2Renato Watanabe1,2
Rachel Armani1,2Aluizio B. Carvalho1,2Silvia R. Manfredi1,2Monique V. Rocha E. Silva1,2Thamires B. Gratão1,2Lidia Silva1,2Renato Watanabe1,2 Maria Eugenia Canziani1,2*
Maria Eugenia Canziani1,2*- 1Department of Medicine, Paulista School of Medicine, Federal University of São Paulo, São Paulo, São Paulo, Brazil
- 2Hrim - Kidney Hospital, São Paulo, São Paulo, Brazil
Introduction: The interaction between blood and dialysis membrane increases the risk of clot formation. Membrane properties can interfere with coagulation activation during dialysis. Heparin is usually used to ensure anticoagulation, which can be monitored by the Activated Clotting Time (ACT) test. The purpose of this study was to compare the ACT of patients with chronic kidney disease (CKD) undergoing hemodialysis with high-flux (HF) and medium cut-off (MCO) membranes.
Methods: This is a prospective, randomized, crossover study in which 32 CKD patients were dialyzed for 12 weeks with each membrane. Blood clotting measured by ACT was evaluated at the beginning, 2nd, and 4th hour of the dialysis session. Throughout the study, there were no changes in the dose or administration method of heparin.
Results: Patients mainly were middle-aged, non-black males on hemodialysis for eight years. Before randomization, ACT values were 132 ± 56, 195 ± 60, and 128 ± 32 seconds at pre-heparinization, 2nd and 4th hour, respectively. After 12 weeks, ACT values in HF and MCO groups were 129 ± 17, 205 ± 65 and 139 ± 38 seconds, and 143 ± 54, 219 ± 68 and 142 ± 45 seconds, respectively. An ANOVA model adjusted and unadjusted for repeated measures showed a significant time but no treatment or interaction effects. In an additional paired-sample analysis, no difference between ACT values of HF and MCO Groups was observed.
Discussion and Conclusion: There was no difference regarding the ACT test during dialysis therapy using HF or MCO membranes. This data suggests that no adjustment in the dose or administration method of heparin is necessary with the use of MCO dialysis membranes.
Introduction
The number of patients undergoing hemodialysis (HD) is continually increasing worldwide (1). Although substantial technological improvements have been made in HD treatment in the last decades, this population’s hospitalization and mortality rates are still very high (2). These data indicate that there is room to enhance the HD technique.
New dialysis membranes have been developed to accomplish better outcomes in hemodialysis patients. However, there is a lack of information regarding the safety profile of anticoagulation during dialysis procedures using these new membranes. Of note, if patients with CKD have a higher risk of bleeding mainly due to platelet dysfunction, on the other hand, they are chronically exposed to extracorporeal circuits, which favors hypercoagulability (3, 4). Unfractionated heparin is the medication usually administered to ensure anticoagulation during the dialysis procedure (5). The narrow therapeutic window for performing adequate anticoagulation without leading to bleeding emphasizes the need to monitor anticoagulation during hemodialysis (6). The adequacy of heparinization can be assessed with the Activated Clotting Time (ACT) test. This test is used to determine heparin’s pharmacokinetics and pharmacodynamics properties, showing a good correlation with heparin concentrations during the hemodialysis session (7). It is essential to mention that ACT is more practical than the gold-standard test for assessing heparin activity (activated partial thromboplastin time or APTT). ACT is considered a point-of-care test to monitor anticoagulation in HD, as it is quick, reproducible, and possible to perform in the dialysis room (8).
The specific role of dialysis membranes on blood coagulation has been of concern since different membrane biocompatibility properties can interfere with the coagulation pattern (9–11). It is well known that exposure to the dialyzer leads to platelet and complement activation. These activations consequently stimulate the coagulation cascade, which starts right after the beginning of the dialysis session (12–15). Recently, new medium cut-off membranes (MCO) were developed to optimize the removal of uremic toxins, and no information regarding its effect on the coagulation pattern is available (16). The purpose of this study was to compare the ACT of patients with chronic kidney disease (CKD) undergoing hemodialysis with MCO and high-flux (HF) membranes.
Materials and methods
Study population
This trial is a pre-defined exploratory analysis of a prospective study that compared the effect of MCO and HF hemodialysis membranes in CKD patients. This study included 32 adult patients with adequate vascular access, undergoing hemodialysis for at least six months. The exclusion criteria were inadequate dialysis (as defined by KtV < 1.2), the presence of heart failure (III or IV New York Heart Association class), peripheral arterial disease, stroke, active inflammation or infectious disease within three months before the enrollment, as well as pregnancy or breastfeeding.
The study was approved by the Ethics Committee of the Federal University of São Paulo (n. 026386/2019) and registered in the Brazilian Registry of Clinical Trials (REBEC, RBR-2m67zd). All patients signed the informed consent form as the first procedure.
Study design
This study is a randomized, crossover, open-label, 28-week follow-up clinical trial. Selected patients were randomized in a 1:1 ratio to 12-week treatment with a single use of MCO (Theranova 400 dialyzer, Baxter Healthcare, USA) or high-flux (FX 100, Fresenius, Germany) dialysis membranes. After the first treatment period, patients underwent a 4-week washout with reusable HF dialyzers (Hemoflow, Fresenius, Germany) and switched to the second 12-week period, as shown in Figure 1. Hemodialysis sessions during treatments and washout were performed for 4 hours, three times a week, with blood and dialysate flows of 300 and 600mL/min, respectively.
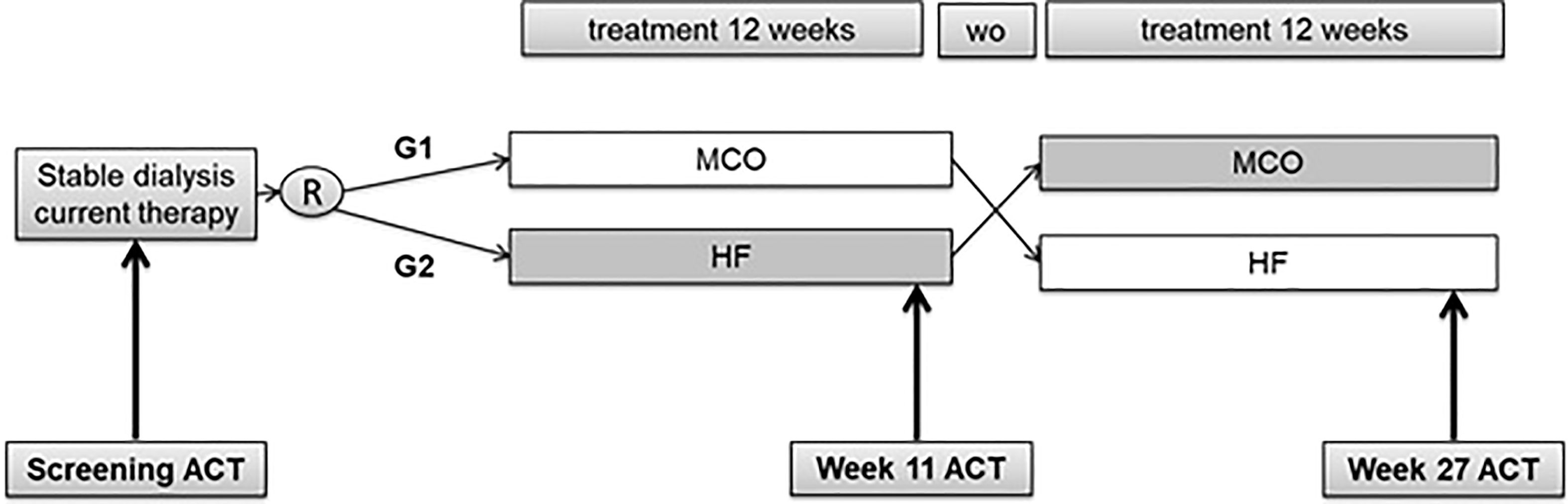
Figure 1 Study design. ACT, Activated Clotting Time; R, Randomization; WO, washout; MCO, medium cut-off membrane; HF, High Flux membrane; G1, Group 1 (MCO followed by HF); G2, Group 2 (HF followed by MCO).
All patients were submitted to an ACT test to construct 3-point curves at the screening week and the end of each treatment (Week 11 and Week 27). The ACT tests (reference values: 80 to 140 seconds) were performed in the ACT-500 equipment (Fundação Adib Jatene, São Paulo, Brazil), comprising a sensor that indicates the time, in seconds, required for the blood sample coagulation. In this test, 2mL blood samples were collected from the arterial pathway of the vascular access in a specific tube, and the same operator performed all tests. In addition, the dialysis room temperature was checked on the days of the ACT tests.
Heparinization was carried out in single bolus or fractionated into 60 and 40% at the beginning (pre-heparinization) and 2nd hour of dialysis, respectively. The unfractionated porcine sodium heparin (Blau Pharmaceutical, São Paulo, Brazil) was used for all patients. An adequate ACT test curve consists of values ranging from 80 to 180% above the baseline after 2 hours of heparinization, and 40% above the baseline, after 4 hours (17). One week before randomization, ACT was performed, and for those whose coagulation pattern was not adequate, the heparin dose was adjusted, and another ACT curve was constructed. Throughout the study, there were no changes in the dose or administration method of heparinization defined during the screening week. Also, bleeding events and extracorporeal system clotting were carefully evaluated and recorded throughout the study.
At baseline, demographic and clinical data were reported, including using medications such as erythropoietin and acetylsalicylic acid. In addition, blood samples were collected in a fasting state at baseline and the end of each treatment period. Besides routine chemistry and hematology tests, inflammatory markers such as IL-6 [reference range (RR) 1.5 to 7.0 pg/mL, Merck Diagnostics’ kit, Germany], IL-1β (RR 0.5 to 12.0 pg/mL, Merck Diagnostics’ kit, Germany), TNFα (RR 1.2 to 15.3 pg/mL, Merck Diagnostics’ kit, Germany), CRP (RR lower than 1.0 mg/dL) and von Willebrand factor (vWf, RR 78 to 1030 ng/mL, Elabscience’s kit, USA) were measured.
Statistical analysis
Mean, standard deviation or frequencies were calculated, and the Kolmogorov-Smirnov test was used to investigate the distribution of all variables. Patients were initially grouped according to randomization in Group 1, composed of patients who started the study with MCO, followed by HF membrane, and Group 2, by those who started with HF, followed by MCO. Comparisons of continuous variables between groups were performed using Student’s t-test or the Mann-Whitney U-test and comparisons of proportions using chi-squared analysis or Fisher’s exact test, as appropriate. Due to the study’s crossover design, the interferences of the order of treatments (sequence effect) and the effect of the first treatment on the second one (carryover effect) were evaluated. In the absence of those conditions, patients were regrouped according to the treatment (MCO and HF), regardless of the observation moment. As appropriate, comparison within groups was evaluated by paired-sample t-test or Wilcoxon. ANOVA analysis for repeated measures evaluating time, group, and interaction effects was performed with and without covariables to compare MCO and High-Flux groups. The selected covariables were the use of erythropoietin, acetylsalicylic acid dose, hemoglobin, platelets, CRP, TNFα, IL-6, IL-1β, and vWf. P < 0.05 was considered statistically significant. All statistical analysis was performed using SPSS 18.0 for Windows (Chicago, IL, USA) and STATA 12 (College Station, TX, USA).
Results
Demographic, clinical data, and laboratory results at baseline are shown in Table 1. The studied population was predominantly composed of middle-aged, non-black males on hemodialysis for eight years, and the main vascular access was an arteriovenous fistula. Hypertension and polycystic kidney disease were the most common CKD etiology. Comorbidities were frequent, and 34% of the patients had cardiovascular disease. Most patients (59%) had been prescribed erythropoietin, 25% acetylsalicylic acid, and none used warfarin or other direct oral anticoagulants. The mean heparin dose per hemodialysis session was 6643 UI, and in 56% of the patients, it was administered as a fractional dose. As expected, the ACT value increased at the 2nd hour, returning to the baseline values at the 4th hour. All demographic and clinical data between Groups 1 and 2 were similar, showing adequate randomization.
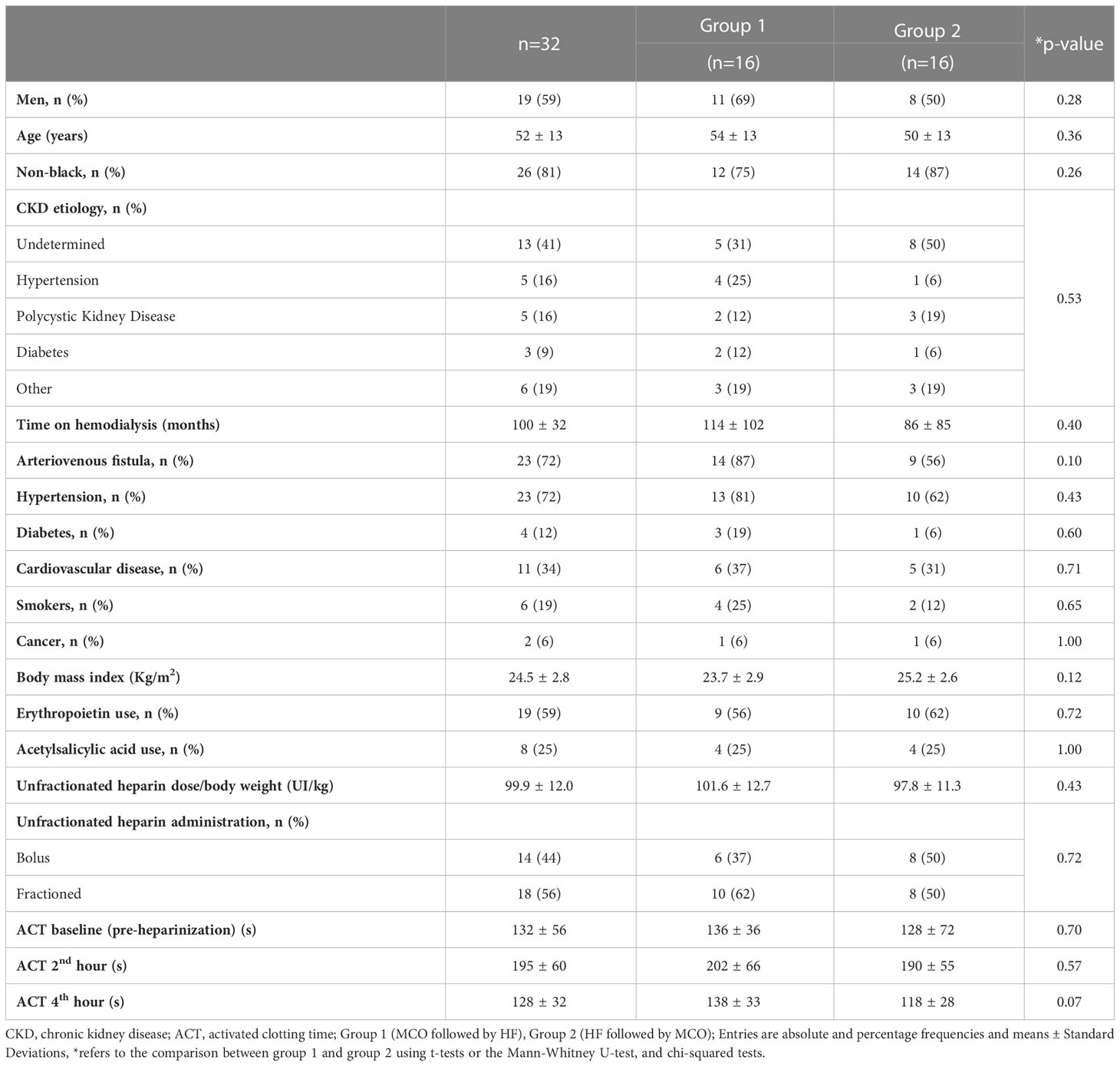
Table 1 Characteristics of the studied population.
Considering the absence of a carryover effect on laboratory, ultrafiltration ratio, and blood pressure parameters, the data were regrouped according to the membrane type regardless of the study week (Table 2). There was no significant difference within groups during the study. An ANOVA model with repeated measures was built to compare the behavior of those parameters on MCO and High-flux groups, and no time, treatment, or interaction effects were observed.
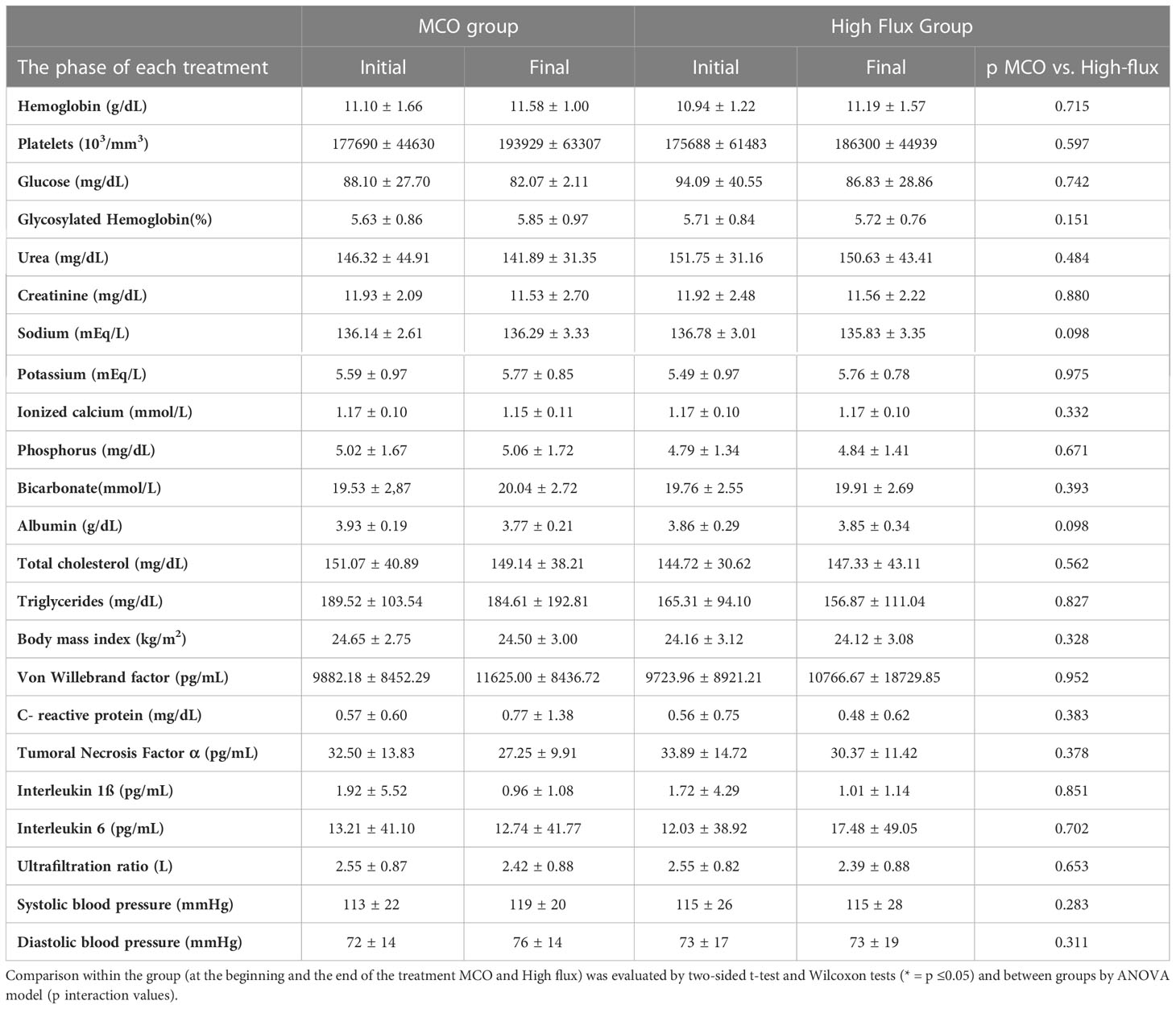
Table 2 Laboratory tests in MCO and High-flux groups before and after 12 weeks of treatment with MCO/High-flux membranes.
There were no carryover effects on the ACT at pre-heparinization (p=0.334), 2nd h (p=0.70), and 4th h (p=0.45). Therefore, the population was regrouped according to the treatment, regardless of the study week. Table 3 shows the ACT values at baseline (pre-heparinization), 2nd, and 4th hour in the MCO and HF Groups. An ANOVA model for repeated measures showed a significant time effect but no treatment or interaction effects (Figure 2).

Table 3 ACT measurements during dialysis sessions before and after 12 weeks of treatment with MCO/High-flux membranes.

Figure 2 ACT curve throughout the dialysis session in the HF and MCO groups. MCO, medium cut-off membrane; HF, High Flux membrane.
A similar result was observed when an adjusted ANOVA model was built. There was a time (p<0.001) but no treatment (p=0.25) or interaction (p=0.69) effects. The covariables used in this model included the use of erythropoietin (p=0.91) and acetylsalicylic acid (p=0.32) and levels of hemoglobin (p=0.50), platelets (p=0.40), vWf (p=0.58), CRP (p=0.35), TNFα (p=0.83), IL6 (p=0.94), IL1ß (p=0.99), and room temperature (p=0.26).
During the study, there were 4 patients withdrawn due to kidney transplant (n=1), changing dialysis center (n=2), and death (n=1). Considering the patients who completed the study (n=28), additional analysis with paired samples was performed. The ACT values remained similar between MCO and HF Groups, at baseline (143 ± 54 vs. 129 ± 17 sec, MCO vs. HF, respectively, p= 0.20), at 2nd hour (219 ± 68 vs. 201 ± 62 sec, p=0.30) and 4th hour (142 ± 45 vs138 ± 39 sec, p=0.76).
Finally, there were no bleeding events or clotting of the extracorporeal system in the groups throughout the study.
Discussion/Conclusion
This study showed no difference between the effect of MCO or HF membranes on the ACT test during hemodialysis.
The interaction between blood and the extracorporeal circuit on hemodialysis, mainly the dialysis membrane, activates the complement system and the coagulation cascade, requiring anticoagulants during the procedure (6, 18). The coagulation activation by the dialyzer is partially dependent on its biocompatibility characteristics. The switch of the former cellulosic membranes to the more biocompatible synthetic membranes, currently used on chronic hemodialysis, has decreased inflammation and the activation of the complement system, leading to a decreased hypercoagulable state (11). MCO dialyzer membranes could activate coagulation at a minor level by providing a better clearance of the middle molecules as inflammatory cytokines. However, a recent study using an in vitro model demonstrated that the activity of coagulation factors and their inhibitors remains unaltered with MCO membranes (16, 19). In the present study, we could not show differences in the ACT curves between both HF and MCO membranes, regardless of the adjustment to CRP, IL6, TNFα, IL1ß, and vWf. There was also no significant difference in inflammatory markers found in HF and MCO groups, which can be inconsistent with studies that show that MCO membranes reduce inflammation (16). This might be due to the population included in the study, as the presence of active inflammation was one of the exclusion criteria.
Moreover, the bigger pore size of MCO membranes compared to HF could be a concern regarding the heparinization scheme (20). Firstly, this physical characteristic of that membrane leads to a higher ultrafiltration rate and, consequently, to hemoconcentration inside the dialyzer (21). It is well known that the initial blood coagulation reaction could be accelerated under a hemoconcentration state (22). Interestingly, patients undergoing post-dilution hemodiafiltration that favors hemoconcentration within the dialyzer may need to increase the heparin dose (23). Secondly, the bigger pore size allows some loss of middle molecules, like albumin, which weighs 68000 Da (24). Considering that heparin’s molecular weight ranges from 3000 to 30000 Da, one could consider that heparin loss occurs during hemodialysis with the MCO membrane (25). Those two conditions could increase blood coagulability, requiring higher doses of heparin. However, we observed no difference in the ACT values with the use of MCO compared to HF membranes, despite the heparin dose being maintained unchanged during the study.
The ACT test was used in this study as a measurement method to evaluate the coagulation pattern (8). Although this test has been considered a point of care for monitoring anticoagulation during dialysis, some factors, such as platelet activation, room temperature, and hypothermia, could interfere with the reliability of its results (26, 27). In the present study, room temperature, hypothermia, and the number of platelets were controlled and included as covariables in the adjusted model.
One limitation of this study is the relatively small sample size, but the crossover and randomized design might strengthen it. To the best of our knowledge, this was the first study evaluating the MCO membrane coagulation activation pattern during hemodialysis.
In conclusion, there was no difference regarding the ACT test during dialysis therapy using HF or MCO membranes. This data suggests that no adjustment in the dose or administration method of heparin is necessary with the use of MCO dialysis membranes.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving human participants were reviewed and approved by Ethics Committee of Federal University of São Paulo (n. 026386/2019). The patients/participants provided their written informed consent to participate in this study.
Author contributions
Conception and design of the study: MC and SM. Generation, collection, analysis, and interpretation of data: IP, RA, MR, TG, LS and RW. Drafting and revision of the manuscript: IP, RA, AC and MC. Approval of the final version of the manuscript: IP, RA, AC and MC. All authors contributed to the article and approved the submitted version.
Funding
This is an investigator-driven study supported by a study grant from BAXTER Healthcare Corporation. The company had no part in the study design, patient inclusion, data collection, statistical analysis, and manuscript writing.
Conflict of interest
MC is an employee of the Federal University of São Paulo, a recipient of scholarships from the Brazilian Council for Research CNPq, and receives research grants, consulting fees, and honoraria from Baxter Healthcare, Fresenius Medical Care, AstraZeneca, Bayer, and Novartis. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be constructed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Collaboration GCKD. Global, regional, and national burden of chronic kidney disease, 1990-2017: A systematic analysis for the global burden of disease study 2017. Lancet (2020) 395(10225):709–33.
2. Ronco C. The rise of expanded hemodialysis. Blood Purif (2017) 44(2):I–VIII. doi: 10.1159/000476012
3. Castillo R, Lozano T, Escolar G, Revert L, López J, Ordinas A. Defective platelet adhesion on vessel subendothelium in uremic patients. Blood (1986) 68(2):337–42. doi: 10.1182/blood.V68.2.337.337
4. Ambühl PM, Wüthrich RP, Korte W, Schmid L, Krapf R. Plasma hypercoagulability in hemodialysis patients: Impact of dialysis and anticoagulation. Nephrol Dial Transpl (1997) 12(11):2355–64. doi: 10.1093/ndt/12.11.2355
5. Shen JI, Winkelmayer WC. Use and safety of unfractionated heparin for anticoagulation during maintenance hemodialysis. Am J Kidney Dis (2012) 60(3):473–86. doi: 10.1053/j.ajkd.2012.03.017
6. Fischer KG. Essentials of anticoagulation in hemodialysis. Hemodial Int (2007) 11(2):178–89. doi: 10.1111/j.1542-4758.2007.00166.x
7. Kandrotas RJ, Gal P, Douglas JB, Deterding J. Pharmacokinetics and pharmacodynamics of heparin during hemodialysis: Interpatient and intrapatient variability. Pharmacotherapy (1990) 10(5):349–55.
8. Ouseph R, Ward RA. Anticoagulation for intermittent hemodialysis. Semin Dial (2000) 13(3):181–7. doi: 10.1046/j.1525-139X.2000.00052.x
9. Woffindin C, Hoenich NA. Blood-membrane interactions during haemodialysis with cellulose and synthetic membranes. Biomaterials (1988) 9(1):53–7. doi: 10.1016/0142-9612(88)90069-5
10. Hofbauer R, Moser D, Frass M, Oberbauer R, Kaye AD, Wagner O, et al. Effect of anticoagulation on blood membrane interactions during hemodialysis. Kidney Int (1999) 56(4):1578–83. doi: 10.1046/j.1523-1755.1999.00671.x
11. Chanard J, Lavaud S, Randoux C, Rieu P. New insights in dialysis membrane biocompatibility: Relevance of adsorption properties and heparin binding. Nephrol Dial Transpl (2003) 18(2):252–7. doi: 10.1093/ndt/18.2.252
12. Sirolli V, Ballone E, Di Stante S, Amoroso L, Bonomini M. Cell activation and cellular-cellular interactions during hemodialysis: effect of dialyzer membrane. Int J Artif Organs (2002) 25(6):529–37. doi: 10.1177/039139880202500607
13. Lucchi L, Ligabue G, Marietta M, Delnevo A, Malagoli M, Perrone S, et al. Activation of coagulation during hemodialysis: Effect of blood lines alone and whole extracorporeal circuit. Artif Organs (2006) 30(2):106–10. doi: 10.1111/j.1525-1594.2006.00188.x
14. Chen SF, Chen M. Complement activation in progression of chronic kidney disease. Adv Exp Med Biol (2019) 1165:423–41. doi: 10.1007/978-981-13-8871-2_20
15. Poppelaars F, Gaya da Costa M, Faria B, Berger SP, Assa S, Daha MR, et al. Intradialytic complement activation precedes the development of cardiovascular events in hemodialysis patients. Front Immunol (2018) 9:2070. doi: 10.3389/fimmu.2018.02070
16. Zickler D, Schindler R, Willy K, Martus P, Pawlak M, Storr M, et al. Medium cut-off (MCO) membranes reduce inflammation in chronic dialysis patients-a randomized controlled clinical trial. PloS One (2017) 12(1):e0169024. doi: 10.1371/journal.pone.0169024
18. Huang Z, Gao D, Letteri JJ, Clark WR. Blood-membrane interactions during dialysis. Semin Dial (2009) 22(6):623–8. doi: 10.1111/j.1525-139X.2009.00658.x
19. Voigt M, Gebert M, Haug U, Hulko M, Storr M, Boschetti-de-Fierro A, et al. Retention of beneficial molecules and coagulation factors during haemodialysis and haemodiafiltration. Sci Rep (2019) 9(1):6370. doi: 10.1038/s41598-019-42783-w
20. Hutchison CA, Wolley M. The rationale for expanded hemodialysis therapy (HDx). Contrib Nephrol (2017) 191:142–52. doi: 10.1159/000479262
21. Clark WR, Gao D, Neri M, Ronco C. Solute transport in hemodialysis: Advances and limitations of current membrane technology. Contrib Nephrol (2017) 191:84–99. doi: 10.1159/000479258
22. Sagesaka T. Influence of red blood cell concentration on the initiation time of blood coagulation: risk of thrombus formation by hemoconcentration. Clin Hemorheol Microcirc (2004) 31(4):243–9.
23. Klingel R, Schaefer M, Schwarting A, Himmelsbach F, Altes U, Uhlenbusch-Körwer I, et al. Comparative analysis of procoagulatory activity of haemodialysis, haemofiltration and haemodiafiltration with a polysulfone membrane (APS) and with different modes of enoxaparin anticoagulation. Nephrol Dial Transpl (2004) 19(1):164–70. doi: 10.1093/ndt/gfg459
24. Ronco C, La Manna G. Expanded hemodialysis: A new therapy for a new class of membranes. Contrib Nephrol (2017) 190:124–33. doi: 10.1159/000468959
25. Adams RL, Bird RJ. Review article: Coagulation cascade and therapeutics update: relevance to nephrology. part 1: Overview of coagulation, thrombophilias and history of anticoagulants. Nephrol (Carlton) (2009) 14(5):462–70.
26. Ferguson JJ. Conventional antithrombotic approaches. Am Heart J (1995) 130(3 Pt 2):651–7. doi: 10.1016/0002-8703(95)90302-X
Keywords: medium cut-off membrane, Theranova, high-flux dialysis, coagulation pattern, activated clotting time
Citation: Lucca IP, Armani R, Carvalho AB, Manfredi SR, Silva MVRE, Gratão TB, Silva L, Watanabe R and Canziani ME (2023) The effects of medium cut-off and high-flux membranes on activated clotting time of patients on hemodialysis. Front. Nephrol. 3:1133910. doi: 10.3389/fneph.2023.1133910
Received: 29 December 2022; Accepted: 30 January 2023;
Published: 14 February 2023.
Edited by:
Michal Nowicki, Medical University of Lodz, PolandReviewed by:
Yupei Li, West China Hospital, Sichuan University, ChinaBernd Stegmayr, Umeå University, Sweden
Copyright © 2023 Lucca, Armani, Carvalho, Manfredi, Silva, Gratão, Silva, Watanabe and Canziani. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maria Eugenia Canziani, bWVjYW56aWFuaTFAZ21haWwuY29t