
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Nephrol., 31 October 2022
Sec. Onconephrology
Volume 2 - 2022 | https://doi.org/10.3389/fneph.2022.1041819
This article is part of the Research TopicWomen in Onconephrology: 2022View all 6 articles
 T. Van Meerhaeghe1*
T. Van Meerhaeghe1* J.F. Baurain2
J.F. Baurain2 O. Bechter3
O. Bechter3 C. Orte Cano4
C. Orte Cano4 V. Del Marmol4
V. Del Marmol4 A. Devresse5
A. Devresse5 P. Doubel6
P. Doubel6 M. Hanssens7R. Hellemans8D. Lienard4A. Rutten9
M. Hanssens7R. Hellemans8D. Lienard4A. Rutten9 B. Sprangers10
B. Sprangers10 A. Le Moine1
A. Le Moine1 S. Aspeslagh11
S. Aspeslagh11Background: Kidney transplant recipients (KTR) are at increased risk of cancer due to chronic immunosuppression. Non-melanoma skin cancer has an excess risk of approximately 250 times higher than the general population. Moreover, in solid organ transplant recipients (SOTR) these cancers have a more aggressive behavior, with an increased risk of metastasis and death. Cemiplimab, a human monoclonal IgG4 antibody against programmed cell death (PD-1) has shown considerable clinical activity in metastatic and locally advanced cutaneous squamous cell carcinoma (cSCC) in patients for whom no widely accepted standard of care exists. Cemiplimab has therefore been approved since 2018 for the treatment of advanced cSCC. However, data regarding the use of cemiplimab in SOTR and particularly in KTR are scarce and based on published case reports and small case series. In this study, we report on the real-life outcome of cemiplimab use in a Belgian cohort of seven KTR suffering from advanced cSCC.
Objective: To report on the overall response rate (ORR) and safety of cemiplimab in KTR in Belgium.
Results: Seven patients suffering from advanced cSCC, treated with cemiplimab, between 2018 and 2022, in Belgium were identified. Three patients were on corticosteroid monotherapy, one patient on tacrolimus monotherapy and three patients were on at least 2 immunosuppressants at start of cemiplimab. The ORR was 42.8%, stable disease was seen in 14.3% and progressive disease was found in 42.8% of the patients, respectively. The median administered number of cycles was 12, interquartile range (IQR) 25-75 [3.5 – 13.5]. All patients were treated with surgery before administration of cemiplimab, 71.4% received additional radiotherapy and only 1 patient was treated with chemotherapy prior to receiving cemiplimab. Biopsy-proven acute renal allograft rejection was observed in one patient, who eventually lost his graft function but showed a complete tumor response to treatment. Low grade skin toxicity was seen in one patient of the cohort.
Conclusion: The present case series shows that the use of cemiplimab in KTR with advanced cSCC who failed to respond to previous surgery, chemo – and/or radiotherapy treatment is associated with an ORR of 42.8% with minimal risk of graft rejection (14.3%) and good tolerance.
Malignancy is a significant adverse event in kidney transplant recipients (KTR). The overall risk of developing cancer has been reported to be 2 - and 4 – fold higher compared to the general population (1, 2). Some cancer types are overrepresented in KTR, especially non-melanoma skin cancer (NMSC) with an excess risk of approximately 250 times higher than the general population (3). The most frequent NMSC encountered in KTR is cutaneous squamous cell carcinoma (cSCC). Moreover, KTR patients tend to have a more aggressive behavior of the disease and an increased risk of metastasis and cancer related death (4, 5). cSCC tumors harbor a high mutation burden, which has been associated with good response to immune checkpoint inhibitors (6). Cemiplimab, a human monoclonal IgG4 antibody against anti-PD-1 has shown favorable overall survival and progression free survival in immunocompetent patients suffering from advanced cSCC (7–9). However, these trials excluded patients with a history of solid organ transplantation owing to concerns about alloimmunity, organ rejection, and the use of concomitant immunosuppressive therapy possibly abolishing the efficacy of immunotherapy. Evidence on efficacy of immune checkpoint inhibitors (ICI) in KTR is mainly based on case reports, case series and a few systematic reviews reporting on its postmarketing use (10–17).
Herein, we review the real-world experience with cemiplimab in KTR for advanced cSCC in Belgium.
Kidney transplant recipients, who presented an advanced cSCC for which they were treated with cemiplimab between 2018 and first of January of 2022 in Belgium were included in the present study. Advanced cSCC was defined as either locally advanced disease not amenable to curative surgery or radiotherapy (RT) or metastatic disease. cSCC stage was defined according to the American Joint Committee on Cancer (AJCC) TNM Staging system for cSCC of Head and Neck (18). Immune response was evaluated according to the iRECIST criteria for solid tumors (19). Objective response rate (ORR) was defined as complete response (CR) or partial response (PR). Seven patients were identified across 5 different centers. Clinical and demographic features, immunosuppression, allograft function, efficacy and outcomes were reviewed. Central and Local ethics’ committees of the different centers involved, approved the study.
Data are described using mean ± standard deviation (SD) or medians and interquartile ranges (IQR) 25-75 depending on the distribution of the data. Estimates of overall survival (OS, the time from introduction of cemiplimab to death due to any cause) was assessed by the Kaplan-Meier method for the 7 patients. Statistical analysis was done by using MedCalc Software Ltd.
A total of 7 KTR treated with cemiplimab from 5 different centers in Belgium were identified between 2018-2022 in Belgium. Table 1 illustrates baseline characteristics of included patients. All patients but one patient suffered from stage IV cSCC according to the AJCC and one patient had a locally advanced cSCC with eye localization, which was not treatable neither with surgery nor with radiotherapy. The mean age of the patients was 68.1 ± 10.5 years and most patients were male (71.4%). The mean body mass index (BMI) of the patients was 23.8 ± 3.9 kg/m2 and the median Karnofsky score of the patients was 80 (IQR 25-75 [65-90]). All patients were dialyzed prior to renal transplantation. The etiology of the end-stage kidney disease was diverse: genetic in 3, vascular in 1, tubulo-interstitial disease in 1, chronic pyelonephritis in 1 and glomerulonephritis in 1. No patient was suffering from an underlying auto-immune disorder (see Table 1).
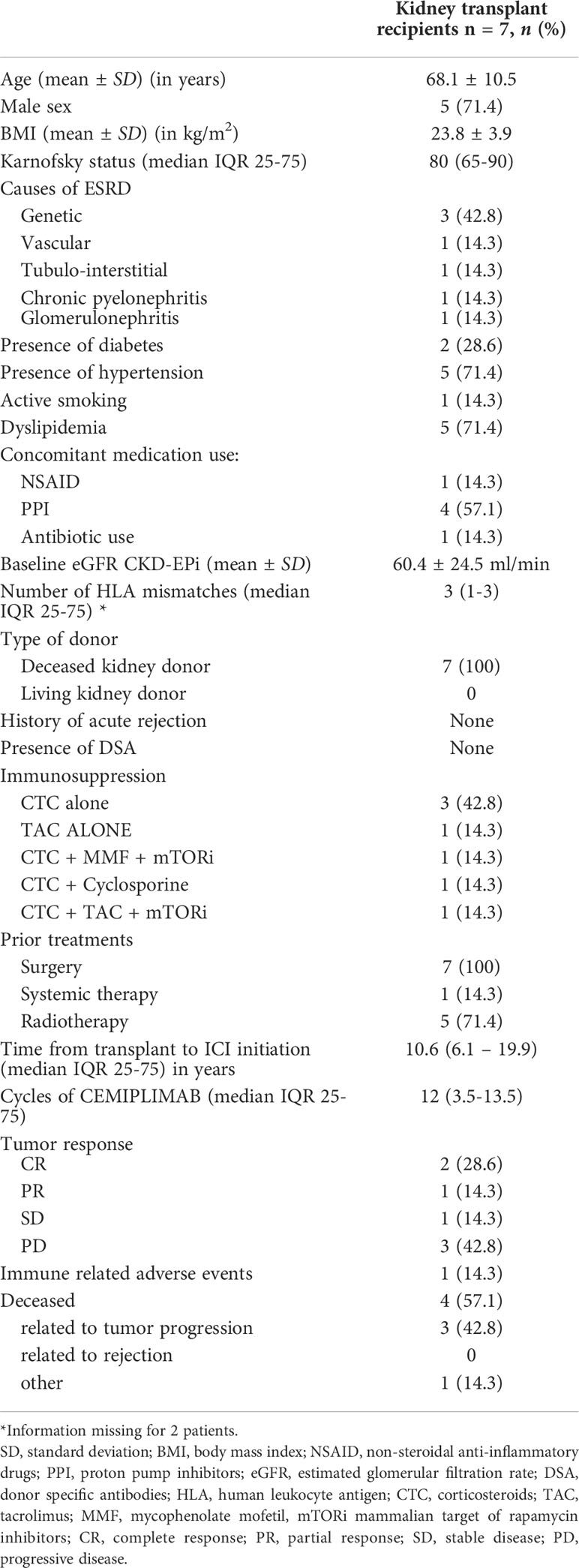
Table 1 Patients’ characteristics and main outcomes.
Diabetes was seen in 28.6%, arterial hypertension in 71.4%, active smoking in 14.3% and dyslipidemia in 71.4% of the patient population.
Mean baseline estimated Glomerular Filtration Rate (eGFR) according to Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) was 60.4 ± 24.5 ml/min. No patient in the study had donor specific antibodies and none had a history of acute rejection. Median HLA mismatches were 3 (IQR 25-75 [1-3], but information was lacking for 2 patients in the study. All patients received a deceased donor kidney. Immunosuppression was lowered prior to introduction of cemiplimab in 6 out of 7 patients. Three patients (42.8%) were treated with low dose methylprednisolone, 1 patient was on tacrolimus monotherapy (14.3%), and 3 patients (42.8%) received 2 or more than 2 immunosuppressive drugs. Prior to introduction of cemiplimab, all patients were treated with surgery, 1 patient had chemotherapy (14.3%) and 5 patients (71.4%) received radiotherapy. The median time from transplantation to cemiplimab initiation was 10.6 years (IQR 25-75 [6.1-19.9]). The median cycles administered of cemiplimab were 12 (IQR 25-75 [3.5-13.5]).
ORR was seen in 3 patients (42.8%), stable disease (SD) in 1 (14.3%) and progressive disease in 3 (42.8%). Death due to tumoral progression was seen in 3 patients (42.8%) (Table 2). The median overall survival (OS) estimated by the Kaplan Meier was 12 months (95% CI of the median 2 – 15 months) (Figure 1).
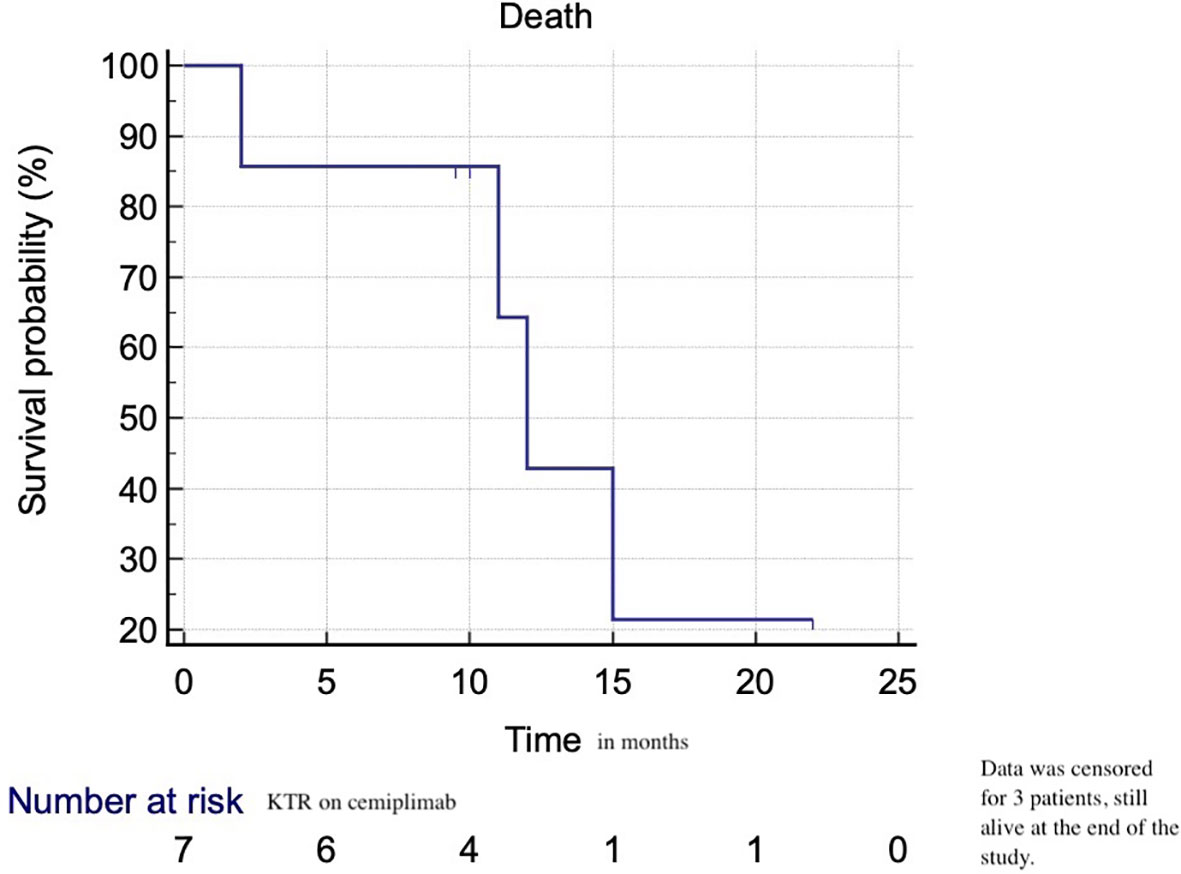
Figure 1 Overall survival of KTR on cemiplimab for advanced cSSC.
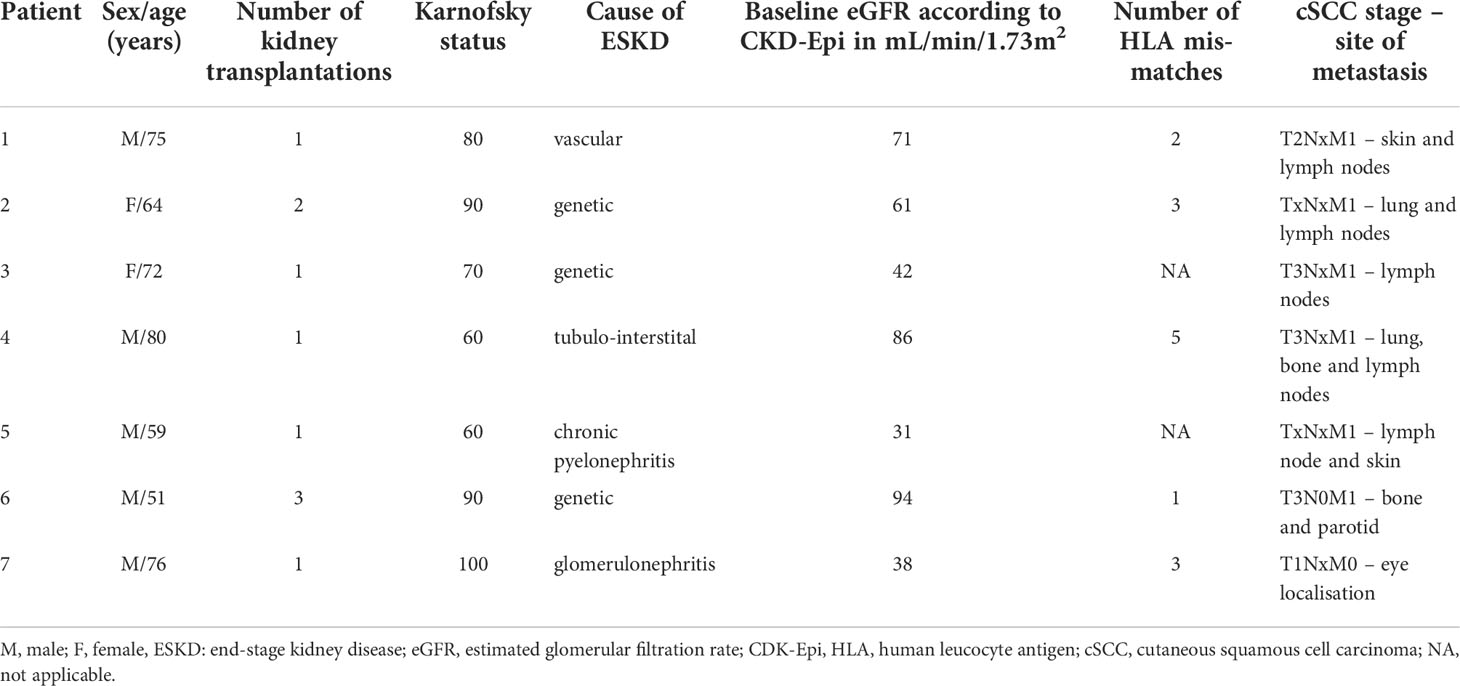
Table 2A Details of the characteristics and outcomes of the patients included in the study.
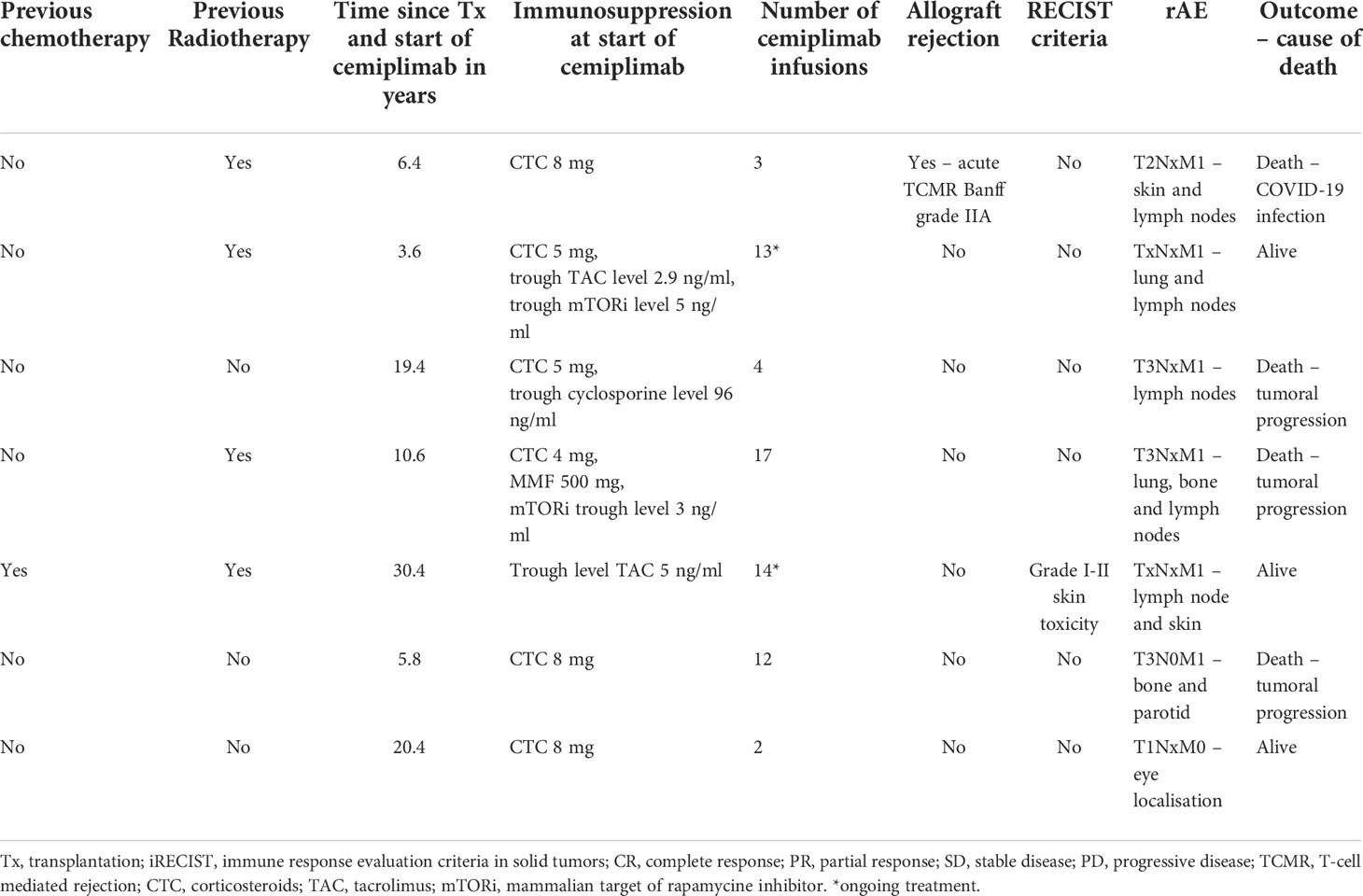
Table 2B Details of the characteristics and outcomes of the patients included in the study.
In patients with a CR or PR response to cemiplimab, 1 patient suffered from a difficult to treat eye localization, and 2 patients had lymph node and skin metastasis. There was no involvement of other organs or bone lesions. On the contrary 2 of the 3 patients with progressive disease (PD) had lung and/or bone lesions. Patients on monotherapy (CTC or TAC alone) tended to have a better tumoral response compared to patients with at least two immunosuppressive treatments.
Only one patient (14.3%) developed biopsy-proven acute graft rejection during his treatment with cemiplimab within 2 weeks after administration of the first dose. He was on corticosteroid monotherapy at the time of rejection. Histopathological analysis showed acute T-cell mediated rejection Banff grade IIA. Treatment consisted of high dose glucocorticosteroids and subsequent transplantectomy for life-threatening rupture of his graft. He showed however a complete tumor response (Table 2).
IrAEs other than graft rejection occurred only in one patient of the entire cohort and consisted of a grade I-II skin toxicity, without need to withhold immunotherapy.
The present case series shows that in KTR with advanced cSCC, who failed to respond to surgery, chemo- and/or radiotherapy, cemiplimab is associated with a good ORR of 42.8% and a low risk of graft rejection (14.3%). Indeed, the two major concerns regarding the use of immune checkpoint inhibitors in solid organ transplant recipients (SOTR) are the risk of allograft rejection and the potential reduction in the anti-cancer response related to the concomitant immunosuppression. Anti-PD-1, anti-PD-L1 and anti-CTLA-4 based therapies activate the immune system, causing the expansion and activation of various immune cell subsets. These changes in immunity can enhance anti-tumor response but also autoimmunity and alloimmunity, therefore increasing the risk of allograft rejection. Due to the fact that patients with a history of organ transplant and with concomitant immunosuppressive therapy are almost always excluded from immunotherapy trials, data on the efficacy of ICI in SOTR are scarce.
One case series of 7 patients, including kidney, liver and lung transplant recipients suffering from advanced cSCC treated with anti-PD-1, showed an ORR of 57.1% (14). Another multicenter study including 69 KTR reported an ORR of 36% in the subgroup of patients suffering from cSCC, with a significantly prolonged survival with the use of ICI (median overall survival 19.8 months vs. 10.6 months) (13). The efficacy of ICI in cSCC was further confirmed in a larger systematic review, showing that SOTR suffering from cSCC derived the most clinical benefit from treatment with ICI compared to other cancer types with an ORR of 68.2%. Our data are in line with these findings (17).
The Kaplan-Meier estimate of the median survival was 12 months in our study and data were censored for 3 patients (still alive at the end of the study). We do not have a control KTR population treated with standard therapy to compare our results. An integrated analysis of a phase 2 study of cemiplimab in advanced cSCC in patients without SOTR, the Kaplan-Meier estimated probability of OS was 73.3% (95% CI: 66.1% to 79.2%) at 24 months, with median OS not reached (20). Whether OS on cemiplimab is prolonged in SOTR suffering from advanced cSCC needs to be addressed in further prospective trials.
The main concern of the usage of ICI in KTR is graft rejection. Cancer after transplantation is mostly managed by a reduction in immunosuppression and with the addition of ICI this might trigger allograft rejection (1). In most case reports and case series published so far, the highest rejection rates were identified in KTR (around 42-44%) compared to other SOTR (10–17). Factors associated with graft rejection were a history of acute rejection, anti-PD-1 usage and single agent immunosuppressive treatment. However, treatment with at least one other IS than corticosteroids, usage of mechanistic target of rapamycine inhibitors (mTORi) and longer time after transplantation (> 8 years) was associated with lower risk of rejection (10–17). Graft rejection in the study of Murakami et al. was associated with high comorbidity as 65.5% of the patients lost their graft function after rejection (13). The patient who rejected his graft in our case series was on low dose methylprednisolone and developed rejection within 2 weeks after his first infusion of cemiplimab, in line with the timing seen in other published reports, where the median time to rejection was 21 days. Despite rescue treatment with high dose glucocorticosteroids patient lost his graft function, but achieved a complete tumor response. The rejection rate in our study is particularly low, compared to published reports. Factors associated with this low rejection rate could not be identified considering the small number of patients included in the study. Nonetheless, the use of cemiplimab in this patient population to control tumor burden is encouraging. Indeed, cemiplimab seems to be associated with lower rates of graft rejection compared to pembrolizumab and nivolumab (13, 16). This observation could be due to different cancer types treated with pembrolizumab and nivolumab in the different case series.
It is well known that mTORi have anti-proliferative effects and thus may potentially prevent allograft rejection (21). Data reported by Murakami et al. and Portuguese et al., show that KTR on mTORi tend to reject less compared to patients under other immunosuppressive regimens. Two patients in our study on mTORi did not present with allograft rejection. A recent multicenter, single arm, phase I study in KTR with cancer showed that addition of nivolumab without preventive reduction in immunosuppression did not impede on tumor response and reduced rejection rates to 12% (22). The patients enrolled in the study were at low immunological risk with stable graft function, had baseline low immunosuppression and suffered from a variety of cancers. These factors might have biased the results, but this is the first prospective study in KTR and is important to consider when confronted with the decision to lower immunosuppression before starting immunotherapy. Future studies need to address which immunosuppressive regimen is the most feasible to combine with ICI therapy. Two prospective trials are underway to specifically explore the efficacy and safety of ICI in KTR, including the “Tacrolimus, Nivolumab, and Ipilimumab in Treating Kidney Transplant Recipients with Selected Unresectable or Metastatic Cancers” (NCT03816332) and the “Cemiplimab in AlloSCT/SOT Recipients with CSS (CONTRAC)” (NCT04339062) (23, 24). One could indeed speculate that there is a therapeutic window for these patients where immunosuppressive therapy is least interfering with the therapeutic benefit of anti-PD-1 based therapy but is also effectively preventing graft rejection.
Well known side effects of immune checkpoint inhibitors are the development of immune related adverse events. In the case series of Tsung et al., 2 of the 7 SOTR developed irAE and one case study showed severe life-threating pneumonitis after cemiplimab treatment for advanced cSCC (14, 25). In our patient cohort only one patient developed low-grade skin toxicity without the need to withhold cemiplimab, with an ongoing tumor response to cemiplimab. Ideally, predictive biomarkers of graft rejection and tumoral response in KTR need to be identified, to better select those patients that may benefit from ICI without compromising their graft during the administration of ICI. One study showed the possibility to use donor-derived cell free DNA (ddcfDNA) for the early detection of graft rejection after introduction of nivolumab (26). This approach is minimally invasive and could help us detect early graft rejection and to adapt treatment accordingly. Other possible approaches to prevent rejection are the use of non-invasive biomarkers of the immune response induced by ICI: peripheral immune cell composition associated with graft tolerance and/or rejection, changes in the immune repertoire after administration of ICI, blood transcriptomics and urinary cell mRNA/chemokines profiling associated with acute rejection (for example, CXCL9, CD3ϵ, perforin, granzyme B, and IP-10) (27–32). With the advent of personalized medicine this approach is of interest to guide and adapt our treatment and to better inform our patients about the risks of graft rejection.
It has been hypothesized that a better clinical response in KTR may be associated with an increased risk of graft rejection. So far, in the KTR subgroup, graft rejection was not associated neither with a better tumoral response, nor with a higher mortality when compared to other SOTR. However maintaining low dose immunosuppression before start of ICI, the usage of mTORi and longer time elapsed since transplantation seem to be associated with a better ORR (17). ORR in our study is in line with most published reports and points to a possible benefit of cemiplimab in KTR suffering from advanced cSCC. All but one patient had preventive reduction in the dose of immunosuppression and most patients had kidney transplantation for at least 10 years.
The main limitations of our study are the retrospective design, the lack of control group and the low patient number. Only one patient developed graft rejection and our study was unable to identify the factors associated with rejection. However, the high ORR achieved with cemiplimab for advanced cSCC and the low number of graft rejection in our case series are encouraging. An interdisciplinary approach between oncologist and nephrologist is of utmost importance to guide treatment decisions and patient follow-up. Patients should be aware of the risk of graft rejection, but the present case series confirms and extends the data from recent literature regarding the good tumor response in advanced cSCC in KTR treated with ICI, with limited risk of graft rejection. We do however acknowledge the need of good designed prospective studies to search for biomarkers of rejection and/or tumor response, in order to guide our patients concerning the risk/benefit ratio of these treatments. Our center started a multicenter and international project to study allograft rejection in this particular patient population in search of the mechanisms and potential predictive markers of rejection before and during ICI treatment in KTR.
The present case series shows that in KTR with advanced cSCC who failed to respond to conventional treatment, the use of cemiplimab is associated with a good ORR of 42.8% with low risk of graft rejection (14.3%) and irAE. Cemiplimab might be a promising treatment for patients with advanced cSCC and could be considered as second-line treatment in KTR with difficult to treat cSCC.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Comité d’éthique de l’Hôpital Erasme. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
TM collected the data and wrote the manuscript. All authors contributed to the article and approved the submitted version.
TM received research grants from Fonds Erasme, Fonds de la Chirurgie Cardiaque, le Fonds National de Recherche Scientifique Belgium (grant number 40010386), The Belgian Transplant Society Roche grant, The European Society of Organ Transplantation Transplant Fellowship.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Al-Adra D, Al-Qaoud T, Fowler K, Wong G. De novo malignancies after kidney transplantation. Clin J Am Soc Nephrol (2022) 17(3):434−43. doi: 10.2215/CJN.14570920
2. Au E, Wong G, Chapman JR. Cancer in kidney transplant recipients. Nat Rev Nephrol (2018) 14(8):508−20. doi: 10.1038/s41581-018-0022-6
3. Mittal A, Colegio OR. Skin cancers in organ transplant recipients. Am J Transplant (2017) 17(10):2509−30. doi: 10.1111/ajt.14382
4. Rosales BM, de la Mata N, Vajdic CM, Kelly PJ, Wyburn K, Webster AC. Cancer mortality in kidney transplant recipients: An Australian and new Zealand population-based cohort study, 1980–2013. Int J Canc (2020) 146(10):2703−11. doi: 10.1002/ijc.32585
5. Lott DG, Manz R, Koch C, Lorenz RR. Aggressive behavior of nonmelanotic skin cancers in solid organ transplant recipients. Transplantation (2010) 90(6):683−7. doi: 10.1097/TP.0b013e3181ec7228
6. Hanna GJ, Ruiz ES, LeBoeuf NR, Thakuria M, Schmults CD, Decaprio JA, et al. Real-world outcomes treating patients with advanced cutaneous squamous cell carcinoma with immune checkpoint inhibitors (CPI). Br J Canc (2020) 123(10):1535−42. doi: 10.1038/s41416-020-01044-8
7. Migden MR, Rischin D, Schmults CD, Guminski A, Hauschild A, Lewis KD, et al. PD-1 blockade with cemiplimab in advanced cutaneous squamous-cell carcinoma. N Engl J Med (2018) 379(4):341−51. doi: 10.1056/NEJMoa1805131
8. Migden MR, Khushalani NI, Chang ALS, Lewis KD, Schmults CD, Hernandez-Aya L, et al. Cemiplimab in locally advanced cutaneous squamous cell carcinoma: results from an open-label, phase 2, single-arm trial. Lancet Oncol (2020) 21(2):294−305. doi: 10.1016/S1470-2045(19)30728-4
9. Keeping S, Xu Y, Chen CI, Cope S, Mojebi A, Kuznik A, et al. Comparative efficacy of cemiplimab versus other systemic treatments for advanced cutaneous squamous cell carcinoma. Future Oncol (2021) 17(5):611−27. doi: 10.2217/fon-2020-0823
10. Abdel-Wahab N, Safa H, Abudayyeh A, Johnson DH, Trinh VA, Zobniw CM, et al. Checkpoint inhibitor therapy for cancer in solid organ transplantation recipients: an institutional experience and a systematic review of the literature. J Immunother Canc (2019) 7(1):158. doi: 10.1186/s40425-019-0585-1
11. Ros J, Matos I, Martin-Liberal J. Immunotherapy in organ-transplanted cancer patients: efficacy and risk of organ rejection. Ann Oncol (2019) 30(7):1173−7. doi: 10.1093/annonc/mdz129
12. Manohar S, Thongprayoon C, Cheungpasitporn W, Markovic SN, Herrmann SM. Systematic review of the safety of immune checkpoint inhibitors among kidney transplant patients. Kidney Int Rep (2020) 5(2):149−58. doi: 10.1016/j.ekir.2019.11.015
13. Murakami N, Mulvaney P, Danesh M, Abudayyeh A, Diab A, Abdel-Wahab N, et al. A multi-center study on safety and efficacy of immune checkpoint inhibitors in cancer patients with kidney transplant. Kidney Int (2021) 100(1):196−205. doi: 10.1016/j.kint.2020.12.015
14. Tsung I, Worden FP, Fontana RJ. A pilot study of checkpoint inhibitors in solid organ transplant recipients with metastatic cutaneous squamous cell carcinoma. Oncologist (2021) 26(2):133−8. doi: 10.1002/onco.13539
15. Delyon J, Zuber J, Dorent R, Poujol-Robert A, Peraldi MN, Anglicheau D, et al. Immune checkpoint inhibitors in transplantation-a case series and comprehensive review of current knowledge. Transplantation (2021) 105(1):67−78. doi: 10.1097/TP.0000000000003292
16. Nguyen LS, Ortuno S, Lebrun-Vignes B, Johnson DB, Moslehi JJ, Hertig A, et al. Transplant rejections associated with immune checkpoint inhibitors: A pharmacovigilance study and systematic literature review. Eur J Cancer (2021) 148:36−47. doi: 10.1016/j.ejca.2021.01.038
17. Portuguese AJ, Tykodi SS, Blosser CD, Gooley TA, Thompson JA, Hall ET. Immune checkpoint inhibitor use in solid organ transplant recipients: A systematic review. J Natl Compr Canc Netw avr (2022) 20(4):406–416.e11. doi: 10.6004/jnccn.2022.7009
18. Farasat S, Yu SS, Neel VA, Nehal KS, Lardaro T, Mihm MC, et al. A new American joint committee on cancer staging system for cutaneous squamous cell carcinoma: Creation and rationale for inclusion of tumor (T) characteristics. J Am Acad Dermatol (2011) 64(6):1051−9. doi: 10.1016/j.jaad.2010.08.033
19. Seymour L, Bogaerts J, Perrone A, Ford R, Schwartz LH, Mandrekar S, et al. iRECIST: guidelines for response criteria for use in trials testing immunotherapeutics. Lancet Oncol (2017) 18(3):e143−52. doi: 10.1016/S1470-2045(17)30074-8
20. Rischin D, Migden MR, Lim AM, Schmults CD, Khushalani NI, Hughes BGM, et al. Phase 2 study of cemiplimab in patients with metastatic cutaneous squamous cell carcinoma: primary analysis of fixed-dosing, long-term outcome of weight-based dosing. J Immunother Canc (2020) 8(1):e000775. doi: 10.1136/jitc-2020-000775
21. Knoll GA, Kokolo MB, Mallick R, Beck A, Buenaventura CD, Ducharme R, et al. Effect of sirolimus on malignancy and survival after kidney transplantation: systematic review and meta-analysis of individual patient data. BMJ (2014) 349(nov24 1):g6679−g6679. doi: 10.1136/bmj.g6679
22. Carroll RP, Boyer M, Gebski V, Hockley B, Johnston JK, Kireta S, et al. Immune checkpoint inhibitors in kidney transplant recipients: a multicentre, single-arm, phase 1 study. Lancet Oncol (2022) 23(8):1078−86. doi: 10.1016/S1470-2045(22)00368-0
23. Lipson E.J. Tacrolimus, nivolumab, and ipilimumab in treating kidney transplant recipients with selected unresectable or metastatic cancers. Clinical Trials (2022) Available at: https://clinicaltrials.gov/ct2/show/NCT03816332
24. Hanna G.J. Cemiplimab in AlloSCT/SOT Recipients With CSCC (CONTRAC). Clinical Trials (2022) Available at: https://clinicaltrials.gov/ct2/show/NCT04339062
25. Geidel G, Rünger A, Schneider SW, Gebhardt C. Value of cemiplimab in progressive metastatic cutaneous squamous cell carcinoma after kidney transplantation: a case report. J Eur Acad Dermatol Venereol (2022) 36(S1):49−52. doi: 10.1111/jdv.17732
26. Hurkmans DP, Verhoeven JGHP, de Leur K, Boer K, Joosse A, Baan CC, et al. Donor-derived cell-free DNA detects kidney transplant rejection during nivolumab treatment. J Immunother Canc (2019) 7(1):182. doi: 10.1186/s40425-019-0653-6
27. Danger R, Chesneau M, Paul C, Guérif P, Durand M, Newell KA, et al. A composite score associated with spontaneous operational tolerance in kidney transplant recipients. Kidney Int (2017) 91(6):1473−81. doi: 10.1016/j.kint.2016.12.020
28. Yap M, Boeffard F, Clave E, Pallier A, Danger R, Giral M, et al. Expansion of highly differentiated cytotoxic terminally differentiated effector memory CD8 + T cells in a subset of clinically stable kidney transplant recipients: A potential marker for late graft dysfunction. J Am Soc Nephrol (2014) 25(8):1856−68. doi: 10.1681/ASN.2013080848
29. Cherukuri A, Salama AD, Mehta R, Mohib K, Zheng L, Magee C, et al. Transitional b cell cytokines predict renal allograft outcomes. Sci Transl Med (2021) 13(582):eabe4929. doi: 10.1126/scitranslmed.abe4929
30. Jacquemont L, Tilly G, Yap M, Doan-Ngoc TM, Danger R, Guérif P, et al. Terminally differentiated effector memory CD8 + T cells identify kidney transplant recipients at high risk of graft failure. J Am Soc Nephrol (2020) 31(4):876−91. doi: 10.1681/ASN.2019080847
31. Chesneau M, Michel L, Dugast E, Chenouard A, Baron D, Pallier A, et al. Tolerant kidney transplant patients produce b cells with regulatory properties. J Am Soc Nephrol (2015) 26(10):2588−98. doi: 10.1681/ASN.2014040404
Keywords: cemiplimab, kidney transplant recipients, cutaneous squamous cell carcinoma, immune checkpoint inhibitors, rejection
Citation: Van Meerhaeghe T, Baurain JF, Bechter O, Orte Cano C, Del Marmol V, Devresse A, Doubel P, Hanssens M, Hellemans R, Lienard D, Rutten A, Sprangers B, Le Moine A and Aspeslagh S (2022) Cemiplimab for advanced cutaneous squamous cell carcinoma in kidney transplant recipients. Front. Nephrol. 2:1041819. doi: 10.3389/fneph.2022.1041819
Received: 11 September 2022; Accepted: 06 October 2022;
Published: 31 October 2022.
Edited by:
Camillo Porta, University of Bari Aldo Moro, ItalyReviewed by:
Marta Pirovano, University of Milan, ItalyCopyright © 2022 Van Meerhaeghe, Baurain, Bechter, Orte Cano, Del Marmol, Devresse, Doubel, Hanssens, Hellemans, Lienard, Rutten, Sprangers, Le Moine and Aspeslagh. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: T. Van Meerhaeghe, dGVzcy52YW4ubWVlcmhhZWdoZUBlcmFzbWUudWxiLmFjLmJl
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.