 Xinyin Liu
Xinyin Liu Xiaoran Wang
Xiaoran Wang Hongzhen Ma3†
Hongzhen Ma3† Wen Zhang
Wen Zhang
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Nephrol. , 09 November 2022
Sec. Clinical Research in Nephrology
Volume 2 - 2022 | https://doi.org/10.3389/fneph.2022.1006506
This article is part of the Research Topic Reviews in Frontiers in Nephrology View all 18 articles
Chronic kidney disease (CKD) is associated with high incidence, low awareness, and high disability rates among the population. Moreover, the disease significantly affects the physical and mental health of patients. Approximately 25% of patients with CKD develop end-stage renal disease (ESRD) within 20 years of diagnosis and have to rely on renal replacement therapy, which is associated with high mortality, heavy economic burden, and symptoms including fatigue, pain, insomnia, uremia pruritus, and restless leg syndrome. Currently, the means to delay the progress of CKD are insufficient; therefore, developing strategies for delaying CKD progression has important practical implications. In recent years, more and more people are accepting the traditional Chinese medical technique “acupuncture.” Acupuncture has been shown to improve the uncomfortable symptoms of various diseases through stimulation (needling, medicinal moxibustion, infrared radiation, and acupressure) of acupoints. Its application has been known for thousands of years, and its safety and efficacy have been verified. As a convenient and inexpensive complementary therapy for CKD, acupuncture has recently been gaining interest among clinicians and scientists. Nevertheless, although clinical trials and meta-analysis findings have demonstrated the efficacy of acupuncture in reducing albuminuria, improving glomerular filtration rate, relieving symptoms, and improving the quality of life of patients with CKD, the underlying mechanisms involved are still not completely understood. Few studies explored the correlation between acupuncture and renal pathological diagnosis. The aim of this study was to conduct a literature review summarizing the currently known mechanisms by which acupuncture could delay the progress of CKD and improve symptoms in patients with ESRD. This review help provide a theoretical basis for further research regarding the influence of acupuncture on renal pathology in patients with CKD, as well as the differences between specific therapeutic mechanisms of acupuncture in different renal pathological diagnosis. The evidence in this review indicates that acupuncture may produce marked effects on blocking and reversing the critical risk factors of CKD progression (e.g., hyperglycemia, hypertension, hyperlipidemia, obesity, aging, and anemia) to improve the survival of patients with CKD via mechanisms including oxidative stress inhibition, reducing inflammatory effects, improving hemodynamics, maintaining podocyte structure, and increasing energy metabolism.
Chronic kidney disease (CKD) refers to abnormal renal structure or function caused by various reasons or an unexplained decrease in the glomerular filtration rate (GFR<60 mL/min) for >3 months (1). In 2012, the Lancet published the first nationwide cross-sectional survey of CKD in China, showing that there were approximately 120 million patients with CKD, which had a 10.8% prevalence rate among adults (2). According to the five insights of the 2019 Global Disease Burden Study, exposure rate to the risk factors of injury and disability caused by CKD has also increased, second only to hypertension, hyperglycemia, obesity, environmental pollution, and social factors (3). Furthermore, approximately 25% of patients with CKD develop end-stage renal disease (ESRD) within 20 years of diagnosis (4). Patients with ESRD have a high mortality rate and require long-term maintenance dialysis, which incurs substantial medical costs and places a heavy economic burden on families, society, and the country. Currently, the etiology and pathogenesis of CKD are unclear, and there is a lack of effective treatments.
The main treatments of CKD target preventing ESRD to reduce mortality. Modern medicine has made several attempts to treat this disease, including dealing with its complications (e.g., renal hypertension, hyperlipidemia, proteinuria) using glucocorticoids, cytotoxic drugs, immunosuppressants, and biological agents based on individual patient characteristics and renal pathology (5). However, there are currently no ideal treatment schemes, and this disease has become a significant public health concern worldwide. Hence, it is necessary to explore novel methods for its prevention and treatment.
The considerable symptomatic burden associated with CKD greatly affects the quality of life of patients. Common symptoms include fatigue, pain, sleep disorders, restless leg syndrome (RLS), and chronic pruritus, although with considerable variations related to symptom definition, period of prevalence, and levels of severity (6–8). The first-line intervention of pain and pruritus is mainly medication, but their use and management have limitations, and nonpharmacologic approaches have therefore attracted attention. For example, replacement therapy has been shown to be feasible and effective against fatigue and sleep disorders (9).
Acupuncture is an essential component of traditional Chinese medicine (TCM) and substitute auxiliary therapies. According to the TCM theory, there are 12 main and collateral channels on the human body surface and 361 classical acupuncture points on these channels (10). Acupuncture can adjust the qi and blood of the meridians and viscera, improve various uncomfortable symptoms, and treat diseases by stimulating different acupoints. For the purpose of this review, acupuncture is considered as a generalized concept, including procedures involving insertion of fine needles into the skin or deeper tissues at specific locations (acupoints) of the body which are then manipulated manually, electrically, or with combined moxibustion; pressure on the acupoints with fingers; or application of infrared radiation on acupoints instead of fine needles.
Acupuncture has been proven to reduce urine protein levels and improve estimated GFR (11–18). Meanwhile, some studies also focused on the effects of acupuncture on hemodynamics (19) and renal interstitial fibrosis (20–24). Factors such as hyperglycemia, hypertension, hyperlipidemia, obesity, pain, aging, and anemia have a profound relationship with CKD progression (25). Considering that acupuncture can be effective in improving these aspects (26–30), it is believed that acupuncture may improve the prognosis of patients with CKD by controlling the above risk factors. In addition, acupuncture has the potential to alleviate various ESRD-related symptoms (e.g., pain, uremic pruritus [UP], RLS, and sleep disorders) (31–33). The therapeutic effect of acupuncture on CKD cannot be explained entirely by the bidirectional regulation of nerves, which is generally considered the main effective mechanism (34). However, a number of large-scale, randomized controlled clinical trials are still needed to clarify the indications of acupuncture before it can be used widely in clinical practice, especially as the mechanisms by which acupuncture affects disease mechanisms can be quite complex.
The safety of acupuncture has been widely confirmed in clinical practice. A prospective observational study on acupuncture for chronic pain in Germany included 454920 patients, of whom more than 30% were over 60 years old, and reported mild side-effects (pain, hematoma, and bleeding) in 7.9% of patients. Only 13 patients suffered serious adverse events, including pneumothorax, hypertension, hypotension, asthma attacks, and aggravation of suicidal thoughts (35). The safety of acupuncture for CKD has also been proved. A systematic review of 55 randomized controlled trials showed that the most common side-effects associated with needling therapy and acupressure therapy were elbow soreness and bleeding and intradialytic hypotension and dizziness, respectively, and that no adverse effects were reported for moxibustion therapy (36). Some researchers believe that some side-effects of acupuncture are due to malpractice by acupuncturists, which can be avoided by strengthening training (37). The World Health Organization recommends at least 1568 hours of training to meet the basic requirements of acupuncture practitioners of ensuring clinical efficacy and patient safety (38).
However, although acupuncture is one of the safest replacement therapies, especially when provided by well-trained acupuncturists, to the best of our knowledge, the recent progress related to the use of acupuncture in treating CKD has not been summarized. This review aimed to assess the beneficial effects and current known mechanisms of acupuncture with regard to CKD and ESRD-related symptoms. We believe that acupuncture may have a significant impact on the associated risk factors for blocking or reversing the progress of CKD and alleviating the discomfort of patients, thus improving their prognosis.
We designed our literature review to include basic and clinical studies that addressed the effects and mechanisms underlying the effects of acupuncture treatment in CKD. The PubMed databases were queried for full-text studies published between January 1, 2000 and August 31, 2022 in English or Chinese using the following keywords: “acupuncture” and “kidney”.
Inclusion criteria:
1. Description of specific mechanisms of how the acupuncture treatment exerted its effects
2. Exclusive use of acupuncture to treat CKD and related symptoms
3. Related studies cited in these articles
Initially, 747 published articles were identified, of which only 46 articles matched the inclusion criteria and were reviewed. We excluded one withdrawn article, two articles unable to find partial results of changes in renal function, and two articles with imprecise test design that does not control variables. The references of the remaining 41 articles identified an additional 6 articles that also matched our inclusion criteria, which were also included in the final review, resulting in 47 articles in total (Table 1). The studies included randomized controlled animal experiments and clinical experiments and involved kidney injury. Additionally, we conducted a supplementary literature search on hyperlipidemia, which was not identified in the previous search but has been proved to be an important independent risk factor for the development of CKD.

Table 1 Summary of studies in chronic renal injury, and renal physiological function and ESRD-related symptoms (2000-2022).
The 47 studies included in this review employed the use of Sprague Dawley rats, Wistar rats, Golden Syrian hamsters, New Zealand white rabbits, which were used to model ischemic nephropathy, diabetic nephropathy (DN), or hypertensive nephropathy. According to the risk factors of CKD, including hyperglycemia, hypertension, hyperlipidemia, obesity, aging, and anemia (25), we classified and summarized the potential mechanisms of action of the beneficial effects of acupuncture on the progress of CKD (Figure 1) and the common symptoms of ESRD.
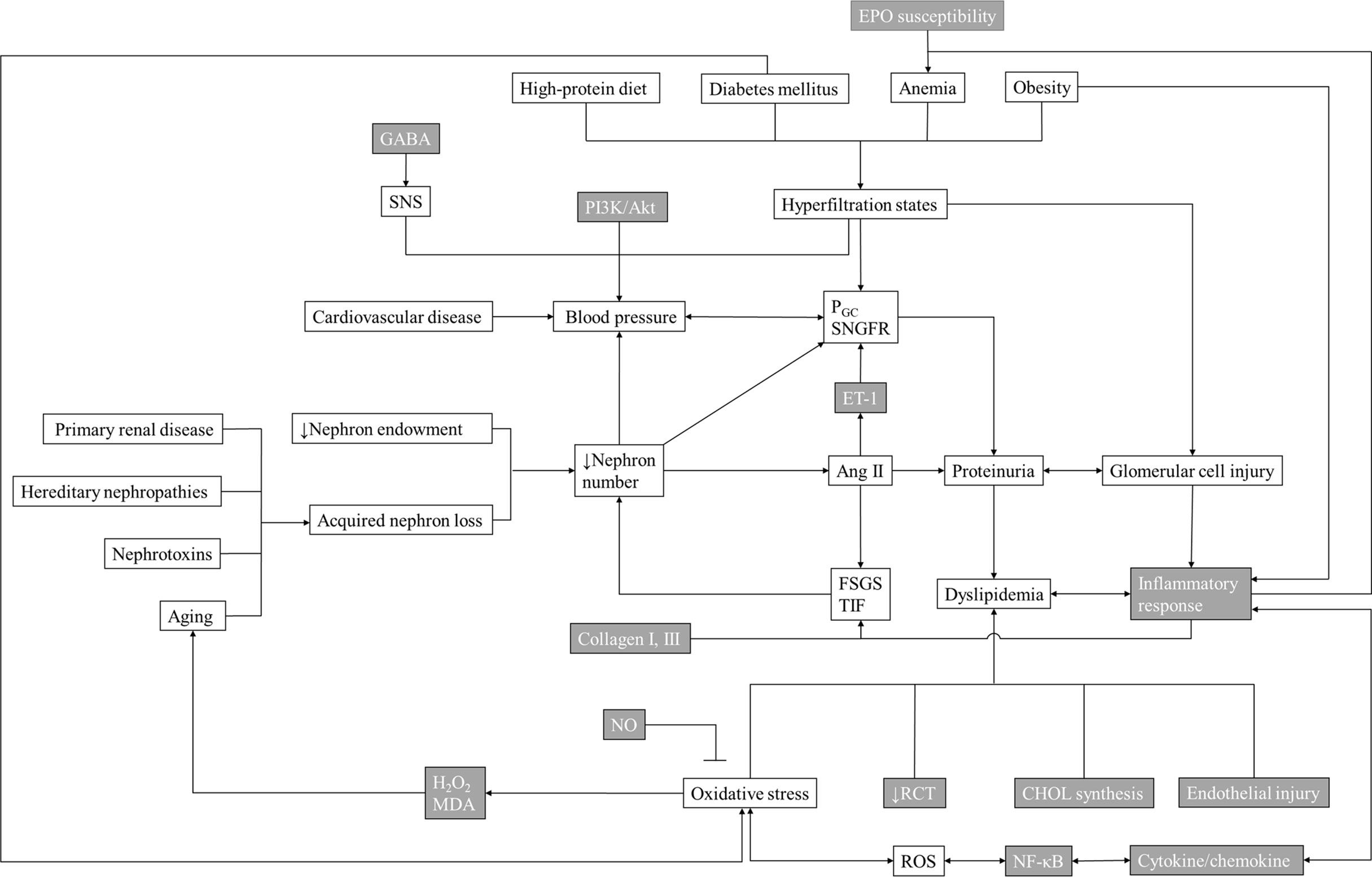
Figure 1 Mechanisms Underlying the Effects of Acupuncture Therapy in Chronic Kidney Disease. The gray grids are the known possible main mechanism/target/downstream product of acupuncture in treating chronic kidney disease. EPO, erythropoietin; GABA, γ-aminobutyric acid; SNS, sympathetic nervous system; PGC, proliferator γ coactivator; SNGFR, single nephron glomerular filtration rate; ET-1, endothelin-1; Ang II, angiotensin II; FSGS, focal segmental glomerulosclerosis; TIF, tubulointerstitial fibrosis; MDA, malondialdehyde; RCT, reverse cholesterol transport; CHOL, cholesterol; NF-κb, nuclear factor-kappa B; ROS, reactive oxygen species.
DN is rapidly becoming the most common cause of ESRD worldwide (25). The pathogenesis of DN is complex and involves various mechanisms, resulting in poor therapeutic outcomes (71). It is generally accepted that the developmental mechanism of DN results from abnormal homeostasis (72). There are many critical links in the progression of DN, e.g., oxidative stress, inflammation, and podocyte structural damage. A reciprocal relationship exists between inflammation and oxidative stress (73, 74). Various Chinese meta-analyses point out that acupuncture can reduce the urine protein, serum creatinine, fasting blood glucose, postprandial blood glucose, glycosylated hemoglobin, total cholesterol, and triglycerides of patients with DN, as well as enhance the efficacy when combined with conventional drugs (26, 75, 76).
The increase in reactive oxygen species (ROS) caused by blood glucose is at the core of the pathogenesis of DN. Hyperglycemia-induced oxidative stress is believed to cause both local and systemic inflammation (77).
Forkhead transcription factor O1 (FOXO1) overexpression reduced ROS in rat mesangial cells and protected mitochondrial function by activating peroxisome proliferator γ coactivator 1 α (PGC-1α) (78). A study on rats with DN showed that electroacupuncture (EA) increased the levels of FOXO1 and PGC-1α in kidney tissue, thus improving renal function (39).
Nitric oxide synthase (NOS), superoxide dismutase (SOD), and malondialdehyde (MDA) are essential indicators of oxidative stress. Reactive species may also be produced enzymatically by uncoupled NOS (79). SOD is an antioxidant that can effectively remove superoxide anions and protect cells from oxidative damage (80). MDA is a metabolite of lipid peroxidation, which can reflect the level of free radicals in tissues and lipid peroxidation caused by free radicals, and indirectly reflects cell damage (40). A study on rats with DN showed that acupuncture and moxibustion have synergistic effects on antioxidant stress, which may be related to their function in downregulating the expression of MDA and upregulating the expressions of NOS and SOD in the kidney (40). Another trial revealed that EA could improve renal function and reduce microcirculation disorders in early DN by up-regulating the levels of serum endothelial NOS and NO (41).
Oxidative stress can directly damage podocytes, mesangial cells, and endothelial cells, resulting in proteinuria and tubulointerstitial fibrosis. One study suggested that EA may effectively alleviate renal injury in rats with DN by promoting renal autophagy. The number of podocytes in rats with DN treated with EA was more than that in the untreated group, while the levels of 24-h urine protein, blood urea nitrogen, and serum creatinine were lower (42).
Nuclear factor 2 related factor 2 (Nrf2) regulates oxidative stress in the antioxidant response system by controlling the expression of more than 250 genes (72, 79). A study on rabbits with acute kidney injury revealed that EA treatment enhanced the expression of phosphorylated Akt, heme oxygenase-1 protein, Nrf2 total protein, and nuclear protein to resist oxidative stress (81).
Continuous inflammation of the circulatory system and renal tissue is the fundamental pathological basis for the development of DN (82). Inflammatory factors such as interleukin-6 (IL-6), tumor necrosis factor-α (TNF-α), transforming growth factor-β, IL-1, and IL-18 are elevated in the blood and have been related to the occurrence and progression of DN (83, 84). Several studies have shown that acupuncture can improve insulin resistance by reducing serum IL-6, IL-8, and IL-1β levels, which might help protect islet B cell function (43, 85).
Increasing evidence has shown the central role of Janus kinase (JAK)-signal transducer and activator of transcription (STAT) pathway (71) in DN pathogenesis. JAK and STAT subtypes expressed on the renal tubulointerstitial increase along with the development of DN and negatively correlated with the estimated GFR. Nuclear factor-kappa B (NF-κB) is a key transcription factor in the inflammatory process of DN and is activated by the JAK-STAT pathway. NF-κB regulates inflammatory cytokines and chemokines, e.g., monocyte chemoattractant protein-1 (MCP-1) and cell adhesion proteins, leading to kidney damage. A study on diabetic mice revealed that acupuncture could suppress the inflammatory response of DN through the NF-κB-related pathway (43). Zhang et al. designed a series of multicenter, randomized, and blinded studies, showing that the needling method of harmonizing the spleen and stomach on patients with early DN might inhibit the NF-κB-related pathway by inhibiting the expression of MCP-1, which can improve renal blood flow and GFR, decrease urinary albumin secretion, protect the glomerulus and renal tubules, thus reducing the inflammatory levels and delaying the progress of DN (44, 45).
The kidney requires a large number of mitochondria to provide the energy to remove waste from the blood and regulate fluid and electrolyte balance. Mitochondrial dysfunction leads to a decrease in ATP production, alterations in cellular functions and structure, and the loss of renal function (86, 87). Figueiredo et al. (88) found that in non-exercised hyperglycemic rats, under the same dose of anesthesia (ketamine, 90 mg/kg body weight), the lactic acid concentration and blood glucose level of the experimental group treated with EA decreased significantly, indicating that acupuncture might reduce blood glucose by enhancing aerobic metabolism and increasing ATP output.
NAD-dependent isocitrate dehydrogenase is present in the mitochondria. It is a momentous rate-limiting enzyme of the tricarboxylic acid cycle (TCA) and plays a crucial role in energy production and anabolism. As the most important source of adenosine triphosphate (ATP), TCA is closely related to the occurrence of nephropathy. Two other studies reached similar conclusions; after needling the “Taixi” (KI 3) point, increased expression of NAD-dependent isocitrate dehydrogenase and quinone reductase was observed in rat kidney tissue, suggesting that targeted acupuncture improves energy metabolism (46, 47).
Metabonomics has also been applied to study EA’s effects on renal metabolism. Alanine is a characteristic metabolite in the kidney, an important energy source for human beings, and is involved in lymphocyte regeneration, thus maintaining immune homeostasis (89). Threonine participates in energy metabolism and promotes the cellular immune system’s defense function (89). Research suggested that the levels of the two metabolites in the kidneys of mice with premature ovarian failure were elevated, and the levels were down-regulated after electroacupuncture stimulation of “Sanyinjiao” (SP6) and “Guanyuan” (CV4), close to the level of healthy mice (90). Another study revealed that the effect of EA on the abnormal increase of metabolites might suggest that it can regulate the disordered amino acid metabolism, thereby improving energy metabolism and regulating the kidney’s immune function (91).
Podocytes are important functional cells in the glomerulus that cannot regenerate when they suffer from injury. Their damage and apoptosis could result in the destruction of the glomerular filtration membrane and induce DN (92). Podocalyxin is one of the main structures responsible for the negative charge on the glomerular membrane (93). CD2-associated protein (CD2AP) is a transmembrane protein that interacts with nephrin to maintain cytoskeleton and slit diaphragm function. Damage to CD2AP leads to the destruction of the podocyte skeleton and marked proteinuria (94). Desmin also maintains the mechanical stability of podocytes to enable morphological changes on the tensile glomerular capillary wall (95). Zhang et al. found that acupuncture partly prevented DN rats from podocyte foot process effacement—which exhibited fusion, complete destruction, or disappearance—and thick glomerular basement membrane. It also upregulates nephrin expression, CD2AP, and podocalyxin but downregulates desmin, thus protecting and maintaining podocytes’ physical and chemical structure (27).
The transient receptor potential-6 channel (TRPC6) is an integral player in the calcium processing in podocytes and in the maintenance of their cellular structure (96, 97). Möller et al. reported that overexpression of TRPC6 in healthy mice leads to the restructuring of the podocyte actin cytoskeleton and alterations in calcium flux, which causes proteinuria (97). Hyperglycemia and elevation in angiotensin II (Ang II) levels are sufficient to cause overexpression of TRPC6, resulting in increased calcium influx and eventual podocyte dysfunction and death (98). Li et al. proved that EA preconditioning could alleviate renal injury in hyperglycemic mice by reducing renal TRPC6 and nephrin expression and inhibiting podocyte activation (48, 49).
Hypertension is considered a result of renal damage and a significant contributor to the progression of CKD (25). Approximately 80–90% of patients with CKD have renal hypertension, which accelerates renal dysfunction (99, 100). Therefore, controlling blood pressure is critical in preventing progressive deterioration of renal function. Renal hypertension is difficult to cure and usually requires the combined use of several antihypertensive drugs with possible non-compliance. The pathological mechanism of renal hypertension is complex, including activation of the sympathetic nervous system (SNS) and renin-angiotensin-aldosterone system (RAAS), oxidative stress, increased endothelin-1 (ET-1), and inflammation. Acupuncture has been shown to have certain clinical effects on renal hypertension (50). A network meta-analysis on acupuncture therapy for essential hypertension, which included 31 trials with 2,649 patients, revealed that acupuncture might have similar effects as common medication. However, the quality of this evidence is not high (101).
ET-1 is a crucial molecule that regulates renal hypertension, and its release is induced by the combination of Ang II and angiotensin II type 1 receptor (AT1R). ET-1 combines with endothelin-1 type A receptor (ETAR), which causes marked renal vasoconstriction (102). A previous study revealed that Ang II and ET-1 receptor blockers could reduce blood pressure in animal models and patients (103). Acupuncture reduces blood pressure by lowering the ET-1 level (104, 105). Additionally, long-term EA blocks the AT1R-ET-1-ETAR pathway by inhibiting the expression of AT1R and ETAR (106). Therefore, it is believed that the AT1R-ET-1-ETAR pathway may be a target for acupuncture treatment of renal hypertension.
The RAAS is a vital blood pressure regulation system that maintains the homeostasis of water and electrolytes in the internal environment. There are two main pathways. 1) The angiotensin-converting enzyme/Ang II (ACE/Ang II) pathway constricts blood vessels and promotes tissue proliferation and remodeling (107). 2) The ACE2/Ang-(1-7) pathway has the opposite effects (108). Moreover, Liu et al. found that acupuncture and moxibustion showed good antihypertensive effects by reducing the content of Ang II and atomic layer deposition in the plasma of hypertensive rats (109).
The development of hypertension partly depends on the increased sympathetic outflow and impaired baroreflex function. The nucleus tractus solitarii (NTS) is the main integration center regulating the autonomic reflex and sympathetic outflow. In the NTS, inhibition of γ-aminobutyric acid (GABA) is essential for pressure reflection signal processing. Evidence shows that an increase in GABA inhibition leads to hypertension (110–112). Therefore, neuronal activity in the NTS is a significant target for acupuncture to regulate the sympathetic excitatory reflex function. A study revealed that EA could reduce sympathetic activity and significantly inhibit the sympathetic excitatory reflex in rats, which may be achieved by regulating functional GABA (113). Moreover, acupuncture reduced local renal sympathetic nerve activity by inhibiting the extracellular regulated protein kinase ½-MAPK pathway to lower blood pressure (51). Another study also verified the relationship between acupuncture and renal sympathetic activity (52).
Renal hypertension induced by ischemic nephropathy is affected by oxidative stress mechanisms involving molecules such as NOS and heme oxygenase (HO-1/2) (114–116). In one study, EA was shown to prevent the reduction of endothelial NOS and nitric NOS levels associated with hypertension (53).
Inducible NOS (iNOS) and HO-1/2 expression is involved in the secretion of insulin-like growth factor-I (IGF-I) in MCF-7 cells (117). IGF-I has been proved to be related to proliferation, differentiation, survival, apoptosis, and cell protection related to oxidative stress (118). Another study showed that EA can reduce the levels of iNOS and HO-1/2 and upregulate IGF-1 levels, thus reducing glomerulosclerosis and renal interstitial fibrosis as well as blood pressure in rats with renal failure (54). Additionally, the possibility of acupuncture being able to directly affect the process of renal fibrosis in hypertensive rats has also been suggested (55, 56).
Recent studies have shown that hyperlipidemia and obesity are two adverse factors associated with the progression of CKD via different mechanisms. However, obese patients are typically at higher risk of hyperlipidemia (119). Obesity is associated with high glomerular filtration and other glomerular hemodynamic alterations, which may aggravate CKD progression (120, 121). Adipocytes produce various hormones and pro-inflammatory molecules, which may lead to progressive renal damage (122). According to the lipid nephrotoxicity hypothesis, hyperlipidemia can lead to inflammation, oxidative stress, and endogenous electrical stress (123).
A study on 1528 obese patients with hyperlipidemia treated with acupuncture suggested that acupuncture had dual effects on obesity and hyperlipidemia. The patients not only effectively lost weight (the total effective rate of the mild obesity group was 98.9%), but they also reduced their levels of total cholesterol, triglycerides, and low-density lipoprotein and improved their high-density lipoprotein (HDL) level (28). Some scholars believe that acupuncture combined with moxibustion reduces the adverse effects of hyperlipidemia and obesity better than acupuncture alone (124). Another study found that different acupoint combinations had different effects on reducing blood lipid levels. The “Quchi” (Li 11), “Zhongwan” (CV 12), and “Fenglong” (ST 40) points had a superior performance on blood lipid metabolism (125).
Nitric oxide (NO) is an endothelium-derived messenger molecule that alleviates oxidative stress. Several studies revealed that EA and moxibustion increase the level of NO to resist oxidative stress and that the effect of moxibustion is regulated by temperature (126–130). Transient receptor potential vanilloid subfamily 1 (TRPV1) is an essential molecular regulator that provides moxibustion with temperature dependence of its hypolipemic properties. There is a relationship between the cholesterol-lowering effect of moxibustion and the activation of TRPV1 (131).
Reverse cholesterol transport (RCT), which is partly mediated by ATP-binding cassette transporter A1 (ABCA1), is a significant physiological link that delays hyperlipidemia progression. ABCA1 regulates intracellular RCT and HDL production, thereby controlling lipid metabolism. As transcription factors, activated peroxisome proliferator-activated receptor (PPAR)-α and liver X receptor α (LXRα) enhance ABCA1 transcription activity (132, 133). Zou et al. believed that moxibustion upregulated PPARγ and scavenger receptor B1 (SR-B1) protein and gene expression in the liver to promote cholesterol reversal (134). HDL binds to SR-B1 and transports cholesterol to the liver for selective metabolism. Another research study found that EA stimulation of the “Fenglong” (ST 40) point contributed to increased expressions of ABCA1, PPARα, LXRα, and retinoid X receptor α messenger RNA, thus contributing to RCT, and somehow had a therapeutic effect on hyperlipidemia (135, 136).
ABCA1 dysfunction leads to excessive cholesterol ester accumulation as lipid droplets in macrophages, thereby contributing to foam cell formation (137). EA at the “Fenglong” (ST 40) point can prevent macrophage transformation into foam cells and increase cholesterol outflow rate in macrophages, thus preventing and reversing foam cell formation (138).
Sterol regulatory element binding protein-1C (SREBP-1C) is a transcription factor involved in the transcriptional regulation of the fatty acid synthase (FAS) gene that controls the synthesis of lipids from glucose in the liver (139). Recent research indicated that FAS could catalyze the de novo synthesis of fatty acids and impact liver physiology through signaling and energy storage (140). It is believed that acupuncture downregulates SREBP-1C and FAS to control the expression of key enzymes regulating cholesterol synthesis in the liver to prevent hyperlipidemia (141).
CKD is an inflammatory state that results in glomerular and tubular lesions and adversely affects lipid balance (142, 143). Several inflammatory markers have been associated with lipid levels (144). Some studies revealed that acupuncture could reduce intercellular cell adhesion molecule-1, MCP-1, TNF-α, IL-6, and IL-1γ, slowing the inflammatory process (145–147).
Adiponectin (ADPN) is the only adipocyte-specific protein negatively associated with obesity. It has anti-diabetic, antiatherosclerotic, anti-inflammatory, and antiangiogenic properties. Hand acupuncture and EA intervention positively affect hyperlipidemia by reducing blood fat content and upregulating serum HDL-C and ADPN levels in hyperlipidemic rats (148).
A longitudinal study among individuals without nephropathy found that the GFR decreases with age, indicating that nephron loss might be part of normal aging (149). Other studies have shown that proteinuria, CKD, and ESRD incidence rates increase with age (149–151). Acupuncture can delay the aging of the kidney tissue by suppressing oxidative stress and reducing apoptosis. An experiment suggested that the apoptosis rate of renal cells and the levels of hydrogen peroxide and malondialdehyde decreased after acupuncture in adult rats (29).
Renal anemia is one of the most common complications of CKD and affects the quality of life and survival time of patients with CKD (152). In a study of 131 patients with CKD, elevated hemoglobin levels were independently associated with reduced mortality (153). Renal anemia is usually caused by the hyposecretion of erythropoietin (EPO). EPO is a protein hormone synthesized by proximal convoluted tubular cells, essential for erythrocytes’ growth. Medical treatments sometimes show poor efficacy, including recombinant human erythropoietin and polysaccharide iron complexes (154). Therefore, there is an urgent need for supplemental therapies to improve the curative effect. One study found that acupoint injection could reduce the level of C-reactive protein, improve the micro-inflammatory state, and help reduce EPO dosage, which is better than the traditional injection method (30). Acupoint injection reduces costs and meets the requirements of patients’ health and the economy.
CKD and ESRD have attracted attention worldwide, and the number of patients on hemodialysis (HD) has increased dramatically. Patients on HD often have many painful complications, such as UP, RLS, insomnia, fatigue, sleep disorders, and hypotension. Acupuncture can alleviate these problems. A systematic review of randomized controlled trials showed that acupuncture had demonstrated efficacy in alleviating sleep disturbance, fatigue, and UP symptoms among patients with CKD (36).
Pain can be one of the most debilitating symptoms of CKD (155). Patients suffer several types of pain, including peripheral neuropathic pain, joint pain, autosomal dominant polycystic kidney disease (ADPKD)-related pain, and pain caused by renal biopsy. A multicenter, cross-sectional study evaluated the impact of pain on the quality of life of patients with ESRD on HD, with the results suggesting that pain significantly impacted their life quality (156). Pain management in patients with CKD is challenging. Non-opioid analgesia using acetaminophen, topical analgesics, and gabapentinoids is preferred, but cannot relieve pain to a great extent (155). Furthermore, the long-term use of non-steroidal, anti-inflammatory drugs poses a risk of liver and further kidney damage. A study on over 400,000 patients with ESRD showed that an opioid prescription was accepted by over half of them (157), even though opioid use is associated with an increased risk of altered mental status, falls, fractures, hospitalizations, and mortality, in a dose-dependent manner (158, 159).
Nevertheless, opioids play a central role in the analgesic mechanism, desensitizing peripheral nociceptors, reducing pro-inflammatory cytokines, and activating the descending inhibitory system (160). A previous study showed that high- and low EA frequencies could relieve heat, mechanical, and spontaneous pain by regulating μ and δ opioid receptors (161). This shows that acupuncture has the prospect of reducing or even replacing opioid use.
Besides, the role of acupuncture in the treatment of chronic lower back pain has been well proven and addressed in the Clinical Practice Guideline of the American College of Physicians (162). It is also effective against chronic lower back pain caused by polycystic kidney disease (163). Unfortunately, at present, there is a lack of large-scale studies on verifying the efficacy of acupuncture and moxibustion on lower back pain in other types of CKD.
Chronic pruritus associated with ESRD is one of the most important causes of systemic pruritus (164). UP is an unpleasant and painful condition causing the desire to scratch, invalidating the skin’s protective barrier, and affecting patients’ health-related quality of life (HR-QOL) (31). A large multicenter study of 18801 patients on HD showed that 42% of them had UP (165). The pathogenesis of UP may involve inflammatory states, such as increased levels of pro-inflammatory cytokines (IL-6, IL-2, and TNF-α), immune changes, and neuropathy. Current drug treatment regimens (e.g., antihistamines, bupropion, and tacrolimus) often lead to many side-effects, including sleepiness, nausea, vomiting, and epilepsy. Patients are unlikely to extract many benefits, and the symptoms usually recur after drug discontinuation (164). Acupuncture, an economical and safe complementary therapy, has obvious advantages in treating pruritus, with one meta-analysis even suggesting the potential of acupuncture to treat UP (166). Studies have shown that one of the mechanisms of acupuncture in treating chronic pruritus is regulating inflammatory cytokines, including reducing IL-4 and IL-2 levels in serum, enhancing the anti-inflammatory cytokine IL-10, and inhibiting the level of the inflammatory cytokine TNF-α (the acupoints are all “Quchi” (LI11), “Hegu” (LI4), “Xuehai” (SP10), and “Yinlingquan” (SP9)) (167–169). Another animal study found that EA increased the serum levels of interferon-γ of mice with atopic dermatitis, with no significant change in IL-4 levels (the acupoints are “Quchi” (LI11) and “Neiguan” (PC6)) (170). This finding suggests that different acupoints lead to different effects.
Karjalian et al. conducted a randomized, double-blind, pre- and post-control clinical trial among 90 patients on HD and found that acupoint pressing could effectively reduce pruritus in patients on HD (31). Four other randomized controlled trials showed that acupuncture, acupoint pressing, transcutaneous acupoint electrical stimulation, and auricular finger pressing could reduce UP symptoms (57–59, 171). Yi et al. believed this effect could continue after the treatment course (57).
RLS is a common chronic sensorimotor disorder characterized by a strong demand to move the legs during rest and bedtime. The development of this disease in patients undergoing HD is progressive (32). The prevalence among European and American adults varies from 7% to 10% (172, 173). Further, the prevalence of RLS has been reported to increase with age (174). RLS affects sleep quality and leads to dysfunction of emotion, cognition, energy, and other daily activities. RLS is associated with an increased risk of cardiovascular disease, osteoporosis, musculoskeletal pain, and mortality (175–177). A single-center, single-blinded, randomized controlled study attempted to treat 60 HD patients with RLS by irradiating lower limb acupoints with near-infrared light, but the symptoms of RLS recurred after irradiation was stopped (32). The mechanism was unknown, and the effects might have been related to the selection of acupoints, treatment cycle, and treatment mode, which require further study.
Sleep disorders in patients on HD can lead to psychosocial function and interpersonal relationship disorders and reduce their HR-QOL (60). More than 85% of patients on HD experience serious sleep problems (178). Zahra et al. and Shariati et al. found that acupoint pressing positively affects sleep quality in patients on HD, but the specific mechanism is still unknown (60, 61).
Acupuncture has been proved to have a significant effect on sleep disorders. Various meta-analyses, which included thousands of patients each, suggested that acupuncture could improve the sleep quality of patients with primary insomnia and patients with insomnia-related primary diseases and conditions (stroke, ESRD, perimenopause, pregnancy, and mental illness) of all ages, with few and mild adverse reactions (33, 179–182). However, because most of the included studies were heterogeneous and the sample size of each experiment was small, and there are few studies related to ESRD, it is still necessary to design randomized controlled trials with larger sample sizes to prove the essential of acupuncture to treat sleep disorders in patients on HD.
HR-QOL is a measure of the value assigned to duration of life as modified by impairments, functional states, perceptions and opportunities, as influenced by disease, injury, treatment and policy (183). Due to the progress of ESRD, the lifestyle restrictions and changes imputed to HD usually lead to fatigue, depression, anxiety, which have a profound impact on HR-QOL. The mental health of elderly patients is an especially serious problem (184). Mid- and long-term fatigue may even increase the risk of cardiovascular events and is associated with higher mortality (185). The clinical trials of this subsection were evaluated through the following questionnaires: Pittsburgh Sleep Quality Index, Piper Fatigue Scale; Visual Analog Scale, Kidney Disease Quality of Life-Short Form, a questionnaire authenticated and approved by the World Health Organization and Patient-Reported Outcomes Measurement Information System. Two studies showed that acupoint pressing could improve the fatigue state of HD patients (62, 63), and several randomized controlled studies found that moxibustion, acupressure, transcutaneous electrical acupoint stimulation, and acupuncture had positive impacts on aspects such as physical functions, general health, and vitality (64–69). However, in 2018, a study on living conditions of 101 HD patients who received short-term acupuncture/massage suggested that although the original Patient-Reported Outcomes Measurement Information System psychological scores of patients improved, the improvement was not significant, and might have been related to the sample capacity and treatment duration (70).
CKD is a significant public health problem worldwide and is characterized by a high incidence rate and complex pathogenesis. The clinical treatment scheme needs to be improved urgently, as currently the main clinical therapeutic strategy is to delay the progress of CKD, which mostly relies on medication. According to Kidney Disease Improving Global Outcome (KDIGO) guidelines, dealing with the complications of CKD (e.g. renal hypertension, hyperlipidemia, proteinuria) is essential, and the use of angiotensin-converting enzyme inhibitors, angiotensin receptor antagonists, and statins is common (5). Different medication schemes, including glucocorticoids, cytotoxic drugs, immunosuppressants, and biological agents are used to treat patients with CKD after assessing their renal pathologies and personal conditions (5). Moreover, if the kidney damage is secondary to other basic diseases, such as diabetes, it is necessary to control the primary disease (186). However, an ideal treatment plan has not yet been found, and the drugs used are usually accompanied by several side-effects, including digestive tract reaction, obesity, liver and kidney damage, bone marrow suppression, and reproductive damage; furthermore, the therapeutic effects may take weeks to months to manifest, which often leads to intolerance (187). About 25% of patients with CKD will eventually progress to ESRD within 20 years of diagnosis and need renal replacement therapy (4).
The evidence of this review reveals several beneficial effects of acupuncture on CKD and ESRD-related symptoms, and a summary of studies on acupuncture therapy in chronic renal injury, renal physiological function and ESRD-related symptoms is presented in Table 1. It is believed that acupuncture may have a significant impact on the risk nodes of the progress of CKD through multiple pathways, so as to improve the prognosis of patients with CKD. This is mainly realized through the following mechanisms: 1. reduced inflammatory reactions and protection of podocytes, mesangial cells, and endothelial cells from antioxidant stress; 2. delaying glomerular and tubular lesions by downregulating inflammatory factors to regulate relevant signal pathways, including NF-κB-related pathways; 3. reducing podocyte apoptosis and protecting the glomerular filtration membrane by reducing renal TRPC6 levels and maintaining podocyte structural proteins; 4. improving glomerular hemodynamics through blood pressure regulation systems (SNS, RAAS, etc.); 5. improving energy metabolism to regulate renal immune function via regulating enzymes involved in aerobic metabolism in mitochondria. The major mechanisms by which acupuncture can relieve ESRD-related symptoms are: 1. activating the descent inhibition system to relieve pain by regulating the release of bioactive chemicals, especially opioids; 2. regulating inflammatory cytokines to relieve chronic pruritus.
This review fully illustrates the advantages of acupuncture in treating CKD. First, acupuncture can act in cooperation with drug therapy to improve its the curative effects (18). Second, the potential mechanisms by which acupuncture may help in treating CKD are diverse; compared with single target therapy, acupuncture improves CKD prognosis through various pathways. Third, acupuncture is a simple supplementary therapy with mild side-effects, which prevent patients from taking additional drugs, especially opioids (161), to improve patient compliance. Fourth, the schedule of acupuncture treatment is flexible and varied (Table 1). Fifth, acupuncture has a wide range of applications with few contraindications and is suitable for the elderly and children (35, 188). Sixth, the cost of acupuncture in China is low, which most patients can afford regardless of economic status.
Furthermore, we focused on other methods that have the potential to help improve the quality of life or relieve symptoms of CKD, including taking TCM prescriptions and Chinese patent medicine, including Tripterygium Wilfordii Hook. f. and Artemisinin, which can effectively reduce albuminuria and protect kidney tissue (189, 190). However, the compositions of traditional Chinese herbs are extremely complex; moreover, patients with advanced CKD may suffer from electrolyte disorders due to metabolic issues. Therefore, more detailed studies and monitoring is required to ensure the safety of patients. The KDIGO guidelines suggest that proper exercise and dietary management, including low sodium, high-quality protein, and low-fat diets, can help improve patients’ quality of life; acupuncture should also be recommended as an effective physical therapy (5).
There are some obvious limitations of this literature review. First, because of the involvement of various acupuncture points, complex physiological aspects, and differing patient characteristics and disease processes, acupuncture-based treatment of CKD is highly personalized, and the specific therapeutic mechanism and indications needs further study. Second, there is still a lack of large-scale, double-blind, multicenter, large sample size, randomized studies to verify the observed effects and provide a high-quality theoretical basis for them. Third, the mechanisms of acupuncture in improving ESRD-related symptoms, especially RLS and sleep disorder, cannot be clarified for now. Finally, the review could only cover studies that focused on therapeutic mechanisms that were not specific to renal pathology, on which there are very few studies. Some literatures mentioned renal interstitial fibrosis without specific pathological diagnosis. Only one clinical trial revealed the effectiveness of moxibustion on membranous nephropathy. Two animal studies mentioned focal segmental glomerulosclerosis (FSGS), one research revealed that moxibustion delay the progress of FSGS via alleviating podocyte injury, the other one did not mention the underlying mechanism.
This review suggests that acupuncture can be beneficial for CKD through several mechanisms, including oxidative stress inhibition, reducing inflammatory effects, improving hemodynamics, maintaining podocyte structure, and increasing energy metabolism. In general, acupuncture has the potential to become a new, simple, safe, and inexpensive treatment modality that can be used to treat CKD, slow the progress of renal dysfunction, and improve patient symptoms. However, the review only covers non-specific therapeutic mechanisms, lacking content related to renal pathology due to a lack of studies on this topic. Moreover, it is unclear whether acupuncture can improve CKD with different pathologies, and rigorous clinical and mechanistic studies are required to design future protocols for the use of acupuncture in such cases. This could prove conducive to understanding the potential mechanisms involved in different renal pathological diagnosis as well as the impact that acupuncture may have on them.
All authors contributed to one or more of the following aspects of the manuscript: conception, acquisition of data, drafting, and revising the article. WZ and XL researched data and wrote the manuscript. XW and HM reviewed the manuscript. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Group IGOCW. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl (2013) 3:1–150. doi: 10.7326/0003-4819-158-11-201306040-00007
2. Zhang L, Wang F, Wang L, Wang W, Liu B, Liu J, et al. Prevalence of chronic kidney disease in China: A cross-sectional survey. Lancet (2012) 379:815–22. doi: 10.1016/S0140-6736(12)60033-6
3. GBD 2019 Viewpoint Collaborators. Five insights from the global burden of disease study 2019. Lancet (2020) 396:1135–59. doi: 10.1016/S0140-6736(20)31404-5
4. Appel GB, Waldman M. The IgA nephropathy treatment dilemma. Kidney Int (2006) 69:1939–44. doi: 10.1038/sj.ki.5000434
5. Rovin BH, Adler SG, Barratt J, Bridoux F, Burdge KA, Chan TM, et al. Kdigo 2021 clinical practice guideline for the management of glomerular diseases. Kidney Int (2021) 100(4):S1–S276. doi: 10.1016/j.kint.2021.05.021
6. Murtagh FEM, Addington-Hall J, Higginson IJ. The prevalence of symptoms in end-stage renal disease: a systematic review. Adv Chronic Kidney Dis (2007) 14:82–99. doi: 10.1053/j.ackd.2006.10.001
7. Almutary H, Bonner A, Douglas C. Symptom burden in chronic kidney disease: a review of recent literature. J Ren Care (2013) 39:140–50. doi: 10.1111/j.1755-6686.2013.12022.x
8. Fletcher BR, Damery S, Aiyegbusi OL, Anderson N, Calvert M, Cockwell P, et al. Symptom burden and health-related quality of life in chronic kidney disease: A global systematic review and meta-analysis. PloS Med (2022) 19:e1003954. doi: 10.1371/journal.pmed.1003954
9. Metzger M, Abdel-Rahman EM, Boykin H, Song MK. A narrative review of management strategies for common symptoms in advanced CKD. Kidney Int Rep (2021) 6:894–904. doi: 10.1016/j.ekir.2021.01.038
10. World Health Organization. Standard acupuncture nomenclature: A brief explanation of 361 classical acupuncture point names and their multilingual comparative list (2014). Available at: https://www.who.int/publications/i/item/9290611057 (Accessed 2022).
11. Melo GAA, Aguiar LL, Silva RA, Pereira FGF, da Silva FLB, Caetano JÁ. Effects of acupuncture in patients with chronic kidney disease: a systematic review. Rev Bras Enferm (2020) 73:e20180784. doi: 10.1590/0034-7167-2018-0784
12. Yu JS, Ho CH, Wang HY, Chen YH, Hsieh CL. Acupuncture on renal function in patients with chronic kidney disease: a single-blinded, randomized, preliminary controlled study. J Altern Complement Med (2017) 23:624–31. doi: 10.1089/acm.2016.0119
13. Wei YH, Li WJ, Wang Z. Efficacy of acupuncture and moxibustion combined with jiawei erxian decoction in the treatment of chronic glomerulonephritis with spleen-kidney qi deficiency syndrome. Asia-Pacific Tradit Med (2021) 17:64–7.10.1097/MD.0000000000027687
14. Jiang XL, Qiu FH. Effect of acupuncture-moxibustion as adjunct treatment on kidney function and prognosis in early-middle stage chronic renal failure. Shanghai J Acupuncture Moxibustion (2018) 37:1363–7. doi: 10.13460/j.issn.1005-0957.2018.12.1363
15. Zhu C, Luo Y. Clinical controlled trial on chronic nephritis albuminuria treated with acupuncture and moxibustion at dong's extra points, "Xiasanhuang". Zhongguo Zhen Jiu (2015) 35:335–8. doi: 10.13703/j.0255-2930.2015.04.006
16. Paterno JC, Freire AO, Soares MF, Franco MF, Schor N, Teixeira VPC. Electroacupuncture and moxibustion attenuate the progression of renal disease in 5/6 nephrectomized rats. Kidney Blood Press Res (2008) 31:367–73. doi: 10.1159/000176189
17. Nie F, Yang Q, Deng K, Sun X, Dong J, Li Z. Acupuncture-moxibustion for chronic allograft nephropathy: A randomized controlled trial. Zhongguo Zhen Jiu (2015) 35:1110–4. doi: 10.13703/j.0255-2930.2015.11.008
18. Mao JY, Yang FW, Liu H, Gao F, Yang B, Zhang Y, et al. Effect of moxibustion on renal function and hypercoagulable state in patients with idiopathic membranous nephropathy of low to medium risk with spleen-kidney deficiency and blood stasis. Zhongguo Zhen Jiu (2021) 41:1216–20.10.13703/j.0255-2930.20200907-0005
19. Matsumoto-Miyazaki J, Miyazaki N, Murata I, Yoshida G, Ushikoshi H, Ogura S, et al. Traditional thermal therapy with indirect moxibustion decreases renal arterial resistive index in patients with chronic kidney disease. J Altern Complement Med (2016) 22:306–14. doi: 10.1089/acm.2015.0276
20. Feng L, Su J, Chi R, Zhu Q, Lv S, Liang W. Effect of amlodipine besylate combined with acupoint application of traditional Chinese medicine nursing on the treatment of renal failure and hypertension by the PI3K/AKT pathway. Int J Mol Med (2019) 43:1900–10. doi: 10.3892/ijmm.2019.4104
21. Li Y, Sun Y, Zhang C, Wang K, Shen P, Huang D, et al. Moxibustion alleviates injury in a rat focal segmental glomerulosclerosis model. Evid Based Complement Alternat Med (2017) 2017:7169547. doi: 10.1155/2017/7169547
22. Zuo Z, Huang P, Jiang Y, Zhang Y, Zhu M. Acupuncture attenuates renal interstitial fibrosis via the TGF−β/Smad pathway. Mol Med Rep (2019) 20:2267–75. doi: 10.3892/mmr.2019.10470
23. Zhang CN, Huang XK, Luo Y, Jiang J, Wan L, Ling W. Effect of electroacupuncture intervention on renal function and expression of renal beta-catenin in rats with chronic renal failure. Zhen Ci Yan Jiu (2014) 39:396–400. doi: 10.13702/j.1000-0607.2014.05.030
24. Li L, Sun YX, Ma JY, Zhang CL, Li Y. Effect of mild moxibustion with different terms at different acupoints on renal functions and renal pathological changes in focal segmental glomerulosclerosis rats. Zhen Ci Yan Jiu (2016) 41:521–7. doi: 10.13702/j.1000-0607.2016.06.008
25. Taal MW, Brenner BM. Predicting initiation and progression of chronic kidney disease: developing renal risk scores. Kidney Int (2006) 70:1694–705. doi: 10.1038/sj.ki.5001794
26. Wang AN, Gao H, Yang YF, Shi Y. A systematic review of acupuncture on diabetic kidney disease. Trad Chi Med Pharm (2019) 25:81–6. doi: 10.13862/j.cnki.cn43-1446/r.2019.09.024
27. Zhang Z, Li X, Liu L, Sun J, Wang X, Zhao Z, et al. Tiaolipiwei acupuncture reduces albuminuria by alleviating podocyte lesions in a rat model of diabetic nephropathy. Evid Based Complement Alternat Med (2018) 2018:1913691. doi: 10.1155/2018/1913691
28. Han JX, Jin X, Liu CZ, Wang T, Lu MX. Effects of acupuncture on blood-lipid levels in the patient of cerebral infarction with hyperlipidemia. Zhongguo Zhen Jiu (2006) 26:399–402.
29. Zhao CJ, Mao JN, Wang LL, Luo W. Effect of zhulian needle insertion by slow twirling technique on peroxidation and apoptosis of kidney tissue in aging rats. Zhongguo Zhen Jiu (2021) 41:531–5. doi: 10.13703/j.0255-2930.20200531-k0005
30. Cao W, Liu JH, Zhang H, Zhang L, Zhang LY, Pan MM. Effect of acupoint injection on erythropoietin resistance in patients with chronic renal failure. Zhongguo Zhen Jiu (2010) 30:891–5. doi: 10.13703/j.0255-2930.2010.11.003
31. Karjalian F, Momennasab M, Yoosefinejad AK, Jahromi SE. The effect of acupressure on the severity of pruritus and laboratory parameters in patients undergoing hemodialysis: a randomized clinical trial. J Acupunct Meridian Stud (2020) 13:117–23. doi: 10.1016/j.jams.2020.05.002
32. Mohammadi MM, Raygani AAV, Ghobadi A, Samadzadeh S, Salari N. Effect of near-infrared light therapy based on acupoints on the severity of restless legs syndrome in patients undergoing hemodialysis: a single-blind, randomized controlled trial. Clin Med Res (2018) 16:1–8. doi: 10.3121/cmr.2018.1389
33. Cheng FK. The effectiveness of acupuncture on sleep disorders: A narrative review. Altern Ther Health Med (2020) 26:26–48.
34. Liu K, Jiang J-F, Lu S-F. Effect characteristics and mechanism of acupuncture in autonomic nerve regulation. Zhen Ci Yan Jiu Acupuncture Res (2021) 46(4):335–41. doi: 10.13702/j.1000-0607.200665
35. Weidenhammer W, Streng A, Linde K, Hoppe A, Melchart D. Acupuncture for chronic pain within the research program of 10 German health insurance funds–basic results from an observational study. Complement Ther Med (2007) 15:238–46. doi: 10.1016/j.ctim.2006.09.005
36. Chu SWF, Ng WJ, Yeam CT, Khan RQ, Low LL, Quah JHM, et al. Manipulative and body-based methods in chronic kidney disease patients: A systematic review of randomized controlled trials. Complement Ther Clin Pract (2022) 48:101593. doi: 10.1016/j.ctcp.2022.101593
37. Ernst E, Lee MS, Choi TY. Acupuncture: does it alleviate pain and are there serious risks? a review of reviews. Pain (2011) 152:755–64. doi: 10.1016/j.pain.2010.11.004
38. World Health Organization. WHO benchmarks for the training of acupuncture (2021). Available at: https://www.who.int/publications/i/item/9789240017962.
39. Wang K-X, Liang F-X, Chen S, Han Y-L, Luo Z-H, Zhang Y-L, et al. Electroacupuncture of" biaoben acupoints" relieves kidney injury by suppressing oxidative stress in diabetic nephropathy rats. Zhen Ci Yan Jiu (2022) 47(5):435–42. doi: 10.13702/j.1000-0607.20210381
40. Pan Y, Chen Y, Li Q, Yu X, Wang J, Zheng J. The synthesis and evaluation of novel hydroxyl substituted chalcone analogs with in vitro anti-free radicals pharmacological activity and in vivo anti-oxidation activity in a free radical-injury alzheimer’s model. Molecules (2013) 18:1693–703. doi: 10.3390/molecules18021693
41. Wang K-X, Liang F-X, Chen S, Luo Z-H, Chen B, Chen Z-Q, et al. Effect of electroacupuncture of" biao-ben" acupoints on renal function and hemorheology and enos level in patients with early diabetic nephropathy. Zhen Ci Yan Jiu (2022) 47(1):46–52. doi: 10.13702/j.1000-0607.20210036
42. Huang H, Chen L, Wu H, Jin JS. Effect of electroacupuncture on renal function and expression of autophagy-related proteins in kidney of rats with diabetic nephropathy. Zhen Ci Yan Jiu (2022) 47:108–14. doi: 10.13702/j.1000-0607.20210329
43. Zhang J, Yang X, Zhang X, Lu D, Guo R. Electro-acupuncture protects diabetic nephropathy-induced inflammation through suppression of NLRP3 inflammasome in renal macrophage isolation. Endocr Metab Immune Disord Drug Targets (2021) 21:2075–83. doi: 10.2174/1871530321666210118161721
44. Zhang ZL, Ji XQ, Zhang P, Zhang XH, Meng ZJ, Yang XJ. Randomized and controlled study on needling method of harmonizing spleen-stomach for early intervention of diabetic nephropathies and the mechanism of protecting kidney. Zhongguo Zhen Jiu (2007) 27:875–80.
45. Zhang ZL, Zhao SH, Li X, Yang YQ, Chen H, Wang M. Clinical observation on repair of lymphocyte injury in patients with diabetic nephropathy treated by regulating spleen-stomach needling. Zhongguo Zhen Jiu (2013) 33:1065–70. doi: 10.13703/j.0255-2930.2013.12.005
46. Li CR, Cheng ZD, Zhang ZX, Kim A, Ha JM, Song YY, et al. Effects of acupuncture at taixi acupoint (KI3) on kidney proteome. Am J Chi Med (2011) 39:687–92. doi: 10.1142/S0192415X11009123
47. Chen YG, Li CR, Song YY, Zheng J. Effect of acupuncture of "Taixi" (KI 3) on protein expression in the renal tissues of healthy rats. Zhen Ci Yan Jiu (2010) 35:170–4. doi: 10.13702/j.1000-0607.2010.03.002
48. Li D, Chen ZB, Yin NN. Electroacupuncture preconditioning alleviates kidney injury in hyperglycemic mice. Zhen Ci Yan Jiu (2021) 46:215–20. doi: 10.13702/j.1000-0607.201084
49. Li D, Chen Z-B, Zheng Z, Yin N-N. Electroacupuncture pretreatment alleviates apoptosis of renal tubular epithelia cells by down-regulating expression of trpc6 in hyperglycemic mice. Zhen Ci Yan Jiu (2022) 47(3):209–15. doi: 10.13702/j.1000-0607.20210195
50. Song YH. Observation on therapeutic effects of combined acupuncture and medicine therapy and simple medication on renal hypertension of chronic kidney disease. Zhongguo Zhen Jiu (2007) 27:641–4.
51. An P, Dang HM, Shi XM, Ye BY, Wu XL. “Qufeng tongluo” acupuncture prevents the progression of glomerulonephritis by decreasing renal sympathetic nerve activity. J Ethnopharmacol (2014) 155:277–84. doi: 10.1016/j.jep.2014.05.019
52. Paterno JC, Bergamaschi CT, Campos RR, Higa EMS, Soares MF, Schor N, et al. Electroacupuncture and moxibustion decrease renal sympathetic nerve activity and retard progression of renal disease in rats. Kidney Blood Press Res (2012) 35:355–64. doi: 10.1159/000336095
53. Kim DD, Pica AM, Durán RG, Durán WN. Acupuncture reduces experimental renovascular hypertension through mechanisms involving nitric oxide synthases. Microcirculation (2006) 13:577–85. doi: 10.1080/10739680600885210
54. Oh YI, Yang EJ, Choi SM, Kang CW. The effect of electroacupuncture on insulin-like growth factor-I and oxidative stress in an animal model of renal failure-induced hypertension. Kidney Blood Press Res (2012) 35:634–43. doi: 10.1159/000339640
55. Yang S-Z, Ning S-S, Sun Y-X, Li L, Ma J-Y, Jin J-H, et al. Effect of electroacupuncture on renal fibrosis in spontaneously hypertension rats and its related mechanisms. Zhen Ci Yan Jiu (2019) 44(12):911–5. doi: 10.13702/j.1000-0607.190167
56. Chen ZJ, Qu Y, Zhang LD, Liu Y, Wang SS, Gu LY. Effects of acupuncture on kidney morphological structure and expression of TGF-beta1 mRNA in rats with spontaneous hypertension. Zhongguo Zhen Jiu (2013) 33:824–8. doi: 10.13703/j.0255-2930.2013.09.019
57. Che-Yi C, Wen CY, Min-Tsung K, Chiu-Ching H. Acupuncture in haemodialysis patients at the quchi (LI11) acupoint for refractory uraemic pruritus. Nephrol Dial Transplant (2005) 20:1912–5. doi: 10.1093/ndt/gfh955
58. Akça NK, Tasci S. Acupressure and transcutaneous electrical acupoint stimulation for improving uremic pruritus: a randomized, controlled trial. Altern Ther Health Med (2016) 22:18–24.
59. Rehman IU, Ahmed R, Rahman AU, Wu DBC, Munib S, Shah Y, et al. Effectiveness and safety profiling of zolpidem and acupressure in CKD associated pruritus: an interventional study. Med (Baltimore) (2021) 100:e25995. doi: 10.1097/MD.0000000000025995
60. Arab Z, Shariati AR, Asayesh H, Vakili MA, Bahrami-Taghanaki H, Azizi H. A sham-controlled trial of acupressure on the quality of sleep and life in haemodialysis patients. Acupunct Med (2016) 34:2–6. doi: 10.1136/acupmed-2014-010369
61. Shariati A, Jahani S, Hooshmand M, Khalili N. The effect of acupressure on sleep quality in hemodialysis patients. Complement Ther Med (2012) 20:417–23. doi: 10.1016/j.ctim.2012.08.001
62. Tsay SL. Acupressure and fatigue in patients with end-stage renal disease–a randomized controlled trial. Int J Nurs Stud (2004) 41:99–106. doi: 10.1016/S0020-7489(03)00079-8
63. Eğlence R, Karataş N, Taşci S. The effect of acupressure on the level of fatigue in hemodialysis patients. Altern Ther Health Med (2013) 19:23–31.
64. Wang SH, Qiu MY, Cheng AH, Li N, Xie YM, Hao JR, et al. Improvement of survival quality of the patients with hemodialysis treated with moxibustion for regulating spleen and stomach functions: multi-central randomized controlled study. Zhongguo Zhen Jiu (2014) 34:319–24. doi: 10.13703/j.0255-2930.2014.04.003
65. Kim KH, Kim TH, Kang JW, Sul JU, Lee MS, Kim JI, et al. Acupuncture for symptom management in hemodialysis patients: A prospective, observational pilot study. J Altern Complement Med (2011) 17:741–8. doi: 10.1089/acm.2010.0206
66. Li N, Qiu MY, Hao JR, Zhang QM, Wang SH, Liang F, et al. Randomized controlled trail on moxibustion for maintenance hemodialysis patients in deficiency syndrome. Zhongguo Zhen Jiu (2011) 31:15–8. doi: 10.13703/j.0255-2930.2011.01.005
67. Su LH, Wu KD, Lee LS, Wang H, Liu CF. Effects of far infrared acupoint stimulation on autonomic activity and quality of life in hemodialysis patients. Am J Chin Med (2009) 37:215–26. doi: 10.1142/S0192415X09006783
68. Sun H, Qiu MY, Li BQ, Wang SH, Chen ZY, Jiang Y, et al. Effect of moxibustion on quality of life in hemodialysis patients. Zhongguo Zhen Jiu (2008) 28:321–4.
69. Tsay SL, Cho YC, Chen ML. Acupressure and transcutaneous electrical acupoint stimulation in improving fatigue, sleep quality and depression in hemodialysis patients. Am J Chin Med (2004) 32:407–16. doi: 10.1142/S0192415X04002065
70. Bullen A, Awdishu L, Lester W, Moore T, Trzebinska D. Effect of acupuncture or massage on health-related quality of life of hemodialysis patients. J Altern Complement Med (2018) 24:1069–75. doi: 10.1089/acm.2018.0030
71. Samsu N. Diabetic nephropathy: challenges in pathogenesis, diagnosis, and treatment. BioMed Res Int (2021) 2021:1497449. doi: 10.1155/2021/1497449
72. Tavafi M. Diabetic nephropathy and antioxidants. J Nephropathol (2013) 2:20–7. doi: 10.5812/nephropathol.9093
73. Castellani P, Balza E, Rubartelli A. Inflammation, DAMPs, tumor development, and progression: A vicious circle orchestrated by redox signaling. Antioxid Redox Signal (2014) 20:1086–97. doi: 10.1089/ars.2012.5164
74. Mittal M, Siddiqui MR, Tran K, Reddy SP, Malik AB. Reactive oxygen species in inflammation and tissue injury. Antioxid Redox Signal (2014) 20:1126–67. doi: 10.1089/ars.2012.5149
75. Jia Y, Chen Q, Zhao M. Systematic review and meta-regression analysis of acupuncture for diabetic nephropathy. Zhejiang J Tradit Chin Med (2019) 54:72–5. doi: 10.13633/j.cnki.zjtcm.2019.01.056
76. Liu R. Meta analysis of combined acupuncture and medicine treating diabetes and its complications. Sun Z. Nanjing Univ Chin Med (2018).
77. Gerber PA, Rutter GA. The role of oxidative stress and hypoxia in pancreatic beta-cell dysfunction in diabetes mellitus. Antioxid Redox Signal (2017) 26(10):501–18. doi: 10.1089/ars.2016.6755
78. Du M, Wang Q, Li W, Ma X, Wu L, Guo F, et al. Overexpression of foxo1 ameliorates the podocyte epithelial–mesenchymal transition induced by high glucose in vitro and in vivo. Biochem Biophys Res Commun (2016) 471(4):416–22. doi: 10.1016/j.bbrc.2016.02.066
79. Marrocco I, Altieri F, Peluso I. Measurement and clinical significance of biomarkers of oxidative stress in humans. Oxid Med Cell Longev (2017) 2017:6501046. doi: 10.1155/2017/6501046
80. Valko M, Leibfritz D, Moncol J, Cronin MTD, Mazur M, Telser J. Free radicals and antioxidants in normal physiological functions and human disease. Int J Biochem Cell Biol (2007) 39:44–84. doi: 10.1016/j.biocel.2006.07.001
81. Yu JB, Shi J, Zhang Y, Gong LR, Dong SA, Cao XS, et al. Electroacupuncture ameliorates acute renal injury in lipopolysaccharide-stimulated rabbits via induction of HO-1 through the PI3K/Akt/Nrf2 pathways. PloS One (2015) 10:e0141622. doi: 10.1371/journal.pone.0141622
82. Lim AK, Tesch GH. Inflammation in diabetic nephropathy. Mediators Inflammation (2012) 2012:146154. doi: 10.1155/2012/146154
83. Pickup JC, Chusney GD, Thomas SM, Burt D. Plasma interleukin-6, tumour necrosis factor α and blood cytokine production in type 2 diabetes. Life Sci (2000) 67:291–300. doi: 10.1016/S0024-3205(00)00622-6
84. Shang J, Wang L, Zhang Y, Zhang S, Ning L, Zhao J, et al. Chemerin/ChemR23 axis promotes inflammation of glomerular endothelial cells in diabetic nephropathy. J Cell Mol Med (2019) 23:3417–28. doi: 10.1111/jcmm.14237
85. Zhang Y, Gong H, Zhan B, Chen S. Acupoint catgut embedding reduces insulin resistance in diabetic patients undergoing open cardiac surgery. Heart Surg Forum (2021) 24:E060–4. doi: 10.1532/hsf.3331
86. Bhargava P, Schnellmann RG. Mitochondrial energetics in the kidney. Nat Rev Nephrol (2017) 13:629–46. doi: 10.1038/nrneph.2017.107
87. Galvan DL, Green NH, Danesh FR. The hallmarks of mitochondrial dysfunction in chronic kidney disease. Kidney Int (2017) 92:1051–7. doi: 10.1016/j.kint.2017.05.034
88. Figueiredo LM, Silva AH, do Prado Neto AX, Hissa MN, de Vasconcelos PRL, Guimarães SB. Electroacupuncture stimulation using different frequencies (10 and 100 Hz) changes the energy metabolism in induced hyperglycemic rats. Acta Cir Bras (2011) 26:47–52. doi: 10.1590/S0102-86502011000700010
89. Ron-Harel N, Ghergurovich JM, Notarangelo G, LaFleur MW, Tsubosaka Y, Sharpe AH, et al. T Cell activation depends on extracellular alanine. Cell Rep (2019) 28:3011–21.e4. doi: 10.1016/j.celrep.2019.08.034
90. Chen M, He QD, Guo JJ, Wu QB, Zhang Q, Yau YM, et al. Electro-acupuncture regulates metabolic disorders of the liver and kidney in premature ovarian failure mice. Front Endocrinol (Lausanne) (2022) 13:882214. doi: 10.3389/fendo.2022.882214
91. Wei GH, Yang ZB, Xie YF, Pei MR, Yang JL, Yu YJ, et al. Nuclear magnetic resonance-based metabolomics revealed metabolite profiles participate in intervention effect of refined moxibustion in gastric ulcer model rats. Zhen Ci Yan Jiu (2021) 46:829–36. doi: 10.13702/j.1000-0607.201351
92. Dai H, Liu Q, Liu B. Research progress on mechanism of podocyte depletion in diabetic nephropathy. J Diabetes Res (2017) 2017:2615286. doi: 10.1155/2017/2615286
93. Nielsen JS, McNagny KM. The role of podocalyxin in health and disease. J Am Soc Nephrol (2009) 20:1669–76. doi: 10.1681/ASN.2008070782
94. Schwarz K, Simons M, Reiser J, Saleem MA, Faul C, Kriz W, et al. Podocin, a raft-associated component of the glomerular slit diaphragm, interacts with CD2AP and nephrin. J Clin Invest (2001) 108:1621–9. doi: 10.1172/JCI200112849
95. Zou J, Yaoita E, Watanabe Y, Yoshida Y, Nameta M, Li H, et al. Upregulation of nestin, vimentin, and desmin in rat podocytes in response to injury. Virchows Arch (2006) 448:485–92. doi: 10.1007/s00428-005-0134-9
96. Dryer SE, Reiser J. TRPC6 channels and their binding partners in podocytes: role in glomerular filtration and pathophysiology. Am J Physiol Renal Physiol (2010) 299:F689–701. doi: 10.1152/ajprenal.00298.2010
97. Möller CC, Wei C, Altintas MM, Li J, Greka A, Ohse T, et al. Induction of TRPC6 channel in acquired forms of proteinuric kidney disease. J Am Soc Nephrol (2007) 18:29–36. doi: 10.1681/ASN.2006091010
98. Sonneveld R, van der Vlag J, Baltissen MPA, Verkaart SAJ, Wetzels JFM, Berden JHM, et al. Glucose specifically regulates TRPC6 expression in the podocyte in an AngII-dependent manner. Am J Pathol (2014) 184:1715–26. doi: 10.1016/j.ajpath.2014.02.008
99. Nahas ME. The global challenge of chronic kidney disease. Kidney Int (2005) 68:2918–29. doi: 10.1111/j.1523-1755.2005.00774.x
100. Namgung S, Yoon JJ, Yoon CS, Han BH, Choi ES, Oh H, et al. Prunella vulgaris attenuates diabetic renal injury by suppressing glomerular fibrosis and inflammation. Am J Chin Med (2017) 45:475–95. doi: 10.1142/S0192415X1750029X
101. Tan X, Pan Y, Su W, Gong S, Zhu H, Chen H, et al. Acupuncture therapy for essential hypertension: a network meta-analysis. Ann Transl Med (2019) 7:266. doi: 10.21037/atm.2019.05.59
102. Zhang J, Rudemiller NP, Patel MB, Karlovich NS, Wu M, McDonough AA, et al. Interleukin-1 receptor activation potentiates salt reabsorption in angiotensin II-induced hypertension via the NKCC2 co-transporter in the nephron. Cell Metab (2016) 23:360–8. doi: 10.1016/j.cmet.2015.11.013
103. Leask A. Potential therapeutic targets for cardiac fibrosis: TGFβ, angiotensin, endothelin, CCN2, and PDGF, partners in fibroblast activation. Circ Res (2010) 106:1675–80. doi: 10.1161/CIRCRESAHA.110.217737
104. Jiang XL. Effects of magnetic needle acupuncture on blood pressure and plasma ET-1 level in the patient of hypertension. J Tradit Chin Med (2003) 23:290–1.
105. Pan P, Zhang X, Qian H, Shi W, Wang J, Bo Y, et al. Effects of electro-acupuncture on endothelium-derived endothelin-1 and endothelial nitric oxide synthase of rats with hypoxia-induced pulmonary hypertension. Exp Biol Med (Maywood) (2010) 235:642–8. doi: 10.1258/ebm.2010.009353
106. Huo ZJ, Li Q, Tian GH, Zhou CM, Wei XH, Pan CS, et al. The ameliorating effects of long-term electroacupuncture on cardiovascular remodeling in spontaneously hypertensive rats. BMC Complement Altern Med (2014) 14:118. doi: 10.1186/1472-6882-14-118
107. Mizuiri S, Ohashi Y. ACE and ACE2 in kidney disease. World J Nephrol (2015) 4:74–82. doi: 10.5527/wjn.v4.i1.74
108. Ferreira AJ, Santos RAS. Cardiovascular actions of angiotensin-(1-7). Braz J Med Biol Res (2005) 38:499–507. doi: 10.1590/S0100-879X2005000400003
109. Liu WN, Jin LW, Han DW, Ren XX, Zhu J, Zhang LF. Effect of electroacupuncture of different acupoints on blood pressure, plasma angiotensin II, aldosterone and atrial natriuretic peptide in spontaneous hypertension rats. Zhen Ci Yan Jiu (2009) 34:393–7.
110. Potts JT. Inhibitory neurotransmission in the nucleus tractus solitarii: Implications for baroreflex resetting during exercise. Exp Physiol (2006) 91:59–72. doi: 10.1113/expphysiol.2005.032227
111. Zhang W, Mifflin S. Plasticity of GABAergic mechanisms within the nucleus of the solitary tract in hypertension. Hypertension (2010) 55:201–6. doi: 10.1161/HYPERTENSIONAHA.109.146407
112. Zubcevic J, Potts JT. Role of GABAergic neurones in the nucleus tractus solitarii in modulation of cardiovascular activity. Exp Physiol (2010) 95:909–18. doi: 10.1113/expphysiol.2010.054007
113. Zhang Q, Tan YY, Liu XH, Yao FR, Cao DY. Electroacupuncture improves baroreflex and γ-aminobutyric acid type b receptor-mediated responses in the nucleus tractus solitarii of hypertensive rats. Neural Plast (2018) 2018:8919347. doi: 10.1155/2018/8919347
114. Stout JM, Gousset MU, Drummond HA, Gray IIIW, Pruett BE, Stec DE. Sex-specific effects of heme oxygenase-2 deficiency on renovascular hypertension. J Am Soc Hypertens (2013) 7:328–35. doi: 10.1016/j.jash.2013.04.004
115. Dinh QN, Drummond GR, Sobey CG, Chrissobolis S. Roles of inflammation, oxidative stress, and vascular dysfunction in hypertension. BioMed Res Int (2014) 2014:406960. doi: 10.1155/2014/406960
116. Martínez-Casales M, Hernanz R, Alonso MJ. Vascular and macrophage heme oxygenase-1 in hypertension: a mini-review. Front Physiol (2021) 12:643435. doi: 10.3389/fphys.2021.643435
117. Oh YI, Kim JH, Kang CW. Oxidative stress in MCF-7 cells is involved in the effects of retinoic acid-induced activation of protein kinase c-δ on insulin-like growth factor-I secretion and synthesis. Growth Horm IGF Res (2010) 20:101–9. doi: 10.1016/j.ghir.2009.10.003
118. Higashi Y, Sukhanov S, Anwar A, Shai SY, Delafontaine P. IGF-1, oxidative stress and atheroprotection. Trends Endocrinol Metab (2010) 21:245–54. doi: 10.1016/j.tem.2009.12.005
119. Wolf G. After all those fat years: renal consequences of obesity. Nephrol Dial Transplant (2003) 18:2471–4. doi: 10.1093/ndt/gfg427
120. Schmitz PG, O'Donnell MP, Kasiske BL, Katz SA, Keane WF. Renal injury in obese zucker rats: glomerular hemodynamic alterations and effects of enalapril. Am J Physiol (1992) 263:F496–502. doi: 10.1152/ajprenal.1992.263.3.F496
121. Park SK, Kang SK. Renal function and hemodynamic study in obese zucker rats. Korean J Intern Med (1995) 10:48–53. doi: 10.3904/kjim.1995.10.1.48
122. Amann K, Benz K. Structural renal changes in obesity and diabetes. Semin Nephrol (2013) 33:23–33. doi: 10.1016/j.semnephrol.2012.12.003
123. Moorhead JF, Chan MK, El-Nahas M, Varghese Z. Lipid nephrotoxicity in chronic progressive glomerular and tubulo-interstitial disease. Lancet (1982) 320:1309–11. doi: 10.1016/S0140-6736(82)91513-6
124. Cui Y-J, Cui P-X, Geng L-Q. Effects of moxibustion on blood-lipid levels in the patient of cerebral infarction with hyperlipidemia. J Sichuan Tradit Chin Med (2016) 34(08):169–71.
125. Zhang GX, Miao JL, Zhang ZY, Wang HJ, Ji LX. Regulation effects of electroacupuncture with different acupoint combinations on blood lipid in rats with hyperlipemia. Zhongguo Zhen Jiu (2014) 34:894–7. doi: 10.13703/j.0255-2930.2014.09.045
126. Shen HB, Zhang L, Guo J, Ji XL, Peng B, Li FY, et al. Protective effect of acupuncture on heart in mice with hyperlipemia and its mechanism. Zhongguo Zhen Jiu (2014) 34:373–8. doi: 10.13703/j.0255-2930.2014.04.020
127. Yeom M, Park J, Lee B, Lee HS, Park HJ, Won R, et al. Electroacupuncture ameliorates poloxamer 407-induced hyperlipidemia through suppressing hepatic SREBP-2 expression in rats. Life Sci (2018) 203:20–6. doi: 10.1016/j.lfs.2018.04.016
128. Ye X, Zhang H. Influence of moxibustion temperatures on blood lipids, endothelin-1, and nitric oxide in hyperlipidemia patients. J Tradit Chin Med (2013) 33:592–6. doi: 10.1016/S0254-6272(14)60026-1
129. Zhou L, Zhang HX, Liu LG, Wan WJ. Effect of electro-acupuncture at fenglong (GV 16) on nitric oxide and endothelin in rats with hyperlipidemia. Zhong Xi Yi Jie He Xue Bao (2008) 6:89–92. doi: 10.3736/jcim20080117
130. Zhang HF, Wang LL, Ji MY, Zhou XY. Effects of mild moxibustion on contents of blood lipoids and serum no in hyperlipidemia rats. Zhongguo Zhen Jiu (2013) 33:438–42. doi: 10.13703/j.0255-2930.2013.05.018
131. Wang GY, Wang LL, Xu B, Zhang JB, Jiang JF. Effects of moxibustion temperature on blood cholesterol level in a mice model of acute hyperlipidemia: Role of TRPV1. Evid Based Complement Alternat Med (2013) 2013:871704. doi: 10.1155/2013/871704
132. Shen X, Zhang S, Guo Z, Xing D, Chen W. The crosstalk of ABCA1 and ANXA1: A potential mechanism for protection against atherosclerosis. Mol Med (2020) 26:84. doi: 10.1186/s10020-020-00213-y
133. Hersberger M, von Eckardstein A. Modulation of high-density lipoprotein cholesterol metabolism and reverse cholesterol transport. In: von Eckardstein A, editor. Atherosclerosis: Diet and drugs. handbook of experimental pharmacology. Berlin: Springer (2005). p. 537–61.
134. Zou YF, Ma MZ, Zhao Z, Tan J, Yang JJ, Shi J, et al. Effect of herbal-cake-separated moxibustion on blood lipid levels and expression of hepatic PPARγ and SR-b 1 proteins and genes in hyperlipidemia atherosclerosis rabbits. Zhen Ci Yan Jiu (2018) 43:86–91. doi: 10.13702/j.1000-0607.170729
135. Zhang HX, Wang Q, Huang H, Yue W, Qin PF. Effect of electroacupuncture at "Fenglong" (ST 40) on rats with hyperlipidemia and its mechanism. Zhongguo Zhen Jiu (2012) 32:241–5. doi: 10.13703/j.0255-2930.2012.03.017
136. Wang Q, Huang H, Yue W. Regulatory functions of electroacupuncture at fenglong (ST40) on blood lipids and hepatic ABCA1 and PPARalpha in hyperlipidemia rats. Zhongguo Zhong Xi Yi Jie He Za Zhi (2012) 32:1245–8.
137. Yu XH, Fu YC, Zhang DW, Yin K, Tang CK. Foam cells in atherosclerosis. Clin Chim Acta (2013) 424:245–52. doi: 10.1016/j.cca.2013.06.006
138. Chen YF, Tian JY, Xiao Y, Wu H, Huang H, Zhang HX. Effects of electroacupuncture at "Fenglong" (ST 40) on formation of macrophage-derived foam cell and efflux of cholesterol in hyperlipidemia rats. Zhongguo Zhen Jiu (2014) 34:475–9. doi: 10.13703/j.0255-2930.2014.05.028
139. Ferré P, Phan F, Foufelle F. SREBP-1c and lipogenesis in the liver: an update. Biochem J (2021) 478:3723–39. doi: 10.1042/BCJ20210071
140. Jensen-Urstad APL, Semenkovich CF. Fatty acid synthase and liver triglyceride metabolism: housekeeper or messenger? Biochim Biophys Acta (2012) 1821:747–53. doi: 10.1016/j.bbalip.2011.09.017
141. Li XZ, Zhang HH, Lan DC, Zhang HT, Chen XZ, Sun J. Effect of eletroacupuncture intervention on insulin resistance, lipid metabolic disorder and expression of hepatic SREBP-1c and fatty acid synthase proteins in rats with hyperlipidemia. Zhen Ci Yan Jiu (2018) 43:8–13. doi: 10.13702/j.1000-0607.170517
142. Reiss AB, Voloshyna I, De Leon J, Miyawaki N, Mattana J. Cholesterol metabolism in CKD. Am J Kidney Dis (2015) 66:1071–82. doi: 10.1053/j.ajkd.2015.06.028
143. Gai Z, Wang T, Visentin M, Kullak-Ublick GA, Fu X, Wang Z. Lipid accumulation and chronic kidney disease. Nutrients (2019) 11:722. doi: 10.3390/nu11040722
144. Papapanagiotou A, Siasos G, Kassi E, Gargalionis AN, Papavassiliou AG. Novel inflammatory markers in hyperlipidemia: Clinical implications. Curr Med Chem (2015) 22(23):2727–43. doi: 10.2174/0929867322666150520095008
145. Le W, Xiao Y, Tian JY, Chen YF, Jin H, Ma W. Effect of electroacupuncture at fenglong (ST40) on expressions of inflammatory factors in macrophages of hyperlipidemia model rats. Zhongguo Zhong Xi Yi Jie He Za Zhi (2013) 33:1361–6.
146. Tian JY, Wang Q, Chen YF, Xiao Y, Yue W, Zhang HX. Effect of electroacupuncture stimulation of "Fenglong" (ST 40) on expression of inflammatory cytokines of celiac macrophages in hyperlipidemia rats. Zhen Ci Yan Jiu (2014) 39:282–7. doi: 10.13702/j.1000-0607.2014.04.005
147. Xiao Y, Le W, Huang H, Zhou L, Tian J, Chen Y. Effect of electroacupuncture of "Fenglong" (ST 40) on levels of blood lipid and macrophage TNF-alpha and IL-6 in hyperlipidemic rats. Zhen Ci Yan Jiu (2013) 38:459–64. doi: 10.13702/j.1000-0607.2013.06.007
148. Yan ZK, Yang ZJ, Chen F. Effect of electroacupuncture intervention on blood-lipid, high-sensitivity c-reactive protein and adiponectin levels in hyperlipidemia rats. Zhen Ci Yan Jiu (2013) 38:365–8,85. doi: 10.13702/j.1000-0607.2013.05.004
149. Iseki K, Iseki C, Ikemiya Y, Fukiyama K. Risk of developing end-stage renal disease in a cohort of mass screening. Kidney Int (1996) 49:800–5. doi: 10.1038/ki.1996.111
150. Fox CS, Larson MG, Leip EP, Culleton B, Wilson PW, Levy D. Predictors of new-onset kidney disease in a community-based population. JAMA (2004) 291:844–50. doi: 10.1001/jama.291.7.844
151. Weller JM, Wu SC, Ferguson CW, Hawthorne VM. End-stage renal disease in michigan. incidence, underlying causes, prevalence, and modalities of treatment. Am J Nephrol (1985) 5:84–95. doi: 10.1159/000166912
152. Ataga KI, Orringer EP. Renal abnormalities in sickle cell disease. Am J Hematol (2000) 63:205–11. doi: 10.1002/(SICI)1096-8652(200004)63:4<205::AID-AJH8>3.0.CO;2-8
153. Ravani P, Tripepi G, Malberti F, Testa S, Mallamaci F, Zoccali C. Asymmetrical dimethylarginine predicts progression to dialysis and death in patients with chronic kidney disease: a competing risks modeling approach. J Am Soc Nephrol (2005) 16:2449–55. doi: 10.1681/ASN.2005010076
154. Xiong W, He FF, You RY, Xiong J, Wang YM, Zhang C, et al. Acupuncture application in chronic kidney disease and its potential mechanisms. Am J Chin Med (2018) 46:1169–85. doi: 10.1142/S0192415X18500611
155. Roy PJ, Weltman M, Dember LM, Liebschutz J, Jhamb M. Pain management in patients with chronic kidney disease and end-stage kidney disease. Curr Opin Nephrol Hypertens (2020) 29:671. doi: 10.1097/MNH.0000000000000646
156. Samoudi AF, Marzouq MK, Samara AM, Zyoud SH, Al-Jabi SW. The impact of pain on the quality of life of patients with end-stage renal disease undergoing hemodialysis: a multicenter cross-sectional study from Palestine. Health Qual Life Outcomes (2021) 19:39. doi: 10.1186/s12955-021-01686-z
157. Daubresse M, Alexander GC, Crews DC, Segev DL, McAdams-DeMarco MA. Trends in opioid prescribing among hemodialysis patients, 2007–2014. Am J Nephrol (2019) 49:20–31. doi: 10.1159/000495353
158. Kimmel PL, Fwu CW, Abbott KC, Eggers AW, Kline PP, Eggers PW. Opioid prescription, morbidity, and mortality in united states dialysis patients. J Am Soc Nephrol (2017) 28:3658–70. doi: 10.1681/ASN.2017010098
159. Ishida JH, McCulloch CE, Steinman MA, Grimes BA, Johansen KL. Opioid analgesics and adverse outcomes among hemodialysis patients. Clin J Am Soc Nephrol (2018) 13:746–53. doi: 10.2215/CJN.09910917
160. Zhang R, Lao L, Ren K, Berman BM. Mechanisms of acupuncture–electroacupuncture on persistent pain. Anesthesiology (2014) 120:482–503. doi: 10.1097/ALN.0000000000000101
161. Kim HY, Wang J, Lee I, Kim HK, Chung K, Chung JM. Electroacupuncture suppresses capsaicin-induced secondary hyperalgesia through an endogenous spinal opioid mechanism. Pain (2009) 145:332–40. doi: 10.1016/j.pain.2009.06.035
162. Qaseem A, Wilt TJ, McLean RM, Forciea MA. Noninvasive treatments for acute, subacute, and chronic low back pain: a clinical practice guideline from the American college of physicians. Ann Intern Med (2017) 166:514–30. doi: 10.7326/M16-2367
163. Chen L, Michalsen A. Management of chronic pain using complementary and integrative medicine. BMJ (2017) 357:j1284. doi: 10.1136/bmj.j1284
164. Reszke R, Szepietowski JC. End-stage renal disease chronic itch and its management. Dermatol Clin (2018) 36:277–92. doi: 10.1016/j.det.2018.02.007
165. Pisoni RL, Wikström B, Elder SJ, Akizawa T, Asano Y, Keen ML, et al. Pruritus in haemodialysis patients: international results from the dialysis outcomes and practice patterns study (DOPPS). Nephrol Dial Transplant (2006) 21:3495–505. doi: 10.1093/ndt/gfl461
166. Zhang L, Li Y, Xiao X, Shi Y, Xu D, Li N, et al. Acupuncture for uremic pruritus: a systematic review and meta-analysis. J Pain Symptom Manage (2022) S0885-3924(22)00871-5. doi: 10.1016/j.jpainsymman.2022.08.017
167. Deng C. Clinical observation on chronic pruritus treated by electroacupuncture with different frequencies and its on il-4 and ifn-γ levels. Yin Y. Hubei Univ Tradit Chin Med (2018).
168. Ni G-B. The clinical observation about the efficacy of electroacupuncture in the treatment of chronic pruritus and its effect on the levels of il-10 and tnf-α in serum. Ding MQ. Hubei Univ Tradit Chin Med (2017).
169. Huang L-L, Yin Y, Fu L-H, Wu S-Y, Li M. Clinical effect of electroacupuncture on chronic pruritus and its influence on il-2 and il-10. Lishizhen Med Mater Med Res (2020) 31:1656–8.
170. Jiang L, Xie C, Huang J, Fu W. Antipruritic effect of electroacupuncture on mice with atopic dermatitis and pruritus and its effect on dynorphin and substance p. Chin J Gerontol (2016) 36:3874–7.
171. Yan CN, Yao WG, Bao YJ, Shi XJ, Yu H, Yin PH, et al. Effect of auricular acupressure on uremic pruritus in patients receiving hemodialysis treatment: a randomized controlled trial. Evid Based Complement Alternat Med (2015) 2015:593196. doi: 10.1155/2015/593196
172. Phillips B, Hening W, Britz P, Mannino D. Prevalence and correlates of restless legs syndrome: Results from the 2005 national sleep foundation poll. Chest (2006) 129:76–80. doi: 10.1378/chest.129.1.76
173. Allen RP, Walters AS, Montplaisir J, Hening W, Myers A, Bell TJ, et al. Restless legs syndrome prevalence and impact: REST general population study. Arch Intern Med (2005) 165:1286–92. doi: 10.1001/archinte.165.11.1286
174. Ohayon MM, O’Hara R, Vitiello MV. Epidemiology of restless legs syndrome: a synthesis of the literature. Sleep Med Rev (2012) 16:283–95. doi: 10.1016/j.smrv.2011.05.002
175. Sahli ZT, Jo J, Mousa SA, Tarazi FI. Clinical management of restless legs syndrome in end-stage renal disease patients. CNS Spectr (2017) 22:14–21. doi: 10.1017/S109285291600064X
176. Winter AC, Berger K, Glynn RJ, Buring JE, Gaziano JM, Schürks M, et al. Vascular risk factors, cardiovascular disease, and restless legs syndrome in men. Am J Med (2013) 126:228–35.e1-2. doi: 10.1016/j.amjmed.2012.06.039
177. Hoogwout SJ, Paananen MV, Smith AJ, Beales DJ, O’Sullivan PB, Straker LM, et al. Musculoskeletal pain is associated with restless legs syndrome in young adults. BMC Musculoskelet Disord (2015) 16:294. doi: 10.1186/s12891-015-0765-1
178. Amidei C, Smeltzer S, Bare B. Management of patients with renal disorder. In: Brunner & suddarth’s textbook of medical-surgical nursing. Philadelphia: Lippincott (2010). p. 1311–58.
179. Cheuk DKL, Yeung WF, Chung KF, Wong V. Acupuncture for insomnia. Cochrane Database Syst Rev (2012) 3:CD005472. doi: 10.1002/14651858.CD005472.pub3
180. Lee SK, Lim SM. Acupuncture for insomnia after stroke: a systematic review and meta-analysis. BMC Complement Altern Med (2016) 16:228. doi: 10.1186/s12906-016-1220-z
181. Kim SA, Lee SH, Kim JH, van den Noort M, Bosch P, Won T, et al. Efficacy of acupuncture for insomnia: a systematic review and meta-analysis. Am J Chin Med (2021) 49:1135–50. doi: 10.1142/S0192415X21500543
182. Zhao FY, Fu QQ, Kennedy GA, Conduit R, Zhang WJ, Wu WZ, et al. Can acupuncture improve objective sleep indices in patients with primary insomnia? A systematic review and meta-analysis. Sleep Med (2021) 80:244–59. doi: 10.1016/j.sleep.2021.01.053
183. M N. Dictionary of quality of life and health outcomes measurement. Milwaukee. WI: International Society for Quality of Life Research (2015).
184. Chan ASW, Ho JMC, Li JSF, Tam HL, Tang PMK. Impacts of COVID-19 pandemic on psychological well-being of older chronic kidney disease patients. Front Med (Lausanne) (2021) 8:666973. doi: 10.3389/fmed.2021.666973
185. Davey CH, Webel AR, Sehgal AR, Voss JG, Huml AM. Fatigue in individuals with end stage renal disease. Nephrol Nurs J (2019) 46:497–508.
186. Kidney Disease: Improving Global Outcomes (KDIGO) Glomerular Diseases Work Group. KDIGO 2021 clinical practice guideline for the management of glomerular diseases. Kidney Int (2021) 100:S1–S276. doi: 10.1016/j.kint.2021.05.021
187. Zotta F, Vivarelli M, Emma F. Update on the treatment of steroid-sensitive nephrotic syndrome. Pediatr Nephrol (2022) 37:303–14. doi: 10.1007/s00467-021-04983-3
188. Yang C, Hao Z, Zhang LL, Guo Q. Efficacy and safety of acupuncture in children: An overview of systematic reviews. Pediatr Res (2015) 78:112–9. doi: 10.1038/pr.2015.91
189. Tong X, Qiao Y, Yang Y, Liu H, Cao Z, Yang B, et al. Applications and mechanisms of tripterygium wilfordii hook. f. and its preparations in kidney diseases. Front Pharmacol (2022) 13:846746. doi: 10.3389/fphar.2022.846746
Keywords: complementary therapy, acupuncture, therapeutic mechanism, chronic kidney disease, end-stage renal disease
Citation: Liu X, Wang X, Ma H and Zhang W (2022) Mechanisms underlying acupuncture therapy in chronic kidney disease: A narrative overview of preclinical studies and clinical trials. Front. Nephrol. 2:1006506. doi: 10.3389/fneph.2022.1006506
Received: 29 July 2022; Accepted: 18 October 2022;
Published: 09 November 2022.
Edited by:
Samar Abd ElHafeez, Alexandria University, EgyptReviewed by:
Alex Siu-Wing Chan, Hong Kong Polytechnic University, Hong Kong SAR, ChinaCopyright © 2022 Liu, Wang, Ma and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wen Zhang, MzA2NzYyODI3QHFxLmNvbQ==
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.