
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Musculoskelet. Disord. , 13 December 2023
Sec. Systemic Inflammatory Joint Diseases
Volume 1 - 2023 | https://doi.org/10.3389/fmscd.2023.1281548
 Mohammed Awad Eltoum Ahmed1
Mohammed Awad Eltoum Ahmed1 Christiaan Scott2
Christiaan Scott2 Ayanda Gcelu1
Ayanda Gcelu1 Jonel Steffen3
Jonel Steffen3 Thuraya Isaacs4
Thuraya Isaacs4 Bridget Hodkinson1*
Bridget Hodkinson1*
Introduction: The high cost and concern of adverse events, particularly infections, limit the use of biologic therapies. We undertook this retrospective study to document their use for immune-mediated diseases, and explore the screening practices, efficacy, safety, and adherence to bDMARDs in a tertiary hospital.
Methods: A folder review of all adult and paediatric patients treated for IMDs with bDMARDs. Changes in disease activity were measured by disease-specific tools at 6, 12, 24-months and at the last available visit, and patient adherence to bDMARDs was explored by folder and pharmacy record review.
Results: We studied 120 folders; 145 bDMARDs were prescribed (23 patients switched bDMARD). BDMARDs prescribed included tumour necrosis factor inhibitors (TNFi) (76), rituximab (54), tocilizumab (9), anakinra (3), abatacept (1), ustekinumab (1) and tofacitinib (1). The vast majority of patients had an excellent response and achieved low disease activity or remission at their last available visit. Adverse events included severe infection (9) including two cases of tuberculosis (TB), mild skin reaction (6) and severe infusion reactions (4). Therapy was discontinued in 13 patients, most commonly due to infection (5), lack of response (4), or poor adherence (3). Poor adherence was noted in 8/120 (6.7%). Complete latent TB infection screening was performed in only 35 patients (29.2%). Screening for Hepatitis B, C and HIV was performed in 28 (23.3%), 62 (51.7%) and 61 (50.8%) patients, respectively. Only 20.8% and 20.0% received the influenza and pneumococcal vaccination.
Discussion and conclusion: Biologic therapy was effective, and the most important serious adverse effect was infection, which was significantly associated with TNFi therapy. Vaccination and screening for TB, viral hepatitis and HIV was suboptimal. Of concern, poor adherence to bDMARDs was frequently encountered.
Biologic disease modifying antirheumatic drugs (bDMARDs) are a class of immunosuppressive drugs produced by a biologic process and include monoclonal antibodies and fusion proteins. These therapies have dramatically improved outcomes in patients with severe immune-mediated diseases (IMD). Ten bDMARDs are currently registered and available in South Africa (SA) (1). These include tumour necrosis factor inhibitors (TNFi) which are infliximab (IFX), etanercept (ETN), adalimumab (ADA), golimumab (GOL); and the non-TNFi, which are abatacept (ABT), rituximab (RTX), tocilizumab (TCZ), ustekinumab (UTK), secukinumab (SCK), and anakinra (ANA). One targeted synthetic therapy is available: the JAK-inhibitor tofacitinib (TFC). Biologic therapies are indicated in patients with a poor response to conventional therapy, and recommendations for their use have been published by international and national bodies representing various subspecialties (2–4).
In SA, there is a heavy background burden of infectious diseases, including tuberculosis (TB), human immune virus (HIV), hepatitis B (HBV) and C virus (HCV) (5, 6). All bDMARDs increase the risk of serious infection (7). Reactivation of latent TB infection (LTBI) is of particular concern in patients treated with TNFi, and HBV reactivation is well described with RTX therapy (8). Thus screening for TB, HBV, HCV and HIV infections prior to initiating bDMARDs is recommended for all patients, together with vaccination (9–12).
The high cost of bDMARDs, together with the concern of serious infection, restricts the use of bDMARDs in resource-constrained settings and makes evaluation of their efficacy and safety vital. In the SA state-sector, resource constraints mean that very few state-sector patients are offered bDMARDs (13). In SA, there are considerable variations in access to bDMARDs between hospitals and provinces. Each clinical division needs to motivate for a biologic on a named patient basis to the hospital pharmacy therapeutics committee. Alternative ways of accessing a bDMARD include patient self-funding or medical insurance schemes.
We undertook this retrospective study to assess the number of patients, indications for, and specific biologic therapies used, in addition to monitoring efficacy, adverse events and screening practices. An understanding of these metrics will improve our current use and future planning of therapies for refractory patients. This study was approved by the University of Cape Town Health Research Ethics Committee.
This retrospective study includes all patients treated with bDMARDs for IMD at a tertiary referral hospital in SA. We included any patient given bDMARDs (minimum one dose) between January 2013 and December 2019, excluding those treated with bDMARDs for inflammatory bowel disease or hematological malignancy. To ensure all patients using bDMARDs were included, lists were obtained from each clinical department, and from the hospital pharmacy.
Folders were reviewed, and demographic and clinical details including the IMD details, disease duration, use of immunosuppressant before bDMARDs, and screening procedures were documented. Disease activity, measured by an accepted disease-specific tool, were documented at baseline, 6, 12 and 24 months, and at the last available encounter, and response was calculated comparing baseline and the last available visit. Adverse events and reason/s for discontinuation of treatment were documented, and patient adherence was assessed by reviewing the pharmacy records of prescriptions filled. Patients who missed two or more months of therapy were considered poorly adherent.
All statistical analyses were done using Stata 10 software (StataCorp, USA). The 2-tailed Fishers' exact test was used to assess significance, and a p-value of 0.05 was considered significant.
We reviewed 120 folders, with 145 bDMARDs prescribed (23 patients used more than 1 biologic), of which 87 were female and 33 male; 60 were adults and 60 pediatric patients (Table 1). The most frequent IMD's treated were rheumatoid arthritis (RA) and spondyloarthritis (SpA), and amongst children, juvenile idiopathic arthritis (JIA), systemic lupus erythematous (SLE) and uveitis. Of initial bDMARDs, the most prescribed were TNFi (total 60 patients (50%), including IFX (18 (12.4%)), ADA (24 (16.6%)), ETA (30(20.7%))), TCZ (9 (6.2%)), GOL (4 (2.8%)) and RTX (54 patients (37.2%). The vast majority of bDMARDs were state-funded, with seven funding their bDMARDs personally or through private medical insurance. Disease duration before starting bDMARD therapy was long: mean (SD) 7.08 (7.21) years, and the majority of patients had used numerous therapies prior to bDMARDs, reflecting the poor access to these expensive therapies.
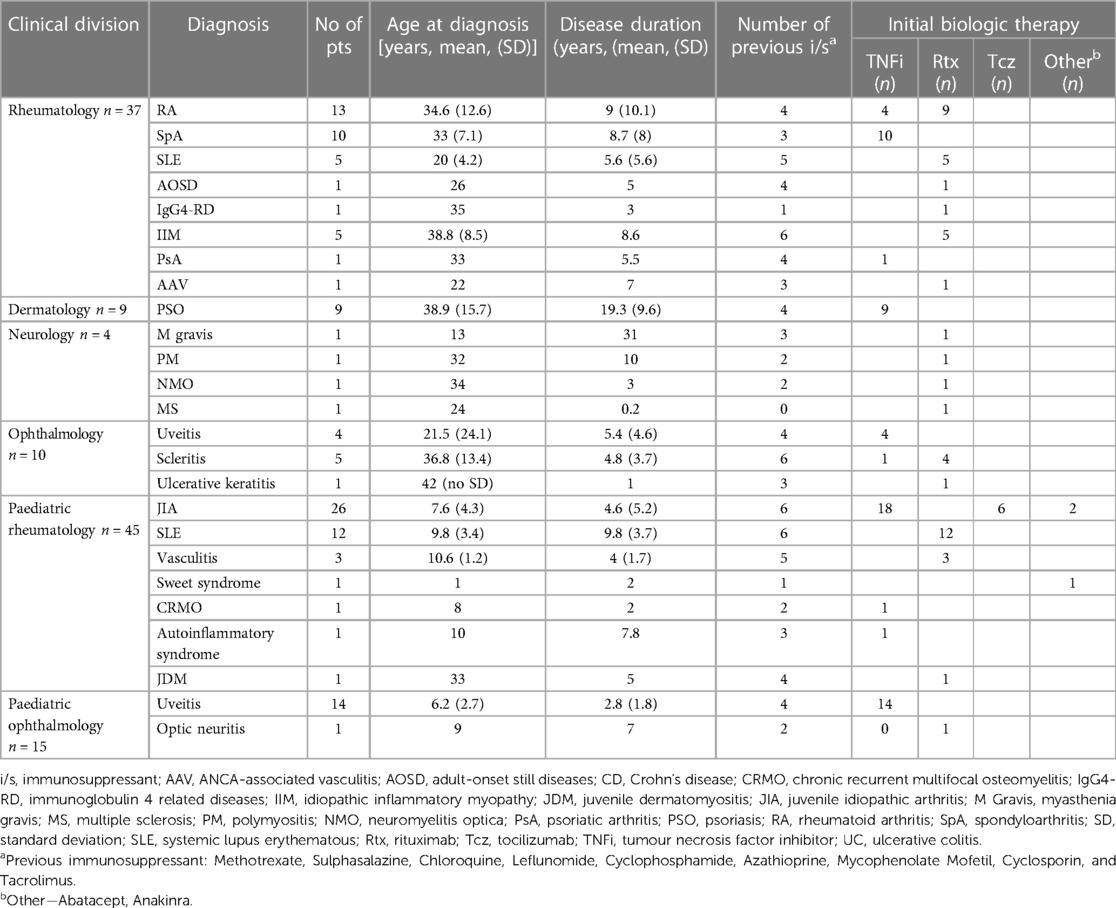
Table 1. Details of 120 patients prescribed biologics.
As expected, the vast majority of patients showed significant improvements in disease activity on biologic therapy (Tables 2, 3). Amongst RA and SpA patients, 66.6% achieved low disease activity, and improvements were seen in 88.8% of psoriasis (PSO) patients, 84.6% of JIA patients and all ophthalmology patients. There were a few patients who showed no improvement: adult-onset still disease (1), polymyositis (4), juvenile dermatomyositis (1) and two neurology patients. Most adult and paediatric SLE patients improved, except for two patients with nephritis with no improvement in any renal parameters. Very few patients had functional assessments at baseline or during bDMARD therapy, and C-reactive protein (CRP) tests were requested in only 11 patients.
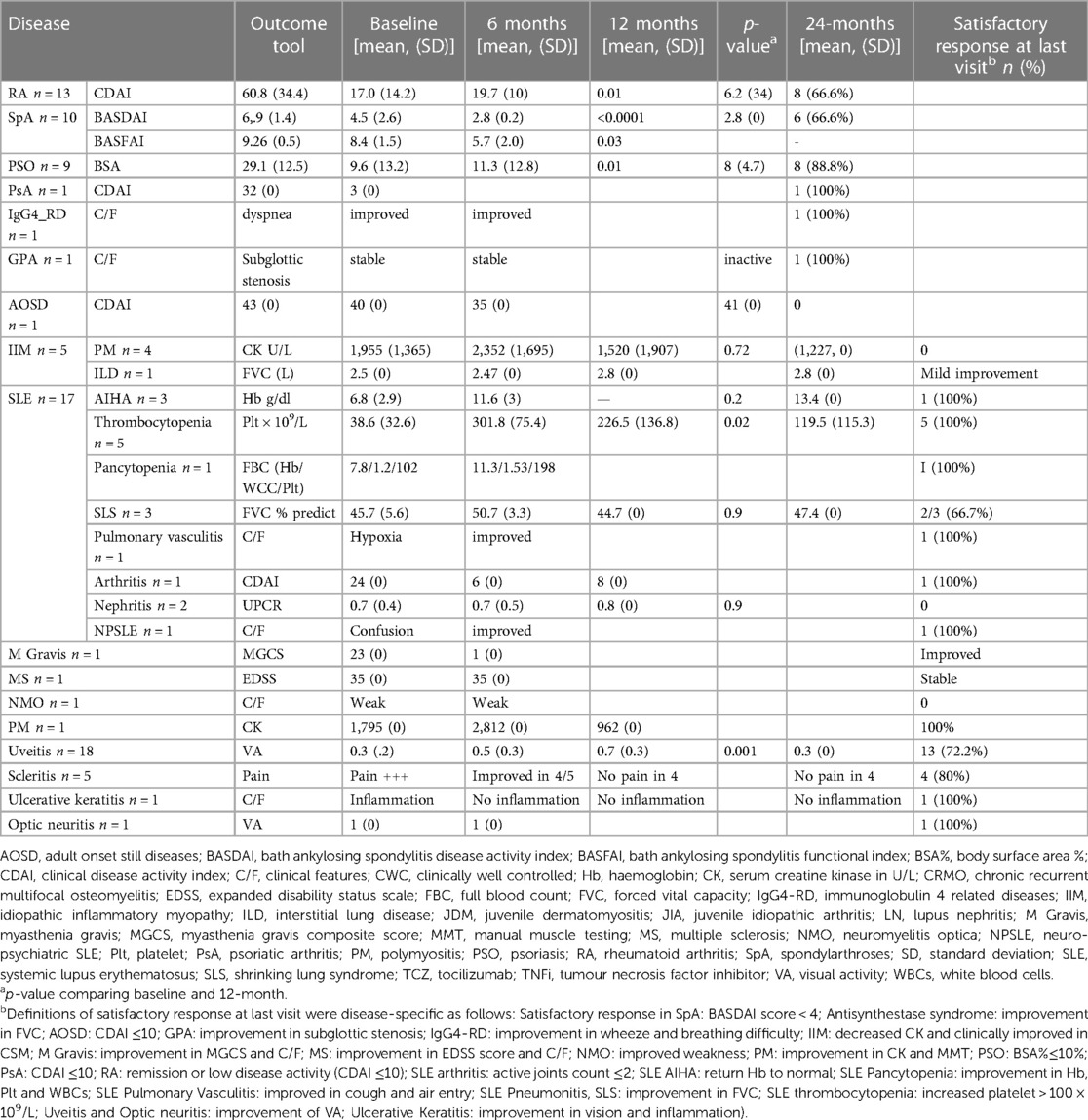
Table 2. Outcomes in adults treated with biologic therapy.
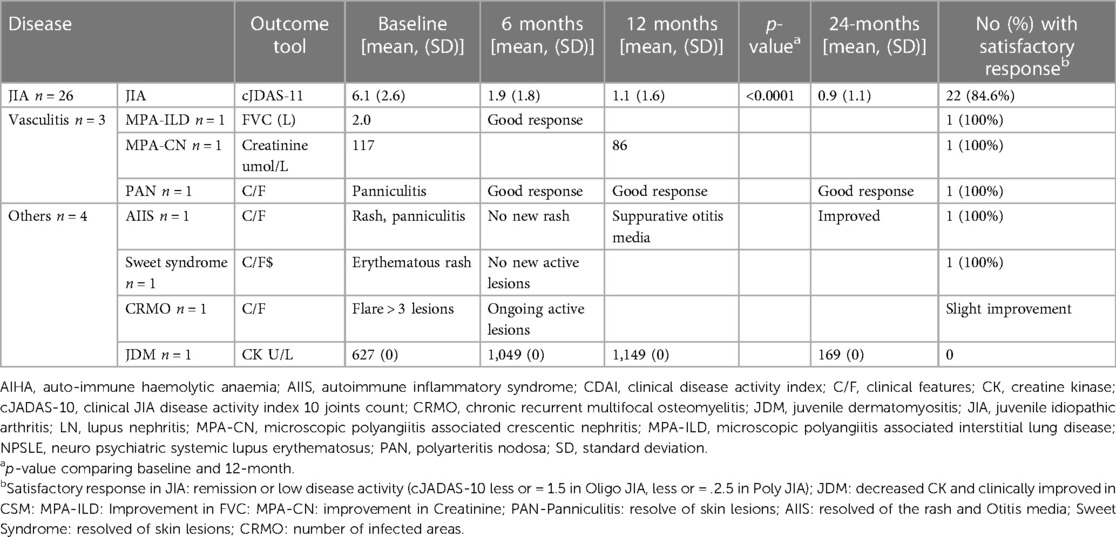
Table 3. Outcomes in paediatric patients treated with biologic therapies.
We reviewed the screening practices prior to biologic initiation (Table 4). In terms of TB, 9 (7.5%) patients reported previous TB; chest radiographs (CXR) were abnormal in 5 (4.2%) patients, normal in 109 (90.8%) patients and not performed in 6 (5.0%) patients. Screening for LTBI with a tuberculin skin test (TST) was positive in 9 (7.5%) patients, negative in 35 (29.2%), and not done in 76 (63.3%). Of the patients treated with TNFi, only 28/76 (36.8%) had a TST performed. Of these, 10/28 (35.7%) were from rheumatology, 9/28 (32.1%) from dermatology, 4/28 (14.3%) from paediatrics, and 5/28 (17.9%) from ophthalmology. Long-term INH prophylaxis for the duration of biologic therapy was given to 69/120 (57.5%) patients, including 26/76 (34.2%) of the patients prescribed TNFi therapy. Short term INH prophylaxis for 6-months was prescribed for 7/120 (5.8%) patients treated with any bDMARD, and 3/76 (3.9%) of patients prescribed TNFi therapy.
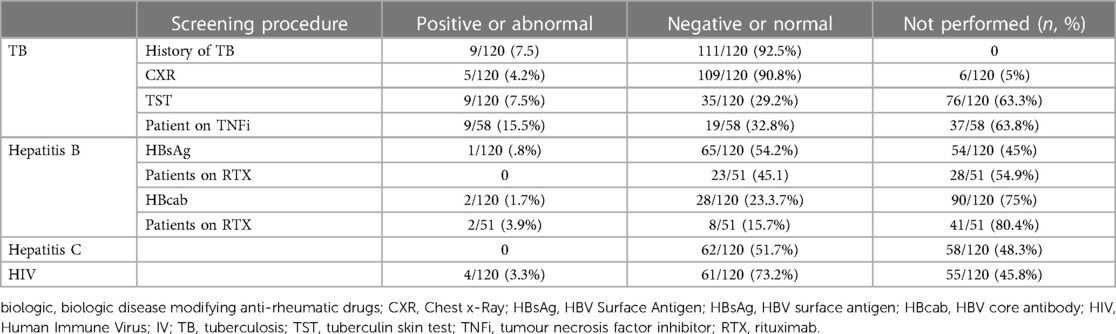
Table 4. Screening prior to prescribing biologics.
Screening for HBV surface antigen (HBsAg) was done in 66 (55%) patients, and by division, 31.8% in rheumatology, 45.5% in pediatric rheumatology, and 22.7% in all paediatric ophthalmology. Most patients (75%) had no testing for HBV core antibody (HBcAb), and 27 (36.5%) of these patients were treated with RTX. Screening for HCV was performed in 62 (51.7%) patients. Testing for HIV was performed in 65 (54.2%) patients, and three patients were HIV positive and virally suppressed before starting bDMARDs.
Few patients were vaccinated prior to initiating biologic: 20.8% and 20.0% of patients received influenza and pneumococcal vaccines respectively. We did not assess the use of HBV vaccine in non-immune patients.
Twenty-one adverse reactions were recorded, and infection is the commonest problem, followed by mild skin reaction to either subcutaneous injection or intravenous infusion (Table 5). Nine patients, eight of them using TNFi, had serious infection that leads to discontinuation of bDMARDs in five. These included two patients with TB, each treated with ETA or ADA. An HIV negative RA patient developed Pneumocystis Jiroveci pneumonia after nearly four years of ETN treatment. Two patients had septicaemia requiring hospital admission and intravenous antibiotics. Varicella zoster was diagnosed in a JIA patient treated with ETN for 3 years. Serious infection was significantly associated with exposure to TNFi, compared to patients treated with other bDMARDs (p = 0.006).

Table 5. Side effects, discontinuation and adherence to biologics.
Thirteen patients (11.9%) discontinued bDMARDs, with infection 5/13 (39.5%), poor response 4/13 (30.8%), or poor adherence 3/13 (23.1%) being the common reasons for discontinuation. One JIA patient stopped treatment after nine months of TCZ due to suspected macrophage activation syndrome. One patient became HIV positive during biologic treatment, had inactive disease and the biologic was stopped.
Of the three HIV positive patients, two had polymyositis, and received RTX after failing numerous immunosuppressive therapies. Both had a mild to moderate clinical and laboratory response to RTX. The third patient with JIA achieved remission with ETN. None of these patients experienced adverse events and they all had undetectable viral loads and normal CD4 count throughout treatment.
Poor adherence to bDMARDs therapy was observed in 8 patients (6.7%), apparent from pharmacy records where seven patients failed to collect their repeat scripts every month, and one patient had to stop BDMARDs because of the cost. Four patients were lost to clinic follow-up, and no details are available despite our attempts to trace these patients. These patients may have relocated or may have died.
There were 23 (19.2%) patients who switched bDMARDs, two of whom switched more than once (Supplementary Tables 1 and 2). The commonest reason for switching bDMARDs was a poor response to bDMARDs (12 patients), infection (4 patients) or infusion reaction (2 patients). Most patients had an excellent response to the second biologic.
We have described 120 patients using bDMARDs for IMD at a tertiary referral hospital and show that the commonest class of bDMARDs prescribed was TNFi, followed by RTX, with the most common indications being RA, PSO and uveitis. Most bDMARDs were state-funded. Encouragingly, more than two thirds of patients had an excellent response to bDMARDs, despite the long disease duration and numerous immunosuppressants used before starting the bDMARD. Serious infections occurred in nine patients (7.5%) and were significantly associated with TNFi use. This high risk of infection with bDMARDs is described elsewhere (14, 15).
Validated disease assessment scores were documented in the folders of most patients. A serum CRP was seldom performed, and this may be an area for improvement, given that CRP is a useful measure of inflammation, and may also be an indicator of infection, including TB (16). The assessment of functional status was very poor, with no regular assessment in either adult or pediatric rheumatology patients. Formal documentation of functional disability is vital to assess how symptoms affect patients, and to measure whether therapy is improving the quality of life (17).
Screening for LTBI is recommended by international and local recommendations before starting bDMARDs (18–20),. Patients with a positive LTBI screening test, or considered to be at high risk and therefore offered long term prophylaxis, are prescribed isoniazid (INH) for four weeks before commencing bDMARD therapy. Adherence to screening was poor, and this is of concern given the high prevalence of TB in SA, and particularly amongst state-sector patients in the Western Cape (21). Although most patients had a CXR, almost a third of patients using bDMARDs had no documented TST. Because of the relatively high cost, the interferon-gamma release assay is currently not available in state-sector hospitals, thus no results for this rest are available. Reasons for the low number of patients screened for LTBI may include the decision in some subspecialties to prescribe long-term INH prophylaxis to all patient on TNFi, regardless of TST result, and a limited or intermittent supply of purified protein derivative in SA. Elsewhere, good uptake of LTBI screening recommendations and reduction in TB incidence has been reported (22, 23). In the current study, chemoprophylaxis with INH was only prescribed for a third of patients on TNFi, despite recommendations by some groups that INH prophylaxis be offered, either long or short-term, to all patients receiving TNFi therapy. In addition, less than a third of patients had complete HBV tests, and only half had HCV tests. Studies from elsewhere have shown that adherence to viral screening recommendations is poor (24). Although SA has one of the highest prevalences of HIV infection in the world, only half of patients using bDMARDs in this study had an HIV test. There is currently little literature available regarding the safety of bDMARDs in HIV positive patients, but careful monitoring is recommended (25, 26). Immunization for influenza and pneumococcus was suboptimal.
Almost 7% of patients were poorly adherent to their bDMARDs, with a further 4 patients lost to followup. This is described elsewhere: in a recent study of patients treated with bDMARDs in five different European countries, 56.3% of patients missed a dose during the 6 months that the study was conducted. Reasons for noncompliance included “feeling better and didn’t need it”, “thinking the therapy was not helping”, or sickness, surgery or infection (27). Adherence to bDMARDs therapy amongst PSO patients in the USA was low with a high discontinuation rate, and a prospective study from the SA private-sector showed a third of the patients discontinue TNFi within one year of treatment (28, 29). We recommend intensive and ongoing education and support for all patients taking bDMARDs.
Limitations of this study include the retrospective design, with missing folders, and missing details including functional disability, and CRP. The other limitation was the lack of specific measurement of activity in some diseases. Further, we did not capture immunosuppressive therapy co-prescribed with bDMARDs.
In conclusion, bDMARDs in our hospital were effective, and generally safe, with common adverse effects being mild skin and transfusion reactions. Severe infection, including TB, was associated with TNFi therapy. We note poor adherence to screening and vaccination recommendations prior to commencing bDMARDs. In addition, adherence to bDMARDs was suboptimal. We recommend standard operating procedures for all patients using bDMARDs across all disciplines, including details of screening tests before starting bDMARDs, assessment of functional disability patients, and intense patient education and counseling. Further studies are planned to assess the success of these interventions.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by University of Cape Town Human Research Ethics Committee. The studies were conducted in accordance with the local legislation and institutional requirements.
MA: Data curation, Formal Analysis, Writing – original draft. CS: Writing – review & editing. AG: Writing – review & editing. JS: Writing – review & editing. TI: Writing – review & editing. BH: Conceptualization, Data curation, Formal Analysis, Methodology, Project administration, Supervision, Visualization, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmscd.2023.1281548/full#supplementary-material
1. Tarr G, Hodkinson B, Hodkinson B, Reuter H, Reuter H. Superheroes in autoimmune warfare: biologic therapies in current South African practice. South African Med J. (2014) 104(11):787–91. doi: 10.7196/SAMJ.8947
2. Hodkinson B, Van Duuren E, Pettipher C, Kalla A. South African recommendations for the management of rheumatoid arthritis: an algorithm for the standard of care in 2013. S Afr Med J. (2013) 103(8 Pt 2):576–85. doi: 10.7196/samj.7047
3. Angeles-Han ST, Ringold S, Beukelman T, Lovell D, Cuello CA, Becker ML, et al. American college of rheumatology/arthritis foundation guideline for the screening, monitoring, and treatment of Juvenile idiopathic arthritis-associated uveitis. Arthritis Care Res. (2019) 71(6):703–16. doi: 10.1002/acr.23871
4. Dick AD, Rosenbaum JT, Al-Dhibi HA, Belfort R, Brézin AP, Chee SP, et al. Guidance on noncorticosteroid systemic immunomodulatory therapy in noninfectious uveitis: fundamentals Of care for uveitiS (FOCUS) initiative. Ophthalmology. (2018) 125(5):757–73. doi: 10.1016/j.ophtha.2017.11.017
5. WHO. WHO. Global Hepatitis Report, 2017. (2017). Available at: https://www.who.int/en/news-Room/fact-Sheets/detail/hepatitis-C (Accessed March 24, March 2019).
7. Nam JL, Takase-Minegishi K, Ramiro S, Chatzidionysiou K, Smolen JS, van der Heijde D, et al. Efficacy of biological disease-modifying antirheumatic drugs: a systematic literature review informing the 2016 update of the EULAR recommendations for the management of rheumatoid arthritis. Ann Rheum Dis. (2017) 76(6):1108–13. doi: 10.1136/annrheumdis-2016-210713
8. De Keyser F. Choice of biologic therapy for patients with rheumatoid arthritis: the infection perspective. Curr Rheumatol Rev. (2011) 7(1):77–87. doi: 10.2174/157339711794474620
9. Furer V, Rondaan C, Heijstek MW, Agmon-Levin N, van Assen S, Bijl M, et al. 2019 update of EULAR recommendations for vaccination in adult patients with autoimmune inflammatory rheumatic diseases. Ann Rheum Dis. (2020) 79(1):39–52. doi: 10.1136/annrheumdis-2019-215882
10. Abreu C, Sarmento A, Magro F. Screening, prophylaxis and counselling before the start of biological therapies: a practical approach focused on IBD patients. Dig Liver Dis. (2017) 49(12):1289–97. doi: 10.1016/j.dld.2017.09.002
11. Smith CH, Jabbar-Lopez ZK, Yiu ZZ, Bale T, Burden AD, Coates LC, et al. British association of dermatologists guidelines for biologic therapy for psoriasis 2017. Br J Dermatol. (2017) 177(3):628–36. doi: 10.1111/bjd.15665
12. Scott C, Chan M, Slamang W, Okong'o L, Petty R, Laxer RM, et al. Juvenile arthritis management in less resourced countries (JAMLess): consensus recommendations from the cradle of humankind. Clin Rheumatol. (2019) 38(2):563–75. doi: 10.1007/s10067-018-4304-y
13. Hodkinson B, Blockman M. Strategies and ethics to ensure equitable access to biological medicines in the treatment of autoimmune inflammatory diseases. Curr Allergy Clin Immunol. (2018) 31(4).
14. Singh JA, Wells GA, Christensen R, Tanjong Ghogomu E, Maxwell LJ, MacDonald JK, et al. Adverse effects of bDMARDs: A network meta-analysis and Cochrane overview. Cochrane Database Syst Rev. (2011) 2011(2):CD008794. doi: 10.1002/14651858.CD008794.pub2
15. Chiu YM, Chen DY. Infection risk in patients undergoing treatment for inflammatory arthritis: non-bDMARDs versus bDMARDs. Expert Rev Clin Immunol. (2020) 16(2):207–28. doi: 10.1080/1744666X.2019.1705785
16. Gossen N, Kostev K. Reduction in C-reactive protein with biologic drugs in rheumatoid arthritis and spondylitis patients in German rheumatologist practices. Value Heal. (2015) 18(7):A635. doi: 10.1016/j.jval.2015.09.2252
17. Wolfe F. A reappraisal of HAQ disability in rheumatoid arthritis. Arthritis Rheum. (2000) 43(12):2751–61. doi: 10.1002/1529-0131(200012)43:12?3.0.CO;2-6
18. Martínez-López A, Rodriguez-Granger J, Ruiz-Villaverde R. Screening for latent tuberculosis in the patient with moderate to severe psoriasis who is a candidate for systemic and/or biologic therapy. Actas DermoSifiliogr. (2016) 107:207–14. doi: 10.1016/j.adengl.2016.01.024
19. Navas C, Torres-Duque CA, Munoz-Ceron J, Alvarez C, García JR, Zarco L, et al. Diagnosis and treatment of latent tuberculosis in patients with multiple sclerosis, expert consensus. On behalf of the Colombian Association of Neurology, Committee of Multiple Sclerosis. Mult Scler J Exp Transl Clin. (2018) 4(1):205521731775220. doi: 10.1177/2055217317752202
20. Theis VS, Rhodes JM. Review article: Minimizing tuberculosis during anti-tumour necrosis factor-alpha treatment of inflammatory bowel disease. Aliment Pharmacol Ther. (2008) 27(1):19–30. doi: 10.1111/j.1365-2036.2007.03553.x
21. Wood R, Lawn SD, Caldwell J, Kaplan R, Middelkoop K, Bekker LG. Burden of new and recurrent tuberculosis in a major South African city stratified by age and HIV-status. PLoS One. (2011) 6(10):e25098. doi: 10.1371/journal.pone.0025098
22. Mponponsuo K, Fisher D. 755. Clinical Adherence to Latent Tuberculosis Screening Recommendations in Adults with Inflammatory Bowel Disease (IBD) Prior to Biologic Therapy. Open Forum Infect Dis. (2018) 5:S271–71. doi: 10.1093/ofid/ofy210.762
23. Carmona L, Gómez-Reino JJ, Rodríguez-Valverde V, Montero D, Pascual-Gómez E, Mola EM, et al. Effectiveness of recommendations to prevent reactivation of latent tuberculosis infection in patients treated with tumor necrosis factor antagonists. Arthritis Rheum. (2005) 52(6):1766–72. doi: 10.1002/art.21043
24. Van der Have M, Belderbos TDG, Fidder HH, Leenders M, Dijkstra G, Peters CP, et al. Screening prior to biological therapy in Crohn's disease: adherence to guidelines and prevalence of infections. Results from a multicentre retrospective study. Dig Liver Dis. (2014) 46(10):881–86. doi: 10.1016/j.dld.2014.07.006
25. Fink DL, Hedley L, Miller RF. Systematic review of the efficacy and safety of biological therapy for inflammatory conditions in HIV-infected individuals. Int J STD AIDS. (2017) 28:110–19. doi: 10.1177/0956462416675109
26. Nakamura M, Abrouk M, Farahnik B, Zhu TH, Bhutani T. Psoriasis treatment in HIV-positive patients: a systematic review of systemic immunosuppressive therapies. Cutis. (2018) 101(1):38–42.
27. Chanroux L, Mboge F, Baldock D. Patient adherence with biologic therapy in rheumatoid arthritis: a real-world review of compliance. Arthritis Rheumatol. (2016) 68(Supplement 10):2927–28. doi: 10.1002/art.39977
28. Doshi JA, Takeshita J, Pinto L, Li P, Yu X, Rao P, et al. Biologic therapy adherence, discontinuation, switching, and restarting among patients with psoriasis in the US Medicare population. J Am Acad Dermatol. (2016) 74(6):1057–1065.e4. doi: 10.1016/j.jaad.2016.01.048
Keywords: South Africa, bDMARDs, efficacy, screening, adverse events
Citation: Ahmed MAE, Scott C, Gcelu A, Steffen J, Isaacs T and Hodkinson B (2023) Screening practices, efficacy, safety and adherence to biologic therapies in a South African tertiary hospital. Front. Musculoskelet. Disord. 1:1281548. doi: 10.3389/fmscd.2023.1281548
Received: 22 August 2023; Accepted: 10 October 2023;
Published: 13 December 2023.
Edited by:
Hirofumi Shoda, The University of Tokyo, JapanReviewed by:
Crescenzio Scioscia, University of Bari Aldo Moro, Italy© 2023 Ahmed, Scott, Gcelu, Steffen, Isaacs and Hodkinson. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bridget Hodkinson ZHJicmlkZ2V0QGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.